
Abstract
In recent years, a strong interest in microinvasive glaucoma surgery (MIGS) has developed due to the significant complication rates associated with more traditional glaucoma filtering procedures. The first-generation trabecular micro-bypass stent (Glaukos iStent®) bypasses the trabecular meshwork, which is the site of highest outflow resistance in open angle glaucoma. In the United States, this device is currently approved to be implanted in conjunction with cataract extraction to lower the intraocular pressure (IOP) and decrease the medication burden load on patients with mild to moderate open angle glaucoma. This chapter summarizes the specifications and indications for this device as well as the clinical studies published on the iStent’s efficacy and safety. There have been multiple randomized controlled trials demonstrating a significant drop in IOP and postoperative medication use while maintaining an excellent safety profile. In all the studies, there have been no serious adverse events directly associated with the device. Recently, Glaukos has developed a new model of the iStent, which is currently undergoing investigational studies, but shows promise in lowering the IOP even further.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
2.1 Introduction
In the past few years, there has been an increasing interest in microinvasive glaucoma surgery (MIGS) procedures as they may play a novel role in the glaucoma treatment algorithm. More traditional ab externo glaucoma procedures such as trabeculectomies and glaucoma drainage devices are known to very effectively reduce intraocular pressure (IOP), but are also associated with numerous sight-threatening complications that may occur even years after surgery (e.g., bleb leak, bleb-related endophthalmitis, hypotony) [1,2]. Because of the relatively high complication rates associated with filtration procedures, practitioners often turn to medications and/or laser trabeculoplasty as first-line therapies to reduce IOP [3]. However, many patients struggle with compliance and ocular surface issues with medications [4,5], and laser trabeculoplasty may only have a limited and modest effect [6,7]. The hope is that MIGS procedures will bridge the gap between medications and more invasive procedures for patients with mild to moderate glaucoma.
MIGS procedures utilize an ab interno approach, sparing the conjunctiva to allow for future glaucoma surgical procedures if necessary, and offer a much higher safety profile with smaller incisions and less distortion of the normal anatomy [8]. Compared to traditional filtering procedures, these procedures are often easier to adopt with fewer postoperative complications and therefore, can be utilized by both glaucoma specialists and comprehensive ophthalmologists in their armamentarium against this potentially blinding disease. Currently, there are several MIGS devices/procedures that may decrease IOP through either (1) improving trabecular outflow to Schlemms’ canal (trabectome, Neomedix, Inc.; iStent, Glaukos, Corp.; Hydrus microstent, Ivantis, Inc.), (2) improving outflow through the suprachoroidal space (Cypass, Transcend Medical, Inc.; iStent Supra, Glaukos, Corp.), or (3) creating an alternative outflow pathway through the subconjunctival space (Xen Gel Stent; Aquesys, Inc.).
It is thought that the primary site of outflow resistance in primary open angle glaucoma (POAG) occurs at the juxtacanalicular component of the trabecular meshwork and the endothelial lining of the inner wall of Schlemm’s canal [9–11]. A trabecular bypass stent bypasses the region of highest outflow resistance and creates a direct pathway between the aqueous and Schlemm’s canal. However, one study demonstrated that about one third of the outflow resistance occurs distal to Schlemm’s canal and therefore, bypassing the trabecular meshwork may not reduce the IOP enough for all glaucomatous eyes [12].
The first trabecular bypass stent was first described by Speigel and Kobuch [13], who implanted a silicone trabecular bypass tube shunt via an ab externo approach in six eyes, with a significant reduction in IOP and glaucoma medications from preoperative levels. The implant was successfully implanted in five out of six eyes. All eyes showed no loss of visual acuity and a reduction of IOP or glaucoma medication use. Two of these eyes developed low diffuse filtering blebs through this ab externo approach.
The Glaukos iStent® trabecular micro-bypass stent (Glaukos Corporation, Laguna Hills, California) also bypasses the trabecular meshwork by connecting the anterior chamber to Schlemm’s canal to enhance physiologic outflow, but through a titanium L-shaped stent and an ab interno approach. This device was approved by the FDA in June 2012 and is the first FDA-approved MIGS device to treat mild to moderate open angle glaucoma in conjunction with cataract surgery. Several clinical studies have been published since the first pilot study in 2007 [14], demonstrating the efficacy and safety of this device for treatment of mild to moderate glaucoma.
