
Abstract
The medical use of cardiac glycosides began in 1785 with the publication of Withering’s monograph on the therapeutic efficacy and toxicity of the leaves of the common foxglove plant,. Various glycosides including digitoxin and ouabain were then extracted from plants, and digitalis glycosides have been widely prescribed for more than 230 years.
Access provided by CONRICYT-eBooks. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Digitalis glycosides
- Cardiac glycosides
- Digitalis purpurea
- Digitoxin
- Ouabain
- Digitalis poisoning
- Oleander
- Convallaria majalis
- Lily of the valley
- Convallarin
- Convallamarin
- Convallatoxin
- Bufo toad
- Magnesium
- Anti-digoxin-specific Fab fragments
The medical use of cardiac glycosides began in 1785 with the publication of Withering’s monograph on the therapeutic efficacy and toxicity of the leaves of the common foxglove plant, Digitalis purpurea . Various glycosides including digitoxin and ouabain were then extracted from plants, and digitalis glycosides have been widely prescribed for more than 230 years.
Digitalis still remains an important and useful therapy for patients with heart failure and/or atrial fibrillation [1]. However, despite a pertinent contribution of their pharmacological properties combining positive inotropic and negative chronotropic effects to reduce symptoms and hospital admissions in heart failure patients, meta-analyses showed neutral effect on all-cause mortality and robust trial data are lacking in patients with atrial fibrillation [2, 3]. Following the availability of therapies providing proved prognostic benefits in these patients including angiotensin-converting enzyme inhibitors, beta-blockers, aldosterone antagonists, and cardiac resynchronization therapy, prescription rates of digoxin have fallen substantially [4]. Their use is now restricted to the treatment of heart failure due to reduced ejection fraction with or without supraventricular dysrhythmias including atrial fibrillation.
Digitalis poisoning may result from either acute suicidal massive ingestion or more frequently from chronic toxicity in patients with cardiac diseases and renal failure. Digitalis overdose may lead to life-threatening toxicity. In 1976, Smith and colleagues reported the first case of human digoxin poisoning treated with anti-digoxin-specific Fab fragments , unveiling the modern era of treatment of cardiac glycoside toxicity [5].
Biochemistry of Digitalis Glycosides
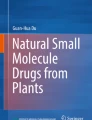
Cardiac glycosides of therapeutic interest share a common steroid nucleus structure with one or more glycosidic residues bound at its C3 (Fig. 1). Their potent and selective properties to inhibit the membrane Na+/K+-ATPase are due to the β-hydroxyl group at its C14 and the unsaturated lactone at its C17. Removal of the glycoside moieties (forming the genin or aglycone part) only minimally affects their pharmacological properties. The absence of a hydroxyl group at the C12 of the nucleus distinguishes digitoxin from digoxin. In addition to foxglove (Digitalis), other cardiac glycosides are divided in two subclasses, the cardenolides and the bufadienolides [6]. Cardenolides are present in Antiaris toxicaria (antiarin), Nerium oleander called common oleander (oleandrin, folineriin, adynerin, digitoxigenin), Thevetia peruviana called yellow oleander (thevetin A and B, peruvoside, neriifolin, thevotoxin, ruvoside, and theridoside), Cerbera odollam called sea mango (cerberin), Convallaria majalis called lily of the valley (convallarin , convallamarin, and convallatoxin ), and Strophanthus sp. (ouabain). Bufadienolides are present in Urginea maritima called red squill (scilliroside and proscillaridin A, scillarene A, scilliglaucoside, and scilliphaeoside) and Rhinella marina called cane toad (bufalin, manrinobufagenin, and telocinobufagin). An ouabain-like compound (resibufogenin) is also found in the skin of the bufo toad (Bufo spp.). Neriifolin, cerberin, and cerberigenin, contained in the fruit kernel of the red-eye-sea mango tree Cerbera manghas L. on which the coconut crab Birgus latro L. feeds, are the toxic agents leading to cardenolide poisoning when eating this kind of crab.

Chemical structure of digoxin. Digitoxin lacks a hydroxyl group on the C ring, resulting in greater lipophilicity
Pharmacology and Mechanisms of Toxicity
Digitalis reversibly inhibits the membrane-bound alpha subunits of the Na+/K+-ATPase pump in cardiac, smooth, and skeletal muscles and lungs and kidneys [1, 7, 8]. By increasing the intracellular sodium concentration in cardiomyocytes, digitalis promotes activity of the Na+/Ca2+-exchanger, thus enhancing the intracellular calcium concentration which is taken up by the sarcoplasmic reticulum. This action directly results in the greater interaction between the myocardial contractile proteins, increasing the force of cell contraction and improving the left ventricular systolic function. Consistently, the intravenous digitalis administration results in the immediate evidence of significant increase in stroke index, cardiac output, left ventricular ejection fraction, exercise tolerance, and decrease in pulmonary capillary wedge pressure [9]. Within the central nervous system, digitalis-mediated Na+/K+-ATPase also reduces the heart rate, by exerting a parasympathomimetic action on the sinoatrial and atrioventricular nodes, slowing their conduction and increasing the refractory period. Additionally, digitalis is responsible for vagal activation shifting the autonomic balance toward parasympathetic dominance. By reducing plasma norepinephrine, digoxin modulates the initially compensatory but finally detrimental neurohormonal activation observed in heart failure patients. This direct anti-sympathetic activity likely reflects the attenuation and sensitization of the augmented baroreflex in heart failure patients with raised filling pressures. Taken together, the pharmacological ability of digitalis to simultaneously increase cardiac inotropy and constrain cardiac chronotropy is unique. Digitalis increases vagal tone and decreases sympathetic activity. The plasma concentration and type of digitalis clearly determine which mechanism predominates. These mechanisms of action are common to all cardiac glycosides , although largely described using digoxin and ouabain ; however, differences exist among the glycosides and influence the toxicity and the therapeutic response. Consistently, insulin reverses the effects of digoxin but not ouabain on Na+/K+-ATPase due to their binding to different sites. Similarly, pharmacokinetics highly varies according to the digitalis molecule (Table 1).
