
Abstract
The Science never before faced such a complex, dynamic and time-dependent process as human aging. Longitudinal studies are a source of fundamental evidence of the multi-factor changes over time, especially those that have contributed to understanding the aging process through research questions related to the course or prognosis of physical or cognitive functioning of the elderly, exposure to comorbidity, health conditions, and biological, environmental, social or emotional negative or positive factors, as well as other questions related to aging.
However these studies have major methodological challenges to keep the validity of information between standardized measurements and the generalization of the results, especially with the loss of participants due different causes. These difficulties motivated the realization of this chapter where we discussed the role of the longitudinal studies in the study of aging, beginning with methodological concepts, the importance of this design in geriatric research and the direction of new research questions, we present also a review of classic longitudinal studies from the literature, which enable us to provide examples of scope and methodological implications, and finally we suggested some strategies about strengthen the validity and generalizing of results.
Longitudinal methodology represents a fundamental pillar in geriatric research. Its implementation always must to be supported by good planning that takes into account-standardized procedures as well as techniques that minimize the probable losses during the follow-up to minimize their effect throughout the study.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
7.1 Introduction
The aging of the population is one of the most remarkable success stories in social development and human health. However, scientific understanding of the aging process has not developed at the same rate as the growth of the generations of older adults and their special health needs.
In this context longitudinal studies take on special importance, especially those that have contributed to understanding the dynamics of the aging process by analyzing physiological, psychological, social or environmental variables [1] that are time variant. These designs have yielded results on successful aging, longevity, frailty and other traits. Thus geriatric research has been nourished by a diversity of studies of an observational and especially a longitudinal nature, oriented to responding to the lack of knowledge about the latent changes in different generations of older adults, and posing new questions about exceptionally healthy old populations linked to the traits of robustness and functioning, in contrast to populations that are frail or disabled/dependent, with or without chronic degenerative illnesses [2].
The present chapter will be concerned with discussing the role longitudinal studies play in the study of aging. First it will analyze the theoretical concept of the longitudinal study, and then it will highlight the importance of this design in geriatric research and the direction of new research questions. In the second part we present a review of classic longitudinal studies from the literature, which will enable us to provide examples of scope and methodological implications, in order to offer some strategies to strengthen the validity and generalizing of results.
7.2 Theoretical Concept of Longitudinal Studies
The broadest notion of longitudinal studies refers to the analysis of a particular sample of individuals who show time-dependent patterns of change (variables of interest), which require the presence of three conditions: (1) that the data be collected during two or more distinct time periods; (2) that the sample elements (individuals) are comparable from one period to the other; and (3) that the analysis involves comparison of the data between two or more time periods [3].
Given that various types of both observational and experimental studies may be framed under these conditions, it is proposed to distinguish them according to the way in which the measurements are collected, the entry of the individuals into the study, the type of information desired [4], and how the differences in each design make them independent. Thus the present chapter will be limited to showing general aspects of observational longitudinal studies, since experimental studies like clinical or quasi-experimental trials form part of a review presented in another chapter.
Within the theme that concerns us, observational longitudinal studies may be classified according to the way the information search will be oriented. We present the way most studies related to aging have been conceived and that are worth mentioning in relation to their particular characteristics. Thus we find among others, those of the type panel, trends and cohort studies. The latter is considered to be the main longitudinal study for epidemiological research.
Given the different perspectives that exist for understanding the designs of the study, we present below the most frequently accepted structure and characteristics of each one:
Panel studies [5] obtain information by repeated measurements of the same group of individuals over fixed periods of time. This kind of study represents the conceptual base of a census or national survey carried out within the same population, with certain time periodicity to answer questions about the change of latent variables through time. It is also used to distinguish permanent characteristics from transitory ones of a specific phenomenon, analyze the life conditions of a group being studied, or differentiate intergenerational changes that are presented in a stage of life. These could be functional dependency, retirement from the labor force or characteristics of longevity in a population, as well as others.
