
Abstract
In the concluding Chapter, the proposed benefits of an Information Technology System for Predictive, Preventive and Personalized Medicine (ITS-PM) will be presented in the form of expert recommendations and outlook for Predictive, Preventive and Personalized Medicine (PPPM) and hepatocellular carcinoma (HCC). To advance PPPM, the subject of HCC will be presented from a more integrated point of view, combining epidemiology, risk factors, infectious etiologies, pathology, microenvironment and biomarkers, screening and diagnostic technologies, and treatment modalities (single, combined, and/or sequential). It is hoped that by means of an ITS-PM for HCC, greater emphasis may be given to individual patient characteristics than is currently achievable. It is also hoped that through extensions to current screening, staging, and treatment algorithms that we can improve the understanding, prevention, and treatment of HCC. Through the development of an ITS-PM, it may be possible to provide and validate a new methodology for Evidence-Based Medicine utilizing model theory, i.e. Model-Based Medical Evidence (MBME). The information processed in the development of this book was used to reinforce and expand a well-established treatment algorithm, i.e. the Barcelona Clinic Liver Cancer (BCLC) staging system, and, to add extensions that include enhanced screening and greater specifics regarding treatment selections. Finally, new algorithms are presented that relate to alternatives in palliative treatments, down staging, and dealing with progression of disease. Treatments for HCC included in these algorithms include surgical resection, liver transplantation, percutaneous ablation, transarterial chemoembolization (TACE), local radiotherapy with Yttrium-90 microspheres, stereotactic body radiation therapy (SBRT), and systemic targeted therapy with the oral multikinase inhibitor, sorafenib.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
- Personalized medicine
- Hepatocellular carcinoma
- Algorithms
- Screening
- Staging
- Information technology
- Information technology system for predictive, preventive and personalized medicine (ITS-PM)
- Model guided therapy
- Digital patient model
- Patient-specific model
- Model-based medical evidence
13.1 Introduction
In this concluding Chapter, the proposed benefits of an Information Technology System for Predictive, Preventive and Personalized Medicine (ITS-PM) will be presented. As we review the current state of knowledge regarding hepatocellular carcinoma (HCC) and current recommendations regarding patient management, undoubtedly there is a role for Predictive, Preventive, and Personalized Medicine (PPPM) to assist in providing care according to best practices. Furthermore, when an ITS-PM has been created, the accompanying database structures and functions may provide tools for PPPM to advance the understanding and treatment of HCC beyond its current limits. This would include a Therapy Imaging and Model Management System (TIMMS), Patient-Specific Modeling and Model Guided Therapy (MGT) as described in previous Chapters.
To restate our position from Chap. 1, it is our hypothesis that if valid patient-specific models (PSMs) (that factor in age, physiologic condition, disease and co-morbidities, genetics, biomarkers, and responses to previous treatments) can be generated, it may be possible to develop a statistically valid methodology, for each individual to predict certain diseases or conditions, to predict treatment outcomes, to prevent specific diseases or complications, and to develop treatment regimens that are personalized for each particular patient. This proposed system, currently under development, has been designated as Model-Based Medical Evidence (MBME). It is postulated to be able to make a major contribution to Evidence Based Medicine through the analysis of a large number of patients, with the assistance of Information Technology (IT). It is further postulated that the Multi-Entity Bayesian Networks (MEBN), used in the construction of the Digital Patient Model (DPM), will be utilized in the development of a practical decision support system.
Many studies are being conducted at clinical research centers to determine the most effective forms of treatment for HCC. However, the role of large random controlled clinical trials comparing a restricted number of variables may be of limited value considering the many treatment devices and regimens that are currently available, especially as new techniques and tools are introduced. In the current environment, where there are so many old and new competing treatment options, it would appear that there are difficulties in applying the usual forms of Evidence Based Medicine. It may be that, in practice, treatment choices often depend on a combination of factors. These may include local expertise; the availability of treatment devices (which, in part, may depend on financial considerations); personal referral patterns; the presence of clinical research protocols involving a particular device; the collective opinions of local tumor boards; and patient preferences that may in part be based on recommendations of friends or opinions expressed on web sites and blogs. In this environment, with so many available treatment options and with so many gaps in medical information, it may be problematic to be able to determine and provide the most ideal form of therapy for each patient based on personal health characteristics.
As originally stated in Chaps. 1 and 2, it is our goal to utilize an IT approach to medical management to maximize the use of established medical information and to assist decision making and advance our understanding when there is incomplete medical knowledge. The approach we are offering, MBME, offers an alternative to evaluate the effectiveness of different treatment modalities, as well as the influence of individual patient responses. Each complete DPM developed through recruitment of patients in the clinical cancer center may be considered a comprehensive study subject. As the number of DPMs increase, the pooling of information will be utilized through the inference system to generate statistically valid medical information, or, MBME. The Bayesian approach we have selected that utilizes MEBNs, with first-order logic, provides a solid backbone of statistical validity. What will remain to be determined is how many individual patient models will have to be accumulated to achieve statistical validity.
