
Abstract
Post-traumatic stress disorder (PTSD) has a prevalence of 6.8 % among the American population and an even greater prevalence among combat veterans. The conventional view of PTSD has been as a psychological adjustment disorder characterized by depression and anxiety in response to stressful circumstances. Recently, however, it has become apparent that it is much more than a psychological adjustment disorder. This began with the appreciation of the fact that dementia is much more common in PTSD, suggesting neurological changes in the disorder. There is now evidence for psychiatric changes (e.g., mood disorders, substance use and abuse), cardiovascular changes, autoimmune changes (e.g., rheumatoid arthritis), tumorigenic changes, etc. The goal of this chapter is to briefly review the evidence for systemic involvement in preparation for subsequent chapters that will focus on detailed discussions of each organ system.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others



Keywords
Introduction
Post-traumatic stress disorder (PTSD) affects those exposed, either directly or indirectly, to life-threatening or severely traumatic events. The diagnosis of PTSD, as defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), requires (1) presentation of symptoms associated with the four diagnostic symptom clusters (intrusion symptoms, avoidance, negative alterations in cognitions and mood, and alterations in arousal and reactivity), (2) all symptoms beginning or worsening after the trauma, (3) symptoms persisting for more than 1 month, (4) significant symptom-related or functional impairment, and (5) that these symptoms are not caused by medication, substance use, or a medical condition (American Psychiatric Association 2013).
PTSD is common in both civilian and military populations. In 2005, the prevalence of PTSD among the general population of the USA was estimated to be 6.8 % (Kessler et al. 2005). The disease is even more prevalent in military veterans, with estimated prevalence rates ranging from 19 % in 2006 for American Vietnam veterans (Dohrenwend et al. 2006) to 22 % in 2009 for US veterans of the Iraqi and/or Afghani theaters (Seal et al. 2009). In addition to the direct costs of treatment for PTSD, the associations of lost productivity, reduced quality of life, and increased incidence of domestic violence, homelessness, suicide, and family strain make PTSD a burdensome disease to both the individuals affected and society (McCrone and Cawkill 2003).
PTSD was first added to the DSM in the manual’s third edition and has conventionally been classified as a psychiatric disorder. However, since its addition to the DSM in 1980, numerous studies have found correlations between PTSD diagnosis and/or severity and medical diseases in other organ systems, including arthritis, asthma, and myocardial infarction (Weisberg et al. 2002; Spitzer et al. 2009).
Systems Involved in PTSD
The goal of this paper is to discuss evidence for systemic involvement in PTSD . To do this, we reviewed published studies and our own work focused on PTSD symptomatology, comorbidities, and associated diseases. By collecting and presenting evidence substantiating the argument that PTSD is more than just a psychiatric disorder, we hope to support the new and constructive viewpoint of PTSD as a systemic disorder that needs to be addressed on multiple fronts in order to improve research and treatment of this critical condition.
Neurological Involvement
Neuroanatomical abnormalities implicated in PTSD include reduced hippocampal volume (Bremner et al. 1995; Pitman and Rauch 2001; Vythilingam et al. 2002; Kitayama et al. 2005; Smith 2005; Karl et al. 2006; Shin 2006; Wang et al. 2010; Morey et al. 2012) and parahippocampal gyrus volume (Meng et al. 2014), reduced amygdalar volume (Karl et al. 2006; Morey et al. 2012; Meng et al. 2014), increased amygdalar response (Pitman and Rauch 2001; Shin 2006), reduced prefrontal cortex activation (Bremner et al. 1995; Sherin and Nemeroff 2011), reduced anterior cingulate cortex volume (Bremner et al. 1995; Karl et al. 2006; Meng et al. 2014), reduced corpus callosum volume (Karl et al. 2006), reduced left insula volume (Meng et al. 2014), and increased gray matter volume of the left insula (Meng et al. 2014) and superior temporal gyrus (De Bellis et al. 2002). Many of these neurobiological abnormalities provide plausible explanations for clinical features associated with PTSD such as altered learning and extinction as well as hyperarousal. However, for many of these abnormalities, it remains unclear whether they are preexisting conditions that predispose patients to developing PTSD or are changes acquired through traumatic stress and subsequent stress responses (Childress et al. 2013).
Reduced hippocampal volume is perhaps the most-studied and consistent neurological abnormality found in patients with PTSD (Childress et al. 2013). Volumetric reductions have been found in both hippocampal hemispheres in subjects with PTSD, either unilaterally [right hemisphere: (Bremner et al. 1995); left hemisphere: (Vythilingam et al. 2002; Morey et al. 2012)] or bilaterally (Pitman and Rauch 2001; Kitayama et al. 2005; Smith 2005; Karl et al. 2006; Wang et al. 2010). Karl et al. (2006) found that bilateral hippocampal volume in patients with PTSD was significantly smaller compared to trauma-exposed patients without PTSD and to nonexposed patients; however, this difference was only apparent when analyzing the hippocampal volumes of adult samples but not pediatric samples. The lack of hippocampal size abnormalities observed in pediatric subjects suggests that PTSD-related reduction in hippocampal volume does not occur or become evident until adulthood. Interestingly, the duration of PTSD was not significantly related to changes in hippocampal volume. This example of altered hippocampal volume in adults with PTSD but not in children with PTSD demonstrates the difficulty in establishing the pathological relation between PTSD and anatomical abnormalities (Table 1).
Endocrine Involvement
The role of the endocrine system in regulating stress response has led to much research focused on the involvement of this system in PTSD. Both the hypothalamic-pituitary-adrenal (HPA) axis and the hypothalamic-pituitary-thyroid (HPT) axis have been implicated in PTSD pathology (Table 2).
