
Abstract
Clinically, ultrasound (US) has been used as a cheap, quick, and effective form of imaging that provides information useful for diagnostic purposes. With the advent of microbubbles as US contrast agents, this simple imaging technique has evolved into a tool capable of providing molecularly targeted visualization of disease and controlled delivery of therapeutics. The simple, yet robust, structure of the microbubble allows for both internal and external modifications, which lead to a wide variety of clinical uses. This chapter will introduce the reader to microbubble fabrication, stabilization, drug loading, and targeting. The reader will also be briefly exposed to specific examples of current work done using microbubbles in areas of cancer treatment and protein/gene therapies. The work reviewed here is only a small fraction of the literature available on the subject matter and serves as an introduction to microbubbles as contrast agents, drug delivery vehicles, and theranostic particles.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Ultrasound (US) is among the most commonly used imaging modalities in the clinic. In ultrasound imaging, high-frequency (>20-kHz) sound waves are emitted through the skin. Portions of these waves are reflected back towards the transducer when they encounter tissues, and these reflected waves are computed to generate images based on sound attenuation, backscatter, and sound speed (Massoud and Gambhir 2003). Imaging contrast can be greatly improved (Blomley et al. 2001) through the addition of agents with acoustic properties different from surrounding tissues. Among the most commonly used US contrast agents are gas-filled microbubbles.
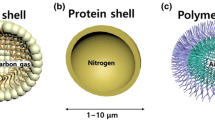
Microbubbles are gas-filled spheres with a shell that can be composed of phospholipids, polymers, or a variety of other substances (Janib et al. 2010; Unger et al. 2004). When exposed to US, these microbubbles undergo alternating contraction and expansion, a process known as cavitation, due to compressibility of encapsulated gas when subjected to acoustic pressure (Phillips and Gardner 2004; Cosgrove 2004; Stride and Saffari 2003). These vibrations cause the microbubbles to return a greater amount of US signal to the transducer, as compared to the practically incompressible surrounding tissues. This difference in signal return accounts for the majority of contrast provided by microbubbles in conventional grayscale ultrasound imaging (Cosgrove 2006). Although there are many other methods of obtaining contrast using microbubbles [Doppler (Harvey et al. 2001) and contrast specific imaging (Phillips and Gardner 2004) among others], the physics underlying these methods are beyond the scope of this chapter.
Currently the only FDA-approved use of microbubble ultrasound contrast agents is for left ventricle opacification. The albumin shelled microbubble, Albunex, was first approved in 1994. Subsequently, only two commercial microbubbles remain in clinical use: Optison™ (GE Medical Diagnostics, Princeton, NJ) and Definity® (Lantheus Medical Imaging, Billerica, NJ), which were FDA-approved in 1997 and 2001, respectively (Castle et al. 2013). While microbubbles have only been used as ultrasound contrast agents in the clinic, a significant amount of work has been devoted to demonstrating the potential role of microbubbles as a complete theranostic tool. Theranostics, or the combination of imaging and therapy, has gained increasing amounts of attention because of its proposed goal of allowing clinicians to diagnose and treat in real time with a single agent. The purpose of this chapter is to highlight strategies and uses of microbubbles in the application of theranostic cancer therapy. After a brief overview of microbubble fabrication and properties affecting their stability, the concept of microbubble use for theranostics is further developed with discussion of their potential for multi-modal imaging. In the remainder of the chapter, techniques for incorporation of drugs, genes, and proteins, and factors that affect success of these payload types are presented from key literature. The work presented here is by no means all-inclusive but merely attempts to introduce these key concepts. We also examine targeting strategies and their use in improving efficiency of microbubble accumulation at the tumor site. Finally, the chapter summarizes future work required to bring theranostic microbubble platforms to the clinic.
