
Abstract
Resection may provide prognostic benefts even in patients with numerous colorectal liver metastases (CLM), achieving in that long-term survival. However, the terms “multiple bilobar” CLM includes a wide range of conditions, from oligometastatic superficial deposits to numerous deep-located lesions. In cases of bilobar superficial lesions, one-stage hepatectomy (OSH) is commonly adopted, but in cases of deep-located CLM, two-stage hepatectomy is preferred in many centers. Recently, we have demonstrated that OSH is possible even for deep-located CLM. This approach relies on the combination of thoraco-phreno-laparotomy, intraoperative ultrasound (IOUS) resection guidance, the detachment of metastases in contact with vessels (R1 vasc), and the identification of communicating veins among hepatic veins to preserve an adequate outflow despite hepatic vein invasion. Strenghtening this policy in an oncological persepctive there is the evidence that R1 vasc margin conveys similar rate of local recurrence when compared to R0. In this chapter we will get deep into these technical points, discussing the related consequences in terms of surgical strategy and resectability.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Tumor resectability
- Intraoperative ultrasound
- One-stage hepatectomy
- Communicating veins
- Minimesohepatectomy
- Liver tunnel
Introduction
Up to now, liver surgery has been the standard treatment of colorectal liver metastases (CLM), provided that complete resection is possible [1,2,3,4]. Resection may benefit even patients with numerous colorectal liver metastases (CLM), achieving long-term survival [5,6,7]. Patients with multiple bilobar nodules are the most complex to treat because a large parenchyma sacrifice is often required, leading to the risk of postoperative liver failure [8]. To prevent this risk, in 2000 Adam et al. proposed two-stage hepatectomy (TSH) [9]. It schedules the cleaning of the less involved hepatic lobe during a first laparotomy, followed or not by the portal vein occlusion of the contralateral lobe in order to induce hypertrophy of the final future liver remnant (FLR), and then the resection of the most involved hemiliver. TSH is now a standardized procedure adopted worldwide, with good short- and long-term results [5, 10,11,12,13,14,15]. The major drawback of TSH is the drop-out risk: one-third to one-fourth of patients do not receive the second hepatectomy because of disease progression between the two stages [11]. More recently, associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) have been proposed [16], again a staged operation like TSH; however, at the first step in addition to the cleaning of the left liver, parenchymal dissection is carried out, dividing the left lobe from the remnant liver or the two hemi-liver. This policy has allowed the relevant reduction of the drop-out, but the significant increment of the risk of postoperative mortality [17].
To overcome the drop-out risk of TSH, and the risk of mortality of ALPPS, one-stage hepatectomy (OSH) has been proposed, at least for those patients suitable for the first two procedures [16]. OSH schedules the simultaneous resection into a single procedure of all the bilobar lesions. In cases of bilobar superficial lesions, OSH is commonly adopted, but in cases of deep-located CLM, TSH is the preferred option. The authors reported the possibility to perform OSH even in presence of deep-located lesions thanks to the combination of thoraco-phreno-laparotomy, intraoperative ultrasound (IOUS) resection guidance, the detachment of metastases in contact with vessels, and the identification of communicating veins (CV) among hepatic veins to preserve an adequate outflow [18,19,20,21]. This strategy has minimized the need for parenchyma sacrifice and major hepatectomy [20, 22, 23]. Even if OSH prevents drop-out risks, some theoretical disadvantages have been raised: the technical complexity of the procedure, and the high rate of 0-mm margin (R1) resections (detachment of CLM from vascular structures). For that, the intraoperative evaluation of the tumor staging, the definition of the tumor–vessel relations, and the recognition of the presence of anatomical peculiarities, are fundamental steps together with the specific preparation of the operative field to allow the proper management of the patient in a OSH perspective.
Surgical Technique
The OSH approach scheduling the complete removal of all the multiple bilobar CLM in a single liver resection is based on the following main pillars.
-
1.
The incision.
-
2.
The IOUS [19].
-
3.
The liver mobilization.
-
4.
The detachment of CLM from intrahepatic vascular structures.
-
5.
The flow analysis.
In this chapter we will get deep into these technical points, discussing the related consequences in terms of surgical strategy and resectability.
Incision
As a general principle, the surgical procedures herein described schedule the surgeon with left hand positioned over the resection area established by means of IOUS, driving together with the IOUS images the liver dissection, and hanging the liver for backflow bleeding control: in this perspective the incision is selected, using J-shaped laparotomy as the standard incision (Fig. 11.1). This last, which includes the removal of the xiphoid process, other than being propaedeutic for liver handling using the left hand (Fig. 11.2), also allows a vertical view of the hepato-caval confluence, both from above with the surgeon standing (Fig. 11.3), and from the right side with the surgeon seated once approaching the hepato-caval plane (Fig. 11.4).

