
Abstract
The Expanded Criteria Donor (ECD) recommends histological evaluation of the kidney not only for donors over 60 but also for donors over 50 with comorbidities (firstly hypertension) even in the setting of normal serum creatinine [1]. The histological parameters to be evaluated include glomerular, vascular, tubular and interstitial injury. However, no studies have provided an absolute threshold beyond which a donor kidney must not be used, and there is no consensus on the value of biopsies for predicting graft function. Histological evaluation of the donor biopsy can be performed at harvesting by on call pathological examination or by means of implantation biopsies. Tissue sample analysis of implantation biopsies includes the immunohistochemistry (IHC) evaluation of C4d to identify pre-sensitized patients and immunofluorescence to highlight misdiagnosed glomerular diseases. The biopsies can be obtained through a wedge resection or needle core biopsy: superficial sampling in wedge resections can overestimate the glomerular sclerosis and fibrosis because the outer cortex is more sensitive to ischaemic damage (Fig. 21.1). Adequate sampling must contain at least 25 glomeruli and 2 arteries.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Delay Graft Function
- Thrombotic Microangiopathy
- Acute Cellular Rejection
- Acute Interstitial Nephritis
- Glomerular Capillary
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Donor Biopsy
The Expanded Criteria Donor (ECD) recommends histological evaluation of the kidney not only for donors over 60 but also for donors over 50 with comorbidities (firstly hypertension) even in the setting of normal serum creatinine [1]. The histological parameters to be evaluated include glomerular, vascular, tubular and interstitial injury. However, no studies have provided an absolute threshold beyond which a donor kidney must not be used, and there is no consensus on the value of biopsies for predicting graft function. Histological evaluation of the donor biopsy can be performed at harvesting by on call pathological examination or by means of implantation biopsies. Tissue sample analysis of implantation biopsies includes the immunohistochemistry (IHC) evaluation of C4d to identify pre-sensitized patients and immunofluorescence to highlight misdiagnosed glomerular diseases. The biopsies can be obtained through a wedge resection or needle core biopsy: superficial sampling in wedge resections can overestimate the glomerular sclerosis and fibrosis because the outer cortex is more sensitive to ischaemic damage (Fig. 21.1). Adequate sampling must contain at least 25 glomeruli and 2 arteries.

A panoramic view of the donor biopsy stained with H&E (a), PAS (b) and trichrome stain (c) showing the ischaemic subcapsular area with inflammatory infiltrate, moderate fibrosis and obsolescent and sclerotic glomeruli. The punch biopsy can sometimes overestimate the real state of the kidney if the biopsy falls in such areas. Magnification 2×
The pathological report of the donor biopsy includes:
-
Glomerular disease
-
The percentage of sclerotic glomeruli. Glomerulosclerosis alone is not an independent predictor of graft function [2] even though glomerulosclerosis >10 % correlates with a major rate of delayed graft function (DGF), primary nonfunction and graft loss [3]. The degree of glomerulosclerosis can be a predictor of serum creatinine value at 12 months [4].
-
Any thrombotic microangiopathies (TMA) (Fig. 21.2). Glomerular fibrinoid thrombi can be dissolved by the graft recipient’s fibrinolytic system without any anticoagulant therapy. In one series, some recipients experienced a primary nonfunction, while others had an initial DGF without any impairment of graft function at 2 years [2, 5, 6].
-
Any glomerular disease, i.e. lupus nephritis or diabetic glomerulonephropathies (Fig. 21.3). These features do not enter into the Karpinski score. Some studies suggest that diabetic kidneys can be used safely and that early diabetic lesions can regress with transplantation. However, no guidelines are currently available on the use of diabetic kidneys [7–9].
Fig. 21.2 
At high magnification (PAS, 40×) the capillary lumen of the glomerulus is filled with a pale amorphous material extending into the vascular pole, occluding the lumen
Fig. 21.3 
The pictures (a, b) highlight the mesangial expansion with a nodular appearance. This feature does not enter into the Karpinski score. The biopsy in other fields showed just a mild interstitial and arterial intimal fibrosis without remarkable tubular atrophy. Magnification 40×, PAS
-
-
Vascular disease
-
Tubulointerstitial disease


At our centre all these parameters are evaluated according to the Karpinski score system [12].
Glomerular score | |
Score 0 | No globally sclerotic glomeruli |
Score1 | <20 % globally sclerotic glomeruli |
Score 2 | 20–50 % globally sclerotic glomeruli |
Score 3 | >50 % globally sclerotic glomeruli |
Tubular score | |
Score 0 | Absent |
Score 1 | <20 % of tubules affected |
Score 2 | 20–50 % of tubules affected |
Score 3 | >50 % of tubules affected |
Interstitial score | |
Score 0 | No evidence of fibrosis |
Score 1 | <20 % of cortical parenchyma replaced by fibrotic tissue |
Score 2 | 20–50 % of cortical parenchyma replaced by fibrotic tissue |
Score 3 | >50 % of cortical parenchyma replaced by fibrotic tissue |
Vascular score(arterial fibrosis and arteriolar hyalinosis are evaluated, but the most severe lesion determines the final score) | |
Score 0 | Absent |
Score 1 | Increase in wall thickness that is less than the diameter of the lumen |
Score 2 | Increase in wall thickness that is equal to the diameter of the lumen |
Score 3 | Increase in wall thickness that exceeds the diameter of the lumen |
1.1 Other Predictive Factors
-
Prediction of ischaemic injury effects
-
Neutrophils in glomerular capillaries
-
Endothelial loss of capillaries (correlated to a transiently impaired function)
-
Tubular degeneration: necrosis or apoptosis of tubular cells, regenerative features with enlargement of tubular cell nuclei and simplification and loss of the brush borders of distal tubular cells
-
Tubular CAST (precipitation of proteinaceous amorphous/detritic material in renal tubules)
-
Microvascular thrombi in capillaries and small arteries without granulocytes
-
-
Prediction of acute rejection
-
Neutrophils, macrophages and platelets in capillaries (glomerular and peritubular).