2 Microbubbles: Basic Fabrication Methods
Microbubbles can be made in a variety of ways, with the two most common methods being mechanical agitation (Fang et al. 2007; Klibanov 1999) and microfluidic flow focusing (Hashimoto et al. 2008; Ganan-Calvo and Gordillo 2001; Hettiarachchi et al. 2007). In mechanical agitation, a tip sonicator or vial shaker is used to violently mix the solution containing the shell components with a headspace of gas in order to create a microbubble emulsion. Microfluidic flow focusing uses micron sized flow channels in order to mitigate flow of immiscible fluids to emulsify one phase into another immiscible phase. In the context of microbubbles, the gas phase (microbubble core) flows into the liquid phase containing shell components (lipids, polymers, etc.). These two phases are then focused at a small opening called the orifice and pinch off to form gas-filled microbubbles (Hashimoto et al. 2008). Figure 12.1 shows a general overview of these two techniques.

Fabrication methods of microbubbles. (a) The microbubble starting materials (shell materials and gas) are flowed through a microfluidic device designed to focus the two immiscible phases at an orifice. The two colliding flows then pinch off and form microbubbles. (b) The shell materials are placed into a vial with a gas headspace. Then, using mechanical agitation (shaking or sonicating), the two phases are forced to partition into gas-cored microbubbles
There are many things to consider when choosing which method of microbubble fabrication to use. The sonication technique can produce a large number of microbubbles within minutes; however, some issues may arise from resulting broad distributions of size and shell thickness (Xu et al. 2012; Lee and Lee 2010; Parhizkar et al. 2013). In contrast, microfluidic flow focusing methods yield uniform size distributions; yet different shell thicknesses and bubble sizes can still be created by modifying fabrication parameters such as flow rates or device geometries (Lee and Lee 2010; Parhizkar et al. 2013; Gunduz et al. 2012). The narrow microbubble size distributions from flow focusing have been shown to improve echogenicity (Talu et al. 2007). However, a major drawback of microfluidic-driven microbubble production is the difficulty to mass-produce these bubble populations. To address these concerns, there has been a growing literature of new methods for mass production of bubbles that include increasing microbubble production speed (Castro-Hernandez et al. 2011) and running multiple devices in parallel on a single chip (Nisisako and Torii 2008; Romanowsky et al. 2012; Kendall et al. 2012).
3 Microbubble Stabilization
The visualization of blood flow in left ventricle opacification is a relatively brief imaging technique and does not require long-term microbubble stability for systemic circulation. However, with the expanding number of applications for which microbubbles are being explored, long-term stability of these contrast agents has become increasingly important. This section focuses on microbubble stability against gas dissolution, coalescence, and under ultrasound.
Microbubble instability arises from a variety of physical properties. Microbubble emulsions are thermodynamically unstable and have a tendency to minimize free energy of the system by separating gas and liquid into two bulk phases. This energy minimization leads to coalescence in which microbubbles aggregate together. These patches of gathered microbubbles eventually undergo Ostwald ripening and fuse into larger microbubbles, continuing this process until gas and liquid phases are completely separated (Kwan and Borden 2012). Another form of instability is gas dissolution which occurs due to the difference between gas partial pressures within and surrounding the microbubble. This difference causes an efflux of the gas core into the surroundings, which leads to microbubble shrinkage and ultimately, dissolution (Sarkar et al. 2009; Kwan and Borden 2010). Other mechanisms for microbubble instability have been explored, including microbubble shell collapse. However, a complete discussion of microbubble collapse dynamics is beyond the scope of this chapter and has been covered in detail elsewhere by Kwan and Borden (2012).
Although microbubble dissolution cannot be completely prevented, the literature reports many techniques proposed to slow down the diffusional process. Gases with low aqueous solubility, such as perfluorocarbons, have been used as microbubble cores to decrease gas dissolution (Cui et al. 2005) and different microbubble shell compositions have been explored in an effort to increase structural integrity (Paradossi et al. 2003; Ferrara et al. 2007; Duncanson et al. 2010). Additionally, researchers have added PEG to the microbubble shell to prevent aggregation and subsequent Ostwald ripening (Duncanson et al. 2010; Park et al. 2012). By using polymer-based shell compositions, increased shelf life, suspension stability, and stability under ultrasound have been obtained. However, these microbubbles exhibit decreased echogenicity and nonlinearity when compared with soft, lipid shelled microbubbles (Sciallero and Trucco 2013).