In overdose, digitalis-related Na+/K+-ATPase inhibition may result in excessive intracellular Ca2+ increase resulting in a transient late depolarization (delayed afterdepolarization) accompanied by aftercontraction. Additionally, the increase in sympathetic activity accompanied by nonuniform increase in automaticity and vagal nerve-mediated depression of conduction in His-Purkinje and ventricular myocytes may cause life-threatening dysrhythmias.
Clinical Presentation and Life-Threatening Complications
Poisonings mainly result from pharmaceutical preparations of digitalis and more rarely from self-made preparations of cardiac glycoside-containing plants. Acute digitalis poisoning may result from accidental or suicidal exposure to a single elevated dose. Due to its narrow therapeutic index, chronic toxicity of digitalis has been reported in 6–23% of treated patients, particularly in the elderly [10, 11]. Several factors may alter patient’s sensitivity to digitalis including acute renal impairment and drug-drug interactions (Table 2) [10–17]. Macrolides, quinidine, verapamil, diltiazem, amiodarone, and others increase digoxin concentrations, mainly by competitions on their binding sites in tissues with a risk of digitalis toxicity.
Clinical and ECG Features
In the setting of acute poisoning, symptoms generally occur within 6 h of ingestion, but life-threatening symptoms may occur with delay, reflecting the relatively slow tissue distribution of digitalis. The noncardiac manifestations of digitalis toxicity are highly prevalent including gastrointestinal symptoms (anorexia, nausea, vomiting, abdominal pain, and diarrhea), neurological symptoms (fatigue, weakness, hallucinations, delirium, and psychiatric disorders), and visual manifestations (scotoma, blurred vision, color aberration, and blindness). Mesenteric ischemia has been reported rarely. Physician should suspect digitalis toxicity and measure serum digoxin concentration in the onset of unexplained gastrointestinal, neurological, or visual manifestation in a digitalis-treated patient.
Digitalis-related cardiac toxicity results from the combination of conduction and rhythm disturbances [6]. Toxicity should be suspected when there is evidence of increased automaticity and depressed atrioventricular conduction. Flattening or inversion of the T wave and depression of the ST segment related to long-term digitalis treatment should not be considered as toxicity criteria. The most common cardiac abnormality induced by digitalis is sinus bradycardia. Characteristic electrocardiogram (ECG) changes in the setting of digitalis overdose show dysrhythmias like atrial tachycardia, accelerated junctional rhythms, and fascicular tachycardia, as well as conduction disturbances like premature contractions of junctional or ventricular origin, sinoatrial block, and all degrees of atrioventricular blocks. In the chronic poisoning, the combination of atrial fibrillation and conduction disturbances is commonly observed resulting in irregular bradycardia. Onset of junctional tachycardia is highly suggestive too. Sinus arrest or exit block may occur. Ventricular ectopics and tachycardias are also reported and may be related to the underlying cardiac disease. Life-threatening arrhythmias primarily consist of third-degree atrioventricular block, ventricular tachycardia, and ventricular fibrillation. The contribution of the underlying cardiac disease including cardiomyopathy and coronary artery disease to digitalis toxicity is not clear [12].
When digitalis toxicity is suspected, kalemia and renal function should be urgently measured. Other electrolyte abnormalities should be interpreted in the onset of chronic digitalis poisoning according to concomitant conditions and medications.
Fatality and Prognosticators
Digitalis poisoning -attributed mortality rate ranged from 4.6% to 41% before the availability of anti-digoxin Fab fragments [18, 19] but remained between 6% and 29% after their availability [12, 15, 21]. Poor prognostic factors in acute digitalis poisoning were determined based on series of acute digitoxin poisoning and include age older than 55 years, male sex, hyperkalemia, and any degree of atrioventricular block (Table 3) [20]. Fatality rate significantly increases when serum potassium concentration is >4.5 mmol/L in the absence of adequate treatment. Ventricular dysrhythmias refractory to electrical cardioversion are the leading cause of death (70%), followed by advanced atrioventricular block resulting in asystolic arrest (20%) and cardiac insufficiency causing multi-organ failure (10%). Rarely, death may result from mesenteric infarction.
Diagnosis
Diagnosis depends on whether digitalis poisoning is chronic or acute. Acute poisoning is typically straightforward. QT interval modifications are of diagnostic value only in patients not previously treated with digitalis. Diagnosis is confirmed by the measurement of the serum digitalis concentration. By contrast, in chronic poisoning, diagnosis is more difficult because noncardiac symptoms are nonspecific and some ECG abnormalities look like those related to the underlying cardiac disease. Thus, serum determination of digitalis concentration is the key step to assess the diagnosis and should be largely prescribed in cases of suspected digitalis intoxication, although digoxin toxicity occurs to date less frequently than historically reported.