One of its main weaknesses is that the sample responses could be subordinated to a “period effect,” caused by an unexpected event or general circumstance (epidemic, climate change, or civil unrest, for example) at the time of the measurements, which could change the responses issued differentially among the subjects of the study. As well, the panel study could have a significant decline in the number of responses in each cycle of information collection, losses which would have a cumulative effect on the study’s variables. This is related to the progressive loss of members of the sample during the course of the study [5], a phenomenon common to any longitudinal study. These losses have to be given special consideration in studies on aging, where it happens more frequently, since the losses are related to events such as change of domicile, death, hospitalization of the participant, or a decision to stop participating. It causes the sample to get smaller in each measurement period, a phenomenon called “panel fraying” or attrition. Given the importance of this possibility it will be described in more detail at the end of the chapter.
Trend designs [5] differ from panel studies because they analyze changes through time of different individuals in each evaluation period. With this characteristic, the data collected are analyzed collectively and not individually. Thus, as the name indicates, the information analyzed enables researchers to predict future trends about the individuals or the study universe, and the prediction variables may be evaluated through time. In this type of study unforeseen factors in the sample subjects are not considered, but the results may be easily influenced by other time-related variables not taken into account. For this reason, this type of design must be clearly delimited and the information collection strategies must be strictly replicated in each measurement period.
Lastly, the cohort design [6] is the longitudinal study most used on epidemiology and clinical research, since it is thought to be closer to experimental studies in terms of the search for causality and scientific evidence [7]. However, for the social and demographic sciences the cohort study represents the measurement of differences or changes in a population (or group) selected according to a common condition or experience where the main point is rooted in analysis, together with the population and the magnitude of the time-dependent change of events, which is often defined by the researcher [3]. This definition has a common denominator with other scientific areas, in that the longitudinal data are compiled in a time sequence that clarifies the direction as well as the magnitude of change in the variables. For epidemiological and clinical research, the cohort design makes it possible to check for a cause-effect association through time between the course of an exposure and an outcome of interest (event) that is produced over a period of time, where each subject makes an individual contribution [8, 9]. Like the other longitudinal studies, its objective is to describe the occurrence of time-dependent results [9], but the scope of this type of epidemiological study is related more to the incidence or occurrence of phenomena from the composition of the groups for an exposure variable that is present or absent among the subjects being studied. It follows through time in a prospective or retrospective manner up to the appearance of the event of interest. It should be mentioned that retrospective cohort studies are not discussed in this chapter. This is because, in relative longitudinal studies on aging, there are few variables that might respond to complex questions related to time changes, and the exposure events of interest occurred in the past, in other words before the study was begun. That is why the researcher does not have control over the nature and quality control of prior measurements or over data that could be important for a specific question and that were not gathered in the past. For that reason the study of diverse events in aging such as functioning, cognition, memory, depression, levels of physical activity, changes in body composition and others requires a prospective methodology that allows the researcher to include changes in the present time from their identification in repeated observations, for periods of time established by the researcher or until an outcome of interest is presented.
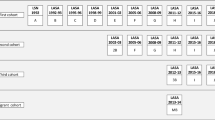
It must be taken into account that older persons differ from other types of populations in several ways. With this in mind, we present a proposal outline of scenarios that could be represented in a longitudinal study within the scope of research on aging. This outline was prepared taking as a reference the proposal of Fuller for the study of falls among old people [10] and the analysis of levels of complexity present in geriatric research among different populations of old people by Faes et al. [1].
Figure 7.1 starts by identifying variables to be evaluated in the study, both in the population of interest or group being studied and in the comparison group. At the start of the study (present time) initial measurements are made that enable the researcher to define the state or presence of specific variables, to show later the change of the variables of interest or new outcomes differentiated between the group being studied and the comparison group. This makes it possible to identify causal relationships between individuals with or without a specific risk factor (cause), and to attribute the changes related to the outcomes (effect). Different covariates or potential confusing factors that could interrelate among the groups in the follow-up are evaluated in parallel, as well as the presence of normal changes in the process of aging that are present and interconnected throughout the study in such a way that, if the perspective of aging in these studies were not considered, they could establish spurious and non-causal relations between the initial state of the variables of interest, their exposure, and their final outcomes [11, 12] (Fig. 7.1).

