
Abstract
In patients with hemophilia, musculoskeletal problems can affect the joints or the muscles. Virtually 90 %, however, involve the joints and they normally begin in childhood. Hemarthroses tend to recur in spite of the synovial membrane’s capacity to reabsorb the blood. When there is a lot of blood in the joint, the synovial membrane becomes hypertrophied. Then, the hypertrophic synovium is more prone to bleed again, ending up in a vicious circle of hemarthrosis-synovitis-hemarthrosis. In addition, the blood in the joint can directly cause death of the chondrocytes in the joint cartilage. The joint pain caused by the above processes can lead to an antalgic flexion deformity of the affected joint which is initially reversible, but will eventually become permanent (fixed deformity). The hyperemic reaction caused by the hemarthrosis leads to asymmetrical hypertrophy of the epiphyseal growth plates which can go on to result in axial deviation of the affected limbs. This all leads to joint damage, which progresses within only a few years to destruction of the joint (hemophilic arthropathy). The non-joint-related musculoskeletal problems in hemophilia, which account for over 10 % of orthopedic lesions in the patient with hemophilia, are essentially soft-tissue hematomas, muscle hematomas, and pseudotumors. Advances in hematology and orthopedic surgery have made it possible to improve the musculoskeletal manifestations of hemophilia in these patients through orthopedic surgical interventions (arthroscopic synovectomy and debridement, total joint replacements). The risk of bleeding in surgical interventions is higher for people with hemophilia than for other patients, and there is also a greater risk of infection. Whatever the surgical procedure, adequate surgical hemostasis must be achieved by infusion of concentrate of the deficient factor.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1.1 Introduction
In patients with hemophilia, orthopedic (musculoskeletal) problems can affect the joints or the muscles [1–3]. Virtually 90 %, however, involve the joints and they normally begin in childhood. Hemarthroses (bleeding into the joints) tend to recur in spite of the synovial membrane’s capacity to reabsorb the blood. When there is a lot of blood in the joint, the synovial membrane becomes hypertrophied because the cytokines and angiogenic factors from the intra-articular hemorrhage stimulate the synovial cells to replicate [3]. Then, the hypertrophic synovium is more prone to bleed again (it becomes very friable and hypervascularized), ending up in a vicious circle of hemarthrosis-synovitis-hemarthrosis. In addition, the blood in the joint can directly cause death of the chondrocytes in the joint cartilage [3].
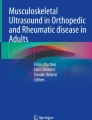
The joint pain caused by the above processes can lead to an antalgic flexion deformity of the affected joint which is initially reversible, but will eventually become permanent (fixed deformity) (Fig. 1.1). The hyperemic reaction caused by the hemarthrosis leads to asymmetrical hypertrophy of the epiphyseal growth plates which can go on to result in axial deviation of the affected limbs. This all leads to joint damage, which progresses within only a few years to destruction of the joint (hemophilic arthropathy) (Fig. 1.2) [4].

Irreversible flexion contracture of the knee, secondary to multiple hemarthroses. Note the posterior subluxation of the tibia associated with the problem

Clinical appearance of severe hemophilic arthropathy in both knees (a) and the radiographic images confirming the joint disease (b). A bilateral total knee replacement was performed in two stages, with a satisfactory result (c)
The non-joint-related musculoskeletal problems in hemophilia, which account for over 10 % of orthopedic lesions in the patient with hemophilia, are essentially soft-tissue hematomas, muscle hematomas, and pseudotumors [4].
With adequate prophylaxis, at least from the age of 2–18 (ideally lifelong), it is possible to convert severe hemophilia into a moderate condition, considerably reducing (although not totally preventing) the associated musculoskeletal problems [5–7].
The main benefit of orthopedic surgery in hemophilia is that it markedly improves the patient’s quality of life [8]. This is achieved by appropriately managing the joint problems (hemophilic arthropathy) and the muscle hematomas and their complications (hemophilic pseudotumors, nerve paralysis caused by compression, and compartment syndrome) [7].
The level of evidence of hemophilia literature is very low. In fact, no study on the musculoskeletal complications of hemophilia has been included in the Cochrane Library so far. The aim of this chapter is to discuss the management of the musculoskeletal manifestations of hemophilia.
1.2 Management of Muscle Hematomas and Their Complications
1.2.1 Compartment Syndrome and Compression Neuropathy
Muscle hematomas can occur in any part of the body (Fig. 1.3) although the most common sites are the iliopsoas muscle and the flexor compartment of the forearm [4, 9]. If not adequately dealt with, they can lead to compartment syndrome and a possible need for urgent surgical decompression of the compartment [10]. Iliopsoas hematomas are often associated with paralysis of the crural nerve. It is important to remember that a right iliopsoas hematoma can be confused with appendicitis. The diagnosis of iliopsoas hematoma should be confirmed by ultrasound and/or computed tomography (CT). Crural nerve paralysis often requires rehabilitation for as long as 18 months before it fully resolves. Electromyography (EMG) is useful for the diagnosis and for assessing progress. Periodic ultrasounds are essential to confirm that the hematomas have been completely reabsorbed, and with the appropriate hematological treatment, this does usually occur. New bleeding, however, is common, and the treatment must therefore be continued for several weeks or even months until complete reabsorption is certain. Surgical decompression of the compartment is not appropriate for an iliopsoas bleed even if there is crural nerve involvement.