The range of therapeutic (steady-state) concentrations of digoxin and digitoxin are 0.5–2.0 ng/mL (0.6–2.6 nmol/L) and 10–30 ng/mL (13–39 nmol/L), respectively. According to the various factors that may influence digitalis toxicity, no single serum concentration can definitively establish the presence or absence of toxicity [12]. Of 3434 serum digoxin concentrations assayed in 2009 patients, 320 (9.3%) were higher than the upper limit of the therapeutic range, but only 83 of the 138 patients evaluable for digoxin toxicity had clinical evidence of toxicity for an overall incidence of 4.1% [22]. In another retrospective study reporting 6133 digoxin concentrations measured in 5100 patients, only 13 among the 460 patients with serum digoxin concentration >2 ng/mL (>2.6 nmol/L) were diagnosed as digoxin overdose before obtaining the laboratory results [23]. Hospitalized patients with serum digoxin > 2.1 ng/mL (>2.7 nmol/L) spent a mean of 12.1 ± 17.1 days in hospital. The mean time to death for the patients who died was 5 ± 3.1 days. Two thirds of the patients who died in the hospital had increasing digoxin levels before death. In this study, renal failure was not significantly associated with increased mortality while serum digoxin concentration was. Mortality rate in patients with elevated digoxin concentrations and preexisting ECG abnormalities was 8% compared with 40% in patients with elevated digoxin concentrations and new ECG abnormalities [23]. A fatality rate of 50% was reported in patients with digoxin concentrations > 6 ng/mL (7.7 mmol/L).
Serum potassium concentration significantly influences the toxicity associated with a given digitalis concentration [24]. In contrast to acute poisoning, most of the more serious arrhythmias found in patients with chronic toxicity are associated with serum potassium concentrations < 3.7 mmol/L [25]. An indication for transient pacemaker placement was present more frequently when digitalis intoxication was accompanied by hypokalemia (72%) than normokalemia (37%). In patients with digitalis intoxication-related dysrhythmias, normokalemic patients had a mean serum digoxin concentration of 6.68 ± 0.17 ng/mL (8.55 ± 0.22 mmol/L), whereas hypokalemic patients had a mean serum digoxin level of 1.13 ± 0.04 ng/mL (1.45 ± 0.05 mmol/L). Repletion of serum potassium sometimes corrected the dysrhythmia without significant changes in serum digoxin concentration. Hypomagnesemia likewise increases digitalis-related toxicity and may be a more frequent contributor to digoxin toxicity than hypokalemia [25]. Finally, prompt termination of the arrhythmias when stopping the drug administration or after infusing anti-digoxin-specific Fab fragments supports the diagnosis of chronic toxicity.
Management
Most cases of chronic toxicity are minor, and the patient may only require temporary withdrawal or reduction in his digitalis dosage on an outpatient or inpatient basis. However, more aggressive hospital treatment is sometimes mandatory to reduce the risk of death.
Gastrointestinal Decontamination
A single dose of activated charcoal (50 g) should be administered to all patients with acute ingestion of a potentially toxic exposure if ingestion occurred less than 2 h before. Although no clinical trial confirmed its efficacy, this approach is based on the ability of charcoal to reduce digoxin peak in serum as well as on its safety (Grade III recommendation). There are insufficient clinical data to support or exclude the use of repeated doses of activated charcoal to enhance digitalis elimination [26]. Similarly, usefulness of gastrointestinal decontamination in chronically poisoned patients remains to be determined.
Extracorporeal Removal Techniques
The international EXTRIP work group published a systematic review and recommendations on the extracorporeal treatment for digoxin poisoning [27]. Based on data from 84 patients including six fatalities, they concluded that digoxin is slightly dialyzable (level of evidence = B) and that extracorporeal removal techniques are unlikely to improve the outcome of digoxin-toxic patients whether or not anti-digoxin Fab fragments are administered. Despite the lack of robust clinical evidence, they recommended against the use of extracorporeal removal techniques in cases of severe digoxin poisoning when Fab fragments were available (1D) and also suggested against the use of extracorporeal removal techniques when Fab fragments were unavailable (2D).
Indications for ICU Admission
All patients suspected of acute or chronic digitalis poisoning with symptoms, ECG or electrolyte abnormalities, or any other significant underlying morbidity should be admitted to the intensive care unit given the high fatality rate associated with digitalis poisoning. In contrast, clinically stable patients receiving digoxin who meet the following criteria:
-
Mildly elevated serum digoxin concentrations
-
Without signs and symptoms of digoxin toxicity
-
With serum potassium >3.7 mmol/L and <4.5 mmol/L
-
With no history of severe cardiac disease
are at low risk of developing serious digoxin toxicity and may not require treatment beyond the discontinuation of digoxin therapy.
Electrolyte Disorders
Correction of hypokalemia, hypomagnesemia, and dehydration is important in the presence of chronic toxicity. In chronically treated patients, hyperkalemia may result not only from digitalis toxicity but also from renal insufficiency and other medications (potassium-sparing diuretics, nonsteroidal anti-inflammatory drugs, angiotensin-converting enzyme inhibitors, and nonselective β-blockers) that should be withdrawn temporarily. In acute poisoning, hyperkalemia (>4.5 mmol/L) is the hallmark of severe toxicity, and the patient may thus require anti-digoxin Fab fragments. Calcium salts should be avoided since one major mechanism of digitalis toxicity is primarily calcium loading of the myocardium. In the presence of severe hyperkalemia (>5.6 mmol/L), glucose/insulin, sodium bicarbonate, and sodium polystyrene sulfonate enema may be started; but severe hypokalemia may result if anti-digoxin Fab fragments are simultaneously administered.