-
C4d deposition in peritubular capillaries may be predictive of acute antibody-mediated rejection (AMR).
-
-
Prediction of DGF
-
Thrombotic angiopathy in glomerular capillaries
-
2 Surgical Complications
2.1 Ureteral Obstruction/Leak/Reflux
The presentation is with oliguria, haematuria and elevated creatinine. At histology only non-specific alterations can be seen: interstitial inflammation, oedema and tubular injury.
2.2 Lymphocele
Lymphocele consists in a collection of lymphatic fluid in the perinephric space. At histological examination the renal biopsy shows changes related to obstruction, with interstitial oedema, dilatation of the collecting ducts and mild inflammation.
2.3 Arterial/Venous Thrombosis
The clinical presentation is of macrohaematuria and acute renal failure. At histology, microthrombi and loss of the endothelium can be seen together with haemorrhage of the cortex and mild neutrophils in capillaries. The most important differential diagnosis is with acute cellular rejection (ACR) and hyperacute or AMR. Imaging findings (US and angiography) and immunohistochemistry for C4d lead to the correct diagnosis.
2.4 Arterial Stenosis
The clinical presentation is of DGF, hypertension and renal dysfunction. The histological picture may disclose cholesterol emboli (if the stenosis is due to an atheromatous plaque). Non-specific tubular atrophy with fibrosis or acute tubular injury (if the stenosis is intermittent) is evident.
3 Rejection
3.1 Hyperacute Rejection
Nowadays the incidence of hyperacute rejection is very low due to improved pre-transplant testing for antibody against donor major antigens. The presentation is very rapid: from a few minutes (at the time of graft reperfusion) to a few days after transplantation, depending on the recipient’s titres of specific antibody against the donor antigens. Anuria, primary graft nonfunction, fever, lack of perfusion by imaging studies, thrombocytopenia and increased circulating fibrin split characterize the clinical onset. At gross examination the graft is cyanotic, flaccid, haemorrhagic and oedematous with necrotic areas. Thrombosis of the renal artery can be found.
3.1.1 Histological Examination
Early features (1–12 h):
-
1.
Platelet and neutrophil margination in glomerular and peritubular capillaries
-
2.
Vascular congestion with scattered thrombi in glomerular capillaries and small arteries
Late features (12–24 h) include:
-
1.
Interstitial oedema and haemorrhage
-
2.
Widespread thrombotic microangiopathy
-
3.
Fibrinoid arterial necrosis
-
4.
Parenchymal necrosis
3.1.2 Ancillary Techniques
-
1.
C4d peritubular capillaries and glomerular IHC staining.
-
2.
Negative staining does not exclude a hyperacute rejection since C4d-negative cases are possible (related to decreased perfusion or to insufficient time to produce the C4d molecule, a product of the activation of the classical complement pathway).
3.1.3 Differential Diagnoses
-
1.
Renal artery or vein thrombosis due to technical problems or hypercoagulable state (in these cases the thrombi are limited to the large vessels, and C4d staining is negative).
-
2.
Perfusion nephropathy with loss of the endothelium. In this case congestion and thrombotic microangiopathy can be found without C4d staining.
-
3.
Donor thrombotic microangiopathy.
3.2 Acute Humoral Rejection or Acute Antibody-Mediated Rejection
About 5–7 % of transplanted patients experienced an episode of antibody-mediated rejection (AMR) and a component of humoral rejection can be found in at least about 24 % of acute rejection cases. Presentation occurs from a few days to the first weeks after transplant, with anuria and acute renal failure. Circulating anti-donor-specific antibodies can be detected in about 90 % of recipients. At gross examination the graft is swollen, haemorrhagic and oedematous.
3.2.1 Histological Examination
-
Glomeruli
-
Tubules
-
Acute tubular injury represented by a simplification of tubular cells with loss of the brush border, ischaemic necrosis with loss of nuclei, thinning of the tubular cell cytoplasm and naked basal membranes
-
Tubulitis with neutrophil infiltrate
-
-
Peritubular capillaries: dilatation and congestion of capillaries filled with neutrophils and occasional microthrombi
-
Interstitium: oedema, occasionally haemorrhagic areas, inflammatory infiltrate predominantly with neutrophils
-
Vessels
-
Necrosis of the media with fragmentation of the lamina elastica and fibrinoid necrosis
-
Inflammatory cells within the vessel wall
-
Activation of capillary and artery endothelial cells showing plump cytoplasm and nuclear enlargement
-
3.2.2 Ancillary Techniques
-
IHC positivity for C4d along the peritubular and glomerular capillaries (Fig. 21.4). Early biopsies may not disclose C4d deposition, but this does not rule out a diagnosis of AMR since this may become positive in repeated biopsies taken after 1–3 days. Conversely, some studies have demonstrated that positive immunostaining for C4d in protocol biopsies appears before the clinical manifestation of an AMR episode [17].
Fig. 21.4 
Immunohistochemical stain for C4d shows a diffuse and continuous linear positivity in glomerular (a) and along peritubular capillaries (b). Magnification 20×
-
IHC staining for CD68 does not improve the sensitivity of identifying glomerulitis when the Banff 2013 definition is applied.
-
Wide and diffuse immunopositivity for C4d at immunofluorescence (IF), which is more sensitive than IHC.

