
Abstract
Gonioscopy is an essential technique for the diagnosis and treatment of glaucoma. It is important for viewing the anterior chamber angle. Other techniques such as slit-lamp biomicroscopy or imaging techniques such as anterior segment optical coherence tomography or ultrasound biomicroscopy, may allow collection of the same information we can obtain by gonioscopy. So in eyes with angle-closure glaucoma it is possible to recognize if an angle is occludable or if there is an appositional or synechial closure. But in open angle glaucoma also it is possible to observe the landmarks, the iris insertion and the pigmentation of the angle. Gonioscopic examination is an invaluable tool in glaucoma and would have been incorporated into the routine examination as a standard protocol. In this chapter there are figures to show the anatomy of a normal angle, the landmarks, and the grading systems, and there are different images of angle-closure and open angle glaucomas.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
2.1 History, Principles, and Technique
Gonioscopy is a clinical biomicroscopic technique that allows the structures in the anterior chamber angle to be visualized. The angle was first visualized by Alexios Trantas in1907 with a digital pressure with a direct ophthalmoscope using positive lens powers [1]. Salzmann introduced modern gonioscopy by the first goniolens in 1914 [2, 3]. Many other authors such as Curran, Koeppe, Troncoso, Barkan, Sugar, Schaffer, Scheie, Goldmann, and Spaeth et al. contributed to the comprehension of the angle and its role in the different types of glaucoma [4–12].
The angle of the anterior chamber cannot be visualized directly during a routine clinical examination. It can be observed only by gonioscopy, which is based on an optical phenomenon called “total internal reflection” (Fig. 2.1). It occurs when the angle of incidence of the light is so great that the light will be completely reflected (critical angle). When light crosses a boundary between materials with different refractive indices, the light beam is partially reflected and partially refracted (Fig. 2.2). But if the angle of incidence is greater than the critical angle the light is totally reflected back [13].

Total internal reflection phenomenon

The principle of total internal reflection
In the eye the critical angle is 46° at the air-cornea interface. The use of a goniolens eliminates total internal reflection by replacing the tear film-air interface with a new tear film-goniolens interface. Direct gonioscopy provides a direct view of the angle. Indirect gonioscopy provides a mirror image of the opposite angle.
This method utilizes a dome-shaped lens, which provides a panoramic view and direct visualization of the angle structures with a hand-held microscope and with the patient in supine position. The lenses commonly used for direct gonioscopy have been realized by Koeppe (Fig. 2.3) and Swan-Jacob. The patient lies in a supine position. The lens is placed on the cornea, and a saline or viscous solution is used to bridge the gap between the lens and the cornea. The angle is examined using a counterbalanced hand-held binocular microscope and an illuminator. An operating microscope can also be used. The advantages of this technique are the panoramic view, an erect image, the binocularity and the possibility to examine both eyes simultaneously. The disadvantages include a deeper angle due to the supine position, poor details, and special equipment. Direct gonioscopy is employed mainly in congenital glaucoma surgery.

Direct gonioscopy by the Koeppe lens
This technique utilizes some lenses called gonioprisms. These lenses may have 1–6 mirrors with angles ranging from 59° to 64° to the horizontal (Fig. 2.4). The light reflected from the angle of the anterior chamber passes into the lens and is reflected by a mirror onto the examiner (Fig. 2.5). The examination is performed at the slit lamp with the patient in sitting position. This method provides the clearest visualization of the anterior chamber angle structures while the illumination and magnification is provided by the slit lamp. Indirect gonioscopy can be divided into two sections: static gonioscopy and dynamic gonioscopy.

A scheme of the Goldmann three mirror lens

The mirror reflects the light from the angle to the examiner
Static gonioscopy can be performed by scleral type lenses. They have a broad area of contact and a steep convex surface. A viscous methylcellulose fluid is used as coupling substance between the lens and the corneal surface. There are a lot of lenses available for static gonioscopy, the most commonly used is the Goldmann three mirror lens (Fig. 2.6). This lens has the following features: a mirror inclined at 59°, a posterior diameter of 12 mm and a posterior radius of curvature of 7.38 mm. Many other lenses by Goldmann (1–6 mirrors), Ritch, Latina, Karickhoff, and Russel-Fankhauser (Fig. 2.7) etc. can be used.

The Goldmann three mirror lens

The Russel-Fankhauser single mirror lens
The anterior chamber angle width should be evaluated with the lens located centrally on the cornea; indentation should be avoided because of the narrowing of the angle; inadvertent pressure of the lens can also determine corneal folds (Fig. 2.8), or blood to reflux into the Schlemm’s canal. If the iris profile is convex and the structures of the angle cannot clearly be visualized, a more tangential viewing is necessary. In this case there are two options to look “over the hill”: moving the mirror toward the angle being viewed (Fig. 2.9), or asking the patient to look in the direction of the mirror (Fig. 2.10).