PTSD has been associated with dysregulation of the HPA axis hormones at both basal levels and with low-dose dexamethasone suppression testing (Yehuda 2006). Several studies have found that patients with PTSD have decreased cortisol levels in plasma samples and urine samples (Olff et al. 2006; Sherin and Nemeroff 2011; Wahbeh and Oken 2013), increased glucocorticoid receptor function (Yehuda et al. 1991; Yehuda 2006), and increased corticotropin releasing hormone (CRH) concentrations in cerebrospinal fluid (CSF) from one-time lumbar puncture samples and serial samples taken throughout a 24-h period (Baker et al. 1999, 2005).
In an unaltered HPA axis, CRH secreted from the hypothalamus binds to receptors on cells of the anterior pituitary, which in turn produce and secrete adrenocorticotropin from the anterior pituitary into the adrenal cortex. Glucocorticoids such as cortisol are then produced and secreted by the adrenal gland, thereby activating sympathetic nervous pathways and initiating negative feedback to the hypothalamus and anterior pituitary. The relation between PTSD and hypocortisolism suggests a disinhibition of the negative feedback to the hypothalamus and anterior pituitary, resulting in altered stress encoding and fear processing as well as sustained elevated levels of CRH (Kolber et al. 2008).
Prolonged exposure of the hippocampus to CRH is also associated with hippocampal neuronal degeneration (VanItallie 2002; Sherin and Nemeroff 2011). The hippocampus contains high concentrations of mineralocorticoid receptors and glucocorticoid receptors, which are thought to regulate basal-level HPA activity and mediate glucocorticoid negative feedback, respectively (McDonald et al. 2005; Smith and Vale 2006). Therefore, findings of an atrophic relation between elevated CRH exposure and hippocampal volume provide an explanation for this common neuroanatomical abnormality as well as evidence for the disinhibition of the negative feedback pathways of the HPA axis (Smith and Vale 2006).
Several studies have found a positive association between PTSD severity and a disproportionate increase of triiodothyronine (T3 and FT3) concentration relative to that of thyroxine (T4 and FT4), indicating elevation in the peripheral deiodination (Wang and Mason 1999; Sherin and Nemeroff 2011). PTSD has also been associated with a decrease in thyroid-stimulating hormone (thyrotropin) (Boscarino 2004; Olff et al. 2006).
Similar to the neurological involvement of PTSD, it is difficult to determine whether abnormalities in the endocrine system associated with PTSD are consequences of the body’s response to traumatic stress or preexisting conditions that increase susceptibility to the development of PTSD. Therefore, further investigation regarding the pathological role of endocrine involvement in PTSD is necessary in order to better understand the complex stress responses and their systemic consequences in patients with PTSD.
Psychiatric Involvement
Major psychiatric comorbidities of PTSD include anxiety and depressive disorders, particularly major depressive disorder (MDD) (Marshall 2001; David 2004; Cohen et al. 2009; Rytwinski et al. 2013) and substance abuse, such as alcohol abuse (AB) or alcohol dependency (AD) [AB/AD: (Cohen et al. 2009; Pietrzak et al. 2011; Debell et al. 2014)]; Opioid use (Meier et al. 2014); and, Cocaine use (Meier et al. 2014). PTSD has also been associated with increased suicidal ideation and behavior (Davidson et al. 1991; Marshall 2001; Sareen et al. 2007; Jakupcak et al. 2009; Nock et al. 2009; Gradus et al. 2010; Panagioti and Tarrier 2012), especially when comorbid with MDD (Jakupcak et al. 2009; Gradus et al. 2010; Panagioti and Tarrier 2012; Ramsawh et al. 2014), alcohol abuse or dependency (Rojas et al. 2014), or other substance abuse (Moylan et al. 2001; Table 3).
There are also associations between PTSD and increased prevalence of neuropsychiatric conditions, including dementia (Qureshi et al. 2010, 2011; Childress et al. 2013), both chronic and episodic migraines (Buse et al. 2013), attention deficit hyperactive disorder (Antshel et al. 2013), somatic pain symptoms (Andreski and Breslau 1998; Beckham et al. 1998; Sareen et al. 2007; Defrin et al. 2008; Moeller-Bertram and Strigo 2012), hypervigilance and insomnia (Pigeon 2013), heightened aggression (Taft et al. 2009), increased rates of smoking (Fu et al. 2007) and emotional eating (Talbot et al. 2013), and deficits in executive functioning (Qureshi et al. 2011; Polak et al. 2012; Flaks et al. 2014).
The large number of psychiatric comorbidities in PTSD is critical to address because they cause significant functional impairment to those affected by PTSD. Furthermore, patients with PTSD-associated affective disorders will often self-medicate with alcohol and other illicit substances, which can further contribute to the severity and complexity of their affective disorders and can produce additional neurological damage and dysfunction (Fig. 1). Therefore, proper screenings and treatments for comorbid psychiatric and behavioral disorders in patients with PTSD are crucial in order to maintain patients’ well-being and avoid further neuropsychiatric damage.

Potential positive-feedback mechanisms compounding neuropsychiatric impairment in patients with PTSD. PTSD-inducing stimuli may directly impair neurological function and may produce mood disorders. Patients may self-medicate their mood disorders with illicit drugs and alcohol, which causes a positive-feedback loop thereby producing further neurological damage. This, in turn, may further enhance the neurological impairment and mood disorders associated with PTSD. This model supports the need for comprehensive screenings for both physical (e.g., cardiovascular risk factors) and behavioral changes (e.g., alcohol and drug use) in patients with PTSD
Cardiovascular Involvement
Cardiovascular associations with PTSD include hypertension (Buckley and Kaloupek 2001; Norman et al. 2006; O’Toole and Catts 2008; Cohen et al. 2009; Qureshi et al. 2009; McFarlane 2010; Pietrzak et al. 2012; Paulus and Egge 2013), angina pectoris (Spitzer et al. 2009; Pietrzak et al. 2012), tachycardia (Gerardi et al. 1994; Buckley and Kaloupek 2001; Blechert et al. 2007; Pole 2007; Pietrzak et al. 2012; Paulus and Egge 2013), elevated heart rate (HR) and blood pressure in response to trauma-related cues (Shalev et al. 1992; Gerardi et al. 1994; Buckley and Kaloupek 2001; Barkay et al. 2012; Paulus and Egge 2013), peripheral arterial disease (Spitzer et al. 2009), atherosclerotic coronary artery disease (Ahmadi et al. 2011), heart failure (Spitzer et al. 2009; Pietrzak et al. 2012), myocardial infarction (Qureshi et al. 2009; Spitzer et al. 2009), and general cardiovascular disease (McFarlane and Rafalowicz 1994; Boscarino 1997; Schnurr and Paris 2000; David 2004; Sareen et al. 2007; Qureshi et al. 2009; Pietrzak et al. 2012).
