
Abstract
Ultrasound images are coupled with anatomical schemes explaining probe positioning and scanning technique for the Adductors, Gracilis and Pectineus muscles. For each muscle, a brief explanation of normal anatomy is also provided, together with a list of tricks and tips and advice on how to perform the ultrasound scan in clinical practice.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Adductors and Pectineus Muscles
1.1 Anatomy key points: Adductors
The adductor muscles are composed of the adductor longus, brevis, and magnus muscles (Fig. 10.1).

Anatomical scheme of medial thigh muscles. PE pectineus, GR gracilis, AL adductor longus, AB adductor brevis, AM adductor magnus
The main function of these muscles is to adduct and to rotate internally the thigh and to stabilize the hip joint. The adductor longus can also flex the extended thigh, while the adductor magnus extends the thigh at the hip joint level. The adductor longus muscle is the most anterior muscle in the adductor group and originates from the anterior pubis, just lateral to the pubic symphysis. It is a slender and triangular muscle, lateral to adductor brevis and magnus muscles and medial to the vastus medialis muscle. The muscle belly of adductor longus becomes progressively thinner caudally, and its fibers run downwards and laterally to attach to the middle third of linea aspera of femur, anterior to adductor magnus and brevis and posterior to vastus medialis insertions.Linea aspera is a rough crest of bone running down the posterior shaft of the femur in its middle third. The adductor brevis muscle is a short and triangular-shaped muscle; the upper aspect of its belly is posterior to pectineus, while its lower aspect is posterior to adductor longus muscle. It originates from the lateral part of the front of the body of the pubis and from the inferior pubic ramus. It distally attaches between the lesser trochanter and the superior end of linea aspera, anteriorly to adductor magnus insertion. Finally, the largest and the most posterior of adductor muscle group is the adductor magnus muscle. It is a large triangular-shaped muscle with a thick medial margin that originates from the femoral surface of the ischiopubis ramus and the lateral part of the inferior surface of the ischial tuberosity. It lies anteriorly to semimembranosus and semitendinosus muscles and posteriorly to adductor longus and brevis muscles. This muscle has two different components: the adductor and the hamstring part. The adductor portion attaches with a wide aponeurosis on the medial margin of the linea aspera of the femur; the hamstring part attaches by a rounded tendon to adductor tubercle on top of the medial condyle of femur. Some of these fibers continue vertically downwards fusing with the medial collateral ligament of the knee. The most anterior ischiopubic fibers course from linea aspera to the greater trochanter medially to the insertion of the gluteus maximus. The two bellies converge distally forming the roof of the adductor canal, a conical-shaped pathway that contains the femoral vessels, saphenous nerve, and fibrous tissue.
1.2 Anatomy Key Points: Pectineus
The pectineus muscle is a flat and quadrangular-shaped muscle; it is located in the upper and medial aspect of the thigh deep in the groin. It lies between iliopsoas and adductor longus muscles. These three muscles form the floor of the femoral triangle of Scarpa. The pectineus muscle consists of two layers: the superficial and the deep one. It arises from the pectin pubis (pectineal line of the pubis) and from the surface of bone in front of it, between the iliopectineal eminence and pubic tubercle. Some fibers also come from the fascia covering the anterior surface of the muscle. It runs vertically downward, backward, and lateral and inserts into the posterior surface of the femur, along the line of the lesser trochanter to the linea aspera. This line is called the pectineal line of the femur. The pectineus muscle is in relation anteriorly with the pubic portion of the fascia lata, which separates it from the femoral artery and vein and internal saphenous vein and posteriorly with the capsule of the hip joint and with the obturator externus and adductor brevis muscles. The femoral nerve provides the main innervation of the pectineus muscle although it may sometimes receive additional innervation for its deep portion from the obturator nerve called the accessory obturator nerve.
1.3 Ultrasound Examination Technique
The patient is supine, with the thigh abducted and externally rotated and the knee bent (frog leg position) (Fig. 10.2).