Non-antidotal Therapies
Atropine antagonizes cardiac glycoside vagal activation, increasing heart rate. Atropine is the first-line treatment of digitalis-induced sinus bradycardia or atrioventricular conduction disturbance [6, 28]. The therapeutic success of atropine is unpredictable because the more direct non-vagotonic cardiac effects of digitalis at toxic doses may predominate. Doses of 0.5–1 mg are recommended but higher doses up to 2–3 mg have been used for persistent bradycardia. However, the use of a large cumulative dose of atropine may lead to deleterious anticholinergic encephalopathy.
Antidysrhythmics, including phenytoin, lidocaine, procainamide, propranolol, and amiodarone, have been used to treat digitalis-induced arrhythmias [29] (Grade II-3 evidence). Propranolol and procainamide must be avoided due to the risk of depression of cardiac conduction and contractility. Quinidine should not be used since it may prolong digoxin toxicity as a result of drug-impaired clearance. Lidocaine and phenytoin should be considered antiarrhythmic drugs of choice in the absence of anti-digoxin Fab fragments to treat digitalis-induced dysrhythmias because they have little effect on the sinus node and on AV conduction [7]. The role of fosphenytoin has not been evaluated in this setting.
Magnesium sulfate was effectively used to treat digoxin-induced arrhythmias, even in patients with normal or slightly elevated serum magnesium concentrations [30–32] (Grade II-3 evidence). Magnesium potentiates the activity of Na+/K+-ATPase without altering digoxin binding. A decrease in serum potassium concentration after magnesium therapy is obtained, but adverse effects from hypermagnesemia, particularly in patients with impaired renal function, may be observed. Hypermagnesemia is unlikely to occur with an initial 10–20 mmol magnesium bolus, but is a real issue with infusion or repeated doses. Anti-digoxin Fab fragments are the most effective and safe antidysrhythmic strategy to prevent and reverse digitalis-induced life-threatening arrhythmias.
Transvenous or transcutaneous cardiac pacing may be used to correct digitalis-induced bradycardia or conduction disturbances and to prevent ventricular dysrhythmias [33]. Retrospective studies have suggested that pacing does not significantly decrease the mortality rate of acute digitalis intoxication [33, 34]. Given the high rate of nonfatal and fatal complications associated with cardiac pacing in acute digitalis toxicity, electrical cardioversion is potentially hazardous, and Fab fragment therapy should be considered first-line treatment.
Anti-digoxin-Specific Fab Fragments
The efficacy and safety of anti-digoxin-specific Fab fragments have been consistently reported in adults [11–17, 21] and children [35–39] as well as in acute and chronic poisonings (Grade I evidence). A cost-effectiveness analysis supported the use of Fab fragments in the treatment of digoxin toxicity [40]. According to their cross-reactivity, Fab fragments can effectively neutralize digoxin, digitoxin, methyl-digoxin, β-acetyl-digoxin, lanatoside, ouabain, proscillaridin, and scilliroside and cardiac glycosides contained in yellow oleander and in toad and crab venom [41–46]. Anti-digoxin Fab fragments are indicated, based on internationally accepted criteria, to treat patients who present life-threatening tachy-bradyarrhythmias, hyperkalemia (>6 mmol/L), or hemodynamic instability with an elevated digoxin concentration (>2 ng/mL or 2.6 nmol/L) [47].
The theoretical maximum dose of anti-digoxin Fab Fragments is the one required to neutralize the body burden of digitalis. This dose can be calculated using either the supposed ingested dose or the serum digitalis concentration (Table 4). When no data are available regarding the presumed ingested dose or the plasma concentration, empirical dosing recommendations are to administer 400–800 mg of Fab (closely equivalent to 10–20 vials of DigiFab®) in acute toxicity and 120–240 mg of Fab (3–6 vials of DigiFab®) in chronic toxicity.
However the necessity of administering an equimolar dose of anti-digoxin Fab fragments to obtain an initial beneficial response is not supported by the literature [12, 21, 47]. The calculation of the equimolar dose of Fab fragments based on either the estimated ingested dose or the serum digitalis concentration frequently overestimates the amount of digitalis in the body. The calculation based on the estimate of ingested dose uses only the theoretical bioavailability of cardiac glycosides , whereas during the time interval between ingestion of digitalis and Fab administration, a fraction of the dose of digitalis has been already eliminated [48]. The relationship between the serum digitalis concentration and the corresponding actual amount in the body should also be questioned in patients admitted early during the course of the acute poisoning, since it is only accurate during the drug elimination phase and not during its distribution phase, which may last 6 h for digoxin [29]. Thus, since the lowest effective ant-digoxin Fab dose regimen is still not clearly determined, dosing regimens based on much lower initial doses were recently proposed, with 40 mg (one vial) for chronic poisoning and 80 mg (two vials) for acute poisoning, to be repeated after 60 min if inadequate response or recurrence, or earlier if there is a clinical deterioration [47]. Larger initial doses, including that which will achieve full neutralization, were recommended only in peri-arrest patients. Consistently, effectiveness of only 1–2 vials of anti-digoxin Fab fragments to bind all free digoxin in chronic digoxin poisonings was reported in a recent prospective observational study [16]. However, moderate improvement in heart rate and potassium following the Fab administration was usually observed, suggesting that bradyarrhythmia and hyperkalemia in the chronically poisoned patients could be related to other comorbidities including chronic renal failure, heart diseases, and medications like β-adrenoceptor blockers and calcium antagonists.