One possible explanation for the cardiovascular abnormalities and damage associated with PTSD is increased sympathetic arousal (Bedi and Arora 2007) indicated by greater skin conductance (Shalev et al. 1992; Blechert et al. 2007; Pole 2007), elevated HR (Buckley and Kaloupek 2001; Pole 2007; Paulus and Egge 2013), low respiratory sinus arrhythmia (Blechert et al. 2007), and dysregulation of HPA axis hormones (VanItallie 2002; Bedi and Arora 2007). Because of the many interactions between the HPA axis and the sympathetic nervous system, the cardiovascular involvement of PTSD is likely to originate from a combination of both autonomic nervous system and HPA axis dysregulation (Bedi and Arora 2007; Dedert et al. 2010; Table 4).
Because of the greater cardiovascular involvement in PTSD than in controls, we tested the hypothesis that patients with PTSD would have a shorter life expectancy than control veterans. We compared controls to veterans with Purple Hearts (awarded for significant physical injury in battle) and to veterans with PTSD. The mortality rates in veterans over 65 years of age were greater for patients with PTSD than for controls (Kimbrell et al. 2011). Interestingly, veterans both with and without PTSD who had received a Purple Heart had a longer life expectancy.
Immunological Changes in PTSD
Considering the many changes found in the neuroendocrine system in PTSD and the significant impact of the neuroendocrine system on immune function (Bornstein and Rutkowski 2002; Boscarino 2004; Baker and O’connor 2012), significant PTSD-related immune abnormalities are plausible. In fact, autoimmune conditions associated with PTSD include rheumatoid arthritis (Weisberg et al. 2002; Boscarino 2004; Norman et al. 2006; O’Toole and Catts 2008; Qureshi et al. 2009; Pietrzak et al. 2012), anemia (Weisberg et al. 2002), autoimmune-related dermatological diseases [eczema: (Weisberg et al. 2002; Boscarino 2004; O’Toole and Catts 2008; Qureshi et al. 2009); psoriasis: (Boscarino 2004); chronic idiopathic urticaria: (Chung et al. 2010)], diabetes [type 1: (Weisberg et al. 2002; Boscarino 2004); type 2: (Boyko et al. 2010; Lukaschek et al. 2013; Vaccarino et al. 2014); and unspecified: (Weisberg et al. 2002; David 2004; Qureshi et al. 2009)] (Table 5).
Studies have also found correlations between PTSD and decreased natural killer cell cytotoxicity (Gotovac et al. 2010), elevated T-lymphocyte counts, increased immunoglobulin-M levels (Boscarino 2004), and greater C-reactive protein levels (Spitzer et al. 2010).
Musculoskeletal Involvement in PTSD
Poorer overall musculoskeletal condition is associated with PTSD (McFarlane and Rafalowicz 1994; Schnurr and Paris 2000; O’Toole and Catts 2008). Particular musculoskeletal disorders that have been associated with PTSD include fibromyalgia (Amir et al. 1997), osteoarthritis (David 2004), and temporomandibular disorder (Afari et al. 2008). The exact relationship between musculoskeletal diseases and PTSD is unclear, but these findings could be related to the association of PTSD with generalized somatic pain (Andreski and Breslau 1998; Defrin et al. 2008; Table 6).
Digestive and Genitourinary Involvement
PTSD has been associated with a higher prevalence of gastrointestinal disorders (Boscarino 1997; Schnurr and Paris 2000; Graham-Bermann and Seng 2005; Norman et al. 2006; Sareen et al. 2007), a relation that is common with anxiety disorders (Mayer et al. 2001). Digestive conditions with a greater prevalence in patients with PTSD include irritable bowel syndrome (Irwin et al. 1996), gastroesophageal reflux disease and subsequent dyspepsia (Li et al. 2011), hepatic disease (Spitzer et al. 2009; von Känel et al. 2010), renal diseases such as glomerulonephritis (Weisberg et al. 2002; Boscarino 2004), gastritis (Pietrzak et al. 2012), and ulcer development (Davidson et al. 1991; Weisberg et al. 2002; Qureshi et al. 2009; Pietrzak et al. 2012). PTSD has also been associated with several genitourinary diseases, including endometriosis (Seng et al. 2006; Qureshi et al. 2009) and cervical dysplasia (Seng et al. 2006; Qureshi et al. 2009; Table 7).
Respiratory Involvement
Respiratory issues have also been associated with PTSD (McFarlane and Rafalowicz 1994; Boscarino 1997; Blechert et al. 2007; Sareen et al. 2007), including shortness of breath (Baker et al. 1997), increased frequency of sighing (Blechert et al. 2007), and general pulmonary diseases (Weisberg et al. 2002; Spitzer et al. 2009) such as asthma (Davidson et al. 1991; Weisberg et al. 2002; Graham-Bermann and Seng 2005; O’Toole and Catts 2008; Qureshi et al. 2009; Spitzer et al. 2009) and bronchitis (Spitzer et al. 2009; Table 8).