Lower limb position (frog leg position) to evaluate the adductor muscles
Holding the transducer in a longitudinal position localize the anterior surface of the pubis, which can be considered an important bony landmark for US examination. Then identify the insertional components of the adductor muscles and three muscle layers: from the most superficial to the deepest, the adductor longus, the adductor brevis, and the adductor magnus (Fig. 10.3). The myotendinous junction of the adductor longus is seen with its triangular hypoechoic shape and its tendon results eccentric to muscle belly.

(a) Anatomical scheme of medial thigh compartment muscles. (b) Probe position to evaluate the proximal insertion of adductor muscles in the anterior surface of the pubis on the sagittal plane. PE pectineus, AB adductor brevis, AL adductor longus, AM adductor magnus, GR gracilis. (c) US sagittal scan: note the three muscle layers represented from superficial to deepest by adductor longus (AL), adductor brevis (AB), and adductor magnus (AM) muscles
With the probe always in the same position, pay attention to the profile of the pubic symphysis because a bone surface irregularity could represent a direct sign of osteitis pubis.
Shift the transducer cranially to evaluate the tendon of rectus abdominis muscle, which is in direct continuity with the adductor longus tendon. Therefore a single continuous structure, termed the common adductor–rectus abdominis origin, forms a critical anatomic and biomechanical structure, playing an important role as dynamic stabilizer of the pubic symphysis (Fig. 10.4).

US longitudinal scan at level of pubic symphysis (P) that shows the anatomical relationship between the tendon of the adductor longus (AL) and the tendon of the rectus abdominis (RA)
The long-axis US plane is useful for determining an avulsion injury of the tendon of the adductor muscles especially of the adductor longus tendon and less frequently of the adductor brevis tendon.
Rotate the transducer by 90° to evaluate the adductor insertions on axial plane and move down the transducer to detect and evaluate the course of each muscle belly (Fig. 10.5).

US axial scan at proximal third of the thigh that shows the anatomical relationship between the adductor longus (AL), adductor brevis (AB), adductor magnus (AM), and gracilis (G) muscles
Three muscle layers are recognized on axial planes: the superficial one is represented by the adductor longus (lateral) and the gracilis (medial) muscles, the intermediate by the adductor brevis muscle, and the deepest by the adductor magnus muscle (Figs. 10.6 and 10.7).

US axial scan performed with a convex probe at proximal third of the thigh, showing a panoramic view of muscular anatomy of the medial compartment. AL adductor longus muscle, AB adductor brevis muscle, AM adductor magnus muscle, GM gluteus maximus muscle, GR gracilis muscle, F femur, FV superficial femoral vascular bundle

Anatomical scheme correlated to EFV US axial scan at the proximal third of the thigh showing the anatomical relationship among the pectineus (PE), adductor longus (AL), adductor brevis (AB), adductor magnus (AM), and gracilis (GR). At this level the most superficial muscles are AL and GR; AB lies just deeper to AL; AM appears as a large muscle posterior and deeper to AB. Note the superficial femoral neurovascular bundle
Swipe the transducer distally on an axial scan to distinguish each muscle belly. Femoral neurovascular bundle, placed between the vastus intermedius, the sartorius, and the adductor longus muscles, should be used as an important landmark: the adductor muscles lie medially to the femoral artery and vein (Fig. 10.8).

US axial scan with color Doppler at level of the femoral vascular bundle. The adductor longus (AL) and the pectineus (PE) muscles lie medial to the femoral vascular bundle
Following the course of the adductor longus muscle, its cross-sectional area progressively decreases until its distal insertion on the middle third of the linea aspera (Fig. 10.9).

