
Abstract
Hypertension impacts the vasculature through the mechanical effects of blood pressure and shear stress, as well as those of hormonal systems such as the renin-angiotensin-aldosterone system, endothelin, catecholamines, substances produced in perivascular fat, and inflammatory and immune mediators such as lymphocytes and macrophages and their products. The vascular phenotype of hypertension varies according to the age of subjects. In younger individuals with elevated blood pressure, vascular remodeling occurs in small arteries and arterioles and is eutrophic with reduced lumen diameter and unchanged media cross-sectional area, reduced or enhanced stiffness, and increased extracellular matrix deposition and endothelial dysfunction. In severe or long-standing hypertension and in secondary forms and refractory hypertension, hypertrophic vascular remodeling of small arteries and arterioles is more typically found. In subjects older than 50 years of age, vascular changes are increasingly found in aorta, which becomes stiffer as arteriosclerosis develops, resulting in increased pulse pressure. Enhanced pulsatility may injure small arteries and arterioles, leading to remodeling of these and endothelial dysfunction. Arteriolar and capillary rarefaction promotes tissue underperfusion that contributes to myocardial ischemia and cardiovascular events, heart failure, stroke, nephrosclerosis and chronic kidney disease, and peripheral vascular disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Vascular remodeling
- Hypertrophic remodeling
- Eutrophic remodeling
- Media-to-lumen ratio
- Endothelial dysfunction
- Renin-angiotensin system
- Angiotensin II
- Aldosterone
- Endothelin-1
- Vascular inflammation
- T lymphocytes
1 Introduction
Blood pressure load and numerous hormonal and locally acting agents mediate vascular damage associated with elevated blood pressure, leading to the complications of hypertension that include stroke, myocardial infarction as a consequence of accelerated atherosclerosis [1], heart failure, and chronic kidney disease, the latter resulting from nephroangiosclerosis. Increased peripheral resistance as a result of changes in small arteries and arterioles has been classically presented as the mechanism for blood pressure elevation in essential hypertension. However, this occurs primarily in younger individuals. In older people, especially after age 50–60, aging and cardiovascular risk factors contribute to stiffen the wall of large arteries such as the aorta and other elastic vessels, which leads to elevated systolic blood pressure.
2 Mechanisms of Remodeling of the Vasculature
Chronically elevated blood pressure initiates a number of complex signal transduction cascades that lead to remodeling of the vasculature [2]. A critical regulator of vascular tone is the endothelium [3], which becomes dysfunctional in people with high blood pressure. As a result, vasodilation is diminished, and in addition, there develops a pro-inflammatory and prothrombotic state. Endothelial dysfunction is a key early determinant of progression of atherosclerosis and is independently associated with increased cardiovascular risk [4]. Low-grade inflammation localized in the vascular wall and perivascular fat also contributes to the mechanisms of hypertension [5] and participates in the initiation and progression of atherosclerosis [6, 7] (see Chap. 3).
Activation of the renin-angiotensin-aldosterone system (RAAS) plays a significant role in the pathophysiology of hypertension [2, 8]. Angiotensin (Ang) II, one of the final products and major mediators of the RAAS, induces vascular remodeling and injury by several mechanisms including vasoconstriction, cell growth, oxidative stress, and inflammation. Ang II induces hyperplasia and hypertrophy of vascular smooth muscle cells (VSMCs) of resistance arteries of patients with essential hypertension and small arteries from hypertensive rats. Ang II and aldosterone, as well as endothelin-1 (ET-1) produced by the endothelium, enhance reactive oxygen species (ROS) generation by stimulating reduced nicotinamide adenine dinucleotide phosphate (NADPH) oxidase and expression of its subunits by pathways that involve c-Src, protein kinase C, phospholipase A2, and phospholipase D. NADPH oxidase is indeed the major source of ROS in the vascular wall and is expressed in endothelial cells, VSMCs, fibroblasts, and monocytes/macrophages [9–11], although uncoupled nitric oxide (NO) synthase, xanthine oxidase, myeloperoxidase, cytochrome P450 enzymes, and mitochondria are also involved in generating vascular oxidative stress. Increased ROS generation induced by Ang II, aldosterone, and ET-1 contributes to vascular remodeling through VSMC proliferation and hypertrophy and collagen deposition and by modulating cytokine release and pro-inflammatory transcription factors such as NF-κB, as well as by reducing the bioavailability of NO.
