
Abstract
Leishmaniases are diseases caused by several species of Leishmania protozoa and occur in all continents, except Antarctica. Almost 20 species have been isolated from humans, and they may cause cutaneous, mucocutaneous, and visceral forms of the disease. The severity of the infection depends on the protozoon species and strain, host immune response, nutritional status, and, to a lesser extent, sand fly species involved in the transmission. Depending on the parasite tropism, amastigotes invade macrophages in the skin, mucosa, and internal organs, mostly the spleen, liver, and bone marrow, causing their depletion. Clinical presentations may vary from localized skin lesions to generalized disease, with fever, weight loss, enlargement of the spleen and liver, anemia, leucopenia, and thrombocytopenia. Transmission primarily occurs by the bites of sand flies, the only proven biological vectors of Leishmania parasites. Secondary transmission routes have been demonstrated in both humans and dogs, including congenital transmission. The epidemiology of leishmaniases is complex, as it involves different vector, host, and parasite species, living in a constantly changing environment. Disease diagnosis and treatment are still complicated, particularly in developing countries. More effective control strategies are urgently needed to reduce the burden of leishmaniases in endemic areas. Meanwhile, education and better living conditions for people residing in risk areas are key to controlling this group of diseases.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Leishmaniases are a group of diseases affecting humans and several other animal species, being widely distributed in all continents, except Antarctica. They cause a major burden in endemic areas, with approximately 1.5 million new cases each year and at least 350 million people at risk in the world. Their distribution is mostly tropical and subtropical, but they are expanding their distribution to new areas in Europe and in the Americas. Due to multiplicity of species of Leishmania, reservoir hosts, and vectors, their epidemiology is complex and should be studied locally to allow the planning of more effective control and prevention strategies.
The infection has been known for centuries, and cutaneous forms have been represented in potteries, “huacos,” in pre-Colombian Andes and were well known in the Mediterranean region as “bouton de Aleppo.” At the end of the nineteenth century, their etiological agents were described, and epidemics of visceral leishmaniasis (VL) occurred frequently associated to famine, for example, in the Indian continent.
Transmission of Leishmania spp. occurs through the bites of sand flies (Phlebotominae), the only proven biological vectors of the parasites, although biting midges infected by Leishmania sp. have been found in Australia. Sexual and congenital transmissions are considered secondary modalities of infection in dogs, as well as transmission via blood transfusion (Freitas et al. 2006). Amastigotes of Leishmania infantum have been found in 34–52 % of discarded syringes of drug addicts in a study in Madrid, which raised the question on possible mechanical transmission among drug users.
The origin of Leishmania was supposed to be South American, ca. 46–36 million of years ago. Then, ca. 14–24 million of years ago, the ancestor of Leishmania donovani and L. infantum would have diverged from other species in Central Asia before being imported from Europe with the conquistadores, about 500 years ago (Lukes et al. 2007).
1 Etiology
Several species of Leishmania can infect humans and other animals causing diseases with different degrees of severity. For example, L. infantum is usually associated with VL but can also cause small cutaneous lesions, whereas species that typically causes cutaneous leishmaniasis (CL) in humans but may eventually invade the viscera, as it is the case of Leishmania amazonensis.
Species of Leishmania have been classified according the localization of developmental stages in the digestive tract of their sand fly vectors and to their biochemical and molecular characters. Therefore, they have been distributed in two subgenera (Leishmania and Viannia) (Table 16.1) , and Leishmania of lizards are included in the subgenus Sauroleishmania. Besides the occurrence of Leishmania in Eurasia, Africa, and the Americas, a Leishmania infecting and causing cutaneous lesions on macropods (kangaroos, wallaroos, and wallabies) has been recently characterized in the north of Australia.
Correct identification of species of Leishmania causing human disease is crucial for a better evaluation of the prognosis of the disease and for planning control strategies. The etiological identification is particularly important in the New World, where several Leishmania spp. may simultaneously occur. Also in the Old World, the etiological diagnosis may be very important for planning strategies to follow. For example, in addition to L. infantum, L. tropica has been implicated in some cases of VL in the south of Iran and Iraq. The utilization of insecticide impregnated collars in dogs in Iran reduced the incidence of L. infantum in both dogs and children, but this strategy would probably have no impact on L. tropica incidence, which emphasizes the need for a precise parasite identification to elaborate proper control strategies.
The etiological diagnosis of leishmaniasis should ideally rely not only on cytological examination of stained smears prepared with material obtained by puncture of cutaneous lesions or viscera but also on the isolation of parasite in culture and characterization by multilocus enzyme electrophoresis or other reference method. In this perspective, molecular techniques are frequently necessary for the correct identification at species level.
Monoclonal antibodies also are useful and can be obtained free of charge from WHO. Nonetheless, they may present cross-reactions among closely related species and are not able to discriminate strain-level differences. Indeed, different L. braziliensis genotypes have been associated to different forms of CL (Schriefer et al. 2004), and, in this perspective, molecular techniques are accelerating and refining the etiological diagnosis of leishmaniasis at both species and strain level.
2 Life Cycle of Leishmania
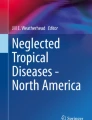
Mammals are usually infected when metacyclic promastigotes are inoculated during the bite of sand flies. Promastigotes are phagocytized by macrophages, in which they become amastigotes (Fig. 16.1), multiplying and eventually destroying them, before invading other macrophages. When amastigotes are ingested by a sand fly (Fig. 16.2) during its blood feeding, they can differentiate in its digestive tract to different promastigote forms (Fig. 16.3). The cycle in sand flies involves at least six forms (amastigotes, procyclic promastigotes, nectomones, leptomones, haptomones, and metacyclic promastigotes) (Kamhawi 2006), but for didactic purposes, only promastigotes are usually referred as occurring in these insects.

Amastigote of Leishmania. Kindly authorized by M. Steindel

Phlebotomine sand fly biting skin. From CDC

Cycle of Leishmania. From CDC
The destruction of macrophages in several parts of the organism will cause several consequences, and the skin, mucosa, and several viscera can be affected, sometimes reducing the host defense against the invaders. The effort of the organism to produce macrophages can reduce the production of erythrocytes and other blood cells, causing anemia with tendency to hemorrhage. If amastigotes are concentrated in the skin and mucosa or abnormal reactions occur, variable lesions can be found. The development of VL or CL will depend on the species of Leishmania involved and several other factors. For example, dogs remain infected for long periods of time and frequently have a high rate of infection with no clinical manifestations even if seropositive. The latter animals are less infectious than dogs with multiple clinical signs. Also, the sand fly species involved in transmission of L. infantum seem to affect the clinical presentation in humans as it does the individual susceptibility and immune response.
3 Clinical Forms of Leishmaniasis
3.1 Visceral Leishmaniasis
3.1.1 Agents
VL is caused by L. donovani (in Africa and Indian subcontinent, where the disease is also known as kala-azar) and L. infantum (in the Mediterranean area, Middle East, China, and Southwest Asia and American continent). In addition, L. amazonensis has been incriminated in some cases in Brazil. Visceralization is usually influenced by several factors, including the biology of the parasite, the host immunological status, and the vector strain.
3.1.2 Disease in Humans and Domestic Animals
The disease is characterized by the development of amastigotes in visceral macrophages, mostly in the spleen, liver, lymph nodes, and intestinal mucosa. After inoculation by the vector, VL evolves for several weeks, with mild symptoms , including fever and enlarged lymph nodes, spleen, and liver, weakening worsened by anemia, immunosuppression due to the destruction of macrophages and deviation of function of hematopoietic tissues, and weight loss. Undernourished children, after a period from 1 month to 1 year, can die, mostly of concurrent infections, like pneumonia, diarrhea, and tuberculosis, which can often confuse the diagnosis.
Although the clinical presentation is similar in endemic areas, enlarged lymph nodes are rarely observed in the Indian continent, while hyperpigmentation , previously common in this region, is today rare. The ratio of asymptomatic infections to clinical cases varies from 1:2.6 in Sudan to 50:1 in Spain and is strongly influenced by species of parasites and nutrition.
