
Abstract
Understanding of death and expression of grief are determined by chronologic age and levels of cognitive development.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Critical life events
- Impact of mass media
- Adoption
- Psychosomatic disorders
- Sleep disorders
- Vulnerable child syndrome
- Rumination
- Pain
- Gifted child
- Chronic illness and handicapping conditions
- Child abuse
- Factitious disorder (Munchausen syndrome) by proxy
- Sexual abuse
Critical Life Events
Death
-
Understanding of death and expression of grief are determined by chronologic age and levels of cognitive development. These are coupled with circumstances of death; and the family’s cultural and religious background .
-
Levels of cognitive and behavioral development differ by age (Table 1):
Table 1 Level of cognitive and behavioral aspects of developing an understanding of death by age. (Adapted from Pediatrics in Review, Vol. 30 No. 9, September 2009) -
children less than 2 years have sensorimotor.
-
children with 2–6 years have preoperational.
-
children with 6–10 years have concrete operational.
-
adolescents have a formal operational development stage.
-
-
Grief reactions occur in different domains that include the emotional, cognitive, physical, and social domains:
-
Usual expressions of grief include repeated questioning, somatic complaints, regressive behaviors, separation anxiety, school phobia, or academic difficulty
-
Adolescents may present with increased high-risk behavior with drugs, alcohol, delinquency, or precocious sexual activity.
-
Kubler-Ross introduced the concept of the stages of grief
-
Denial
-
Anger
-
Bargaining
-
Depression
-
Acceptance
Management
-
When death is anticipated, information about expectations and effective counseling will help family bereavement.
-
Every member of the family needs to be included in the process as appropriate.
-
Depending on the child developmental stage, a dying child benefits from open communication about death.
-
The pediatrician can provide information and support by listening and communicating well to the family.
-
It is also appropriate for pediatricians to show emotion. Parents do appreciate the depth of their doctor’s emotional feelings.
-
Scheduling an appointment with the family about 1 month after the death to evaluate the family’s coping ability.
-
Pediatricians need resources and support within the medical community to help cope most effectively with the death of a patient.
Divorce
-
Long-lasting effects of divorce or separation on the child and the family:
-
Exposure to high levels of parental conflict is predictive of poor emotional adjustment by the child regardless of the parents’ marital status.
-
Children exposed to high-conflict parental interactions are significantly more likely to exhibit externalizing behavioral problems, emotional dysregulation, and decreased academic performance.
-
The developmental stage of a child will also have an effect on the child’s response to a blended family.
-
A child’s emotional adjustment to divorce may affect his/her own subsequent intimate relationships.
-
Families may experience increased financial difficulties.
-
-
Protective factors that may increase the likelihood of long-term positive psychological adjustment:
-
Adjustment to new relationships may be smoothed if children are allowed adequate time to adjust first to the parents’ separation or divorce.
-
The introduction of the new partner should be done slowly and with sensitivity to the child’s reactions.
-
Transitioning to blended families will be smoothest when stepparents do not take over responsibility for discipline of their stepchildren.
-
Children with regular and consistent involvement of the father after divorce were reported to have fewer social problems.
-
Management
-
The developmental stage of a child will have an effect on the child’s response to divorce.
-
Consistency in parenting techniques and discipline as a way to promote stability and predictability
-
Pediatrician should avoid taking sides or overidentifying with one parent versus another.
-
If there is suspicion of abuse or neglect, significant parental substance abuse, or significant parental mental health problems, the pediatrician must counsel the parent on the appropriate resources to consult.
-
Medical professionals should be careful to refrain from providing legal advice and refer those questions to the parent’s legal counsel.
-
Pediatricians are encouraged to monitor the emotional and behavioral adjustment of children of divorced parents.
-
Parenting plans could result from agreement between two cooperating parents, mediation, and through the courts.
-
Parents who succeed through the mediation process tend to avoid escalation of conflict, improve co-parenting cooperation, and save significant legal costs.
Transition of Adolescents to Young Adulthood for Vulnerable Populations
Background
-
Adolescents with chronic medical conditions and disabilities have immense challenges transitioning to adult medical care.
-
These could affect all domains of daily living such as health care, education, vocation, and independent living.
General considerations
-
Transition of adolescents to young adulthood may be facilitated by the medical homes.
-
These vulnerable populations should have written transition plan by 14 years of age and should be updated annually.
-
The timing of transition to an adult health-care practitioner should be individualized for each patient and not based solely on chronologic age.
-
The portable medical summary should include all relevant medical and care information.
-
Encourage patients and families to identify an adult health-care practitioner and involve the practitioner during the transition process.