Large hematoma in the right thigh of a hemophilia patient, anterior view (a) and posterior view (arrow) (b).
In the forearm, surgical opening of the entire flexor compartment may be necessary, since once compartment syndrome is established, it has a considerable effect on the function of the whole arm [4]. In some patients (particularly the immunosuppressed), a soft tissue hematoma can become spontaneously infected and turn into an abscess. Diagnosed early, this can generally be resolved with treatment based on intravenous antibiotics and surgical drainage.
1.2.2 Hemophilic Pseudotumors
Although rare, pseudotumors are a serious complication of hemophilia. They are progressive cyst-like inflammations that affect the muscles, caused by recurrent bleeding and associated with radiographic evidence of bone involvement [11–13]. Most pseudotumors are seen in adult patients and occur near the proximal ends of the long bones. However, they can occur distally in the wrist and ankle in young patients before skeletal maturity. If left untreated, proximal pseudotumors may destroy the soft tissues, erode the bone, and cause serious vascular and/or nerve damage.
Despite having a mortality rate of 20 %, the treatment of choice for proximal pseudotumors is surgical removal [11]. This mortality is primarily due to surgery. Regression, although not true cure, has been reported with long-term treatment with the deficient clotting factor and immobilization. This treatment should only be used in inoperable cases, such as patients with inhibitors who are poorly controlled. Percutaneous evacuation of the pseudotumor followed by filling with fibrin glue and/or cancellous bone can at times provide satisfactory results. Preoperative embolization of large pelvic pseudotumors may help to reduce intraoperative bleeding when removing surgically.
Distal pseudotumors can be controlled with hematological treatment and immobilization. It is important to be aware of the possibility of pseudotumors when one or more masses are detected in the limbs or pelvic region of a person with hemophilia. However, chondrosarcoma and liposarcoma have been confused with hemophilic pseudotumors in these patients [14]. Ultrasound, CT, and MRI (magnetic resonance imaging) will help to confirm the diagnosis in each case.
1.3 Management of Hemophilic Arthropathy
Hemophilic arthropathy is polyarticular (knees, ankles, elbows, hips, shoulders) and affects the patients from early childhood. Hemarthroses are accompanied by severe pain and an initially reversible antalgic flexion contracture. The blood within the joint alters chondrocyte (cartilage cells) proteoglycan synthesis, causing their death (apoptosis).
1.3.1 Hemarthrosis
Proper treatment of hemarthrosis should include early diagnosis, adequate hematological treatment, evacuation of the blood in the joint (arthrocentesis), physiotherapy, and prevention of new episodes of bleeding [7]. Clinical diagnosis should be confirmed by ultrasound. X-rays should also be performed to rule out (or confirm) radiological signs of joint disease.
A great deal of debate continues to surround the subject of joint aspiration (evacuation of the hemarthrosis or arthrocentesis) in hemophilia. Until very recently, it was considered to be extremely dangerous due to the high risk of new bleeding and infection (septic arthritis). My view is that major hemarthroses must be aggressively treated to prevent progression to synovitis and recurrent joint bleeds. However, there is no evidence of grade I in the literature confirming the role of arthrocentesis in the setting of hemarthrosis. The use of joint aspiration is more a matter of experience based in empirical data [4]. Therefore, we use arthrocentesis in acute and tense hemarthroses. The joint puncture must be done under tight hematological control and strict aseptic conditions [4].
Following arthrocentesis, it is recommended that the joint be immobilized for 3–5 days with a compression bandage. Ice should not be used for acute hemarthroses, as that seems controversial now [15]. The patient should then undergo a course of controlled physiotherapy, as rehabilitation is essential in order to prevent, as far as possible, chronic synovitis. The duration of the physiotherapy will depend on the time required for full recovery of joint mobility and muscle strength. Recurrent bleeding episodes must be avoided during the recovery period. Patients should be seen every 3 months in order to assess their progress closely.
1.3.2 Synovitis
Another problem is synovitis (synovial hypertrophy), caused by the cytokines and angiogenic factors from the intra-articular hemorrhage that stimulate the synovial cells to replicate, which eventually leads to a vicious circle of hemarthrosis-synovitis-hemarthrosis [3]. The circle must be broken by synovectomy. This may be medical or surgical. Medically, the best type is radiosynovectomy, the alternative being chemical synovectomy. Surgical synovectomy can be performed arthroscopically or by open surgery [16–20].
Short courses of intra-articular prednisone should be taken into account as an option prior to synovectomy [21].
Review of literature prior to 2002 showed no reports of malignancy related to 32P [22, 23]. However, in 2002 and 2009 two cases of acute lymphocytic leukemia (ALL) were reported after radiosynovectomy in two hemophilic children [23]. Given the short latency between exposure and diagnosis of ALL in both patients, the casual relationship between 32P exposure and ALL could not be firmly established. It is important to note, however, that there was also insufficient data to rule out causality.