3.2.3 Diagnostic Criteria (Banff Classification)
The definition of AMR has now been revised [15]: histological evidence of acute tissue injury (glomerulitis and/or peritubular capillary infiltration and/or acute thrombotic microangiopathy and/or tubular necrosis) (Fig. 21.5) must be present together with evidence of a recent endothelial/antibody reaction (positivity for C4d IHC and/or microvascular inflammation highlighted by glomerulitis or peritubular capillaritis) and serological evidence of anti-donor-specific antibodies.


In AMR there is a diffuse interstitial oedema highlighted by the pale light green trichrome stain (a magnification 4×), tubulitis with neutrophil infiltrate (b PAS, magnification 20×), activation of the endothelial cells (arrow, c H&E, magnification 40×) and acute tubular necrosis (d H&E, magnification 40×)
The histological pattern can be graded from grade 1 with acute tubular damage and minimal inflammatory infiltrate to grade 2 with peritubular capillaritis or glomerulitis with occasional microthrombi or grade 3 with fibrinoid arterial necrosis. The presence of only one or two of these criteria leads the pathologist to a diagnosis of “suspect” AMR (Fig. 21.6).

This is a biopsy 5 days after kidney transplantation in a patient with oliguria. The histological pictures (a PAS, magnification 40×) demonstrated only an acute tubular necrosis of the parenchyma with a mild peritubular capillaritis without any interstitial inflammatory infiltrate or tubulitis. The main differential diagnosis is with a tubular cell necrosis with a delayed graft function. The C4d stain (b magnification 40×) reveals a diffuse deposition of the molecule along the peritubular capillaries: the patient was given a steroid bolus before the biopsy because of the clinical suspicion of AMR
Biopsies with a C4d-positive immunostaining without any inflammation can be considered a kind of “accommodation”.
3.2.4 Differential Diagnoses
-
Acute cellular rejection: generally the infiltrate is composed predominantly of T lymphocytes. Fibrinoid necrosis of renal small arteries, glomerulitis, microvascular thrombosis and areas of infarction are less prominent [18].
-
Chronic humoral rejection: the clinical setting shows a slow decline.
-
Accommodation: C4d deposition in the absence of an inflammatory reaction.
-
Acute tubular injury/acute tubular necrosis: simplification of the renal tubules with loss of nuclei, thinning of tubular cell cytoplasm and naked basal membranes in the absence of an inflammatory reaction. C4d is negative.
-
Acute pyelonephritis: dirty casts in the tubules (composed of neutrophils and necrotic material) with a diffuse infiltrate of neutrophils in the parenchyma. A positive urine culture and C4d negativity favour the diagnosis.
-
Thrombotic microangiopathies: due to drug toxicity or recurrent disease. There is no C4d immunoreactivity.
3.3 Acute Cellular Rejection or T-Cell-Mediated Rejection
Acute cellular rejection (ACR) involves 5–10 % of kidney recipients in the first year posttransplant, generally in the first few weeks. The frequency tends to decline after the first 6 months, but ACR can arise at any time in the recipient. In acute renal failure increased serum creatinine concentration, decline in urine output and oliguria, weight gain, fever and malaise define the clinical picture. Circulating anti-donor-specific antibodies can be detected in about 90 % of recipients. At US the graft becomes enlarged, oedematous and tender. At gross examination the graft is swollen, pale, haemorrhagic with congestion of the medulla, and oedematous. Foci of infarction may be evident on the cortex.
3.3.1 Histological Examination
-
Glomeruli
-
Only occasional mild inflammatory infiltrate of mononuclear cells (generally in only 10 % of cases) in glomeruli with mild reactive swelling in endothelial cells (Fig. 21.7a).
-
In <5 % of cases a severe mononuclear cell glomerular infiltrate (acute allograft glomerulopathy) can be found, giving the appearance of endocapillary hypercellularity. Endothelial injury with areas of mesangiolysis is associated. This picture is often seen in the setting of moderate ACR with endoarteritis, but it can also represent the only histological feature of rejection.
Fig. 21.7 
The picture on the left (a PAS, magnification 40×) shows a mild inflammatory infiltrate of mononuclear cells in the glomerulus, while the picture on the right (b PAS, magnification 40×) shows marked tubulitis: note the lymphocytes between the tubular epithelium and the basement membrane and the moderate interstitial oedema
-
-
Tubules
-
Tubulitis with T-cell lymphocytes (CD8+) (Fig. 21.7b)
-
Tubular cell injury, occasionally with a granulomatous reaction
-
-
Interstitium
-
Oedema, occasionally with haemorrhagic areas.
-
Chronic inflammatory infiltrate (involving at least 25 % of the cortex) with a predominance of T-cell lymphocytes and macrophages (Fig. 21.8). Macrophages/monocytes can be the major cell type, notably in the setting of T-cell-depleting drugs (such as CAMPATH 1).
-
A plasma cell-rich subset and a CD20+ B-cell-rich subset AR have a worse prognosis.
Fig. 21.8 
The picture on the left (a PAS, magnification 20×) shows a chronic inflammatory infiltrate: the double immunostaining for T lymphocytes CD4/CD8 (b magnification 20×) shows that the tubulitis is caused by CD8+ T-cell lymphocytes (in red) and that the CD4+ T-cell lymphocytes (in brown) are localized predominantly in perivascular and interstitial sites
-
-
Peritubular capillaries: dilatation and mononuclear cell infiltrate
-
Vessels
-
T cells within the lumen of small arteries (endarteritis) with endothelial injury.
-
Activation of endothelial cells of capillaries and arteries.
-
In severe cases the inflammatory infiltrate is transmural with myocyte necrosis (Fig. 21.9).
Fig. 21.9 
A case of ACR type 3 with transmural arterial inflammation and fibrinoid necrosis (PAS, magnification 40×)
-



3.3.2 Ancillary Techniques
-
Immunostaining for C4d is negative. C4d positivity can highlight a concomitant AHR component.
3.3.3 Grading According to Banff Classification [16]
-
1.