Aldosterone increases as well as tissue angiotensin-converting enzyme activity is enhanced [12] and upregulates angiotensin receptors [13], thus potentiating effects of other components of the RAAS. Indeed, aldosterone and other mineralocorticoids affect blood vessels in the heart and kidneys by inducing oxidative stress and impairing endothelial function [13], which can be blunted by mineralocorticoid antagonism. Some of aldosterone’s actions may be mediated by stimulation of endothelial production of ET-1 [14].
Ang II, aldosterone, and ET-1 trigger endothelial dysfunction and vascular inflammation by inducing oxidative stress, which upregulates inflammatory mediators in the endothelium and stimulates immune cells such as T effector lymphocytes [15]. Ang II and aldosterone as well as ET-1 stimulate fibrosis via TGF beta. Vasoconstriction induced by Ang II thus becomes embedded in the enhanced collagen deposited in the vascular wall [1, 2, 16]. Collagen I and III mRNA and collagen protein synthesis by fibroblasts are increased in vessels from essential hypertensive patients [17], contributing to thickening of the media in hypertrophic remodeling and reorganization of components of the vascular wall in eutrophic remodeling [18–21]. Reduction in the activity of matrix metalloproteinases (MMPs) may also participate in the stiffening of the vascular wall as collagen and other extracellular matrix components are not degraded and consequently collagen type IV and V and fibronectin accumulate in resistance arteries [22]. MMP-1 and MMP-3 activity is reduced in SHR before hypertension is established [23]. In hypertensive patients with increased vascular type I collagen, serum concentrations of MMP-1 are reduced [24]. Ang II stimulates hyperplasia and hypertrophy of VSMCs [25, 26]. Other processes participating in remodeling of blood vessels include apoptosis, cell elongation, reorganization, and inflammation [25–29]. Also, inflammation in perivascular fat with enhanced generation of tumor necrosis factor (TNF)-alpha and reduced adiponectin, which has anticontractile and thus antihypertensive properties [30, 31], is critically involved in small artery remodeling [32].
Myogenic tone, the intrinsic ability of vessels to constrict in response to increases in intraluminal pressure, participates early on in the alterations occurring in the arterial wall [33]. Among the mechanisms involved in the control of myogenic tone are changes in intracellular calcium, protein kinases, diacylglycerol, modulation of transient receptor potential-like channels, and ion transport [34]. Structural narrowing of the lumen may amplify vasoconstriction. Constriction may be a consequence of increased concentration of specific agents at the level of receptors, greater receptor density, or postreceptor signaling alterations associated with enhanced Ang II signaling leading to increased ROS generation and enhanced constriction and vessel growth [25, 28, 34, 35].
Endothelial dysfunction is involved in the initiation of vascular inflammation and development of atherosclerosis [36]. The number of circulating endothelial progenitor cells (EPCs), a bone marrow–derived population of cells capable of developing into competent mature endothelial cells, is an important determinant of endothelial function [37]. Decreased EPC numbers are associated with arterial stiffness and decreased endothelial function [38]. Endothelial dysfunction is not only accompanied by reduced vasodilation and increased endothelium-dependent contraction but also by cell proliferation, platelet activation, vascular permeability, and a pro-inflammatory and prothrombotic vascular phenotype. Detachment of endothelial cells (anoikis), increases in circulating microparticles derived from the endothelium, and reduced endothelial progenitor cells contribute also to dysfunction and remodeling of the microcirculation in hypertension [39].
