
Abstract
As advances in medicine have significantly reduced mortality and ameliorated morbidity for children, thus increasing numbers of children are living with congenital or acquired physical disabilities and related special health care needs. The consequence of disability on function, independence, ease of care and personal comfort is a priority for this group of children and their families. Pediatric Physical Medicine and Rehabilitation, also known as pediatric physiatry, focuses on comprehensive care to optimize patient function and manage complex issues in collaboration with other health care professionals. Interventions occur via consultation in both inpatient and outpatient settings, or through ongoing management in structured care programs. Medical decisions and approaches are augmented by procedural interventions directed at improving diagnostic specificity and prognostic outcomes. Pediatric physiatrists fill a unique niche in the care of medically complex children who have historically been received less integrated and more fragmented care. This results in improved continuity of care, improved coordination across multiple providers, more efficient use of therapeutic and technological interventions, and better patient/family satisfaction.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Traumatic Brain Injury
- Spinal Cord Injury
- Cerebral Palsy
- Child With Special Health Care Need
- Traumatic Brain Injury
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Physiatry has its origin from the Greek words “physis,” pertaining to physical phenomena, and “iatreia,” meaning physician. The field of physiatry first developed in the United States, as a consequence of the need to treat injuries sustained during World War I, as well as the often long lasting rehabilitation needs that followed. However, it was not until after World War II, with more substantial war injuries and the poliomyelitis epidemic that soon followed, that rehabilitation services and care became more relevant. The specialty of physical medicine and rehabilitation (henceforth referred to as physiatry) became a board-recognized subspecialty in 1947 [1]. The field of pediatric physiatry has a history that started with Dr. Gabriella E Molnar (1926–2011). She focused on the unique needs of children, and how they were different from the needs of adults, by acknowledging in her plans the evolution of physical, intellectual and emotional abilities of children over time [2].
The goal of a physiatrist is to develop a comprehensive treatment plan for patients with physical disabilities. The physiatrist develops the treatment plan individually, or participates in the development of an interdisciplinary plan, that incorporates other providers such as speech and language pathologists, physical therapists or other physicians such as neurosurgeons or orthopedic surgeons. By evaluating a patient holistically, the physiatrist seeks to help patients improve their function and quality of life [1].
-
MS is a 10 year-old boy who was involved in a motor vehicle accident resulting in a seat-belt injury. He suffered a chance fracture tear his thoraco-lumbar junction and damage to his liver, spleen and kidneys. The pediatric physiatrist first saw the patient in the intensive care unit (ICU), then admitted him to the inpatient rehabilitation service. Following discharge from the inpatient service, the patient participated in a day rehab program, and then moved to outpatient follow up care.
Inpatient Consultation
In the pediatric ICU, the patient (MS) was extubated following surgery to repair the fractures of his spine. The injuries to his internal organs were managed conservatively. It was noted that the patient was not moving his lower extremities and he had some swelling in his lower extremities, and he had significant challenges with urine and stool voiding. The pediatric physiatrist’s role was to help frame the diagnosis, explain how the seemingly disparate patient symptoms were related and chart a course forward to functional recovery. That conversation started with the patient and family to help them understand the clinical findings of a “complete” spinal cord injury resulting in paraplegia, a neurogenic bowel and a neurogenic bladder. It continued with the primary team in the ICU to discuss associated conditions and their management to prevent secondary complications and speed recovery. Next, there began a series of interventions by a team of therapists and family support professionals to evaluate and document the degree of independence the patient had with various mobility tasks and activities of daily living, as well as the patient and family’s response to this catastrophic injury. It is crucial in these instances to understand the medical aspect of the patient’s diagnoses. However, the physiatrist maps those findings to functional deficits and provides a prognosis for recovery of those deficits. In mapping interventions to address the deficits, it is important to understand the psychosocial context of the recovery. For example, was the patient environment amenable to one that has challenges walking independently, or does the patient live in a setting dominated by stairs? Finally, during the initial discussion about diagnosis and prognosis, the patient and family first start to register the gravity of the injury and begin the stages of grief associated with loss. Coordinating support for the grief associated with catastrophic disability is a critical part of physiatry planning.
