
Abstract
Retinal break: A full-thickness defect of the neurosensory retina.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Definitions
-
Retinal break: A full-thickness defect of the neurosensory retina.
-
Horseshoe retinal tear: A type of retinal break where a strip of retina is pulled anteriorly by vitreoretinal traction. Also known as a flap tear.
-
Operculated retinal hole: A retinal break in which vitreous traction amputates the flap of the tear from the retinal surface. The separated retina (“operculum”) becomes suspended within the posterior hyaloid above the retinal surface, leaving a hole within the retinal surface that is not typically associated with persistent vitreoretinal traction.
-
Atrophic retinal hole: A retinal break that is not associated with vitreoretinal traction.
-
Giant retinal tear: A retinal break extending circumferentially more than 3 clock hours (90°).
-
Retinal dialysis: A circumferential retinal break occurring along the ora serrata.
2 Symptoms
Patients will often endorse symptoms of floaters and/or flashing lights [2]. Condition may be asymptomatic if the patient has an operculated hole, atrophic retinal hole, or a retinal dialysis. Visual field loss is a sign that a retinal tear may be progressing to a retinal detachment.
3 Signs
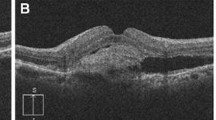
Small clumps of pigment cells may be seen suspended in the vitreous cavity or anterior segment; this is known as “tobacco dust” or a positive Shafer’s sign. Retinal tears or breaks can be visualized on ophthalmoscopy (Figs. 50.1 and 50.2). A complete or partial posterior vitreous detachment is most often present. Patients may have associated vitreous hemorrhage.

Horseshoe retinal tear (arrow) surrounded by laser retinopexy scars

Giant retinal tear
4 Predisposing Conditions
-
Lattice degeneration
-
Posterior vitreous detachment
-
Myopia
-
Cataract surgery
-
Blunt trauma
-
Penetrating trauma
5 Differential Diagnosis
Horseshoe retinal tear, operculated retinal hole, atrophic retinal hole, giant retinal tear, and retinal dialysis (Table 50.1).
6 Etiology
Retinal tears develop as a result of vitreous traction being exerted on an area of preexisting vitreoretinal adhesion, leading to a full-thickness defect of the neurosensory retina. The most common scenario is that a patient develops a posterior vitreous detachment and a flap tear or hole develops as the vitreous exerts traction on and/or separates from the retinal surface. Retinal breaks typically develop at sites of strong vitreoretinal adhesion, commonly at the posterior margin of the vitreous base.
7 Workup/Testing
The diagnosis is made clinically from a dilated fundus examination. Wide-field fundus photography can be used to document retinal tears. In the presence of a vitreous hemorrhage or other media opacity, ultrasonography can be used to identify retinal tears that cannot be seen clinically.
8 Prognosis and Management
Approximately 6 % of treated retinal tears will still go on to develop into a retinal detachment. In contrast, 30–50 % of untreated horseshoe retinal tears will go on to develop retinal detachment. Symptomatic retinal tears are treated with laser retinopexy or cryopexy surrounding the retinal break. Asymptomatic operculated and atrophic retinal holes are typically observed. Giant retinal tears resulting in retinal detachment require surgical repair.
9 Follow-Up
Patients with symptomatic flap tears treated with laser retinopexy or cryopexy are typically followed within 1 week. Asymptomatic and stable operculated retinal holes and atrophic holes can be followed annually.
References and Suggested Reading
American Academy of Ophthalmology. Basic and clinical science course. Section 12: Retina. Chapter 11: Peripheral retinal abnormalities. p. 277–301.
Tasman WS. Posterior vitreous detachment and peripheral retinal breaks. Trans Am Acad Ophthalmol Otolaryngol. 1968;72:217–24.
Robertson DM, Norton EW. Long-term follow-up of treated retinal breaks. Am J Ophthalmol. 1973;75:395–404.
Davis MD. Natural history of retinal breaks without detachment. Arch Ophthalmol. 1974;92:183–94.
Colyear Jr BH, Pischel DK. Clinical tears in the retina without detachment. Am J Ophthalmol. 1956;41:773–92.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Henry, C.R. (2016). Retinal Tears. In: Medina, C., Townsend, J., Singh, A. (eds) Manual of Retinal Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-20460-4_50
Download citation
DOI: https://doi.org/10.1007/978-3-319-20460-4_50
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-20459-8
Online ISBN: 978-3-319-20460-4
eBook Packages: MedicineMedicine (R0)