
Abstract
Thoracic trauma is the cause of significant mortality amongst trauma patients. In this chapter, mechanisms, work-up, and management of various injuries are discussed. Abnormal presence of air within the pleural cavity. Lung compression reduces lung compliance, volumes, and diffusion capacity. If left untreated, air can accumulate without decompressing adequately, leading to high positive pleural pressures, causing severe lung collapse, and compression of the mediastinum, great vessels, and heart, and ultimately hemodynamic compromise secondary to decreased venous return.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Pneumothorax
- Hemothorax
- Rib fracture
- ED thoracotomy
- Thoracoabdominal injury
- Blunt cardiac injury
- Diaphragmatic injury
Pneumothorax
Pathophysiology
-
Abnormal presence of air within the pleural cavity.
-
Lung compression reduces lung compliance, volumes, and diffusion capacity.
• Tension Pneumothorax:
-
If left untreated, air can accumulate without decompressing adequately, leading to high positive pleural pressures, causing severe lung collapse, and compression of the mediastinum, great vessels, and heart, and ultimately hemodynamic compromise secondary to decreased venous return.
-
Patients in tension pneumothorax require immediate needle decompression in the second intercostal space at the mid-clavicular line, followed by tube thoracostomy.
Mechanism
-
Abnormal communication between the pleural cavity and either the alveoli or airways cause the air to flow into the pleural cavity, eliminating its negative pressure and leading to collapse of the lung (Fig. 7.1). This can happen with penetrating or blunt chest traumas.
Fig. 7.1. 
Patient presenting with a traumatic pneumothorax after blunt trauma to the chest. Black arrows denote the outline of the collapsed lung.
-
Massive air leak suggests injury to major airways.
-
Penetrating: Air enters the pleural cavity either directly through the wound in the chest wall or from a parenchymal laceration caused by the injury.
-
Blunt: Parenchymal laceration secondary to an associated injury (rib fracture, bronchial rupture, alveolar rupture).

• Open Pneumothorax (Sucking Chest Wound):
-
Air enters the pleural cavity through the chest wall defect with inspiration, thereby eliminating the pressure gradient between the pleural cavity and alveoli.
-
Should be initially covered with a 3-way occlusive dressing, followed by tube thoracostomy and an occlusive dressing.
Diagnosis
-
Pleuritic chest pain and dyspnea are the most common symptoms.
-
On primary survey, several signs are indicative of a pneumothorax, including decreased or absent breath sounds, subcutaneous emphysema (Fig. 7.2), and hyperresonance. A tension pneumothorax may also present with tracheal deviation to the contralateral side, severe respiratory distress, and hemodynamic instability.
Fig. 7.2. 
Significant subcutaneous emphysema seen on the chest X-ray of a patient with a pneumothorax after blunt trauma to the chest.
-
Diagnosis is established by an upright chest X-ray. If clinical signs of tension physiology are evident, X-ray confirmation should be omitted and immediate decompression should ensue, followed by a chest tube.
-
An expiratory view accentuates the separation of the parietal and visceral pleura.
-
Pneumothorax in supine patients accumulates into the dependent regions of the anterior and subdiaphragmatic pleura and may be detected as a deep sulcus sign.
-
CT scan is the gold standard for diagnosis and can detect occult pneumothoraces undetected by chest radiograph.
-
Ultrasound is also an accurate, rapid, and noninvasive test in trauma patients.
-