J-shaped laparotomy. The incision starts from the xiphoid process on the midline to approximately 3–4 cm above the umbilicus. Then, it curves laterally towards the right hypocondrium until it reaches to the costal arch, at the level of the ninth intercostal space

Liver handling after a J-shaped laparotomy. This incision allows the surgeon’s left hand to be positioned behind the liver at the posterior aspect of the defined dissection plane. Furthermore, it allows controlling the backflow bleeding by hanging the liver

Vertical view of the hepato-caval confluence achieved by means of the removal of the xiphoid process

Lateral view of the hepato-caval confluence with the surgeon seated: this perspective facilitates the mobilization of the right liver from the inferior vena cava (IVC). Tumor (T)
When the tumor is located in the para-caval portion of segment 1 or anyway at the hepato-caval confluence, and control of the hepatic veins at this level does not seem fully achievable with the abdominal incision only due to patient characteristics and/or the tumor features (position, relations and size), two solutions are possible, both featured by representing an extension of the J-shaped laparotomy, and both having the aim of extending the working space for the surgeon, especially at the mid–late phases of the dissection and in general when the major veins are approached.
A J-shaped thoraco-phreno-laparotomy has the peculiarity of allowing the operator himself to have more space for left-hand positioning and the related liver handling (Fig. 11.5), and moreover opening a better view of the hepato-caval plane, which becomes in line with the visual plane of the operator (Fig. 11.6) [24], this being particularly useful for affording conservative resection of large tumor located in segment 1 (Fig. 11.7) [25]. It is worth stressing the fact that the need for opening the chest may not be evident during mobilization of the liver, but generally it appears crucial during the dissection, and more often at the end of it when the specimen is going to be detached from the hepatic veins, and more space for handling, particularly with the left hand, could be needed. Therefore, paradoxically, chest-opening is a maneuver more frequently carried out by expert surgeons rather than young fellows, since it is a decision taken taking advantage moreover of the background experience which leads the surgeon to foresee the potential difficulties of the resection, and to shift to a thoraco-phreno-laparotomic approach without hesitation.

J-shaped thoraco-phreno-laparotomy. The incision is a standard J-shaped laparotomy which continues along the ninth intercostal space up to mid-axillary line on the skin and the posterior axillary on the intercostal space. In this way, the space for the surgeon’s left hand is increased, with a better control of the hepato-caval confluence

Lateral view of the hepato-caval confluence after a J-shaped thoraco-phreno-laparotomy. The space for the surgeon’s left hand is increased with a better view and control of the hepato-caval confluence. Right lung (L); inferior vena cava (IVC)

J-shaped thoraco-phreno-laparotomy for a large tumor located in segment 1. The liver and the tumor (T) have been completely mobilized from the inferior vena cava (IVC)
A median extension to the lower abdomen is selected (Fig. 11.8), particularly in the event of existing median incision: this access facilitates the caudal tilting of the liver once mobilized, and like the previous incision a larger space for positioning the left hand and then for handling the liver. However, this access is not provided by a surgeon’s visual plane being perpendicular to the hepato-caval space, and is probably linked to a higher risk of wound hernias.

Schematic representation of a J-shaped laparotomy (or thoraco-phreno-laparotomy in yellow) with a median extension to the lower abdomen
IOUS Intraoperative Staging
In the case of CLM, the increment of the detection power of IOUS is still relevant. Indeed, in these patients the detection of any tiny nodule undiscovered preoperatively becomes crucial for attempting a reduction of the still high postoperative early recurrence rate [26]. Between 10 and 40% of patients who are carriers of colon cancer have not palpable CLM [27, 28]; as a consequence of that, IOUS exploration of the liver remains crucial, and contrast-enhanced intraoperative ultrasound (CE-IOUS) seems able to enhance its role in this sense. In a maximized parenchymal-sparing perspective, the relevance of an accurate staging is obvious for avoiding missing any tiny lesion, and otherwise resulting in a resection which would be radical but is in fact an R2 operation.
CE-IOUS in these conditions seems useful in a particular setting of patients carrying multiple CLM: those without a bright liver (steatotic) at IOUS [29], and presenting isoechoic CLM [30] (Fig. 11.9).

Contrast-enhanced intraoperative ultrasound (CE-IOUS on the right) which is better revealing a isoechoic colorectal liver metastasis (T) compared with unenhanced IOUS (left)
New perspectives can be obtained by using liver-specific contrast agents, which allow prolonged exploration. In a preliminary experience CE-IOUS only showed new lesions in 2 out of 8 patients [31]. More recent studies have shown that the prolonged persistence of the black-hole effect may help also in detecting intraoperatively those metastatic foci which disappear after chemotherapy [32].
Mobilization
For right-sided segmentectomies or subsegmentectomies or sectionectomies, the bare area is dissected and the right hemiliver is mobilized till the surgeon’s left hand is positioned behind the hemiliver, sustaining it, and is comfortably positioned over the posterior aspect of the drawn dissection plane (Fig. 11.10). This mobilization should be extensive enough to allow allocation of the surgeon’s hand, minimizing the risk during the traction maneuvers of damaging the adjacent structures, and particularly any short hepatic vein which should be preventivly divided whenever at the edge of the dissection area: in the unfortunate event, their damaging could be the source of conspicuous bleeding from the inferior vena cava (IVC), which could even be massive because recognized late since it occurs back to the liver, and could be source of vessel fractures extended to the caval wall, meanwhile the surgeon is concentrated on dissecting the liver.