On another hand, since equimolar neutralization with Fab fragments is expensive and sometimes not available in small hospitals, antidote administration is often delayed or withheld until serious arrhythmias occur. Under these conditions, ventricular fibrillation and asystole often result in postanoxic brain damage or refractory cardiogenic shock [11–17, 21]. Interestingly, factors associated with the use of anti-digoxin Fab fragments were identified based on a retrospective review of patient records over 2 years in 20 city hospitals in France [17]. Acute overdose (odds ratio, 15.74), antidote availability in the hospital (11.06), serum potassium (1.81), and heart rate (0.96) were significantly linked to the use of anti-digoxin Fab fragments. Mortality was clearly lower in Fab-treated (6%, 4/67) compared to untreated patients (15%, 117/770). Thus, considering their safety, prophylactic administration of anti-digoxin Fab fragments to prevent the occurrence of life-threatening arrhythmias was proposed [48]. In France, this approach was refined, taking into account (1) the prognosticators of acute digitoxin poisoning [20, 49], (2) the lack of evidence for the efficacy of pacing [33, 34], and (3) the frequency and severity of adverse effects of cardiac pacing. Two treatment strategies for two distinct situations of digitalis poisonings were proposed [50]. In patients exhibiting life-threatening disturbances, an equimolar neutralizing dose of anti-digoxin Fab fragments (curative dose) was recommended to be rapidly administered. In patients with mild bradycardia (<50/min), regardless of the conduction disturbances, especially if associated poor prognostic factors [20], when atropine fails to accelerate the cardiac rhythm to greater than 50/min, a half equimolar neutralizing dose of anti-digoxin Fab fragments (“prophylactic” dose) was recommended. Particular attention was requested to >55-year-old patients, patients with underlying cardiac disease, and patients with serum potassium >4.5 mmol/L [51]. This French strategy based on the first-line use of anti-digoxin Fab fragments as curative vs. prophylactic treatment according to the patient’s conditions was associated with a reduced mortality rate (7.6%) [21].
There are no known contraindications, apart from allergy to sheep immunoglobulin. No interactions with other medications have been reported. During and after Fab administration, vital signs, ECG, and serum potassium levels should be recorded frequently to assess the efficacy and safety of treatment. Improvement in cardiac and noncardiac signs and symptoms of digitalis toxicity occurs rapidly after the anti-digoxin Fab fragments administration, with an initial response at a median of 19 min from termination of infusion and complete response at a median time of 88 min. [15] Neither age nor concurrent cardiac disease was associated with any significant delay in the initial response. Partial or no response resulted from (1) a moribund situation with multi-organ failure at the time of infusion, (2) an inadequate dose of Fab, (3) a concomitant toxicity from other drugs, and (4) an underestimated severity of underlying cardiac disease. None of the patients without heart disease who ingested a single acute digitalis dose did not respond to Fab [12]. The administration of additional doses of anti-digoxin Fab fragments should be considered in patients in whom life-threatening toxicity reappears or persists despite initial treatment. Recrudescent toxicity was reported in 20 of the 717 patients (2.8%) within 3 days of the initial Fab treatment in most of the patients, although as late as 4–11 days in a few patients [12]. Inadequacy of the initial dose was the only factor associated with recrudescent digitalis toxicity. In cases of massive digitoxin poisoning, recurrent toxicity has been reported 1–4 days after Fab administration and when the initial dose was less than the estimated adequate dose [35].
Measurement of serum digoxin concentrations after the administration of Fab fragments using the conventional analytical methods is no longer useful since measuring free plus bound digitalis. Detectable free digoxin concentrations may reappear 5–24 h or longer after Fab administration [53]. Measurement of the free digoxin concentration may be of value to determine the need for additional doses of Fab. When free serum digoxin concentration rebounds beyond 0.8 ng/mL (1.02 nmol/L), signs of digoxin intoxication recurred in some patients [53].
Safety is not an actual concern. Mild hypersensitivity reactions, including pruritic rash, facial swelling and flushing, urticaria, thrombocytopenia, shaking, and chills, rarely (~0.8%) occur. Hypokalemia may occur as elevated serum potassium concentrations decline rapidly, starting as soon as 1 h and completely normalizing within 4 h [15, 52]. Worsening of cardiac dysfunction after Fab fragment infusion is rare too (<3%) [15]. Data regarding the safety of Fab fragments in patients treated for more than one episode of digitalis toxicity are limited to draw any conclusion. Therapeutic redigitalization of the patient, if necessary, should be delayed until elimination of anti-digoxin Fab fragments is complete. Digoxin therapy can be administered safely 48–72 h after Fab infusion in patients with normal renal function [ 53].
Special Populations
Pediatric Patients
Digitalis poisoning has been reported in pediatric patients ranging from 1 day to 17 years old [35–39]. Iatrogenic intoxication is due to errors in the calculation or administration of the digitalizing and maintenance doses in smaller children. Accidental poisonings occur in young children and less commonly, adolescents may ingest digitalis in a suicidal attempt. Digitalis intoxication is most often accompanied by few clinical effects. Neurologic manifestations, life-threatening arrhythmias, conduction defects, and secondary hypotension may be observed like in adults. Hyperkalemia is uncommon. Anti-digoxin Fab fragments were consistently reported to be effective and safe in pediatric patients. Indications of antidote administration are based on the following recommendations: [39]
Known Digoxin Intoxication
-
Strong evidence of acute ingestion of ≥0.1 mg/kg digoxin
-
Elevated (steady-state) serum digoxin concentration ≥5 ng/mL (6.4 nmol/L)
Signs and Symptoms of Digitalis Toxicity
-
Rapidly progressing features of digoxin toxicity
-
Potentially life-threatening arrhythmias, including cardiac conduction disturbances
-
Severe hyperkalemia (≥6.0 mmol/L)
The prophylactic administration of anti-digoxin Fab fragments was also considered in children, the main objective being, however, to avoid any delay in their administration. Dosage is similar to adults, paying attention to the dilution to avoid fluid overload in small children. The empirical Fab dosing is 400–800 mg in acute poisoning and 40–80 mg in chronic toxicity. Increased serum potassium concentration usually normalizes within 4 h of administration [36]. In the main study, no cases of hypersensitivity have been reported, while hypokalemia occurred in one case and recurrence of cardiac conduction defects after treatment in three children requiring a repeated dose to reverse [39].