ACR type 1 or tubulointerstitial. inflammatory infiltrate in at least 25 % of the cortex together with foci of moderate tubulitis (1A) or severe tubulitis (1B).
-
2.
ACR type 2 with endarteritis. It is then subdivided into 2A when the infiltrate affects <25 % of the luminal areas and 2B when the infiltrate affects ≥25 % of the luminal areas.
-
3.
ACR type 3 with transmural arterial inflammation associated with myocyte foci and fibrinoid necrosis.
-
4.
Suspicious/borderline for ACR. Inflammatory infiltrate in <20 % of the cortex associated with mild tubulitis.
3.3.4 Differential Diagnoses
-
Polyomavirus infection (BK): typically BK shows a more evident plasma cell infiltrate with tubular cell intranuclear viral inclusions, also detectable in the urine and with IHC on biopsy.
-
Cytomegalovirus infection: tubular cell intranuclear viral inclusions detectable with IHC on biopsy.
-
Pyelonephritis: a neutrophil infiltrate with dirty tubular casts; the infection can be confirmed by a positive urine culture.
-
Posttransplant lymphoproliferative disease (PTLD): monotonous infiltrate of B lymphocytes. Tubulitis and endarteritis can be present. The in situ hybridization for EBV-RNA is diagnostic.
-
Drug-induced tubulointerstitial nephritis: an eosinophilic-rich infiltrate is evident, sometimes infiltrating tubular cells.
-
Thrombotic microangiopathy (TMA): endoluminal thrombi in small arteries in the absence of endarteritis. Mucoid intimal thickening with progressive luminal obstruction appears.
3.4 Chronic Rejection
Ten years after transplantation, about 20 % of patients lose their grafts due to CR, defined as a progressive loss of the graft due to a continuous humoral or cellular immunological reaction against the donor antigens. Clinical presentation is characterized by progressive renal failure, proteinuria and hypertension.
Depending on the kind of immunological mechanism involved, CR can be distinguished in:
-
Chronic humoral rejection (CHR) or chronic antibody-mediated rejection
-
Chronic cellular rejection (CCR)
3.5 Chronic Humoral Rejection
The diagnosis of CHR has been revised as a category of AMR (see above) according to Banff 2013. This diagnosis requires the histological picture, evidence of an endothelial/antibody reaction (defined by the C4d IHC positivity and/or microvascular inflammation) and serological evidence of anti-donor-specific antibodies.
3.5.1 Histological Examination
-
Glomeruli
-
Transplant glomerulopathy (or chronic glomerulopathy, CG) (Fig. 21.10a) defined as duplication of the glomerular basement membrane (BM) (railway track) identified in at least one glomerular capillary loop (revised according to Banff 2013) [15]. The definition of CG 1a was introduced when the double contour is detectable only at electron microscopy and CG1b when the double contour is also evident at histology.
-
Glomerulitis with prevalent monocyte/mononuclear cells (CD68+) (Fig. 21.10b).
-
Possible mesangial expansion and sclerosis.
Fig. 21.10 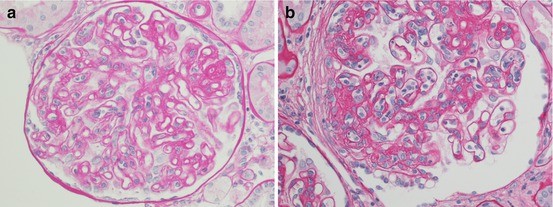
On the left (a) a moderate/severe case of transplant glomerulopathy with duplication of the basement membrane of the glomerular capillary tuft (PAS, magnification 40×). On the right (b) a case of glomerulitis associated with moderate mesangial expansion together with a thickening of the glomerular basement membrane (PAS, magnification 40×)
-
-
Tubules
-
Atrophic tubules with occasional thickening of the basement membrane with duplication (Fig. 21.11)
Fig. 21.11 
The picture (a PAS, magnification 4×; b trichrome stain, magnification 4×) demonstrates a mild chronic inflammatory infiltrate with diffuse tubular atrophy and totally sclerotic glomeruli. There is also severe chronic vascular damage
-
-
Interstitium
-
Fibrosis
-
Mild chronic inflammatory infiltrate
-
-
Peritubular capillaries
-
Dilatation and mononuclear cell infiltrate (peritubular capillaries)
-
Duplication of the BM, generally best seen by electron microscopy
-
-
Arteries
-
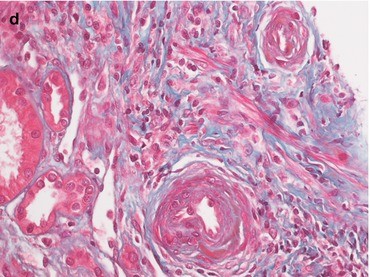
Fibrous intimal thickening with luminal narrowing, incorporating T lymphocytes and macrophages (transplant arteriopathy or chronic allograft arteriopathy). The intima shows concentric thickening without multilayering of the lamina elastica (characterizing vascular hypertensive damage): at the beginning a loose matrix is evident, becoming more fibrotic as it evolves into an “onionskin” appearance (Fig. 21.12). The media generally shows no marked alteration.
Fig. 21.12 
The intima shows concentric thickening creating an “onionskin” appearance without any particular alteration of the media. (a) PAS, 20×; (b) trichrome stain, 20×
-



3.5.2 Ancillary Techniques
-
Evidence of C4d deposition along peritubular and glomerular capillaries
3.5.3 Differential Diagnoses (Transplant Glomerulopathy)
-
Chronic thrombotic microangiopathy associated with calcineurin inhibitor toxicity or a history of haemolytic uraemic syndrome. The absence of intracapillary fibrin thrombosis with necrosis, the anamnesis and other signs of immunosuppressive drug toxicity may help in the diagnosis.