2.2 Anatomical Basis
2.2.1 First-Generation iStent
The iStent is a heparin-coated titanium single piece L-shaped device that measures 1.0 mm in length, 0.33 mm in high, and has a snorkel length of 0.25 mm. The snorkel diameter measures 120 μm. The iStent is the smallest medical device to be implanted in the human body and is nonferromagnetic. The canal portion is an open half-pipe body with the “closed” side lying against the inner wall of the canal and the “open” side against the outer wall where the collector channels reside. Three retention arches fixate the device to the inner wall of Schlemm’s canal. The “snorkel” sits in the anterior chamber and acts as a conduit for the aqueous to bypass the trabecular meshwork into Schlemm’s canal (Fig. 2.1a). The stent comes attached to the end of a disposable inserter and is sterilized by gamma irradiation. Should the stent become dislodged into the anterior chamber during implantation, the inserter is capable of recovering the device.

(a) First-generation iStent®. (b) Second-generation iStent inject®. Image Courtesy of Glaukos
The two models GTS100R and GTS100L are identical except the body faces opposite directions to assist with nasal stent placement. The GTS100R is designed for the right eye and GTS100L is designed for the left eye. The inferonasal quadrant is the preferred site for insertion as it is thought to be the area with the highest density of collector channels [15]. There are about 20–30 collector channels surrounding the globe that drain aqueous from Schlemm’s canal to aqueous and episcleral veins [16].
2.2.2 Second-Generation iStent Inject®
Glaukos has recently developed a second-generation trabecular bypass stent, the iStent inject® (GTS400), which is currently CE (Conformité Européenne) marked in Europe and is undergoing clinical trials in the United States (Fig. 2.1b). This device is also a single-piece, heparin-coated, titanium device. This device is smaller than the first-generation device, measuring 360 μm in length and the conical head measuring 230 μm in width. The conical head sits in Schlemm’s canal with four flow outlets, each measuring 50 μm in diameter. The trabecular meshwork holds the thinner thorax region and the flange contains an inlet orifice measuring 80 μm in diameter. Since this device is symmetrically designed, it can be used in either eye. The iStent inject is preloaded on the G2-M-IS injector which houses two stents, enabling insertion of two devices with one injector.
2.3 Indications
The iStent® trabecular micro-bypass stent is currently FDA approved to be used in conjunction with cataract surgery for the reduction of IOP in open angle glaucoma. Approximately 1 in 5 patients with a visually significant cataract is on at least one ocular hypotensive medication for glaucoma or ocular hypertension [17]. However, the appropriate patient should have mild to moderate glaucoma, demonstrating less than −12 dB MD on their visual field. A patient who has uncontrolled glaucoma, who is on three or more ocular hypotensive medications, or who requires very low IOPs (below episcleral venous pressure) would likely benefit from the more traditional combined phacoemulsification/trabeculectomy or tube shunt procedure, which provides better control for IOP in more advanced glaucoma.
FDA approval guidelines require that the iStent be implanted concurrently with phacoemulsification. There is often better visualization of the angle structures after the cataract is removed. Furthermore, cataract surgery alone has been shown in multiple studies to lower the IOP [18–20]. It is thought that the IOP lowers because there is a reversal of the compression of the ciliary body, Schlemm’s canal and trabecular meshwork complex after the enlarged cataractous lens is removed. The conventional wisdom is that the IOP lowers an average about 2–4 mmHg after cataract surgery [21]. Recent studies have shown IOP can lower as much as 8 mmHg especially when starting with a higher preoperative IOP [22]. By creating a bypass through the trabecular meshwork, the iStent can work in conjunction with cataract extraction to enhance the natural physiologic outflow system.
This device has been successfully implanted in eyes with POAG and secondary open angle glaucoma such as pseudoexfoliation and pigmentary glaucoma. Preoperative gonioscopy should rule out peripheral anterior synechiae (PAS), rubeosis, or other angle abnormalities that may make proper placement difficult. A more pigmented trabecular meshwork will also ease proper placement of the device, but is not necessary as identification of Schlemm’s canal can be seen with blood reflux into the episcleral venous system during periods of transient intraoperative hypotony. With experience, one can consider implanting the device in eyes with a slightly narrow angle that is expected subsequently to deepen after phacoemulsification.