Corneal folds induced by an excessive pressure on the lens. The angle cannot be visualized in detail

In narrow angles, it is possible to move the mirror toward the angle to study the anatomy

Alternatively, in narrow angles it is possible to ask the patient to look at the mirror we are looking at
Dynamic gonioscopy can be performed by corneal type 4 mirror lenses (Sussmann, Posner, Zeiss). The Zeiss lens (Fig. 2.11) has a posterior diameter of 9 mm and a posterior radius of curvature of 7.72. This allows usage of the lens without a coupling fluid, obtaining a central depression of the corneal surface and a posterior displacement of the iris root (Figs. 2.12 and 2.13).

The Zeiss four mirror lens

The central depression of the corneal surface causes a peripheral displacement of the aqueous humor and a posterior displacement of the iris root

Dynamic gonioscopy in a narrow angle. The posterior displacement of the iris opens the angle
In narrow angles, performing dynamic gonioscopy is crucial (Fig. 2.14). The corneal indentation displaces the aqueous humor peripherally and the iris root posteriorly. If the angle is not visible there is a synechial angle closure, otherwise there is an appositional closure that is reversible and the angle structures become visible with indentation. An anteriorly displaced lens or a larger diameter lens can also be involved in the angle closure mechanism (Fig. 2.15).

Dynamic gonioscopy in a narrow angle with a convex iris profile. Visualization before performing central corneal indentation

Mechanism of dynamic gonioscopy. Indentation can open appositional angle closures, but it does not work in chronic or synechial angle closures. Sometimes an increased lens also could not allow the opening of the angle
2.2 Anatomy
Gonioscopy allows evaluation of the normal anatomy of the anterior chamber angle. Looking at the angle to understand the normal anatomy is important to recognize the angle landmarks. The following structures should be identified during the angle examination in primary gaze and on manipulation or indentation:
-
1.
Level of iris insertion
-
2.
Shape of peripheral iris profile
-
3.
Width of the angle recess
-
4.
Degree of trabecular pigmentation
-
5.
Areas of iridotrabecular apposition
-
6.
Anterior synechiae
To examine the angle direct focal illumination is necessary, and a narrow beam should be used to evaluate the width of the angle. It is important to avoid pupillary constriction, which can open the angle recess and deepen the anterior chamber. Sometimes, to identify the scleral spur retro-illumination is necessary. A fixation light may be used to maintain ocular alignment.
At first, the inferior quadrant should be examined because of its greater depth and pigmentation, so that it is easier to identify the structures mentioned above. Then in a clockwise direction, all the other quadrants can be observed. The following structures are present in a normal angle starting from the iris root (Fig. 2.16):

Normal anatomy of an anterior chamber angle visible by gonioscopy. The following landmarks can be recognized: Schwalbe’s line (red arrow), non-pigmented trabecular meshwork (blue arrow), pigmented trabecular meshwork (white arrow), Schlemm’s canal, scleral spur (yellow arrow), ciliary body band (green arrow)
-
(a)
Ciliary body band
-
(b)
Scleral spur
-
(c)
Schlemm’s canal
-
(d)
Pigmented trabecular meshwork
-
(e)
Non-pigmented trabecular meshwork
-
(f)
Schwalbe’s line
Scleral spur and Schwalbe’s line should be identified at first and then all the other structures can be recognized [14].
2.2.1 Schwalbe’s Line
The Schwalbe’s line appears as an opaque translucent line that represents the peripheral termination of Descemet’s membrane and the anterior limit of the trabeculum. It marks the transition between the endothelium of the cornea and the trabecular meshwork. Sometimes, it may be prominent and anteriorly displaced (posterior embryotoxon) (Fig. 2.17), or heavy pigmented; pigmentation anterior to the Schwalbe’s line constitutes the Sampaolesi’s line (Fig. 2.18), and this is often disposed noisily, resembling salt and pepper.

A prominent anteriorly displaced Schwalbe’s line

Pigment distribution anterior to the Schwalbe’s line (red arrows) to constitute the Sampaolesi’s line
The parallelepiped or the corneal wedge technique can be used to identify the exact position of the Schwalbe’s line (Figs. 2.19, 2.20, and 2.21). By using a thin slit of light inclined 10–15° from the angle of the oculars, two separate corneal reflections can be seen, one from the inner surface of the cornea, and one from the outer surface. These two reflections meet at Schwalbe’s line, which extends in a perpendicular direction across the trabecular meshwork and marks the anterior border of the trabecular meshwork itself. This technique is very useful in lightly pigmented angles and in angles with a confusing anatomy (Fig. 2.22). In the superior and inferior quadrant, it is easiest to generate a vertical slit and to identify the corneal wedge.