Pregnant Patients
During pregnancy, digitalis overdose may result in maternal and fetal digitalis poisoning. Pregnant patients with acute digitalis overdose should be treated similarly to nonpregnant patients. However, there are no definitive data regarding the efficacy or safety of anti-digoxin Fab fragments in pregnant women.
Elderly Patients
Digoxin toxicity in the elderly is common, ranging from minor gastrointestinal symptoms to life-threatening dysrhythmias. Increased risk of toxicity in the elderly is related to their multiple medications, their decreased renal clearance, and the increased risk of unintentional ingestion of repeated doses due to their cognitive impairments. Mild-to-moderate digoxin toxicity in the elderly may be difficult to recognize from other “signs of old age,” i.e., somnolence, decreased hearing, confusion, agitation, poor appetite, nausea, vomiting, and diarrhea [54]. In the treated elderly patients, chronic toxicity should be suspected in the new onset of dysrhythmias, malaise, gastrointestinal disturbances, or mental status changes. Lethargy, depression, and confusion seem to occur almost exclusively in the elderly [55]. Advanced age seems to be an independent poor prognostic factor.
Renal Dysfunction Patients
Patients with renal dysfunction are at high risk of digoxin poisoning. Fab therapy is effective in patients with renal dysfunction [11–17]. Fab fragments should be given to patients with renal impairment at the same dose as for patients with normal renal function [56]; however, elimination of digoxin-specific Fab complexes is prolonged. Total body clearance of Fab fragments is related linearly to creatinine clearance, whereas their apparent volume of distribution is not affected [56]. Free digoxin concentrations decrease rapidly after Fab therapy but rebound at about 77 ± 46 h postinjection [57]. The magnitude by which free digoxin concentration rebounds is unaffected by the degree of renal dysfunction. There is no evidence to support a dissociation of the Fab/digoxin complexes over extended periods [53]. Because there are rarely complications resulting from circulating Fab/digoxin complexes for a prolonged period, however, there is little evidence to recommend any extrarenal technique to enhance their elimination [27]. Monitoring free serum digoxin concentrations may be of value in selected patients to guide additional Fab dosing, confirm possible rebound toxicity, or guide the re-initiation of digoxin therapy [ 57].
Key Points in Digitalis Poisoning
-
1.
To date, digoxin poisoning mainly results from chronic toxicity in long-term treated elderly patients with underlying cardiac diseases due to acute renal onset or drug-drug interactions rather than from the suicidal or accidental exposure to a single high digoxin dose.
-
2.
Digitalis poisoning may be life-threatening with the sudden onset of fatal ventricular dysrhythmias.
-
3.
Mild-to-moderate digoxin toxicity in the elderly may be difficult to recognize from other “signs of old age.”
-
4.
The emergency determination of the serum digitalis concentration is mandatory in each patient with suspected digitalis toxicity.
-
5.
Prognosticators including age >55 years, serum potassium >4.5 mmol/L, and atrioventricular block of any degree should be recognized on patient management.
-
6.
Antidysrhythmic drugs and cardiac pacing should be not be used anymore if anti-digoxin Fab fragments are available.
-
7.
Anti-digoxin Fab fragments represent the first-line antidote in the presence of hyperkalemia, cardiac conduction disturbances, or life-threatening arrhythmias.
-
8.
The currently recommended dosing regimen of anti-digoxin Fab fragments is to administer 40 mg (one vial) for chronic poisoning and 80 mg (two vials) for acute poisoning and repeat after 60 min if inadequate response or recurrence or earlier if clinical deterioration.
-
9.
Prophylactic semi-molar dosing of anti-digoxin Fab fragments in the presence of bad prognosticators has been proposed with success to reduce digitalis-related fatality.
-
10.
The extracorporeal removal techniques are unlikely to improve the outcome of digoxin-toxic patients whether or not anti-digoxin Fab fragments is administered.
References
Ziff OJ, Kotecha D. Digoxin: the good and the bad. Trends Cardiovasc Med. 2016;pii: S1050-1738(16)30006-8.
The Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336:525–33.
Ahmed A, Rich MW, Fleg JL, et al. Effects of digoxin on morbidity and mortality in diastolic heart failure: the ancillary digitalis investigation group trial. Circulation. 2006;114:397–403.
Goldberger ZD, Alexander GC. Digitalis use in contemporary clinical practice: refitting the foxglove. J Am Med Assoc Intern Med. 2014;174:151–4.
Smith TW, Haber E, Yeatman L, Butler Jr VP. Reversal of advanced digoxin intoxication with Fab fragments of digoxin-specific antibodies. N Engl J Med. 1976;294:797–800.
Roberts DM, Gallapatthy G, Dunuwille A, Chan BS. Pharmacological treatment of cardiac glycoside poisoning. Br J Clin Pharmacol. 2016;81:488–95.
Smith TW. Digitalis: mechanisms of action and clinical use. N Engl J Med. 1988;318:358–65.
Wasserstrom JA, Aistrup GL. Digitalis: new actions for an old drug. Am J Physiol Heart Circ Physiol. 2005;289:H1781–93.