Endothelial dysfunction promotes vascular inflammation through generation of ROS and by the production of vasoconstrictor agents, adhesion molecules, and growth factors [40, 41]. Inflammation is central in cardiovascular disease and could be involved in triggering myocardial and cerebrovascular ischemia [36, 42]. Blood pressure itself [43] or activation of the RAAS [26, 32] may induce an inflammatory process characterized by increased expression of adhesion molecules VCAM-1 (vascular cell adhesion molecule 1) and ICAM-1 (intercellular adhesion molecule 1) on endothelial cells, leukocyte extravasation, increased oxidative stress, cytokine production, and activation of immune cells and pro-inflammatory signaling pathways. Greater expression of adhesion molecules on the endothelial cell membrane and accumulation of monocyte/macrophages, dendritic cells, natural killer (NK) cells, and B and T lymphocytes are some of the mechanisms that participate in the inflammatory response in the vascular wall [44]. Patients with cardiovascular disease present indeed increased expression and plasma concentration of inflammatory markers and mediators [41, 45, 46]. High levels of inflammatory mediators, particularly IL-6, ICAM-1, and C-reactive protein (CRP), may be independent risk factors for the development of hypertension [47, 48] and have been associated with increased risk of diabetes [49] and cardiovascular disease. CRP levels correlate with insulin resistance, systolic blood pressure, pulse pressure, and hypertension [49, 50] and with markers of endothelial dysfunction (plasma levels of von Willebrand factor, tissue plasminogen activator, and cellular fibronectin) [51].
A role of innate immunity in mechanisms that contribute to the low-grade inflammatory response in hypertension has also been described. In an osteopetrotic mouse model that is deficient in vascular macrophages because of a mutation in the mCSF gene (csf1), neither Ang II nor DOCA-salt induced hypertension or vascular remodeling [5]. Dendritic cells, which are antigen presenting cells originating in the bone marrow but present in other tissues, including the vasculature, are critically involved in activation of adaptive immune responses. As such, their presence in the vasculature in hypertension and atherosclerosis suggests that they are associated with disease onset and progression through priming of T cells in cardiovascular disease in response to danger-associated molecular patterns (DAMPs) [52]. Recent evidence also suggests that different subsets of T lymphocytes may be involved in the mechanisms leading to the inflammatory response described in cardiac and metabolic diseases when an imbalance exists between the pro-inflammatory T helper lymphocytes (Th) 1, Th2, and Th17 and the anti-inflammatory T regulatory (Treg) subsets [44]. Mice deficient in T and B lymphocytes presented blunted hypertensive response to Ang II and DOCA-salt as well as reduced vascular remodeling in response to Ang II [53]. Effector T cell but not B lymphocyte adoptive transfer corrected the lack of response to Ang II. The central and pressor effects of Ang II are also critical for T-cell activation and development of vascular inflammation [54]. One of the mechanisms whereby T lymphocytes participate in hypertension and peripheral inflammation is in response to increased oxidative stress [55]. We recently showed that adaptive immunity could be enhanced as a result of a genetic predisposition with loci on chromosome 2 (which carries many pro-inflammatory genes) in a consomic strain of rats (SSBN2), which contains the genetic background of hypertensive Dahl-salt-sensitive rats and chromosome 2 from Brown-Norway normotensive rats [56]. The presence of the normotensive chromosome 2 was associated with upregulation of Treg markers, which were depressed in the Dahl-salt-sensitive rats. Enhanced Treg (CD8+ and CD4+ lymphocytes which were CD25+) and increased expression of Foxp3 (transcription factor that is a marker of Treg) as well as IL-10 and TGF-beta production (typically produced by Treg) were found in consomic rats, and the opposite in Dahl rats. Thus Treg decrease and T effector upregulation are associated to increased blood pressure and vascular inflammation. The potential protective role of Treg in cardiovascular disease is supported by the more recent evidence that adoptive transfer of Treg cells ameliorated cardiac damage and improved electric remodeling in Ang II-infused mice, independently of blood pressure-lowering effects [57], suggesting a role of T regulatory lymphocytes in the pathogenesis of blood pressure-induced cardiovascular remodeling. We have also recently shown that Treg adoptive transfer lowered blood pressure and protected from vascular remodeling in mice infused with either angiotensin II [58] or aldosterone [59].
Interestingly, inflammation may activate the RAAS, which in turn may further contribute to vascular remodeling and hypertension. Activators of nuclear receptors, such as the peroxisome proliferator-activated receptors (PPARs), downregulate the vascular inflammatory response in experimental animals [60] and decrease serum markers of inflammation in humans [61]. Thus, PPARs may be endogenous modulators of the inflammatory process involved in vascular structural changes occurring in hypertension. On the other hand, Ang II downregulates PPARs through activation of nuclear factor (NF)-κB [62]. Also, gene inactivation of PPAR gamma was shown to be associated with enhanced responses to Ang II including greater hypertrophic and inflammatory response as well as enhanced endothelial dysfunction [63].