A relatively new concept of microbubble formulation has been explored in which a lipid-shelled microbubble is made using polymerizable diacetylene lipids. Park et al. (2012) showed that by varying the amount of this polymerizable lipid, microbubble stability could be tuned. Figure 12.2 shows that the 25 % polymerizable lipid shell condition provided increased stability against microbubble dissolution (Fig. 12.2a) as well as increased stability under ultrasound (Fig. 12.2b) when compared with lower polymerizable lipid shell concentrations and commercially available microbubbles, Vevo MicroMarker (VMM).

(a) Normalized number of microbubbles remained with time. The stability against gas dissolution of the different shell materials is informed: (diamond) 25 % DA; (circle) 15 % DA; (triangle) non-polymerizable lipids; (square) VMM. (b) Ultrasound image intensity (at 7.5 MHz) vs. time for a variety of microbubble shell materials: (diamond) 25 % DA; (circle) 15 % DA; (triangle) nonpolymerizable lipids; (square) Vevo MicroMarker (VMM). The intensity in the ROI was normalized by the initial intensity and then converted to dB. The vertical lines represent standard error [adapted with permission from Park et al. 2012). Copyright (2012) American Chemical Society]
4 Theranostics
The advances made in improving microbubble stability have expanded the potential applications of microbubbles to include triggered delivery of a therapeutic payload. Many researchers envision the use of microbubbles as a theranostic particle that both provides targeted image contrast to aid in diagnostic procedures and carries a therapeutic agent to the intended target. Ideally, such theranostic particles would be injected systemically and accumulate at the desired target through use of specific targeting moieties, such as antibodies. Once at the intended target, a clinician could image and identify the location of the target using clinical US. Finally, US of a frequency specific to the microbubble, distinct from the frequency used for imaging, can be applied to burst the microbubble and release the payload. Figure 12.3 gives a simplistic overview of this concept, which remains the ultimate goal of the field.

(a) Drug-loaded, targeted microbubbles are injected into the bloodstream and only attach to diseased tissues that exhibit specific targets. (b) Using a low powered ultrasound, this diseased area is located via ultrasound for diagnostic purposes and then (c) switching to a higher powered ultrasound, the bubbles in the specified area will burst and locally deliver therapeutic agents to the diseased tissue
Some early studies have shown microbubbles as a promising platform to develop this theranostic concept. Leong-Poi et al. used microbubbles loaded with plasmid DNA encoded for VEGF to induce formation of microvessels in hind limbs of rats, which in turn increased microvascular blood flow (Leong-Poi et al. 2007). Although these particular microbubbles were not used for imaging in the rats, but merely as DNA delivery vehicles, it could be reasoned that acoustic contrast enhancement of these particles would be ideal for visualization of increased microvascular blood flow (Kiessling et al. 2012). Rapoport et al. used doxorubicin-loaded nanobubbles which collected at tumor sites and coalesced into microbubbles. These in vivo-formed microbubbles were then imaged using US and destroyed to release the drug, which led to tumor growth inhibition (Rapoport et al. 2007). Although these studies and others show potential of microbubbles as theranostic tools, the field is still relatively young, and much more work is needed before true clinical translation can be achieved. While the role of microbubbles in ultrasound contrasting has already been elucidated, combinations of microbubbles with other contrasting agents allow for a more complete diagnostic tool. In the following section we review further enhancements to the imaging aspect of theranostics. Beginning from Sect. 5, we will discuss current efforts in the literature that address drug delivery aspects of theranostic function.