The corneal wedge technique

The two light reflections, respectively, from the inner and the outer surface of the cornea, meet at Schwalbe’s line (red arrow)

Corneal wedge technique in a lightly pigmented angle. The apex indicates the Schwalbe’s line (red arrow)

An easiest representation of the angle’s landmarks: Sampaolesi’s line (blue arrow), Schwalbe’s line (red arrow), trabecular meshwork (white arrow), scleral spur (yellow arrow), ciliary body band (green arrow)
2.2.2 Trabecular Meshwork
This extends posteriorly from the Schwalbe’s line to the scleral spur. It is possible to distinguish an anterior nonfunctional part next to the Schwalbe’s line with a whitish color; and a posterior functional part adjacent to the scleral spur, which is pigmented (Fig. 2.23). Trabecular pigmentation increases with age and is accentuated in the inferior quadrant due to gravitational setting and aqueous circulation; an increase in the pigmentation of the angle could be related to pathological conditions such as exfoliation syndrome, pigment dispersion syndrome, or inflammation. Pigmentation has little relation to skin or hair color. At gonioscopy, it appears with an irregular and rough surface; the trabecular meshwork band appears as 5 mm wide at the slit-lamp examination.

The trabecular meshwork. It can be divided into two parts: a lightly or non-pigmented anterior (blue arrow) trabecular meshwork and a pigmented posterior (white arrow) trabecular meshwork
2.2.3 Scleral Spur
Going posteriorly between the trabecular meshwork and the ciliary body there is the scleral spur, which appears as a narrow whitish band that marks the posterior border of the trabecular meshwork (Fig. 2.24). Sometimes it is not visible because of an anterior iris insertion, iris processes (Fig. 2.25), excessive pigmentation (Fig. 2.26), or peripheral anterior synechiae (PAS).

The scleral spur (yellow arrows)

Iris processes may obscure the scleral spur

The scleral spur is not visible due to an excessive pigmentation
2.2.4 Ciliary Body Band
Anterior to the iris insertion, a portion of the ciliary body is visible (Fig. 2.27). The width of the band depends on the position of the iris insertion, and it may be wide in myopia or following trauma, but it also can be narrow in hyperopia and anterior insertion of the iris. The band appears as gray or dark brown at gonioscopic examination. Before commenting on any abnormality, the width of the band must be compared between the two eyes.

A wide ciliary body band (green arrow)
2.2.5 Iris and Iris Process
The iris insertion is usually at the anterior face of the ciliary body, and normally the iris has radial markings with crypts. Three features are really important to determine the angle anatomy: the contour of the iris (convex, concave, or flat), the site, and the way of the iris insertion. It is important during the examination of the iris to notice the presence of nevi, tumors, atrophy, iridodonesis, and abnormal pigmentation. The peripheral iris configuration may provide important clues to the presence of pigment dispersion syndrome, plateau iris, or pupillary block.
Iris processes are small extensions of the anterior surface of the iris, which insert at the level of the scleral spur (Figs. 2.25 and 2.28). The iris processes are more frequent in young patients and in brown eyes. They appear as gray or brown finger-like extensions of the peripheral iris at gonioscopy and do not block the iris movements during indentation gonioscopy.

Iris processes between the peripheral iris and the scleral spur
2.2.6 Schlemm’s Canal
Schlemm’s canal is not normally visible, it is located within the posterior trabecular meshwork and is anterior to the scleral spur. It may be seen when there is blood inside the canal for example, if the goniolens compresses the episcleral veins such that the episcleral venous pressure exceeds the intraocular pressure (IOP) (Fig. 2.29).

The Schlemm’s canal can be visualized as a red discontinuous line
At gonioscopic examination it is seen deep in the posterior half of the trabecular meshwork as a red discontinuous line (Figs. 2.30 and 2.31). The pressure of the episcleral veins may be high also in different conditions: carotid-cavernous fistula, in Sturge-Weber syndrome, venous compression, ocular hypotony, or sickle cell disease.

The Schlemm’s canal can be visualized if there is blood inside

Bleeding from the Schlemm’s canal
2.2.7 Blood Vessels
Blood vessels may be visible in the normal anterior chamber angle (Fig. 2.32). They are more visible in blue eyes rather than in dark eyes. Normally the vessels run in a radial pattern at the base of the angle recess or perpendicular to the iris plane deep in the ciliary body. Normal vessels as a rule do not cross the scleral spur, are large and have a radial or circumferential orientation (Figs. 2.33 and 2.34). Pathological vessels are usually thinner, have a disordered orientation with anastamoses, and may run across the scleral spur.