Definition of the resection area. a The surgeon’s left-hand fingertip and the probe act simultaneously to draw the optimal dissection plane to be followed. b The corresponding IOUS image in which the yellow dashed line indicates the ideal dissection plane that runs from the echoic shadow generated by the electrocautery interposed between the liver surface and the probe (EC) to the surgeon’s fingertip (F); tumor (T)
Therefore, a slight mobilization of the right hemiliver just dividing the triangular ligament and partially or completely the bare area will be accomplished for lesions located in segments 5, 6, 7 inferior and 8 ventral. Conversely, the right side of the retrohepatic IVC is reached for lesions located in the segments 7 and 8 dorsal. If the lesion is close to the hepatocaval confluence (last 4 cm), but not in contact with the hepatic veins, the retro-hepatic caval ligament is not divided, and only the space between the right hepatic vein (RHV) and the middle hepatic vein (MHV) is dissected allowing for finger-tip insertion and eventual compression. The caval confluence of the RHV is recognized following the trajectory of the right inferior phrenic vein, which flows near the RHV at this level and which is a constant landmark (Fig. 11.11) [33].

Lateral view of the hepato-caval confluence after a J-shaped laparotomy. The right inferior phrenic vein (RIPV) represents a constant landmark for the caval confluence of the right hepatic vein (RHV) into the inferior vena cava (IVC)
If the lesion is still right-sided but in contact with an hepatic vein at its caval confluence (Fig. 11.12), or is involving the para-caval portion of the segment 1 (Fig. 11.13), liver mobilization includes division of the retro-hepatic caval ligament and exposure of the retro-hepatic IVC until the area to be resected is under control of the surgeon’s left hand (surgeon’s finger tip being placed over the most distal portion of the planned dissection plane). This detachment proceeds unless control is obtained, even though this means reaching the complete detachment from the IVC (Fig. 11.14): in this case, once the mobilization of the segment 1 is complete, and carried out through a right-sided approach, the left-hand fingertips are positioned at the edge between the segment 2 and 1 where the Arantius’ ligament runs, somehow hooking the caudate lobe (Fig. 11.15).

IOUS image that shows a tumor (T) in contact with the right hepatic vein (RHV) at its confluence into the inferior vena cava (IVC). Middle hepatic vein (MHV); portal branch to the right anterior section (P5–8)

IOUS image showing a tumor (T) involving the para-caval portion of the segment 1; middle hepatic vein (MHV); inferior vena cava (IVC)

Complete detachment of the liver from the inferior vena cava (IVC). The fossa where the IVC was laying is shown

The surgeon’s left-hand fingertips are positioned at the edge between segments 2 and 1 where the Arantius’ ligament runs, hooking the Spigelian lobe (SL)
For segment 2 and 3 segmentectomies or subsegmentectomies, the left triangular ligament and the left coronary ligament are divided, and the left lobe is handled with the surgeon’s left hand.
For lesions located at the segment 4 superior at the hepato-caval junction, the mobilization combines the one described for lesions at the segments 7 inferior and 8 ventral and for those in the left lobe. For these lesions, once a relationship with the main trunk of the MHV is established, particular attention should be paid to the fact that MHV generally features a vertical confluence into the IVC (Fig. 11.16), which makes its length shorter than the others, and moreover, its central position makes its compression more difficult; for these reasons, the injury of this vein during the dissection could be source of massive bleeding, and therefore a preventive check of the control of the vein flow by finger compression, or vein encirclement itself, have always to be considered.

IOUS image showing the perpendicular, and straight confluence of the middle hepatic vein (MHV) into the inferior vena cava (IVC)
A particular trick which deserves to be mentioned is the use of IOUS to help mobilization once there are adhesions which may mask important structures to be recognized and preserved such as the hepatic hilum, the IVC, and the hepatic veins: just positioning the probe to check the position of these structures in relation to the dissection area (the surgeon’s finger tips positioned in there would be helpful), and the distance between the latter and the structures themselves, helps to avoid them being damaged, with the severe consequences related with that.
Tumor–Vessel Detachment
The glissonian pedicle may be spared when in contact with an encapsulated hepatocellular carcinoma (HCC) or a CLM, with integrity of the vessel wall appreciable at IOUS without any sign of bile duct dilation (Fig. 11.17). In the presence of bile duct dilation, tumor thrombus, invasion of the vessel wall, and for CLM, contact wider than half of the pedicle circumference, the pedicle must be divided (Fig. 11.18). In these conditions, extension of the hepatectomy is required for complete tumor clearance.