Inpatient Rehabilitation
Once MS was stable enough to leave the ICU, he could not yet be discharged home. Barriers to discharge included a lack of mobility and positioning equipment, a lack of patient and family training to manage a spinal cord injury and associated symptomology and, in this case, disability, and continued medical management of anemia, leg swelling, pain and healing surgical wounds. The pediatric physiatrist is crucial in documenting the needs of the patient, presenting a detailed personalized plan for recovery, and assisting in planning for any continued inpatient hospitalization and/or inpatient rehabilitation services. In the era of accountable-care and patient-centered interventions, the comprehensive functional perspective of the pediatric physiatrist serves a critical function of documenting the starting point or baseline of a patient, laying out reasonable patient-centric functional targets, and then estimating how long it should take to reach those functional goals. For MS, he was completely paralyzed as evidenced by the T12 ASIA A classification of his spinal cord injury. That classification infers that he has no motor or sensory control below the level of his navel. Thus, he will not be able to stand or walk under his own strength, he has no volitional control over his urine and stool voiding, and he is at risk for pressure ulcers and wounds due to poor sensation in his lower extremities. A child with these types of injuries can be expected to require 20–30 days of inpatient rehabilitation services based on national averages. By discharge from inpatient rehabilitation, a child like M.S. should be able to transfer into and out of a custom wheelchair, and demonstrate wheelchair mobility independence on household and some community surfaces. In addition, the patient should be weaned off of pain medications as postoperative pain decreases. Bowel and bladder management is a skill possible in children cognitively older than 8–9 years. Thus, in addition to training the parents in clean intermittent catheterization of the bladder and a program of suppositories and digital stimulation for the bowels, MS was trained directly. Lastly, adaptive and durable medical equipment appropriate to the disability are sought based on the coordinated efforts of the physiatrist and the therapist. Patient input and perspective is an important part of the success of any inpatient rehabilitation process.
Day Rehabilitation Programs
Once MS was medically stable and suitably mobile to live outside of the hospital, a coordinated program to transition him back to school and the community was in order. A day rehabilitation program was the next step in MS’ recovery and progression towards independence. In this setting, MS was supported toward his return to school, as well as in exploring his avocational interest in the context of his new physical deficits. Patients in this stage are also monitored for late complications related to their initial injury. Higher-level wheelchair skills, problem solving for the patient as they navigate accessible and less accessible aspects of their community is important. Often, this is when the depth and true impact of a child’s disability becomes tangible to the patient and family. Thus, psychological support services and family counseling are as important to the patient outcome as minimizing skin sores, urinary tract infections and insufficiency fractures. Throughout this complicated medical and emotional process, there must be continued functional progress toward maximal independence. This phase of rehabilitation care lasts weeks to months depending on the progress of the child, the complexity of their home environment and the minimization of complications.
Outpatient Rehabilitation Management
Finally, the patient transitions to the outpatient maintenance phase of care. At this stage of recovery, anticipatory guidance about lifetime issues related to reproduction, bone strength, scoliosis, and sport/recreation become essential to the intersection of health and function for the child. The physiatrist continues to manage bowel and bladder programs as well as muscle spasticity related to the spinal cord injury. The pediatric physiatrist communicates with the primary care doctor, as well as any other provider appropriate to the needs of the child, to make certain that any special aspects of care are integrated into the standard growth and developmental issues. For example, involving urology if bladder management is suboptimal due to poor capacity or frequent infection, or engaging with an orthopedic surgeon for a neuromuscular scoliosis, are appropriate functions of the physiatrist.
Background
The incidence of childhood disability has dramatically increased over the past half of a century from approximately 3 % in 1969 to 15.1 % in 2009. This dramatic rise is in part due to the advances in medical treatments and technology as well as to awareness of disability and the inclusion of children with behavioral and developmental disorders [3, 4]. Although children with disabilities are a relatively small part of the population, they account for nearly 50 % of hospital days and hospital charges [5].