Management
-
Management depends on the clinical setting, mechanism of injury, size of the pneumothorax, and associated conditions. Advanced Trauma Life Support (ATLS) guidelines should be followed for all trauma patients [3].
-
The appropriate initial diagnostic tests and management options should be tailored to the presentation of the patient:
-
Hemodynamically unstable patients with clinical signs of a pneumothorax should have a large-bore chest tube placed as part of the primary survey (with or without needle decompression preceding it for suspected tension pneumothorax).
-
For patients who are stable, imaging studies can confirm the diagnosis prior to definitive management.
-
-
Observation:
-
Reserved for asymptomatic patients with small or occult pneumothoraces who are unlikely to have an ongoing air leak. Follow-up radiography should be obtained at 3 h to document improvement or to make sure there is no worsening.
-
Supplemental oxygen can help decrease the concentration of nitrogen in the body, thus creating a gradient to drive the air in the pleura (mostly composed of nitrogen) into the body.
-
-
Percutaneous Catheters:
-
Small- to medium-calibre tube thoracostomy can be performed percutaneously via the Seldinger technique and attached to either a Heimlich one-way valve or a suction.
-
Use is limited to a pneumothorax with small or no associated hemothorax.
-
-
Tube Thoracostomy:
-
Large-bore chest tubes are the standard of care for treatment of traumatic pneumothoraces, unstable patients, persistent or large air leaks, and associated effusions or hemothoraces.
-
Hemothorax
Mechanism and Pathophysiology
-
Abnormal presence of blood in the pleural cavity.
-
Significant hemothorax may be caused by injury to the great vessels, heart, lung parenchyma, or chest wall/intercostal vessels, secondary to either blunt or penetrating injury.
Diagnosis
-
Clinical presentation and diagnosis are similar to pneumothorax, except for dullness to percussion.
-
Upright chest X-ray will confirm the diagnosis if >300 mL of blood is present (Fig. 7.3).
Fig. 7.3. 
Traumatic hemothorax diagnosed on chest X-ray. (a) Patient presenting with a massive left hemothorax after blunt trauma to the chest. The mediastinal structures, including the heart, trachea, and major airways, are shifted to the right. Typically blood can be identified on upright chest X-ray (b, c); however this may not always be the case if the patient is supine (d).
-
Hemodynamically unstable patients with signs of pneumohemothorax require immediate decompression without imaging.

Management
-
ATLS protocols should be followed, starting with a primary and secondary survey.
-
Goal is complete removal of all blood. Residual blood is a nidus for the development of empyema and fibrothorax, which can also occur due to improper positioning or obstruction of the chest tube [4].
-
If this is not feasible with one chest tube, residual blood can either be removed by additional chest tube(s) or surgically (thoracoscopically if patient is clinically stable).
-
-
Posttraumatic empyema can also occur secondary to a foreign body, lung abscess, bronchopleural fistula, esophageal perforation, or an abdominal source [5]. See Chap. 4 : Pleural Disorders (Empyema).
-
Tube thoracostomy is initially performed using a 32–36 French chest tube.
-
Indications for thoracotomy:
-
Hemodynamic instability
-
>1,500 mL of blood drains initially upon insertion of chest tube
-
Persistent bleeding of >200 mL/h for 4 h
-
Chest Wall Injuries
-
The types of chest wall injuries vary depending on the mechanism of trauma, force of injury, and the patient’s characteristics. Certain injuries such as fractures of the first rib, sternum, scapula, lower ribs, and bilateral ribs are associated with other life-threatening injuries.
Rib Fractures:
Mechanism and Pathophysiology:
-
Most common injury following blunt chest trauma (30–40 % of all thoracic trauma) [6].
-
Physiologic sequelae of rib fractures are related to their impact on normal pulmonary mechanics mostly due to significant pain, causing decreased ability to cough, reduced lung volumes, and an increased risk for pneumonia.
-
This is especially true for the elderly who have reduced chest wall compliance, reduced bone density, and higher incidence of underlying lung disease [7].
-
-
Flail Chest: Occurs when three or more adjacent ribs are fractured in two places (Fig. 7.4). The most common mechanism is direct-impact injury (e.g., steering wheel).
Fig. 7.4. 
Patient presenting with multiple rib fractures, sternal fracture, flail chest, and associated lung injuries (bilateral pneumohemothoraces and pulmonary contusions) after a crush injury to the chest. Subcutaneous emphysema can be seen throughout the anterior and lateral chest wall.
-
Leads to severe disruption of lung mechanics with paradoxical motion during breathing, placing patients at very high risk of respiratory failure. Patients also often have severe pulmonary contusions.
-
Paradoxical motion may not be obvious during positive-pressure ventilation.
-