Tumorigenic Involvement
A few studies have shown a significant association between PTSD and the prevalence of cancer (Norman et al. 2006; Sareen et al. 2007); however, the pathophysiological relation of the two conditions remains uncertain. It has been suggested that enhanced tumorigenesis in PTSD is caused by dysregulation of the sympathetic nervous system and HPA axis, as well as compromised cellular immunity (McDonald et al. 2005). The recent finding of an association between PTSD and DNA breakage supports the possible relationship between PTSD and tumorigenic pathways (Morath et al. 2014; Table 9).
Practice and Procedures
PTSD is very common and is associated with great morbidity and suffering. It is critical to understand more about the disease in order to design new, innovative therapies. It has become increasingly evident that PTSD is more than simply a psychological adjustment disorder, and this article offers the thesis that PTSD is, in fact, a systemic disorder. This article did not cover all of the systems affected by PTSD but gives a broad overview, upon which other articles will expand. Nonetheless, enough systems were discussed here to support the assertion that PTSD involves much more than just the brain. This, in turn, indicates that one may study other organ systems to gain great insights into the pathophysiological underpinnings of PTSD: investigations will no longer be limited to the brain or direct effects of neuroanatomical changes. Moreover, the systemic hypothesis also helps explain the many symptoms outside the brain from which PTSD patients suffer.
As a result of systemic involvement, we suggest that patients with PTSD undergo comprehensive screenings for associated disorders, particularly for cardiovascular diseases and dementias, in order to prevent or mitigate their effects. While this paper recommends broadening the scope of conventional screenings for patients with PTSD because of the systemic nature of PTSD, it remains critical to screen and treat for psychiatric diseases in light of the highly negative compounding effect of comorbid major depressive disorder as well as increases in high-risk behaviors, impulsivity, and suicide in patients with PTSD, whose substance abuse to self-medicate may further impair neurological function.
Key Facts About Systemic Involvement in PTSD
-
PTSD has conventionally been considered to be primarily a psychiatric illness; consequently, much of the PTSD-related research and treatments heretofore have focused on the psychiatric manifestations of PTSD.
-
Recent studies have associated PTSD with diseases in multiple other organ systems, thus supporting the thesis that PTSD is a systemic disorder.
-
Behavioral changes, particularly an increase in substance abuse and tobacco use, have been identified in many patients with PTSD. These behaviors can enhance neurological impairment associated with PTSD, for example, via producing stroke. These can add to the other disorders associated with PTSD, such as mood disorders, and can indirectly impact the systemic manifestations of PTSD (Fig. 1).
-
The role of PTSD in more complex pathologies (e.g., tumorigenic, gastric, and respiratory diseases) is also enhanced by PTSD-associated behavioral changes that are implicated in the pathology of these diseases, such as increased tobacco use and alcohol consumption (Fig. 2).
Fig. 2 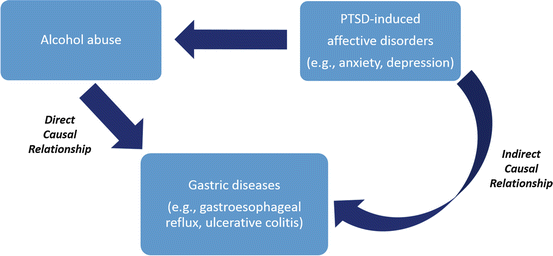
Potential PTSD-related pathological pathways leading to development of gastric diseases. Just as with the neuropsychiatric disorders noted in Fig. 1, PTSD may have both direct and indirect effects on other systemic organs. For example, PTSD-induced affective disorders may be associated with gastric diseases. But PTSD may also be associated with alcohol abuse, which further promotes the development of gastric disease. For many such systemic disorders, PTSD may act via several pathways, and it can be difficult to determine whether it has direct, indirect, or both effects when producing organ dysfunction
-
A major area of research needed in PTSD is determining whether findings in PTSD, such as abnormally small hippocampal volumes, are caused by PTSD or are preexisting conditions that are risk factors for the development of PTSD.

Summary Points
-
Studies have begun to explicate the specific neuroanatomical changes associated with PTSD that underlie certain neuropsychiatric symptoms and findings.
-
This article summarizes recent findings that support the thesis that PTSD produces systemic changes that extend far beyond the brain.
-
PTSD is associated with behavioral changes, including tobacco consumption, illicit drug use, and alcohol abuse, that can have additional deleterious effects on brain and body function.
-
This review supports the thesis that a broader perspective on the systemic symptomatology and pathophysiology of PTSD is appropriate in future studies and treatments.
-
The increased incidence of serious systemic disorders in PTSD suggests that clinicians should be vigilant in screening for many systemic disorders and unhealthy behaviors in PTSD patients, including risk factors for heart attacks and stroke, digestive diseases, dementia, and drug abuse.
-
Despite the advancement in our understanding of PTSD, further research is needed to elucidate the cause-and-effect relationship between PTSD and distinct physical abnormalities, such as whether small hippocampal volumes are a risk factor for PTSD or are caused by PTSD.
-
More research is needed to better understand whether treating PTSD-induced psychiatric symptoms leads to a change in behaviors that reduces downstream physiological effects, such as PTSD-induced anxiety, alcohol abuse, and gastric disease (Fig. 2).
Abbreviations
- AB:
-
Alcohol abuse
- AD:
-
Alcohol dependency
- CRH:
-
Corticotropin releasing hormone
- CSF:
-
Cerebrospinal fluid
- DNA:
-
Deoxyribonucleic acid
- DSM:
-
Diagnostic and statistical manual of mental disorders
- FT3:
-
Free triiodothyronine
- FT4:
-
Free thyroxine
- HPA:
-
Hypothalamic-pituitary-adrenal
- HPT:
-
Hypothalamic-pituitary-thyroid
- HR:
-
Heart rate
- MDD:
-
Major depressive disorder
- PTSD:
-
Post-traumatic stress disorder
- T3:
-
Protein-bound triiodothyronine
- T4:
-
Protein-bound thyroxine
References
Afari N, Wen Y, Buchwald D, Goldberg J, Plesh O. Are post-traumatic stress disorder symptoms and temporomandibular pain associated? Findings from a community-based twin registry. J Orofacial Pain. 2008;22:41–9.
