
Abstract
Although the long-term outcomes of total hip arthroplasty continue to improve, their survival in adolescent patients still remains a serious concern. In adolescent patients with severe degenerative joint disease of the hip, it can be argued that hip fusion is still the preferred treatment option. Short-term problems with hip fusion include nonunion, malalignment, and limb length discrepancy. Long-term problems include degenerative low back pain and ipsilateral knee pain as well as a difficult conversion to total hip arthroplasty. While the short-term problems can be minimized using the approach described below, the long-term problems of adjacent segment degenerative joint disease cannot and may in fact necessitate future conversion to total hip arthroplasty. Avoiding the use of complex plating techniques and minimizing trauma to the abductor musculature during hip arthrodesis are important factors to consider for future total hip arthroplasty.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Brief Clinical History
This adolescent male was first seen at age 13 years and 3 months for a history of worsening right hip pain. The hip pain started insidiously 2–3 years earlier and had been progressively worsening to the point where he had a constant limp and decreased ability to participate in sports. His hip pain was located in the groin. He had start-up pain in the groin and developed lateral hip pain over the course of the day with activities. There was no history of antecedent hip problems. Gait assessment revealed an abductor lurch as well as a 1.5 cm LLD. He had a positive Trendelenburg sign and had virtually no abduction/adduction or internal/external rotation. He had 90° of hip flexion and a minimal hip flexion contracture. Radiographs revealed Tonnis grade-3 osteoarthritis of the right hip with an LLD of 1.5 cm. A discussion regarding possible treatment options including hip fusion and total hip replacement was undertaken, and he was sent for a rheumatologic, hematologic, and infectious workup which all came back negative. He returned to the clinic 4 months later with a further decline in function and had stopped participating in all activities due to increasing pain. He was managing to ambulate without an assistive device; however, his limp had worsened quite markedly and he was prescribed a cane at that visit. A further discussion regarding treatment was undertaken and he was booked for a hip fusion by surgical hip dislocation, internal fixation, offloading subtrochanteric osteotomy, and iliofemoral external fixation . In addition, he was booked for growth modulation of the opposite limb to ensure that the LLD was minimized.
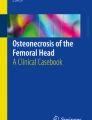
2 Preoperative Clinical Photos and Radiographs
See Fig. 1.

(a) Anteroposterior pelvis radiograph reveals severe osteoarthritis with lateral subluxation. (b) Anteroposterior lower extremity image performed with a 2 cm left under the right foot demonstrates a 1.5 cm limb length discrepancy secondary to joint collapse. (c) A coronal plane computed tomography cut of the pelvis shows severe joint space loss with subchondral cysts within the acetabulum and femoral head
3 Preoperative Problem List
-
Hip OA of unknown origin in an adolescent patient
-
LLD 1.5 cm
4 Treatment Strategy
The treatment strategy entails obtaining an adequate fusion of the hip with the leg in a functional position with minimal disruption of the abductor mechanism. In order to achieve an optimal surface preparation for the fusion, the surgical hip dislocation approach (Ganz et al. 2001) is chosen as it gives excellent exposure of the femoral head and acetabulum. Furthermore, this approach is abductor sparing. Rigid compressive fixation is achieved with partially threaded 7.3 mm cannulated screws without the need for complex plating techniques that can further compromise the abductor mechanism either during the initial surgery or at the time of conversion to a total hip. An offloading osteotomy is performed to decrease the lever arm and moment on the hip fusion fixation and thus allow for an adequate fusion and minimize the risk of nonunion (Benaroch et al. 1996). An iliofemoral fixator is applied to stabilize the osteotomy. The external fixator consists of a hinge at the offloading osteotomy site and a rail to allow for realignment and lengthening if desired.
5 Basic Principles
-
Surface preparation
-
Alignment
-
Rigid compressive fixation
-
Offloading osteotomy
6 Images During Treatment

(a) Intraoperative photograph of the femoral head exposed by a surgical hip dislocation reveals a completely destroyed femoral head prior to preparing the femoral head (b) using humeral head resurfacers to obtain a spherical cancellous surface for fusion