IOUS image showing a CLM (T) in contact with the portal branch to the right anterior section (P5–8) without signs of infiltration (integrity of the vessel wall and no signs of bile duct dilation). The glissonian pedicle may be spared

In the presence of bile duct dilation (BD), the pedicle must be divided
The hepatic vein may be spared when in contact with an encapsulated HCC with integrity of the vessel wall appreciable at IOUS (Fig. 11.19). Initially for the CLM, its contact was considered an indication for hepatic vein resection; more recently sparing of the hepatic vein is always attempted when the contact extension is less than two-thirds of the vein circumference at IOUS (Fig. 11.20).

a IOUS image showing an encapsulated HCC (T) in contact with the middle hepatic vein (MHV) and the right hepatic vein (RHV). b In this case, the hepatic veins could be spared

a IOUS image showing a CLM (T) in contact with the right hepatic vein (RHV) at its confluence into the inferior vena cava (IVC). b In this case, the hepatic vein is spared
Flow Analyses
In the presence of tumor thrombus, invasion of the vessel wall, and contact wider than two-thirds of the vein circumference in CLM, the hepatic vein must be divided (Fig. 11.21). In these conditions, extension of the hepatectomy is not compulsorily considered, even if the hepatic vein is invaded at its caval confluence (the last 4 cm). Indeed, an extension of the resection to the liver parenchyma theoretically drained by the hepatic vein to be resected is considered only if one of the following US signs is missing:
-
Presence of accessory hepatic veins at IOUS as an inferior right hepatic vein (IRHV) (Fig. 11.22) [34] in the presence of an invasion at the caval confluence of the right hepatic vein.
-
Color-flow IOUS (CF-IOUS) showing hepatopetal blood flow in the feeding portal branch, once the hepatic vein to be resected is clamped [35] by means of encirclement, or more simply by vein compression at its extrahepatic route using a fingertip [36]
-
Communicating veins connecting adjacent hepatic veins (Fig. 11.23), these being more easily detectable using CF-IOUS to disclose their presence [19].

a IOUS image showing a CLM (T) infiltrating (red arrows) the right hepatic vein (RHV). b In this case, the hepatic vein is resected

IOUS image showing an inferior right hepatic vein (IRHV). This vein typically runs behind the right portal branch (RPV). Portal branch to the right anterior section (P5–8); portal branch to the right posterior section (P6–7); inferior vena cava (IVC)

CF-IOUS serial images showing the entire route of a communicating vein (CV) connecting the right hepatic vein (RHV) and the middle hepatic vein (MHV). The detection of these communicating veins represents a crucial step for the “radical but conservative” policy, aimed to minimize the rate of parenchymal sacrifice
New Operations
The aforementioned technical tricks assembled together have made it possible to devise new operation minimizing the rate of major hepatectomy in these patients. These new operations are herein listed.
Systematic Extended Right Posterior Sectionectomy
Systematic extended right posterior sectionectomy (SERPS) is a surgical technique that allows the systematic sparing of part of the right anterior section in the presence of tumors with the presentation shown in Fig. 11.24 [37].

Eligibility criteria for systematic extended right posterior sectionectomy (SERPS): in all cases, in CF-IOUS the hepatopetal blood flow must be evident in the portal branch to the right anterior section (P5–8) once the right hepatic vein (RHV) is clamped if not already occluded. a Presence of vascular invasion of the RHV at the hepatocaval confluence (within 4 cm), with tumors (T) also in segment 6. b Presence of vascular invasion of the RHV at the hepatocaval confluence, without any tumor in segment 6, but without accessory veins and with hepatofugal portal blood flow in the portal branch to segment 6 (P6) once the RHV clamped if not already occluded. c Presence of vascular invasion of the right posterior portal branch (P6–7) or anyway biliary dilation of the bile ducts draining segment 6 and segment 7 (BD), with T in contact also with P5–8 but without signs of infiltration
Eligibility Criteria
Patients suitable for SERPS are those with tumors showing one of three conditions:
-
1.
Invasion of the right hepatic vein (RHV) is evident within 4 cm of the hepatocaval confluence, with other lesions involving segment VI and eventually segment VII (Fig. 11.24a).
-
2.
Invasion of the RHV within 4 cm of the hepatocaval confluence is evident, without other lesions involving segment VI, without an inferior RHV (IRHV), and with hepatofugal portal blood flow at CF-IOUS in the portal branch to segment VI (P6) when the RHV is clamped if not already occluded (Fig. 11.24b). In the event an IRHV is present, or, if not, when the flow direction in P6 remains hepatopetal, resection of segments VII and VIII together with the RHV is carried out [34] rather than SERPS; therefore, SERPS is applied as an alternative to resection of segments VII and VIII in those patients who do not have proper outflow for segment VI once the RHV is divided.
-
3.
Contact with the right anterior glissonian sheath and a relationship with the right posterior section is evident, with at least one of the following features: contact with the right posterior section determining proximal bile duct dilation, vessel wall invasion, or, for CLM, contact wider than half of the pedicle circumference (Fig. 11.24c, d).
Procedure
In the first two conditions, extension to the right anterior section is tailored to guarantee the complete removal of the tumor, and a dissection line is drawn on the left side of the RHV, which is also resected (Fig. 11.25); flow direction in the right anterior portal branch at CF-IOUS is estimated as previously described, once the RHV is clamped, if it is not occluded. The right anterior pedicle is not necessarily exposed on the liver cut surface. In the third condition, the extension of the resection into the right anterior section is tailored to preserve most of the parenchyma of segment VIII, the tract of the RHV at the hepatocaval confluence, and the left portion of segment V without division of the right anterior pedicle, which is exposed on the cut surface.