2.4 Contraindications
This device is contraindicated in eyes with primary or secondary angle closure glaucoma, as access to the trabecular meshwork is restricted. This device is also contraindicated in patients with pathology that may cause increased episcleral venous pressure such as thyroid eye disease or Sturge–Weber Syndrome. In these cases, the cause of increased IOP is not secondary to resistance in the juxtacanalicular meshwork and so the iStent would not be expected improve IOP. Lastly, one should be cautious while implanting this device in patients with corneal haze or opacities due to limitations in visualization of the angle structures.
2.5 Surgical Procedure
-
1.
Preoperatively, one should carefully examine the angle gonioscopically to ensure that the angle structures, in particular the trabecular meshwork, are clearly visible. There should be no evidence of angle closure, rubeosis, angle recession, trauma, or other angle abnormalities that may make implantation of the iStent difficult.
-
2.
It is advisable to perform phacoemulsification in the standard technique through a temporal clear corneal incision or limbal approach. This will allow implantation of the iStent nasally.
-
3.
After implantation of the intraocular lens (IOL), if the pupil is extremely dilated, an intracameral miotic can be instilled.
-
4.
After irrigation/aspiration, the anterior chamber should be filled with additional cohesive viscoelastic to maintain the anterior chamber.
-
5.
Position the microscope for better gonioscopic viewing of the angle. Rotate the patient’s head 35° away from you and rotate the microscope 35° towards you. An intraoperative gonio prism is placed on the cornea to adequately view the trabecular meshwork. To ensure a clear view, a light touch is required to prevent striae induced from the gonio prism.
-
6.
The iStent can then be inserted through the same temporal incision for cataract surgery (use the GTS100R for the right eye and the GTS100L for the left eye).
-
7.
Traverse the anterior chamber with the inserter with the implant on the tip of the inserter.
-
8.
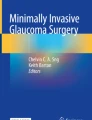
View the angle under high magnification and approach the upper third of the nasal TM at a 15° angle with the tip pointed inferiorly (Fig. 2.2). If it is difficult to visualize the trabecular meshwork, transient hypotony can help cause blood reflux into Schlemm’s canal for better visualization. Schlemm’s canal is located just posterior to the TM.
Fig. 2.2 
iStent® aimed 15° into the trabecular meshwork (TM) under high magnification. Blood reflux from Schlemm’s canal with hypotony can improve visualization of TM
-
9.
Engage the TM and advance the iStent into Schlemm’s canal. The device should be placed close to areas of heavier pigmentation as the collector channels are expected to be nearby. Proper placement into Schlemm’s canal typically demonstrates a small reflux of blood; however, this does not always occur even with proper placement.
-
10.
The device is released by pushing the button on the inserter. Tap the snorkel on the side to ensure it is placed securely.
-
11.
If there is resistance on insertion, one can try again a half clock hour more inferiorly.
-
12.
Irrigate the anterior chamber with irrigation/aspiration to remove all viscoelastic to achieve physiologic pressure at the end of surgery.
-
13.
Some surgeons prefer to perform phacoemulsification after implantation of the iStent device. The advantage to this is that there may be less corneal edema and one can use a smaller corneal incision, which may help with anterior chamber stability during implantation of the device. Furthermore, the extra viscoelastic needed to implant the iStent if performed after the cataract surgery is not necessary. However, the advantage of placing the iStent after phacoemulsification is that the angle will be deeper after the lens is removed, aiding visualization of angle structures.
-
14.
Routine postoperative management after phacoemulsification should be used after cataract surgery with iStent placement. If the patient was on only one preoperative ocular hypotensive drop, one can consider stopping this postoperatively and resume it if necessary. Some surgeons use loteprednol instead of prednisolone acetate postoperatively to avoid a steroid response.