Arterial aging is a predominant risk factor for the onset of cardiovascular diseases such as hypertension; on the other hand, hypertension is an important factor in accelerated aging of the vasculature, resulting in premature cardiovascular disease. The hypertensive vascular phenotype and the age-associated changes in blood vessels are similar. They include structural changes consisting in increased arterial wall thickness, reduced compliance, increased stiffness, and decreased lumen diameter and an associated pro-inflammatory phenotype [64, 65]. These structural changes are associated with impaired endothelial function, caused by oxidative stress and decreased production of vasodilators (NO and prostacyclins). The activation of the RAS and increased oxidative stress, decreased telomerase activity and telomere shortening, DNA damage, and genomic instability are all important promoters of cellular senescence [64].
3 Remodeling of Small Resistance Arteries and Arterioles in Hypertension
As mentioned above, increased peripheral vascular resistance appears to be a mechanism for diastolic or systo-diastolic hypertension found mostly in younger individuals with essential hypertension [65] which results mostly from resistance to flow in small arteries (with a lumen diameter of 100–300 μm) and arterioles (smaller than 100 μm) [1, 18]. Since according to Poiseuille’s law resistance is inversely related to the fourth power of the radius of the blood vessel, small decreases in the lumen diameter will increase resistance to a significant degree. Remodeling of resistance arteries (reduced vascular lumen with increased media thickness not correlated with stiffness changes) may be functional, mechanical, and structural [1]. Increases in the media-to-lumen ratio (M/L) are typical and the most reproducible parameter to compare changes in small arteries in subjects followed in repeat studies and when comparing different subjects [1, 18]. Our work has suggested that increased M/L of small arteries may be the most prevalent and possibly the earliest alteration that occurs in the cardiovascular system of hypertensive patients aged less than 60 years of age [16] and may be much more frequent than and in fact precede endothelial dysfunction in humans. Enhanced M/L of small arteries has been demonstrated to be associated with increased cardiovascular events, especially in high-risk patients [66].
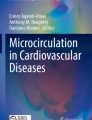
In stage 1 hypertension in individuals younger than 60 years, eutrophic remodeling of small arteries and arterioles is usually found (Fig. 5.1). In this type of remodeling, the outer diameter and the lumen are reduced, but the media cross section does not increase; thus there is no vascular hypertrophy [1, 18]. Smooth muscle cells are rearranged around a smaller lumen leading to increased media width and M/L. Whether vascular smooth muscle cells are increased in volume, length, or number remains a subject of controversy. Media growth toward the lumen combined with enhanced apoptosis in the periphery of the vessel may also contribute to these changes [32]. The smaller lumen decreases circumferential tension, according to Laplace’s law, and the increased media width reduces media stress, which protects the vessel’s wall from the effects of elevated blood pressure. When blood pressure elevation is severe or of long duration, increased wall stress results in hypertrophic remodeling of small arteries and arterioles as smooth muscle cell growth becomes greater than apoptosis and media cross-sectional area is enhanced [1, 67, 68]. Eutrophic and hypertrophic remodeling may be found in the same experimental animals in different arteries. Interestingly, hypertrophic remodeling of resistance arteries is found, particularly in humans, in renovascular hypertension [68], diabetes [69, 70], and acromegaly [71]. In experimental animals, hypertrophic remodeling can be demonstrated in those hypertensive models that are associated with excess endothelin, such as one-kidney one-clip renovascular hypertension, DOCA-salt hypertension, aldosterone-salt hypertension, and Dahl-salt-sensitive hypertension. Folkow’s model (Fig. 5.2) demonstrates that at all levels of vascular constriction, arteries with eutrophic remodeling generate more resistance to blood flow than arteries with hypertrophic remodeling, which in turn, generate more resistance than those from normotensive animals.