Systematic extended right posterior sectionectomy (SERPS). a The dissection line (yellow arrows) is drawn. b The liver at the end of the resection, with the stump of the right hepatic vein (RHVs) which is evident; inferior vena cava (IVC)
Minimesohepatectomy
This procedure represents an alternative to the conventional mesohepatectomy in patients with tumors invading the MHV at its caval confluence; it consists of a limited resection, including the tract of the invaded vein without its reconstruction, sparing part of segment IV, and/or of the right anterior section, as shown in Fig. 11.26a and as described in the next section [23].

Minimesohepatectomy. a Schematically it consists in a limited resection of segment 4 superior and 8 with the invaded tract of the middle hepatic vein (MHV). The presence of communicating veins (CV) between the MHV itself and one or both of the adjacent hepatic veins allows the blood to be drained by those veins (white arrows). b CF-IOUS showing communicating veins (CV) between the middle hepatic vein (MHV) and the left hepatic vein (LHV). c The liver at the end of the resection with the stump of the MHV (MHVs) exposed on the cut surface. Right hepatic vein (RHV); inferior vena cava (IVC)
Eligibility Criteria
Patients suitable for minimesohepatectomy (MMH) are those with tumors having macroscopic signs of vascular invasion of MHV at hepatocaval confluence on preoperative imaging and IOUS.
Procedure
Mobilization of the right and left hemiliver is tailored based on the size of the lesion and its cranial extension toward the MHV caval confluence. As a general rule, mobilization of the liver to obtain the encirclement of the hepatic veins at caval confluence should be recommended. For planning an MMH (Fig. 11.26a), at least one of these three findings should be confirmed by means of CF-IOUS:
-
1.
Detection on CF-IOUS without, and, if negative, with clamping of the MHV, of communicating veins between the MHV and RHV and/or LHV and/or IVC (Fig. 11.26b).
-
2.
If no communicating veins are evident at CF-IOUS, reversal flow on CF-IOUS in the peripheral portion of the clamped MHV should be confirmed; this finding suggests the existence anyway of communicating veins with the adjacent hepatic veins, despite not found at their direct search.
-
3.
Hepatopetal flow in residual portion of the central segments (IV, V, and VIII); this finding also suggests the existence anyway of communicating veins with the adjacent hepatic veins, despite them not found at direct search.
If none of these findings is confirmed, and especially if hepatofugal flow direction in portal branches to segments V and/or IV inferior is detected, hepatectomy should be extended to the area fed by those portal branches.
The posterior wall of the MHV, or of the tumor involving the paracaval portion, is used as a deep landmark for delimiting the resection area. A crucial point for proper performance of the MMH is, in the event a communicating vein is visualized, detecting and preserving the latter, on the contrary, keeping the dissection nearby the tumor to avoid division of communicating veins which anyway exists although not visualized.
Upper Transversal Hepatectomy (UTH)
For tumors involving more than one and up to all the hepatic veins at the hepato-caval confluence, major hepatectomy or vascular reconstruction, or even unresectabilty are considered. In 1987, Makuuchi et al. [34] reported that once the presence of a thick IRHV is evident at preoperative imaging or at IOUS, resection of the tumor together with the RHV could be feasible without carrying out a formal right hepatectomy rather limiting the liver tissue removal to that of segments VII and VIII. That was the first paper showing how just the disclosure of an anatomical feature makes feasible surgical procedures otherwise unfeasible. Taking profit of the pioneering experience of Makuuchi, both SERPS and MMH have been released, and we have further proceeded with the herein-described UTH [20].
Eligibility Criteria
Tumor at caval confluence invading two of the hepatic veins at caval confluence in presence of IRHV and communicating veins, or just communicating veins. The tumor could lie over the hilar plate, with contact with but no invasion of the right and left portal branches and the segmental portal branches to segments IV inferior, V, and VI.
Procedure
UTH consists in the total or partial resection of the superior liver segments (II, III, IVsup, VII, VIII) including partially or completely segment I together with up to the three hepatic veins but preserving the inferior portion of the liver, preserving the communicating veins with or without accessory veins to guarantee the outflow of the inferior portion of the liver theoretically drained by the resected hepatic veins (Fig. 11.27).

