
Abstract
The rate of orthopedic implant use is increasing, and this trend is expected to continue in the next decades due to aging population and improving medical care. Biomaterials can be grouped under the four headings metallic, ceramic, polymeric, and composite materials. In addition to the competency of the surgeon, the success of these synthetic or natural biomaterials is dependent on the properties of the biomaterial, biocompatibility of the implant, and the condition of the recipient tissue. Despite major advances in orthopedic biomaterials and allergic and foreign body response, biomaterials-related complications such as implant loosening and infection are still restricting the use of biomaterials in daily practice. Surface modification of biomaterials has been developed for tailoring of surface properties of the orthopedic implants. These altered surface properties mostly improve tissue-biomaterial interactions and also mechanical characteristics of the implants.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara Learning OutcomesAfter reading this chapter, you will understand the following:
-
1.
Rationale for use of the different biomaterials in clinical applications
-
2.
Structure and properties of different metals commonly used for making orthopedic implants
-
3.
The general definition, classifications, and common properties of different bioceramics
-
4.
Principles underlying surface modification techniques
-
5.
Biological response to orthopedic implants
- Biocompatibility:
-
Acceptance of an artificial implant by the surrounding tissues and by the body as a whole.
- Biodegradation:
-
Materials that could be broken down by nature either through hydrolytic mechanisms without the help of enzymes or enzymatic mechanism.
- Biomaterial:
-
A synthetic material used to make devices to replace part of a living system or to function in intimate contact with living tissue.
- Bone cement:
-
Mixture of polymethylmethacrylate powder and methylmethacrylate monomer liquid to be used as a grouting material for the fixation of orthopedic joint implants.
- Calcium phosphate:
-
A family of calcium phosphate ceramics including calcium phosphate, hydroxyapatite, and tricalcium phosphate (TCP) are used to substitute or augment bony structures and deliver drugs.
- Corrosion:
-
Unwanted reaction of metal with environment.
- Fibrous membrane:
-
Thin layer of soft tissue which covers an implant to isolate from the body.
- Graft:
-
Set of living cells, living tissue, or living organ surgically inserted into a body to replace a damaged part or a defect of an organ. This is an autograft if the donor and recipient is the same individual; this is an allograft when the donor and recipient belong to the same species but are genetically distinct; this is a xenograft when the donor and recipient are of different species.
- Hydroxyapatite:
-
A calcium phosphate ceramic with a calcium-to-phosphorus ratio of 5/3 and a nominal composition Ca1O(PO4)6(OH)2. Hydroxyapatite is the mineral constituent of bone.
- Implant:
-
An implant is a medical device (apparatus, prosthesis, etc.) made of one or several biomaterials, which is introduced into the human body in the long term to replace an organ or to supply a function or to treat a disease.
- Osseointegration:
-
Direct contact of bone tissues to an implant surface without fibrous membrane.
- Osteolysis:
-
Dissolution of bone mineral from the bone matrix.
- Passivation:
-
Production of corrosion resistance by a surface layer of reaction products.
- Prosthesis:
-
A device implanted in the body to supply a missing organ (limb, tissue) or to restore a deficient function.
- Stress shielding:
-
Bone is protected from stress by the stiff implant.
-
1.
Refer to Fig. 1.1 and consider a 66-year-old patient with a total knee arthroplasty. This modular knee arthroplasty implant is composed of a cobalt-chrome femoral component, titanium alloy tibial component, and a polyethylene insert. Would you be concern of crevice and galvanic forms of corrosion in this patient?
Fig. 1.1 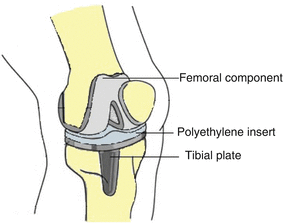
Total knee artroplasty
When you have a total knee replacement, the surgeon removes damaged cartilage and bone from the surface of the knee joint and replaces them with a metal and plastic. Because of the modularity of the cobalt-chromium femoral and titanium tibial components, crevice corrosion will be relevant. Because there is a polyethylene insert separating the cobalt-chromium component and the titanium plate, galvanic corrosion will be limited. Though wear through of the liner would present other concerns as well [31].

In engineering any substance that is used for manufacturing is called material. Biomaterials are natural or synthetic materials that treat, augment, or replace tissues and organs. Biomaterials are utilized to fulfill or support the task of living tissue in the human body which continuously or periodically comes into contact with body fluids. Biomaterials are different from other materials in the sense that they must have the ability to remain in contact with tissues from the human body without creating too much adverse or a hostile response. If a material is used in a human body, it has to be able to resist mechanical forces and chemical effects. Also this material is expected to exhibit osseointegration properties [1–4].