-
The portable medical summary and written transition plan can be transferred to the new medical home to facilitate sharing of information.
Management
-
Early discussion of future goals with the patient, family, and other members of the team to coordinate the process
-
Promote independence and shared decision-making
-
Identification of potential obstacles to a successful transition in the domains of health care, education, vocation, and independent living
-
Provision of resources to address identified obstacles to a successful transition such as insurance coverage
-
Parents should be encouraged to acknowledge the sexuality of their adolescent and young adult children as well as to foster the development of their social independence.
-
The role of a surrogate decision-maker should be discussed for those with severe intellectual disabilities or mental health conditions.
-
Full independence for medical or other decisions may not be appropriate.
Discipline
-
Disciplinary approaches depend on the child developmental stage.
-
Time-out for negative behavior is an effective strategy for age 1 year to early adolescence.
-
Time-out will be effective if parents also provide time-in with short nonverbal physical contact on a frequent basis for acceptable behavior.
-
Extinction occurs when parent should withdraw all attention with an undesirable behavior. This may initially increase the intensity of the undesirable behavior (extinction burst), but with parental perseverance, the undesirable behavior will diminish.
-
In planned ignoring, the parents gradually ignore the child’s behavior; it tends to take longer but does not lead to an increased undesirable behavior.
-
In chip system, the child earns a chip for positive behavior (ages 3–7 years).
Adoption
General considerations
-
Depending on their country of origin, international adoptees may be at risk for certain infectious diseases, particularly parasitic infections .
-
Children adopted from institutional or orphanage cares are more at risk for such medical and developmental problems than are their counterparts who have resided in foster care.
-
The pediatrician also should help review any information about the child’s medical history (if available) before and after adoption.
-
Adoptive parents need to provide sufficient time, security, and love when the adopted child arrives.
-
Family or parental leaves are recommended to provide consistent caregivers for the child and allow bonding to occur.
-
This will ease the transition of adoptees and their adoptive families.
Evaluation of adopted children
-
Comprehensive physical examination, immunization status and appropriate catch-up immunization
-
Hearing and vision screening
-
Blood specimens for complete blood count (CBC), serum lead concentrations, hepatitis B , human immunodeficiency virus, and syphilis infection status, stool sent for ova and parasites, Giardia lamblia, and Cryptosporidium
-
A tuberculin skin test placed regardless of bacillus Calmette-Guérin (BCG) status. Hepatitis C serologies, if emigrating from hepatitis C endemic area
-
Newborn metabolic screen for infants
Media
Impact of mass media
-
Children younger than 2 years of age should not watch television (TV) .
-
Solitary television viewing should be discouraged in young children.
-
Limiting TV viewing to 2 h/day or less for all children including other forms of screen times.
-
Discourage parents having TV in a child’s bedroom, as it causes sleep disturbance (sleep latency prolongation).
-
Education of parents on links between television viewing, obesity, and diminished academic performance
Potential negative effects of TV viewing on children include
-
Increased aggressive behavior, acceptance of violence, obscures distinction between fantasy and reality; trivializes sex and sexuality
-
Increased passivity, obesity, and risk of suicidal behavior
-
Less time spent in healthier activities
Foster Care
-
Foster care is a system in which a minor who has been placed into a ward, group home, or private home of a state certified caregiver that are compensated for expenses.
-
This is usually arranged through the government or a social-service agency.
-
All legal decisions are made by the state through the family court and child protection agency, the foster parent is responsible for the day-to-day care.
-
Legal guardian/foster parents can consent to medical treatment for children under their care.
-
Family-based foster care is generally preferred to other forms of out-of-home care.
-
Foster care is intended to be a short-term solution until a permanent placement or adoption can be made.
-
Children in foster care suffer more physical, psychological, and cognitive problems.
Enuresis
Background
-
Nocturnal enuresis is involuntary passage of urine during sleep in children older than 5 years of age and occurs in approximately 15 % of children at age 5 and 1 % of teens at age 15.
-
Commoner in males than in females and often a positive family history
-
Nocturnal enuresis is common among school-age children.
-
Children with nocturnal enuresis have been shown abnormal circadian release of antidiuretic hormone (ADH).
-
Most daytime wetting can be classified either as storage or an emptying problem.
Etiology
-
Genetic
-
Gender
-
Maturational delay
-
Psychosocial
-
Sleep state
Risk factors
-
Regressive bed-wetting could be related to a stressful environment or event such as the birth of siblings or moves.
-
Daytime wetting could result from stressful events such as divorce, death of family members, or abuse.