Gheorghiade M, St Clair J, St Clair C, Beller GA. Hemodynamic effects of intravenous digoxin in patients with severe heart failure initially treated with diuretics and vasodilators. J Am Coll Cardiol. 1987;9:849–57.
Wofford JL, Ettinger WH. Risk factors and manifestations of digoxin toxicity in the elderly. Am J Emerg Med. 1991;9(2 Suppl 1):11–5.
Hauptman PJ, Blume SW, Lewis EF, Ward S. Digoxin toxicity and use of digoxin immune Fab: insights from a national hospital database. JACC Heart Fail. 2016;4:357–64.
Hickey AR, Wenger TL, Carpenter VP, Tilson HH, Hlatky MA, Furberg CD, et al. Digoxin immune Fab therapy in the management of digitalis intoxication: safety and efficacy results of an observational surveillance study. J Am Coll Cardiol. 1991;17:590–8.
Nordt SP, Clark RF, Machado C, Cantrell FL. Assessment of digoxin-specific fab fragment dosages in digoxin poisoning. Am J Ther. 2016;23:e63–7.
Chhabra N, Valento M, Bryant SM, Aks SE. Digoxin-specific antibody fragment dosing: a case series. Am J Ther. 2016 (in press).
Antman EM, Wenger TL, Butler Jr VP, Haber E, Smith TW. Treatment of 150 cases of life-threatening digitalis intoxication with digoxin-specific Fab antibody fragments: final report of a multicenter study. Circulation. 1990;81:1744–52.
Chan BS, Isbister GK, O’Leary M, Chiew A, Buckley NA. Efficacy and effectiveness of anti-digoxin antibodies in chronic digoxin poisonings from the DORA study (ATOM-1). Clin Toxicol (Phila). 2016;54:488–94.
Lapostolle F, Borron SW, Verdier C, Arnaud F, Couvreur J, Mégarbane B, et al. Assessment of digoxin antibody use in patients with elevated serum digoxin following chronic or acute exposure. Intensive Care Med. 2008;34:1448–53.
Yang EH, Shah S, Criley JM. Digitalis toxicity: a fading but crucial complication to recognize. Am J Med. 2012;125:337–43.
Kanji S, MacLean RD. Cardiac glycoside toxicity: more than 200 years and counting. Crit Care Clin. 2012;28:527–35.
Dally S, Alperovitch A, Lagier G, Bismuth C, Fournier E. Prognostic factors in acute digitalis poisoning. Nouv Presse Med. 1981;10:2257–60.
Lapostolle F, Borron SW, Verdier C, Taboulet P, Guerrier G, Adnet F, et al. Digoxin-specific Fab fragments as single first-line therapy in digitalis poisoning. Crit Care Med. 2008;36:3014–8.
Ordog G, Benaron S, Bhasin V. Serum digoxin levels and mortality in 5100 patients. Ann Emerg Med. 1987;16:32–9.
Shapiro W. Correlative studies of serum digitalis levels and the arrhythmias of digitalis intoxication. Am J Cardiol. 1978;41:852–9.
Williamson KM, Thrasher KA, Fulton KB, LaPointe NM, Dunham GD, Cooper AA, et al. Digoxin toxicity: an evaluation in current clinical practice. Arch Intern Med. 1998;158:2444–9.
Lehmann HU, Witt E, Temmen L, Hochrein H. Life-threatening digitalis intoxication with and without additional diuretic treatment. Dtsch Med Wochenschr. 1978;103:1566–71.
Position statement and practice guidelines on the use of multi-dose activated charcoal in the treatment of acute poisoning. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol. 1999;37:731–51.
Mowry JB, Burdmann EA, Anseeuw K, Ayoub P, Ghannoum M, Hoffman RS, et al. Extracorporeal treatment for digoxin poisoning: systematic review and recommendations from the EXTRIP Workgroup. Clin Toxicol (Phila). 2016;54:103–14.
Navab F, Honey M. Self-poisoning with digoxin: successful treatment with atropine. Br Med J. 1967;3:660–1.
Mooradian A. Digitalis: an update of clinical pharmacokinetics, therapeutic monitoring techniques and treatment recommendations. Clin Pharmacokinet. 1988;15:165–79.
Cohen L, Kitzes R. Magnesium sulfate and digitalis-toxic arrhythmias. JAMA. 1983;249:2808–10.
French JH, Thomas RG, Siskind AP, Brodsky M, Iseri LT. Magnesium therapy in massive digoxin intoxication. Ann Emerg Med. 1984;13:562–6.
Reisdorff EJ, Clark MR, Walters BL. Acute digitalis poisoning: the role of intravenous magnesium sulfate. J Emerg Med. 1986;4:463–9.
Bismuth C, Motte G, Conso F, Chauvin M, Gaultier M. Acute digitoxin intoxication treated by intracardiac pacemaker: experience in sixty-eight patients. J Toxicol Clin Toxicol. 1977;10:443–56.
Taboulet P, Baud FJ, Bismuth C, Vicaut E. Acute digitalis intoxication – is pacing still appropriate? J Toxicol Clin Toxicol. 1993;31:261–73.
Berkovitch M, Akilesh MR, Gerace R, Verjee Z, McGuigan M, Whyte H, et al. Acute digoxin overdose in a newborn with renal failure: use of digoxin immune Fab and peritoneal dialysis. Ther Drug Monit. 1994;16:531–3.
Gittelman MA, Stephan M, Perry H. Acute pediatric digoxin ingestion. Pediatr Emerg Care. 1999;15:359–62.