Recently, a report of Infante-Rivard et al. demonstrated that there was no dose-response relationship with the amount of radioisotope administered or the number of radiosynovectomy treatments [19]. The study provided some indication for the safety of the procedure, but homogenous diagnostic groups of younger patients (such as hemophilic patients) receiving radiosynovectomy will need more evaluation.
The principal aim in hemophilia is, as far as possible, to prevent hemarthrosis before the synovitis can occur. Once developed, the aim is to treat it as early and aggressively as possible. The diagnosis should be confirmed by ultrasound or MRI (magnetic resonance imaging). Ultrasound is particularly useful for the knee, while MRI is more accurate for the elbow and the ankle. Nowadays power Doppler ultrasonography (US) is a very important tool for assessing knee bleeds [24, 25]. When conservative treatment, i.e., deficient clotting factor replacement therapy plus physiotherapy, fails to break the hemarthrosis-synovitis-hemarthrosis vicious circle, intervention is required to destroy the synovial membrane.
A medical synovectomy is simply the injection of a substance into the joint to “stabilize” the synovial membrane. The main reason for performing any type of synovectomy is the presence of an excessive amount of synovial membrane in a particular joint (hemophilic synovitis). We consider medical synovectomy the procedure of choice in cases of hemophilic synovitis with recurrent hemarthrosis, and that surgical synovectomy should only be used in cases where medical synovectomy has repeatedly failed. In view of its efficacy and minimal risk, medical synovectomy may also be used in patients with inhibitors [13, 14, 26].
The differential diagnosis between synovitis and hemarthrosis can, and should, be made by US and/or MRI. Plain X-rays are useful for assessing the degree of joint disease when deciding on synovectomy. It is logical to expect that the worse the synovitis, the more difficult it will be to resolve it by synovectomy. Indeed, in severe cases, multiple consecutive medical synovectomies can be necessary, and even then, surgical synovectomy may still be required.
The main indication for medical synovectomy is the presence of chronic hemophilic hypertrophic synovitis causing recurrent hemarthroses that do not respond to hematological treatment. The most commonly used these days are chemical synovectomy (rifampicin, oxytetracycline) and isotopic synovectomy or radiosynovectomy (with yttrium-90, phosphorus-32, or rhenium-186). In general, medical synovectomy has a 70 % efficacy rate, and it can be used at any point in the patient’s life; the main aim is to reduce the number and severity of hemarthroses and the damage the blood in the joint causes to the cartilage over the medium and long term.
Radiosynovectomy can be repeated if the first injection fails, up to three times at 6-month intervals if radioactive isotopes are used, or weekly, as many as 10–15 times if using rifampicin or oxytetracycline. Radiosynovectomy has been used worldwide for over 40 years, and no evidence has been found of any harm caused by the radioactive isotopes [27, 28]. In my opinion, assuming the isotopes are available, radiosynovectomy (with yttrium for knees and rhenium for elbows and ankles) is the procedure of choice in children aged over 12. We prefer rhenium for elbows and ankles because its therapeutic penetration power (1 mm) correlates well with the size of the synovium of medium-sized joints. However, in the knee we prefer yttrium because its therapeutic penetration power is 2.8 mm and it correlates well with the size of the knee synovium. Failing radiosynovectomy, rifampicin, and oxytetracycline are the alternatives (multiple, fairly painful, weekly injections are required for effective chemical synovectomy) [16–20].
Surgical synovectomy can be performed by open surgery or by arthroscopy. Most authors recommend arthroscopy [20, 29]. Once skeletal maturity has been reached, open surgery synovectomy may be indicated for the elbow, combined with resection of the radial head to improve pronation and supination of the elbow. In our center, we now always opt for radiosynovectomy with yttrium-90 (knees) or rhenium-186 (elbows and ankles) as the first option, and then if, after 2–3 radiosynovectomies at 6-month intervals, we have not managed to control the synovitis, we turn to surgical synovectomy (preferably arthroscopic) [26]. Prior radiosynovectomy does not lessen the chance for optimal response with surgical synovectomy (radiation does not cause fibrosis that makes complete resection difficult).
In terms of radiosynovectomy, our experience has confirmed a 70 % reduction in the mean rate of bleeds. Regarding pain and ROM, the rate of improvement is 70 % (statistically significant) and 3 % (not significant), respectively [18]. We use yttrium-90 (185 MBq, TPP-therapeutic penetration power of 2.8 mm) in the knees and rhenium-186 (TPP 1 mm) in the elbows (56–74 MBq) and ankles (74 Mbq). We have given over 400 injections to date (1–3 per patient, at 6-month intervals). The risk of complications is 1.5 % (four inflammatory responses, one mild radiation burn to the skin, one septic arthritis of the knee). Radiosynovectomy is our first option for the treatment of synovitis (450 euros per injection), with arthroscopic synovectomy as second-line treatment (4,500 euros). We opt for arthroscopic synovectomy after the failure of three attempts at radiosynovectomy at 6-month intervals. So far, only 3.5 % of patients have required this technique [18].