4.1 Combined Imaging Modalities to Enhance Diagnostic Imaging
While US is the primary mechanism for both imaging and triggering therapeutic release, others have further developed these particles to provide greater diagnostic practicality by combining them with other imaging modalities. For example, there have been microbubbles developed that are infused with contrast agents for magnetic resonance imaging (MRI) to provide a theranostic agent with both imaging capabilities. MRI is a non-invasive and widely clinically used technique that provides excellent soft tissue contrast with high morphological and spatial resolution. Superparamagnetic iron oxide nanoparticles (SPIONs) alter transverse (T2) relaxation times of water protons, providing dark negative signal intensity in images that can be used to visualize tumors (Lee et al. 2006). Additionally, SPIONs are non-toxic, biodegradable, and have a wide degree of versatility in biomedical applications. Current research of SPION applications includes drug delivery, bio-sensing, and molecular targeting (Laurent et al. 2008). By combining SPIONS with microbubbles, clinicians can optimize use of two imaging modalities through only one injectable contrasting agent. Using polymer-coated microbubbles, SPIONs can be incorporated into the shell of ultrasound contrast agents during synthesis steps and released upon microbubble rupture. Using a double emulsion solvent evaporation interfacial deposition (water-in-oil-in-water emulsion) process, SPIONs can be incorporated into an internal shell layer of polymer and then further encapsulated within a second shell layer all while maintaining a gas core (Yang et al. 2009). Incorporation of SPIONs into the inner shell increased MRI relaxation time as SPION concentration increased but reached a maximum in ultrasound contrast, after which additional SPIONs reduced the response of the microbubble. Thus, there exists a trade-off between MRI and ultrasound signals that must be optimized for an effective contrast agent. Using a similar oil-in-water emulsion technique, Liu et al. (2011) demonstrated significant image contrast observed in vascularized areas of a myxoid liposarcoma (MLS) ovarian carcinoma in rats upon i.v. injection of their hybrid contrast agent. Additionally, this study demonstrated a significant increase in longitudinal and transversal relaxivities after US-induced bubble destruction, which demonstrated triggerable MR imaging properties.
While MRI/US contrast combination continues to be evaluated as a future clinical technique, microbubbles are also being investigated in combination with other imaging modalities. Specifically, photoacoustic imaging can be coupled with ultrasound to provide enhanced spatial and temporal resolution (Xu and Wang 2006). Photoacoustic imaging uses nonionizing waves, such as short laser or radio-frequency pulses, of electromagnetic energy to excite ultrasound waves in biological tissues. A promising biomedical application lies in the detection of breast cancer by near-infrared light or radio-frequency–wave-induced photoacoustic imaging, which has important potential for early detection (Pramanik et al. 2008). Dove et al. demonstrated that binding of avidin-conjugated gold nanoparticles to a biotinylated microbubble shell provided stoichiometric control over nanoparticle surface density and optical absorption, while still retaining essential acoustic properties of the microbubble. Furthermore, the acoustic efficiency was 8.9-fold higher for microbubbles with conjugated nanoparticles than for nanoparticles alone, suggesting a potential for beneficial coupling between microbubbles and nanoparticles for enhanced photoacoustic response (Dove et al. 2013).
5 Microbubbles as a Therapeutic Delivery Device
To achieve a fully integrated theranostic particle, various techniques are employed to specifically tailor microbubble properties for payload incorporation and release. Microbubbles with a therapeutic payload have been used for a number of therapeutic strategies including delivering drugs across the blood–brain barrier (Hynynen et al. 2001; Mesiwala et al. 2002; Mesiwala and Mourad 2002), gene delivery (Martinez et al. 2002; Urban-Klein et al. 2005; Kinoshita and Hynynen 2005; Carson et al. 2012; Li et al. 2009), and targeted drug delivery (Willmann et al. 2008; Borden et al. 2008; Pochon et al. 2010; Tardy et al. 2010). As shown in Fig. 12.4, the methods to incorporate drugs into a microbubble can vary depending on the properties of the therapeutic payload.