Anatomical scheme correlated to US axial scans at different levels (a–d) of the adductor longus muscle . Note that muscle cross-sectional area progressively decreases
US are not able to distinguish the thin distal tendon because it is positioned too deep.
Continue the exam with an axial scan of the adductor brevis muscle performed at the upper third of the thigh. At this level, it lies superolaterally to adductor longus muscle. Caudally it becomes deeper than adductor longus muscle.
With axial scans, also evaluate the adductor magnus muscle that appears as a large muscle deep and posterior to adductor longus (Fig. 10.10).

At middle third of the thigh (a) US axial scan (b) that shows the anatomical relationship between the adductor longus (AL), adductor magnus (AM) muscles
Ultrasound allows a reliable assessment of the proximal components of adductor muscles; conversely the distal insertion of these muscles is hard to examine because of the deep location and the anatomical intrinsic complexity.
Also color Doppler examination may be useful to evaluate the femoral vessels patency, representing a crucial part of ultrasound examination of the medial compartment of the thigh.
Conclude the examination of the adductor muscles performing axial or longitudinal scan during isometric contraction, which is useful to evaluate even small muscular injuries.
2 Gracilis Muscle
2.1 Anatomy Key Points
The gracilis muscle, as its name implies, is a long, slim, strip-like muscle. It is the most superficial adductor muscle and lies on the medial aspect of the thigh and the knee. Gracilis muscle adducts and flexes the thigh at the hip joint and aids the flexion of the knee. It originates by a thin aponeurosis from the front of the body and the inferior ramus of the pubis. It runs vertically downwards between semimembranosus posteriorly and sartorius anteriorly, and its belly develops a fusiform shape at its middle third. The gracilis muscle becomes tendinous above the knee and inserts into the anteromedial surface of the superior aspect of the tibial shaft. This distal attachment is located anteriorly to the semitendinosus and blends with the posterior aspect of the sartorius insertion. A few fibers of the lower part of the tendon continue into the deep fascia of the leg. Crossing both hip joint and knee joint, it is the only two-joint adductor muscle. Gracilis, sartorius, and semitendinosus tendons, which are conjoined proximally on the medial side of the tibia, form the pes anserine. These three tendons are separated from the medial collateral ligament by the pes anserinous bursa, which is a fluid-filled vesicle. It secretes synovial fluid in order to reduce friction between tissues and also works as a cushion for bones, tendons, and muscles. The inflammation of the bursa does not appear suddenly but rather progresses over a period of time.
2.2 Ultrasound Examination Technique
Continue the exam visualizing the gracilis muscle in short axis from proximal to distal insertion (Figs. 10.11 and 10.13).

Anatomical scheme, probe position and US axial scans at different levels of the gracilis muscle (GR). Cross-sectional area progressively decreases from the proximal third of the thigh to the distal myotendinous junction (arrowhead) (a–c). AB adductor brevis muscle
Place the probe with an axial scan at upper third of the thigh and identify the gracilis muscle belly superficial and medial to adductor muscles, just below the subcutaneous tissue. Follow it up to the anteromedial aspect of the superior tibial shaft where the gracilis tendon inserts.
Then turn the probe by 90° to evaluate the myotendinous junction and the distal attachment of gracilis tendon on the anteromedial aspect of the tibia on its long axis (Figs. 10.12, 10.16, and 10.17).

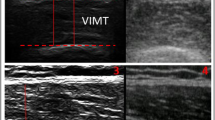
(a) US probe position to assess the myotendinous junction and the distal insertion of gracilis (GR) muscle on longitudinal plane. (b) US longitudinal scan of gracilis (GR) muscle myotendinous junction

US axial scan performed with convex probe at proximal third of the thigh showing a panoramic view of muscular anatomy of the medial compartment. AL adductor longus muscle, AB adductor brevis muscle, AM adductor magnus muscle, GM gluteus maximus muscle, GR gracilis muscle, F femur, * superficial femoral vascular bundle
3 Pes Anserinus
3.1 Anatomy Key Points
The common attachment of the sartorius, gracilis, and semitendinous tendons, on the anteromedial aspect of the proximal tibia, forms a structure that resembles the natatory membrane of the goose; therefore, it has been called “goosefoot” or, from the Latin, “pes anserinus” (Fig. 10.14). The main function of these muscles is to flex the knee but also to aid the internal rotation of the tibia, protecting the knee against valgus stress.