1.3.3 Advanced Joint Disease
The literature seems to support the use of the intra-articular injections of hyaluronic acid (so-called viscosupplementation) in the treatment of knee osteoarthritis, because it diminishes pain and improves disability, generally within 1 week and for up to 3–12 months (but especially at the 5–13-week postinjection period). There are only five reports in the literature on the efficacy of knee viscosupplementation in hemophilia, all of them with a low level of evidence [30]. The five studies dealing with viscosupplementation in hemophilia recommend it for hemophilic arthropathy of the knee as a way of delaying the need of operative treatment when noninvasive medical therapy (relative rest, oral anti-inflammatory drugs, oral analgesics, and physical therapy) has failed. My view is that the short-lived improvement afforded by viscosupplementation does not seem to warrant its use in hemophilic patients given the risks and the cost involved. Further trials are required to ascertain whether viscosupplementation should be indicated in painful radiological hemophilic arthropathy of the knee [30].
When the extent of joint involvement progresses as a result of the joint bleeds being impossible to control, patients will not only develop certain joint deformities and contractures but also subchondral cysts and osteophytes. Valgus deformity of the knee and the ankle is common, while the most typical in the elbow is hypertrophy of the radial head. Hemophilia patients may therefore present with valgus flexion deformities in one or both knees, equinus (Fig. 1.4) in one or both ankles, and in one or both elbows in flexion. Osteotomy is often necessary on the knee and ankle to correct the poor joint alignment [31].

Severe equinus deformity of the ankle in a patient with hemophilia
Flexion contractures are common in hemophilia and difficult to resolve once they become fixed. The joints most affected are the elbows, knees, and ankles. The contracture is initially antalgic and is related to a hemarthrosis, which means that within the first few weeks, the contracture can be resolved with the appropriate treatment (hematological treatment plus rehabilitation) [32]. The deformity will subsequently become fixed, with the resulting negative effects on function, and may even require surgery. In the knee, lengthening of the tendons in the popliteal fossa (hamstrings release) combined with a posterior capsulotomy or supracondylar extension osteotomy may correct the flexion deformity. In the ankle, Z-lengthening of the Achilles tendon may also be necessary [4].
In the hip, patients may develop a disease similar to Perthes disease in relation to the recurrent joint bleeds. Perthes is a condition in children characterized by a temporary loss of blood supply to the hip. Without an adequate blood supply, the rounded head of the femur dies. The area becomes intensely inflamed and irritated. Perthes is really a complex process of stages. Treatment of Perthes may require periods of immobilization or limitations on usual activities. The long-term prognosis is good in most cases. After 18 months to 2 years of treatment, most children return to normal activities without major limitations. Perthes disease usually is seen in children between 4 years and 10 years of age. It is five times more common in boys than in girls. Initial treatment is with an abduction orthosis, thereby making surgery rarely necessary (varus osteotomy of neck of the femur). Juxta-articular cysts are also common and, when large and symptomatic, may require curettage and filling with bone graft, with or without fibrin glue. The formation of large anterior osteophytes is common in the ankle, and when symptomatic, surgical excision may be necessary.
Many hemophilia patients under the age of 40, and as young as 10, already have severe joint damage (advanced joint disease). At this point, the possible treatments are radial head resection, total hip replacement, arthroscopic debridement of the knee, total knee replacement (TKR), and ankle arthrodesis [4]. When there is multiple joint involvement, operating on only one joint may not improve the patient’s overall functioning, and our objective should therefore be to achieve one functional limb. It is recommended in hemophilia that multiple joint interventions be done in one single operation, since the complication rate is lower than would be expected and the rehabilitation time after multiple-joint surgery is relatively short [33].
In the elbow, radial head resection tends to reduce the number of joint bleeds and improve the degree of pronation and supination. Elbow deformity can cause ulnar nerve damage, which may require surgical neurolysis (release) [34, 35].
In the hip, the best solution is total hip replacement (THR). A spontaneously ankylosed hip can even be converted into a prosthesis, with the aim of improving the severe low back and knee pain suffered by patients with an ankylosed hip [36, 37].
In the knees, if the patient is very young and has a long life expectancy, it may be worthwhile debriding arthroscopically in order to relieve the pain for a few years [38]. If the arthroscopic knee debridement fails, TKR may be an option [39–47]. THR and TKR appear to last longer in people with hemophilia than in people of a similar age with osteoarthritis [45]. It is evident that in the age of joint replacement, hip and knee replacement should be offered to the hemophilia patient with massive joint damage associated with severe pain and marked functional disability. Nonetheless, the surgeon and the patient must weigh up the risks and benefits (especially if the patient is severely immunosuppressed).
THR and TKR have a limited span of use due to wear and tear (15 years for knees, 20 years for hips). Ideally, the youngest age joint replacement can be done without having to replace it later is 60 for THR and 65 for TKR. Our preferred type/brand of prosthesis for the knee is a posterior stabilized (PS) design with cemented components (with antibiotic-loaded cement), always with patellar resurfacing (Insall-Burstein type). For the hip we prefer a cemented Charnley design.