Pediatric physiatrists treat children who have or are at increased risk for a chronic physical, developmental, behavioral or emotional conditions and who also require health and related services of a type or amount above what are required by children generally. This group of children who frequently require multiple subspecialists and other providers to meet their health care needs has been identified as Children with Special Health Care Needs (CSHCN) [6]. For this group of children coordination of care has been shown to result in better outcomes and fewer hospitalizations. This coordination of care has been characterized as a medical home by the American Academy of Pediatrics, is “accessible, comprehensive, coordinated, compassionate, family-centered, community-based, and culturally effective” [6]. A medical home not only improves that access to quality services [7], but also results in enhanced parent satisfaction [8].
In pursuit of improved function and quality of life for CSHCN and their families, a pediatric physiatrist relies on being able to communicate with other providers to better understand a child’s function. This is particularly important in several aspects of care, including the ways in which appropriate therapeutic goals for are determined and communicated, as well as setting reasonable expectations for the child and the family.
Classification of Function
Scales that are used to assess functioning of children with neuromotor disabilities are very helpful in guiding interventions as well as gauging benefits of interventions and progress. There are many different scales that are used in different clinical situations.
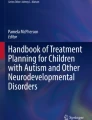
For example, children who have CP are classified by gross motor function (see Fig. 87.1). This scale measures the ability of the child to move and control his or her body in space. Those in Level I are able to function without limitations, but still may have impairments with speed, balance and coordination. In Level II, children are also able to be independent but may have functional limitations in climbing stairs, uneven terrain or in crowds. Children in Level III need an assistive device such as a walker or crutches for even surfaces but may need a manual wheelchair for longer distances or more complicated terrain or spaces. Children in Level IV require a wheelchair for the majority of their mobility but are able to control their wheelchairs. Children in Level V require complete support for positioning and mobility.


Classifying cerebral palsy (Adapted from Graham HK. Classifying cerebral palsy. J Pediatr Orthop 2005;25:128)
The levels are further defined by age of the patient to show the developmental progression of a child at a given level over time. By way of these functional classifications, a health care provider is able to predict what functional tasks are within the future ability of a given patient and plans can be made to provide appropriate mobility support over the lifetime of the child [9]. A child may also have a different classification based particular environmental consideration. For example, a child may be classified at Level III at home and in school, but at Level IV when in the community more generally.
For spinal cord injury patients, the American Spinal Injury Association created a consensus classification system across medical and surgical specialties with input from therapists. It classifies children with a spinal cord injury based on motor and sensory function. In addition to being descriptive of the child’s level and extent of paralysis, there are accepted functional abilities for each level and clear associated prognoses of recovery [10].
The Rancho Los Amigos Scale is one used for Traumatic Brain Injury. The revised edition (see Table 87.1) categorizes patients from level I (most impaired) to level X (least impaired). It allows providers to move beyond the binary notation of injured or intact and give more indication of degree [11]. Using a scale such as this allows providers to use common language in treatment and planning, and can be useful information for the patient and family about future expectations and challenges. It also allows interventions to be structured in a manner most appropriate for the patient’s cognitive and functional impairment, as well as in measuring progress in the patient’s recovery.
In addition to disorder-specific scales, there are more global scales like WeeFIM, an adaptation for children of the FIM (the Functional Independence Measure), that are helpful in classifying functional skills by developmental/age expectation. Thirteen of the scale’s 18 items are motor tasks, with the remaining five related to cognitive function. Each item is ranked using an ordinal scale from 0 (activity does not occur) to 7 (activity is done with full independence). The WeeFIM is used extensively to demonstrate the functional impact of treatment interventions on patients over time and to show progress.
Physiatrists incorporate many scales in practice to communicate with other health providers, plan appropriate interventions, allow accurate functional prognostication, and demonstrate progress.
Procedures
Pediatric physiatrists manage the consequences of disability. There are multiple interventions within the tool kit of the specialty. Complex Spasticity management, musculoskeletal interventions and EMG/NVS diagnostics represent the majority of the procedures done by this specialty. For spasticity management, focal intervention is typified by botulinum toxin injections. Dosing and dilution is essential and muscle selection, with an eye towards function, is critical for executing an intervention what will have the desired effect to improve patient function. More global spasticity management, without using oral medications, is achieved with intrathecal Lioresal. For this intervention, 1/100th the oral dose of Lioresal is administered in the intrathecal space to allow direct action at the level of the spinal cord. For musculoskeletal pain and inflammation, injection of local anesthetics along with or in place of steroids is efficacious. Bursal injections, joint space injections and trigger point injections (or dry needling), are done by pediatric physiatrists – especially for older teens. Finally, EMG and NCS are diagnostic extensions of the physical exam that clarify pathologies of the peripheral nervous system and muscles.