Men have used various materials to replace organs or parts of organs since the beginning of history. Glass for eyes, wood for teeth, gold in dentistry, and linen, horsehair, and cotton for suture were some examples of the uses of materials for various replacements. These materials were those used in everyday life. The evidence of their use as implants or prostheses were mainly discovered on human skeletons during the excavations of sites from different ancient civilizations: Egyptian, Roman, and Greek. Gold, as a metal, appears to be one of the earliest and main materials used by old civilizations, and, incredibly, it is still used today [5].
Musculoskeletal disorders are the principal cause of disability in all over the world and are responsible for chronic conditions. For a very long time, the use of materials mainly was more cosmetic than functional. Then surgeons and scientists were interested in the subject, and they developed functional materials for orthopedic and other surgeries. Because of their mechanical properties and resistance to corrosion, simple metals were chosen in the beginning, but incredible development of the plastics and ceramic sciences make possible the use of new materials, with diverse physicochemical and mechanical properties. The rate of orthopedic implant use is increasing, and this trend is expected to continue in the next decades due to aging population and improving medical care. Nowadays, the development of new biomaterials and their use in medicine has been an important domain. Despite major advances in orthopedic biomaterials and allergic and foreign body response, biomaterials-related complications such as implant loosening and infection are still restricting the use of biomaterials in daily practice [1–6].
The response of a material to deforming forces is characterized by its mechanical properties. Mechanical properties of biomaterials determine the deformation, failure behavior, and fracture of materials under the action of tensile, compressive, torsional, or combinations of these forces. As an example, mechanical properties would be very important for a joint replacement implant because it would be expected to withstand heavy loads generated during walking, and such loads can be very high. To determine the mechanical properties of a material, force versus deformation tests are conducted. In these tests, samples of a material are loaded at a constant rate, and both the deformation and the force required to cause that deformation are measured at various time points.
Biomaterials can be grouped under the four headings metallic, ceramic, polymeric, and composite materials. The biomaterials most commonly used in orthopedic surgery are metallic implants such as steel, cobalt-chrome, or titanium alloys, as they provide satisfactory mechanical performance. Screws, plates, and nails used for the treatment of fractures, hip and knee prostheses used in joint diseases, and spine implants are typical examples of metallic biomaterials used in orthopedic surgery. Most commonly used implantation devices in orthopedic surgery are made of metallic, ceramic, and polymeric biomaterials [1–4].
Metals
All materials are constituted of atoms that are bonded together by interactions. In metals, metallic atoms are closely packed in a crystal structure, and atoms are held together through a nondirectional strong metallic bond. Metals are group of materials with high corrosion resistance, biocompatibility, high wear resistance, and excellent mechanical properties such as good ductility and strength. Due to their crystal structure and strong metallic bonds with superior mechanical properties, they are used frequently as implant material. Metals have been preferred practically completely for load-bearing applications, such as joint arthroplasties and fracture fixation wires, pins, screws, and plates. Although pure metals can be used, metal alloys are preferable. Some characteristics, such as strength and corrosion resistance of metal implants, can be improved when used as a metal alloy by varying the composition or by using different manufacturing processes [7, 8].
Convenient mechanical properties, corrosion resistance, biocompatibility, and reasonable cost are the main considerations in preferring metal alloys for implant use. It is important to know the physical and chemical properties of the different metal alloys used in a surgery as well as their interaction with the host tissue of the human body, to be able to make knowledgeable decisions. Elastic modulus, yield stress, ultimate tensile stress, and fatigue stress are the most important characteristics of a metal implant defining its strength and stiffness. These properties of a metal can be seen from stress-strain curves. The strength characteristics of a metal can be influenced by the grain size, inclusion content, and surface porosity. A metal with a smaller grain size has a higher tensile and fatigue strength compared to the larger grain size. High surface porosity and too much inclusion content will weaken the metals [7, 8].
Extracellular fluid of human body contains various ions such as dissolved oxygen, chloride, and hydroxide. Therefore, the human body with a different ion concentration and pH changes in fluids is a highly corrosive environment for metals when used as implants. Corrosion is degradation of materials’ properties due to interactions with their environments, and corrosion of most metals is inevitable. While primarily associated with metallic materials, all material types are susceptible to degradation. Corrosion weakens the material; also corrosion products that enter into tissues can cause damage to cells. Three types of corrosion are common in implant materials: fatigue, galvanic, and crevice corrosion. Fatigue is the weakening of a material caused by repeatedly applied loads. It is the progressive and localized structural damage that occurs when a material is subjected to cyclic loading. If the loads are above a certain threshold, microscopic cracks will begin to form at the stress concentrators such as the surface and grain interfaces. Eventually a crack will reach a critical size, and the structure will fracture. Galvanic corrosion occurs when two different metals have physical or electrical contact with each other. An electric current is established between two metals that cause degradation. To avoid tragic galvanic corrosion, stainless steels should never be used with cobalt or titanium alloys. Crevice corrosion is a localized form of corrosion occurring in confined spaces, to which the fluid in contact with a metal becomes stagnant, resulting in a local oxygen depletion and decrease in pH. Stainless steel corrodes more readily than other alloys. Approaches available for controlling corrosion include the application of protective coatings to metal surfaces to act as a barrier or alteration of an alloy chemistry to make it more resistant to corrosion and the treatment of the surface of a metal to increase its resistance to corrosion. The chromium and molybdenum content of alloys produces a corrosion-resistant surface layer. Titanium alloys have an oxide passive film layer that provides their corrosion resistance. Nitric acid, by forming an oxide surface layer, is used to make the surface of the implant passive to corrosion [1–4].