Blood vessels may be visible in a normal angle

Large vessels in a normal angle

Circumferential normal vessel not crossing the scleral spur
2.3 Gonioscopy Grading Systems
Determination of the angle width is really important in order to understand the functional status of the angle, the degree of angle closure, and the risk of future closure.
Grading of the angle can be obtained by the Van Herick method or by a gonioscopic grading system.
The Van Herick technique is used to assess the limbal anterior chamber depth. A narrow beam of light is directed perpendicularly at the temporal limbus, and the depth of the anterior chamber is evaluated as a fraction of the adjacent corneal thickness (Fig. 2.35) [15].

The Van Herick method. Grade 0: iridocorneal contact (angle closed). Grade 1: the space between the iris and corneal endothelium is <¼ of corneal thickness (angle closure likely). Grade 2: the space is >¼ – <1/2 of corneal thickness (angle occludable). Grade 3: the space is >1/2 of corneal thickness (angle not occludable). Grade 4: the space is equal to the corneal thickness (open angle)
The width of the angle is determined by the insertion of the iris root on the ciliary body, the convexity of the iris, the prominence of the peripheral iris roll and the pupillary size.
Gonioscopy provides a subjective assessment of the angle width, but grading of the angle is essential for a systematic approach in the evaluation of the angle anatomy.
The use of a grading system allows comparison of findings at different times in the same patient, or to classify different patients.
There are three grading systems currently in use:
-
1.
Shaffer
-
2.
Spaeth
-
3.
Scheie
2.3.1 Shaffer’s System
The Shaffer’s system describes the angle between the iris and the trabecular meshwork [9].
The angle is recorded in degrees of arc subtended by two imaginary tangential lines: a line tangential to the inner surface of the trabeculum and the other line tangential to the iris surface about one-third of the distance from its periphery. In practice, the angle is graded according to the visibility of various angle structures. Angle >20° is considered open. The system assigns a numerical grade (4-0) to each angle with associated anatomical description, angle width in degrees, and implied clinical interpretation (Fig. 2.36).

The Shaffer’s System
-
Grade 4 (35-45°) is the widest angle in which the ciliary body can be visualized, closure is impossible
-
Grade 3 (20–35°) is an open angle in which the scleral spur can be identified, closure is impossible.
-
Grade 2 (20°) is a moderately narrow angle in which only the trabeculum can be identified; angle closure is possible but unlikely.
-
Grade 1 (10°) is a very narrow angle in which only Schwalbe’s line can be identified; there is a high risk of angle closure.
-
Slit angle no angle structures can be identified; this angle has the danger of imminent closure.
-
Grade 0 (0°) is a closed angle; there is iridocorneal contact, and it is not possible to recognize the apex of the corneal wedge.
2.3.2 Scheie Grading System
The Scheie grading system describes with Roman numerals the degree of angle closure, with larger numbers signifying a narrower angle; the system is based on the extent of visible angle structures (Fig. 2.37) [10].

The Scheie grading system
-
Grade 0 the widest angle in which the ciliary body can be seen.
-
Grade I wide angle in which a narrow ciliary body band can be seen.
-
Grade II is an open angle in which at least the scleral spur can be identified.
-
Grade III is a moderate narrow angle in which only the anterior trabecular meshwork is visible.
-
Grade IV angle is closed.
2.3.3 Spaeth System
The Spaeth system grades three aspects of angle configuration [12]:
2.3.3.1 Angular Width of Angle Recess
The examiner estimates the width of the angle, considering the angle between a line tangential to the trabecular meshwork and a line tangential to the iris surface about one-third of the way from the periphery (Fig. 2.38).

The Spaeth System: angular width of angle recess
-
(a)
Slit
-
(b)
10° Narrow
-
(c)
20°
-
(d)
30° Wide
-
(e)
40°
2.3.3.2 Level of Iris Insertion (Fig. 2.39)

The Spaeth System: level of iris insertion. The letters on the (arrows) identifies the level of the iris insertion (Anterior, Behind Schwalbe’s line, Centered on the sclera, Deep to scleral spur, Extremely deep)
-
(a)
Anterior: iris insertion anterior to the Schwalbe’s line
-
(b)
Behind Schwalbe’s line: iris insertion behind the Schwalbe’s line
-
(c)
Centered on sclera: on the scleral spur
-
(d)
Deep to scleral spur: behind the scleral spur
-
(e)
Extremely deep: on the ciliary band
2.3.3.3 Iris Configuration (Fig. 2.40)

The Spaeth System: iris configuration
-
s: steep, anteriorly convex
-
r: regular or flat
-
q: queer, anteriorly concave.
It also considers the grade of trabecular meshwork pigmentation (TMP) from 1 (minimal) to 4 (dense) (Fig. 2.41).