2.6 Outcomes
2.6.1 First-Generation iStent Prospective Studies
Initial studies by Spiegel et al. [23,24] first demonstrated the successful implantation of the iStent with phacoemulsification. Their prospective noncomparative studies demonstrated an IOP reduction of 4.4 ± 4.5 mmHg after 12 months of follow-up, with 50 % of subjects achieving adequate IOP control off of medications (Table 2.1). Fea [25], was the first published double-masked randomized controlled trial comparing IOP reduction between phacoemulsification alone (control) and phacoemulsification combined with iStent implantation. After a washout of all postoperative medications at 15 months follow-up, the mean IOP difference was almost 2.5 mmHg between the two groups with the combined group having the lower mean IOP. Furthermore, after a 15-month follow-up, 67 % of the combined group no longer required glaucoma medications compared to only 24 % in the control group, demonstrating that the iStent is an effective way to reduce the medication burden in patients with concomitant cataracts with mild to moderate glaucoma.
Samuelson et al. [26] reported on the largest multicenter randomized controlled trial to date, which demonstrated a significant IOP and medication reduction in the combined group (phacoemulsification + iStent) compared to the control group (phacoemulsification alone). This study included 240 eyes with IOP controlled on 1–3 medications preoperatively, with 111 eyes receiving the iStent. At all times points up to 2 years, there was a higher proportion of subjects in the combined group who achieved both the primary and secondary end points. The primary end point was an IOP ≤ 21 mmHg without medications and the secondary end point with an IOP reduction ≥20 % without medications at 1-year follow-up. Those in the control group (phacoemulsification only) had a substantially higher level of glaucoma medication use and restarted medications sooner postoperatively compared to the group that had the iStent implanted. Using the same study group, Craven et al. [27] showed that IOP was stable in the iStent group for a longer follow-up duration, between 12 and 24 months of follow-up. Mean IOP and medication use was still lower in the combined iStent and cataract extraction group compared to cataract extraction alone after 24 months of follow-up (p = 0.36).
Most importantly, the safety profile was excellent in the combined group in this large cohort of patients. The most frequent adverse events occurred with similar frequencies in both groups. The only stent-related adverse events were stent obstruction (iris, fibrin, blood, etc.), which occurred in 4 % of eyes, and stent malposition which occurred in 3 % of eyes. Three of the malpositioned stents were repositioned and one was removed and replaced. Levels of iritis were similar between both groups. These stent-related events occurred early in the postoperative course and were much less serious compared to the complications that can occur with more traditional surgeries such as trabeculectomies and tube shunt implantation. The only severe adverse event was deemed not related to the ophthalmic surgery, in which one patient experienced a stroke and retinal ischemia from carotid artery stenosis. In another prospective study with a longer mean follow-up of 54 months, there were no late-onset complications, such as endophthalmitis or tube shunt exposure, which can occur with more traditional incisional glaucoma procedures [28].
2.6.2 Implantation of Multiple Stents and the iStent Inject®
All the initial studies with the iStent used one device only for a moderate but significant IOP reduction in conjunction with phacoemulsification. Recent studies have investigated the efficacy and safety of multiple iStent implantations. Investigation into the efficacy of multiple stent placement began with in vitro studies with cultured anterior segments from normal human eyes obtained at autopsy [35]. This study demonstrated that although one stent produces the greatest IOP reduction, additional stents may further lower IOP.
In a clinical study, Belovay et al. [30] demonstrated that implantation of two or three iStents with phacoemulsification results in a significant reduction in IOP and medication use. Furthermore, the three-stent group was on significantly fewer postoperative glaucoma medications than the two-stent group. In a comparative study between implantation of two stents with cataract surgery to cataract surgery alone, the combined group with two stents demonstrated increased trabecular outflow facility and a reduction in IOP and medications at 1-year follow-up compared to the cataract only group [29]. This study deduced an increase in outflow facility of 157 % after 1 year of follow-up through two stents alone.
Recently, a few studies have been published describing the implantation of the iStent without concurrent phacoemulsification. Ahmed et al. [31] recently demonstrated that IOP is reduced from 25.3 ± 1.8 mmHg to 17.1 ± 2.2 mmHg at 13 months postoperatively with two iStent implantation after washout. At 12 months, 100 % of patients had achieved an IOP reduction of 20 % or more, an IOP of 18 mmHg or less, and a reduction of one glaucoma medication. Phacoemulsification was not performed during these surgeries. There were no intraoperative adverse events with multiple stent placements. The most common postoperative event was a progression of cataract over the 18-month period, which occurred in 4 out of 39 eyes. This study demonstrates that implantation of multiple stents even without phacoemulsification is safe and will lower IOP significantly with a reduction in medications.