In dogs the disease is characterized by usually long incubation periods (from 2 months to years), a systemic evolution due to the infection of macrophages in all tissues and organs and alterations due to an exacerbated immune response with a hyperproduction of antibodies and immunocomplex deposition (e.g., uveitis, vasculitis, and glomerulonephritis).
Although it is difficult or even impossible to identify specific clinical signs for the infection, infected dogs appear in poor body conditions, with enlarged lymph nodes and other nonspecific clinical signs. Dog owners may refer a sudden aging of the animal in a few months. In addition, cutaneous lesions, when present, are characterized by non-pruritic exfoliative dermatitis (large, abundant, and gray scales), alopecia, and skin ulcers at the bony prominences, ear pinnae, and footpad. However, nodular or pustular dermatitis, nose bleeding, colitis, as well as neurological disorders may also occur.
3.1.3 Leishmaniasis-HIV Coinfection
Leishmaniasis can affect the presentation, diagnosis, and course of malignant disorders, sometimes complicating treatment (Kopterides et al. 2007). HIV infection, due to low cell-mediated immune response, mostly if associated to malnutrition, increases risk of developing clinical disease (Chappuis et al. 2007). For example, low CD4+ counts (<100 cells/ml) and the absence of an increase of these cells at follow-up are predictors of VL relapse, when associated to HIV (Cota et al. 2011). Coinfection by HIV can cause different clinical consequences (Table 16.2), and special care with diagnosis and follow-up is necessary. Leishmania-HIV coinfected patients tend to be more frequently malnourished, to have less fever and hepatosplenomegaly, compared to non-HIV-infected ones, possibly complicating initial diagnosis (Cota et al. 2014).
3.1.4 PKDL
In East Africa and the Indian subcontinent, after symptomatic or asymptomatic VL by L. donovani, a skin infection, called post-kala-azar dermal leishmaniasis (PKDL) , develops respectively in 50–60 % and 5–10 % of patients, during or after the treatment. It is characterized by maculopapular, papular, and nodular rash, starting around the mouth and affecting most of the face, trunk, arms, and legs (Zijlstra et al. 2003) (Fig. 16.4). In Indian subcontinent, the nodules tend to evolve to plaques, while in Africa ulceration is frequent (Singh et al. 2011). Eyes can be affected, causing blindness (Khalil et al. 2011).

Post-kala-azar dermal leishmaniasis (PKDL). From WHO
Some cases of PKDL caused by L. infantum were reported from northwestern Iran (Badirzadeh et al. 2013). In Sudan, most cases are spontaneously cured, but in the Indian subcontinent, most need treatment (Zijlstra et al. 2003). Discrepancies between immunohistopathological findings in Indian and Sudanese patients were reported (Zijlstra et al. 2003). Four cases of PKDL in the south of the Brazilian state of Bahia were associated to L. amazonensis.
PKDL is frequently more severe at a younger age and a shorter interval between VL treatments, and has been associated to more severe disease. Differential diagnosis with leprosy, in both areas, must be done; neuritis in small cutaneous nerves in some cases of PKDL may cause some confusion in the differential diagnosis. Besides the clinical importance of PKDL, the patients have been supposed to constitute sources of amastigotes for sand flies in the long term and between epidemics.
Infection by L. infantum in dogs may span from the absence of clinical signs (in even more than 50 % of the infected animals) to skin and ocular lesions, lymph node enlargement, severe weight loss, splenomegaly, onychogryphosis, and renal failure. Other Leishmania species have been implicated in cases of canine VL, including L. colombiensis and L. amazonensis, but the actual clinical and epidemiological relevance of these cases remains uncertain.
3.2 Cutaneous Leishmaniasis
3.2.1 Agents
CL is caused by several species of Leishmania, which varying epidemiology and clinical presentations. L. braziliensis is the most common species in the American continent, but at least 12 other species (L. colombiensis, L. amazonensis, L. garnhami, L. guyanensis, L. infantum, L. lainsoni, L. lindenbergi, L. mexicana, L. naiffi, L. panamensis, L. peruviana, L. pifanoi) can cause cutaneous lesions. In the Old World, L. aethiopica, L. infantum, L. killicki, L. major, and L. tropica besides L. donovani (in PKDL) can cause CL (Table 16.1).
3.2.2 Disease in Humans
After transmission of promastigotes by sand fly bites, usually a small red papule develops, rupturing after some weeks, producing a scaly plate (Fig. 16.5) or more frequently a slowly growing ulcer (Fig. 16.6), which may spontaneously heal. Lesions usually occur in exposed areas, but multiple lesions can be produced by hematogenous or lymphatic dispersion to districts other than those of original bites. In L. guyanensis, transmitted by sand flies associated to large trees, a massive attack by these insects can cause dozens of lesions. Simultaneous to cutaneous lesions or even 20 years after their healing, the nasopharyngeal mucosa can be affected. Nasal lesions are always present, with nodules and infiltration of cartilaginous septum, obstruction of nostril, perforation of the septum, and even total destruction of the nose (Fig. 16.7). In part of the patients, the pharynx, palate, trachea, and upper lip can be affected, with lymphadenopathy. Mucosal lesions are associated to poorly modulated T-cell response, with high levels of IFN-γ and TNF-α and a decreased ability of IL-10 and TGF-β to modulate this response (Bacellar et al. 2002).

Cutaneous lesions caused by L. major . (a) Negev desert. (b) Iran. Kindly authorized by O. Katz and R. Yaghoob

Ulcer caused by L. braziliensis . From CDC

Mucocutaneous leishmaniasis (L. braziliensis) from southern Brazil. Kindly authorized by M. Steindel
Diffuse CL, with several non-ulcerated nodules in all parts of the body, is mostly caused by L. amazonensis in the Amazon region and also by L. braziliensis. Indeed, the latter species may cause disseminated CL, with several papulous, acneiform, and rarely ulcerated lesions, associated to chills and fever, which indicates hematogenous dispersion (Guimarães et al. 2005). Diffused CL is characterized by persistent T-cell anergy. Patients usually present negative results in the leishmanin test and do not respond to therapy with antimonials and amphotericin B, only to pentamidine. In turn, the disseminated CL (Fig. 16.8) is frequently associated with mucosal lesions, with patients being positive in the leishmanin test and responding to amphotericin B therapy but not to antimonials.

Disseminated cutaneous leishmaniasis caused by L. braziliensis, south of Brazilian state of Bahia. Kindly authorized by L. H. Guimarães
Most cases of mucocutaneous leishmaniasis (MCL) have been associated to L. braziliensis and L. panamensis in the New World and to L. aethiopica in the Old World. Leishmania donovani may cause mucosal lesions in Sudan, usually not associated to cutaneous lesions (El-Hassan and Zijlstra 2001). The association to HIV infection favors the onset of diffuse or mucosal forms (Table 16.2).
Cutaneous lesions can become infected by bacteria, being painful and wet, restricting amastigotes mostly to ulcer borders. Antibiotics are frequently the first treatment for many cutaneous lesions, and, although the failure of treatment is not an adequate method of diagnosis, the nonhealing of ulcers after elimination of bacteria by this treatment may raise suspicion of CL. As examples, in Alagoa Grande, in northeastern Brazil, many CL patients referred previous treatment by “a painful injection with a white liquid” (penicillin), before the correct diagnosis,Footnote 1 and a girl with a lesion in the ear in Ecuador had previously been treated by oral ciprofloxacin and clindamycin for 10 days and fusidic acid as a topical ointment, with no improvement (Hinojosa et al. 2013).
Scars derived from CL are atrophic and whiter than the surrounding skin (Fig. 16.9), in consequence more evident in dark skin patients, and amastigotes can be present in the scars, even several years after healing, potentially dispersing through the organism and causing new lesions.