The Spaeth System: trabecular meshwork pigmentation
2.4 Pathology
2.4.1 Congenital and Developmental Glaucoma
In infants gonioscopy is performed using Koeppe lens or the Swan-Jacob lens; the baby could be sedated for the examination on the operating microscope; but the examination could also be performed at the office. Gonioscopy distinguishes primary congenital glaucoma from secondary glaucoma and is really helpful in planning surgery. Congenital glaucoma presents at birth or between 1 month and 2 years of age. It is the consequence of the developmental arrest of the anterior chamber angle tissue; the trabeculo-dysgenesis is the only ocular anomaly in 50 % of cases; with a higher insertion of the iris and ciliary body onto the posterior trabecular beams which causes their compression and creates an obstruction to aqueous outflow. It is typical to observe an open angle with high insertion of the iris root, which forms a line with small curves.
-
(a)
The iris insertion could be at or anterior to the scleral spur (Fig. 2.42), and the ciliary body is covered by this insertion and is not visible (in normal infants the iris inserts flatly on the ciliary body face). The appearance of the trabecular meshwork is orange peel and the iris stroma may be thin and may expose radial blood vessels.
Fig. 2.42 
Congenital glaucoma. The iris insertion is at the Schwalbe’s line
-
(b)
The iris insertion could be into the chamber angle. The plane of the iris is posterior to the scleral spur, but the anterior stroma inserts just behind the Schwalbe’s line.

Usually, abnormal tissue with a glistening appearance is seen in the angle and seems to pull the peripheral iris anteriorly. Above the iris root loops of vessels from the major arterial circle are sometimes visible, and there could be a fine tissue covering the peripheral iris, which usually is thinner and flatter.
2.4.1.1 Axenfeld-Rieger Syndrome
Axenfeld-Rieger Syndrome is a set of diseases, which includes Axenfeld anomaly (posterior embryotoxon associated with iridocorneal adhesions) (Fig. 2.43); Axenfeld syndrome (Axenfeld anomaly with glaucoma) (Fig. 2.44); Rieger anomaly (Axenfeld anomaly, iris stromal thinning, iris hole, corectopia); and Rieger Syndrome (Rieger anomaly with systemic developmental anomalies) (Fig. 2.45) [16].

Axenfeld syndrome. Irido-corneal adhesions at biomicroscopy

Gonioscopy of the same patient. Tissue strands in the anterior chamber

Rieger syndrome
Glaucoma originates from the developmental arrest of the anterior segment tissue derived from the neural crest cells.
Typical gonioscopic features are:
-
1.
Anteriorly displaced Schwalbe’s line (posterior embryotoxon) (Fig. 2.17); sometimes the line is suspended from the cornea by a thin membrane.
-
2.
Tissue strands in the anterior chamber angle; similar in color and texture to the iris (Fig. 2.46).
Fig. 2.46 
Axenfeld syndrome. Tissue strands in the anterior chamber angle
-
3.
Open angle.
-
4.
The scleral spur is covered by the iris insertion.

2.4.1.2 Aniridia
Aniridia is characterized by the absence of the iris; even if at gonioscopy a rudimentary stump of the iris is usually present (Figs. 2.47 and 2.48) [17]. The angle is open and sometimes strands of tissue in the angle with fine blood vessels extending from the iris root to the trabecular meshwork are visible. In 10–15 years the angle progressively closes and the iris comes to lie over the trabecular meshwork.

Aniridia. A small part of the iris is visible

Aniridia. The ciliary body is visible. It is visible also a blue loop of the IOL in the bag
Gonioscopy can demonstrate anomaly of the angle in primary and secondary developmental glaucoma. It is possible to observe anterior iris insertion, prominent iris process, and featureless angle. Iris processes are the remnants of normal development of angle and can be a normal variation.
2.4.2 Open Angle Glaucomas
2.4.2.1 Pseudoexfoliation Syndrome
The deposition of fibrillar protein matrix throughout the anterior segment (on the lens, the angle, the iris, the corneal endothelium, the zonula and the ciliary body) is the main feature of this syndrome. In these patients the IOP can increase to higher values than in POAG patients. It is very important to observe the angle to recognize the syndrome [18] even if the severity of the material deposition cannot be related to an increased risk of glaucoma development. It is possible to observe flecks of exfoliation material adherent to the trabecular meshwork (Fig. 2.49) and pigmentation may be increased with a discontinuous segmental distribution (Fig. 2.50) [19]. A scalloped band of pigment running anterior to the Schwalbe’s line (Sampaolesi’s line) is frequent (Figs. 2.51 and 2.52).