Different ways that drugs can be incorporated into a microbubble. The drugs can be attached to the outer shell of the bubble (a), incorporated into the bubble’s shell (b), bound noncovalently to the surface of the microbubbles (c), and entrapped within the microbubbles (d), or hydrophobic drugs can be incorporated into a layer of oil within the microbubble (e). Reprinted with permission from Elsevier (Unger et al. 2001, 2004)
Therapeutic agents can be attached to the outer shell of the microbubble either as a free drug bound to the surface or within another carrying vehicle (micelles or liposomes) that is in turn bound to the microbubble (Fig. 12.4a) (Lentacker et al. 2007). Hydrophobic drugs, such as paclitaxel and doxorubicin, can also be incorporated into the shell layer of the microbubble (Fig. 12.4b) (Cochran et al. 2011; Tinkov et al. 2010a; Kang et al. 2010). For gene therapy applications, genetic material can potentially be electrostatically bound to the microbubble surface using shell components that give an overall positive shell charge (Fig. 12.4c) (Chen et al. 2006). Therapeutic agents can also be encapsulated directly within the microbubble itself (Fig. 12.4d). For lipophilic drugs that require a larger payload than microbubble surface binding can provide, an additional oil layer can be introduced within the microbubble between the gas core and bubble shell (Fig. 12.4e) (Fang et al. 2007; Lentacker et al. 2010; Shortencarier et al. 2004). Due to numerous drug loading options and manipulations of the microbubble itself, there has been much work done in exploring possible clinical uses for these drug-loaded microbubbles. The following sections will discuss current literature in regard to payload categories of small molecule drugs, gene delivery, or protein therapeutics and application of these loading techniques.
5.1 Drug Therapies
Microbubbles have been explored as potential drug carriers for numerous oncological drugs including doxorubicin, paclitaxel, and docetaxel (Cochran et al. 2011; Tinkov et al. 2010a; Kang et al. 2010). The allure of using these microbubbles is due in part to their ability to facilitate reduction of in vivo toxicity (Unger et al. 1998), potential for targeted drug delivery, and combination of therapy and imaging in a single platform. Additionally, triggered release of the microbubble payload can potentially ensure that chemotherapeutic agents are only released at the tumor site, thereby reducing systemic effects.
5.2 Drug Loading
Depending on drug characteristics (size, hydrophobicity, charge) and microbubble properties, one method of incorporation into the microbubble may be more suitable than others. Although hydrophobic drugs can be incorporated directly to microbubble shells through hydrophobic interactions, there are many instances in which this method alone does not provide the necessary effective payload. Unger et al. (1998) circumvented this problem by solubilizing paclitaxel into soybean oil and by using the drug-loaded oil as a medial layer between the gas core of the microbubble and the lipid shell. Hettiarachchi et al. (2009) used a double emulsion microfluidic device design to create a gas-in-oil-in-water microbubble with paclitaxel dissolved in the oil phase. Each of these methods increased the payload of drug per microbubble, allowing for release of a more effective dose from the microbubble.
Hydrophilic drugs are less amenable to such methods of loading, as they generally prefer to leave hydrophobic spaces and solubilize into the surrounding water-based solution. Various approaches have been used to encapsulate the hydrophilic drug, doxorubicin. One common technique is through tethering of smaller drug carrying particles to the microbubble instead of through hydrophobic interaction between the drug and microbubble shell, as with hydrophobic drugs. Lentacker et al. loaded doxorubicin into aqueous cores of liposomes. Then, by using an avidin–biotin linkage, they tethered these drug loaded liposomes onto gas-filled microbubbles (Lentacker et al. 2010). Geers et al. (2011) performed a similar experiment, but tethered doxorubicin-loaded liposomes to microbubbles using a thiol–maleimide linkage. Once microbubbles are ruptured, these drug-loaded liposomes are released, and the drug payload is released either by diffusion or through being endocytosed by target cells. Other research has attempted fabricating microbubbles in high concentrations of drug solution to load the microbubble through use of a concentration gradient. Villa et al. (2013) used a polyvinyl alcohol (PVA) shelled microbubble with a chitosan brush coating to load doxorubicin by dialyzing microbubbles in the presence of high concentration. Once microbubbles were removed from the drug solution, the chitosan brush acted as a physical barrier to diffusion, slowing down drug leakage from the microbubble. Fabiilli et al. dissolved drugs into water and created a water-in-gas emulsion by mixing drug-doped water with gas. This gas was then used to form the core of a microbubble, creating an acoustically active microbubble, with drug loaded into the gas core of the microbubble (Fabiilli et al. 2010).