-
Daytime wetting and a difficult temperament are at increased risk for constipation and encopresis .
Management
-
Diurnal enuresis after continence is achieved should prompt evaluation.
-
Treatment approaches for nocturnal enuresis includes counseling, hypnosis, enuresis alarm, imipramine, DDAVP, and reassurance.
-
The use of a bedwetting alarm has the highest rate of success in young children.
-
Daytime incontinence could be secondary to environmental stress, a resistant child or urgency incontinence.
-
Treatment approaches for daytime enuresis include counseling, hypnosis, bladder-training exercises, and anticholinergic (oxybutynin).
-
Patients who have both daytime incontinence and nocturnal enuresis have a higher degree of functional bladder abnormalities and a higher failure rate with conventional treatment than patients experiencing nocturnal enuresis alone.
-
Reassuring parents about coping with enuresis without causing psychological problems.
Encopresis
Background
-
Functional encopresis is defined as repeated involuntary fecal soiling that is non-organic.
-
The most common cause is functional constipation with overflow incontinence.
-
Enuresis and urinary tract infections are comorbidities that need to be addressed.
-
Encopresis predisposes to urinary tract infection and enuresis
-
Anorectal manometry and rectal suction biopsies may rule out Hirschsprung’s disease or neuronal intestinal dysplasia in suspected cases.
Etiology
-
Organic
-
Behavioral
-
Environmental
Management
-
Disimpaction, e.g., GoLytely via NG tube until clear
-
Miralax to be used everyday not as needed
-
Maintenance therapy, which involves a combination of medical therapy, behavioral modification, and counseling.
-
Successful treatment of encopresis varies with the age of onset; and relapses are common.
Psychosomatic Disorders
Somatization
-
Somatization disorders occur in children who are genetically predisposed .
-
Somatization disorders lead to tendency to experience and communicate somatic distress and symptoms unaccounted by pathological findings.
-
Conversion disorders indicate symptoms and signs of sensory or voluntary motor function (e.g., blindness, paresis) without any neuro-anatomical and pathophysiologic explanation.
-
Lack of school attendance should be assessed with every complaint of recurrent pain.
-
Psychosomatic disorders with chronic pain may be manifestations of parental anxiety and parental pressure for a child to succeed.
Clinical presentation
-
The symptoms could be a symbolic attempt to resolve unsolved and unconscious conflicts (primary gain).
-
The symptoms often result in increased attention for the patient (secondary gain).
-
Any form of stress could contribute to psychosomatic disorders; these include bullying, physical or sexual abuse .
-
Organic illnesses must be considered in the differential diagnoses.
-
The common symptoms include chronic pain syndromes of head, chest, abdomen, and legs .
-
Differential diagnosis of conversion symptoms include:
-
Psychophysiology hypochondriasis
-
Malingering
-
Somatic delusions
-
Treatment approaches for psychosomatic disorders include
-
Reassurance when appropriate
-
Cognitive and behavioral interventions
-
Use positive and negative reinforcement
-
Teach self-monitoring techniques (e.g., hypnosis, relaxation, and biofeedback), family and group therapies.
-
Improve communication between clinicians and school
-
Aggressively treat comorbid psychiatric conditions
-
Psychopharmacologic interventions as appropriate
Pain
-
Dealing with and tolerance to pain vary with a child’s developmental stage .
-
Pain is subjective, and repeated painful experiences can result in altered pain sensitivity and behavioral disturbances.
-
Undertreatment of pediatric pain is a concern, especially among neonates.
-
Newborns may be at greater risk for pain wind-up, in which repeated painful stimuli produce central sensitization and a resultant hyperalgesic state. This necessitates adequate management of pain.
-
The goals of pain management are anticipation, treatment, and reassessment.
-
Non-pharmacologic measures include open communication, reassurance, and parental presence.
-
Sucrose use depends on developmental status and condition of the patient .
Sibling Rivalry
-
Sibling rivalry is common.
-
Children should be allowed to resolve their differences initially, but parents need to intervene if physical or verbal abuse happens.
-
The family should be provided guidelines on implementing a behavior intervention strategy.
-
Referral to a therapist may be considered if behavior continues to be challenging and not responsive to initial parental interventions.
-
Sibling rivalry could also manifest with regressive behavior following the birth of a new sibling.
Separation Anxiety and School Refusal
General considerations
-
Anxiety disorders are the most common psychiatric illness in children and adolescents.
-
Anxiety disorders have genetic predisposition and environmental factors.
-
The neurobiology of anxiety disorders is linked to dysregulation in the fear and stress response system in the brain.