The mechanical properties of the metal are important and should satisfy the requirements of the specific application in the body. For instance, when a metal is used to augment a bone, the elastic modulus of the metal should be ideally equivalent to that of the bone. If the elastic modulus of the metal is greater than that of bone, then the load experienced by the bone is reduced due to a phenomenon known as stress shielding. This can cause the bone to remodel to adjust to the lower load and eventually result in the loss of bone quality. Metals are passed through a series of processes to provide materials desired properties such as harder, softer, or durable.
Three material groups dominate biomedical metal implants: stainless steel, cobalt-chromium alloy, and titanium alloys. Other metals used in the biomedical industry include nitinol, tantalum, and magnesium. Nitinol, a nickel-titanium alloy, belongs to the class of shape memory alloys. At low temperature, these alloys can be plastically deformed but return back to their original predeformed shape when exposed to a high temperature. Tantalum (Ta) has been used for making biomedical implants and devices, either in its commercially pure (99.9 %) state or as an alloying element in titanium alloys. Tantalum is well known for its excellent corrosion resistance and biocompatibility because of a stable surface oxide layer. It has also been used as coatings on other metallic devices, such as 316 L stainless steel, to improve the substrate’s corrosion resistance and to enhance biocompatibility. The use of magnesium (Mg) for orthopedic applications dates back nearly half a century. Mg is well known for its light weight and biodegradability. The density, elastic modulus, yield strength, and fracture toughness of Mg are close to that of bone [1–9].
Stainless Steel
Stainless steel was successfully used as the first material in surgery. Stainless steel is essentially iron and carbon alloy which contain at least 10, 5 % chromium. Molybdenum and a small amount of manganese and silicon are added. The corrosion resistance of stainless steel is due to the formation of chromium oxide (Cr2O3) on its surface. The corrosion-resistant properties of stainless steel can be further improved by increasing the chromium content. These properties and other physical and mechanical properties can also be improved by the addition of several other alloying elements. For instance, addition of molybdenum increases pitting corrosion resistance, while the addition of nitrogen increases mechanical strength and pitting corrosion resistance.
Stainless steel is the common name for a number of different steels. Stainless steels with a smaller percentage of carbon, which are labeled 316 L, are used for orthopedic implants. The letter “L” represents low carbon content (<0.030 %). The low carbon content is highly preferred for excellent corrosion resistance. 316 L stainless steel consists of primarily iron (60–65 %), chromium (17–20 %), nickel (12–14 %), and smaller amounts of molybdenum, manganese, copper, carbon, nitrogen, phosphorous, silicon, and sulfur.
Stainless steel has been used for wide range of application due to easy availability, lower cost, excellent fabrication properties, accepted biocompatibility, and great strength. Despite composition modification, stainless steels are susceptible to corrosion; therefore, they are most appropriate for temporary implants such as plates, screws, hip nails, and intramedullary nails. The most common reason for corrosion of stainless steels is incorrect metal composition, which increases the chance that galvanic corrosion will occur. Molybdenum that is added in 316 L stainless steels hardens the passive layer and increases corrosion resistance. Another reason for corrosion is mismatch of implant components, especially when plates and screws are used. It is important to use implants manufactured by the same company with similar lots to avoid compositional differences of implant components [1–8].
Cobalt-Chrome Alloys
The cobalt-based alloys are characterized by high fatigue and wear resistance and high tensile strength levels. These properties make them desirable for load-bearing and articulating surface applications, appropriate for applications requiring long time use and ability to resist fracture. Cobalt-chromium alloys can be separated into two types: first one which has been used for making artificial joints consists of Cr (27–30 %), Mo (5–7 %), and Ni (2.5 %) and the second one which has been used for making the stems of prostheses contains Cr (19–21 %), Ni (33–37 %), and Mo (9–11 %). Cobalt-based alloys are highly resistant to corrosion due to spontaneous formation of passive oxide layer within the human body. Molybdenum is added to produce finer grains which result in higher strength. Elastic modulus of the alloy containing cobalt is greater than that of stainless steel. The corrosion products of Co-Cr-Mo are more toxic than those of stainless steel [1–4].