(a) Anteroposterior radiograph of the pelvis done immediately postoperatively demonstrates the transarticular fixation screws, trochanteric fixation, low-energy oblique subtrochanteric osteotomy, and iliofemoral external fixation. During the subtrochanteric osteotomy, a fracture line was noted to propagate distally, ending just before the femoral fixation pin. (b) Anteroposterior lower extremity image reveals adequate lower limb alignment in the coronal plane and the placement of growth modulation at the contralateral knee to limit the limb length discrepancy
7 Technical Pearls
The keys to a good outcome after a hip fusion are obtaining union, ensuring adequate alignment of the leg, and minimizing an LLD to <2 cm. The procedure is performed in the lateral decubitus position. The surgical hip dislocation technique is used as it gives excellent access to the femoral head and acetabulum without compromising the abductors. The use of acetabular reamers for the acetabulum and humeral head resurfacing reamers for the femoral head enables an excellent surface preparation. The acetabulum is lightly reamed starting with a small reamer gradually increasing the size until there is punctate bleeding throughout. The femoral head is reamed starting with a large-diameter reamer gradually decreasing to 2 mm less than the acetabulum. The femoral head reamings are used as bone graft. At this stage, the leg is positioned in 20–30° of hip flexion, 5° of adduction, and 5–10° of external rotation. The leg must stay in this position until the external fixator is on; therefore, sponge blocks are used to maintain this position. The hip is then transfixed with a short threaded 7.3 mm cannulated screw to obtain compression and then a long threaded 7.3 mm cannulated screw to add further rigidity to the fixation. The hip capsule is closed and the trochanter is transfixed back to its original position. An iliofemoral external fixator is then assembled with a ball hinge placed at the location of the offloading subtrochanteric osteotomy which is performed in an oblique fashion to maximize the surface area for bone healing. Once the wounds have been closed and the dressings have been placed, the patient is repositioned in the supine position and the position of the limb is reassessed. If required, repositioning of the limb can be performed through the subtrochanteric osteotomy. At about 10 days postoperatively, the patient is assessed by an occupational therapist and a physiotherapist to help decide on whether or not the hip fusion position is adequate. At this point, if required, further adjustments can be made through the osteotomy site in regard to flexion/adduction/rotation. In addition if there is a limb length discrepancy greater than 1.5–2 cm, limb lengthening can be done through the subtrochanteric osteotomy. The patient is kept non-weight bearing. A CT scan is performed at 3 months to assess both the hip fusion and the subtrochanteric osteotomy. If there is minimal healing on the CT scan, the scan is repeated in 4–6 weeks. Weight bearing is started once the scan shows evidence of bony union, and the frame is removed in 4–6 weeks.
8 Outcome Clinical Photos and Radiographs
See Fig. 4.

(a) Anteroposterior left hip radiograph reveals a robust arthrodesis of the hip . (b) Anteroposterior lower extremity image reveals the final alignment in the healed position. Growth modulation at the knee resulted in a mild varus alignment of the contralateral knee. In retrospect, a bony epiphysiodesis should have been performed. At 6 months postoperatively, the limb discrepancy measured 1.5 cm and the patient reported no pain. Gait assessment revealed a mild asymmetry. By 12 months, he had returned to all sports activities and was playing on his high school basketball team
9 Avoiding and Managing Problems
The main problem postoperatively is drift of the osteotomy alignment at the ball hinge. In order to avoid this, the ball hinge can be cemented; however, this precludes any future realignment. Another approach is to monitor the alignment on a weekly basis and adjust it in the clinic as necessary during the first 6 weeks of treatment. Typically, the distal fragment will drift toward adduction and extension, both of which can be corrected through the ball hinge. In addition, pillows should be kept under the leg whenever the patient is in the supine position, to decrease the tendency toward extension.
References and Suggested Reading
Benaroch TE, Richards BS, Haideri N, Smith C (1996) Intermediate follow-up of a simple method of hip arthrodesis in adolescent patients. J Pediatr Orthop 16(1):30–36
Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U (2001) Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 83(8):1119–1124
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this entry
Cite this entry
Saran, N. (2015). Case 109: Hip Fusion with an External Fixator. In: Rozbruch, S., Hamdy, R. (eds) Limb Lengthening and Reconstruction Surgery Case Atlas. Springer, Cham. https://doi.org/10.1007/978-3-319-18023-6_343
Download citation
DOI: https://doi.org/10.1007/978-3-319-18023-6_343
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18022-9
Online ISBN: 978-3-319-18023-6
eBook Packages: MedicineReference Module Medicine