
Abstract
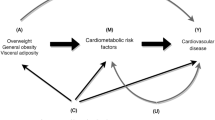
Obesity, in particular central obesity, is a major risk factor for cardiovascular disease (CVD) [1]. A great portion of the adverse impact of (central) obesity on cardiovascular health may be explained through related haemodynamic and metabolic mediators such as blood pressure (BP), cholesterol and glucose [2]. These risk factors tend to cluster within individuals forming the metabolic syndrome (MetS) [3]. Obesity and/or MetS-related adverse changes in the arterial wall provide a structural and functional background for clinical events such as myocardial infarction, stroke and peripheral artery disease, all known to occur at higher rates in these conditions [4–7]. This chapter revises the current epidemiological evidence around the adverse effects that (central) obesity and the MetS may exert on large artery properties, particularly, arterial stiffening. Focus is put on evidence derived, whenever available, from representative prospective observational and intervention studies conducted over the last decade.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Obesity, in particular central obesity, is a major risk factor for cardiovascular disease (CVD) [1]. A great portion of the adverse impact of (central) obesity on cardiovascular health may be explained through related haemodynamic and metabolic mediators such as blood pressure (BP), cholesterol and glucose [2]. These risk factors tend to cluster within individuals forming the metabolic syndrome (MetS) [3]. Obesity and/or MetS-related adverse changes in the arterial wall provide a structural and functional background for clinical events such as myocardial infarction, stroke and peripheral artery disease, all known to occur at higher rates in these conditions [4–7]. This chapter revises the current epidemiological evidence around the adverse effects that (central) obesity and the MetS may exert on large artery properties, particularly, arterial stiffening. Focus is put on evidence derived, whenever available, from representative prospective observational and intervention studies conducted over the last decade.
1 Body Fatness/Fat Distribution and Arterial Stiffness: An Early Phenomenon
Many studies have shown that higher levels of body fatness, in particular, a central pattern of fat distribution, are associated with arterial stiffness (reviewed in [6, 8]). These primarily cross-sectional studies may be fairly summarised into two key observations: firstly, deleterious adaptations related to increased adiposity seem to occur across all age categories [9–11]; secondly, such adaptations are observed with higher levels of adiposity even when within the ranges of normal weight and are thus not confined to obesity. Indeed, the increased levels of arterial stiffness observed already among children/adolescents [12–17] and young adults [9, 18, 19] suggest that higher levels of (central) adiposity do not need to be long lasting to have deleterious effects on the arterial system. In addition, the fact that higher levels of (central) adiposity at young(er) ages are associated with higher arterial stiffness later in life [18, 20–22] and that a favourable change in obesity status from childhood to adulthood is associated with less arterial stiffness in adulthood [23] emphasise the importance of healthy lifestyle promotion early in life. The strong tracking of (central) obesity throughout the life course [20] further corroborates this need because early and cumulative exposures to adverse levels of (central) body fatness may hamper considerable and sustainable improvements in arterial properties resulting from interventions targeting obese adults, given that such interventions will invariably be much shorter than a person’s lifetime.
2 Do Changes in Body Fatness Affect Arterial Stiffness?
The extent to which changes in body fatness affect changes in arterial stiffness remains unclear because most of the longitudinal (observational or intervention) studies available thus far have been restricted to the appreciation of the impact of changes in body weight, which does not discern fat from lean body mass. Indeed, some observational studies have shown that increases in weight were associated with increases in arterial stiffness among young and healthy [24] and overweight middle-aged adults [25]. Several small intervention studies, all confined to individuals with obesity or diabetes, have shown that weight loss led to arterial de-stiffening [26–30]. More recent and larger randomised controlled trials (RCTs) confirmed the beneficial effects of weight loss attained by means of behavioural interventions (diet and/or exercise) among nondiabetic overweight/obese individuals with (e.g. the ENCORE study [31]) or without hypertension (e.g. the SAVE trial [32, 33]). Assuming that the weight loss attained indeed reflected reductions in body fatness, these findings support the view that body fatness may impact on arterial stiffness independently, at least in part, of related changes in BP. Still, it remains that arterial adaptations related to weight changes do not clarify the extent to which any of the favourable effects observed could be attributed to reductions in specific types of fat depots (e.g. visceral vs. subcutaneous) and/or its distribution (e.g. central vs. peripheral) or even be attenuated by concomitant loss of muscle mass.