Scar of dermal leishmaniasis from Brazilian state of Pernambuco
3.2.3 Disease in Domestic and Sylvatic Animals
Several species of Leishmania can cause lesions similar to those observed in humans, mostly in domestic animals (Fig. 16.10) , but amastigotes can be present in intact skin, mostly in sylvatic animals, facilitating the infection of the vectors. Besides cutaneous lesions observed in VL by L. infantum (e.g., non-pruritic exfoliative dermatitis with large, abundant, and gray scales, alopecia, skin ulcers at the bony prominences, ear pinnae, footpad), L. braziliensis, L. peruviana, and other species which cause CL in humans may also induce localized skin lesions in dogs (Dantas-Torres 2009). Most of the dogs infected by L. braziliensis live in rural areas, and they may present single cutaneous or mucosal lesions. Their role as spreaders of the infection to humans has been suspected even if it is actually only minor.

Cutaneous lesions in dogs : (a) L. braziliensis (American continent); (b) L. major (Iran). Kindly authorized by CDC and R. Yaghoob
4 Diagnosis
The diagnosis of visceral and CL in humans and dogs is a complex task, which relies on several aspects (e.g., anamnesis, epidemiology, clinical presentation, and laboratory findings), including laboratory evidence of infection, which ultimately drives the clinician from a suspicion to the direct or indirect confirmation of the infection. Indeed, before clinical examination laboratory testing, data on the provenience, age, sex, attitude, and lifestyle of the patient as well as the occurrence of other concomitant infections needs to be carefully considered in order to appreciate the likely risk of infection. After this preliminary assessment and a complete clinical examination, parasitological, serological, and/or molecular tests should be requested to confirm the diagnosis.
4.1 Clinical Diagnosis
In human medicine, long-term low fever, associated to hepatosplenomegaly, lymph node enlargement, and anemia, mostly in known endemic areas, raises the suspicion of VL. An adequate comparative diagnosis has to be made with other diseases, like schistosomiasis, mononucleosis, AIDS, malaria, and other diseases with similar presentation.
CL must be suspected for cutaneous lesions, mostly localized in regions of the body not covered by clothes and/or in patients potentially exposed to sand fly bites, with more than 1 month of development. The appearance of lesions, if an ulcer has already developed, may lead to suspect CL. However, lesions characterized by several nodules following the trajectory of lymphatic vessels and simulating sporotrichosis may finally conduct to the diagnosis of an infection by L. guyanensis (Hinojosa et al. 2013). Atypical manifestations (erysipeloid, recidiva cutis, and disseminated CL) were related to L. panamensis in Ecuador.
In MCL caused by L. braziliensis and L. panamensis in New World and L. donovani in Sudan, mucosa and cartilaginous parts of the nose and nearby areas are largely compromised. The PKML is differentiated from several other diseases by histopathology and appropriate laboratory tests. Less often, mucosa of other regions of the face, like tongue and lips, is affected (Mignogna et al. 2014), and dentists can collaborate on the diagnosis. Allergic rhinitis, histoplasmosis, cancrum oris, lymphoma, and other neoplasia, leprosy, and sarcoidosis may mimic this form of leishmaniasis, and parasitological, immunological, and molecular techniques should drive physicians to the correct etiological diagnosis. The presence of concomitant or previous cutaneous lesions may be suggestive for MCL.
Clinical signs in canine leishmaniasis (CanL) are often inconsistent being primarily characterized by emaciation, enlargement of peripheral lymph nodes, non-pruritic exfoliative dermatitis with alopecia and also nodular or pustular dermatitis, lesions of mucous membranes (nodules and ulcers), and ocular lesions (blepharitis, keratoconjunctivitis, uveitis). Also laboratory abnormalities, such as hyperglobulinemia (polyclonal beta and/or gammaglobulinemia), hypoalbuminemia, and decreased albumin/globulin ratio, may be suggestive of CanL. Clinical CanL is characterized by a wide spectrum of clinical signs, which may occur alone or in combination, and severity (e.g., weight loss, lethargy, muscular atrophy, anemia, lymphadenomegaly, splenomegaly, epistaxis, diarrhea, renal disorders, ocular lesions, polyarthritis, onychogryphosis, and skin lesions). Importantly, in endemic areas, a large number of subclinical infections have been recorded in dogs and humans. Despite the conflicting results of different studies regarding the infectiousness of asymptomatic versus sick dogs, the former may eventually serve as a source of infection to sand fly vectors, albeit to a lesser extent in comparison with sick dogs. The diverse presentation of disease in infected animals is primarily linked to the many pathogenic mechanisms involved and the immune response elicited in the host, which ultimately make the diagnosis of infection in clinically healthy but infected animals challenging.
4.2 Parasitological Diagnosis
Cytological examination of Giemsa-stained smears prepared with bone marrow aspirates, preferentially from sternum, is usually useful for the diagnosis of VL. Liver and spleen aspirates may be productive but are too risky. HIV patients, mostly if severely immunosuppressed, may present other opportunistic infections, which may complicate the diagnosis. In these patients, the parasite load is higher, sometimes in unusual sites. All patients with unusual presentations of leishmaniasis need to be tested to HIV.
For the parasitological diagnosis of CL, samples can be obtained, with adequate local anesthesia, from skin lesions by slide impression, biopsy, or aspiration from the border of the ulcer, which are richer in protozoa and less contaminated by bacteria. The material obtained from skin lesions should be smeared on a glass slide, stained by Giemsa or similar. Other preparations with staining adequate for fungi and culture media can be utilized for diagnosis of concomitant or alternative infections. It can also be inoculated in the snout, feet, or peritoneal cavity of laboratory animals, preferably the golden hamster, for in vivo isolation and subsequent identification, mostly in reference laboratories. Nonetheless, with the advent of molecular techniques, the biological isolation is not any more commonly employed, also due to ethical reasons. In vitro culture, although reliable, is prone to microbiological contamination, especially if skin samples or samples collected under field conditions are used.
In MCL, parasites are usually rare, and detection of parasite DNA by PCR is a sensitive method for diagnosis. Amastigotes are particularly easy to find in cutaneous lesions in PKDL (Singh et al. 2011) and in those caused by L. amazonensis, but monoclonal antibodies and molecular techniques should be utilized in case of negative results.
The observation of amastigotes by cytology or histology in lymph node or bone marrow samples is often used for diagnosing CanL. Cytological examination is a straightforward method, though time-consuming, but may lack in sensitivity, particularly in asymptomatic dogs. Thus, a negative cytological examination does not exclude the possibility of infection in a dog with suspicious CanL. As far as histology, it may present high sensitivity if immunohistochemistry is performed.
4.3 Immunological Diagnosis
Indirect immune fluorescence test (IFAT) and mostly enzyme-linked immunosorbent assay (ELISA) displayed good performance in terms of sensitivity and specificity for the diagnosis of VL but require equipments that are not adapted to field conditions. Conversely rapid immunochromatographic tests (ICT) are well adapted for field utilization. Persistent positive reactions are a limitation of all serological tests, and these tests must always be utilized in conjunction with adequate clinical evaluation.
Leishmanin skin test (Montenegro reaction) (injection of a suspension of killed Leishmania promastigotes sonicated and kept in merthiolate solution at 1:10,000, with a volume of 0.1 mL of the antigen with 40 μg/mL of nitrogen) is usually positive from 1 month after infection, for most cases of CL, except those of anergic diffuse CL, mostly caused by L. amazonensis, and some cases of disseminated CL, and continues to be positive even after cure.
IFAT can detect both symptomatic and asymptomatic dogs, and it is widely used in large screening surveys. Among serological tests, IFAT still represents one of the most widely used serological techniques for diagnosing CanL, even if this technique has recently been replaced by Immunochromatographic Strip Test (ICT) in Brazil, for example. However, the definitive diagnosis of L. infantum infection in asymptomatic dogs is troublesome since both serological and parasitological methods have inherent limitations, especially in terms of sensitivity in this particular group of animals. Indeed, serology may not be a good indicator of infection in cross-sectional studies due to the varying time spanning between infection and seroconversion (i.e., from 1 to several months).