Anatomical scheme of pes anserinus. SA sartorius muscle, GR gracilis muscle, ST semitendinosus muscle
The anserinus bursa is located deep to pes anserina tendons and superficial to the insertion of the tibial collateral knee ligament. Usually, this bursa does not communicate with the knee but sometimes can communicate with the subtendinous bursa of sartorius.
3.2 Ultrasound Examination Technique
US is an excellent imaging technique to evaluate superficial soft tissues, such as tendons and bursae.
For examination of pes anserine tendons, the patient lies supine and rotates the leg externally with the knee flexed about 30° (Fig. 10.15).

Lower limb position to evaluate the pes anserinus
Place the transducer on the medial aspect of the obliquely oriented knee, over the long axis of the medial collateral ligament. Then, move the transducer caudally following the medial collateral ligament (Fig. 10.16). Distally, rotate the transducer forward to visualize the “goosefoot” tendons (sartorius, gracilis, and semitendinosus) in their short axis (Fig. 10.17).

(a) US probe position to evaluate the pes anserinus on longitudinal plane. (b) Anatomical scheme of pes anserinus. SA sartorius muscle, GR gracilis muscle, ST semitendinosus muscle. (c) US longitudinal scan shows the distal insertion of the pes anserinus tendons (arrowheads) on the surface of the tibia (T) medial to the tibial tuberosity

(a) US probe position to evaluate the pes anserinus on axial plane. (b) Anatomical scheme of pes anserinus. SA sartorius muscle, GR gracilis muscle, ST semitendinosus muscle. (c) US axial scan shows the distal insertion of the pes anserinus tendons on the surface of the tibia (T) medial to the tibial tuberosity. circles sartorius tendon, arrowhead gracilis tendon, * semitendinosus tendon
These tendons are very close to each other at the level of the tibial insertion, so they cannot be easily distinguished from each other with ultrasound.
Complete the examination with the measurement of the thickness of the pes anserine insertion (mean normal value ≤2,5 mm), the intratendinous and subcutaneous fat features, and the physiological absence of fluid collection in the bursa, which results to be virtual in normal conditions.
4 Hunter’s Canal
Focus On
The adductor canal, or Hunter’s canal (Fig. 10.18), was firstly described by John Hunter in 1786; it is an aponeurotic-fibromuscular tunnel delimitated by the vastus medialis muscle anterolaterally, adductor longus and magnus muscles posteriorly, and sartorius muscle medially and by a strong aponeurosis that extends between the adductors across the vessels, to vastus medialis (vastoadductor membrane) anteromedially. This aponeurotic tunnel, located in the middle third of the thigh, runs from the apex of the femoral triangle (Scarpa’s triangle) to a passage in adductor magnus. The femoral vessels leave the adductor canal to reach the popliteal fossa.

Anatomical scheme of Hunter’s canal with focus on the proximal (a) and distal part (b). SA sartorius muscle, AL adductor longus muscle, AM adductor magnus, VM vastus medialis muscle, * saphenous nerve, ° femoral artery, ^ femoral vein, @ descending genicular artery
Two different entrapment syndromes are related to compression of the neurovascular bundle inside the adductor canal: the vascular one presents as a claudication syndrome, while the nervous one brings on the compression of the saphenous nerve at the adductor hiatus resulting in pain on the medial aspect of the knee. The muscular hypertrophy may play an important role in the pathophysiological compressive mechanism.
4.1 Ultrasound Examination Technique
High-end ultrasound machine equipped with high-resolution transducers are required for the evaluation of Hunter’s canal and its neurovascular content.
The patient lies supine with the thigh abducted and externally rotated and the knee bent (frog leg position) (Fig. 10.1).
Place the linear probe on an axial plane at level of crural region, at the apex of the Scarpa’s triangle, where the sartorius muscle crosses anteriorly the superficial femoral artery: a superficial vessel in relation with the deep fascia of sartorius muscle.
Move the transducer caudally to reach the superficial femoral artery, branch of the common femoral artery, when it enters in the adductors’ canal (Fig. 10.19).