-
Separation anxiety disorder is one of the most common causes of school refusal.
-
Separation anxiety is developmentally appropriate in the preschool child and during the first few months of school in kindergarten or first grade.
-
School refusal related to anxiety differs from conduct problems and subsequent truancy.
-
Youth who exhibit truancy generally do not report other symptoms of anxiety or issues of separation from parents.
Treatment
-
In school refusal due to separation anxiety disorder, the child needs to go back to school environment as soon as possible
-
Cognitive behavioral therapy (CBT)
-
Pharmacotherapy: Selective serotonin reuptake inhibitors (SSRIs)
-
Decrease stress, sleep hygiene, healthy eating, and regular exercise, predictable routine and social supports
Sleep Disorders
Normal sleep (Table 2 )
-
Newborns can sleep 16–20 h in a 24-h period, alternating between 1- and 4-h periods of sleep and 1–2 h of being awake .
-
Newborns cycle between rapid eye movement (REM) and non-REM sleep every 50 min
-
At the end of each cycle, the newborn may experience an arousal that is not true awakening.
-
During REM sleep (active sleep in the newborn period), associated movements may occur, which may include facial movements, sucking, and limb movements.
-
By 2 months of age, infants are able to establish a day-night cycle.
-
By 4 months, many infants can sleep uninterrupted through the night.
-
A child of 1 year should be sleeping 13–14 h, primarily during the night.
-
Night waking may be associated with separation anxiety .
Night Terrors
Definition
-
It is a disorder of arousal from delta sleep (slow wave sleep) occurring in the first few hours during rapid transition from non-rapid eye movement (NREM) to REM sleep.
Clinical presentation (Table 3 )
-
Recurrent periods where the individual abruptly wakes from sleeping with a scream accompanied by autonomic nervous system and behavioral manifestations of intense fear
-
Difficulty in arousing the child and the child wants to fall asleep soon after the episode
-
Mental confusion when awakened from an episode and inconsolable
-
Amnesia for the episode
-
The disturbance is not due to the effects of a substance or general medical condition.
Management
-
Awaken child 15 min before terrors occur. Avoid overtiredness.
-
Acute: Be calm; speak in soft, soothing, repetitive tones; help child return to sleep.
-
Protect child against injury.
Nightmare Disorder
-
Clinical presentation
-
Nightmares usually occur during the second half of REM sleep.
-
Recurrent episodes of awakening from sleep
-
Recall of an intensely disturbing bad dream
-
Full alertness on awakening, with little confusion or disorientation
-
Delayed return to sleep after the episode
Management
-
Reassure the child that he or she had a bad dream.
-
Leave bedroom door open, use a nightlight, and demonstrate that there are no monsters under the bed.
-
Discuss dream the following day.
-
Avoid scary movies or television shows.
Vulnerable Child Syndrome
Background
-
Unfounded parental anxiety about the health of a child resulted in disturbances of the parent-child interaction .
-
The parents are overprotective, show separation anxiety, unable to set age-appropriate limits, and display excessive concerns about their child’s health. These lead to overuse medical services.
Risk factors
-
History of serious illness or injury in the child
-
Fertility issues
-
Illness in any family members
-
Serious maternal problems during and after delivery
-
Precious child
-
Prematurity
Exacerbating factors
-
Environmental stress
-
Family stress
-
Lack of social support
-
Low socioeconomic status
-
Poor rating of mother’s health
Effect on children
-
Exaggerated separation anxiety
-
Sleep disorders
-
Peer relationships, self-control, discipline problems
-
School underachievement
-
Hypochondria
-
They may become abusive to their parents.
Management
-
Early recognition and treatment
-
Inquire the sources of the parental anxiety and reeducating them about their child’s health
-
Inquire about connection between past threats and present concerns
-
Close, regular communication between physician and parent should be exact and clear
-
Referral should be made for appropriate therapy .
Rumination
Background
-
Rumination is effortless regurgitation of undigested food meals after consumption .
-
No associated retching, nausea, heartburn odors, or abdominal pains
-
Affecting infants and young children with cognitive disability
-
It has been linked with depression.
-
Due to overstimulation and understimulation from parents and caregivers
-
Seek self-gratification and self-stimulation due to the lack or abundance of external stimuli
-
Habit-induced in adolescents as in past history of bulimia nervosa or of intentional regurgitation
-
Trauma-induced as in emotional or physical injury
Clinical presentation
-
Chewing and swallowing of regurgitated food that has come back into the mouth through a voluntary increase in abdominal pressure within minutes of eating or during eating.
-
It can adversely affect normal functioning and the social lives of individuals.
