
Abstract
Rubella is a rare, acute, contagious disease spread via droplet transmission that has become infrequent worldwide due to effective vaccination programs. The clinical syndromes vary based on the manner of exposure to the virus. The congenital rubella syndrome consists of hearing impairment, ocular anomalies, and congenital heart disease. Acquired rubella most commonly manifests as a conjunctivitis that requires no treatment. There is growing evidence to support a causal association with Fuchs heterochromic iridocyclitis and chronic rubella infection as demonstrated by the presence of rubella-specific intraocular antibody production in the anterior chamber.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Rubella, also called German measles, is an acute exanthematous disease spread by droplet transmission. The virus is comprised of single-stranded RNA that is highly contagious. Since the advent of vaccination programs, the incidence of outbreaks of rubella has plummeted worldwide. By 2004, the US Centers for Disease Control (CDC) declared that rubella had been eliminated in the United States [1]. There are two distinct clinical syndromes that involve the eye: congenital and acquired. The classic triad of congenital rubella includes hearing impairment, ocular anomalies, and congenital heart disease. Acquired rubella typically manifests as a mild febrile illness with associated maculopapular rash that initially appears on the face and then spreads to involve the whole body within 24 h. The ocular manifestations of acquired rubella can include conjunctivitis, keratitis, uveitis, and retinitis. There is an association between rubella virus with Fuchs heterochromic iridocyclitis (please see chapter in this book).
Epidemiology
Before the advent of widespread vaccination programs, outbreaks of rubella usually occurred every 6–9 years in the United States mostly affecting children ages 5–9. Since the introduction of the rubella vaccine in 1969, occurrences are rare in those countries with high vaccination rates. By 2002, rubella vaccines were available worldwide and by 2006, 123 of 212 countries had national immunization programs (~58 %) [2]. The CDC declared the rubella virus was eliminated from the US in 2004 [1].
Clinical Manifestations
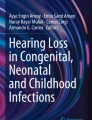
The clinical manifestations of rubella are differentiated based on the mode of exposure to the virus. Congenital rubella syndrome can occur in a developing fetus of a pregnant woman who has contracted the rubella virus usually in the first trimester. If the infection occurs within the first month of conception, the infant has a 43 % chance of being affected [3]. The classic triad of congenital rubella syndrome includes hearing impairment (58–80 %), ocular anomalies (43–78 %), and congenital heart disease (30–50 %) [4]. Cognitive impairment is also a common associated complication. The ocular manifestations include pigmentary retinopathy (aka “salt and pepper” retinopathy—see Fig. 11.1), cataract, strabismus, and glaucoma. Pigmentary retinopathy is the most common ophthalmic complication of the syndrome (reported in 9–88 % of patients with ocular involvement) [5].

Fundus photograph montage of a patient with pigmentary retinopathy secondary to congenital rubella syndrome
Acquired rubella manifests as a maculopapular rash and mild systemic symptoms including fever and lymphadenopathy. The incubation period for the virus is 14–18 days, and infected individuals may shed virus and are potentially contagious for 1–2 weeks before the onset of classic symptoms. Arthritis and arthralgias occur in approximately 70 % of teenagers and adult females; this complication rarely develops in children and adult males [1]. The most common ocular manifestation is conjunctivitis which is present in 70 % of patients. Other ocular sequelae include epithelial keratitis and retinitis. There has been growing evidence to support a causal association with chronic rubella virus infection and Fuchs heterochromic iridocyclitis. This has been proposed due to the presence of rubella-specific intraocular antibody production in the anterior chamber of patients with Fuchs [6].
Diagnosis
The diagnosis of congenital rubella is established via the presence of maternal rubella infection and congenital anomalies. Serologic data can confirm the diagnosis via the detection of rubella-specific IgM antibodies in the infant or cord blood. The diagnosis of acquired rubella can be established by a fourfold increase in rubella-specific IgG titers obtained 1–2 weeks apart or the new appearance of rubella-specific IgM.
Treatment
Treatment for those afflicted with rubella virus is typically supportive care: there is no specific therapy. For women in the first 20 weeks of pregnancy with exposure to the virus, immune globulin may be administered to prevent both maternal and fetal infection. For those with acquired rubella, no treatment is indicated for the conjunctivitis or keratitis as these are self-limited. The uncommon manifestation of rubella retinitis responds well to systemic steroids. The treatment for Fuchs heterochromic iridocyclitis is detailed in the respective chapter of this text.
Conclusion
Rubella is an exceedingly rare acute infection spread via droplet transmission that has been eradicated in the United States per the CDC due to effective vaccination programs. The congenitally acquired variant of this disease can induce significant harm to the fetus including hearing loss and pigmentary retinopathy. The acquired form generally poses little risk to ocular structures.
References
Atkinson W, Wolfe S, Hamborsky J. Centers for disease control and prevention epidemiology and prevention of vaccine-preventable diseases, Pink Book, Washington. DC: Public Health Foundation; 2011.
Reef SE, Cochi SL. The evidence for the elimination of rubella and congenital rubella syndrome in the United States: a public health achievement. Clin Infect Dis. 2006;43(Supplement 3):S123–5.
Freij BJ, South MA, Sever JL. Maternal rubella and the congenital rubella syndrome. Clin Perinatolo. 1988;15(2):247–57.
Oster ME, Riehle-Colarusso T, Correa A. An update on cardiovascular malformations in congenital rubella syndrome. Birth Defects Res Part A: Clin Mol Teratolo. 2010;88(1):1–8.
Givens KT, Lee DA, Jones T, Lustrup DM. Congenital rubella syndrome: ophthalmic manifestations and associated systemic disorders. Br J Ophthalmol. 1993;77:358–63.
de Groot-Mijnes JD, De Visser L, Rothova A, Schuller M, van Loon AM, Weersink AJ. Rubella virus is associated with Fuchs heterochromic iridocyclitis. Am J Ophthalmol. 2006;141(1):212–4.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Papaliodis, G.N. (2017). Rubella. In: Papaliodis, G. (eds) Uveitis. Springer, Cham. https://doi.org/10.1007/978-3-319-09126-6_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-09126-6_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-09125-9
Online ISBN: 978-3-319-09126-6
eBook Packages: MedicineMedicine (R0)