Remodeling of small arteries and arterioles in hypertension is inward (smaller lumen) and could be eutrophic, with no increase in the media cross-sectional area despite a thickened media (in essential hypertension), or it could be hypertrophic, in which case the media cross-sectional area is increased (generally associated with severe or secondary forms of hypertension). In both, media-to-lumen ratio (M/L) is greater than in normotension. Media cross-sectional area is calculated as πr o 2−πr i 2

Folkow’s model shows that at each level of vascular constriction (e.g., at the level of the dashed vertical line), resistance to blood flow is increased more in eutrophic remodeling than in hypertrophic remodeling; and in the latter, resistance to flow is greater than in vessels from normotensive subjects
4 Rarefaction of Arterioles and Capillaries
Rarefaction is another type of remodeling that is found in hypertension. It occurs at the level of small arterioles with a lumen diameter smaller than 40 μm and capillaries [1]. With rarefaction, the density of arterioles and capillaries in tissues is diminished and consequently vascular resistance is increased [72, 73] and tissue perfusion is impaired [74]. Arteriolar rarefaction is functional initially as a result of vasoconstriction, and later anatomical and permanent, followed by rarefaction of capillaries with decreased tissue perfusion. Decreases in tissue perfusion have been associated with vascular complications and cardiovascular events [75].
5 Conclusion
Vascular remodeling and endothelial dysfunction in small resistance arteries are features regularly reported in hypertension. Functional, structural, and mechanical alterations of resistance arteries are probably the earliest alterations in the vasculature found in hypertensive subjects younger than 60 years of age. They take the form of eutrophic inward remodeling accompanied by endothelial dysfunction associated eventually to enhanced stiffness. These changes have been shown to have prognostic significance with respect to outcomes. They could contribute through wave reflection to increases in stiffness of large arteries and thus to systolic hypertension and the increased pulse pressure found in older subjects with hypertension. Alternatively, increased large artery stiffness could increase pulsatility, which when conducted into the microcirculation, may cause injury and remodeling of small arteries and arterioles. Activation of the RAAS plays a key role in vascular remodeling and endothelial dysfunction through redox-sensitive pathways that promote growth and inflammation in the blood vessel wall.
References
Schiffrin EL (2004) Remodeling of resistance arteries in essential hypertension and effects of antihypertensive treatment. Am J Hypertens 17:1192–1200
Schiffrin EL, Touyz RM (2004) From bedside to bench to bedside: role of renin angiotensin aldosterone system in remodeling of resistance arteries in hypertension. Am J Physiol Heart Circ Physiol 287:H435–H446
Endemann DH, Schiffrin EL (2004) Endothelial dysfunction. J Am Soc Nephrol 15:1983–1992
Lerman A, Zeiher AM (2005) Endothelial function: cardiac events. Circulation 111:363–368
De Ciuceis C, Amiri F, Brassard P et al (2005) Reduced vascular remodeling, endothelial dysfunction, and oxidative stress in resistance arteries of angiotensin II-infused macrophage colony-stimulating factor-deficient mice: evidence for a role in inflammation in angiotensin-induced vascular injury. Arterioscler Thromb Vasc Biol 25:2106–2113
Savoia C, Schiffrin EL (2007) Reduction of C-reactive protein and the use of the anti-hypertensives. Vasc Health Risk Manag 3(6):975–983
Savoia C, Schiffrin EL (2006) Inflammation in hypertension. Curr Opin Nephrol Hypertens 2:152–158
Kranzhofer R, Schmidt J, Pfeiffer CA et al (1999) Angiotensin induces inflammatory activation of human vascular smooth muscle cells. Arterioscler Thromb Vasc Biol 19:1623–1629
Fukui T, Ishizaka N, Rajagopalan S et al (1997) p22phox mRNA expression and NAD(P)H oxidase activity are increased in aortas from hypertensive rats. Circ Res 80:45–51