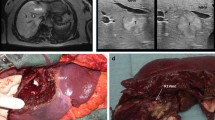
Upper transversal hepatectomy. a Indications: pre-operative CT scan showing the right (RHV) and middle hepatic veins (MHV) affected by two large tumors (T). b IOUS image that confirms the vascular involvement (red arrows) of the MHV, the RHV, and the inferior vena cava (IVC) by the tumor. c Schema showing the vascular drainage (white arrows) at the end of the resection. The preservation of communicating veins between the RHV and the MHV and between the MHV and the LHV is a crucial point to perform this kind of procedure. d The liver at the end of the resection; the stumps of the RHV and MHV are shown (RHVs, MHVs)
The US study in these patients should precisely map the accessory veins, IRHV included, and the communicating veins depicting their pattern is just connecting two adjacent HV or an HV and the IVC: in the latter circumstance, the short hepatic vein connected to the obstructed HV through the communicating vein has to be preserved. Inversely, in the absence of accessory veins flowing into the IVC, even in a similar tumor presentation, the caval plane can fully be freed (Fig. 11.28). Furthermore, adequate exposure and mobilization should allow positioning the left hand at the posterior aspect of the defined dissection plane. For all these reasons, a J-shaped thoraco-phreno-lapatorotic access is frequent in these circumstances. The direct view favored by this incision to the hepato-caval plane allows tailoring the adequate mobilization of the liver from the caval plane; in the event that an IRHV exists, this approach facilitates this mobilization without sectioning this vein root. The access, the mobilization, the in- and outflow mapping and the IOUS-guidance lead to the removal of a relatively small and almost completely diseased part of the liver, preserving the vast majority of the functioning liver parenchyma with adequate in and outflow. The existence and preservation of an IRHV and the communicating vein could make feasible the removal of all the superior segments and of the three HVs [21], sparing also segments IV inf, V and even III, compared with the preservation of just segment VI, as initially described by Makuuchi in 1987 [34].

Fully mobilization of the liver in the absence of accessory veins flowing into the inferior vena cava (IVC). The fossa where the IVC was laying is shown (IVC fossa)
Liver Tunnel
This procedure represents an extension of the MMH, including the total removal of segment I [38, 39].
Eligibility Criteria
Schematic representations of the procedure are shown in (Fig. 11.29). Patients eligible for this approach are those with tumoral involvement of segments VIII, IV superior and I, including the MHV at its caval confluence (within 4 cm), in presence of communicating veins between the MHV, the RHV, and/or the LHV; similarly, patients with tumors involving segments IV superior or VIII and segment I without invasion of the MHV are eligible too. It consists in a limited resection including or not the MHV [40].

“Liver Tunnel”. This procedure represents an extension of the mini-mesohepatectomy, including the total removal of segment I. a Schema showing the vascular drainage (white arrows) at the end of the resection in case of resection of the middle hepatic vein (MHV). The presence of communicating veins (CV) between the MHV itself and one or both of the adjacent hepatic veins allows the blood to be drained by those veins. b Schema showing the vascular drainage at the end of the resection in case of preservation of the MHV. Inferior vena cava (IVC); right hepatic vein (RHV), left hepatic vein (LHV)
Procedure
Once the anterior surface of the hepatocaval confluence is exposed. Complete mobilization of the liver has to be accomplished with full detachment of the retrohepatic IVC. Resection area is drawn under IOUS guidance. Dissection is started from the low-medial side of the drawn resection area, having the left hand positioned between the posterior surface of the liver and the IVC (Fig. 11.30): the surgeon’s left hand finger-tips grip the Arantius ligament shifting at IOUS almost on the same axis the MHV and the Arantius ligament itself. MHV resection is carried out according with the criteria described for the MMH procedure. Resection of the MHV or its tumoral detachment is accomplished first then the dissection proceeds towards the posterosuperior aspect of the left glissonian pedicle, then to the right and the dorsal portion of P5–8; finally, the RHV is exposed and following its route towards the IVC the resection is completed (Fig. 11.30c).