Ahmadi N, Hajsadeghi F, Mirshkarlo HB, Budoff M, Yehuda R, Ebrahimi R. Post-traumatic stress disorder, coronary atherosclerosis, and mortality. Am J Cardiol. 2011;108:29–33.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Publishing; 2013.
Amir M, Kaplan Z, Neumann L, Sharabani R, Shani N, Buskila D. Posttraumatic stress disorder, tenderness and fibromyalgia. J Psychosom Res. 1997;42: 607–13.
Andreski P, Chilcoat H, Breslau N. Post-traumatic stress disorder and somatization symptoms: a prospective study. Psychiatry Res. 1998;79:131–8.
Antshel KM, Kaul P, Biederman J, Spencer TJ, Hier BO, Hendricks K, Faraone SV. Posttraumatic stress disorder in adult attention-deficit/hyperactivity disorder: clinical features and familial transmission. J Clin Psychiatry. 2013;74:e197–204.
Baker DG, West SA, Orth DN, Hill KK, Nicholson WE, Ekhator NN, Bruce AB, Wortman MD, Keck PE Jr., Geracioti TD Jr. Cerebrospinal fluid and plasma beta-endorphin in combat veterans with post-traumatic stress disorder. Psychoneuroendocrinology. 1997;22:517–29.
Baker DG, West SA, Nicholson WE, Ekhator NN, Kasckow JW, Hill KK, Bruce AB, Orth DN, Geracioti TD Jr. Serial CSF corticotropin-releasing hormone levels and adrenocortical activity in combat veterans with posttraumatic stress disorder. Am J Psychiatry. 1999;156:585–8.
Baker DG, Ekhator NN, Kasckow JW, Dashevsky B, Horn PS, Bednarik L, Geracioti TD Jr. Higher levels of basal serial CSF cortisol in combat veterans with posttraumatic stress disorder. Am J Psychiatry. 2005;162:992–4.
Baker DG, Nievergelt CM, O’connor DT. Biomarkers of PTSD: neuropeptides and immune signaling. Neuropharmacology. 2012;62:663–73.
Barkay G, Freedman N, Lester H, Louzoun Y, Sapoznikov D, Luckenbaugh D, Shalev AY, Chisin RG, Bonne O. Brain activation and heart rate during script-driven traumatic imagery in PTSD: preliminary findings. Psychiatry Res Neuroimaging. 2012;204:155–60.
Beckham JC, Moore SD, Feldman ME, Hertzberg MA, Kirby AC, Fairbank JA. Health status, somatization, and severity of posttraumatic stress disorder in Vietnam combat veterans with posttraumatic stress disorder. Am J Psychiatry. 1998;155:1565–9.
Bedi US, Arora R. Cardiovascular manifestations of posttraumatic stress disorder. J Natl Med Assoc. 2007;99:642–9.
Blechert J, Michael T, Grossman P, Lajtman M, Wilhelm FH. Autonomic and respiratory characteristics of posttraumatic stress disorder and panic disorder. Psychosom Med. 2007;69:935–43.
Bornstein SR, Rutkowski H. The adrenal hormone metabolism in the immune/inflammatory reaction. Endocrine Res. 2002;28:719–28.
Boscarino JA. Diseases among men 20 years after exposure to severe stress: implications for clinical research and medical care. Psychosom Med. 1997;59:605–14.
Boscarino JA. Posttraumatic stress disorder and physical illness: results from clinical and epidemiologic studies. Ann N Y Acad Sci. 2004;1032:141–53.
Boyko EJ, Jacobson IG, Smith B, Ryan MaK, Hooper TI, Amoroso PJ, Gackstetter GD, Barrett-Connor E, Smith TC. Risk of diabetes in U.S. Military service members in relation to combat deployment and mental health. Diabetes Care. 2010;33:1771–7.
Bremner JD, Randall P, Scott TM, Bronen RA, Seibyl JP, Southwick SM, Delaney RC, Mccarthy G, Charney DS, Innis RB. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry. 1995;152:973–81.
Buckley TC, Kaloupek DG. A meta-analytic examination of basal cardiovascular activity in posttraumatic stress disorder. Psychosom Med. 2001;63:585–94.
Buse DC, Silberstein SD, Manack AN, Papapetropoulos S, Lipton RB. Psychiatric comorbidities of episodic and chronic migraine. J Neurol. 2013;260:1960–9.
Childress JE, Mcdowell EJ, Dalai VV, Bogale SR, Ramamurthy C, Jawaid A, Kunik ME, Qureshi SU, Schulz PE. Hippocampal volumes in patients with chronic combat-related posttraumatic stress disorder: a systematic review. J Neuropsychiatry Clin Neurosci. 2013;25:12–25.
Chung MC, Symons C, Gilliam J, Kaminski ER. The relationship between posttraumatic stress disorder, psychiatric comorbidity, and personality traits among patients with chronic idiopathic urticaria. Compr Psychiatry. 2010;51:55–63.
Cohen BE, Marmar C, Ren L, Bertenthal D, Seal KH. Association of cardiovascular risk factors with mental health diagnoses in Iraq and Afghanistan war veterans using VA health care. JAMA. 2009;302:489–92.
David D. Comparison of comorbid physical illnesses among veterans with PTSD and veterans with alcohol dependence. Psychiatr Serv. 2004;55:82–5.
Davidson JRT, Hughes D, Blazer DG, George LK. Post-traumatic stress disorder in the community: an epidemiological study. Psychol Med. 1991;21:713–21.