Equipment/TECH/DME
In addition to physiological and physical interventions, durable medical equipment, assistive technology, orthotics and prosthetics are important tools in improving function and independence. Equipment and devices should be developmentally appropriate and of a weight and size that the child is able to utilize. The pediatric physiatrist will work in conjunction with therapists, orthotists, prosthetists and others engaged in the design and customization of equipment to the needs of a child in order to determine the appropriate equipment for a child. Most important in prescribing any piece of equipment such as an augmentative communication device or environmental controls, however, is the patient and the family, who together must agree on the necessity and function of the device in order to maximize the chances that it will be fully and most effectively used.
Durable medical equipment, which includes specialized bedding, specialized seating and mobility devices, positioning apparatus, recreational devices and technology to assist with communication, can be a significant need for improvement of function and quality of life for the child and for the family. Orthotics are bracing and support devices for an existing part of the body that requires stabilization. Prosthetics are devices that replace a missing portion of the body. In children, these devices must be altered to allow for physical growth and must be adaptable to developmental milestones.
General Health Issues to Consider in Healthcare and Rehabilitation
Many childhood disabilities affect growth and nutrition. Children with neurologic impairment often have difficulties maintaining appropriate caloric intake due to difficulties with swallowing, coordination, or communication and are at significant risk of under nutrition [3]. Conversely, children who are non-ambulatory and have less muscle bulk (i.e. a patient with a spinal cord injury or spina bifida) are less active and have less caloric needs than their ambulatory peers and therefore, are at risk of obesity and the associated medical complications, including a further significant loss of function.
CSHCN are also vulnerable to sleep disorders. Poor sleep may be due to motor impairment, pain, visual impairment, abnormal muscle tone and frequent repositioning, medications or overnight feeding needs that may also cause frequent interruptions in sleep. Stays in hospital, which are more common and frequent for CSHCN, may also impact sleep-wake cycles. Sleep dysfunction can cause problems with both daytime behavior and school performance. Furthermore, if the child is having more sleep difficulties the child’s family is also getting poor sleep, which may further exacerbate stress and irritability within the home [12].
Visual and Hearing impairments are also frequent in CHSCN. Children with CP or traumatic brain injuries (TBI) are at significant risk for cortical and other visual impairments, requiring frequent evaluations by an ophthalmologist [13]. Children who require steroids for health maintenance such as children with cancer, juvenile rheumatoid arthritis or muscular dystrophy are at risk for cataracts. Many children who have had complicated Neonatal Intensive Care Unit (NICU) stays requiring ototoxic antibiotics, or who contracted meningitis, CMV or have had TBI are at risk for hearing impairments and must have appropriate health screening exams.
Children with CP are at significant risk for contracture(s) due to both immobility and/or spasticity. If a joint is immobilized or under mobilized, structural changes in the joint and soft tissue can lead to contractures [14]. Spasticity results from an imbalance between the excitatory or inhibitory input from the alpha motor neurons and causes an increase in activation of the antagonist muscle due to damage to central nervous system. Spasticity can also contribute to weakness and poor coordination [15], as well as secondary changes to muscle, tendon and collagen tissue causing stiffness, fibrosis and atrophy [16]. Uncontrolled spasticity will interfere with mobility and range of motion, contribute to contractures and interfere with activities of daily living, as well as result in pain [17]. When managing spasticity, the physiatrist must balance both the positive and negative effects of increases in muscle tone [18].
In patients who are immobile or wheelchair dependent there is an increased risk of pressure ulcers. Factors that contribute to an ulcer may include prolonged pressure, immobility, shearing, friction, and poor nutrition. Urine and fecal incontinence may also play a role in the development sores [19]. This group of children are also at increased risk for osteopenia and osteoporosis that can contribute to pathologic fracture or chronic pain. Immobility, poor nutrition and seizure medications increase risks of developing decreases in bone mineral density [20].