Titanium Alloys
Titanium alloys due to its outstanding characteristics such as lightweight, high strength, good resistance to corrosion, improved biocompatibility, and better elastic modulus are a suitable choice of metal for implantation. Although it is a lightweight material, titanium provides excellent mechanical and chemical properties comparable to stainless steel and cobalt-chromium alloy. Long-term use of titanium alloys has raised some concerns because of releasing aluminum and vanadium ions which might be related to Alzheimer disease and neuropathy.
The mechanical properties of materials are very important when using load-bearing orthopedic implants. Some mechanical properties of metallic biomaterials are listed in Table 1.1. The mechanical properties of an implant depend not only on the type of metal used but also on the processes used to manufacture the material and implant. The elastic moduli of the most metals listed in Table 1.2 are many times greater than that of natural bone. Titanium alloys have a surface passive oxide layer which is mainly responsible for its extremely good corrosion resistance and biocompatibility. Titanium alloy plates are gaining popularity because of these material characteristics [1–5].
Polymers
Polymers are organic materials that form large chains made up of many repeating units. Compared to metallic implants, polymeric materials are used on a variety of applications in surgery. Flexibility, resistance to biochemical attack, good biocompatibility, to be lightweight, and to be available in diverse compositions are their unique properties. Polymethyl methacrylate (PMMA) and ultrahigh-molecular-weight polyethylene (UHMWPE) are two main classes of polymer used in orthopedic surgery.
Polymers have the advantage that they can be easily formed into desired shapes using a variety of techniques. Polymers can also be made reactive so that different chemical molecules can be attached to the surface of implants in order to make them more compatible with the surrounding environment in the body. Some polymers are biodegradable in the body. If used to make implants for temporary needs, these polymers offer the advantage that the implant can gradually biodegrade within the body after it has served its function, thus mitigating the potential for any long-term complications. If a biodegradable polymer is used as an implant, it can potentially also be designed to release therapeutic drugs or growth factors during the degradation process. Composition and structure of the macromolecular chains and their molecular weight affect the mechanical properties of polymers. Polymers are usually not as robust or rigid as metals or ceramics and therefore may not be the right choice when an implant is required to carry large loads in its function.
Polymethyl Methacrylate (PMMA)
PMMA is used as bone cement in orthopedics to stabilize joint prostheses as well as a bone substitute in pathologic vertebral and other fractures. The success of any joint prostheses used with bone cement is dependent on the performance of the PMMA cement. Bone cement does not adhere well to either metal or adjacent bone. It is not an adhesive and functions mostly as a space-filler or grout. Increased surface roughness of the metal and higher porosity of adjacent bone both result in better infiltration of the polymer and better interlocking. On the other hand, the presence of air bubbles at the metal interface leads to decreased adhesion and possible failure.
The bone cement used clinically is available as a kit that contains a dry component and a liquid component. The dry powder component consists of prepolymerized PMMA beads, barium sulfate (opacifier), and dibenzoyl peroxide (initiator). The initiator is the source of free radicals that starts the reaction. The liquid component contains the MMA monomer and N,N-dimethyl-p-toluidine, which is an accelerator. Once the solid and liquid components are mixed, the initiator, aided by the accelerator, produces free radicals which drive the polymerization of the monomer. The polymerization reaction can cause tissue damage due to an increase in temperature. The polymerization reaction is characterized by different time periods. The dough time typically lasts for 2–4 min and is the time elapsed from the point of the initial mixing of the solid-liquid components to the time when the mixture has reached enough viscosity that it can be handled as a mass. The time period between the end of the dough time and the point where the polymer is too hard to mold is known as the working time.
The inclusion of antibiotics with bone cement has led to a decrease in infections. However, the inclusion of antibiotics also leads to a lower strength for the PMMA. Other potential problems with the use of PMMA in medical applications include the release of monomer into the blood stream, leading to toxic effects such as a drop in blood pressure and death in extreme cases [1–11].
Ultrahigh-Molecular-Weight Polyethylene (UHMWPE)
With 90 % success rates at 15 years of metal on polyethylene articulation, UHMWPE is commonly used as a bearing surface in total hip, knee, and shoulder joint arthroplasty. UHMWPE has better wear properties compared to other polymers. Although UHMWPE has good wear characteristics in terms of degree of wear, it produces submicron and nano-sized wear debris in large quantities which can exceed the body’s ability to remove the debris material. This problem was encountered more by the oxidation of UHMWPE if it is sterilized in air using gamma radiation.
Osteolysis or bone loss in the surroundings of total joint prostheses was first thought to be due to bone cement (PMMA). Therefore, it was called cement disease. Later it was discovered that this osteolysis, which often results in the loosening of implants, is caused by the wear particles shed by the UHMWPE components of the prostheses. It was estimated that billions of such particles were released into the surrounding tissue every year. In recent years, cross-linking of the UHMWPE in a non-oxygen environment has led to significantly reduced wear and osteolysis.