Lastly, a few preliminary studies regarding the efficacy and safety of the iStent inject® have recently been published [32–34] (Table 1.1). This device is currently CE marked in Europe. All three studies demonstrated a favorable safety profile. Fea et al. [33] demonstrated a mean IOP decrease of 8.1 ± 2.6 mmHg after 12 months of follow-up and Voskanyan et al. [34] demonstrated a similar IOP reduction of 10.4 ± 3.2 mmHg. These recent studies show promise that the second-generation iStent may have the ability to reduce IOP and medication use even further.
2.6.3 The ICE Procedure
There has also been a recent interest in the triple procedure called ICE, which stands for iStent, cataract extraction, and endocyclophotocoagulation. Endoscopic cyclophotocoagulation (ECP) has been used to reduce IOP in conjunction with phacoemulsification [36]. ECP ablates the ciliary body, thereby decreasing aqueous production and reducing IOP. In the “ICE” procedure, ECP decreases “inflow” and iStent implantation increases “outflow,” thereby targeting two methods of IOP reduction. In a retrospective noncomparative series of 24 eyes that underwent the “ICE” procedure, Radcliffe et al. [37] demonstrated a reduction of IOP from 19.1 ± 6.3 mmHg to 15.5 ± 3.9 mmHg with a reduction in glaucoma medications. No adverse events or hypotony occurred. Further prospective studies are warranted to investigate the efficacy and safety of this combined procedure.
2.7 Conclusion
With the advent of MIGS procedures, there is hope for a new set of glaucoma surgical procedures that can effectively control IOP in a safe manner and reduce the medication burden in those with mild to moderate glaucoma. The iStent trabecular micro-bypass stent has demonstrated in several prospective randomized controlled trials to reduce IOP and glaucoma medications in conjunction with cataract surgery for those with mild to moderate open angle glaucoma. Further studies are needed on the second-generation iStent, iStent implantation without phacoemulsification, and iStent placement with other MIGS procedures. Overall, this is an exciting time for the field of glaucoma with the myriad of tools and procedures we have available to battle this progressive and potentially blinding disease.
References
Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC, Group TVTS. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–14. doi:10.1016/j.ajo.2011.10.024.
DeBry PW, Perkins TW, Heatley G, Kaufman P, Brumback LC. Incidence of late-onset bleb-related complications following trabeculectomy with mitomycin. Arch Ophthalmol. 2002;120(3):297–300.
McIlraith I, Strasfeld M, Colev G, Hutnik CML. Selective laser trabeculoplasty as initial and adjunctive treatment for open-angle glaucoma. J Glaucoma. 2006;15(2):124–30.
Anwar Z, Wellik SR, Galor A. Glaucoma therapy and ocular surface disease: current literature and recommendations. Curr Opin Ophthalmol. 2013;24(2):136–43. doi:10.1097/ICU.0b013e32835c8aba.
Tsai JC. A comprehensive perspective on patient adherence to topical glaucoma therapy. Ophthalmology. 2009;116(11 Suppl):S30–6. doi:10.1016/j.ophtha.2009.06.024.
Wong MO, Lee JW, Choy BN, Chan JC, Lai JS. Systematic review and meta-analysis on the efficacy of selective laser trabeculoplasty in open-angle glaucoma. Surv Ophthalmol. 2015;60(1):36–50. doi:10.1016/j.survophthal.2014.06.006.
Realini T. Selective laser trabeculoplasty: a review. J Glaucoma. 2008;17(6):497–502. doi:10.1097/IJG.0b013e31817d2386.
Saheb H, Ahmed IIK. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96–104. doi:10.1097/ICU.0b013e32834ff1e7.
Grant W. Experimental aqueous perfusion in enucleated human eyes. Arch Ophthalmol. 1963;69:783–801.