Children with cerebral palsy (CP), muscular dystrophies and spinal cord injuries are at greater risk for restrictive lung disease and nocturnal hypoventilation, hypoxemia and/or hypercapnia.
Attention to health promotion and prevention of these and other secondary medical problems is crucial in order to optimize physical performance, function and quality of life.
Team-Based Support
Pediatric physiatrists are also involved in multidisciplinary clinics where they work in concert with other physicians or allied health professionals to develop medical and care plans. Real time input from multiple specialties allows for specific interventions and care plans to be carried out with enhanced continuity and efficiency. The physiatrist will also participate in disorder-specific interdisciplinary clinics such as a spina bifida clinic, which will include the physiatrist, urologist, neurosurgeon and orthopedic surgeon; a neuromuscular clinic may consist of a physiatrist, a neurologist, orthopedic surgeon, a pulmonologist and a genetic counselor; a cerebral palsy clinic may include therapists, orthotists, wheelchair specialists, developmental pediatricians, nutritionists, psychologists, and social workers. Team-based, coordinated care is crucial in addressing and preventing problems associated with complex medical diseases and maximizing function and quality of life and is also highly beneficial for the families who have one visit for many services – and they are coordinated!
Some Team Members
Physical therapists (PT) work on improving strength, range of motion, balance, coordination and complex motor skills. They utilize an array of manual techniques, treatment modalities and equipment to provide age and developmentally appropriate interventions. These therapists are essential in developing care plans and identifying appropriate medical and therapeutic equipment to address functional deficits and build skills for the children.
Occupational therapists (OT) work on improving strength, range of motion, fine motor skills, and gross motor skills towards improving a child’s activities of daily living and independence, such as personal care (e.g., feeding), hygiene (e.g., bathing and grooming) and independent community activities (e.g., shopping). Occupational therapists, as with their PT colleagues, also frequently make use in treatment planning of durable medical equipment, such as a shower chair, to help assist in performing activities of daily living. In some centers, OT’s work with body positioning and motor skills to improve feeding.
Speech and language pathologists (SLP) evaluate and provide interventions for expressive and receptive language skills as well as with the oral motor aspects feeding and swallowing. They often recommend advanced studies evaluating swallowing function like oral-pharyngeal motility studies (OPMS) and fiber-optic endoscopic evaluation of swallow (FEES) studies and often partner with radiology for these studies.
Psychology and neuropsychology services perform patient-centered testing and supportive intervention for the identification of strengths and deficits. They may also participate in managing the larger family stress and dynamics associated with the multiple aspects of managing their child. Full neuropsychological evaluations are often required and can be very helpful with the development and implement of Individualized Educational Programs (IEP) at school. The neuropsychological evaluation includes multiple neurocognitive domains including intellectual abilities, verbal and language skills, visual-spatial, sensorimotor, visual motor skills, attention, memory, learning, executive functioning, adaptive skills, and pre-academic and/or academic abilities [21].
In addition to these aforementioned disciplines, a comprehensive team should include other providers that may be appropriate to a particular patient’s health status and/or intervention needs.
A teacher or appropriate educational specialist can be an essential interface between the treatment team and the home and school systems facilitating the necessary integration of the medical plan and neuropsychology recommendations into the school program.
Recreational therapists work with children to help restore motor, social and cognitive functioning. They work to improve participation in community and social situations using modalities such as arts and crafts, drama, music, dance, sports, games, and community reintegration field trips. This helps children to develop coping skills, build confidence, and integrate skills learned in treatment settings into community settings as well as improve the child’s physical, social, and emotional well-being.
Child life therapists provide therapeutic play and activities in the hospital setting to assist children with processing medical procedures, diagnoses and side effects. They are also important to facilitate re-entry of children from a hospital setting into the community, especially if the children had spent prolonged periods in the hospital with newly acquired disabilities.
Future Needs
Pediatric physiatry is a unique specialty providing comprehensive and coordinated care to the most vulnerable children requiring treatment. Successful practitioners have a strong foundation in medicine, a mastery of physical interventions and equipment, and prowess in procedural interventions. The small pipeline of candidates and the duration of training required limit the growth of the specialty. In addition, there are limited opportunities in training as there are less than 20 certified centers that produce one to two graduates per year. In addition, outcomes research on the treatment options utilized in the field is critical to providing a stronger evidence basis for the field. Pediatric physiatrists focus on optimizing function and are valuable leaders of a team of professionals that provide care for children with acquired or congenital physical disabilities.