For HIV-VL patients, different serological tests (e.g., IFAT and ELISA) have shown variable, often low, sensitivities and specificities in the Mediterranean region (Monge-Maillo et al. 2014) and in Latin America (Lindoso et al. 2014). Nonetheless, tests such as immunoblotting and direct agglutination test (DAT) have shown better results for the diagnosis of VL in this group of patients (Monge-Maillo et al. 2014; Lindoso et al. 2014)..
4.4 Molecular Diagnosis
A number of PCR assays such as conventional and real-time PCR on various tissues, including blood, lymph node, bone marrow, and spleen, have improved the sensitivity of the diagnosis of Leishmania infection in both animals and humans. PCR methods have been standardized for the amplification of several target genes including genomic DNA of the internal transcribed spacer 1 (ITS1) region of the ribosomal RNA (rRNA) and kinetoplast DNA (kDNA) minicircle sequence. For sure the sensitivity of the PCR is correlated with the number of copies of target genes and with the type of samples used. For example, PCR tests of material obtained from bone marrow, lymph nodes, and the skin are preferred samples in relation to blood. Refined techniques, such as real-time PCR and loop-mediated isothermal amplification (LAMP), further increased the sensitivity and specificity of the molecular diagnosis of leishmaniases.
Although the use of molecular diagnostic techniques has become widespread in recent years, they are still mostly restricted to urban centers and to reference laboratories. The lack of standardization of molecular assays is a problem in both private and public laboratories. Scientists should endeavor to standardize the protocols, including target genes, primers, amplification conditions, and samples to be tested in order to make studies comparable and to standardize the diagnosis of the disease in both developing and developed countries.
For HIV-VL patients, real-time PCR (qPCR) is indicated to predict relapse after treatment; parasite loads >0.03 and 0.9 parasites/mL, respectively, at 3 and 12 months after treatment indicate 100 % of probability of a relapse (Lindoso et al. 2015).
5 Treatment
Treatment should be started soon after the diagnostic confirmation, and, in areas where different Leishmania species may occur, the diagnosis should ideally be at species level. National and regional guidelines provided by public health authorities should be followed. Early diagnosis and treatment are essential to prevent mucosal lesions and parasite dissemination.
There are several drugs and protocols for treatment, and the choice will depend on the clinical form, species of Leishmania, and other factors, like concomitant diseases and malnutrition. More detailed schemes must be easily chosen in WHO’s (2010) review. Some more usual drugs and schemes are referred below.
5.1 Pentavalent Antimonials
Meglumine antimoniate (8.1 % of Sb5+) and sodium stibogluconate (10 % of Sb5+) selectively inhibit leishmanial glycolysis and fatty acid oxidation. Their toxicity is similar, and they must be injected intravenously or intramuscularly, by infusion (5–10 min) or through a fine needle (23–25 gauge) to avoid the risk of thrombosis. Anorexia, abdominal pains, nausea, vomiting, headache, and other symptoms are usual. Electrocardiographic changes, depending on the doses and duration of treatment, including T-wave inversion, prolonged Q-T interval, and arrhythmia, are the most common, and, rarely, cardiotoxicity and sudden death can occur. The prolongation of Q-T interval signals the onset of serious and fatal arrhythmia. The rise of pancreatic enzymes, but not clinical pancreatitis, is common. Elevated liver enzyme concentration, leucopenia, anemia, and thrombocytopenia are not uncommon. Patients must be monitored for serum chemistry, complete blood counts, and electrocardiography. If serious side effects arise, mostly hepato- and cardiotoxicity, the drug must be changed. Mortality on VL-HIV patients is particularly high when treated by antimonial, and WHO recommends utilizing liposomal amphotericin B for these individuals.
Association of immunotherapy by the injection of dead promastigotes of L. amazonensis to antimonial reduced the doses and length of treatment of infections by L. braziliensis in Brazil (Mayrink et al. 2006). Antimonial association with pentoxifylline, an inhibitor of TNF-α, decreased the inflammatory reaction responsible for the tissue damage in mucocutaneous lesions.
5.2 Amphotericin B
It acts by binding to ergosterol in the parasite’s cell membrane and altering its permeability. However, their use is limited by the nephrotoxicity and might endanger dogs with CanL that already have existing renal pathology. Treatment must always be given in hospital, for continuous monitoring of patients. Amphotericin B deoxycholate may be replaced by lipidic formulations, equally efficacious but less toxic.
5.3 Pentamidine
This drug has been utilized in French Guiana for CL caused by L. guyanensis, usually not very responsive to treatment by antimonials, but the high doses (>2000 mg) necessary for the treatment of MCL can cause diabetes mellitus. Even one dose of 200 mg can cause glicosuria and hyperglycemia, and blood sugar and glycemia must be carefully checked.
5.4 Milfetosine
Milfetosine was originally an oral anticancer drug, shown to have good antileishmanial action. Gastrointestinal side effects can force a temporary interruption of treatment, and it can have some hepatotoxicity and is potentially teratogenic.
5.5 Intralesional Treatment
It seems to be more efficient in curing cutaneous lesions caused by L. major than by L. tropica (Minodier et al. 2005). However, an efficacy of 75.2 % and 97.2 % in curing L. tropica infection was obtained in Afghanistan and Turkey, respectively. The injections are painful and the quantity of material can attain 1 L (Minodier et al. 2005). In a study in state of Rio de Janeiro performed on patients infected by L. braziliensis (Oliveira-Neto et al. 2008), intralesional treatment achieved good results (80 % of healing after 12 weeks), without relapses or mucosal lesions in 10-year observation; nevertheless such treatment, due to the risk of mucosal lesions caused by L. braziliensis and L. panamensis, would not be recommended for leishmaniasis treatment in the New World, except for L. mexicana (Blum et al. 2004).
5.6 Others
Cryotherapy and heat for cutaneous lesions and natural products have been tested and deserve additional studies.
As far as CanL treatment, there are different standardized therapeutic protocols in Europe, with first- and second-line drugs (reviewed in Solano-Gallego et al. 2011). The most frequently used drug combinations are meglumine antimoniate plus allopurinol and miltefosine plus allopurinol. Both meglumine antimoniate and miltefosine are registered for veterinary use in most European countries. The prognosis depends mostly on the clinical staging and on the protocol used. Whenever possible, medicines primarily used for treating humans should be avoided in dogs. For example, amphotericin B is rarely used for dogs in Europe, as this is the main drug used for humans. The Ministry of Health in Brazil is against the treatment of CanL with drugs currently used for humans, to prevent the development of resistance, but there is an intense debate on this issue currently in Brazil.
6 Epidemiology
Detailed reviews of distribution of all human-infecting species of Leishmania, their vectors, and reservoirs were recently published by WHO (2010) and Ready (2013).
VL is the disease of the poorest of the poor, mostly in Indian subcontinent and eastern Africa. The density of Ph.Footnote 2 argentipes in houses in the Indian subcontinent has been shown to be related to the quality of houses, dampness of floor, presence of animals in and around houses, and socioeconomic conditions, and these factors are also important for endophilic vectors. Poverty, including poor housing and peridomestic sanitary conditions and difficult access to healthcare, may help increasing vector populations and their contact with humans, causing more disease and hampering treatment. VL is more frequent in populations living in poor suburban areas, where vectors and reservoirs may be abundant.
Leishmania transmission is influenced by several meteorological and behavioral factors related to complex epidemiology, contact between vectors and reservoirs, and human biting. Topography and vegetation coverage are very important risk indicators. For example, human-sand fly contact is increased in villages situated in rock hills and river banks in East Africa, in areas of transmission of L. aethiopica (WHO 2010), and houses situated in the periphery of a village in French Guiana, near primary forest, had a higher incidence of infection by L. guyanensis.