Proposed outline of the scenario of a longitudinal study on aging
A clear example of the theoretical concept of this design is presented by the Canadian Longitudinal Study on Aging (CLSA) [13]. It is considered one of the most important studies in present and future geriatrics because it has the possibility of following up a representative sample of the Canadian population over 20 years, and will evaluate many medical and non-medical factors in the aging process (biological, psychological, social, lifestyle and economic). It will analyze how illness, health and well-being are influenced in older adults, and thereby achieve a better understanding of aging. The study began recruiting men and women between the ages of 45 and 85 years in 2010. Its Internet page announced in July 2014 that it has the first 40,000 subjects and its goal is to include a total of 50,000 participants to start the follow-up.
7.3 Advantages and Disadvantages of Longitudinal Studies
Longitudinal studies present important advantages over other observational designs (Table 7.1). It makes it possible to evaluate the incidence of a particular illness or outcome, and helps when investigating potential causes of a possible outcome, whereby evidence is shown from the follow-up of exposed and non-exposed subjects at the moment they present an event being studied for the first time, or when it is modified by action of the exposure. In addition, it reduces bias between the exposure and the event when observing these sequentially. This type of design allows researchers to evaluate multiple results that could be related to the exposure factor [12].
Longitudinal studies in the senior citizen population have helped with the understanding of the many complicated relationships among primary and secondary risk factors and health outcomes. Given that older adults have an increasing risk of adverse outcomes (of death and disability, for example) compared with other age groups, and numerous physio-pathological processes can be almost simultaneous, longitudinal observation of the facts during aging is of great value for scientific research [1, 2].
On the other hand, longitudinal studies share the disadvantages of observational studies if they are taken as the gold standard in the search for causality in clinical trials. The interpretation of causal relationships can always be limited by the presence of many confusing variables. Other disadvantages are the lack of control in allocation of exposure (the realm of experimental studies), which could bring about differential biases in factors related to the occurrence of the event within the exposed and non-exposed group [8, 13] and lastly, the follow-up brings with it uncontrollable losses for the researcher.
In studies based on the older population, the final statistical power of the sample is often affected for a number of health-related reasons. These could include problems like mortality rates of up to 20 % per year if people older than 70 years of age are included, hospitalization and reports of illness, disablement and accidents, all of which commonly account for high rates of non-response and therefore losses for the study. As well, unlike what is likely to happen with other age groups, there may be causes of a social nature that could affect the quality of the information between measurements such as: changes of domicile, given that old people often move from one house to another since they depend on their support and care network, or frequent changes of a key informant with consequent difficulty in obtaining consistent and valid information.
The definition of “baseline evaluation” could also constitute a serious dilemma when dealing with old people. This is because of a complex interdependence with time and relationships among individual factors and measurements of results that could fluctuate even at time zero in a study, involving the exposure factor and the event being studied, along with other associations of change. These must be taken into account for an adequate interpretation of the results. Thus, when working with older populations the causal relationships are multiple and bi-directional, and the qualification of exposure must be identified with care, based on a solid theoretical framework.
The changes or modifications in the exposure factor or added variables that influence the exposure as much as the event of interest through time require broad and organized field logistics as well as more financial resources to maintain the cohort [8, 14]. Despite the advantage of being able to study several results, they could turn out to be difficult to analyze when one result produces a secondary one, and so on.