-
Immune complex glomerulonephritis recurrent or de novo. This diagnosis requires a positive IF pattern and the typical immunocomplex at electron microscopy. The anamnesis is helpful.
3.5.4 Differential Diagnoses (Transplant Arteriopathy)
-
Arteriosclerosis. Elastic fibre accumulation and thickening of the media in the absence of an inflammatory infiltrate in the vessel wall are more typical of a hypertensive injury. Evaluation of the donor biopsy can help distinguish lesions already present in the kidney prior to transplantation. Notably arteriosclerosis may coexist with transplant arteriopathy.
-
Chronic thrombotic microangiopathy. The disease typically affects the smaller arteries, in contrast to rejection that is more evident in medium-sized vessels.
3.5.5 Differential Diagnoses (Tubulointerstitial Lesions)
-
Calcineurin inhibitor toxicity associated with other signs of immunosuppressive drug toxicity such as nodular arteriolar hyalinosis.
-
Chronic obstruction leads to an interstitial fibrosis with tubular atrophy in the absence of a diffuse inflammatory mononuclear infiltrate.
3.6 Chronic Cellular Rejection
3.6.1 Histological Examination
-
Glomeruli
-
Global glomerulosclerosis
-
Focal/segmental sclerosis with adhesions
-
-
Tubules
-
Tubulitis and atrophic tubules
-
-
Interstitium
-
Fibrosis
-
Mononuclear inflammatory infiltrate meeting the criteria of ACR
-
-
Arteries
-
The same alterations as for CHR
-
3.6.2 Ancillary Techniques
-
There is no evidence of C4d deposition along peritubular and glomerular capillaries.
3.6.3 Differential Diagnoses
-
CHR. This situation presents transplant glomerulopathy and multi-lamination of the basement membrane of peritubular capillaries and tubules together with C4d positivity.
-
Calcineurin inhibitor toxicity. See below.
-
Hypertensive arteriosclerosis. See below.
4 Calcineurin Inhibitor Toxicity
4.1 Histological Examination
-
Tubules. The most common tubular alteration is the so-called isometric vacuolization of the cytoplasm, found more frequently in the proximal tubules and sometimes associated with a loss of tubular cell brush borders (Fig. 21.13a, b). The lesion is reversible with dose reduction. Other alterations include giant mitochondria and dystrophic microcalcification.
Fig. 21.13 
The picture presents the classical tubular “isometric vacuolization” of the cytoplasm (a PAS, magnification 40×; b trichrome stain, magnification 40×) and arteriolar hyalinosis (c PAS, magnification 40×; d trichrome stain, magnification 40×)
-
Arterioles and arteries. Commonly the alterations are present in the arterioles; when very diffuse they can also be found at the vascular pole of the glomeruli. The early lesion is a marked swelling of the muscular cells of the media with clearing of the cytoplasm that evolves into a diffuse hyalinosis (nodular accumulation of hyaline material along the media replacing the necrotic smooth muscle cells of the media) (Fig. 21.13c, d). This lesion can be found within a few days after transplant, and a cumulative use of the drug can induce arteriolopathies in close to 100 % of allografts after 10 years [19]. In the most severe cases, calcineurin toxicity can induce a TMA with fibrin thrombi in capillaries and mucoid intimal thickening with oedematous swelling of the arterioles that evolves into a sclera-fibrotic lesion with an “onionskin” appearance.
The Banff 1997 scheme, adapted by Mihatsch, is used to score calcineurin inhibitor hyaline arteriolopathies [20].
-
Glomeruli. The glomeruli can be affected as a direct effect of the calcineurin inhibitor or as a consequence of vascular damage: the end point, however, is sclerosis. Sometimes glomerular basement membrane duplication can be found but only focally and segmentally, together with mesangial expansion (the so-called calcineurin inhibitor glomerulopathy that enters the differential diagnosis with the “transplant glomerulopathy”).
Focal segmental glomerulosclerosis, the collapsing variant, is another glomerular lesion that can be an expression of drug damage.
-
Interstitium. Typically there is a sparse and mild inflammatory infiltrate, with a “striped” fibrosis. In acute toxicity mild oedema can occasionally be found.


4.1.1 Differential Diagnoses
-
Tubules. Tubular cell vacuolization can also be found in osmotic nephrosis following therapy with plasma cell expanders, radiolabelled contrast media or intravenous immunoglobulin solution. Giant mitochondria are also found in cases of ischaemic damage, and dystrophic calcification can be the consequence of marked acute tubular necrosis (as ischaemic/reperfusion damage).
-
Arterioles and arteries. Hypertension and metabolic changes such as diabetes mellitus can induce arteriolar hyalinosis. In hypertension damage the hyaline deposits are subendothelial (and not in the media of the vascular wall) with an intact or atrophic appearance of the muscle cells of the media. Diabetes mellitus injury, however, is histologically similar to that of calcineurin inhibitors.
-
Glomeruli. A partially duplicated basement membrane in the glomeruli involves three major differential diagnoses:
-
1.
A late phase of a TMA not induced by a calcineurin inhibitor (e.g. a recurrence of the recipient disease or a de novo TMA caused by other drugs): this condition has to be considered in the correct clinical setting.
-
2.
Membranoproliferative glomerulonephritis (de novo or recurrent): this situation has to be confirmed by typical IF and electron microscopic examination.
-
3.
Transplant glomerulopathy in the setting of chronic rejection.
-
1.
5 Posttransplant Lymphoproliferative Disorder
5.1 Epidemiology
PTLD is one of the most common posttransplant malignancies (>90 %), representing the most common posttransplant cancer in children and the second most common malignancy after skin cancer in adults. The incidence of PTLD in renal transplant recipients is 1 %, and the renal allograft is affected in >30 % of cases [21, 22].