A recent comprehensive review listed 42 species of Phlebotomus in the Old World and 56 of Lutzomyia Footnote 3 in the New World as vectors of Leishmania spp. (Maroli et al. 2013). Nonetheless, different criteria have recently been proposed for the incrimination of sand fly species as vectors of Leishmania spp., and currently there is no consensus (Maroli et al. 2013; Ready 2013). In any case, the diversity of potential vectors of Leishmania is remarkable.
6.1 Visceral Leishmaniasis
Although VL is known from 74 countries, 90 % of cases occur in six countries: India, Bangladesh, Sudan, South Sudan, Ethiopia, and Brazil. VL is mostly caused by L. infantum (synonymous of Leishmania chagasi or Leishmania infantum chagasi) and L. donovani, but other species such as L. tropica and L. amazonensis can also invade viscera and cause VL. The disease caused by L. infantum is a zoonosis, whereas that caused by L. donovani is a zoonosis in East Africa and an anthroponosis in the Indian continent.
VL causes an estimated 50,000 deaths annually, a rate only surpassed by malaria among protozoal diseases, with 2,357,000 disability-adjusted life years (DALY). Since a great proportion of cases is asymptomatic or undiagnosed, the estimate of 0.5 million new cases annually (WHO 2010) may be an underestimate.
In Europe, VL by L. infantum occurs in the Mediterranean region. Dogs are considered to be the main reservoirs of the parasite, but other animals including foxes (Vulpes vulpes), black rats (Rattus rattus), and hares (Lepus europaeus and Lepus granatensis) have also been found naturally infected and suspected to play a role in the epidemiology of VL. Humans and cats may also infect sand flies. VL in this region is mostly restricted to children, but adults became half of the total number of infected patients, when HIV positive. Leishmania infantum, besides causing VL, has also been incriminated as the agent of CL in several countries around the Mediterranean Sea and in Kyrgyzstan and Mauritania. Due to the dog and human traveling and dog relocation from southern to central Europe, the disease has the potential to spread to northern temperate areas, mostly in Austria,Footnote 4 Switzerland, and Germany, where potential vectors may occur. Parasites are usually transmitted by Ph. ariasi and Ph. Perniciosus in France, these plus Ph. perfiliewi and Ph. neglectus in Italy, and some others have also been suspected as vectors in other countries. VL caused by L. infantum is widely distributed in Central Asia and China, and several species of Phlebotomus (Larroussius) are suspected as vectors (Ready 2013).
In the Middle East (a poorly defined region from Turkey to AfghanistanFootnote 5), several species of Leishmania may cause VL and CL, and many vectors and reservoirs for L. infantum (e.g., dogs and rodents) are known to occur. For example, L. tropica and mostly L. infantum have been isolated from human VL patients, being the latter isolated from wild hamsters along with L. donovani.
Circa 4500–6800 cases per year of VL occur in the American continent (Alvar et al. 2012), of which 96 % occur in Brazil . The disease, previously found mostly in the northeastern Brazil, is nowadays present in all regions, including in center-west and southeast, and it expanded into several medium and large cities, such as Campo Grande and Belo Horizonte. VL is also spreading in northern Argentina and Paraguay, Colombia, Venezuela, and some Central American countries. Lutzomyia longipalpis is the primary vector in most VL foci in Latin America. However, other species such as Lutzomyia cruzi (in Brazil), Pifanomyia evansi (in Colombia), and Migonemyia migonei (in Argentina and Brazil) may also be involved in some foci, mostly in areas without L. longipalpis.
Dogs are important reservoirs and wild dogs and opossums have sometimes been found infected; infectivity of wild dogs for sand flies is considered negligible for the introduction of parasites in new areas in Amazon region. The role of chickens in the epidemiology of VL is considered ambiguous, because they may contribute for increasing domestic populations of L. longipalpis, but they may also potentially reduce the number of sand fly bites on potential reservoirs, thus acting as zooprophylatic agents.
VL caused by L. donovani is distributed through northeastern India, Bangladesh, Bhutan, and Nepal, where Ph. argentipes, a sand fly mostly associated to cattle, is the primary vector. Antibodies against Leishmania and sand fly saliva have been detected in cattle but no parasite DNA was found. Similarly, 3.1 % of tested goats in Bihar (total number 867) reacted to rK39 antigen, and 20 of them had Leishmania DNA; the recent finding of goats infected by L. donovani (Singh et al. 2013) and the lack of scientific evidence (Singh 2014, pers. commun.) enhance the need to more thorough studies on the occurrence of the infection in this animal species. Cases of VL and/or CL attributed to L. donovani have also been found in some Middle East countries (Israel, Iraq, Saudi Arabia, Yemen), in China, and in Europe (Ukraine) (WHO 2010). In the East of Africa, the disease, also caused by L. donovani, is widely distributed, causing many cases and mortality, mostly in Sudan; in Acacia balanites forest, it is transmitted by Ph. orientalis, while Ph. martini s.l. is the vector in savanna with termite mounds (Ready 2013). Epidemics are related to mass migrations, malnutrition, and associated diseases. Infection of 6.9 % Ph. orientalis was observed, and mongooses were suspected as reservoirs in Dinder National Park, which is currently inhabited. Although dogs are very attractive to Ph. orientalis and may become infected by L. donovani, they are not considered as important reservoirs of this parasite.
HIV pandemic influenced the occurrence of leishmaniasis, mostly of VL. In Europe, HIV patients living in rural areas are highly exposed to the risk of infection and disease development (Desjeux and Alvar 2003). In Brazil, the dissemination of HIV from big cities to smaller ones and rural areas overlapped with the distribution of leishmaniasis (Rabello et al. 2003). As a consequence, from 2001 to 2012, the incidence of VL-HIV increased tenfold in Brazil, possibly also influenced by the improvement of HIV diagnosis (Lindoso et al. 2014).
6.1.1 Other Modes of Transmission
The role of ticks and fleas as possible vectors of L. infantum has been suspected, mostly in areas in the absence of the proven sand fly vectors. However, caution is needed before considering any of these arthropods as actual vectors of this parasite. Although L. infantum may remain viable in other arthropods, there is no proof that they may act as vectors.
Several observations of congenital transmission of L. donovani and L. infantum in humans (Figueiró-Filho et al. 2004) and of L. infantum in dogs in the USA have been reported (Petersen and Barr 2009). In an early study, no infection was confirmed in 63 puppies from 18 naturally L. infantum-infected female dogs from Belo Horizonte, Brazil. Later on, a study reported a vertical transmission in Brazil, as confirmed by PCR and immunohistochemistry techniques in samples from the spleen and liver of two stillborn pups from a female dog naturally infected with L. infantum. For VL cases in dogs in the east of the USA and Canada, congenital and venereal transmission should also be suspected, even if Psathyromyia shannoni is susceptible to infection and widely distributed in these areas. Lesions in the genital tract of male dogs positive for L. infantum and the presence of Leishmania in 13/15 (86.6 %) dogs indicate the possibility of venereal transmission.
The recent finding in Finland of three autochthonous cases of VL in dogs, probably infected through contact to a dog that visited Spain, emphasizes the possibility of direct transmission of the parasite and the need of attention to the possibility of occurrence of disease in areas without sand flies.
High prevalence of VL was observed in hemodialysis patients and blood donors in Natal (Luz et al. 1997), a low-endemicity area in Brazil, while several cases of transmission of Leishmania through blood transfusion in humans have been reported (Cardo 2006). Intravenous drug users are at greater risk of infection by HIV and by Leishmania/HIV in southwestern European countries (Desjeux and Alvar 2003). Transmission by blood transfusion among dogs was reported in Brazil and in the USA. Overall, these reports indicate the occurrence of secondary modes of transmission, but their actual epidemiological significance is still poorly understood.