Rosenquist R, Epstein D, Melamed S, Johnson M, Grant WM. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr Eye Res. 1989;8(12):1233–40.
Johnson MC, Kamm RD. The role of Schlemm’s canal in aqueous outflow from the human eye. Invest Ophthalmol Vis Sci. 1983;24(3):320–5.
Schuman JS, Chang W, Wang N, de Kater AW, Allingham RR. Excimer laser effects on outflow facility and outflow pathway morphology. Invest Ophthalmol Visual Sci. 1999;40(8):1676–80.
Spiegel D, Kobuch K. Trabecular meshwork bypass tube shunt: initial case series. Br J Ophthalmol. 2002;86(11):1228–31.
Spiegel D, Wetzel W, Haffner DS, Hill RA. Initial clinical experience with the trabecular micro-bypass stent in patients with glaucoma. Adv Ther. 2007;24(1):161–70.
Ascher K. The aqueous veins, American lecture series, no. 403. Springfield, IL: Charles C. Thomas; 1961.
Dvorak-Theobald G. Schlemm’s canal: its anastomoses and anatomic relations. Trans Am Ophthalmol Soc. 1934;32:574–95.
2002–2007 Medicare Standard Analytical File. Centers for Medicare and Medicaid Services, US Dept of Health and Human Services; 2007.
Tennen DG, Masket S. Short-and long-term effect of clear corneal incisions on intraocular pressure. J Cataract Refract Surg. 1996;22(5):568–70.
Shingleton BJ, Pasternack JJ, Hung JW, O’Donoghue MW. Three and five year changes in intraocular pressures after clear corneal phacoemulsification in open angle glaucoma patients, glaucoma suspects, and normal patients. J Glaucoma. 2006;15(6):494–8. doi:10.1097/01.ijg.0000212294.31411.92.
Kim DD, Doyle JW, Smith MF. Intraocular pressure reduction following phacoemulsification cataract extraction with posterior chamber lens implantation in glaucoma patients. Ophthalmic Surg Lasers. 1999;30(1):37–40.
Friedman DS, Jampel HD, Lubomski LH, Kempen JH, Quigley H, Congdon N, Levkovitch-Verbin H, Robinson KA, Bass EB. Surgical strategies for coexisting glaucoma and cataract: an evidence-based update. Ophthalmology. 2002;109(10):1902–13.
Poley BJ, Lindstrom RL, Samuelson TW, Schulze R. Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg. 2009;35(11):1946–55. doi:10.1016/j.jcrs.2009.05.061.
Spiegel D, García-Feijoó J, García-Sánchez J, Lamielle H. Coexistent primary open-angle glaucoma and cataract: preliminary analysis of treatment by cataract surgery and the iStent trabecular micro-bypass stent. Adv Ther. 2008;25(5):453–64. doi:10.1007/s12325-008-0062-6.
Spiegel D, Wetzel W, Neuhann T, Stuermer J, Hoeh H, Garcia-Feijoo J, Martinez-De-La-Casa JM, Garcia-Sanchez J. Coexistent primary open-angle glaucoma and cataract: interim analysis of a trabecular micro-bypass stent and concurrent cataract surgery. Eur J Ophthalmol. 2009;19(3):393–9.
Fea AM. Phacoemulsification versus phacoemulsification with micro-bypass stent implantation in primary open-angle glaucoma: randomized double-masked clinical trial. J Cataract Refract Surg. 2010;36(3):407–12. doi:10.1016/j.jcrs.2009.10.031.
Samuelson TW, Katz LJ, Wells JM, Duh Y-J, Giamporcaro JE, Group UiS. Randomized evaluation of the trabecular micro-bypass stent with phacoemulsification in patients with glaucoma and cataract. Ophthalmology. 2011;118(3):459–67. doi:10.1016/j.ophtha.2010.07.007.
Craven ER, Katz LJ, Wells JM, Giamporcaro JE, Group iS. Cataract surgery with trabecular micro-bypass stent implantation in patients with mild-to-moderate open-angle glaucoma and cataract: two-year follow-up. J Cataract Refract Surg. 2012;38(8):1339–45. doi:10.1016/j.jcrs.2012.03.025.