Kaufman J, Leikin J, Kendzierski D, Polin K. Use of digoxin Fab immune fragments in a seven-day-old infant. Pediatr Emerg Care. 1990;6:118–21.
Schmitt K, Tulzer G, Hackel F, Sommer R, Tulzer W. Massive digitoxin intoxication treated with digoxin-specific antibodies in a child. Pediatr Cardiol. 1994;15:48–9.
Woolf AD, Wenger T, Smith TW, Lovejoy Jr FH. The use of digoxin-specific Fab fragments for severe digitalis intoxication in children. N Engl J Med. 1992;326:1739–44.
Mauskopf JA, Wenger TL. Cost-effectiveness analysis of the use of digoxin immune Fab (ovine) for treatment of digoxin toxicity. Am J Cardiol. 1991;68:1709–14.
Kurowski V, Iven H, Djonlagic H. Treatment of a patient with severe digitoxin intoxication by Fab fragments of anti-digitalis antibodies. Intensive Care Med. 1992;18:439–42.
Hess T, Stucki P, Barandun S, Scholtysik G, Riesen W. Treatment of a case of lanatoside C intoxication with digoxin-specific F(ab′)2 antibody fragments. Am Heart J. 1979;98:767–71.
Eddleston M, Rajapakse S, Rajakanthan K, Jayalath S, Sjöström L, Santharaj W, et al. Anti-digoxin Fab fragments in cardiotoxicity induced by ingestion of yellow oleander: a randomized controlled trial. Lancet. 2000;355:967–71.
Bandara V, Weinstein SA, White J, Eddleston M. A review of the natural history, toxinology, diagnosis and clinical management of Nerium oleander (common oleander) and Thevetia peruviana (yellow oleander) poisoning. Toxicon. 2010;56:273–81.
Roberts DM, Buckley NA. Antidotes for acute cardenolide (cardiac glycoside) poisoning. Cochrane Database Syst Rev. 2006;4, CD005490.
Maillaud C, Barguil Y, Mikulski M, Cheze M, Pivert C, Deveaux M, et al. First successful curative use of digoxin-specific Fab antibody fragments in a life-threatening coconut crab (Birgus latro L.) poisoning. Toxicon. 2012;60:1013–7.
Chan BS, Buckley NA. Digoxin-specific antibody fragments in the treatment of digoxin toxicity. Clin Toxicol (Phila). 2014;52:824–36.
Smolarz A, Roesch E, Lenz E, Neubert H, Abshagen P. Digoxin specific antibody (Fab) fragments in 34 cases of severe digitalis intoxication. J Toxicol Clin Toxicol. 1985;23:327–40.
Bismuth C, Motté G, Fréjaville JP, Conso F. Hyperkalemia in massive digitalis intoxication. Prognostic value and therapeutic implications. Arch Mal Coeur Vaiss. 1973;66:1537–41.
Taboulet P, Baud FJ, Bismuth C. Clinical features and management of digitalis poisoning – rationale for immunotherapy. J Toxicol Clin Toxicol. 1993;31:247–60.
Mégarbane B, Baud FJ. Early digoxin-specific antibody fragments for treating patients at risk of life-threatening digoxin toxicity. Clin Toxicol (Phila). 2014;52:985–6.
Wenger TL, Butler Jr VP, Haber E, Smith TW. Treatment of 63 severely digitalis-toxic patients with digoxin-specific antibody fragments. J Am Coll Cardiol. 1985;5(5 Suppl A):118A–23.
Ujhelyi MR, Robert S. Pharmacokinetic aspects of digoxin-specific Fab therapy in the management of digitalis toxicity. Clin Pharmacokinet. 1995;28:483–93.
Brunner G, Zweiker R, Krejs GJ. A toxicological surprise. Lancet. 2000;356:1406.
Portnoi V. Digitalis delirium in the elderly. J Clin Pharmacol. 1979;19:747–50.
Renard C, Grene-Lerouge N, Beau N, Baud F, Scherrmann JM. Pharmacokinetics of digoxin-specific Fab: Effects of decreased renal function and age. Br J Clin Pharmacol. 1997;44:135–8.
Ujhelyi MR, Robert S, Cummings DM, Colucci RD, Green PJ, Sailstad J, et al. Influence of digoxin immune Fab therapy and renal dysfunction on the disposition of total and free digoxin. Ann Intern Med. 1993;119:273–7.
Acknowledgments
The author would like to thank Prof. Frédéric Lapostolle who contributed to the first version of this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Grading System for Levels of Evidence Supporting Recommendations in Critical Care Toxicology, 2nd Edition
-
I
Evidence obtained from at least one properly randomized controlled trial.
-
II-1
Evidence obtained from well-designed controlled trials without randomization.
-
II-2
Evidence obtained from well-designed cohort or case-control analytic studies, preferably from more than one center or research group.
-
II-3
Evidence obtained from multiple time series with or without the intervention. Dramatic results in uncontrolled experiments (such as the results of the introduction of penicillin treatment in the 1940s) could also be regarded as this type of evidence.
-
III
Opinions of respected authorities, based on clinical experience, descriptive studies and case reports, or reports of expert committees.
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this entry
Cite this entry
Mégarbane, B. (2017). Digitalis Glycosides. In: Brent, J., et al. Critical Care Toxicology. Springer, Cham. https://doi.org/10.1007/978-3-319-17900-1_185
Download citation
DOI: https://doi.org/10.1007/978-3-319-17900-1_185
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-17899-8
Online ISBN: 978-3-319-17900-1
eBook Packages: Biomedical and Life SciencesReference Module Biomedical and Life Sciences