6.2 Cutaneous Leishmaniasis
CL is widely distributed and in expansion in all continents, possibly influenced by human activities, like agricultural projects, deforestation, and migration, and climate changes. Several species of Leishmania can cause CL, and new species are likely circulating among sylvatic mammals, possibly infecting humans in the future. For example, a new species, L. siamensis, has been associated to VL, CL, and disseminated CL in HIV-infected humans in Thailand, and a similar species was found infecting horses in central Europe. The epidemiology of CL is extremely variable and is briefly described below.
In the New World, L. braziliensis causes most cases of CL and is broadly distributed. It is transmitted by several species of sand flies , both by sylvatic species like Psychodopygus wellcomei and Ps. complexus and by those well adapted to domiciles, like Nyssomyia intermedia, Ny. neivai, and Ny. whitmani. Rodents are considered important reservoirs, but opossums and other mammals have been found infected; dogs may be infected but do not seem to constitute good reservoirs (Dantas-Torres 2007); cats and donkeys also have been found infected.
Leishmania mexicana is found in Central America and has been mostly associated to Ny. olmeca. The closely related L. amazonensis, in the Amazon region, is associated to floodable areas (“igapós”) and transmitted mostly by Bichromomyia flaviscutellata, whose preference to bite rodents may explain its low incidence in humans; it has also been found in other regions of Brazil and nearby countries, with unknown vectors and reservoirs.
Leishmania guyanensis occurs in forested areas in Argentina, Bolivia, Brazil, Colombia, Ecuador, French Guiana, Guyana, Peru, Suriname, and Venezuela. Sloths (Choloepus didactylus) and anteaters (Tamandua tetradactyla) are the main reservoirs. The most important vector is Ny. umbratilis, which can bite in great numbers when humans invade their microhabitat (around trunks of large trees). Leishmania panamensis, distributed in Central America and eastern Ecuador, is mostly associated to preserved forests, with sloths as reservoirs and sand flies of Nyssomyia and Psychodopygus as major vectors. Transmission has also been confirmed in peridomestic environments of Andean valleys with coffee plantations in Colombia. Other species, like L. peruviana, occurring in high Andean valleys in Peru, and L. colombiensis, occurring in forests in Colombia, Panama, and Venezuela, have a more restricted distribution.
In the Old World, L. tropica causes anthroponotic CL (ACL) in India, Central Asia, the Middle East (from Afghanistan to Israel and Syria), and Morocco; cases are found predominantly in densely populated settlements, transmitted among humans by Ph. sergenti, and patients with leishmaniasis recidivans can be infective for sand flies for several years. In the same areas, sporadic cases of CL caused by L. tropica have been associated to other reservoirs, mostly hyraxes. In the focus at Rajasthan desert, in the northwest of India, cases of CL are caused by L. tropica, but some cases in the state of Himachal Pradesh are caused by L. donovani, and cases of CL caused by this species have been reported from Kenya, Nepal, and Sri Lanka.
Leishmania major causes zoonotic CL (ZCL), mostly associated to arid regions, with gerbils (Rhombomys opimus and Psammomys obesus) as reservoirs in Central Asia, North Africa, and Palestine, besides sub-Saharan areas; in most regions, Ph. papatasi has been incriminated as the major vector, but Ph. duboscqui in sub-Saharan Africa and probably Ph. salehi in southeast Iran, Pakistan, and northwest India may be vectors (Ready 2013).
7 Control and Prophylaxis
7.1 Visceral Leishmaniasis
Control of VL requires variable strategies according to parasites involved and to disease epidemiology. In all foci, active detection of human cases and treatment, besides improvement of nutrition, is highly recommended to reduce mortality and morbidity.
In L. donovani -caused VL at Indian subcontinent, treatment of human patients and control of Ph. argentipes by the utilization of DDT in houses and animal sheds reduced the incidence, during and after the control of malaria. However, restriction of DDT utilization and the appearance of resistance in sand flies, besides operational difficulties and resistance to drugs, complicated VL control in this subcontinent. The presence of cattle near houses has a doubtful effect on control, because they can deviate biting from humans, but the production of dung can increase populations of sand flies. The utilization of impregnated bed nets has had a partial effect on quantity of bites (Gidwani et al. 2011), causing variable reduction of incidence. Since PKDL and asymptomatic patients constitute a good source of parasites, they also need to be adequately managed. Although infection of goats and oxen by L. donovani has been found in some Indian foci, their role as reservoirs needs to be established.
In the African foci of VL caused by L. donovani , control depends on the biology of vectors and reservoirs. Since this parasite is transmitted by exophilic vectors, application of insecticides on termite mounds (for Ph. martini) needs to be adequately evaluated. The use of insecticide-treated bed nets reduced the number of bites of Ph. martini and the incidence in Sudan, and a good effect was also obtained with permethrin-impregnated curtains in Kenya. Passive diagnosis and treatment are important to reduce mortality and morbidity, but the influence on transmission is unknown. In densely populated areas, mostly with nonimmune migrants (or refugees), spraying of houses may be necessary; though the actual effect in the long term has not been fully evaluated.
In the American continent, the association of elimination of positive dogs; spraying walls of houses, henhouses, and kennels with insecticides; and treatment of human cases was proposed in the 1950s and has been extensively applied. However, difficulty on the elimination of dogs, restriction of the utilization of DDT, and poor effect of pyrethroids on L. longipalpis has jeopardized control, stimulating the discussion on the use of DDT for the control of VL in Brazil (Marcondes and Costa 2014).
The application of insecticides in the environment may have momentary effect, but they are usually unsustainable in the long term for technical and economic reasons. Importantly, environmental and human health hazard concerns around the employment of organochlorines and other chemical groups (e.g., organophosphates and carbamates) have spurred their substitution by synthetic pyrethroids (e.g., α-cypermethrin, cypermethrin, deltamethrin, and λ-cyhalothrin), which are currently used by public health authorities, usually when human cases are reported and a high density of sand flies is found nearby human habitations. Other compounds have shown promising results under laboratory conditions, but their use under field conditions need to be better assessed. For example, azadirachtin , a secondary metabolite present in neem seeds, was demonstrated to be a potent growth inhibitor (for larvae) and a potent sterilizer (for females) that could be used against L. longipalpis. Nonetheless, the limited information on the breeding sites of this vector currently impairs its utilization, at least, to control pre-imago stages. In any case, the insecticidal spraying should also be associated with the elimination of microhabitats favorable to sand fly development (e.g., crevices and cracks on the walls and humid soil in shaded areas).
In foci of VL caused by L. infantum with dogs as known or assumed reservoirs, infection in dogs should be monitored. The World Health Organization recommends that the management of infected dogs should be treatment or elimination. In the same way, stray and feral dog populations should be controlled, even if these actions may not be enough to control the disease, also due to the presence of other reservoirs (WHO 2010). On the other hand, the use of topical insecticides on dogs may reduce the infection in both dogs and humans (Otranto and Dantas-Torres 2013). Both laboratory and field studies have demonstrated the efficacy of different products currently available in the veterinary market. For instance, a spot-on formulation of permethrin plus imidaclopridFootnote 6 has been highly effective in preventing L. infantum infection in dogs in Italy under field conditions for 1 month. Similarly, different studies have proven the usefulness of collars containing deltamethrin or flumethrin plus imidacloprid in protecting dogs from L. infantum infection for up to 8 months (Killick-Kendrick 1999; Otranto et al. 2013). Laboratory studies showed an anti-feeding effect on sand flies ranging from 84 to 96 % and an insecticidal activity of near 100 %, in the few fed females. Field studies demonstrated that a collar containing 4 % deltamethrin (Maroli et al. 2010) and a spot-on formulation with 10 % imidacloprid and 50 % permethrin reduced the risk of L. infantum infection in dogs. Furthermore, the field efficacy of a new collar containing 10 % imidacloprid and 4.5 % flumethrin was also demonstrated in different studies in southern Italy. Altogether, these results indicate the usefulness of topical insecticides to prevent L. infantum infection in dogs in endemic areas. Nonetheless, the large-scale use of these collars may be impaired by several factors, including operational, economic, and political reasons, particularly in developing countries.