Intraoperative pictures of a “liver tunnel”. a Full mobilization of the liver with the surgeon’s left-hand fingertips positioned at the edge between segments 2 and 1 where the Arantius’ ligament runs, hooking the Spigelian lobe (SL). b The resection is carried out with the surgeon’s left hand positioned between the posterior surface of the liver and the inferior vena cava (IVC). c The liver at the end of the resection. The right hepatic vein (RHV) and the middle hepatic vein (MHV) are exposed on the cut surface at their confluence in the IVC. Portal branch to the right anterior section (P5–8); portal branch to the right posterior section (P6–7); right portal vein (RPV)
Conclusions
The terms “multiple bilobar” CLM includes a wide range of conditions, ranging from oligometastatic superficial deposits to numerous deep-located lesions. The authors suggest that OSH (pure surgical one-stage approach) is possible even for deep-located CLM [16]. This approach relies on: (1) the IOUS-guided detachment of CLM from glissonean pedicles and HVs whenever not infiltrated; (2) the HV resection and reconstruction when they are marginally infiltrated, and (3) an accurate flow analysis, including disclosure of CVs among HVs and of inflow direction after HV clamping, to preserve liver parenchyma despite main outflow resection [16, 21]. All these maneuvers require an adequate incision, e.g., a thoraco-phreno-laparotomy in most cases, and an extensive liver mobilization.
The main potential drawback of this policy is its oncological adequacy. Up to now, a negative surgical margin (≥1 mm) has been the standard for CLM. However, in multiple bilobar deep-located CLM a 0-mm margin is often mandatory to achieve resectability, which is the case in most presentations with tumor–vessel relations. The so called R1vasc, once the CLM is detached from the vessel to which it was in contact although without a clear infiltration, has shown in our experience local recurrence rates which are in line with those experienced removing CLM in the parenchyma and leaving ≥1 mm of tumor-free resection margin [41]. Once confirmed in a large and multi-institutional series, these results are more than encouraging for several reasons:
-
1.
they validate the intraoperative criteria herein described in confirming parenchyma-sparing resectability;
-
2.
they provide more technical solutions;
-
3.
they introduce the concept of a R1 oncologically suitable surgery once the 0-mm margin corresponds to the area of tumor vessel detachment (R1vasc).
In conclusion, the herein-described intraoperative criteria allows radical parenchyma-sparing surgery for multiple CLM, even when some of them show complex and deep located presentations. Thus, these criteria act as fundamental steps in determining the surgical strategy and then the resectability.
References
Abdalla EK, Adam R, Bilchik AJ, et al. Improving resectability of hepatic colorectal metastases: expert consensus statement. Ann Surg Oncol. 2006;13:1271–80.
Adam R, Wicherts DA, de Haas RJ, et al. Patients with initially unresectable colorectal liver metastases: is there a possibility of cure? J Clin Oncol. 2009;27:1829–35.
Poston GJ, Adam R, Alberts S, et al. OncoSurge: a strategy for improving resectability with curative intent in metastatic colorectal cancer. J Clin Oncol. 2005;23:7125–34.
Vigano L, Russolillo N, Ferrero A, et al. Evolution of long-term outcome of liver resection for colorectal metastases: analysis of actual 5-year survival rates over two decades. Ann Surg Oncol. 2012;19:2035–44.
Wicherts DA, Miller R, de Haas RJ, et al. Long-term results of two-stage hepatectomy for irresectable colorectal cancer liver metastases. Ann Surg. 2008;248:994–1005.
Saiura A, Yamamoto J, Hasegawa K, et al. Liver resection for multiple colorectal liver metastases with surgery up-front approach: bi-institutional analysis of 736 consecutive cases. World J Surg. 2012;36:2171–8.
Vigano L, Capussotti L, Majno P, et al. Liver resection in patients with eight or more colorectal liver metastases. Br J Surg. 2015;102:92–101.
Vibert E, Pittau G, Gelli M, et al. Actual incidence and long-term consequences of posthepatectomy liver failure after hepatectomy for colorectal liver metastases. Surgery. 2014;155:94–105.
Adam R, Laurent A, Azoulay D, et al. Two-stage hepatectomy: a planned strategy to treat irresectable liver tumors. Ann Surg. 2000;232:777–85.
Brouquet A, Abdalla EK, Kopetz S, et al. High survival rate after two-stage resection of advanced colorectal liver metastases: response-based selection and complete resection define outcome. J Clin Oncol. 2011;29:1083–90.
Lam VW, Laurence JM, Johnston E, et al. A systematic review of two-stage hepatectomy in patients with initially unresectable colorectal liver metastases. HPB (Oxford). 2013;15:483–91.
Karoui M, Vigano L, Goyer P, et al. Combined first-stage hepatectomy and colorectal resection in a two-stage hepatectomy strategy for bilobar synchronous liver metastases. Br J Surg. 2010;97:1354–62.
Narita M, Oussoultzoglou E, Jaeck D, et al. Two-stage hepatectomy for multiple bilobar colorectal liver metastases. Br J Surg. 2011;98:1463–75.
Tanaka K, Shimada H, Matsuo K, et al. Remnant liver regeneration after two-stage hepatectomy for multiple bilobar colorectal metastases. Eur J Surg Oncol. 2007;33:329–35.
Jaeck D, Oussoultzoglou E, Rosso E, et al. A two-stage hepatectomy procedure combined with portal vein embolization to achieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases. Ann Surg. 2004;240:1037–51.