Another feature of this approach that enhances PPPM is that rather than selecting a sufficiently large number of patients to minimize the impact of individual patient variation on the outcome, all relevant information regarding the unique features of each patient is preserved. Thus, when the number of patients included in the database reaches a critical level, it may be possible to not only predict the outcome of therapy by treatment modality (specific forms and combinations of ablation, radiation, chemotherapy, radiation therapy, and surgery) but it may be possible to determine the role of individual components of the patient’s make-up that have contributed to the success or failure of the treatment.
13.2 Building on the Barcelona Clinic Liver Cancer Staging System
If we examine the Barcelona Clinic Liver Cancer (BCLC) Staging System for HCC [1, 2] (Fig. 13.1) that serves as the basis for the management of many patients with HCC worldwide, we observe a very well thought out and evidence-based approach to patient management. Clear recommendations have been made for the initial management of patients with HCC, according to a variety of factors: performance status, Child-Pugh classification, lesion size and number, portal vein pressures, and the presence of tumor invasion, comorbidities, and extensive disease.

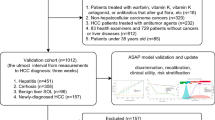
The Barcelona Clinic Liver Cancer (BCLC) staging system algorithm for Hepatocellular Carcinoma—Revised 2011 [3]
The BCLC Staging System Algorithm provides a flow chart that was designed for the staging of patients with HCC to determine the most appropriate form of therapy. In addition, we have found that the BCLC Algorithm provides an excellent platform for the development and investigation of extended treatment pathways. Ablation technologies that are currently available include radiofrequency ablation (RFA), microwave ablation (MW), cryoablation (CRYO), interstitial laser thermotherapy (ILT), and irreversible electroporation (IRE). Transarterial embolotherapy includes techniques that employ either oil-based materials or drug-eluting particles to deliver the chemotherapeutic agents (transarterial chemoembolization; TACE), as well as techniques for the catheter delivery of radiopharmaceuticles (Yttrium-90). Several different forms of radiation therapy are available as well. In addition to individual therapies, combinations of these techniques are also under investigation to control advanced disease and/or to down-stage more advanced disease so that the patient hopefully may become a candidate for a curative treatment.
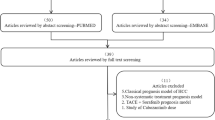
The IEs identified in Chap. 12 may be used to expand and reinforce the BCLC Algorithm in several ways. Extensions may be added to the BCLC Algorithm (Fig. 13.2) that: (1) facilitate enhanced screening for HCC; (2) explore ways in which targeted therapies may be used to improve outcomes; and (3) provide statistically validated evidence regarding the selection of the best treatment from the many options available for palliative, down-staging and bridging therapies.

It may be possible to build on the BLCL staging system algorithm with an IT system for predictive, preventive and personalized medicine (ITS-PM). The first goal will be, through enhanced screening, to have patients seek medical attention earlier in the course of their disease, so that they may enter the algorithm at a more favorable stage; i.e.—a “shift to the left”. The second goal will be to improve outcomes through a better understanding of treatment subcategories, combined treatments, and the effects of down-staging. (Modified from [2])
13.2.1 Enhanced Screening and “Shift to the Left”
It may be possible to positively influence where in the BCLC Staging System a patient enters the algorithm. It would be desirable to achieve a “shift to the left” with a greater number of patients seeking medical attention at a stage of the disease when there is a greater chance of cure. As more data are accumulated it may become possible to evaluate current screening techniques and criteria, and to improve them in light of accumulated information, with the establishment of more comprehensive programs for earlier and more effective screening.
13.2.2 Possible Expanded Role of Targeted Therapies
Currently, targeted therapies for HCC are finding applications in patients with advanced disease. However, it may also be possible to expand the role of targeted therapies in the future to influence the development or progression of disease in earlier stages. It may even become possible to shift high risk patients into low risk categories, thereby averting the development of HCC altogether.
13.2.3 Improved Outcomes with Further Personalized Approach
The BCLC Staging System Algorithm is concerned primarily with the initial treatment choices for patients with HCC. While several treatment options are indicated for patients with intermediate and advanced disease, the complexities relating to these treatment options have not yet been developed within the context of the Algorithm (although these issues are discussed with elsewhere [1–3]). The ITS-PM may be employed to generate MBME to obtain a better understanding of role of locoregional treatment options, combined treatments, and the effectiveness of down-staging and/or bridging therapies to achieve improved outcomes. The Algorithm may be expanded to include, in greater detail, the currently available treatments for HCC, individually or in combination.