2.1 Visceral Fat as Main Determinant of Arterial Stiffness
Abdominal visceral fat is thought to be more strongly associated with arterial stiffness than abdominal subcutaneous fat [34–37]. In an important proof of concept study, and despite its small sample and highly experimental setting, Orr et al. indeed showed that abdominal visceral (VAT), not subcutaneous adipose tissue (SAT), was associated with the increases in arterial stiffness resulting from 5 kg weight gain induced by overfeeding nonobese young adults for 6–8 weeks [38]. In addition, in a recent study in which the biopsies from visceral (greater omentum) and subcutaneous (abdominal) white adipose tissue samples were obtained from obese subjects scheduled for bariatric surgery, the visceral fat cell size (i.e. volume), but not number, was strongly associated with arterial stiffness, whereas no such association was found with SAT (volume or number) [39]. It must be mentioned that recent studies suggest that the adverse effect of VAT on arterial stiffness (as on metabolic disturbances relating central obesity to poorer cardiovascular outcome) may not only be due to the effects of omental hypertrophy of adipose tissue but also due to adipose tissue accumulating specifically around the epicardium [40–42] and/or in the liver (a typical feature of non-alcoholic fatty liver disease) [43–45]. Because this evidence derives from cross-sectional studies, the interrelations, relative contributions and specific pathobiological mechanisms through which these fat depots may impact on general and local arterial stiffening, and haemodynamic factors still need to be further investigated in prospective studies.
2.2 The Beneficial Role of Peripheral Fat on Arterial Stiffness
Studies examining the role of the whole-body fat distribution on arterial stiffness rather than of central fatness only have unveiled a complex scenario: in contrast to central fat (i.e. that accumulated in the trunk/abdominal areas), higher levels of peripheral fat mass (i.e. that accumulated in the limbs and thus stored mainly subcutaneously) may have an independent favourable impact on arterial stiffness [19, 46, 47]. Indeed, the different lipolytic activity of the two fat regions/tissues provides biological support for their opposite effects on arterial stiffness. These ‘dysfunctional’ [1] vs. ‘functional’ [48] effects of fat could explain why, in general, central fat estimates correlate more strongly with health outcomes than estimates of total body fatness. As such, adverse changes in body fat distribution may occur with ageing (i.e. increases in central accompanied by decreases in peripheral fat mass) without being detected by appreciable changes in total body weight or body mass index (BMI), though both contributing, additively, to accelerated arterial stiffening. This hypothesis was tested in the Amsterdam Growth and Health Longitudinal Study, in a first study to have examined in detail, how naturally occurring changes in body fat and its distribution (assessed by dual x-ray absorptiometry) correlated with changes in arterial stiffness indexed by a large set of valid estimates throughout the arterial tree [49]. The study had three key findings: first, throughout the 6-year longitudinal study (between the ages of 36 and 42), greater levels of central fat were adversely associated with carotid, femoral and aortic stiffness, whereas greater levels of peripheral fat were favourably associated with these stiffness estimates; these associations reflected the more ‘chronic’ (deleterious) effects of persistent adverse fat distribution over time. Second, increases in trunk fat were adversely associated with 6-year changes in carotid and aortic, though not femoral, stiffness, whereas increases in peripheral fat were favourably associated with changes in these stiffness estimates; these observations suggested a more ‘acute’ component to the deleterious effects of changes in body fat distribution on arterial stiffness of predominantly elastic arterial segments. Finally, the detrimental effects of increases in central fat and decreases in peripheral fat on arterial stiffness were independent of one another and concomitant changes in lean mass and other risk factors (including mean BP) and were accompanied by only minor increases in body weight [49]. Noteworthy, increases in trunk but decreases in peripheral fat mass formed a relatively prevalent phenotype (one third of the study population) that displayed the steepest rates of progression in carotid and aortic stiffness (Fig. 16.1a, b, respectively) despite changes in BMI that ranged within the limits assigned to normal weight (Fig. 16.1c). This phenotype is consistent with the existence of a relative prevalent subgroup of individuals at the population level designated as ‘metabolically obese but normal weight’, who are often characterised by elevated visceral adiposity (despite a BMI <25) and a more atherogenic lipid and/or glucose metabolism profile and who thus may be at a particular high risk for metabolic and arterial disease and in need of appropriate screening and preventive measures [50, 51].