De Bellis MD, Keshavan MS, Frustaci K, Shifflett H, Iyengar S, Beers SR, Hall J. Superior temporal gyrus volumes in maltreated children and adolescents with PTSD. Biol Psychiatry. 2002;51:544–52.
Debell F, Fear NT, Head M, Batt-Rawden S, Greenberg N, Wessely S, Goodwin L. A systematic review of the comorbidity between PTSD and alcohol misuse. Soc Psychiatry Psychiatr Epidemiol. 2014;49:1401–25.
Dedert EA, Calhoun PS, Watkins LL, Sherwood A, Beckham JC. Posttraumatic stress disorder, cardiovascular, and metabolic disease: a review of the evidence. Ann Behav Med. 2010;39:61–78.
Defrin R, Ginzburg K, Solomon Z, Polad E, Bloch M, Govezensky M, Schreiber S. Quantitative testing of pain perception in subjects with PTSD – implications for the mechanism of the coexistence between PTSD and chronic pain. Pain. 2008;138:450–9.
Dohrenwend BP, Turner JB, Turse NA, Adams BG, Koenen KC, Marshall R. The psychological risks of Vietnam for U.S. Veterans: a revisit with new data and methods. Science. 2006;313:979–82.
Flaks MK, Malta SM, Almeida PP, Bueno OFA, Pupo MC, Andreoli SB, Mello MF, Lacerda ALT, Mari JJ, Bressan RA. Attentional and executive functions are differentially affected by post-traumatic stress disorder and trauma. J Psychiatr Res. 2014;48:32–39.
Flaks MK, Malta SM, Almeida PP, Bueno OFA, Pupo MC, Andreoli SB, Mello MF, Lacerda ALT, Mari JJ, Bressan RA. Post-traumatic stress disorder and smoking: a systematic review. Nicotine Tob Res. 2007;9:1071–84.
Gerardi RJ, Keane TM, Cahoon BJ, Klauminzer GW. An in vivo assessment of physiological arousal in posttraumatic stress disorder. J Abnormal Psychol. 1994;103:825–7.
Gotovac K, Vidović A, Vukušić H, Krčmar T, Sabioncello A, Rabatić S, Dekaris D. Natural killer cell cytotoxicity and lymphocyte perforin expression in veterans with posttraumatic stress disorder. Prog Neuro-Psychopharmacol Biol Psychiatry. 2010;34:597–604.
Gradus JL, Qin P, Lincoln AK, Miller M, Lawler E, Sorensen HT, Lash TL. Posttraumatic stress disorder and completed suicide. Am J Epidemiol. 2010;171:721–7.
Graham-Bermann SA, Seng J. Violence exposure and traumatic stress symptoms as additional predictors of health problems in high-risk children. J Pediatr. 2005;146:349–54.
Irwin C, Falsetti SA, Lydiard RB, Ballenger JC, Brock CD, Brener W. Comorbidity of posttraumatic stress disorder and irritable bowel syndrome. J Clin Psychiatry. 1996;57:576–8.
Jakupcak M, Cook J, Imel Z, Fontana A, Rosenheck R, Mcfall M. Posttraumatic stress disorder as a risk factor for suicidal ideation in Iraq and Afghanistan war veterans. J Traum Stress. 2009;22:303–6.
Karl A, Schaefer M, Malta L, Dorfel D, Rohleder N, Werner A. A meta-analysis of structural brain abnormalities in PTSD. Neurosci Biobehav Rev. 2006;30:1004–31.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62:593–602.
Kimbrell T, Pyne JM, Kunik ME, Magruder KM, Petersen NJ, Yu HJ, Hudson TJ, Schulz PE, Qureshi SU. The impact of purple heart commendation and PTSD on mortality rates in older veterans. Depress Anxiety. 2011;28:1086–90.
Kitayama N, Vaccarino V, Kutner M, Weiss P, Bremner JD. Magnetic resonance imaging (MRI) measurement of hippocampal volume in posttraumatic stress disorder: a meta-analysis. J Affect Disord. 2005;88:79–86.
Kolber BJ, Roberts MS, Howell MP, Wozniak DF, Sands MS, Muglia LJ. Central amygdala glucocorticoid receptor action promotes fear-associated CRH activation and conditioning. Proc Natl Acad Sci. 2008;105:12004–9.
Li J, Brackbill RM, Stellman SD, Farfel MR, Miller-Archie SA, Friedman S, Walker DJ, Thorpe LE, Cone J. Gastroesophageal reflux symptoms and comorbid asthma and posttraumatic stress disorder following the 9/11 terrorist attacks on world trade center in New York City. Am J Gastroenterol. 2011;106:1933–41.
Lukaschek K, Baumert J, Kruse J, Emeny RT, Lacruz ME, Huth C, Thorand B, Holle R, Rathmann W, Meisinger C, Ladwig K-H. Relationship between posttraumatic stress disorder and type 2 diabetes in a population-based cross-sectional study with 2970 participants. J Psychosom Res. 2013;74:340–5.
Marshall RD. Comorbidity, impairment, and suicidality in subthreshold PTSD. Am J Psychiatry. 2001;158:1467–73.
Mayer EA, Craske M, Naliboff BD. Depression, anxiety, and the gastrointestinal system. J Clin Psychiatry. 2001;62(Suppl 8):28–36; discussion 37.
Mccrone P, Knapp M, Cawkill P. Posttraumatic stress disorder (PTSD) in the armed forces: health economic considerations. J Trauma Stress. 2003;16:519–22.
Mcdonald PG, Antoni MH, Lutgendorf SK, Cole SW, Dhabhar FS, Sephton SE, Stefanek M, Sood AK. A biobehavioral perspective of tumor biology. Discov Med. 2005;5:520–6.
Mcfarlane AC. The long-term costs of traumatic stress: Intertwined physical and psychological consequences. World Psychiatry. 2010;9:3–10.
Mcfarlane AC, Atchison M, Rafalowicz E, Papay P. Physical symptoms in post-traumatic stress disorder. J Psychosom Res. 1994;38:715–26.