In some cases, the chain of causality is not clear or there is no conceptual consensus about certain topics, as is the case for issues like geriatric syndromes, frailty and the sequence between functioning and frailty. The inefficiency of longitudinal studies for studying “rare” or “low-frequency” events is an important point when discussing the senior citizen population. This means data collection requires extended periods of time during which the possibility increases of encountering correlated events that make it difficult to define the predictive factors. For that reason it is fundamental to analyze clearly the type of topic that can be evaluated using this methodology, as will be discussed later.
7.4 The Importance of Longitudinal Studies in Research on Aging
It is a fact that aging and its relationship with demographic, social and technological changes have created important knowledge needs at every level, especially in the area of health. An example of this is the longitudinal study of several pathologies with aging that break the classic patterns of its natural history compared with younger generations [2]. Another is the study of variables that have a positive impact on the health of senior citizens for achieving longevity or successful aging or failing to do so, and the presence of events such as loss of functioning, cognitive deterioration and frailty. These studies help to meet the need for understanding aging from different perspectives [15–18].
With respect to the evaluation of interventions, although controlled clinical trials provide most of the evidence for evaluating their effectiveness, this type of design faces important ethical and logistical dilemmas, especially when evaluating older populations [18]. The presence of cognitive deterioration, multiple morbidity, polypharmacy, and other factors are variables that often limit the inclusion of these participants in clinical trials, in addition to the difficulty encountered when using a proxy to obtain informed consent [19, 20]. For those reasons observational follow-up of interventions added to the normal care of old people represents a viable alternative to carrying out clinical trials, where longitudinal evaluations of programs is especially important.
7.5 Methodological Scopes and Implications of Longitudinal Studies of Aging
Longitudinal studies have made important contributions to understanding aging [18], with research questions related to the course or prognosis of physical or cognitive functioning of old people, exposure to comorbidity, health conditions, and biological, environmental, social or emotional factors both negative and positive. One point that has also attracted much interest is the scientific history of large-scale longitudinal studies in which groups from young populations have been included who are evaluated right through until they reach old age, thus providing evidence of latent changes over time and the multiple relationships with their environment. Those contributions base their knowledge about the course of life in the older population not only on the demographic evolution of the cohorts but on biological changes, roles and socio-cultural needs presented through time and dependent on the different stages of development of human beings from birth to death [21, 22].
To analyze the changes caused by aging over time and the relevant issues for that stage of life, a systematic review that included 51 longitudinal studies of aging was taken as a reference point [22], identified from the data base of longitudinal studies of the United States federal government’s National Institute on Aging (NIA). This enabled the researchers to establish six non-exclusive topics of frequent interest. In 44 % of the studies questions were asked about cognitive function, 51 % on health and physical performance, 55 % on socio-economic status and 63 % of the cases analyzed predictors of multi-morbidity and mortality. However, it is interesting that areas considered important such as health costs or genetic factors were not reported among the most frequent themes.
The authors of this review postulate that the guidelines of the longitudinal studies on aging should be broader to provide strategic information on health systems for the care for old people. Table 7.2 summarizes the topics identified by the authors as being those most frequently considered in the studies didactically included in their review. For this chapter issues are included in place of variables or measurement scales as expressed in Table 7.3 of the original article. Despite the fact that the topics are analyzed relatively frequently, their relationship with other variables is reported less frequently. This is the case of the impact of cognitive decline in the results on health and the use of services, or the effect of social determinants on quality of life. As for clinical questions, what stood out was those biological variables that could become predictors of morbidity-mortality as metabolic, hormonal, immunological or other measurements that require time-dependent analysis.