Comparisons of (a) changes in carotid Young’s elastic modulus (cYEM), (b) changes in carotid-femoral pulse wave velocity (cfPWV) and (c) baseline and follow-up body mass index (BMI), between different phenotypes of change in body fat distribution as observed in a 6-year follow-up from the Amsterdam Growth and Health Longitudinal Study. BMI data were adjusted for sex; arterial data were adjusted for sex, body height and changes in mean arterial pressure, lean mass and other biological risk factors. Error bars indicate the standard errors of the means (Reproduced from Schouten et al. [49] with permission from the American Society of Nutrition)
2.3 The Role of Muscle Mass: The Need for Comprehensive Whole-Body Composition Studies
Adopting a whole-body composition (i.e. examining also the independent contribution of muscle mass in addition to body fat) rather than a body fat/fat distribution-only model has revealed that also appendicular muscle mass may be an independent beneficial determinant of arterial stiffness, particularly though not confined to the elderly [19, 46, 49, 52–55]. Currently, there is a great concern about the cardiometabolic consequences of the increasing prevalence of (central) obesity and sarcopenia (i.e. the degenerative loss of skeletal muscle mass and strength) associated with ageing, especially when occurring in combination – i.e. sarcopenic obesity [56]. How decreases in lean mass may affect arterial stiffness is not clear as the evidence so far has been mainly derived from cross-sectional studies [19, 46, 52–55]. It is possible that the relationship is not causal in the sense that higher muscle mass may simply reflect higher (lifelong) physical activity and/or less sedentary habits, better nutrient intake status and/or better glucose uptake/insulin sensitivity, all of which protect against arterial stiffness [57–61]. Alternatively, arterial stiffness may promote sarcopenia by reducing limb blood flow and inducing rarefaction and dysfunction in the microcirculation, thereby affecting muscle contraction and ultimately leading to muscle mass rarefaction. This hypothesis was supported by a recent prospective study from the Health, Aging and Body Composition Study, showing that older individuals with higher cfPWV at baseline had poorer levels of leg lean mass and sarcopenic index at baseline and over a 6-year follow-up period, independently of age, BMI, BP, diabetes, physical activity, smoking, total fat mass, low-grade inflammation, peripheral artery disease and CHD status [62]. Further longitudinal and intervention studies are needed to clarify the role of muscle mass on arterial stiffening (or vice versa), if any. Nevertheless, the existence of a link between muscle mass and arterial stiffness retains relevant clinical implications because it stresses the need to carefully monitor and secure that weight-loss interventions do not occur at the expense of muscle mass, particularly among the elderly.
3 Metabolic Syndrome and Arterial Stiffness: An Early Phenomenon
Increased arterial stiffness has been consistently reported in individuals with the MetS or with increasing clustered load or number of traits of the MetS (reviewed in [7]). Like for (central) fatness, a major force underlying the MetS risk factor clustering, such adverse arterial changes have been shown across all ages [63, 64], including young children and adolescents, with [65] or without overt obesity [12, 66], and young [67–71] and older adults [72], including those treated [73] or untreated for hypertension [74, 75]. The increased arterial stiffness in the MetS thus seems to be caused by subtle metabolic abnormalities that characterise prediabetic states but not necessarily fully developed diabetes. In addition, the recent findings from the Cardiovascular Risk in Young Finns Study showing higher levels of arterial stiffness among young adults who had the MetS during youth but also of arterial stiffness reduced to levels similar to those who had never had the MetS throughout the life course among those who, by adulthood, recovered from the MetS [76], support the potential reversibility of the adverse effects of the MetS if prevented/targeted early in life.