Meier A, Lambert-Harris C, Mcgovern MP, Xie H, An M, Mcleman B. Co-occurring prescription opioid use problems and posttraumatic stress disorder symptom severity. Am J Drug Alcohol Abuse. 2014;40:304–11.
Meng Y, Qiu C, Zhu H, Lama S, Lui S, Gong Q, Zhang W. Anatomical deficits in adult posttraumatic stress disorder: a meta-analysis of voxel-based morphometry studies. Behav Brain Res. 2014; 270C:307–15.
Moeller-Bertram T, Keltner J, Strigo IA. Pain and post traumatic stress disorder – review of clinical and experimental evidence. Neuropharmacology. 2012;62:586–97.
Morath J, Moreno-Villanueva M, Hamuni G, Kolassa S, Ruf-Leuschner M, Schauer M, Elbert T, Bürkle A, Kolassa I-T. Effects of psychotherapy on DNA strand break accumulation originating from traumatic stress. Psychother Psychosom. 2014;83:289–97.
Morey RA, Gold AL, Labar KS, Beall SK, Brown VM, Haswell CC, Nasser JD, Wagner HR, Mccarthy G. Amygdala volume changes in posttraumatic stress disorder in a large case-controlled veterans group. Arch Gen Psychiatry. 2012;69.
Moylan PL, Jones HE, Haug NA, Kissin WB, Svikis DS. Clinical and psychosocial characteristics of substance-dependent pregnant women with and without PTSD. Addict Behav. 2001;26:469–74.
Nock MK, Hwang I, Sampson N, Kessler RC, Angermeyer M, Beautrais A, Borges G, Bromet E, Bruffaerts R, De Girolamo G, De Graaf R, Florescu S, Gureje O, Haro JM, Hu C, Huang Y, Karam EG, Kawakami N, Kovess V, Levinson D, Posada-Villa J, Sagar R, Tomov T, Viana MC, Williams DR. Cross-national analysis of the associations among mental disorders and suicidal behavior: findings from the who world mental health surveys. PLoS Med. 2009;6:e1000123.
Norman SB, Means-Christensen AJ, Craske MG, Sherbourne CD, Roy-Byrne PP, Stein MB. Associations between psychological trauma and physical illness in primary care. J Traum Stress. 2006;19:461–70.
O’toole BI, Catts SV. Trauma, PTSD, and physical health: an epidemiological study of Australian Vietnam veterans. J Psychosom Res. 2008;64:33–40.
Olff M, Güzelcan Y, De Vries G-J, Assies J, Gersons BPR. HPA- and HPT-axis alterations in chronic posttraumatic stress disorder. Psychoneuroendocrinology. 2006;31:1220–30.
Panagioti M, Gooding PA, Tarrier N. A meta-analysis of the association between posttraumatic stress disorder and suicidality: The role of comorbid depression. Compr Psychiatry. 2012;53:915–30.
Paulus EJ, Argo TR, Egge JA. The impact of posttraumatic stress disorder on blood pressure and heart rate in a veteran population. J Traum Stress. 2013;26:169–72.
Pietrzak RH, Goldstein RB, Southwick SM, Grant BF. Prevalence and axis I comorbidity of full and partial posttraumatic stress disorder in the United States: results from wave 2 of the national epidemiologic survey on alcohol and related conditions. J Anxiety Disord. 2011;25:456–65.
Pietrzak RH, Goldstein RB, Southwick SM, Grant BF. Physical health conditions associated with posttraumatic stress disorder in U.S. Older adults: results from wave 2 of the national epidemiologic survey on alcohol and related conditions. J Am Geriatr Soc. 2012;60:296–303.
Pigeon WR. Longitudinal relationships of insomnia, nightmares, and PTSD severity in recent combat veterans. J Psychosom Res. 2013;75:546–50.
Pitman RK, Shin LM, Rauch SL. Investigating the pathogenesis of posttraumatic stress disorder with neuroimaging. J Clin Psychiatry. 2001;62(Suppl 17):47–54.
Polak AR, Witteveen AB, Reitsma JB, Olff M. The role of executive function in posttraumatic stress disorder: a systematic review. J Affect Disord. 2012;141:11–21.
Pole N. The psychophysiology of posttraumatic stress disorder: a meta-analysis. Psychol Bull. 2007;133:725–46.
Qureshi SU, Pyne JM, Magruder KM, Schulz PE, Kunik ME. The link between post-traumatic stress disorder and physical comorbidities: a systematic review. Psychiatr Q. 2009;80:87–97.
Qureshi SU, Kimbrell T, Pyne JM, Magruder KM, Hudson TJ, Petersen NJ, Yu HJ, Schulz PE, Kunik ME. Greater prevalence and incidence of dementia in older veterans with posttraumatic stress disorder. J Am Geriatr Soc. 2010;58:1627–33.
Qureshi SU, Long ME, Bradshaw MR, Pyne JM, Magruder KM, Kimbrell T, Hudson TJ, Jawaid A, Schulz PE, Kunik ME. Does PTSD impair cognition beyond the effect of trauma? J Neuropsychiatry Clin Neurosci. 2011;23:16–28.
Ramsawh HJ, Fullerton CS, Mash HBH, Ng THH, Kessler RC, Stein MB, Ursano RJ. Risk for suicidal behaviors associated with PTSD, depression, and their comorbidity in the U.S. Army. J Affect Disord. 2014;161:116–22.
Rojas SM, Bujarski S, Babson KA, Dutton CE, Feldner MT. Understanding PTSD comorbidity and suicidal behavior: associations among histories of alcohol dependence, major depressive disorder, and suicidal ideation and attempts. J Anxiety Disord. 2014;28:318–25.
Rytwinski NK, Scur MD, Feeny NC, Youngstrom EA. The co-occurrence of major depressive disorder among individuals with posttraumatic stress disorder: a meta-analysis. J Traum Stress. 2013;26:299–309.