To exemplify the approach and methodology of longitudinal studies in aging, we present below a review of some of the projects that we believe to be representative of this type of study [23–27]. We should mention that the examples presented correspond to follow-up studies more than to the classic epidemiological cohort design that include the definition of an exposure. A brief summary of these studies is presented in table 7.3. The central themes are similar: identifying functional, social and environmental variables as predictors that change outcomes in aging. The average time of follow-up was 10 years. In Mexico the study with the longest follow-up is the Mexican Health and Aging Study (MHAS) [23] with three measurements over 11 years. The longest study is the Baltimore Longitudinal Study of Aging (BLSA) [24] at 54 years; it is also the longest of its kind in the United States. The Australian Longitudinal Study of Aging (ALSA) [25, 26] carried out a total of 11 measurements on its participants over a period of 18 years. With respect to the populations selected, only the English Longitudinal Study of Aging (ELSA) [27] and the MHAS took representative samples from their country of origin. The average age of the cohorts when they entered the study was 50 years, except for the BLSA, which included healthy volunteers of 18 years of age or more to recreate the normal course of aging over time, in contrast with the ALSA, which started with senior citizens 70 years of age or older.
As for methodological aspects, the ELSA included five measurements at two-year intervals, the first one in March 2002 with 11,391 subjects and their spouses (n = 708), chosen from the base of participants in the Health Survey of England (HES), a transversal survey carried out between 1998 and 2001. The criteria of eligibility were: having been born before March 1, 1952, participated in the HES, and lived in a private house at the time of the first measurement; the last measurement was done in 2011 with 10,317 subjects, with a response rate of 78 %. The lack of response was minimized from subsequent imputations. In the BLSA, the first transversal measurements were done in 1948, and ten years later it was integrated the first measurement of the cohort that started with 1,200 healthy volunteers 18 years of age and over; between 1958 and 1998 there were 2,264 participants. This study was conceived as an active cohort with transversal measurements every three years and the entry of new participants. Despite being the study with the largest biological data bank, its sample is not representative.
The ALSA is a classic example of longitudinal studies in adults 70 years of age or older in Australia, but despite the fact that the population was taken from a random sample from the electoral data bases and stratified by age and sex, the size of the sample was not representative of the population. This study included 11 measurements starting form a baseline measurement done in 1992 with 2,087 participants. The sample shrank over the time of the measurements and by the eighth measurement the population was 349 participants. Compared with the other studies analyzed, it had the largest attrition rate of response, with mortality being the most probable event for the subjects in the cohort.
Lastly, the MHAS is a panel study representative of the Mexican population of subjects born in 1951. The purpose of this study is to evaluate the aging process of the Mexican population, especially changes in morbidity, disability, intergenerational transference systems, migration and economy, for which measurements were carried out. In 2001, 15,402 interviews were completed, directly or with a proxy, with a response rate of 93 %. In 2003 the survey included 14,386 subjects, and in 2012 it included those interviewed in 2003 plus a new sample of persons born between 1952 and 1962, for a total of 18,465 persons, with one measurement more planned in 2015.
7.6 Strategies for Improving the Validity and Generalization of Longitudinal Study Results
One of the objectives of the longitudinal studies is to recreate, from an initial exposure or measurement, the natural history or trend of an illness or event at the time it occurs. To do that, measurement stages are established that enable the identification of changes in a particular group that is followed through time [19]. Most phenomena related to aging are time-dependent [18, 28], as much in their appearance as in their duration, so it is necessary to predict the changes over time or the cumulative effect of multiple associations with respect to the intervals of the measurements done, for example variables associated with functional or cognitive decline, or predictors of morbidity-mortality or frailty.
Another peculiarity of longitudinal studies in geriatric population is the speed of change of age-related variables that might be presented in cutoff periods or jump between subsequent measurements. Thus the basic threat to this design is centered on the study’s losses from any number of causes. There is a lack of response in key variables [29, 30] before the presence of unexpected adverse events that could arise in the development of the longitudinal studies, such as death, hospitalization, disability of a participant or even changes in geographic mobility, for which the data are lacking, and so losses in longitudinal studies become a frequent challenge. For this reason, prior to the start of the study, strategies for containment of losses should be established, such as strategies of quality control and retention that minimize these problems and ensure the validity of the information.