4 Do Changes in Metabolic Syndrome Status Affect Arterial Stiffness?
Confirming the suggestions derived from cross-sectional observations showing that the increases in arterial stiffness with advancing age were accentuated in the presence of the MetS [68, 64], recent prospective cohort studies have shown that individuals with the MetS not only have higher arterial stiffness at baseline but also display steeper increases in arterial stiffness with ageing as compared with those without the MetS [70, 77–80]. In addition, analyses of the impact of changes in MetS status among young [80, 81] and middle-aged [82] adults showed that those with incident and persistent MetS over the course of time displayed the steepest increases in arterial stiffness as compared with their peers who remained MetS-free throughout. Importantly, increases in arterial stiffness with ageing among those who recovered from the MetS tended to be somewhat less steep than those with persistent MetS [80] or even comparable to those who remained MetS-free throughout [82, 81]. An important observation in one of these longitudinal studies was that the MetS-related increase in carotid stiffness seemed to have preceded structural and local haemodynamic changes consistent with maladaptive (outward) carotid remodelling, an important process that may explain the increase risk of stroke in individuals with the MetS [80]. Taken together, the longitudinal data reviewed above [70, 76–82] demonstrate accelerated arterial stiffening and maladaptive remodelling, which may explain, at least in part, the increased CVD risk in individuals with the MetS [7]. These findings also emphasise the importance of primary prevention given the observed reversibility of the adverse impact of MetS on arterial structural and functional properties among those individuals who recovered from the MetS.
4.1 Specific Clusters of the Metabolic Syndrome’s Traits and Arterial Stiffness
It is important to stress that the association between the MetS and arterial stiffness seems not only to be attributable to elevated BP, one of its most common traits and a main determinant of arterial stiffness. Indeed, in addition to (and independently of) elevated BP, (central) obesity and increased glucose levels are traits often associated with arterial stiffness [70, 72, 80, 83], whereas dyslipidaemia (as ascertained by elevated triglycerides and/or decreased HDL cholesterol) has been less or not consistently so. The clustering of central obesity, increased glucose levels and BP appears to be the most prevalent across several populations in the western world [64, 84, 83], and this phenotype is not only associated with the highest arterial stiffness levels [64, 83] but also with the greatest mortality risk [84].
5 Pathobiological Mechanisms Linking (Central) Obesity and the Metabolic Syndrome to Arterial Stiffening
The adverse association of the critical axis (central) obesity - MetS with arterial stiffness raises important questions about the potential underlying molecular processes. These may include some of the effects central obesity and related insulin resistance are known to exert at the vascular wall level, for instance, through inflammatory reactions, endothelial dysfunction and sympathetic activation [34, 32, 85]. These abnormalities are interrelated and affect vascular tone and stimulate vascular smooth muscle cell proliferation. In addition, changes in the type or structure of elastin and/or collagen in the arterial wall due to hyperglycaemia, particularly the formation of cross-links through nonenzymatic glycosylation of proteins that generate advanced glycation end products, could constitute another mechanism [7]. Several of these putative mediators are thus likely to account for the obesity- or MetS-related increases in arterial stiffness, but currently we have only fragments of insight among a likely large set of players involved [5]. Teasing apart their individual contribution and/or identification of predominant operative pathways may provide key information for tailored interventions aiming at the treatment of arterial stiffening and related cardiovascular sequelae [6]. A comprehensive analysis of these issues in the context of representative prospective cohort studies or RCTs is still lacking and thus most warranted.
6 Summary
In this chapter, recent epidemiological evidence pertaining to the role of (central) obesity and the MetS on arterial stiffness was reviewed. Reinforced by recent prospective data, there is convincing evidence that these interrelated risk factors increase arterial stiffness, a mechanism that may explain the associated higher CVD risk. However, there is still relatively few data on (1) the molecular basis of greater arterial stiffness associated with these risk factors, (2) the prognostic significance of arterial stiffness indices in individuals with these risk factors and (3) the extent to which intervention on these risk factors improves cardiovascular outcome through beneficial impact on arterial stiffness. Given the high and increasing prevalence of obesity and the MetS, these questions constitute an important research agenda.