References
The history of physical medicine and rehabilitation: An overview. Association of Academic Physiatrists, Hanover. URL: http://www.physiatry.org/?page=history.
Alexander MA, Matthews DJ, editors. Pediatric rehabilitation: principles and practice. 4th ed. New York: Demos Medical; 2010.
Ayyangar R. Health maintenance and management in childhood disability. Phys Med Rehabil Clin N Am. 2002;13(4):793–821.
Kaziny BD. The prehospital care of children with special health care needs. Clin Pediatr Emerg Med. 2014;15(1):89–95.
Berry JG, Hall M, Hall DE, Kuo DZ, Cohen E, Agrawal R, et al. Inpatient growth and resource use in 28 children’s hospitals: a longitudinal, multi-institutional study. JAMA Pediatr. 2013;167(2):170–7.
American Academy of Pediatrics. The medical home. Pediatrics. 2002;110(1 Pt 1):184–6.
Benedict RE. Quality medical homes: meeting children’s needs for therapeutic and supportive services. Pediatrics. 2008;121(1):e127–34.
Drummond A, Looman WS, Phillips A. Coping among parents of children with special health care needs with and without a health care home. J Pediatr Health Care. 2012;26(4):266–75.
Palisano RJ, Rosenbaum P, Bartlett D, Livingston MH. Content validity of the expanded and revised Gross Motor Function Classification System. Dev Med Child Neurol. 2008;50(10):744–50.
Waring 3rd WP, Biering-Sorensen F, Burns S, Donovan W, Graves D, Jha A, et al. 2009 review and revisions of the international standards for the neurological classification of spinal cord injury. J Spinal Cord Med. 2010;33(4):346–52.
Simard-Tremblay E, Constantin E, Gruber R, Brouillette RT, Shevell M. Sleep in children with cerebral palsy: a review. J Child Neurol. 2011;26(10):1303–10.
Ghasia F, Brunstrom J, Gordon M, Tychsen L. Frequency and severity of visual sensory and motor deficits in children with cerebral palsy: gross motor function classification scale. Invest Ophthalmol Vis Sci. 2008;49(2):572–80.
Akeson WH, Amiel D, Abel MF, Garfin SR, Woo SL. Effects of immobilization on joints. Clin Orthop Relat Res. 1987;219:28–37.
Zafonte R, Lombard L, Elovic E. Antispasticity medications. Am J Phys Med Rehabil. 2004;83(Suppl):S50–8.
Watanabe TK. Role of oral medications in spasticity management. PM R. 2009;1(9):839–41.
Ronan S, Gold JT. Nonoperative management of spasticity in children. Childs Nerv Syst. 2007;23(9):943–56.
Thibaut A, Chatelle C, Ziegler E, Bruno MA, Laureys S, Gosseries O. Spasticity after stroke: physiology, assessment and treatment. Brain Inj. 2013;27(10):093–105.
Benbow M. Pressure ulcer prevention and pressure-relieving surfaces. Br J Nurs. 2008;17(13):830–5.
Apkon SD. Osteoporosis in children who have disabilities. Phys Med Rehabil Clin N Am. 2002;13(4):839–55.
Zaccario M, Salsberg D, Gordon R, Bilginer L. Psychological and neuropsychological issues in the care of children with disabilities. J Pediatr Rehabil Med. 2009;2(2):93–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Vova, J., Sholas, M.G. (2016). Pediatric Aspects of Physiatry and Function. In: Rubin, I.L., Merrick, J., Greydanus, D.E., Patel, D.R. (eds) Health Care for People with Intellectual and Developmental Disabilities across the Lifespan. Springer, Cham. https://doi.org/10.1007/978-3-319-18096-0_87
Download citation
DOI: https://doi.org/10.1007/978-3-319-18096-0_87
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18095-3
Online ISBN: 978-3-319-18096-0
eBook Packages: MedicineMedicine (R0)