Schnitzbauer AA, Lang SA, Goessmann H, et al. Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Ann Surg. 2012;255:405–14.
Schadde E, Ardiles V, Robles-Campos R, et al. Early survival and safety of ALPPS: first report of the International ALPPS Registry. Ann Surg. 2014;260:829–38.
Torzilli G, Procopio F, Botea F, et al. One-stage ultrasonographically guided hepatectomy for multiple bilobar colorectal metastases: a feasible and effective alternative to the 2-stage approach. Surgery. 2009;146:60–71.
Torzilli G, Garancini M, Donadon M, et al. Intraoperative ultrasonographic detection of communicating veins between adjacent hepatic veins during hepatectomy for tumours at the hepatocaval confluence. Br J Surg. 2010;97:1867–73.
Torzilli G, Procopio F, Donadon M, et al. Upper transversal hepatectomy. Ann Surg Oncol. 2012;19:3566.
Torzilli G. Ultrasound-guided liver surgery. An atlas. 1st ed. Milan: Springer; 2014.
Torzilli G, Montorsi M, Donadon M, et al. “Radical but conservative” is the main goal for ultrasonography-guided liver resection: prospective validation of this approach. J Am Coll Surg. 2005;201:517–28.
Torzilli G, Palmisano A, Procopio F, et al. A new systematic small for size resection for liver tumors invading the middle hepatic vein at its caval confluence: mini-mesohepatectomy. Ann Surg. 2010;251:33–9.
Donadon M, Costa G, Gatti A, et al. Thoracoabdominal approach in liver surgery: how, when, and why. Updat Surg. 2014;66:121–5.
Viganò L, Costa G, Procopio F, et al. Parenchyma-sparing liver surgery for large segment 1 tumors: ultrasound-guided lateral and superior approaches as safe alternatives to major hepatectomy. J Am Coll Surg. 2015;221:e65–73.
Yoshidome H, Kimura F, Shimizu H, et al. Interval period tumor progression: does delayed hepatectomy detect occult metastases in synchronous colorectal liver metastases? J Gastrointest Surg. 2008;12:1391–8.
Machi J, Isomoto H, Kurohiji T, et al. Accuracy of intraoperative ultrasonography in diagnosing liver metastasis from colorectal cancer: evaluation with postoperative follow-up results. World J Surg. 1991;15:551–6.
Agrawal N, Fowler AL, Thomas MG. The routine use of intra-operative ultrasound in patients with colorectal cancer improves the detection of hepatic metastases. Color Dis. 2006;8:192–4.
Chen CH, Lin ST, Yang CC, et al. The accuracy of sonography in predicting steatosis and fibrosis in chronic hepatitis C. Dig Dis Sci. 2008;53:1699–706.
Torzilli G, Botea F, Donadon M, et al. Criteria for the selective use of contrast-enhanced intra-operative ultrasound during surgery for colorectal liver metastases. HPB (Oxford). 2014;16:994–1001.
Nakano H, Ishida Y, Hatakeyama T, et al. Contrast-enhanced intraoperative ultrasonography equipped with late Kupffer-phase image obtained by Sonazoid in patients with colorectal liver metastases. World J Gastroenterol. 2008;14:3207–11.
Uetake H, Tanaka S, Ishikawa T, et al. Fate of metastatic foci after chemotherapy and usefulness of contrast-enhanced intraoperative ultrasonography to detect minute hepatic lesions. J Hepatobiliary Pancreat Sci. 2012;19:509–14.
Torzilli G, Montorsi M, Palmisano A, et al. Right inferior phrenic vein indicating the right hepatic vein confluence into the inferior vena cava. Am J Surg. 2006;192:690–4.
Makuuchi M, Hasegawa H, Yamazaki S, et al. Four new hepatectomy procedures for resection of the right hepatic vein and preservation of the inferior right hepatic vein. Surg Gynecol Obstet. 1987;164:68–72.
Torzilli G, Montorsi M, Del Fabbro D, et al. Ultrasonographically guided surgical approach to liver tumors involving the hepatic veins close to the caval confluence. Br J Surg. 2006;93:1238–46.
Torzilli G, Donadon M, Palmisano A, et al. Back-flow bleeding control during resection of right-sided liver tumors by means of ultrasound-guided finger compression of the right hepatic vein at its caval confluence. Hepatogastroenterology. 2007;54:1364–7.
Torzilli G, Donadon M, Marconi M, et al. Systematic extended right posterior sectionectomy: a safe and effective alternative to right hepatectomy. Ann Surg. 2008;247:603–11.
Kosuge T, Yamamoto J, Takayama T, et al. An isolated, complete resection of the caudate lobe, including the paracaval portion, for hepatocellular carcinoma. Arch Surg. 1994;129:280–4.
Takayama T, Makuuchi M, Watanabe K, et al. A new method for mapping hepatic subsegment: counterstaining identification technique. Surgery. 1991;109:226–9.
Torzilli G, Cimino M, Procopio F, et al. Conservative hepatectomy for tumors involving the middle hepatic vein and segment 1: the liver tunnel. Ann Surg Oncol. 2014;21:2699.
Viganò L, Procopio F, Cimino M, et al. Is tumor detachment from vascular structures equivalent to R0 resection in surgery for colorectal liver metastases? An observational cohort. Ann Surg Oncol. 2016;23:1352–60.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Torzilli, G., Costa, G., Procopio, F., Viganó, L., Donadon, M. (2017). Intraoperative Evaluation of Resectability. In: de Santibañes, E., Ardiles, V., Alvarez, F., Busnelli, V., de Santibañes, M. (eds) Extreme Hepatic Surgery and Other Strategies. Springer, Cham. https://doi.org/10.1007/978-3-319-13896-1_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-13896-1_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-13895-4
Online ISBN: 978-3-319-13896-1
eBook Packages: MedicineMedicine (R0)