This phenomenon of losses during the course of a study is known as attrition or wearing away. It affects the sample size and makes it difficult to calculate the estimators, such as making an adequate statistical inference. As well, it could result in selection bias when the participants who remain in the study present conditions different from those who were lost. The causes of attrition in studies of old people are often related to death, hospitalization or disability that occur when the participant cannot be evaluated during the measurement period. However, the participants might reappear in a third or fourth measurement, so that subsequent analyses could be more complex [31].
On the other hand, the missing data could be due to a general pattern when a participant refuses to participate. Or, it might follow specific patterns when the individuals fail to answer specific questions, or when the interviewer does not properly follow the steps for questioning, or the data capture process is wrong. For that it is necessary to analyze some variables that make it possible to contrast them with the sample in general, and could be estimated if the absence of data affects the internal validity of the study [30, 31].
There are strategies that could be planned and executed during fieldwork, such as home visits, telephone contact, or the incorporation of interviews with proxy informants such as primary care givers or the participant’s spouse, who could provide responses close to what would have been given by the participant. Fieldwork could be enriched by using retention methods (positive messages, contact on important dates, information on the progress of the study, etc.) with the goal of minimizing the fatigue of staying in a follow-up over many years. A special element when working with older populations is offering the profile of interviewers, which demonstrates interest and empathy with the interviewees. It is thought to be useful in retaining subjects if the same interviewers are present during the different measurements, since that could create a climate of confidence with older adults and avoid rejection in subsequent measurements.
With the real possibility of failure to get information or sustaining losses during follow-up (whether they are occasional or constant), analytic strategies are required that reliably estimate the measurements made. However, it must be kept in mind how important it is to plan a study of this magnitude properly, especially in key sections that will be tied to the occurrence of losses, as well as including supervision strategies of data quality that enable later analysis to minimize the losses.
7.6.1 Sampling and Sample Size
It is crucial to make the right decision on how the sample in the first measurement will be set up, since errors committed in this phase will be very difficult to correct later. In this sense it must be ensured that each sample unit or individual is chosen randomly from the sample framework as a probability sample, to increase the precision of the study by being able to ensure that the samples are really independent right from the start of the study. As well, the sample size must in all cases take into account a percentage of real losses consistent with the theme of the study or area of influence of the participants. It is necessary to have a large enough number of observations, given that attrition tends to reduce the number of individuals over time, and so a size that will allow for the occurrence of said losses must be ensured. That way, the analysis may be carried out in the sub-groups of the population of interest without exposing the statistical power of the study at risk.
7.6.2 Standardization of the Measurements
As discussed earlier, longitudinal studies are based on the change of variables through time, for which the presence of random errors in the measurements represents a very complex problem, which could even overestimate the final results of the measurements. In this situation is especially useful to include not only previously validated and standardized instruments, but also to carry out exhaustive training of the field personnel, adding control questions that permit the analysis of differences at a given time and reduction of false data of change in the variables of interest, and carrying out a periodic calibration of the measurement equipment.
7.6.3 Imputing Lost Data
This requires the implementation of generalized equations, for which there are several statistical methods. In general, it is thought that in the first instance variables should be created that identify the data “without response or without measurement” in each measurement cut-off. This dichotomy of variables will serve as sub-groups within the study for the key variables, the reason for the imputation [30]. These variables must be compared between the defined times as losses (for example, an initial or baseline measurement vs. the second or third vs. the fourth measurement). This type of analysis considers the measurements between periods to be dependent, since they are from the same subjects, as happens in the case of the panel type study or the design of cohort study, so they must be seen as paired statistical tests, in order to establish whether or not there are statistically significant variations between the measurement times. If not, it will verify that the losses did not affect the behavior of the variables; otherwise, if it proves that the data do have variations between measurements, a multivariate probit model will be integrated that predicts the probability of attrition conditional on a set of variables measured in each cut-off during the study. This model identifies the common source of the data variation and is integrated as a possible response to the matrix model in seeking the most common responses. In any case it can mathematically predict the variability of the error, and if this does not have statistical significance, the data are presented as being free from error [29, 32, 33].