The risk of infection is higher for hemophilia patients undergoing total joint replacement, with a mean risk of approximately 7 % [48], than in the non-hemophilia population, where this figure is only 1–2 %. One of the risks inherent with joint replacement in the hemophilic patient is risk of Staphylococcus infection from central venous catheters (CVCs). To reduce that risk systematic preoperative screening by swab is very important. Prevention of positive cases by means of nasal decontamination (mupirocin 3 days) is advisable. Preoperative antibiotic prophylaxis has shown itself to be an efficient method to lower infection rates. Operating theaters ideally should be equipped with laminar flow [49]. In persons with hemophilia, there are three additional risk factors: insufficient hemostasis, HIV-positive status, and central venous catheters (CVCs). Implementing the preventive measures for the general population and a sufficient level of clotting factor for 2–3 weeks can help diminish the infection in persons with hemophilia undergoing TKR. In HIV-positive patients with CD4 count less than 200 cells/μl, early, vigorous treatment should be instituted for suspected infection and surgical intervention individualized based on the balance of risks and benefits. Strict adherence to hand washing and aseptic technique are essential elements of catheter care. Caregiver education is an integral part of CVC use, and the procedural practices of users should be regularly reassessed [49]. On the other hand, continuous infusion (CI) of factor is preferable to bolus infusion (BI) to reduce bleed risk which we know can be associated with higher infection risk.
The standard treatment for end-stage osteoarthritis of the ankle joint in hemophilic patients has been fusion of the ankle joint [50]. Total ankle replacement (TAR) is still controversial as a treatment option. Barg et al. [51] analyzed 10 total ankle replacements performed in eight hemophilia patients. Their mean age was 43 years and the average follow-up was 2.7 years. They stated that for patients with hemophilic osteoarthritis of the ankle joint, TAR is a valuable alternative treatment to ankle fusion.
1.4 Potential Complications of Treatment
The main risks of orthopedic surgery in hemophilia are infection and bleeding [4]. The mean risk of TKR infection is 7 %, as opposed to 1–2 % in the osteoarthritis population. Two operations are generally necessary (two-stage revision arthroplasty) to solve it (with an 85–90 % likelihood of success). Many hemophilia patients are infected with HIV (human immunodeficiency virus) and HCV (hepatitis C virus). HIV infection can increase the risk of postoperative infection. In HIV-positive persons with hemophilia with CD4 count less than 200 cells/μl, early, vigorous treatment should be implemented for suspected infection and surgical orthopedic intervention individualized based on the balance of risks and benefits [49]. What also must be remembered is the risk of HIV and HCV infection for the “surgical team” in the event of accidental puncture wounds.
Excessive postoperative bleeding can be the result of inadequate hemostasis or the development of a pseudoaneurysm during the intervention, which usually becomes evident in the immediate postoperative period (sooner or later). After ruling out a problem with hemostasis (that the levels of clotting factor are not too low), the diagnosis of pseudoaneurysm must be confirmed by CT angiogram or conventional angiogram. Embolization of the artery is the first treatment option, and artery ligation (with or without distal bypass) is the next alternative (open surgery). Early diagnosis and treatment of this complication is essential, in particular to prevent the risk of infection of the associated excess blood in the joint. It appears that pseudoaneurysms do not develop more commonly in hemophiliac arthroplasties than in non-hemophiliac arthroplasties [52].
In orthopedic surgery for hemophilia patients, general anesthesia is recommended, since spinal anesthesia can lead to serious complications (deriving from development of a spinal hematoma) [53].
In patients with inhibitor (antibody to the clotting factor given by intravenous infusion), hemostasis can be achieved using bypassing agents such as aPCCs (FEIBA: factor VIII inhibitor bypassing agent, Baxter) and rFVIIa (recombinant activated factor VII, NovoSeven, Novo Nordisk) [54–58]. However, if surgical management of inhibitor patients is made, we should outweigh the risks and the advantages of surgery. In other words, given the high risk of bleeding complications and need to resort to rescue therapy, surgery in patients with inhibitors is not to be undertaken lightly.
The risk of venous thromboembolism (VTE) after orthopedic surgery in hemophilia patients is very low [59]. In fact, little has been published addressing the role of thromboembolic prophylaxis in the hemophilic patient population following THR and TKR. Although the American College of Chest Physicians (ACCP) and the American Academy of Orthopedic Surgeons (AAOS) have set guidelines for thromboembolic prophylaxis in the general population, no such standard of care is in place for hemophilic patients. While the risk of thrombosis in hemophilic patients following THR and TKR is thought to be lower, cases have been reported of pulmonary embolism and deep vein thrombosis (DVT) in hemophilic patients [59]. In our center we do not use pharmacological prophylaxis of VTE in persons with hemophilia. In fact, we have never seen such complication in patients with hemophilia so far. However, in non-hemophilia patients we use daily subcutaneous low-molecular-weight heparin (LMWH) for 2 weeks after THR and TKR. In all patients we advise mechanical prophylaxis by means of early mobilization after surgery.