Flecks of exfoliation material adherent to the trabecular meshwork (red arrows) in pseudoexfoliation syndrome

The discontinuous distribution of the pigment throughout the angle in pseudoexfoliative glaucoma

The Sampaolesi’s line (red arrow) above the Schwalbe’s line

The Sampaolesi’s line (red arrow) in pseudoexfoliative glaucoma
2.4.2.2 Pigment Dispersion Syndrome
Pigment dispersion syndrome is usually a bilateral disorder characterized by the liberation of pigment granules from the iris pigment epithelium and their deposition throughout the anterior segment, mainly in the trabecular meshwork. The diagnosis is possible by the slit-lamp observing mid-peripheral iris trans-illumination defects, diffuse and dense brownish pigmentation of the angle, and pigment granules on the corneal endothelium (Krukenberg spindle) [20]. The angle is open with a deeper anterior chamber both because the iris could be more posterior inserted or the iris stroma could be floppy. The iris has a marked concave configuration in the mid periphery (Fig. 2.53). The pigment distribution can be positioned over all the angle structures (Fig. 2.54), even if usually a homogeneous dense, very dark band covering the trabecular meshwork can be observed (Figs. 2.55, 2.56, and 2.57) [21].

In pigment dispersion syndrome there is a wide concavity of the iris profile

Deposition of pigment all over the angle structures

Pigmentary glaucoma. Deposition of pigment mainly on the trabecular meshwork

Deposition of pigment over the trabecular meshwork. The Sampaolesi’s line and the scleral spur are visible

Pigment granules in the angle
2.4.2.3 Post-traumatic Glaucoma
Gonioscopy must be performed in every patient with unexplained unilateral glaucoma or in patients with a history of ocular trauma, even after many years [22]. Many different signs may be observed after a blunt trauma. A bleeding vessel may be noted (Fig. 2.30), a blood clot may obscure the angle structures (Fig. 2.58) or blood may be present in the Schlemm’s canal (Figs. 2.29 and 2.30). An increased irregular pigmentation after anterior inflammation (Fig. 2.59) or peripheral anterior synechiae (Figs. 2.60 and 2.61) may be observed. The posterior displacement of the iris root, the angle recession (Fig. 2.62), or an iridodialysis (Figs. 2.63 and 2.64) could lead more frequently to a post-traumatic glaucoma. An irregularly broadened ciliary body band must be compared with the fellow eye to diagnose an angle recession.

Post-traumatic hyphema covering the angle landmarks

Pigment granules in the angle after an iridociclitis

Wide angular synechiae and precipitates in anterior uveitis

A peripheral anterior synechia

A post-traumatic angle recession, mydriasis, lens subluxation, and ciliary body visualization

A wide iridodialysis with visualization of the ciliary processes

Iridodyalisis
2.4.3 Angle Closure Glaucomas
Angle closure is identified by gonioscopy, the “reference standard” diagnostic procedure. A narrow angle recess, usually narrower than 20°, characterizes primary angle closure. Fundamental during gonioscopy is the manipulation and the indentation of the angle to establish if the closure is appositional or synechial.
Looking at a narrow angle, the following features should be evaluated [4, 23]
-
1.
Schwalbe’s line visible or not; if not the angle is closed (Fig. 2.65).
Fig. 2.65 
Angle closure. The Schwalbe’s line is not visible
-
2.
Trabecular meshwork visible or not; if not in at least three quadrants in primary position without manipulation, the angle can be classified as occludable (Fig. 2.66).
Fig. 2.66 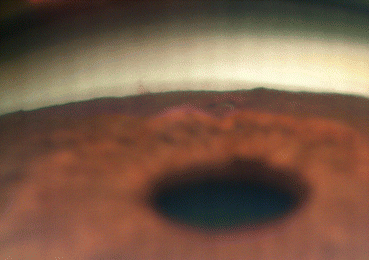
Occludable angle. The trabecular meshwork is visible under the Schwalbe’s line
-
3.
Evidence of a previous angle closure attack: goniosynechiae, peripheral anterior synechiae, glaukomflecken, iris atrophy, increased or pattern pigmentation.
-
4.
Symmetry of gonioscopic findings between the two eyes and between the superior and inferior quadrants of the same eye (Figs. 2.67 and 2.68).
Fig. 2.67 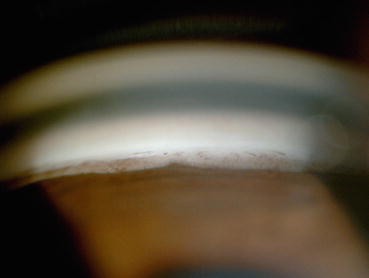
The inferior sector of an angle. The Schwalbe’s line and the trabecular meshwork are visible
Fig. 2.68 
The superior sector of the same eye. Some synechiae are visible and the angle is partially closed. An iridotomy is also visible