Griendling KK, Sorescu D, Lassegue B, Ushio-Fukai M (2000) Modulation of protein kinase activity and gene expression by reactive oxygen species and their role in vascular physiology and pathophysiology. Arterioscler Thromb Vasc Biol 20:2175–2183
Touyz RM, Chen X, Tabet F et al (2002) Expression of a functionally active gp91phox-containing neutrophil-type NAD(P)H oxidase in smooth muscle cells from human resistance arteries: regulation by angiotensin II. Circ Res 90:1205–1213
Harada E, Yoshimura M, Yasue H et al (2001) Aldosterone induces angiotensin-converting enzyme gene expression in cultured neonatal rat cardiocytes. Circulation 104:137–139
Schiffrin EL, Gutkowska J, Genest J (1984) Effect of angiotensin II on deoxycorticosterone infusion on vascular angiotensin II receptors in rats. Am J Physiol Heart Circ Physiol 246:H608–H614
Pu Q, Fritsch Neves M, Virdis A, Touyz RM, Schiffrin EL (2003) Endothelin antagonism on aldosterone-induced oxidative stress and vascular remodeling. Hypertension 42:49–55
Idris-Khodja N, Mian MOR, Paradis P, Schiffrin EL (2014) Dual roles of adaptive immunity in hypertension. Eur Heart J 35:1238–1244
Park JB, Schiffrin EL (2001) Small artery remodeling is the most prevalent (earliest?) form of target organ damage in mild essential hypertension. J Hypertens 19:921–930
Delva P, Lechi A, Pastori C et al (2002) Collagen I and III mRNA gene expression and cell growth potential of skin fibroblasts in patients with essential hypertension. J Hypertens 20:1393–1399
Schiffrin EL (1992) Reactivity of small blood vessels in hypertension: relation with structural changes. Hypertension 19(Suppl 2):II-1–II-9
Schiffrin EL, Deng LY (1999) Structure and function of resistance arteries of hypertensive patients treated with a β-blocker or a calcium channel antagonist. J Hypertens 14:1247–1255
Intengan HD, Thibault G, Li JS, Schiffrin EL (1999) Resistance artery mechanics, structure and extracellular components in spontaneously hypertensive rats effects of angiotensin receptor antagonism and converting enzyme inhibition. Circulation 100:2267–2275
Intengan HD, Deng LY, Li JS, Schiffrin EL (1999) Mechanics and composition of human subcutaneous resistance arteries in essential hypertension. Hypertension 33:569–574
Marchesi C, Dentali F, Nicolini F et al (2012) Plasma levels of matrix metalloproteinases and their inhibitors in hypertension: a systematic review and meta-analysis. J Hypertens 30:3–16
Intengan HD, Schiffrin EL (2000) Structure and mechanical properties of resistance arteries in hypertension role of adhesion molecules and extracellular matrix determinants. Hypertension 36:312–318
Laviades C, Varo N, Fernandez J et al (1998) Abnormalities of the extracellular degradation of collagen type I in essential hypertension. Circulation 98:535–540
Touyz RM, Schiffrin EL (2000) Signal transduction mechanisms mediating the physiological and pathophysiological actions of angiotensin II in vascular smooth muscle cells. Pharmacol Rev 52:639–672
Schiffrin EL, Touyz RM (2003) Multiple actions of angiotensin II in hypertension: benefits of AT1 receptor blockade. J Am Coll Cardiol 42(5):911–913
Nurnberger J, Keflioglu-Scheiber A, Opazo Saez AM et al (2002) Augmentation index is associated with cardiovascular risk. J Hypertens 20:2407–2414
Touyz RM, Deng LY, He G et al (1999) Angiotensin II stimulates DNA and protein synthesis in vascular smooth muscle cells from human arteries: role of extracellular signal-regulated kinases. J Hypertens 17:907–916
Diep QN, Li JS, Schiffrin EL (1999) In vivo study of AT1 and AT2 angiotensin receptors in apoptosis in rat blood vessels. Hypertension 34:617–624
Marchesi C, Ebrahimian T, Angulo O et al (2009) Endothelial NO synthase uncoupling and perivascular adipose oxidative stress and inflammation contribute to vascular dysfunction in a rodent model of metabolic syndrome. Hypertension 54:1384–1392
Greenstein AS, Khavandi K, Withers SB et al (2009) Local inflammation and hypoxia abolish the protective anticontractile properties of perivascular fat in obese patients. Circulation 119:1661–1670