-
It can also present with weight loss.
Management
-
Complete history and physical examination
-
Minimal invasive investigations
-
Reassurance, explanation, and habit reversal
-
Behavioral and mild aversive training
-
Supportive therapy and diaphragmatic breathing
Gifted Child
Definition
-
Significantly advanced skills and abilities in any developmental domains
Clinical presentation
-
Alertness during infancy
-
Early language development.
-
Advanced vocabulary
-
Abstract thinking; and the ability to generate original ideas
-
Exceptional problem-solving skills
-
Excellent memory skills
-
Provocative and penetrating questions, exceptional curiosity and a heightened sense of wonder
-
Early development of empathy, concern with truth and fairness in play, a mature sense of humor, leadership in cooperative play, and perfectionism
-
Cognitive and academic skills often exceed social emotional and motor skills.
-
They tend to have asynchronous developmental patterns, very advanced in one domain area compared to the rest.
Associated conditions
-
Attention-deficit/hyperactivity disorder
-
Asperger syndrome
-
Oppositional defiant disorder.
-
Learning disabilities
-
All these can have tremendous social and emotional effects on the child, family functioning, and family dynamics.
Management
-
A multidisciplinary team for medical diagnosis, educational, and behavioral interventions
-
Educational decisions such as early school entrance, home schooling, and enrichment programs
-
Home schooling may impair interpersonal experiences and socialization .
Chronic Illness and Handicapping Conditions
General effect of a child with chronic conditions on the family
-
Parents of children with handicapping conditions may exhibit grief reactions and this could affect the siblings .
-
There is increased risk of child abuse among handicapped children.
-
Chronic illness (e.g., asthma , seizures, inflammatory bowel disease) may lead to psychosocial issues.
-
Use of home medical equipment (e.g., oxygen monitors, physical therapy, transportation, hygiene) may have psychosocial effects on the family dynamics.
Management
-
Supportive and nonthreatening discussion with parents whose children have chronic diseases
-
Appropriate ethical decisions relating to children with chronic and handicapping diseases
-
A pediatrician can help the family in the facilitation of a normal progression of a chronically ill or handicapped child to adult behavior, including separation from parents and emerging sexuality in spite of chronic illness .
Transplantation
-
Growth impairment is common after all solid organ transplants.
-
Etiologies of growth impairment may be multifactorial.
-
There may be psychosocial stresses of chronic illness on the child and other family members.
-
Waiting for future of transplantation and the guilt of realizing that someone else has to die to receive a lifesaving organ transplant.
-
Financial burden of time lost from work and fear of organ rejection, organ loss, malignancy, and death
-
Support groups for pretransplantation and posttransplantation periods
-
Adherence with clinic follow-up and medication regimens.
Family Violence
Risk factors
-
Maternal depression,
-
Substance use/abuse
-
Physical injuries may indicate intimate partner violence.
Precipitants of violence by batterers may be
-
Pregnancy
-
Efforts by partner to leave the home
-
Seeking separation or divorce
-
Moving to a shelter
Effect of violence on children
-
Intimate-partner violence may have devastating effects on children such as physical abuse, injury while protecting mother, injury from assault directed at mother, learned aggression , post-traumatic stress disorder and hypervigilance.
-
They may have perception that the world is hostile, little awareness of options for conflict resolution, poor peer relations and impulsiveness.
-
Children exposed to corporal punishment and intimate-partner violence is more likely to exhibit aggressive/violent behaviors than other children.
-
The precipitants of violence by batterers may be pregnancy, efforts by partner to leave the home, seeking separation or divorce, or moving to a shelter.
-
The abused partner frequently seeks medical attention, hesitation in leaving the office; frequent visits to the emergency department and requests for support with transportation or other social concerns.
Management
-
Early identification and reporting especially if suspected child abuse
-
Emergency social work or child protective services
-
Children witnessing intimate partner abuse are more likely to exhibit aggressive behaviors than other children.
Child Abuse
Background
-
Under state laws physicians are legally obligated to report any suspected abuse .
-
Neglect is the most common form of child abuse.
-
Caregiver is the abuser of a child in 90 % of child abuse cases.
-
Failure to thrive may be a manifestation of abuse or neglect in children.
-
Siblings of abused children are at increased risk of abuse.
-
Intimate-partner violence frequently is a risk factor for child abuse.
Risk factors
-
Handicap, hyperactivity
-
Social/situational stresses (e.g., poverty, isolation, family discord, multiple births, parent-child conflicts)
-
Parent stress (e.g., abused as a child, depression, substance abuse)
-
Abusive and neglectful parents often have severely unrealistic expectations for their children’s behavior.