5.1.1 Clinical Features
-
Fever.
-
Lymphadenopathy.
-
Extranodal involvement occurs in more than two thirds of cases and may also involve the allograft. The central nervous system is frequently involved (in up to 30 % of cases) and can be the only site of disease.
5.1.2 Macroscopic Examination
In section, the kidney surface presents a bloated and blurred corticomedullary junction, diffuse petechiae and vaguely nodular involvement.
5.1.3 Histological Examination
The 2008 World Health Organization (WHO) [23] classification system recognizes four major histopathological subtypes of PTLD:
-
1.
Early hyperplastic lesions
-
2.
Polymorphic lesions (polyclonal or monoclonal)
-
3.
Monomorphic lesions (B, T, NK)
-
4.
Classic Hodgkin-type lymphomas:
5.1.3.1 Plasmacytic Hyperplasia (PH) and Infectious Mononucleosis-like PTLD
This entity usually occurs in young patients and appears as a mononucleosis-type acute infectious illness characterized by polyclonal B-cell proliferation with no evidence of malignant transformation: the lymphoid follicles are floridly reactive or hyperplastic. In these cases EBV infection can often be demonstrated.
5.1.3.2 Polymorphic PTLD
This entity can have polyclonal or monoclonal lymphoid infiltrates with evidence of malignant transformation but does not fulfil all the criteria for typical B-cell or T-/NK-cell lymphomas. At histology, there is an effacement of the underlying tissue with a mixed infiltrate: immunoblasts, plasma cells and small–intermediate-sized lymphoid cells. Areas of geographic necrosis may be present with a high mitotic rate and nuclear atypia; EBV infection can often be demonstrated.
5.1.3.3 Monomorphic PTLD
This is a monoclonal lymphoid proliferation meeting the criteria for one of the B-cell or T-/NK-cell lymphomas recognized in immunocompetent patients. Burkitt lymphoma (BL) or plasma cell neoplasms occur less frequently. The WHO 2008 does not include small B-cell lymphoid neoplasms (e.g. follicular lymphomas, small lymphocytic lymphoma) and marginal zone (MALT) lymphomas arising in the posttransplant setting among the PTLD. At histological examination destruction of the underlying parenchyma is evident, and the lymphoid infiltrate shows malignant cytological features.
5.1.3.4 Classic Hodgkin-Type Lymphomas
This rare form of PTLD shows the histology of classic Hodgkin lymphoma and can be seen as a late complication of transplantation. Biopsy shows Reed-Sternberg cells and variants on a mixed background of small lymphocytes, histiocytes and eosinophils.
5.1.4 Differential Diagnoses
-
Rejection. Tubulitis and endarteritis may be present. Rejection shows a predominance of T lymphocytes and macrophages; negativity for EBER-1 in situ hybridization for EBV provides further assurance that the cases classified as acute rejection did not have complicating PTLD lesions.
-
Inflammatory or infectious conditions.
-
EBV-positive spindle-cell neoplasms.
-
6 Infection
Over 50 % of transplant patients have at least one infection in the first year following transplantation [24], and the risk of contracting any specific infection changes according to the posttransplant period. Within the first month the weakening effects of immunosuppression have not been completely realized, and more than 90 % of infections are caused by bacterial or fungal agents. Conversely, from 1 to 6 months after transplantation, viruses are the most frequent cause of infections [25].
6.1 CMV Infection
Cytomegalovirus (CMV) remains one of the most important pathogens and results in a significant morbidity and mortality in kidney transplant recipients. About 20–60 % of patients develop symptomatic CMV infection [26], which may increase the incidence of infections, acute rejection, chronic allograft nephropathy and chronic vascular injury with adverse effects on the long-term outcome of both the patient and allograft [27].
6.1.1 Histological Examination
-
1.
Large intranuclear inclusions in tubular epithelial cells (rare in endothelial cells) with variable degrees of interstitial inflammation
-
2.
Large eosinophilic intranuclear inclusions in endothelial cells; thrombotic microangiopathy
-
3.
Acute glomerulonephritis (rare): endocapillary hypercellularity, crescents and inclusions in glomerular endothelial cells
6.1.2 Differential Diagnoses
-
Polyomavirus nephropathy: see below.
-
Adenovirus tubulointerstitial nephritis: tubular necrosis, granulomatous inflammation.
-
ACR: tubulitis, interstitial inflammation and endarteritis.
-
Acute allograft glomerulopathy: mesangiolysis, C4d-negative immunohistochemistry and no virus inclusion.
-
Acute glomerulonephritis: glomerular immune complexes evident with IF.
6.2 Polyomavirus (BKV) Infection
BKV is a ubiquitous double-stranded DNA virus representing a major pathogen in kidney transplantation. The clinical presentation is variable: from completely asymptomatic to allograft dysfunction and graft loss. BKV nephropathy may precede or follow a treatment for acute rejection [28]. Screening for decoy cells in the urine is a useful tool, but diagnosis of BKV nephropathy requires identification of the virus in kidney tissue by either IHC or electron microscopy. PCR quantification of viraemia appears to correlate with the likelihood of BKV nephropathy and serves as a guide in monitoring response to therapy.