As aforementioned, the treatment of dogs suffering from VL is routinely performed in Europe, where different drugs have been marketed for use in dogs, including meglumine antimoniate and miltefosine . The main objective of the treatment of dogs is to promote clinical cure, prevent relapses, and reduce parasite burden. All dogs, under treatment or not, must also be treated with repellents to reduce the risk of reinfection and of transmission to sand flies. While the reduction of transmissibility is not the primary objective of the treatment, studies have demonstrated that some drug combinations were effective in blocking the transmission of parasites to sand flies (Miró et al. 2011).
Removing positive dogs has been practiced for over 50 years in Brazil, but both practical and scientific evidence indicates that this strategy should be replaced by more effective ones, such as the use of topical repellents. Several factors may explain the inefficacy of dog culling for the control of VL, including delay between sample collection and dog removal, rapid replacement of removed dogs by susceptible puppies, high number of dogs daily exposed to infected sand fly bites, presence of other reservoirs, lack of infrastructure and human resources, among others. Mathematical models have indicated that the control of insect vectors and reduction of infectivity of reservoirs are more efficient than dog culling for controlling human VL (Dye 1992).
Vaccines for dogs may be very useful for reducing the risk of disease development but has limited impact on the risk of infection, as vaccinated dogs remain exposed to sand fly bites. To date, three vaccines have been registered for use in dogs, two in Brazil (Leishmune® and Leish-Tec®), and one in Europe (CaniLeish®); the license for one of these vaccines (Leishmune®) has recently been suspended in Brazil. When exposed to infection, vaccinated dogs usually are less prone to disease development, and even if the infection is established, they are less infectious to sand flies. Indeed, these vaccines represent an additional tool for the prevention of CanL, but it is important to emphasize that the use of repellents and/or fast-killing insecticides is the simplest and most effective way to reduce the risk of infection in dogs. While the use of repellents and vaccines can undoubtedly reduce the risk of infection and disease development in dogs, further studies are necessary to better quantify their impact on the incidence of the disease in humans in different epidemiological contexts.
7.2 Cutaneous Leishmaniasis
Control of CL depends on the epidemiology of disease in each area. Personal protection, including the utilization of impregnated bed nets and repellents, is useful for reducing the exposure to sand fly bites and the risk of infection by most species of Leishmania.
In the anthroponotic cycle of L. tropica, diagnosis and treatment of infected humans, associated to insecticide use on houses and annexes, and reduction of potential breeding sites for the vectors, by asphalting streets and covering the soil of backyards with bricks, are considered efficient strategies. Control must be carefully planned to effectively reduce the global number of cases, and not only temporarily reducing the risk of infection in children (WHO 2010).
In foci of L. major with Rhombomys as reservoirs, the control of rodent colonies by plowing or poisoning and by preventing colonization or reinvasion by artificial (irrigation canals) or natural barriers has led to very good results in the former USSR. However, for foci with Psammomys in the Middle East and Tunisia, this strategy has been difficult to implement. Control of CL caused by L. aethiopica in the East of Africa has been obtained by the control of hyraxes around houses, and breeding rabbits (which are very attractive to Ph. papatasi but not susceptible to L. major infection) around houses was proposed for the control of L. major in rural areas in Tunisia.
In the New World, indoor and peridomestic transmission of L. peruviana and L. braziliensis has been controlled by the utilization of insecticides on houses and annexes, but for the later and for other species present in the forests, personal protection by repellents and clothes is the only available prophylactic measure. Spraying insecticides on large trees caused a temporary reduction of the quantity of vectors of L. panamensis and L. guyanensis, respectively, in Panama and Brazil, but this method is obviously not viable for large-scale use. Although deforestation around villages in Panama and French Guiana was efficient to reduce infection by L. panamensis and L. guyanensis, respectively, such modification has a doubtful effect on the transmission of L. braziliensis, due to replacement of vectors (sylvatic → intermediate → domestic). Although the reduction of humidity and shadow around houses and removal of pigsties and henhouses reduced the quantity of potential vectors in the Brazilian state of Paraná (Teodoro et al. 2004), the direct association between sand flies and garbage is doubtful.
8 Conclusion
Due to the multifaceted epidemiology and local nature of leishmaniases, control strategies must be adequate to local situations, being very difficult to propose general rules. Knowledge on the Leishmania species circulating in humans, reservoirs, and sand flies in a given area is necessary to attain efficient control. Information on the local ecology of vector species, seasonal fluctuation, and frequency of contact with humans and reservoirs and blood feeding patterns is primordial before any hope of control.
As a matter of fact, leishmaniases remain neglected diseases that affect disproportionally the poorest of the poor. Therefore, better living conditions, including adequate housing and food supply, are a priority for affected populations living in endemic areas in Latin America, Africa, and Asia. Last but not least, education is fundamental to provide affected populations with information on disease prevention and control. Without access to healthcare and information diseases such as leishmaniases will remain one of the main Achilles’ hells of public health in developing countries.
Notes
- 1.
Personal observation (CBM)
- 2.
Special abbreviations (Marcondes 2007), similar to those for mosquitoes, were utilized for sand fly genera.
- 3.
Lutzomyia lato sensu, as proposed by D. Lewis and revised by Young and Duncan, and not s.s. as utilized in this chapter
- 4.
Phlebotomus mascitti, considered a poor vector, has been found in Austria.
- 5.
This concept of the Middle East is as arbitrary as the more usual, proposed by the American naval officer and historian Alfred Thayer Mahan in 1902, which included lands from Arabia to India.
- 6.
When applied in the general environment, imidacloprid is very toxic for bees and bumblebees, (Van der Sluijs et al. 2013), but since it has very high LD50 for mammals (2000 mg/kg for dermal exposition in rats and 450 and 131 mg/kg for ingestion, respectively, for rats and mice) (Hovda and Hooser 2002), the application on dogs would not probably be dangerous (CBM).