Clinical presentation
-
Poisonous ingestions may be manifestations of child abuse.
-
Bruises
-
Keys to the diagnosis of cutaneous injury include the child’s developmental stage, location, and pattern.
-
Abnormal bruises will be multiple in different planes and different stages of healing.
-
Patterned bruises (belt marks, whips, straps), human bite marks, and frenulum tear.
-
-
Burn
-
Non-accidental burn injury usually involves lower extremities and symmetric.
-
Immersion burns when a child is forcibly held in hot water, show clear delineation between the burned and healthy skin and uniform depth.
-
They may have a stock and glove distribution.
-
Immersion burns may have doughnut pattern in the buttocks.
-
No splash or spill injury indicating that the child was held in place.
-
They may have a stock and glove distribution (Fig. 1)
Fig. 1 
Left:stocking or glove pattern burns and distinct line of demarcation: waterlines. Right: sparing of the soles of the feet
-
-
Common fractures suggestive of child abuse
-
Abusive fractures are seen in children younger than 18 months.
-
Any fracture can be the result of abuse especially in a nonambulatory child.
-
Posterio-medial rib fractures near the costovertebral junction (Fig. 2)
Fig. 2 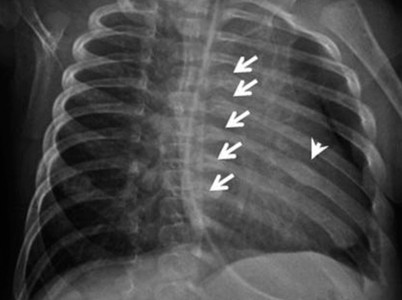
Bone survey done for suspected child abuse showing callus formation posteriorly in ribs 5–9 on the left side (arrows). Callus formation is seen also on the left seventh more laterally (arrow head)
-
Classic metaphyseal lesion (CML) in infants
-
Multiple fractures at different sites and different stages of healing
-
Spiral/oblique or metaphyseal fractures of the humerus (Fig. 3)
Fig. 3 
A 5-month-old boy is brought to the emergency department because of swelling and deformity of the left arm. a Radiograph shows mid shaft humeral fracture. b Bone survey was done which showed meta-physeal corner fracture in the left distal femur (arrow)
-
Spiral/oblique or metaphyseal fractures of the femur (especially in preambulatory children)
-
Fractures of scapulae and sternum are rarely accidental.
-
Dislocated elbow, clavicular fracture, toddler fracture of the tibia are infrequently indicative of physical abuse .
-



Clinical features commonly mistaken with child abuse
-
Normal bruises occur over a bony prominence: forehead, knees, elbows, and shins.
-
Facial scratches on babies from their fingernails
-
Bruises that appear in the same stage of healing
-
-
Mongolian spot, coining, cupping, and urticaria pigmentosa .
-
Accidental burn injuries usually involve the upper part of the body due to exploration and are usually asymmetric.
-
Spill or splash injury is characterized by irregular margins and non-uniform depth.
-
-
Contact burns will show branding type and mirror the object used.
-
Differential diagnosis of inflicted burns includes: staphylococcal impetigo , herpes, contact dermatitis, and toxic epidermal necrolysis.
-
Fractures:
-
Osteogenesis imperfecta
-
Hypophosphatasia
-
Infantile cortical hyperostosis
-
Osteoid osteoma
-
Management
-
Skeletal survey is mandatory in suspected child abuse or in a child with subdural hematoma.
-
Fractures are present in a minority of physically abused children.
-
Chip fracture of metaphysis is commonly due to wrenching or pulling injuries.
-
Radionuclide bone scan can reveal subtle areas of skeletal trauma that may not be seen on plain-film x-ray studies of bones.
-
Physical abuse is the most common cause of serious intracranial injuries during the first year after birth.
-
Absence of neurologic symptoms in infants with intracranial injuries should not exclude the need for imaging.
-
Shaking is a possible cause of coma in the absence of signs of cutaneous trauma.
-
An ophthalmology consultation is needed to identify retinal hemorrhage in suspected head trauma due to shaking.
-
Sexual abuse should usually be reported to the law enforcement agency and must be reported to a state child protection agency.
-
Under state laws, physicians are legally obligated to report suspected abuse although unsubstantiated cases of child abuse produces stress in a family.
-
Unsubstantiated report/finding by a child protection agency does not necessarily mean that abuse or neglect did not occur.
-
The standard of proof in a civil court is the preponderance of evidence.
-
Foster home placement is associated with continued risk of child abuse .