Other properties, such as charge, have also been used to incorporate drugs into microbubbles. Tinkov et al. (2010b) used anionic phospholipids to form microbubbles and electrostatically bound doxorubicin, which has a positive charge in physiological conditions, to the surface of the microbubbles. With the wide variety of possible characteristics to manipulate for drug incorporation, microbubbles offer a versatile palette for incorporation and delivery of drugs.
5.2.1 US-Triggered Anti-cancer Drug Delivery
Most anti-cancer drug delivery techniques use US to trigger drug release through microbubble collapse. Cochran et al. used scanning electron microscopy to compare the morphology of drug containing polymer-shelled microbubbles after fabrication (Fig. 12.5a) to the morphology after ultrasound destruction (Fig. 12.5b). The change in morphology confirmed microbubble destruction due to ultrasound. They also found that with destruction of these drug-loaded microbubbles, there was an increase in the amount of drug released (Fig. 12.5c) (Cochran et al. 2011).

Scanning electron images of drug loaded microbubbles before (a) and after (b) ultrasound exposure. (c) The graph shows that the insonated drug-loaded microbubbles [diamond] released more drugs than non-insonated microbubbles [cross] (*p < 0.0374). Reprinted with permission from Elsevier (Cochran et al. 2011)
Additionally, US sonoporation increases effectiveness of the chemotherapy agent by increasing drug accumulation in nearby cells. Lin et al. showed that by adding microbubbles with focused ultrasound and freely dissolved drug, the ability of doxorubicin to reduce tumors in mice was enhanced. With doxorubicin alone, tumor size was consistently larger than when treated in conjunction with microbubbles and ultrasound (Fig. 12.6a). They found that addition of US and microbubbles led to nearly a tenfold more effective treatment over free drug alone. This indicated that the combination of ultrasound and microbubble significantly increased the amount of drug that accumulated in tumor tissues (Lin et al. 2012). Using drugs that were actually attached to the microbubble itself, Yan et al. showed that using PTX-liposome–microbubble complexes (PLMC) for breast tumor treatment reduced tumor sizes in mice. When using just PLMC, the tumor was able to grow to 872.46 ± 125.82 mm3. However, addition of ultrasound reduced final tumor size to only 360.01 ± 131.24 mm3 in volume, indicating that ultrasound could be used to trigger localized release of paclitaxel even when anchored to the microbubble (Yan et al. 2013). Figure 12.6b summarizes in vivo work done and shows effectiveness of these PLMCs when ultrasound is applied in addition to PLMCs alone. We will further discuss the mechanism by which sonoporation increases effectiveness of drug delivery later in the chapter.

(a) Effect of initial size of treated tumors on tumor growth response for treatments with 5 mg/kg of DOX. The arrows indicate schedule for treatments (Lin et al. 2012). (b) 4T1-tumor bearing mice were treated with PBS (squares, PBS only control), unloaded MBs (circles, unloaded MBs + US), PLMC (upwards triangles, PLMC without US), PL (downwards triangles, PL + US), and PLMC (diamonds, PLMC + US) on day 10, day 13, and day 16 after tumor cell injection. Systemic therapy with PLMC resulted in significantly greater tumor growth inhibition vs. PBS control, PLMC without US, unloaded MBs, and PL under US exposure. The results represent the mean ± SD, n = 6. *p < 0.05, **p < 0.01. PTX = paclitaxel. Reprinted with permission from Elsevier (Yan et al. 2013)
5.3 Gene Therapy
Gene therapy is a promising alternative for treatment of a diverse array of cancers. Through targeting and suppression of oncogenes or insertion of apoptotic genes, gene therapy has become an intense area of research due to the possibility of avoiding severe side effects associated with traditional chemotherapy agents. However, naked nucleic acids are quickly degraded by nuclease activity or cleared from the tumor area, posing a difficult challenge to delivery (Roth and Cristiano 1997). In an attempt to improve gene transfection and prolong circulation, both viral and non-viral vectors have been evaluated for gene delivery. Viral vectors, such as retrovirus and herpes simplex virus (HSV), delivered systemically result in transduction of non-target tissues leading to adverse side effects. Additionally, viral vectors also elicit an immune response that can limit their effectiveness and prevent repeated use of the vectors (El-Aneed 2004). Non-viral vectors currently suffer from low transfection efficiency, where the amount of genetic material delivered fails to result in a functional effect (Niidome and Huang 2002). As a result of these difficulties, current gene therapy treatments remain in clinical or preclinical testing.