Management
-
Aggressive pain control is fundamental in managing rib fractures and improving lung mechanics. For limited rib fractures (≤3) in healthy young adults, this might be the only necessary management and can be carried out as an outpatient.
-
Various methods available: regional anaesthesia, epidural infusion, paravertebral block, intrapleural infusion, patient-controlled analgesia pumps, oral or intravenous narcotics, and nonsteroidal anti-inflammatories.
-
-
Chest physiotherapy, incentive spirometry, and frequent pulmonary toilet should be encouraged.
-
Patients with severe respiratory compromise may require mechanical ventilation.
-
Surgical fixation (Fig. 7.5) is indicated in select patients [8]. Acceptable indications include:
Fig. 7.5. 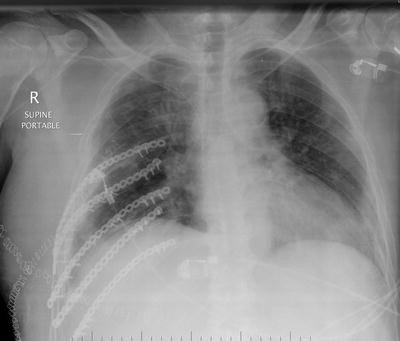
Patient with flail chest who underwent surgical fixation.
-
Flail chest
-
Pain refractory to conservative management options
-
Significant chest wall deformity
-
Chest wall instability and symptomatic nonunion
-
Displaced ribs found on thoracotomy performed for other reasons
-
Open fractures
-

Sternal Fracture:
Mechanism
-
Occurs in less than 0.5 % of all traumas [9].
-
Most commonly caused after rapid deceleration from motor vehicle collisions.
-
Almost always transverse at the sternomanubrial joint or midbody of the sternum.
-
Associated with the use of three-point restraints.
-
Can be associated with other injuries due to the large force necessary required to cause fracture—especially in unrestrained passengers and crush injuries.
-
Associated injuries include rib fractures, myocardial contusion, vertebral fractures, hemopericardium, hemothorax, pneumothorax, and retrosternal hematoma.
-
-
Patients should undergo a CT scan to rule out other injuries and an electrocardiogram to screen for blunt cardiac injury (BCI) (Fig. 7.4).
Management
-
Initially, care is directed towards the primary and secondary survey, exclusion of other injuries, and adequate pain control.
-
According to the severity of the fracture and associated injuries, the patient might need a surgical fixation (if severely displaced or unstable fractures) or cardiac monitoring [10, 11].
Pulmonary Contusions
Mechanism and Pathophysiology:
-
Bruising of the lung, mostly caused by blunt thoracic trauma and associated with chest wall injuries.
-
Blood accumulating in the alveoli results in right-to-left shunting, leading to ventilation-perfusion mismatch and subsequent hypoxia.
-
Radiographic evidence of contusions may be delayed, and appear only 24–48 h after the injury (Fig. 7.6).
Fig. 7.6. 
Bilateral pulmonary contusions after blunt trauma to the chest.