References
Hajer GR, van Haeften TW, Visseren FL (2008) Adipose tissue dysfunction in obesity, diabetes, and vascular diseases. Eur Heart J 29(24):2959–2971
Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration, Lu Y, Hajifathalian K, Ezzati M et al (2014) Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: a pooled analysis of 97 prospective cohorts with 1.8 million participants. Lancet 383(9921):970–983
Grundy SM (2000) Metabolic complications of obesity. Endocrine 13(2):155–165
Safar ME, Czernichow S, Blacher J (2006) Obesity, arterial stiffness, and cardiovascular risk. J Am Soc Nephrol 17(4 Suppl 2):S109–S111
Seals DR, Gates PE (2005) Stiffening our resolve against adult weight gain. Hypertension 45(2):175–177
Ferreira I, van de Laar RJ, Stehouwer CD (2014) Obesity, metabolic syndrome, diabetes and smoking. In: Safar ME, O’Rourke MF, Frohlich ED (eds) Blood pressure and arterial wall mechanics in cardiovascular diseases. Springer, London, pp 409–422
Stehouwer CD, Henry RM, Ferreira I (2008) Arterial stiffness in diabetes and the metabolic syndrome: a pathway to cardiovascular disease. Diabetologia 51(4):527–539
Stehouwer CD, Ferreira I (2006) Diabetes, lipids and other cardiovascular risk factors. In: Safar ME, O’Rourke MF (eds) Arterial stiffness in hypertension, vol 23, Handbook of hypertension. Elsevier, Amsterdam, pp 427–456
Wildman RP, Mackey RH, Bostom A et al (2003) Measures of obesity are associated with vascular stiffness in young and older adults. Hypertension 42(4):468–473
Zebekakis PE, Nawrot T, Thijs L et al (2005) Obesity is associated with increased arterial stiffness from adolescence until old age. J Hypertens 23(10):1839–1846
Scuteri A, Orru M, Morrell CH et al (2012) Associations of large artery structure and function with adiposity: effects of age, gender, and hypertension. The SardiNIA Study. Atherosclerosis 221(1):189–197
Whincup PH, Gilg JA, Donald AE et al (2005) Arterial distensibility in adolescents: the influence of adiposity, the metabolic syndrome, and classic risk factors. Circulation 112(12):1789–1797
Geerts CC, Evelein AM, Bots ML et al (2012) Body fat distribution and early arterial changes in healthy 5-year-old children. Ann Med 44(4):350–359
Urbina EM, Gao Z, Khoury PR et al (2012) Insulin resistance and arterial stiffness in healthy adolescents and young adults. Diabetologia 55(3):625–631
Sakuragi S, Abhayaratna K, Gravenmaker KJ et al (2009) Influence of adiposity and physical activity on arterial stiffness in healthy children: the lifestyle of our kids study. Hypertension 53(4):611–616
Urbina EM, Kimball TR, Khoury PR et al (2010) Increased arterial stiffness is found in adolescents with obesity or obesity-related type 2 diabetes mellitus. J Hypertens 28(8):1692–1698
Aggoun Y, Farpour-Lambert NJ, Marchand LM et al (2008) Impaired endothelial and smooth muscle functions and arterial stiffness appear before puberty in obese children and are associated with elevated ambulatory blood pressure. Eur Heart J 29(6):792–799
Ferreira I, Twisk JW, van Mechelen W et al (2004) Current and adolescent body fatness and fat distribution: relationships with carotid intima-media thickness and large artery stiffness at the age of 36 years. J Hypertens 22(1):145–155
Ferreira I, Snijder MB, Twisk JW et al (2004) Central fat mass versus peripheral fat and lean mass: opposite (adverse versus favorable) associations with arterial stiffness? The Amsterdam Growth and Health Longitudinal Study. J Clin Endocrinol Metab 89(6):2632–2639
Ferreira I, van de Laar RJ, Prins MH et al (2012) Carotid stiffness in young adults: a life-course analysis of its early determinants: the Amsterdam Growth and Health Longitudinal Study. Hypertension 59(1):54–61
McEniery CM, Spratt M, Munnery M et al (2010) An analysis of prospective risk factors for aortic stiffness in men: 20-year follow-up from the Caerphilly prospective study. Hypertension 56(1):36–43
Johansen NB, Vistisen D, Brunner EJ et al (2012) Determinants of aortic stiffness: 16-year follow-up of the Whitehall II study. PLoS One 7(5):e37165
Aatola H, Hutri-Kahonen N, Juonala M et al (2010) Lifetime risk factors and arterial pulse wave velocity in adulthood: the cardiovascular risk in Young Finns Study. Hypertension 55(3):806–811