References
Alvar J, Vélez ID, Bern C et al (2012) Leishmaniasis worldwide and global estimates of its incidence. Plos One 7, e35671
Bacellar O, Lessa H, Schriefer A et al (2002) Up-regulation of Th1-type responses in mucosal leishmaniasis patients. Infect Immun 70:6734. doi:10.1128/IAI.70.12.6734-6740.2002
Badirzadeh A, Moheball M, Ghasemian M et al (2013) Cutaneous and post kala-azar dermal leishmaniasis caused by Leishmania infantum in endemic areas of visceral leishmaniasis, northwestern Iran 2002–2011: a case series. Pathog Global Hlth 107:104–197
Blum J, Desjeux P, Schwartz E et al (2004) Treatment of cutaneous leishmaniasis among travellers. J Antimicrob Chemother 53:158–166
Cantacessi C, Dantas-Torres F, Nolan MJ et al (2015) The past, present, and future of Leishmania genomics and transcriptomics. Trends Parasitol 31:100–108
Cardo LJ (2006) Leishmania: risk to the blood supply. Transfusion 46:1641–1645
Chappuis F, Sundar S, Hailu A et al (2007) Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol 5:873–882
Cota GF, Sousa MR, Mendonça ALP et al (2014) Leishmania-HIV co-infection: clinical presentation and outcomes in an urban area in Brazil. PLoS Negl Trop Dis 8, e2816. doi:10.1371/journal.pntd.0002816
Cota GC, Sousa MR, Rabello A (2011) Predictors of visceral leishmaniasis relapse in HIV infected patients: a systematic review. PLoS Negl Trop Dis 5, e1153. doi:10.1371/journal.pntd.0001153.g001
Dantas-Torres F (2007) The role of dogs as reservoirs of Leishmania parasites, with emphasis on Leishmania (Leishmania) infantum and Leishmania (Viannia) braziliensis. Vet Parasitol 149:139–146
Dantas-Torres F (2009) Canine leishmaniosis in South America. Paras Vect 2 (Suppl I). doi:10.1186/1756-3305-2-S1-S1
Desjeux P, Alvar J (2003) Leishmania/HIV co-infections: epidemiology in Europe. Ann Trop Med Parasitol 97(Suppl 1):S3–S15
Dye C (1992) Leishmaniasis epidemiology: the theory catches up. Parasitology 104:S7–S18
El-Hassan AM, Zijlstra EE (2001) Leishmaniasis in Sudan: 2. Mucosal leishmaniasis. Trans R Soc Trop Med Hyg 95(Suppl 1):S1/19–S1/26
Figueiró-Filho EA, Duarte G, El-Beitume P et al (2004) Visceral leishmaniasis (kala-azar) and pregnancy. Infect Dis Obstet Gynecol 12:31–40
Freitas E, Melo MN, Costa-Val AP et al (2006) Transmission of Leishmania infantum via blood transfusion in dogs: potential for infection and importance of clinical factors. Vet Parasitol 137:159–167
Gidwani K, Picado A, Rijal S et al (2011) Serological markers of sand fly exposure to evaluate insecticidal nets against visceral leishmaniasis in India and Nepal: a cluster-randomized trial. PLoS Negl Trop Dis 5, e1296
Guimarães LH, Machado PRL, Lessa HA et al (2005) Clinical aspects of tegumentary leishmaniasis. Gaz Med Bahia 75:66–74
Hinojosa MC, Alvarez DR, Kato H et al (2013) Cutaneous sporotrichoid lesion in a patient from a subtropical region of Ecuador. Enferm Infecc Microbiol Clin. doi:10.1016/j.eimc.2014.02.007
Hovda LR, Hooser SB (2002) Toxicology of newer insecticides for use in dogs and cats. Vet Clin North Am Small Anim Pract 23:455–467
Kamhawi S (2006) Phlebotomine sand flies and Leishmania parasites: friends or foes? Trends Parasitol 22:439–445
Killick-Kendrick R (1999) The biology and control of phlebotomine sand flies. Clin Dermatol 17:279–289
Kopterides P, Mortzoukou EG, Skopelitis E et al (2007) Aspects of the association between leishmaniasis and malignant disorders. Trans R Soc Trop Med Hyg 101:1181–1189
Lindoso JA, Cota GF, Cruz AM et al (2014) Visceral leishmaniasis and HIV coinfection in Latin America. PLoS Negl Trop Dis 8, e3136
Lindoso JAL, Lima ACS, Cunha MA et al (2015) Diagnosing neglected tropical diseases in HIV coinfection. Hum Parasit Dis 7:11–18. doi:10.4137/HPD.S19569
Lukes J, Mauricio IL, Schönian G et al (2007) Evolutionary and geographical history of the Leishmania donovani complex with a revision of current taxonomy. PNAS 104:9375─9380.doi:10.1073_pnas.0703678104
Luz KG, Silva VO, Gomes EM et al (1997) Prevalence of anti-Leishmania donovani antibody among Brazilian blood donors and multiply transfused hemodialysis patients. Am J Trop Med Hyg 57:168–171
Marcondes CB (2007) A proposal of generic and subgeneric abbreviations for Phlebotomine sandflies (Diptera: Psychodidae: Phlebotominae) of the world. Entomol News 118:351–356
Marcondes CB, Costa CHN (2014) Visceral leishmaniasis control in Brazil: time to re-evaluate DDT? Terr Arthr Rev 7:21–39
Maroli M, Gradoni L, Oliva G et al (2010) Guidelines for prevention of leishmaniasis in dogs. J Am Vet Med Assoc 236:1200–1206
Maroli M, Feliciangeli MD, Bichaud L et al (2013) Phlebotomine sand flies and the spreading of leishmaniases and other diseases of public health concern. Med Vet Entomol 27:123–147
Mayrink W, Botelho ACC, Magalhães PA et al (2006) Immunotherapy, immunochemotherapy and chemotherapy for American cutaneous leishmaniasis treatment. Rev Soc Bras Med Trop 39:14–21
Mignogna MD, Celentano A, Leuci S et al (2014) Mucosal leishmaniasis with primary oral involvement: a case series and a review of the literature. Oral Dis. doi:10.1111/odi.12268
Minodier P, Noël G, Blanc P et al (2005) Traitement des leishmanioses cutanées de l’adulte e de l’infant. Med Trop 65:487–495Miró G, Gálvez R, Fraile C et al (2011) Infectivity to Phlebotomus perniciosus of dogs naturally parasitized with Leishmania infantum after different treatments. Paras Vectors 4:529
Monge-Maillo B, Norman FF, Cruz I et al (2014) Visceral leishmaniasis and HIV coinfection in the Mediterranean region. PLoS Negl Trop Dis. 8(8), e3021. doi:10.1371/journal.pntd.0003021
Oliveira-Neto MP, Schubach A, Mattos M et al (2008) Intralesional therapy of American cutaneous leishmaniasis with pentavalent antimony in Rio de Janeiro, Brazil ─ an area of Leishmania (V.) braziliensis. Int J Dermatol 36:463–468
Otranto D, Dantas-Torres F (2013) The prevention of canine leishmaniasis and its impact on public health. Trends Parasitol 29:339–345
Otranto D, Dantas-Torres F, de Caprariis D et al (2013) Prevention of canine leishmaniosis in a hyper-endemic area using a combination of 10% imidacloprid/4.5% flumethrin. PLoS One 8, e56374
Petersen CA, Barr SC (2009) Canine leishmaniasis in North America: emerging or newly recognized? Vet Clin North Am Small Anim Pract 39:1065–1074
Rabello A, Orsini M, Disch J (2003) Leishmania/HIV co-infection in Brazil: an appraisal. Ann Trop Med Parasitol 97(Suppl 1):S18–S28
Ready PD (2013) Biology of Phlebotomine sand flies as vectors of disease agents. Annu Rev Entomol 58:227–250
Schriefer A, Schriefer ALF, Góes-Neto A et al (2004) Multiclonal Leishmania braziliensis population structure and its clinical implication in a region of endemicity for American tegumentary leishmaniasis. Infect Immun 72:508–514
Singh S, Sharma U, Mishra J (2011) Post-kala-azar dermal leishmaniasis: recent developments. Int J Dermatol 50:1099–1108
Singh N, Mishra J, Singh R et al (2013) Animal reservoirs of visceral leishmaniasis in India. J Parasitol 99:64–67
Solano-Gallego L, Miró G, Koutinas A et al (2011) LeishVet guidelines for the practical management of canine leishmaniosis. Parasit Vectors 4:86, http://www.parasitesandvectors.com/content/4/1/86
Teodoro U, Silveira TG, dos Santos DR et al (2003) Influência da reorganização, da limpeza do peridomicílio e a da desinsetização de edificações na densidade populacional de flebotomíneos no Município de Doutor Camargo, Estado do Paraná, Brasil. Cad Saúde Publ 19:1801–1813
Van der Sluijs JP, Simon-Delso N, Goulson D et al (2013) Neonicotinoids, bee disorders and the sustainability of pollinator services. Curr Opin Environ Sustain 5:293–305
WHO (2010) Towards universal access: scaling up priority HIV/AIDS interventions in the health sector - progress report. WHO, Geneva. Available at: http://www.whoint/hiv/pub/2010progressreport/full_report_enpdf. Accessed in 31 May 2013
Zijlstra EE, Musa AM, Khalil EAG et al (2003) Post-kala-azar dermal leishmaniasis. Lancet Infect Dis 3:87–98
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Marcondes, C.B., Otranto, D., Dantas-Torres, F. (2017). Leishmaniasis. In: Marcondes, C. (eds) Arthropod Borne Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-13884-8_16
Download citation
DOI: https://doi.org/10.1007/978-3-319-13884-8_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-13883-1
Online ISBN: 978-3-319-13884-8
eBook Packages: MedicineMedicine (R0)