Sareen J, Cox BJ, Stein MB, Afifi TO, Fleet C, Asmundson GJG. Physical and mental comorbidity, disability, and suicidal behavior associated with posttraumatic stress disorder in a large community sample. Psychosom Med. 2007;69:242–8.
Schnurr PP, Spiro A, Paris AH. Physician-diagnosed medical disorders in relation to PTSD symptoms in older male military veterans. Health Psychol. 2000;19:91–7.
Seal KH, Metzler TJ, Gima KS, Bertenthal D, Maguen S, Marmar CR. Trends and risk factors for mental health diagnoses among Iraq and Afghanistan veterans using department of veterans affairs health care, 2002–2008. Am J Public Health. 2009;99:1651–8.
Seng JS, Clark MK, Mccarthy AM, Ronis DL. PTSD and physical comorbidity among women receiving medicaid: results from service-use data. J Trauma Stress. 2006;19: 45–56.
Shalev AY, Orr SP, Peri T, Schreiber S, Pitman RK. Physiologic responses to loud tones in Israeli patients with posttraumatic stress disorder. Arch Gen Psychiatry. 1992;49:870–5.
Sherin JE, Nemeroff CB. Post-traumatic stress disorder: the neurobiological impact of psychological trauma. Dialogues Clin Neurosci. 2011;13:263–78.
Shin LM. Amygdala, medial prefrontal cortex, and hippocampal function in PTSD. Ann NY Acad Sci. 2006;1071:67–79.
Smith ME. Bilateral hippocampal volume reduction in adults with post-traumatic stress disorder: a meta-analysis of structural MRI studies. Hippocampus. 2005;15:798–807.
Smith SM, Vale WW. The role of the hypothalamic-pituitary-adrenal axis in neuroendocrine responses to stress. Dialogues Clin Neurosci. 2006;8:383–95.
Spitzer C, Barnow S, Völzke H, John U, Freyberger HJ, Grabe HJ. Trauma, posttraumatic stress disorder, and physical illness: findings from the general population. Psychosom Med. 2009;71:1012–7.
Spitzer C, Barnow S, Völzke H, Wallaschofski H, John U, Freyberger HJ, Löwe B, Grabe HJ. Association of posttraumatic stress disorder with low-grade elevation of C-reactive protein: evidence from the general population. J Psychiatr Res. 2010;44:15–21.
Taft CT, Weatherill RP, Woodward HE, Pinto LA, Watkins LE, Miller MW, Dekel R. Intimate partner and general aggression perpetration among combat veterans presenting to a posttraumatic stress disorder clinic. Am J Orthopsychiatry. 2009;79:461–8.
Talbot LS, Maguen S, Epel ES, Metzler TJ, Neylan TC. Posttraumatic stress disorder is associated with emotional eating. J Traum Stress. 2013;26:521–5.
Vaccarino V, Goldberg J, Magruder KM, Forsberg CW, Friedman MJ, Litz BT, Heagerty PJ, Huang GD, Gleason TC, Smith NL. Posttraumatic stress disorder and incidence of type-2 diabetes: a prospective twin study. J Psychiatr Res. 2014;56:158–64.
Vanitallie TB. Stress: a risk factor for serious illness. Metabolism. 2002;51:40–5.
Von Känel R, Abbas CC, Begré S, Gander M-L, Saner H, Schmid J-P. Association between posttraumatic stress disorder following myocardial infarction and liver enzyme levels: a prospective study. Digestive Dis Sci. 2010;55:2614–23.
Vythilingam M, Heim C, Newport J, Miller AH, Anderson E, Bronen R, Brummer M, Staib L, Vermetten E, Charney DS, Nemeroff CB, Bremner JD. Childhood trauma associated with smaller hippocampal volume in women with major depression. Am J Psychiatry. 2002;159:2072–80.
Wahbeh H, Oken BS. Salivary cortisol lower in posttraumatic stress disorder. J Traum Stress. 2013;26:241–8.
Wang S, Mason J. Elevations of serum T3 levels and their association with symptoms in world war II veterans with combat-related posttraumatic stress disorder: replication of findings in Vietnam combat veterans. Psychosom Med. 1999;61:131–8.
Wang H-H, Zhang Z-J, Tan Q-R, Yin H, Chen Y-C, Wang H-N, Zhang R-G, Wang Z-Z, Guo L, Tang L-H, Li L-J. Psychopathological, biological, and neuroimaging characterization of posttraumatic stress disorder in survivors of a severe coalmining disaster in China. J Psychiatr Res. 2010;44:385–92.
Weisberg RB, Bruce SE, Machan JT, Kessler RC, Culpepper L, Keller MB. Nonpsychiatric illness among primary care patients with trauma histories and posttraumatic stress disorder. Psychiatr Serv (Washington, D.C.). 2002;53:848–54.
Yehuda R, Lowy MT, Southwick SM, Shaffer D, Giller EL Jr. Lymphocyte glucocorticoid receptor number in posttraumatic stress disorder. Am J Psychiatry. 1991;148:499–504.
Yehuda R. Advances in understanding neuroendocrine alterations in PTSD and their therapeutic implications. Ann N Y Acad Sci. 2006;1071:137–66.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this entry
Cite this entry
Bukhbinder, A., Schulz, P.E. (2016). Evidence for PTSD as a Systemic Disorder. In: Martin, C., Preedy, V., Patel, V. (eds) Comprehensive Guide to Post-Traumatic Stress Disorders. Springer, Cham. https://doi.org/10.1007/978-3-319-08359-9_106
Download citation
DOI: https://doi.org/10.1007/978-3-319-08359-9_106
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-08358-2
Online ISBN: 978-3-319-08359-9
eBook Packages: Behavioral Science and PsychologyReference Module Humanities and Social SciencesReference Module Business, Economics and Social Sciences