Polylactic Acid (PLA) and Polyglycolic Acid (PGA)
Polylactic acid (PLA) and polyglycolic acid (PGA) and their family of materials are biodegradable polymers. These polymers and their copolymers are used commonly in the field of orthopedics as fixation devices for bone and soft tissue in the form of biodegradable plates, screws, and anchors. They are also very popular as the scaffolding material for tissue engineering applications. Additionally, they are used for a variety of controlled drug-delivery applications.
Ceramics
Ceramics are another materials used in orthopedics. Ceramics are polycrystalline materials which are usually known as inorganic, nonmetallic materials. Depending on the atomic arrangements, ceramics can either exist as amorphous or crystalline structures. An example of an amorphous ceramic is glass, whereas an example of a crystalline ceramic is porcelain. The atomic bonds in a ceramic crystal have both covalent and ionic characteristics. These strong bonds are responsible for the great stability of ceramics and impart very useful properties such as hardness, high modulus of elasticity, and resistance to heat and chemical attack. Ceramics are also strong in compression but weak in tension.
Ceramics can be grouped as inert, degradable or resorbable, and bioactive ceramics according to their reactivity. Inert ceramics, such as alumina and zirconia, are chemically stable, that is, they do not corrode, wear, or react to the host environment. Inert ceramics do not induce any immunologic host reactions and little or no chemical change occurs during the long-term exposure to the host environment. Resorbable and surface reactive ceramics react to the host resulting in surface chemical changes. Bioglass and glass ceramics are bioactive. Bioactive glass is an example of surface reactive ceramics. Calcium phosphate ceramics such as hydroxyapatite and tricalcium phosphate are examples of bioresorbable ceramics, and these ceramics are capable of degrading in the presence of a biological environment. The main purpose of the use of biodegradable porous ceramics implantation in bone tissue is to provide replacement for defective region.
The first-generation bioceramics are inert ceramics used in medicine, whereas the second-generation bioceramics include degradable and surface reactive ceramics. The main applications of inert ceramics in orthopedics are related to total hip and knee replacement. The use of bioceramic components has reduced the wear rate and the amount of ion release to a negligible level. The bioactivity of the porous ceramic material is limited mostly to osteoconductivity. Ceramic composites may be used alone or in conjunction with other materials with osteogenic, osteoinductive, or osteoconductive properties to enhance bone healing. Ceramics used as temporary structures or scaffolds in regenerative medicine are known as the third-generation bioceramics. Ceramics can also be used as carriers for cells, growth factors, antibiotics, and anticancer drugs [12, 13].
Alumina
The harmful effects of implant loosening due to polyethylene wear debris caused interest in using other materials at the articulating surface. Aluminum oxide, also known as alumina (Al2O3), has been used since 1960s as an implant biomaterial. High-density and high-purity alumina hip replacement was the first ceramic application widely used as femoral head because it shows excellent corrosion resistance, good biocompatibility, and high wear resistance and high strength. Then, ceramic material is used as the acetabular cup. The reason for the excellent wear behavior of alumina related to the frictionless surface of this ceramic. Alumina is very responsive to microstructural defect which could result in wear and breakage. Alumina-on-alumina joint articulations produce almost 5,000 times less wear than metal-on-polyethylene articulations. The elastic modulus of aluminum oxide is 20 times greater than that of cortical bone.
Zirconia
Zirconia also known as zirconium oxide (ZrO2) is one of the ceramic used in orthopedic with the highest power. High mechanical strength and fracture toughness are main characteristics of zirconia. The mechanical and wear properties of zirconium oxide are superior to those of aluminum oxide. The main application of zirconia ceramics is to replace the femoral head used in hip arthroplasties. There are some concerns that zirconia may contain very small traces of radioelements. The cytotoxicity of zirconia was also speculated in some experimental studies.
Bioglass Ceramics
Bioactive glasses are silicate-based material containing calcium and phosphate. As an implantable material, the porosity of bioglass is advantageous for resorption and bioactivity. Bioactive glasses have been widely used for filling of bone defects and modification of the implant surface characteristic (coating material).
Calcium Phosphate Ceramics
Several different forms of calcium phosphate (CaP) ceramics including hydroxyapatite (HA) and tricalcium phosphate (TCP) can be found in a human bone. In addition to the naturally occurring forms of CaP ceramics, these ceramics can be synthetically produced in the laboratory. The synthetically produced CaP ceramics are similar in composition, biodegradation, bioactivity, and osteoconductivity to the biological apatites. Calcium phosphate ceramics form a bone-like apatite layer on their surface which offers property of bioactivity and bond to living bone. Porosity is one of the main characteristics of calcium phosphate ceramics. The optimum pore size for bioceramic is identical to that of spongy bone. In general, the degradation rate of CaP ceramics is dependent on porosity, grain or crystal size, crystal perfection, inclusion of chemical impurities, and chemical composition.