7.6.4 Data Weighting
This process is fundamental for an adequate estimate of the data. Reasons for the need to weigh the variables involved include the lack of responses, unequal selection of groups, adjustments in medication, and others.
Weighting involves giving each sample unit a numeric value that would be representative of its population being studied. Thus the weight of each variable in particular includes the relative value of the sub-sample it represents and the relationship between the size of the sample and the proportion of subjects interviewed. A process of statistical inference for each variable or time period involved is developed from these values. It should be mentioned that weighting in a longitudinal study could include transversal weighting (within the same measurement time) or between subsequent measurements –time zero vs. n times involved [31, 34].
7.7 Conclusions
Science had never before faced such a complex, dynamic and time-dependent process as human aging. Longitudinal studies are a source of fundamental evidence of the multi-factor changes over time, which enables it to maintain the evaluation of interventions that have a timely and positive impact on the course of aging in the population.
Longitudinal methodology represents a milestone in geriatric research. Its implementation always has to be backed up by good planning that takes into account standardized procedures as well as techniques that minimize the probable losses during the follow-up and the consequent effect throughout the study. Finally, it will be expected that the results derived from the follow-up will reflect the evidence of a phenomenon present in the senior citizen population.
References
Faes M, Van Iersel M, Olde Rikkert M (2007) Methodological issues in geriatric research. J Nutr Health Aging 11(3):254–259
Tappen RM, Ouslander JG (2010) State-of-the-art in longitudinal studies on aging: an overview of the supplement. J Am Geriatr Soc 58(Suppl 2):S283–S286. doi:10.1111/j.1532-5415.2010.02912.x
Ruspini E (1999) Longitudinal research and the analysis of social change. Qual Quant 33(3):219–227
Goldstein H (1979) The design and analysis of longitudinal studies: their role in the measurement of change. Academic, London
Trivellato U (1999) Issues in the design and analysis of panel studies: a cursory review. Qual Quant 33:339–352
Eldredge J (2002) Cohort studies in health sciences librarianship. J Med Libr Assoc JMLA 90(4):380–392
Furst DE (2004) Observational cohort studies and well controlled clinical trials–we need them both! J Rheumatol 31(8):1476–1477
Burch TK (2001) Longitudinal research in social science: some theoretical challenges. Can Stud Popul 28(2):263–283
Hernández-Ávila M, Garrido-Latorre F, López-Moreno S (2000) Methodologic studies design. Salud Publica Mex 42(2):144–154
Fuller GF (2000) Falls in the elderly. Am Fam Physician 61(7):2159–2168
McNutt LA, Wu C, Xue X, Hafner JP (2003) Estimating the relative risk in cohort studies and clinical trials of common outcome. Am J Epidemiol 157(4):940–943
Lazcano-Ponce E, Fernández E, Salazar-Martínez E, Hernández-Ávila M (2000) Cohort studies. Methodology, bias and application. Salud Publica Mex 42(3):230–241
Kirkland S. The Canadian longitudinal study on aging as a platform for resear on aging. In: Gerontology CAo, ed. 41st annual scientific and education meeting of the Canadian Association on Gerontology; Vancouver. http://www.clsa-elcv.ca/news/clsa-cag20122012
Healy P, Devane D (2011) Methodological considerations in cohort study designs. Nurse Res 18(3):32–36
Bowling A (2002) Research methods in health: investigating health and health services, 2nd edn. Open University Press, Philadelphia/Buckingham