Most authors replace the deficient coagulation factor for 10–14 days. However, a high rate of infection has been reported when using insufficient hemostasis [46]. To achieve adequate hemostasis during major surgery, our recommendation in hemophilia A patients is to perform clotting factor replacement preoperatively until a minimum level of 100 % of normal is achieved; then the level is maintained at 60 % of normal for 14 postoperative days, and then clotting factor replacement is infused to obtain a level of 30 % of normal prior to rehabilitation sessions for 8–10 weeks.
The World Federation of Hemophilia (WFH) guidelines [60] endorsed by the International Society of Thrombosis and Hemostasis (ISTH) suggest that in hemophilia A patients undergoing major surgery, plasma factor peak level (when there is no significant resource constraint) must be 80–100 (IU/dL) preoperatively. In the postoperative period such a level must be 60–80 in days 1–3, 40–60 in days 4–6, and 30–50 in days 7–14. In minor surgery, the desired level in hemophilia A must be 50–80 preoperatively. Postoperatively it must be 30–80 during days 1–5, depending on the type of procedure. In patients with hemophilia B undergoing major surgery, the preoperative recommended level is 60–80. In the postoperative period the level must be 40–60 in days 1–3, 30–50 in days 4–6, and 20–40 in days 7–14. In minor surgery the preoperative level in hemophilia B must be 50–80, while the postoperative level must be 30–80 in days 1–5, depending on the type of procedure.
1.5 Conclusions
A multidisciplinary team is essential if satisfactory results are to be obtained in orthopedic surgery in people with hemophilia. Prophylaxis with the deficient clotting factor from the age of 2 until the patient reaches 18 seems to be the only effective way to minimize the joint bleeding and joint deformities typical of hemophilia in adulthood (joint disease). Surgical interventions that are commonly required by hemophilia patients include joint aspiration (arthrocentesis), synovectomy (arthroscopic or radiosynovectomy), osteotomy, arthroscopic debridement, tendon lengthening, arthrodesis (fusing of joints), total joint replacements, resection or percutaneous treatment of pseudotumors, fasciotomy for compartment syndrome, arthrotomy for septic arthritis, drainage of infected hematomas (abscesses), and other orthopedic interventions. With the current hematological treatments, any of the aforementioned orthopedic surgical interventions can be carried out in people with hemophilia with a high degree of safety (although not as high as in patients without congenital clotting disorders). Orthopedic surgery in hemophilia patients tends to be complex and involves a higher risk of both bleeding and infection. With collaboration between hematologists, orthopedic surgeons, and other specialists, we can make a big difference in the quality of life of people with hemophilia. Good hemostasis, appropriate surgical technique, and good postoperative rehabilitation are essential.
References
Rodriguez-Merchan EC (1996) Effects of hemophilia on articulations of children and adults. Clin Orthop Relat Res 328:7–13
Rodriguez-Merchan EC (1997) Pathogenesis, early diagnosis, and prophylaxis for chronic hemophilic synovitis. Clin Orthop Relat Res 343:6–11
Valentino LA (2010) Blood-induced joint disease: the pathophysiology of hemophilic arthropathy. J Thromb Haemost 8:1895–1902
Rodriguez-Merchan EC (2012) Aspects of current management: orthopaedic surgery in haemophilia. Haemophilia 18:8–16
Key N, Negrier C (2007) Coagulation factor concentrates: past, present, and future. Lancet 370:439–448
Manco-Johnson MJ, Abshire TC, Shapiro AD, Riske B, Hacker MR, Kilcoyne R et al (2007) Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med 357:535–544
Rodriguez-Merchan EC, Jimenez-Yuste V, Aznar JA, Hedner U, Knobe K, Lee CA et al (2011) Joint protection in haemophilia. Haemophilia 17(Suppl 2):2–23
Schik M, Stucki G, Rodriguez M, Meili EO, Huber E, Miche BA, Brühlmann P (1999) Haemophilic; arthropathy: assessment of quality of life after total knee arthroplasty. Clin Rheumatol 18:468–472
Lim MY, Nielsen B, Ma A, Key NS (2014) Clinical features and management of haemophilic pseudotumours: a single US centre experience over a 30-year period. Haemophilia 20:e58–e62
Rodriguez-Merchan EC (2013) Acute compartment syndrome in haemophilia. Blood Coagul Fibrinolysis 24:677–682