Savoia C, Schiffrin EL (2007) Vascular inflammation in hypertension and diabetes: molecular mechanisms and therapeutic intervention. Clin Sci 112:375–384
Izzard AS, Bund SJ, Heagerty AM (1996) Myogenic tone in mesenteric arteries from spontaneously hypertensive rats. Am J Physiol (Heart Circ Physiol) 270:H1–H6
Touyz RM, Yao G, Schiffrin EL (2003) c-Src induces phosphorylation and translocation of p47phox role in superoxide generation by Ang II in human vascular smooth muscle cells. Arterioscler Thromb Vasc Biol 23:981–987
Intengan HD, Schiffrin EL (2001) Vascular remodeling in hypertension – roles of apoptosis, inflammation, and fibrosis. Hypertension 38:581–587
Libby P, Tabas I, Fredman G, Fisher EA (2014) Inflammation and its resolution as determinants of acute coronary syndromes. Circ Res 114:1867–1879
Urbich C, Dimmeler S (2004) Endothelial progenitor cells: characterization and role in vascular biology. Circ Res 95(4):343–353
Hill JM, Zalos G, Halcox JP et al (2003) Circulating endothelial progenitor cells, vascular function, and cardiovascular risk. N Engl J Med 348(7):593–600
Burger D, Schock S, Thompson CS et al (2013) Microparticles: biomarkers and beyond. Clin Sci 124:423–441
Ross R (1999) Atherosclerosis – an inflammatory disease. N Engl J Med 340:115–126
Ridker PM (2014) Inflammation, C-reactive protein, and cardiovascular disease: moving past the marker versus mediator debate. Circ Res 114:594–595
Luna JM, Moon YP, Liu KM et al (2014) High-sensitivity C-reactive protein and interleukin-6–dominant inflammation and ischemic stroke risk: the Northern Manhattan Study. Stroke 45:979–987
Wung BS, Cheng JJ, Chao YJ et al (1996) Cyclical strain increases monocyte chemotactic protein-1 secretion in human endothelial cells. Am J Physiol 270:H1462–H1468
Schiffrin EL (2010) T lymphocytes: a role in hypertension? Curr Opin Nephrol Hypertens 19:181–186
Sesso HD, Buring JE, Rifai N et al (2003) C-reactive protein and the risk of developing hypertension. J Am Med Assoc 290:2945–2951
Preston RA, Ledford M, Materson BJ et al (2002) Effects of severe, uncontrolled hypertension on endothelial activation: soluble vascular cell adhesion molecule-1, soluble intercellular adhesion molecule-1 and von Willebrand factor. J Hypertens 20:871–877
Blake GJ, Rifai N, Buring JE, Ridker PM (2003) Blood pressure, C-reactive protein, and risk of future cardiovascular events. Circulation 108:2993–2999
Thorand B, Lowel H, Schneider A et al (2003) C-reactive protein as a predictor for incident diabetes mellitus among middle-aged men: results from the MONICA Augsburg cohort study, 1984–1998. Arch Intern Med 163:93–99
Barzilay JI, Peterson D, Cushman M et al (2004) The relationship of cardiovascular risk factors to microalbuminuria in older adults with or without diabetes mellitus or hypertension: the cardiovascular health study. Am J Kidney Dis 44:25–34
Chae CU, Lee RT, Rifai N, Ridker PM (2001) Blood pressure and inflammation in apparently healthy men. Hypertension 38:399–403
Engstrom G, Janzon L, Berglund G et al (2002) Blood pressure increase and incidence of hypertension in relation to inflammation-sensitive plasma protein. Arterioscler Thromb Vasc Biol 22:2054–2058
Christ A, Temmerman L, Legein B et al (2013) Dendritic cells in cardiovascular diseases: epiphenomenon, contributor, or therapeutic opportunity. Circulation 128:2603–2613
Guzik TJ, Hoch NE, Brown KA et al (2007) Role of T cell in the genesis of angiotensin II induced hypertension and vascular dysfunction. J Exp Med 204:2449–2460
Marvar PJ, Thabet SR, Guzik TJ et al (2010) Central and peripheral mechanisms of T-lymphocyte activation and vascular inflammation produced by angiotensin II-induced hypertension. Circ Res 107:263–270
Lob HE, Marvar PJ, Guzik TJ et al (2010) Induction of hypertension and peripheral inflammation by reduction of extracellular superoxide dismutase in the central nervous system. Hypertension 55:277–283