13.3 New Algorithms
New algorithms are presented here that address issues and patient selection relating to alternatives in palliative treatments and efforts to achieve down-staging. Currently available treatments for HCC included in these algorithms are surgical resection, liver transplantation, percutaneous ablation, TACE, radioembolization with Yttrium-90 [Y90] microspheres, stereotactic body radiation therapy (SBRT), and systemic targeted therapy with the oral multikinase inhibitor, sorafenib. In accordance with the BCLC Staging System, the efficacy and safety of each treatment modality depends on the stage of liver disease, performance status of the patient, and severity of underlying liver disease.
Treatment algorithms are presented here (Figs. 13.3–13.5) that represent extensions to the BCLC Staging System algorithm by providing a flexible approach to alternative therapies and by introducing the possibility of down-staging and bridging therapy.


Alternative therapy chart: single lesions

Alternative therapy chart: multiple lesions
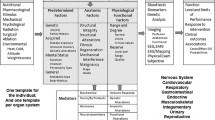
These algorithms present treatment pathways based on the current literature, and provide a framework for the accumulation of data regarding specific treatment protocols. The outcomes of these varied treatments can be linked to extensive data collected for each patient (according to the categories itemized in Figs. 12.5a, b, and 12.7 in Chap. 12) within the ITS-PM.
Conclusion
It is the goal of PPPM to identify the best diagnostic tests and treatment modalities objectively, given the patient's actual clinical status. We have presented an approach to advancing the care of patients with HCC, building on the well-established BCLC Staging System, by proposing extensions to include enhanced screening and a means to evaluate more specific treatment regimens. This approach will require the development of a comprehensive ITS-PM that will utilize a computing system for patient modeling and decision support.
The ITS-PM system presented here is in its earliest stages of development, as is the DPM, which is the basic unit for this system. It is the goal of this project to develop a system of Bayesian inference built on large databases of individual patients that will provide a way of giving greater emphasis to individual patient characteristics in expanded patient screening programs and treatment algorithms.
The algorithms presented here, representing extensions to the BCLC Staging System, are based on literature review and current practices. They need to be validated through appropriate prospective clinical studies. In addition, if sufficient individual data regarding each patient are collected it may be possible to generate knowledge that is necessary for a more complete understanding of the pathophysiology, prevention, and treatment of HCC. This may be accomplished through the use of enhanced IT with modeling and inference techniques, thus creating a new methodology for Evidence-Based Medicine utilizing model theory, i.e. Model-Based Medical Evidence.
In addition, as more information is gathered and validated through the ITS-PM, target benchmarks for the effective treatment of hepatocellular carcinoma can be established. Comparative studies of the costs of different treatment protocols may be evaluated with respect to successes and failures in treatment outcomes, and with respect to overall quality of care and the patient’s quality of life.
The tasks that lay before us in the immediate future include the development of the databases that incorporate patient-specific Information Entities (as described in Chap. 2 and itemized in Figs. 12.5a, b and 12.7 in Chap. 12) and the development of the MEBN and the associated decision support structures (as described in Chaps. 2 and 12). As these are populated with data from a growing number of patient records, DPMs will be developed. It will then become possible to begin the study and validation of Predictive, Preventive and Personalized Medicine through Model-Based Medical Evidence.
References
Bruix J, Sherman M (2010) AASLD Practice Guideline. Management of hepatocellular carcinoma. http://www.aasld.org/practiceguidelines/Documents/Bookmarked%20Practice%20 Guidelines/HCCUpdate2010.pdf. Accessed 20 Nov 2011
Sherman M, Bruix J (2011) AASLD Practice Guideline. Management of hepatocellular carcinoma: an update. Hepatology 53:1020–1022
European Association for the Study of the Liver. European Organisation for Research and Treatment of Cancer (2012) EASL–EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 56:908–943
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Berliner, L., Lemke, H., Ashamalla, H., Mohanty, S. (2015). Outlook and Expert Recommendations for Predictive, Preventive and Personalized Medicine and Hepatocellular Carcinoma. In: Berliner, L., Lemke, H. (eds) An Information Technology Framework for Predictive, Preventive and Personalised Medicine. Advances in Predictive, Preventive and Personalised Medicine, vol 8. Springer, Cham. https://doi.org/10.1007/978-3-319-12166-6_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-12166-6_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-12165-9
Online ISBN: 978-3-319-12166-6
eBook Packages: MedicineMedicine (R0)