Arriola-Villalobos P, Martínez-de-la-Casa JM, Díaz-Valle D, Fernández-Pérez C, García-Sánchez J, García-Feijoó J. Combined iStent trabecular micro-bypass stent implantation and phacoemulsification for coexistent open-angle glaucoma and cataract: a long-term study. Br J Ophthalmol. 2012;96(5):645–9. doi:10.1136/bjophthalmol-2011-300218.
Fernández-Barrientos Y, García-Feijoó J, Martínez-de-la-Casa JM, Pablo LE, Fernández-Pérez C, García Sánchez J. Fluorophotometric study of the effect of the glaukos trabecular microbypass stent on aqueous humor dynamics. Invest Ophthalmol Vis Sci. 2010;51(7):3327–32. doi:10.1167/iovs. 09-3972.
Belovay GW, Naqi A, Chan BJ, Rateb M, Ahmed IIK. Using multiple trabecular micro-bypass stents in cataract patients to treat open-angle glaucoma. J Cataract Refract Surg. 2012;38(11):1911–7. doi:10.1016/j.jcrs.2012.07.017.
Ahmed IIK, Katz LJ, Chang DF, Donnenfeld ED, Solomon KD, Voskanyan L, Samuelson TW. Prospective evaluation of microinvasive glaucoma surgery with trabecular microbypass stents and prostaglandin in open-angle glaucoma. J Cataract Refract Surg. 2014;40(8):1295–300. doi:10.1016/j.jcrs.2014.07.004.
Arriola-Villalobos P, Martínez-de-la-Casa JM, Díaz-Valle D, García-Vidal SE, Fernández-Pérez C, García-Sánchez J, García-Feijoó J. Mid-term evaluation of the new Glaukos iStent with phacoemulsification in coexistent open-angle glaucoma or ocular hypertension and cataract. Br J Ophthalmol. 2013;97(10):1250–5. doi:10.1136/bjophthalmol-2012-302394.
Fea AM, Belda JI, Rękas M, Jünemann A, Chang L, Pablo L, Voskanyan L, Katz LJ. Prospective unmasked randomized evaluation of the iStent inject (®) versus two ocular hypotensive agents in patients with primary open-angle glaucoma. Clin Ophthalmol. 2014;8:875–82. doi:10.2147/opth.s59932.
Voskanyan L, García-Feijoó J, Belda JI, Fea A, Jünemann A, Baudouin C, Group SS. Prospective, unmasked evaluation of the iStent® inject system for open-angle glaucoma: synergy trial. Adv Ther. 2014;31(2):189–201. doi:10.1007/s12325-014-0095-y.
Bahler CK, Smedley GT, Zhou J, Johnson DH. Trabecular bypass stents decrease intraocular pressure in cultured human anterior segments. Am J Ophthalmol. 2004;138(6):988–94. doi:10.1016/j.ajo.2004.07.035.
Kahook MY, Lathrop KL, Noecker RJ. One-site versus two-site endoscopic cyclophotocoagulation. J Glaucoma. 2007;16(6):527–30. doi:10.1097/IJG.0b013e3180575215.
Radcliffe NM, Parekh PD, Noecker RJ, Sarkisian S, Chapman KO (2014) ICE surgical technique outcomes: MIGS implantation of trabecular bypass stent, cataract extraction, and endoscopic cyclophotocoagulation. Paper presented at the 2014 American Glaucoma Society Annual Meeting, Washington, DC.
Acknowledgements
Conflicts of Interest: Wanda D. Hu declares that she has no conflict of interest. Marlene R. Moster is a consultant for Glaukos.
Animal Studies: No animal or human studies were carried out by the authors for this article.
Informed Consent: Informed consent was not applicable for this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Hu, W.D., Moster, M.R. (2015). Trabecular Micro-Bypass Stent for the Treatment of Coexistent Cataract and Mild Open-Angle Glaucomas. In: Aref, A., Varma, R. (eds) Advanced Glaucoma Surgery. Essentials in Ophthalmology. Springer, Cham. https://doi.org/10.1007/978-3-319-18060-1_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-18060-1_2
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18059-5
Online ISBN: 978-3-319-18060-1
eBook Packages: MedicineMedicine (R0)