Rodriguez-Merchan EC (2002) Haemophilic cysts (pseudotumours). Haemophilia 8:393–401
Buchowski JM, Cascio BM, Streiff MB, Frassica FJ (2005) Resection and reconstruction of a massive femoral hemophilic pseudotumor. Clin Orthop Relat Res 430:237–242
Vanderhave KL, Caird MS, Hake M, Hensinger RN, Urquhart AG, Silva S, Farley FA (2012) Musculoskeletal care of the hemophiliac patient. J Am Acad Orthop Surg 20:553–563
Allen DJ, Goddard NJ, Mann HA, Rodriguez-Merchan EC (2007) Primary malignancies mistaken for pseudotumours in haemophilic patients. Haemophilia 13:383–386
Forsyth AL, Zourikian N, Valentino LA, Rivard GE (2012) The effect of cooling on coagulation and haemostasis: should “Ice” be part of treatment of acute haemarthrosis in haemophilia? Haemophilia 18:843–850
Rivard GE, Girard M, Belanger R, Jutras M, Guay JP, Marton D (1994) Synoviorthesis with colloidal chromic phosphate for the treatment of hemophilic arthropathy. J Bone Joint Surg Am 76-A:482–488
Rodriguez-Merchan EC, Goddard NJ (2001) The technique of synoviorthesis. Haemophilia 7(Suppl 2):11–15
De la Corte-Rodriguez H, Rodriguez-Merchan EC, Jimenez-Yuste V (2011) What patient, joint and isotope characteristics influence the response to radiosynovectomy in patients with haemophilia? Haemophilia 17:e990–e998
Infante-Rivard C, Rivard GE, Derome F, Cusson A, Winikoff R, Chartrand R, Guay JP (2012) A retrospective cohort study of cancer incidence among patients treated with radiosynoviorthesis. Haemophilia 18:805–809
Eickhoff HH, Koch W, Raderschadt G, Brackmann H-H (1997) Arthroscopy for chronic hemophilic synovitis of the knee. Clin Orthop Relat Res 343:58–62
Rodriguez-Merchan EC, Villar A, Orbe A, Magallon M (1994) Intra-articular methylprednisolone therapy in chronic hemophilic synovitis of the knee. Rev Clin Esp 194:480–482
Dunn A, Busch MT, Wyly JB, Abshire TC (2002) Radionuclide synovectomy for hemophilic arthropathy: a comprehensive review of safety and efficacy and recommendation for a standardized treatment protocol. Thromb Haemost 87:383–393
Dunn A, Manco-Johnson M, Busch MT, Balark KL, Abshire TC (2005) Leukemia and P32 radionuclide synovectomy for hemophilic arthropathy. J Thromb Haemost 3:1541–1542
Acharya SS, Schloss R, Dyke JP, Mintz DN, Christos P, DiMichele DM, Adler RS (2008) Power Doppler sonography in the diagnosis of hemophilic synovitis–a promising tool. J Thromb Haemost 6:2055–2061
Melchiorre D, Linari S, Innocenti M, Biscoglio I, Toigo M, Cerinic MM, Morfini M (2011) Ultrasound detects joint damage and bleeding in haemophilic arthropathy: a proposal of a score. Haemophilia 17:112–117
Rampersad AG, Shapiro AD, Rodriguez-Merchan EC, Maahs JA, Akins S, Jimenez-Yuste V (2013) Radiosynovectomy: review of the literature and report from two haemophilia treatment centers. Blood Coagul Fibrinolysis 24:465–670
De La Corte-Rodriguez H, Rodriguez-Merchan EC, Jimenez-Yuste V (2013) Consecutive radiosynovectomy procedures at 6-monthly intervals behave independently in haemophilic synovitis. Blood Transfus 11:254–259
Teyssler P, Taborska K, Kolostova K, Bobek V (2013) Radiosynoviorthesis in hemophilic joints with yttrium-90 citrate and rhenium-186 sulfide and long term results. Hell J Nucl Med 16:44–49
Rodriguez-Merchan EC (2013) Haemophilic synovitis of the elbow: radiosynovectomy, open synovectomy or arthroscopic synovectomy? Thromb Res 132:15–18
Rodriguez-Merchan EC (2012) Intra-articular injections of hyaluronic acid (viscosupplementation) in the haemophilic knee. Blood Coagul Fibrinolysis 23:580–583
Rodriguez-Merchan EC, Galindo E (1992) Proximal tibial valgus osteotomy for hemophilic arthropathy of the knee. Orthop Rev 21:204–208
De la Corte-Rodriguez H, Rodriguez-Merchan EC (2013) The role of physical medicine and rehabilitation in haemophiliac patients. Blood Coagul Fibrinolysis 24:1–9
Horoszowski H, Heim M, Schulman S, Varon D, Martinowitz U (1996) Multiple joint procedures in a single operative session on hemophilic patients. Clin Orthop Relat Res 328:60–64
Utukuri MM, Goddard NJ (2005) Haemophilic arthropathy of the elbow. Haemophilia 11:565–570
Rodriguez-Merchan EC (2014) Peripheral nerve injuries in haemophilia. Blood Transfus 12(Suppl 1):s313–s318
Miles J, Rodriguez-Merchan EC, Goddard NJ (2008) The impact of haemophilia on the success of total hip arthroplasty. Haemophilia 14:81–84
Mann HA, Choudhury MZ, Allen DJ, Lee CA, Goddard NJ (2009) Current approaches in haemophilic arthropathy of the hip. Haemophilia 15:659–664