Management
-
Pulmonary contusions are managed similarly to all chest wall injuries, including treating associated injuries, pain control, pulmonary toilet, incentive spirometry, and chest physiotherapy.
-
Excessive volume resuscitation can exacerbate the negative physiologic consequences of pulmonary contusions.
-
Aim is to maintain euvolemia.
-
Blunt Cardiac Injury
Mechanism and Pathophysiology
-
The incidence of BCI after blunt thoracic injury is approximately 20 %, occurring most commonly with motor vehicle collisions [14].
-
BCI can manifest itself in several forms, ranging from minor electrocardiogram changes to heart failure and septal or free wall rupture.
-
The most common BCIs are myocardial contusion (60–100 %), right ventricular injury (17–32 %), and right atrial injury (8–65 %) [14].
Diagnosis
-
Electrocardiogram is the initial investigation of choice.
-
Any arrhythmias (e.g., sinus tachycardia, nonspecific ST or T wave changes, heart block, or other forms of dysrhythmias) should be followed by a transthoracic echocardiogram.
-
Controversy exists regarding the utility of troponin levels for patients suspected of having BCI, and given the lack of evidence to support its use, many experts recommend against it. However, the latest Eastern Association for the Surgery of Trauma (EAST) guidelines have changed and now recommend both electrocardiogram and troponin I level for all patients suspected to have suffered BCI (negative predictive value: 100 %) [15].
Management: See Fig. 7.7

Management algorithm for blunt cardiac injury (BCI). EKG electrocardiogram, HD hemodynamically. *Hemodynamically unstable patients are managed separately based on ATLS management protocols. **Some experts also recommend ordering troponin I levels to screen for BCI.
Diaphragmatic Injuries
Mechanism
-
More common after penetrating (4 %) than blunt (1 %) thoracoabdominal trauma [16].
-
Penetrating: Direct injury to the diaphragm
-
Blunt: Sudden increase in intra-abdominal pressure
-
Blunt diaphragmatic injuries are more common on the left due to the liver’s absorptive capacity protecting the right hemidiaphragm.
Diagnosis
-
Early diagnosis can avoid herniation and possibly strangulation of intra-abdominal content into the chest.
-
In patients with other indications for surgical intervention, injury to the diaphragm is ruled out intraoperatively either through the abdomen (laparotomy or laparoscopy) or the thorax (thoracotomy or VATS).
-
For patients without any other indications for surgical intervention, diagnosis may be difficult.
-
Chest X-ray can demonstrate herniated viscus in the thorax (unless positive-pressure ventilation prevents this), and other signs that are suggestive of injury, such as lower rib and sternal fractures, an elevated hemidiaphragm (Fig. 7.8), and a nasogastric tube traveling back up into the chest. Sensitivity however is limited using this and other imaging modalities (i.e., CT, FAST).
Fig. 7.8. 
Chest X-ray of a patient with a diaphragmatic injury.
-
Hemodynamically stable patients who have clinical suspicion of a diaphragmatic injury should be evaluated by either laparoscopy (preferred) or thoracoscopy. If laparoscopy is used, it should be performed after other intra-abdominal injuries have been ruled out.

Management
-
All patients already undergoing trauma laparotomy or thoracotomy for other reasons should undergo careful examination of the diaphragm (Fig. 7.9).
Fig. 7.9. 

(a-c) Patient with a left penetrating (stab) thoracoabdominal injury with the stomach is seen herniating through the chest. This patient underwent an exploratory laparotomy and the diaphragmatic defect (black arrow) was identified and repaired. Used with permission from Dr. Dan L Deckelbaum.Fig. 7.9. (continued) (d-e) Another patient with a similar left diaphragmatic injury (white arrow) that was repaired after an exploratory laparotomy using non-absorbable sutures.
-
Most diaphragmatic injuries should be repaired with nonabsorbable sutures, usually via the abdomen due to the high likelihood of associated injuries [17]. Select hemodynamically stable patients who would otherwise not be explored surgically, with an asymptomatic, small, right-sided injury that is tamponaded by the liver, may be observed.