Carlson MD, Morrison RS (2009) Study design, precision, and validity in observational studies. J Palliat Med 12(1):77–82. doi:10.1089/jpm.2008.9690
Schaie KW, Hofer SM (2001) Longitudinal studies in aging research. In: Birren JE, Schaie KW (eds) Handbook of the psychology of aging, 5th edn, Handbooks on aging. Academic, San Diego, pp 53–77
Newman AB (2010) An overview of the design, implementation, and analyses of longitudinal studies on aging. J Am Geriatr Soc 58(Suppl 2):S287–S291. doi:10.1111/j.1532-5415.2010.02916.x
Rochon PA, Gurwitz JH, Sykora K, Mamdani M, Streiner DL, Garfinkel S et al (2005) Reader’s guide to critical appraisal of cohort studies: 1. Role and design. BMJ 330(7496):895–897. doi:10.1136/bmj.330.7496.895
Kaufman SR, Shim JK, Russ AJ (2004) Revisiting the biomedicalization of aging: clinical trends and ethical challenges. Gerontologist 44(6):731–738
Heinz W, Marshall V (2003) Social dynamics of life course: transitions, institutions and interrelations. Walter de Gruyert Inc., New York
Stanziano DC, Whitehurst M, Graham P, Roos BA (2010) A review of selected longitudinal studies on aging: past findings and future directions. J Am Geriatr Soc 58(Suppl 2):S292–S297. doi:10.1111/j.1532-5415.2010.02936.x
Wong R, Espinoza M, Palloni A (2007) Mexican older adults with a wide socioeconomic perspective: health and aging. Salud Publica Mex 49(Suppl 4):S436–S447
Ferrucci L (2008) The Baltimore Longitudinal Study of Aging (BLSA): a 50-year-long journey and plans for the future. J Gerontol A Biol Sci Med Sci 63(12):1416–1419
Logie H, Hogan R, Peut A (2004) Longitudinal studies of ageing: implication for future studies. AIHW http://www.aihw.gov.au/publication-detail/?id=6442467659. Accessed 18 Dec 2012
Luszcz M (2013) The Australian Longitudinal Study of Ageing: 15 years of aging in south Australia. In: South Australian Department of Families and Communities. http://www.flinders.edu.au/sabs/fcas/alsa/alsa_home.cfm. Accessed 24 Jan 2013
Steptoe A, Breeze E, Banks J, Nazroo J (2013) Cohort profile: the English Longitudinal Study of Ageing. Int J Epidemiol 42(6):1640–1648. doi:10.1093/ije/dys168
Harman D (1981) The aging process. Proc Natl Acad Sci U S A 78(11):7124–7128
Palmer RF, Royall DR (2010) Missing data? Plan on it! J Am Geriatr Soc 58(Suppl 2):S343–S348. doi:10.1111/j.1532-5415.2010.03053.x
Ayala Y, Melo O (2007) Estimación de datos faltantes en medidas repetidas con respuesta binaria. Rev Colomb de Estad 30(2):265–285
Feng D, Cong Z, Silverstein M (2012) Missing data and attrition. In: Newsom J, Jones RN, Hofer SM (eds) Longitudinal data analysis: a practical guide for researchers in aging, health, and social sciences. Taylor & Francis, London, pp 71–97
Erten-Lyons D, Sherbakov LO, Piccinin AM, Hofer SM, Dodge HH, Quinn JF et al (2012) Review of selected databases of longitudinal aging studies. Alzheimers Dement 8(6):584–589. doi:10.1016/j.jalz.2011.09.232
Delgado Rodriguez M, Llorca DJ (2004) Longitudinal studies: concepts and particularities. Rev Esp Salud Publica 78(2):141–148
Lynn P (2005) Metodología de las Encuestas Longitudinales: Concepto y Particularidades. Seminario de Estadística, Euskadi
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
García-Peña, C., Espinel-Bermúdez, C., del Pilar Torres-Arreola, L., Pérez-Zepeda, M.U., Gutiérrez-Robledo, L.M. (2015). Longitudinal Studies. In: García-Peña, C., Gutiérrez-Robledo, L., Pérez-Zepeda, M. (eds) Aging Research - Methodological Issues. Springer, Cham. https://doi.org/10.1007/978-3-319-18323-7_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-18323-7_7
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18322-0
Online ISBN: 978-3-319-18323-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)