Wildman RP, Farhat GN, Patel AS et al (2005) Weight change is associated with change in arterial stiffness among healthy young adults. Hypertension 45(2):187–192
Yamada J, Tomiyama H, Matsumoto C et al (2008) Overweight body mass index classification modifies arterial stiffening associated with weight gain in healthy middle-aged Japanese men. Hypertens Res 31(6):1087–1092
Goldberg Y, Boaz M, Matas Z et al (2009) Weight loss induced by nutritional and exercise intervention decreases arterial stiffness in obese subjects. Clin Nutr 28:21–25
Rider OJ, Tayal U, Francis JM et al (2010) The effect of obesity and weight loss on aortic pulse wave velocity as assessed by magnetic resonance imaging. Obesity (Silver Spring) 18(12):2311–2316
Barinas-Mitchell E, Kuller LH, Sutton-Tyrrell K et al (2006) Effect of weight loss and nutritional intervention on arterial stiffness in type 2 diabetes. Diabetes Care 29(10):2218–2222
Dengo AL, Dennis EA, Orr JS et al (2010) Arterial destiffening with weight loss in overweight and obese middle-aged and older adults. Hypertension 55(4):855–861
Ikonomidis I, Mazarakis A, Papadopoulos C et al (2007) Weight loss after bariatric surgery improves aortic elastic properties and left ventricular function in individuals with morbid obesity: a 3-year follow-up study. J Hypertens 25(2):439–447
Blumenthal JA, Babyak MA, Hinderliter A et al (2010) Effects of the DASH diet alone and in combination with exercise and weight loss on blood pressure and cardiovascular biomarkers in men and women with high blood pressure: the ENCORE study. Arch Intern Med 170(2):126–135
Cooper JN, Buchanich JM, Youk A et al (2012) Reductions in arterial stiffness with weight loss in overweight and obese young adults: potential mechanisms. Atherosclerosis 223(2):485–490
Hughes TM, Althouse AD, Niemczyk NA et al (2012) Effects of weight loss and insulin reduction on arterial stiffness in the SAVE trial. Cardiovasc Diabetol 11:114
Diamant M, Lamb HJ, van de Ree MA et al (2005) The association between abdominal visceral fat and carotid stiffness is mediated by circulating inflammatory markers in uncomplicated type 2 diabetes. J Clin Endocrinol Metab 90(3):1495–1501
Sutton-Tyrrell K, Newman A, Simonsick EM et al (2001) Aortic stiffness is associated with visceral adiposity in older adults enrolled in the study of health, aging, and body composition. Hypertension 38(3):429–433
Lee JW, Lee HR, Shim JY et al (2007) Viscerally obese women with normal body weight have greater brachial-ankle pulse wave velocity than nonviscerally obese women with excessive body weight. Clin Endocrinol (Oxf) 66(4):572–578
Ohashi N, Ito C, Fujikawa R et al (2009) The impact of visceral adipose tissue and high-molecular weight adiponectin on cardio-ankle vascular index in asymptomatic Japanese subjects. Metabolism 58(7):1023–1029
Orr JS, Gentile CL, Davy BM, Davy KP (2008) Large artery stiffening with weight gain in humans: role of visceral fat accumulation. Hypertension 51(6):1519–1524
Arner P, Backdahl J, Hemmingsson P et al (2014) Regional variations in the relationship between arterial stiffness and adipocyte volume or number in obese subjects. Int J Obes (Lond). doi:10.1038/ijo.2014.118
Kim BJ, Kim BS, Kang JH (2013) Echocardiographic epicardial fat thickness is associated with arterial stiffness. Int J Cardiol 167(5):2234–2238
Natale F, Tedesco MA, Mocerino R et al (2009) Visceral adiposity and arterial stiffness: echocardiographic epicardial fat thickness reflects, better than waist circumference, carotid arterial stiffness in a large population of hypertensives. Eur J Echocardiogr 10(4):549–555
Choi TY, Ahmadi N, Sourayanezhad S et al (2013) Relation of vascular stiffness with epicardial and pericardial adipose tissues, and coronary atherosclerosis. Atherosclerosis 229(1):118–123
Huang Y, Bi Y, Xu M et al (2012) Nonalcoholic fatty liver disease is associated with atherosclerosis in middle-aged and elderly Chinese. Arterioscler Thromb Vasc Biol 32(9):2321–2326