6.2.1 Histological Examination
-
Interstitial mononuclear inflammation (Fig. 21.14)
Fig. 21.14 
H&E (magnification 4×) shows a diffuse inflammatory interstitial infiltrate
-
Nuclear inclusions in tubular epithelium (confirmed by IHC) (Figs. 21.15 and 21.16)
Fig. 21.15 
Light microscopy at high power (H&E, magnification 40×) shows the typical cytopathic viral changes of the tubular cells. The images (a, b) show two of the four typical nuclear alterations: ground-glass intranuclear inclusions and the nuclear vesicular changes with irregular chromatin and occasional nucleoli
Fig. 21.16 
H&E on the left (a, magnification 20×) shows the typical tubular nuclear alteration of the infection: a positive SV40 immunohistochemistry (b, on the right, magnification 20×) confirms the diagnosis
-
Tubulitis
-
Immune complex deposition



6.2.2 Differential Diagnoses
-
Acute tubular interstitial rejection (type 1): tubulitis with interstitial inflammation
-
Adenovirus tubular necrosis: prominent interstitial inflammation
-
Acute tubular necrosis: reactive atypia of tubular epithelial cells
-
Acute interstitial nephritis: marked interstitial inflammation, no intranuclear inclusion
6.3 Adenovirus Infections
Adenoviruses (AdV) are emerging pathogens in solid organ transplant recipients with clinical manifestations ranging from subclinical infection to fatal outcome. The reported prevalence of AdV infection during the first year after kidney transplant is about 11 % by urine culture and 6.5 % by serum PCR [29]. Renal allograft involvement is rare, and the infection has a broad range of histological manifestations: tubular cell necrosis with cytopathic viral effects together with interstitial inflammation without glomerular or vascular involvement or as necrotizing tubulointerstitial nephritis and space-occupying lesions with or without ureteral obstruction [30]. The common differential diagnoses include BK- and CMV-mediated interstitial nephritis.
6.3.1 Histological Examination
Severe necrotizing granulomatous lesions with predominant neutrophilic inflammation can be considered characteristic for AdV infection. Additional features that are more pronounced in AdV interstitial nephritis include mixed cellular infiltration with macrophages and histiocytes and tubular basement membrane disruption.
6.3.2 Differential Diagnoses
The presence of granulomatous interstitial nephritis enters the differential diagnosis with mycobacterial, fungal (histoplasmosis, Cryptococcus species and Candida albicans) and viral (adenovirus, HIV, CMV and BKV) infections. Granulomas around tubules represent a useful feature pointing to adenovirus. The virus can be confirmed using in situ hybridization studies. Other differential diagnoses are drug-induced nephritis, antineutrophil cytoplasmic autoantibody-associated vasculitis and sarcoidosis. Rarely, AdV and cellular rejection may coexist and pose a diagnostic challenge. In such conditions, overriding tubulitis, vasculitis and predominant T-lymphocyte infiltration should favour the diagnosis of rejection.
7 Drug-Induced Acute Interstitial Nephritis
Myriad drugs have been implicated in causing acute interstitial nephritis (AIN). Drugs are more often recognized as aetiologic factors in AIN because of the increased frequency in using drugs, the increased use of renal biopsy and the typical clinical presentation [31]. Some classes of medication are often associated with certain clinical features of AIN. The development of drug-induced AIN is not dose related and may become clinically evident from 2 weeks or longer after starting medical therapy.
7.1 Histological Examination
The hallmark of AIN is an interstitial inflammatory infiltrate with oedema, sparing the glomeruli and blood vessels. Interstitial fibrosis is mild and develops later in the disease. The inflammatory infiltrate is composed of mononuclear cells and T lymphocytes, with a variable number of plasma cells and eosinophils. Eosinophils may be totally absent from the infiltrate or may concentrate in small foci, forming eosinophilic microabscesses. In chronic interstitial nephritis, the cellular infiltrate is largely replaced by interstitial fibrosis.
8 De Novo or Recurrent Glomerular Disease
A glomerular disease is deemed de novo when the allograft develops a disease different from that of the native kidney. It is important to know exactly the cause that led to end-stage renal failure to exclude a recurrent disease. De novo or recurrent glomerular disease has the same histological features and IF pattern as those of the native kidney.
References
Haas M. Donor kidney biopsies: pathology matters, and so does the pathologist. Kidney Int. 2014;85:1016–9.
Pokorná E, Vítko S, Chadimová M, Schück O, Ekberg H. Proportion of glomerulosclerosis in procurement wedge renal biopsy cannot alone discriminate for acceptance of marginal donors. Transplantation. 2000;69:36–43.
Mizuiri S, Shigetomi Y, Sugiyama K, Miyagi M, Hatano T, Tajima E, Aikawa A, Ohara T, Kawamura S, Hasegawa A. Successful transplantation of a cadaveric kidney with post-infectious glomerulonephritis. Pediatr Transplant. 2000;4:56–9.
Randhawa PS, Minervini MI, Lombardero M, Duquesnoy R, Fung J, Shapiro R, Jordan M, Vivas C, Scantlebury V, Demetris A. Biopsy of marginal donor kidneys: correlation of histologic findings with graft dysfunction. Transplantation. 2000;69:1352–7.
McCall SJ, Tuttle-Newhall JE, Howell DN, Fields TA. Prognostic significance of microvascular thrombosis in donor kidney allograft biopsies. Transplantation. 2003;75:1847–52.
Bennett WM, Hansen KS, Houghton DC, McEvoy KM. Disseminated intravascular coagulation (DIC) in a kidney donor associated with transient recipient DIC. Am J Transplant. 2005;5:412–4.
Alexander JW. High-risk donors: diabetics, the elderly, and others. Transplant Proc. 1992;24:2221–2.
Ojo AO, Leichtman AB, Punch JD, Hanson JA, Dickinson DM, Wolfe RA, Port FK, Agodoa LY. Impact of pre-existing donor hypertension and diabetes mellitus on cadaveric renal transplant outcomes. Am J Kidney Dis. 2000;36:153–9.
Becker YT, Leverson GE, D’Alessandro AM, Sollinger HW, Becker BN. Diabetic kidneys can safely expand the donor pool. Transplantation. 2002;74:141–5.
Taub HC, Greenstein SM, Lerner SE, Schechner R, Tellis VA. Reassessment of the value of post-vascularization biopsy performed at renal transplantation: the effects of arteriosclerosis. J Urol. 1994;151:575–7.