Primary angle closure may become chronic after an acute attack or due to the long-term use of miotics [24]. The angle is permanently closed and PAS can be easily identified by indentation gonioscopy [25]. Laser iridotomy is mandatory in angle closure glaucoma and gonioscopy should be repeated at least every 6 months to identify any possible change even if there is a patent iridotomy. Irido-trabecular apposition after iridotomy suggests a secondary mechanism of angle closure; mechanisms of secondary angle closure include disorders of the ciliary body, lens-induced angle closure (phacomorphic glaucoma) or malignant glaucoma with a misdirection of the aqueous humor [26]. The treatment of all these types of glaucoma is related to the identification of the underlying pathophysiology.
2.4.3.1 Iridocorneal Endothelial (Ice) Syndrome
ICE syndrome is a rare disorder, more frequent in young to middle-aged females, characterized by unilateral angle closure glaucoma. There are some typical features of these groups of disorders, first of all an abnormal physiology of the endothelium, then corneal edema and progressive iris atrophy. There are three types of the disease:
-
Chandler’s syndrome (corneal edema predominates)
-
Iris Nevus/Cogan Reese Syndrome (nodular iris lesions are present associated with corneal and iris defects)
-
Progressive iris atrophy (iris changes predominate with corectopia, atrophy, and hole formation).
Peripheral anterior synechiae are common findings at gonioscopic examination; PAS usually extends anterior to the Shwalbe’s line [16]. These result from contraction of endothelial cell layers and fibrous tissue that extends from the corneal endothelium onto the trabecular meshwork and the iris (Fig. 2.69).

Irido-corneal-endothelial syndrome. A wide goniosynechia is visible
2.4.3.2 Uveitic Glaucoma
Inflammation in uveitis leads to hypersecretion of aqueous humor and to obstruction of the trabecular meshwork by serum components and inflammatory precipitates (Fig. 2.70), trabeculitis, scarring of trabecular meshwork and peripheral anterior synechiae formation. As a consequence, the intraocular pressure rises and glaucoma develops. In uveitic glaucoma the angle can be open or closed. Closed angle glaucoma is related to several mechanisms: pupillary block, iris bombe, PAS (Fig. 2.60), anterior rotation of lens iris diaphragm or neovascularization. The IOP rise can develop both during the acute phase of the inflammation for trabecular obstruction or later on, due to the scarring of the trabecular meshwork. Observing the anterior chamber angle after iridocyclitis, a typical clod deposition of pigment may be noted (Fig. 2.59). Other frequent findings after inflammation are the anterior peripheral synechiae that can be small or tent-shaped and the angle that remains open (Figs. 2.61 and 2.71). But PAS can also be larger, causing a secondary angle closure (Fig. 2.72).

Acute anterior uveitis. Endothelial inflammatory precipitates

Anterior synechia adherent to the Schwalbe’s line

A wide anterior sinechia. The edge of an anterior chamber IOL is visible
2.4.3.3 Neovascular Glaucoma
Retinal ischemia may lead to a neovascularization of the angle till the development of a neovascular glaucoma. This disease has a pre-glaucoma stage, an open angle glaucoma stage and an angle closure glaucoma stage. In the first stage, neovascularization appears on the pupillary margin or in the angle. Vascular trunks may cross the scleral spur and arborize irregularly on the trabecular meshwork. In the second stage, there is a fine fibrous membrane, invisible on gonioscopy, obstructing the aqueous flow [27] (Fig. 2.73). In the angle closure stage, the fibrovascular membrane pulls the iris toward the trabecular meshwork with peripheral anterior synechiae formation [28] (Fig. 2.74).

Neovascular glaucoma. Vascular trunks cross the scleral spur. The Schlemm’s canal also is filled with blood

New vessels on the iris surface. A secondary angle closure is present
2.4.4 Post-surgical Evaluation of the Anterior Chamber Angle
After filtering surgery gonioscopy is critical to understand the outcome of the surgery. Trabeculectomy represents the gold standard for glaucoma surgery (Fig. 2.75), and with gonioscopy it is possible to study the site where the trabecular tissue is removed during surgery and the site of iridectomy. Sometimes, a rise in IOP can be due to the obstruction of this site by anterior synechiae or any other material (Figs. 2.76, 2.77, and 2.78).

Trabeculectomy. A large vessel is visible in the sclerostomy site

Partially closed trabeculectomy by a basal synechia due to a too central iridectomy

Remnant of a cataract occluding the iridectomy and the trabeculectomy

Through the iridectomy, it is possible to observe the ciliary body and exfoliative material over the ciliary processes
Vitreoretinal surgery sometimes can cause glaucoma; a rise of intraocular pressure may be observed in early postoperative period due to overfilling of the posterior chamber with silicon oil or gas. But also secondary glaucoma may develop for the obstruction of the trabecular meshwork by emulsified silicon oil (Fig. 2.79). Sometimes, perfluorocarbon liquid bubbles can also be observed in the inferior sector as a remnant of intraoperative tamponade to lay down the retina (Fig. 2.80).