-
There is a need for a team approach in the management of child abuse.
-
Failure to substantiate child abuse may be due to failure to locate child, failure to locate parents, parents’ refusal to speak to investigators, duplicate reports, child’s refusal to repeat history, and non-English speaking family.
-
Many abused and neglected children are not removed from their parents or placed in foster care.
Neglect
Factitious Disorder (Munchausen Syndrome) by Proxy
-
Signs of factitious disorder (Munchausen syndrome) by proxy may include recurrent sepsis from injecting fluids, chronic diarrhea from laxatives, false renal stones from pebbles, fever from heating thermometer, and rashes from trauma, sugar or blood in the urine .
-
The parents and children with factitious disorder (Munchausen syndrome) by proxy may exhibit significant ongoing psychologic problems.
-
Mothers have been identified as the sole perpetrators in the majority of cases.
-
Multidisciplinary child protection team that includes the state social service agencies.
-
Family therapy to address ongoing family issues .
Sexual Abuse
Background
-
Incidence of sexual abuse cases that came to the attention of investigators or other community professionals was 2.4/1000 US children under the age of 18 years.
-
Child sexual abuse involves physical contact between the victim and the perpetrator, with or without oral, anal, or vaginal penetration.
-
There may not be touching and the child is made to watch sexual acts or pornography.
-
Delay between the onset of abuse and disclosure is common.
-
Sexual victimization is more common among girls than boys.
-
Boys are less likely to disclose sexual abuse and might be victimized more often than the reported ratio.
-
Teenagers have the highest rates of sexual assault.
-
The child knows most perpetrators of sexual abuse before the abuse occurs.
-
Physical disabilities, prior sexual victimization, and absence of a protective parent are other potential risk factors.
-
There is increased incidence of sexually transmitted disease associated with sexual abuse.
Clinical presentation
-
An explicit description and imitation of adult sexual behavior by children may indicate either victimization or observation of sexual acts (not fantasy).
-
Sexually abused children also can present with nonspecific physical or emotional complaints.
-
Unexplained abdominal pain, genital pain, encopresis, school failure, or sleep disturbance.
-
A complaint of genital pain and genital discharge may infrequently indicate sexual abuse.
-
When sexual abuse is suspected, the child should be interviewed alone.
-
Verbatim statements by a child may qualify as evidence in a criminal court.
Medical history taking
-
In suspected sexual abuse, the first detailed interview of a child is diagnostically critical.
-
It is essential to avoid repetitive interviewing of an allegedly sexually abused child.
-
Repetitive interviewing may create rote quality to responses, increases likelihood of leading questions, increases chance of learned responses, is unnecessarily stressful, and increases chances of inconsistency/retraction.
-
The use of anatomically correct dolls for interviewing have advantages in a child who is nonverbal that can point and there may be risk of overinterpretation.
-
Sexually abused children also can present with nonspecific physical or emotional complaints .
Examination
-
Explanations to parents and the child before, during, and after the examination can ease stress.
-
Supportive, non-offending caretakers also can be comforting to the child.
-
Older patients can indicate if they prefer to undergo the examination with or without their caretaker in the examination room.
-
The use of chaperones is essential during the examination of pediatric patients.
-
Examination positions include supine lithotomy, supine frog leg, and knee chest position.
-
Patients who refuse should not be forced to undergo an examination.
-
A normal physical examination does not exclude the possibility of sexual abuse or prior penetration.
-
The majority of sexual abuse victims have normal anogenital examinations.
-
Findings indicative of trauma include laceration or bruising of the hymen, genital or perianal bruising, and hymenal transection.
-
Labial adhesions, vulvar erythema, and anal tags are not signs of abuse .
Investigations
-
Chlamydial infection may be acquired from the mother at birth and may persist.
-
Sexually transmitted disease in a prepubertal child is presumptive evidence of sexual abuse.
-
It is very important to use gold standard tests to diagnose sexually transmitted diseases in children because of the legal issues involved.
-
Findings diagnostic of sexual contact include pregnancy, sperm on a specimen taken directly from patient’s body.
-
Evidence of seminal fluid is infrequently found in sexually abused children.
-
Seminal fluid is unlikely to be found/persist beyond 72 h in a sexually abused child.
-
Recognize that sexual abuse can recur even when families are receiving treatment.
-
Send serologic studies for human immunodeficiency virus (HIV), syphilis, and hepatitis B .
-
Wet mounts and other studies of vaginal discharge can identify Trichomonas vaginalis and bacterial vaginosis.
-
Bacterial vaginosis can be unrelated to sexual abuse.