Oda A, Morozumi K, Uchida K. Histological factors of 1-h biopsy influencing the delayed renal function and outcome in cadaveric renal allografts. Clin Transplant. 1999;13 Suppl 1:6–12.
Karpinski J, Lajoie G, Cattran D, Fenton S, Zaltzman J, Cardella C, Cole E. Outcome of kidney transplantation from high-risk donors is determined by both structure and function. Transplantation. 1999;67:1162–7.
Pliquett RU, Asbe-Vollkopf A, Scheuermann EH, Gröne E, Probst M, Geiger H, Hauser IA. Cholesterol-crystal embolism presenting with delayed graft function and impaired long-term function in renal transplant recipients: two case reports. J Med Case Rep. 2009;3:6839. doi:10.1186/1752-1947-3-6839.
Remuzzi G, Cravedi P, Perna A, Dimitrov BD, Turturro M, Locatelli G, Rigotti P, Baldan N, Beatini M, Valente U, Scalamogna M, Ruggenenti P, Dual Kidney Transplant Group. Long-term outcome of renal transplantation from older donors. N Engl J Med. 2006;354:343–52.
Haas M, Sis B, Racusen LC, Solez K, Glotz D, Colvin RB, Castro MC, David DS, David-Neto E, Bagnasco SM, Cendales LC, Cornell LD, Demetris AJ, Drachenberg CB, Farver CF, Farris 3rd AB, Gibson IW, Kraus E, Liapis H, Loupy A, Nickeleit V, Randhawa P, Rodriguez ER, Rush D, Smith RN, Tan CD, Wallace WD, Mengel M. Banff meeting report writing committee. Banff 2013 meeting report: inclusion of c4d-negative antibody-mediated rejection and antibody-associated arterial lesions. Am J Transplant. 2014;14:272–83. doi:10.1111/ajt.12590.
Sis B, Mengel M, Haas M, Colvin RB, Halloran PF, Racusen LC, Solez K, Baldwin 3rd WM, Bracamonte ER, Broecker V, Cosio F, Demetris AJ, Drachenberg C, Einecke G, Gloor J, Glotz D, Kraus E, Legendre C, Liapis H, Mannon RB, Nankivell BJ, Nickeleit V, Papadimitriou JC, Randhawa P, Regele H, Renaudin K, Rodriguez ER, Seron D, Seshan S, Suthanthiran M, Wasowska BA, Zachary A, Zeevi A. Banff’09 meeting report: antibody mediated graft deterioration and implementation of Banff working groups. Am J Transplant. 2010;10:464–71. doi:10.1111/j.1600-6143.2009.02987.x.
Haas M, Ratner LE, Montgomery RA. C4d staining of perioperative renal transplant biopsies. Transplantation. 2002;74:711–7.
Jennette JC, Heptinstall RH. Heptinstall’s pathology of the kidney. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.
Nankivell BJ, Borrows RJ, Fung CL, O’Connell PJ, Chapman JR, Allen RD. Calcineurin inhibitor nephrotoxicity: longitudinal assessment by protocol histology. Transplantation. 2004;78:557–65.
Sis B, Dadras F, Khoshjou F, Cockfield S, Mihatsch MJ, Solez K. Reproducibility studies on arteriolar hyaline thickening scoring in calcineurin inhibitor-treated renal allograft recipients. Am J Transplant. 2006;6:1444–50.
Boubenider S, Hiesse C, Goupy C, Kriaa F, Marchand S, Charpentier B. Incidence and consequences of post-transplantation lymphoproliferative disorders. J Nephrol. 1997;10:136–45.
Feng S, Buell JF, Chari RS, DiMaio JM, Hanto DW. Tumors and transplantation: the 2003 third annual ASTS state-of-the-art winter symposium. Am J Transplant. 2003;3:1481–7.
WHO. Classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon: IARC Press; 2008.
Rungta R, Ray DS, Das P, Gupta S. Three different opportunistic infections in the same renal allograft recipient at the same time: unusual case report. Trop J Med Res. 2014;17:45–7.
Weikert BC, Blumberg EA. Viral infection after renal transplantation: surveillance and management. Clin J Am Soc Nephrol. 2008;3 Suppl 2:S76–86. doi:10.2215/CJN.02900707.
Brennan DC. Cytomegalovirus in renal transplantation. J Am Soc Nephrol. 2001;12:848–55.
Freeman Jr RB. The ‘indirect’ effects of cytomegalovirus infection. Am J Transplant. 2009;9:2453–8. doi:10.1111/j.1600-6143.2009.02824.x.
Hariharan S. BK virus nephritis after renal transplantation. Kidney Int. 2006;69:655–62.
Parasuraman R, Zhang PL, Samarapungavan D, Rocher L, Koffron A. Severe necrotizing adenovirus tubulointerstitial nephritis in a kidney transplant recipient. Case Rep Transplant. 2013;2013:969186. doi:10.1155/2013/969186.
Florescu MC, Miles CD, Florescu DF. What do we know about adenovirus in renal transplantation? Nephrol Dial Transplant. 2013;28:2003–10. doi:10.1093/ndt/gft036.
Raghavan R, Eknoyan G. Acute interstitial nephritis – a reappraisal and update. Clin Nephrol. 2014;82:149–62.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Malvi, D., Rosini, F., D’Errico, A. (2015). Kidney. In: Pinna, A., Ercolani, G. (eds) Abdominal Solid Organ Transplantation. Springer, Cham. https://doi.org/10.1007/978-3-319-16997-2_21
Download citation
DOI: https://doi.org/10.1007/978-3-319-16997-2_21
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-16996-5
Online ISBN: 978-3-319-16997-2
eBook Packages: MedicineMedicine (R0)