Vlachopoulos C, Manesis E, Baou K et al (2010) Increased arterial stiffness and impaired endothelial function in nonalcoholic fatty liver disease: a pilot study. Am J Hypertens 23(11):1183–1189
Salvi P, Ruffini R, Agnoletti D et al (2010) Increased arterial stiffness in nonalcoholic fatty liver disease: the Cardio-GOOSE study. J Hypertens 28(8):1699–1707
Snijder MB, Henry RM, Visser M et al (2004) Regional body composition as a determinant of arterial stiffness in the elderly: the Hoorn study. J Hypertens 22(12):2339–2347
Lee M, Choh AC, Demerath EW et al (2012) Associations between trunk, leg and total body adiposity with arterial stiffness. Am J Hypertens 25(10):1131–1137
Frayn KN (2002) Adipose tissue as a buffer for daily lipid flux. Diabetologia 45(9):1201–1210
Schouten F, Twisk JW, de Boer MR et al (2011) Increases in central fat mass and decreases in peripheral fat mass are associated with accelerated arterial stiffening in healthy adults: the Amsterdam Growth and Health Longitudinal Study. Am J Clin Nutr 94(1):40–48
Conus F, Rabasa-Lhoret R, Peronnet F (2007) Characteristics of metabolically obese normal-weight (MONW) subjects. Appl Physiol Nutr Metab 32(1):4–12
Ruderman N, Chisholm D, Pi-Sunyer X, Schneider S (1998) The metabolically obese, normal-weight individual revisited. Diabetes 47(5):699–713
Ochi M, Kohara K, Tabara Y et al (2010) Arterial stiffness is associated with low thigh muscle mass in middle-aged to elderly men. Atherosclerosis 212(1):327–332
Kim TN, Park MS, Lim KI et al (2011) Skeletal muscle mass to visceral fat area ratio is associated with metabolic syndrome and arterial stiffness: The Korean Sarcopenic Obesity Study (KSOS). Diabetes Res Clin Pract 93(2):285–291
Sanada K, Miyachi M, Tanimoto M et al (2010) A cross-sectional study of sarcopenia in Japanese men and women: reference values and association with cardiovascular risk factors. Eur J Appl Physiol 110(1):57–65
Kohara K, Ochi M, Tabara Y et al (2012) Arterial stiffness in sarcopenic visceral obesity in the elderly: J-SHIPP study. Int J Cardiol 158(1):146–148
Prado CM, Wells JC, Smith SR et al (2012) Sarcopenic obesity: a critical appraisal of the current evidence. Clin Nutr 31(5):583–601
Henry RM, Kostense PJ, Spijkerman AM et al (2003) Arterial stiffness increases with deteriorating glucose tolerance status: the Hoorn study. Circulation 107(16):2089–2095
van de Laar RJ, Ferreira I, van Mechelen W et al (2010) Lifetime vigorous but not light-to-moderate habitual physical activity impacts favorably on carotid stiffness in young adults: the Amsterdam Growth and Health Longitudinal Study. Hypertension 55(1):33–39
van de Laar RJ, Stehouwer CD, van Bussel BC et al (2013) Adherence to a Mediterranean dietary pattern in early life is associated with lower arterial stiffness in adulthood: the Amsterdam Growth and Health Longitudinal Study. J Intern Med 273(1):79–93
van de Laar RJ, Stehouwer CD, van Bussel BC et al (2012) Lower lifetime dietary fiber intake is associated with carotid artery stiffness: the Amsterdam Growth and Health Longitudinal Study. Am J Clin Nutr 96(1):14–23
van de Laar RJ, Stehouwer CD, Prins MH et al (2014) Self-reported time spent watching television is associated with arterial stiffness in young adults: the Amsterdam Growth and Health Longitudinal Study. Br J Sports Med 48(3):256–264
Abbatecola AM, Chiodini P, Gallo C et al (2012) Pulse wave velocity is associated with muscle mass decline: Health ABC study. Age (Dordr) 34(2):469–478
Scuteri A, Najjar SS, Muller DC et al (2004) Metabolic syndrome amplifies the age-associated increases in vascular thickness and stiffness. J Am Coll Cardiol 43(8):1388–1395
Scuteri A, Najjar SS, Orru M et al (2010) The central arterial burden of the metabolic syndrome is similar in men and women: the SardiNIA Study. Eur Heart J 31(5):602–613
Iannuzzi A, Licenziati MR, Acampora C et al (2006) Carotid artery stiffness in obese children with the metabolic syndrome. Am J Cardiol 97(4):528–531
Pandit D, Chiplonkar S, Khadilkar A et al (2011) Efficacy of a continuous metabolic syndrome score in Indian children for detecting subclinical atherosclerotic risk. Int J Obes (Lond) 35(10):1318–1324