HA, TCP, and biphasic CaP (combination of HA and TCP) are commonly used CaP phases in biomedical applications. The most commonly known crystalline CaP biomaterial is hydroxyapatite (HA) also known as calcium hydroxide phosphate. HA is an osteoconductive material and used as coatings on metallic implant surfaces to enhance bone healing rather than as solid ceramic implants for orthopedic applications. Another popular crystalline CaP ceramic used in the fabrication of medical devices is tricalcium phosphate (TCP). Having the chemical formula, Ca3(PO4)2, TCP can exist in two forms, namely, α-TCP and β-TCP. The rate of solubility for α-TCP is more rapid compared to β-TCP. Therefore, α-TCP degrades and resorbs more quickly in the body. To take advantage of the benefits of both HA and TCP, biphasic CaP ceramics have also been introduced as biomaterials. These composites benefit from the osteoconductivity of HA and the absorbability of the TCP [1–13].
Biological Response to Orthopedic Implants
In today’s healthcare environment, a large number of devices and implants are being inserted into the human body at an increasing rate. The success of these synthetic or natural biomaterials and implants is highly dependent on three major factors: the properties of the biomaterial (mechanical, chemical, and tribological), the biocompatibility of the implant, and the condition of the recipient tissue/the competency of the surgeon. The design of implants and prostheses is a challenging process since the intended materials must respond to specific requirements and must be biocompatible. The most important prerequisite for a biomaterial is its acceptability by the human body. Many orthopedic implants come into contact with body fluid, whether permanently or temporarily. Any foreign material inserted into the body will cause a host response. The word of biocompatibility is used to indicate the biological performance of materials. It implies the ability of a material to cause an appropriate host response. Biocompatibility is the capacity to exist in contact with tissues of the human body without causing an unacceptable degree of injury to the body. It is not only associated to toxicity, but it must be noncarcinogenic, nonpyrogenic, nontoxic, nonantigenic, blood compatible, nonthrombogenic, and noninflammatory [14, 15].
In contrast to living organ transplants, biomaterials when used in a human body are not generally “rejected,” because biomaterials typically do not generate a specific immune response like living organ transplants. All materials implanted into human body as medical implants cause tissue responses. The host responses to these materials are varied. Under certain conditions, some materials are well tolerated by the body, whereas the some materials are not well tolerated. Materials are classified into several categories such as biotolerant, bioinert, bioactive, and biodegradable. Biotolerant materials induce the worst tissue response. These tissue reactions include injury of implantation, inflammatory state and wound healing, foreign body reactions, and fibrous encapsulation of the implants. When biotolerant materials such as PMMA, polyethylene, and stainless steel are used for implantation, the body produces fibrous tissue layer between the bone and the implant in order to confine the material. The fibrous tissue accommodates plenty of macrophages and foreign body giant cells. The implants made of biotolerant materials release undesirable particles and metal ions which are nonbiocompatible. These wear particles may pile up in tissues, surrounding the implant or they may be moved to other parts of the body. When the wear debris from articulating joint surfaces are not controlled well, the inability of inflammatory cells to phagocytose particles larger than a critical size can lead to the release of enzymes and chemical mediators, such as prostaglandin, tumor necrosis factor-alpha, and interleukin-1, and cause injury to the host tissues. Thus, inflammatory cell products have the capability to damage tissue adjacent to implants. Debris generation has to be minimized [16–18].
Host Tissue Response to Implantation
Implantation of a biomaterial to the human body results in injury to tissues. This injury leads to a series of cellular activity which will cause wound healing that is the part of homeostatic mechanisms. The response of body to this initial injury is variable. The extent of injury, the status of basement membrane, blood-material interactions, the extent of cellular necrosis, and the degree of the inflammatory response all play a role. Host tissue reactions continue with inflammatory and wound healing responses, foreign body reactions, and finally fibrous encapsulation of the medical implants. All these may affect the extent of granulation tissue formation, foreign body reaction, and fibrosis. Blood-implant exposure and beginning of the inflammatory response are closely associated. The aforementioned events can lead to the production of chemical factors that mediate cellular responses of inflammation. In general, neutrophils are main cells during the first couple of days following injury, and then they are replaced by monocytes as the predominant cell type. Depending on the extent of injury, acute inflammation may last minutes to days. Exudation of fluid and plasma proteins also occurs. Neutrophils move to perivascular tissues and the injury/implantation site. Chronic inflammation is variable histologically compared to acute inflammation. Macrophages, monocytes, and lymphocytes, with the proliferation of blood vessels and connective tissue, are main cellular elements of chronic inflammation. This is a foreign body reaction, a special form of nonspecific inflammation. At the implant site, monocytes and macrophages launch healing events, followed by proliferation of fibroblasts and vascular endothelial cells, leading to the formation of granulation tissue. Depending on the extent of injury, granulation tissue may be seen as early as 3–5 days following implantation of a biomaterial. The most important cells in the foreign body reaction are macrophages. Macrophages attempt to phagocytose the material with a varying success. The macrophages, activated in the process of dealing with a biomaterial, may develop cytokines which stimulate inflammation or fibrosis. In general, fibrosis surrounds the implant with foreign body reaction and keeps apart the implant from the local tissue environment. Fibrosis or fibrous encapsulation is the end stage of healing response to biomaterials with exceptions of porous materials implanted into the bone [19–26].