Rodriguez-Merchan EC, Magallon M, Galindo E (1994) Joint debridement for haemophilic arthropathy of the knee. Int Orthop 18:135–138
Rodriguez-Merchan EC (2002) Total knee arthroplasty in patients with haemophilia who are HIV-positive. J Bone Joint Surg Br 84:170–172
Rodriguez-Merchan EC, Wiedel JD (2002) Total knee arthroplasty in HIV-positive haemophilic patients. Haemophilia 8:387–392
Goddard NJ, Rodriguez-Merchan EC, Wiedel JD (2002) Total knee replacement in haemophilia. Haemophilia 8:382–386
Sheth DS, Oldfield D, Ambrose C, Clyburn T (2004) Total knee arthroplasty in hemophilic arthropathy. J Arthroplasty 19:56–60
Rodriguez-Merchan EC (2007) Total knee replacement in haemophilic arthropathy. J Bone Joint Surg Br 89:186–188
Goddard NJ, Mann HA, Lee CA (2010) Total knee replacement in patients with end-stage haemophilic arthropathy: 25-year results. J Bone Joint Surg Br 92:1085–1089
Sikkema T, Boerboom AL, Meijer K (2011) A comparison between the complications and long-term outcome of hip and knee replacement therapy in patients with and without haemophilia; a controlled retrospective cohort study. Haemophilia 17:300–303
Wong JM, Mann HA, Goddard NJ (2012) Perioperative clotting factor replacement and infection in total knee arthroplasty. Haemophilia 18:607–612
Uprichard J, Adamidou D, Goddard NJ, Mann HA, Yee TT (2012) Factor IX replacement to cover total knee replacement surgery in haemophilia B: a single-centre experience, 2000–2010. Haemophilia 18:46–49
Ragni MV, Crossett LS, Herndon JH (1995) Postoperative infection following orthopaedic surgery in human immunodeficiency virus-infected hemophiliacs with CD4 counts < or = 200/mm3. J Arthroplasty 10:716–721
Rodriguez-Merchan EC (2012) Preventing surgical site infection in haemophilia patients undergoing total knee arthroplasty. Blood Coagul Fibrinolysis 23:477–481
Bluth BE, Fong YJ, Houman JJ, Silva M, Luck JV Jr (2013) Ankle fusion in patients with haemophilia. Haemophilia 19:432–437
Barg A, Elsner A, Hefti D, Hintermann B (2010) Haemophilic arthropathy of the ankle treated by total ankle replacement: a case series. Haemophilia 16:647–655
Rodriguez-Merchan EC (2013) Pseudoaneurysms in haemophilia. Blood Coagul Fibrinolysis 24:461–464
van Veen JJ, Nokes TJ, Makris M (2010) The risk of spinal haematoma following neuraxial anaesthesia or lumbar puncture in thrombocytopenic individuals. Br J Haematol 148:15–25
Rodriguez-Merchan EC, Quintana M, Jimenez-Yuste V (2008) Orthopaedic surgery in haemophilia patients with inhibitors as the last resort. Haemophilia 14(Suppl 6):56–67
Giangrande PL, Wilde JT, Madan B, Ludlam CA, Tuddenham EG, Goddard NJ, Dolan G, Ingerslev J (2009) Consensus protocol for the use of recombinant activated factor VII [eptacog alfa (activated); NovoSeven] in elective orthopaedic surgery in haemophilic patients with inhibitors. Haemophilia 15:501–508
Rangarajan S, Austin S, Goddard NJ, Negrier C, Rodriguez-Merchan EC, Stephensen D, Yee TT (2013) Consensus recommendations for the use of FEIBA (®) in haemophilia A patients with inhibitors undergoing elective orthopaedic and non-orthopaedic surgery. Haemophilia 19:294–303
Négrier C, Lienhart A, Numerof R, Stephens D, Wong WY, Baghaei F, Yee TT (2013) SURgical interventions with FEIBA (SURF): international registry of surgery in haemophilia patients with inhibitory antibodies. Haemophilia 19(3):e143–e150
Rodríguez-Merchán EC (2012) Orthopedic surgery is possible in hemophilic patients with inhibitors. Am J Orthop (Belle Mead NJ) 41:570–574
Stein MI, Park J, Raterman S (2011) Prevention of VTE Following total hip and knee arthroplasty in Hemophilia patients. Orthopedics 34:393
Srivastava A, Brewer AK, Mauser-Bunschoten EP, Key NS, Kitchen S, Llinas A, Ludlam CA, Mahlangu JN, Mulder K, Poon MC, Street A, Treatment Guidelines Working Group on Behalf of The World Federation of Hemophilia (2013) Guidelines for the management of hemophilia. Haemophilia 19:e1–e47
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Rodríguez-Merchán, E.C., De la Corte-García, H. (2015). Musculoskeletal Manifestations of Hemophilia. In: Rodríguez-Merchán, E. (eds) Joint Surgery in the Adult Patient with Hemophilia. Springer, Cham. https://doi.org/10.1007/978-3-319-10780-6_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-10780-6_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-10779-0
Online ISBN: 978-3-319-10780-6
eBook Packages: MedicineMedicine (R0)