Ferreira I, Henry RM, Twisk JW et al (2005) The metabolic syndrome, cardiopulmonary fitness, and subcutaneous trunk fat as independent determinants of arterial stiffness: the Amsterdam Growth and Health Longitudinal Study. Arch Intern Med 165(8):875–882
Li S, Chen W, Srinivasan SR, Berenson GS (2005) Influence of metabolic syndrome on arterial stiffness and its age-related change in young adults: the Bogalusa Heart Study. Atherosclerosis 180(2):349–354
Ferreira I, Boreham CA, Twisk JW et al (2007) Clustering of metabolic syndrome risk factors and arterial stiffness in young adults: the Northern Ireland Young Hearts Project. J Hypertens 25:1009–1020
Koskinen J, Magnussen CG, Viikari JS et al (2012) Effect of age, gender and cardiovascular risk factors on carotid distensibility during 6-year follow-up. The cardiovascular risk in Young Finns study. Atherosclerosis 224(2):474–479
Urbina EM, Srinivasan SR, Kieltyka RL et al (2004) Correlates of carotid artery stiffness in young adults: the Bogalusa Heart Study. Atherosclerosis 176(1):157–164
Della-Morte D, Gardener H, Denaro F et al (2010) Metabolic syndrome increases carotid artery stiffness: the Northern Manhattan Study. Int J Stroke 5(3):138–144
Protogerou AD, Blacher J, Aslangul E et al (2007) Gender influence on metabolic syndrome’s effects on arterial stiffness and pressure wave reflections in treated hypertensive subjects. Atherosclerosis 193(1):151–158
Schillaci G, Pirro M, Vaudo G et al (2005) Metabolic syndrome is associated with aortic stiffness in untreated essential hypertension. Hypertension 45(6):1078–1082
Vyssoulis GP, Pietri PG, Karpanou EA et al (2010) Differential impact of metabolic syndrome on arterial stiffness and wave reflections: focus on distinct definitions. Int J Cardiol 138(2):119–125
Koivistoinen T, Hutri-Kahonen N, Juonala M et al (2011) Metabolic syndrome in childhood and increased arterial stiffness in adulthood: the cardiovascular risk in Young Finns Study. Ann Med 43(4):312–319
Nakanishi N, Suzuki K, Tatara K (2003) Clustered features of the metabolic syndrome and the risk for increased aortic pulse wave velocity in middle-aged Japanese men. Angiology 54(5):551–559
Safar ME, Thomas F, Blacher J et al (2006) Metabolic syndrome and age-related progression of aortic stiffness. J Am Coll Cardiol 47(1):72–75
Li CI, Kardia SL, Liu CS et al (2011) Metabolic syndrome is associated with change in subclinical arterial stiffness: a community-based Taichung Community Health Study. BMC Public Health 11:808
Ferreira I, Beijers HJ, Schouten F et al (2012) Clustering of metabolic syndrome traits is associated with maladaptive carotid remodeling and stiffening: a 6-year longitudinal study. Hypertension 60(2):542–549
Koskinen J, Magnussen CG, Taittonen L et al (2010) Arterial structure and function after recovery from the metabolic syndrome: the cardiovascular risk in Young Finns Study. Circulation 121(3):392–400
Tomiyama H, Hirayama Y, Hashimoto H et al (2006) The effects of changes in the metabolic syndrome detection status on arterial stiffening: a prospective study. Hypertens Res 29(9):673–678
Scuteri A, Cunha PG, Rosei EA et al (2014) Arterial stiffness and influences of the metabolic syndrome: a cross-countries study. Atherosclerosis 233(2):654–660
Guize L, Thomas F, Pannier B et al (2007) All-cause mortality associated with specific combinations of the metabolic syndrome according to recent definitions. Diabetes Care 30(9):2381–2387
Beijers HJ, Ferreira I, Bravenboer B et al (2014) Higher central fat mass and lower peripheral lean mass are independent determinants of endothelial dysfunction in the elderly: the Hoorn study. Atherosclerosis 233(1):310–318
Acknowledgement
Dr. Ferreira is supported by a senior postdoctoral fellowship from the Netherlands Heart Foundation (grant no. 2006T050).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Ferreira, I. (2015). Obesity and Metabolic Syndrome. In: Berbari, A., Mancia, G. (eds) Arterial Disorders. Springer, Cham. https://doi.org/10.1007/978-3-319-14556-3_17
Download citation
DOI: https://doi.org/10.1007/978-3-319-14556-3_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-14555-6
Online ISBN: 978-3-319-14556-3
eBook Packages: MedicineMedicine (R0)