(a) US probe position on the crural region at the apex of the femoral triangle. (b) color Doppler axial scan. The deep fascia (arrowhead) of sartorius muscle (SA) is in relation with the anterior aspect of the superficial femoral artery wall (A). V femoral vein
The examination continues with exploration of proximal part of Hunter’s canal: the saphenous nerve, the largest cutaneous branch of the femoral nerve, is lateral to the superficial femoral artery; the femoral vein is posterior to the artery. The saphenous nerve presents a fascicular echostructure, with a hyperechoic oval structure, surrounded by a rim of hypoechoic perineural fat. Note the typical “honeycomb” appearance of the saphenous nerve. The adductor longus muscle is the posterior wall of Hunter’s canal (Fig. 10.20).

(a) US probe position on the anteromedial aspect of the thigh. (b) Axial oblique US scan showing the neurovascular bundle inside the proximal third of the adductor canal. The saphenous nerve (arrowheads) is lateral to the femoral artery ; the femoral vein (fv) is posterior. The posterior wall is represented by adductor longus muscle (AL). Note the “honeycomb” echostructure of the saphenous nerve, adjacent to the arterial wall. SA sartorius muscle, VM vastus medialis muscle
From this position, shift the probe caudally to follow the neurovascular bundle in the second part of the adductor canal where the posterior-medial wall is represented by adductor magnus muscle: the saphenous nerve becomes progressively more anterior to the superficial femoral artery (Fig. 10.21).

(a) US probe position on the anteromedial aspect of the thigh. (b) Axial oblique US scan showing the neurovascular bundle inside the middle third of the adductor canal. The saphenous nerve (calipers) moves from a lateral position to the femoral artery (A) to an anterior position to this vessel near the hiatal region. The saphenous nerve may be identified on axial US scans between the anterior surface of the arterial wall and the deep fascia of sartorius (SA) muscle. VM vastus medialis muscle
Then, move the transducer caudally on the anteromedial aspect of the distal third of the thigh to reach the origin of the descending genicular artery from the superficial femoral artery, which represents a precise landmark to identify the distal end (hiatal region) of the adductor canal. At this level the femoral artery and vein are deeper than saphenous nerve (Fig. 10.22).

(a) US probe position on the anteromedial aspect of the distal third of the thigh. (b) Axial US scan showing the neurovascular bundle inside the middle third of the adductor canal. Femoral vessels (* femoral artery, fv femoral vein) and saphenous nerve (arrowheads) diverge at this level. The saphenous nerve is adjacent to the descending genicular artery (dga), which may not be confused with a large, more proximal, muscular branch of the femoral artery to vastus medialis
Rotate the transducer by 90° to evaluate the descending genicular artery on its longitudinal plane.
The coronal oblique US scan shows the relation between descending genicular artery and adductor magnus rounded tendon, which forms the medial wall of the adductor canal hiatus.
At this level, use the adductor tubercle of the medial femoral condyle as a bony landmark to identify the rounded tendon of adductor magnus that presents a fibrillar echostructure. Slight cranially the probe, always in the coronal oblique scan plane, to visualize the myotendinous junction of the tendon itself. The superficial femoral vessels are lateral to the myotendinous structure (Fig. 10.23).