Viel EC, Lemarié CA, Benkirane K et al (2011) Immune regulation and vascular inflammation in genetic hypertension. Am J Physiol Heart Circ Physiol 298(3):H938–H944
Kvakan HKM, Quadri F, Park J-K et al (2009) Regulatory T cells ameliorate angiotensin II-induced cardiac damage. Circulation 119:2904–2912
Barhoumi T, Kasal DAB, Li MW et al (2011) T regulatory lymphocytes prevent angiotensin II-induced hypertension and vascular injury. Hypertension 57:469–476
Kasal DAB, Barhoumi T, Li MW et al (2012) T regulatory lymphocytes prevent aldosterone-induced vascular injury. Hypertension 59:324–330
Diep QN, Amiri F, Touyz RM et al (2002) PPARa activator effects on Ang II-induced vascular oxidative stress and inflammation. Hypertension 40:866–871
Haffner SM, Greenberg AS, Weston WM et al (2002) Effect of rosiglitazone treatment on nontraditional markers of cardiovascular disease in patients with type 2 diabetes mellitus. Circulation 106:679–684
Tham DM, Martin-McNulty B, Wang YX et al (2002) Angiotensin II is associated with activation of NF-kappaB mediated genes and down regulation of PPARs. Physiol Genomics 11:21–30
Marchesi C, Rehman A, Rautureau Y et al (2013) Protective role of vascular smooth muscle cell PPARγ in angiotensin II-induced vascular disease. Cardiovasc Res 97:562–570
Wang M, Zhang J, Jiang LQ, Spinetti G, Pintus G, Monticone R, Kolodgie FD, Virmani R, Lakatta EG (2007) Proinflammatory profile within the grossly normal aged human aortic wall. Hypertension 50:219–227
Schiffrin EL (2007) The vascular phenotypes in hypertension: relation to the natural history of hypertension. J Am Soc Hypertens 1:56–67
Rizzoni D, Porteri E, Boari G et al (2003) Prognostic significance of small artery structure in hypertension. Circulation 108:2230–2235
Sharifi AM, Schiffrin EL (1998) Apoptosis in vasculature of spontaneously hypertensive rats effect of an angiotensin converting enzyme inhibitor and a calcium channel antagonists. Am J Hypertens 11:1108–1116
Rizzoni D, Porteri E, Guelfi D et al (2000) Cellular hypertrophy in subcutaneous small arteries of patients with renovascular hypertension. Hypertension 25:931–935
Rizzoni D, Porteri E, Guelfi D et al (2001) Structural alteration in subcutaneous small arteries of normotensive and hypertensive patients with non insulin-dependent diabetes mellitus. Circulation 103:1238–1244
Endemann DH, Pu Q, De Ciuceis C et al (2004) Persistent remodeling of resistance arteries in type 2 diabetic patients on antihypertensive treatment. Hypertension 43:399–404
Rizzoni D, Porteri E, Giustina A et al (2004) Acromegalic patients show the presence of hypertrophic remodeling of subcutaneous small resistance arteries. Hypertension 43:561–565
Prewitt RL, Chen II, Dowell R (1982) Development of microvascular rarefaction in the spontaneously hypertensive rat. Am J Physiol (Heart Circ Physiol) 243:H243–H251
Greene AS, Tonellato PJ, Lui J et al (1989) Microvascular rarefaction and tissue vascular resistance in hypertension. Am J Physiol (Heart Circ Physiol) 256:H126–H131
Greene AS, Tonellato PJ, Zhang Z et al (1992) Effect of microvascular rarefaction on tissue oxygen delivery in hypertension. Am J Physiol (Heart Circ Physiol) 262:H1486–H1493
Levy B, Schiffrin EL, Mourad JJ et al (2008) Impaired tissue perfusion: a pathology common to hypertension, obesity and diabetes. Circulation 118:968–976
Disclosure
This study was supported by CIHR grants 13570, 37917, 82790, and 102606, a Canada Research Chair on Hypertension and Vascular Research from the CRC/CIHR Program of the Government of Canada, and a Canada Fund for Innovation grant, all to ELS.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Savoia, C., Schiffrin, E.L. (2015). Vascular Changes in the Microcirculation: Arterial Remodeling and Capillary Rarefaction. In: Berbari, A., Mancia, G. (eds) Arterial Disorders. Springer, Cham. https://doi.org/10.1007/978-3-319-14556-3_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-14556-3_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-14555-6
Online ISBN: 978-3-319-14556-3
eBook Packages: MedicineMedicine (R0)