-
Polymerase chain reaction testing or culture of genital lesions can test for herpes simplex virus.
-
Specimens from the rectum, male urethra, vagina, and urine can be tested for Chlamydia trachomatis and Neisseria gonorrhoeae.
-
Throat specimens also can be tested for gonorrhea.
-
Nucleic acid amplification tests (NAATs) for chlamydia and gonorrhea infections in urine.
-
HIV, trachomatis, gonorrhea, and syphilis are diagnostic of sexual abuse when perinatal, transmission from transfusions or needle sticks, and rare nonsexual transmissions are excluded.
-
Anogenital warts (condyloma acuminata) and genital herpes simplex are suspicious and not diagnostic of abuse.
-
Laboratory testing at the time of initial presentation, convalescent testing for syphilis and HIV are indicated at 6, 12, and 24 weeks’ post-assault.
-
Repeat Chlamydia and gonorrhea testing within 2 weeks after the last contact is indicated in cases in which prophylactic treatment was not given.
-
Pregnancy testing should be performed where indicated based on the patient’s pubertal stage.
Treatment
-
Treatment plans address physical health, mental health, child safety, and psychosocial concerns.
-
Prophylactic antibiotics for gonorrhea, chlamydia infection, trichomonas infection, and bacterial vaginosis for patients who present within 72 h of an assault.
-
These prophylactic antibiotics generally are not prescribed for prepubertal patients because the incidence of sexually transmitted infection (STI) is low. There is low risk of spread to the upper genital tract.
-
HIV postexposure prophylaxis involves a 28-day course of a two to three drug regimen initiated as soon as possible within 72 h of potential exposure, and careful follow-up.
-
Emergency contraception should be offered when female pubertal patients present within 72 h till 120 h.
-
Mental health issues need to be addressed and urgent psychiatric referral if suicidal ideations.
-
It is very important not to assign blame to the victim in helping families cope with sexual abuse.
-
Recognize that sexual abuse can recur even when families are receiving treatment .
Suggested Readings
Asnes AG, Leventhal JM. Managing child abuse: general principles. Pediatr Rev. 2010;31:47–55.
Dubowitz H, Feigelman S, Lane W, Kim J. Pediatric primary care to help prevent child maltreatment: the Safe Environment for Every Kid (SEEK) model. Pediatrics. 2009;123:858–64.
Flaherty EG, Sege RD, Griffith J, et al. From suspicion of physical child abuse to reporting: primary care clinician decision-making. Pediatrics. 2008;122:611–9.
Fortin K, Jenny C. Sexualabuse. Pediatr Rev. 2012;33:19–32.
Brown P, Tierney C. Munchausen syndrome by proxy. Pediatr Rev. 2009;30:414–5.
American Academy of Pediatrics, Committee on Fetus and Newborn; Fetus and Newborn Committee. Prevention and management of pain in the neonate: an update. Pediatrics. 2006;118:2231–41.
Holsti L, Grunau RE. Considerations for using sucrose to reduce procedural pain in preterm infants. Pediatrics. 2010;125:1042–47.
Zeltzer LK, Krane EJ. Pediatric pain management. In: Kliegman RM, Stanton BF, St. Geme JW III, Schor NF, Behrman RE, editors. Nelson textbook of pediatrics, 19th ed. Philadelphia: Saunders Elsevier; 2011. p. 360–75.
Pagel JF. Nightmares and disorders of dreaming. Am Fam Physician. 2000;61:2037–42, 2044.
Zuckerman B. Nightmares and night terrors. In: Parker S, Zuckerman B, Augustyn M, editors. Developmental and behavioral pediatrics: a handbook for primary care. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 251–2.
Gold LM, Kirkpatrick BS, Fricker FJ, Zitelli BJ. Psychosocial issues in pediatric organ transplantation: the parents’ perspective. Pediatrics. 1986;77:738–44.
Bhargava S. Diagnosis and management of common sleep problems in children. Pediatr Rev. 2011;32(3):91–9.
Pipan M, Blum N. Basics of child behavior and primary care management of common behavioral problems. In: Voight RG, Macias MM, Myers SM, editors. Developmental and behavioral pediatrics. Elk Grove Village: Pediatrics; 2011, p. 49–50.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Kukoyi-Maiyegun, S. (2015). Psychological Issues and Problems. In: Naga, O. (eds) Pediatric Board Study Guide. Springer, Cham. https://doi.org/10.1007/978-3-319-10115-6_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-10115-6_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-10114-9
Online ISBN: 978-3-319-10115-6
eBook Packages: MedicineMedicine (R0)