In the wide sense, bioinert materials cause minimal tissue response. Titanium and cobalt-chromium alloys are typical of bioinert materials which usually cause minimal tissue response. Bioactive materials such as calcium phosphate ceramics cause the best tissue response. The body usually responds without local or systemic toxicity without any inflammatory or foreign body reaction. Degradable or resorbable materials such as certain polymers are incorporated into the surrounding tissue or may even dissolve completely over a period of time.
Metal Allergy
“Metal allergy” is a well-recognized incident. It is commonly related to the use of nickel alloy jewelry and can also occur in association with metallic implants. By themselves, metal ions lack the structural complexity required to challenge the immune system. However, when combined with proteins, such as those available in the skin and connective tissues, a wide variety of metals induce immune responses, and this can have clinical effects. Implant degradation products have been shown to be associated with dermatitis, urticaria, and vasculitis. If cutaneous signs of an allergic response appear after implantation of a metal device, metal sensitivity should be considered. Cobalt, chromium, and nickel are included in this category, with nickel perhaps the most potent; at least 10 % of a normal population will be sensitive by skin test to one or more of these metals [27–29].
Surface Modification
The characteristics of biomaterials can be generally divided into two categories: bulk and surface. Material’s bulk controls the mechanical and physical behavior of medical devices. The material’s surface properties are important because the surface properties of a material describe the interactions that occur at the interface with its environment. These usually occur within a narrow depth of less than 1 nm on the surface. The biological response to implants is controlled largely by their surface chemistry and structure. Surface properties can be important because these characteristics influence whether cells would attach to the implant or determine how proteins will interact with the surface.
Surface modification of biomaterials allows the tailoring of surface properties without affecting bulk material properties. Materials can be surface modified by using biological, mechanical, or physicochemical methods. Surface modifications fall into three categories: (1) chemically or physically altering the atoms, compounds, or molecules in the existing surface (chemical modification, etching, and mechanical roughening); (2) overcoating the existing surface with a material having a different composition (coating with thin film); and (3) creating surface textures or patterns. Nanotechnology involves the tailoring of materials at atomic level to obtain unique properties for the desired applications. Nanotechnology has impacted the field of biomaterials in several areas, including the manipulation of surface characteristics. These altered surface properties mostly improve tissue-biomaterial interactions. Modification of biomaterial surfaces may also be performed for the purpose of improving surface mechanical properties such as wear resistance, and these ultimately determine the success or failure of a device placed in the human body [30].
References
Agrawal CM et al (2014) Introduction to biomaterials: basic theory with engineering applications. Cambridge University Press, Cambridge, UK
Ong KL et al (2014) Orthopaedic biomaterials in research and practice, 2nd edn. CRC Press, Taylor & Francis Group, LLC, Boca Raton
Gupta R, Caiozzo V, Cook SD, Barrack RL, Skinner HB (2003) Basic science in orthopedic surgery. In: Skinner HB (ed) Current diagnosis and treatment in orthopedics, 3rd edn. Mc Graw Hill, New York
Patel NR, Gohil PP (2012) A review on biomaterials: scope, applications & human anatomy significance. Int J Emerg Technol Adv Eng 2(4):91–101, Website: www.ijetae.com (ISSN 2250-2459)
Migonney V (2014) History of biomaterials. In: Migonney V (ed) Biomaterials. Wiley, Hoboken. doi:10.1002/9781119043553.ch1
ASM International (2009) Biomaterials in orthopaedic surgery. In: Introduction to biomaterials in orthopaedic surgery, Chapter 1. ASM International, Ohio
Nasab MB, Hassan MR, Sahari BB (2010) Metallic biomaterials of knee and hip – a review trends biomater. Artif Organs 24(Metallic Biomaterials of 2):69–82