Approach to Penetrating Chest Trauma Management (Fig. 7.10)


Management algorithms for penetrating chest trauma to the cardiac box (a) and lateral/posterior chest (b). HD hemodynamic, CXR chest X-ray, FAST Focused Assessment for the Sonographic evaluation of Trauma, PTx pneumothorax, HTx hemothorax, ED emergency department. *Volume resuscitation includes placing large-bore peripheral or central venous catheters and massive transfusion protocol. **Criteria for resuscitative thoracotomy should be met prior to its initiation. ***Significant hemothorax should be followed by a thoracotomy (i.e., >1,500 mL, or >200 mL/h × 4 h).
Resuscitative, Emergency Department (ED) Thoracotomy
-
ED thoracotomy is a life-saving procedure that is performed for patients with specific injuries who have had a recently witnessed loss of measurable blood pressure or palpable pulse (Table 7.1).
Table 7.1. Indications for a resuscitative thoracotomy [13]. -
Outcomes vary significantly amongst patients, with survival rates of 3–35 % in isolated cardiac injuries, 1–14 % in penetrating trauma, and 0–1 % in blunt trauma [12].
-
The ED thoracotomy is limited to very few life-saving therapeutic maneuvers (Fig. 7.11):
Fig. 7.11. 
An ED thoracotomy performed on a patient with a penetrating trauma to the chest. After making the incision just below the nipple line (a) and getting access to the chest cavity, a pericardiotomy is performed (black arrow) to decompress any potential cardiac tamponade (b, c). Cardiac massage (d) can also be performed using a two-hand technique. Used with permission from Dr. Dan L Deckelbaum.
-
Releasing a pericardial tamponade
-
Open cardiac massage
-
Cross-clamping the descending aorta
-
Controlling hemorrhage (cardiac or other intrathoracic sources)
-

References
Dulchavsky SA et al. Prospective evaluation of thoracic ultrasound in the detection of pneumothorax. J Trauma. 2001;50(2):201–5.
Blaivas M, Lyon M, Duggal S. A prospective comparison of supine chest radiography and bedside ultrasound for the diagnosis of traumatic pneumothorax. Acad Emerg Med. 2005;12(9):844–9.
Advanced trauma life support for doctors student course manual. 8th ed. American college of Surgeons Committee on Trauma. 2008.
Aguilar MM et al. Posttraumatic empyema. Risk factor analysis. Arch Surg. 1997;132(6):647–50. discussion 650–1.
Mandal AK et al. Posttraumatic empyema thoracis: a 24-year experience at a major trauma center. J Trauma. 1997;43(5):764–71.
Sirmali M et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg. 2003;24(1):133–8.
Bergeron E et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma. 2003;54(3):478–85.
Lafferty PM et al. Operative treatment of chest wall injuries: indications, technique, and outcomes. J Bone Joint Surg Am. 2011;93(1):97–110.
Recinos G et al. Epidemiology of sternal fractures. Am Surg. 2009;75(5):401–4.
von Garrel T et al. The sternal fracture: radiographic analysis of 200 fractures with special reference to concomitant injuries. J Trauma. 2004;57(4):837–44.
Peek GJ, Firmin RK. Isolated sternal fracture: an audit of 10 years’ experience. Injury. 1995;26(6):385–8.
Rhee PM et al. Survival after emergency department thoracotomy: review of published data from the past 25 years. J Am Coll Surg. 2000;190(3):288–98.
Moore EE et al. Defining the limits of resuscitative emergency department thoracotomy: a contemporary Western Trauma Association perspective. J Trauma. 2011;70(2):334–9.
Schultz JM, Trunkey DD. Blunt cardiac injury. Crit Care Clin. 2004;20(1):57–70.
Clancy K et al. Screening for blunt cardiac injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S301–6.
Rubikas R. Diaphragmatic injuries. Eur J Cardiothorac Surg. 2001;20(1):53–7.
Hanna WC, Ferri LE. Acute traumatic diaphragmatic injury. Thorac Surg Clin. 2009;19(4):485–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Aboalsaud, A., Deckelbaum, D.L. (2015). Chest Trauma. In: Madani, A., Ferri, L., Seely, A. (eds) Pocket Manual of General Thoracic Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-17497-6_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-17497-6_7
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-17496-9
Online ISBN: 978-3-319-17497-6
eBook Packages: MedicineMedicine (R0)