Silicon oil bubbles occlude the angle in the superior sector

Perfluorocarbon liquid bubbles in the inferior sector as remnant of vitreous surgery
References
Trantas A (1918) L’ophthalmoscopie de l’angle irido-cornéen (gonioscopie). Arch Ophthalmol 36:257–276
Salzmann M (1914) Die Ophthalmoskopie der Kammberbucht. Z Augenheilk 31:1–19
Salzmann M (1915) Nachtrag zu Ophthalmoskopie der Kammberbucht. Z Augenheilk 34:160–162
Curran EJ (1920) A new operation for glaucoma involving a new principle in the etiology and treatment of chronic primary glaucoma. Arch Ophthalmol 49:131
Koeppe A (1920) Das stereo-mikroskopische Bild des lebenden Kammerwinkels an der Nernstspaltlampe bein Glaukom. Klin Monatsbl Augenheilk 65:389–391
Troncoso MU (1925) Gonioscopy and its clinical applications. Am J Ophthalmol 8:433–439
Barkan O, Boyle SF, Maisler S (1936) On the genesis of glaucoma. An improved method based on slit lamp microscopy of the angle of the anterior chamber. Am J Ophthalmol 19:209–215
Sugar HS (1949) Newer conceptions in the classification of the glaucomas. Am J Ophthalmol 32:425–433
Shaffer RN, Tour RL (1956) A comparative study of gonioscopic methods. Am J Ophthalmol 41:256–265
Scheie HG (1957) Width and pigmentation of the angle of the anterior chamber; a system of grading by gonioscopy. Arch Ophthalmol 58:510–512
Goldmann H (1968) Biomicroscopy of the eye. Am J Ophthalmol 66:789–804
Spaeth GL (1971) The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Soc UK 91:709–739
Dada T, Sharma R, Sobti A (2013) Gonioscopy. A text and atlas. Jaipee Borthers, New Delhi
Fish BM (1993) Gonioscopy of the glaucomas. Butterworth-Heineman, Boston
Van Herick W, Shaffer RN, Schwartz A (1969) Estimation of width of angle of anterior chamber. Incidence and significance of the narrow angle. Am J Ophthalmol 68:626–629
Schields MB (1983) Axenfeld-Rieger syndrome: a theory of mechanism and distinctions from the iridocorneal endothelial syndrome. Trans Am Ophthalmol Soc 81:736–784
Grant WM, Walton DS (1974) Progressive changes in the angle in congenital aniridia with development of glaucoma. Am J Ophthalmol 78:842–847
Prince AM, Streeten BW, Ritch R, Dark AJ, Sperling M (1987) Preclinical diagnosis of pseudoexfoliation syndrome. Arch Ophthalmol 105:1076–1082
Ritch R (1994) Exfoliation syndrome and occludable angles. Trans Am Ophthalmol Soc 92:845–944
Lehto I, Vesti E (1998) Diagnosis and management of pigmentary glaucoma. Curr Opin Ophthalmol 9:61–64
Lichter PR, Shaffer RN (1970) Iris processes and glaucoma. Am J Ophthalmol 70:905–911
Blanton FM (1964) Anterior chamber angle recession and secondary glaucoma. A study of the aftereffects of traumatic hyphemas. Arch Ophthalmol 72:39–43
Chandler PA (1952) Narrow-angle glaucoma. Arch Ophthalmol 35:1696
Pollack IP (1971) Chronic angle-closure glaucoma; diagnosis and treatment in patients with angles that appear open. Arch Ophthalmol 85:676–689
Forbes M (1966) Gonioscopy with corneal indentation. A method for distinguishing between appositional closure and synechial closure. Arch Ophthalmol 76:488–492
Ritch R (1982) Argon laser treatment for medically unresponsive attacks of angle-closure glaucoma. Am J Ophthalmol 94:197–204
Schulze RR (1967) Rubeosis iridis. Am J Ophthalmol 63:487–495
John T, Sassani JW, Eagle RC Jr (1983) The myofibroblastic component of rubeosis iridis. Ophthalmology 90:721–728
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Figus, M., Taloni, M., Posarelli, C. (2016). Gonioscopy. In: Ferreras, A. (eds) Glaucoma Imaging. Springer, Cham. https://doi.org/10.1007/978-3-319-18959-8_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-18959-8_2
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18958-1
Online ISBN: 978-3-319-18959-8
eBook Packages: MedicineMedicine (R0)