Iorio R, Robb WJ, Healy WL et al (2008) Orthopaedic surgeon workforce and volume assessment for total hip and knee replacement in the United States: preparing for an epidemic. J Bone Joint Surg Am 90:1598–1605
Staiger MP, Pietak AM, Huadmani J, Dias G (2006) Magnesium and its alloys as orthopedic biomaterials: a review. Biomaterials 27(9):1728–1734
Charnley J (1960) Anchorage of the femoral head prosthesis of the shaft of the femur. J Bone Joint Surg [Br] 42:28–30
Bahraminasab M, Sahari BB, Edwards KL, Farahmand F, Arumugam M, Hong TS (2012) Aseptic loosening of femoral components – a review of current and future trends in materials used. Mater Des 42:459–470
Dorozhkin SV (2010) Calcium orthophosphates as bioceramics: state of the art. J Funct Biomater 1(1):22–107
Dalton JE, Cook SD, Thomas KA, Kay JF (1995) The effect of operative fit and hydroxyapatite coating on the mechanical and biological response to porous implants. J Bone Joint Surg 77A:97–110
Williams DF (2008) On the mechanisms of biocompatibility. Biomaterials 29(20):2941–2953. doi:10.1016/j.biomaterials.2008
Dorr LD, Bloebaum R, Emmanual J, Meldrum R (1990) Histologic, biochemical and ion analysis of tissue and fluids retrieved during total hip arthroplasty. Clin Orthop 261:82–95
Treves C, Martinesi M, Stio M, Gutiérrez A, Jiménez JA, López MF (2010) In vitro biocompatibility evaluation of surface-modified titanium alloys. J Biomed Mater Res 92A:1623–1634. doi:10.1002/jbm.a.32507
Goodman SB (1994) The effects of micromotion and particulate materials on tissue differentiation: bone chamber studies in rabbits. Acta Orthop Scand Suppl 258:1–43
Hicks DG, Judkins AR, Sickel JZ, Rosier RN, Puzas JE, O’Keefe RJ (1996) Granular histiocytosis of pelvic lymph nodes following total hip arthroplasty: the presence of wear debris, cytokine production and immunologically activated macrophages. J Bone Joint Surg 78A:482–496
Anderson JM (2001) Biological responses to materials. Annu Rev Mater Res 31:81–110
Schoen FJ (2013) Introduction: biological responses to biomaterials. In: An introduction to materials. Medicine in biomaterials science, 3rd edn. Academic Press; Oxford, pp 499–503
Jacobs JJ, Goodman SB, Sumner DR, Hallab NJ (2000) Biologic response to orthopaedic implants. In: Buckwalter JA, Einhorn TA, Simon SR (eds) Orthopaedic basic sciences, 2nd edn. American Academy of Orthopaedic Surgeons, Rosemont, p 401
Korkusuz P, Korkusuz F Hard tissue-biomaterial interactions. In: Yaszemski MJ, Trantolo DJ, Lewandrowski KU, Hasırcı V, Altobelli DE, Wise DL (eds) (2003) Biomaterials in orthopedics. Marcel Dekker, New York, pp 1–210
Dee KC, Puleo DA, Bizios R (2002) Biomaterials. In: An introduction to tissue-biomaterial interactions. Wiley, New York. doi: 10.1002/0471270598.ch1
Murray DW, Rushton N (1990) Macrophages stimulates bone resorption when they phagocytose particles. J Bone Joint Surg (Br) 72:988
Goodman SB, Huie P, Song Y et al (1997) Loosening and osteolysis of cemented joint arthroplasties: a biologic spectrum. Clin Orthop 337:149–163
Urban RM, Jacobs JJ, Gilbert JL, Galante JO (1994) Migration of corrosion products from modular hip prostheses: particle microanalysis and histopathological findings. J Bone Joint Surg 76A:1345–1359
Jacobs JJ, Skipor AK, Patterson LM, Hallab NJ, Paprosky WG, Black J, Galante JO (1998) Metal release in patients who have had a primary total hip arthroplasty. J Bone Joint Surg 80-A:1447–1458
Case CP, Langkamer VG, James C et al (1994) Widespread dissemination of metal debris from implants. J Bone Joint Surg 76(B):701–712
Deutman R, Mulder TJ, Brian R, Nater JP (1977) Metal sensitivity before and after total hip arthroplasty. J Bone Joint Surg 59(A):862–865
Ratner BD, Hoffman AS (2013) Physicochemical surface modification of materials used in medicine. In: An introduction to materials. Medicine in biomaterials science, 3rd edn. Academic Press; Oxford, pp 259–276
Kretzer JP, Reinders J, Sonntag R, Hagmann S, Streit M, Jeager S, Moradi B (2014) Wear in total knee arthroplasty – just a question of polyethylene? Metal ion release in total knee arthroplasty. Int Orthop 38(2):335–340
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Köse, N. (2016). Biological Response to Orthopedic Implants and Biomaterials. In: Korkusuz, F. (eds) Musculoskeletal Research and Basic Science. Springer, Cham. https://doi.org/10.1007/978-3-319-20777-3_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-20777-3_1
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-20776-6
Online ISBN: 978-3-319-20777-3
eBook Packages: MedicineMedicine (R0)