(a) US probe position on the medial femoral condylar region. (b) Coronal oblique US scan at the adductor tubercle (AT) of the medial femoral condyle; the adductor magnus rounded tendon (arrowheads) shows the typical fibrillar pattern. AM adductor magnus muscle
The color Doppler module may aid the detection of the neurovascular bundle at all levels of the Hunter canal.
5 Summary Table
Muscle | Origin | Insertion | Action | Nerve supply |
|---|---|---|---|---|
Gracilis | Inferior ramus of pubis; ramus of ischium body and inferior ramus of the pubis | Anteromedial surface of the superior part of the shaft of the tibia | Adduction of the thigh; flexion of the leg | Obturator nerve |
Adductor longus | Anterior pubis | Middle third of linea aspera of femur | Adduction of the thigh and assistance in lateral rotation | Obturator nerve |
Adductor brevis | Body of the pubis and inferior pubic ramus | Linea aspera of femur | Adduction of the thigh and assistance in lateral rotation | Obturator nerve |
Adductor magnus | Femoral surface of the ischiopubis ramus and inferior surface of the ischial tuberosity | Linea aspera of femur; adductor tubercle of femur | Adduction of the thigh and assistance in lateral rotation. Hamstring part extends thigh | Obturator nerve and tibial part of sciatic |
Pectineus | Pectineal line and the surface of bone between the iliopectineal eminence and pubic tubercle | Pectineal line | Flexion and adduction of the thigh and assistance in medial rotation | Femoral nerve and accessory obturator nerve |
Suggested Reading
Bianchi S, Martinoli C (2007) US of the musculoskeletal system. Martinoli, Berlin/New York: Springer
de Souza RR, de Carvalho CA, König B Jr (1978) Topographical anatomy of adductor canal: form, limits and constitution of its walls. Rev Paul Med 92(1–2):6–9
Drake RL, Vogl W, Mitchell A (2005) Grey’s anatomy. Elsevier/Churchill Livingstone: Drake, Edinburgh
Gilmore J (1998) Groin pain in the soccer athlete: fact, fiction, and treatment. Clin Sports Med 17:787–793
Hunter LY, Louis DS, O’connor GA (1979) The saphenous nerve: its course and importance in medial arthrotomy. Am J Sports Med 7(4):227–230
Paparo F, Sconfienza LM, Muda A, Grillo G, Lacelli F, Silvestri E (2008) High-resolution ultrasound (HRUS) evaluation of neurovascular and muscular structures of the Hunter canal. Skeletal Radiol 37:575–596
Scholten FG, Mali WP, Hillen B, van Leeuwen MS (1989) US location of the adductor canal hiatus: morphologic study. Radiology 172(1):75–78
Silvestri E, Muda A, Sconfienza LM (2012) Normal ultrasound anatomy of the musculoskeletal system. Silvestri, Milan/New York: Springer
Stoller DW (2007) Stoller’s Atlas of orthopaedics and sports medicine. Lippincott Williams & Wilkins: Stoller, Philadelphia
Tschirch FTC, Schmid MR, Pfirrmann CWA et al (2003) Prevalence and size of meniscal cysts, ganglionic cysts, synovial cysts of the popliteal space, fluid filled bursae, and other fluid filled collections in asymptomatic knees on MR imaging. AJR Am J Roentgenol 180:1431–1436
Tyler TF, Silvers HJ, Gerhardt MB, Nicholas SJ (2010) Groin injuries in sports medicine. Sports Health 2:231–236
Valenti A, Frizziero A, Bressan S, Zanella E, Giannotti E, Masiero S (2012) Insertional tendinopathy of the adductors and rectus abdominis in athletes: a review. Muscles Ligaments Tendons J 2(2):142–148
Vitiello FS (1975) Anatomical and surgical notes on the morphology of Hunter’s canal. Minerva Med 66(15):706–710
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Corazza, A., Silvestri, E. (2015). Adductors, Gracilis, and Pectineus. In: Ultrasound Anatomy of Lower Limb Muscles. Springer, Cham. https://doi.org/10.1007/978-3-319-09480-9_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-09480-9_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-09479-3
Online ISBN: 978-3-319-09480-9
eBook Packages: MedicineMedicine (R0)