5.3.1 Gene Therapy Loading
Incorporation of oligonucleotides directly into the microbubble not only protects genetic material from degradation but also improves spatial targeting of the genetic payload through selective microbubble bursting. The most common method of incorporating oligonucleotides to the microbubble is through electrostatic interactions. Because of the negative charge of DNA, inclusion of positively charged species into or on the microbubble shell can aid in loading a nucleotide payload. In a comparison of cationic and control neutral charged microbubbles, Panje et al. (2012) showed that cationic lipid microbubbles were able to bind plasmid DNA with a capacity that was 7.5-fold higher than neutral microbubbles. As shown in Fig. 12.7, this DNA binding by cationic microbubbles shielded DNA from DNase activity better than neutral microbubbles or free plasmid, as indicated by gel electrophoresis.

Binding of plasmid DNA to cationic MBs and DNase protection assay. (a) Direct binding of YOYO-1-labeled plasmid DNA (10 μg) to cationic MBs (1 × 108) but not neutral MBs (1 × 108) was confirmed visually by confocal microscopy (1,000×, scale bar = 10 μm). (b) Gel electrophoresis confirmed partial protection of plasmid DNA bound to cationic MBs (lane 4) from DNase degradation. Plasmid DNA mixed with and not bound to neutral MBs (lane 5) were completely degraded after DNase treatment. Lane 2 represents control samples containing only plasmid DNA without MBs that were not exposed to DNase. Lane 3 shows complete DNase degradation of plasmid DNA not incubated with either MB type. Original figure from Panje CM, et al. Ultrasound-Mediated Gene Delivery with Cationic Versus Neutral Microbubbles: Effect of DNA and Microbubble Dose on In Vivo Transfection Efficiency. Theranostics 2012; 2(11):1078–1091. http://www.thno.org/v02p1078.htm. Reprinted with permission from Theranostics Publishing (Panje et al. 2012)
As an alternative to including cationic lipid in the microbubble shell, cationic polymers can also be used to coat the surface of the microbubble with complexed oligonucleotides. By using the layer-by-layer (LbL) assembly technique to attach multiple layers of DNA and poly-l-lysine (PLL) onto preformed lipid-coated microbubbles, Borden et al. (2007) showed that a tenfold increase in DNA loading capacity was possible. Similarly, Lentacker et al. coated albumin-shelled microbubbles with poly(allylamine hydrochloride) (PAH) and showed minimal changes in microbubble size distributions and ultrasonic function. Additionally, the cationic coating yielded increased binding of DNA to microbubbles and helped to protect bound DNA from nuclease degradation (Lentacker et al. 2006).
5.3.2 Gene Therapy Treatment
Two major types of gene therapies involve use of either DNA or short interfering RNA (siRNA). The delivery of DNA seeks to up-regulate expression of an immune response marker or suicide gene in tumor cells. Cells expressing HSV thymidine kinase (TK) are easily targeted and eliminated by treatment with ganciclovir. Using a mouse model of squamous cell carcinoma, tumors sonoporated in the presence of microbubbles loaded with TK displayed longer doubling times (p < 0.02), and TK-treated tumors displayed increased apoptosis (p < 0.04) and more areas of cellular dropout (p < 0.03) (Carson et al. 2011). Further studies additionally demonstrated effective in vivo delivery of DNA genes to cancer tumors. Using a commercially available microbubble, Sonidel MB101 microbubble (Sonidel Ltd, Ireland), Li et al. optimized cell transfection in vitro and demonstrated transfection efficiencies of up to 18 % using ultrasound. After optimization, the group used episomal plasmid-based gene with a luciferase reporter to deliver DNA in mouse hind leg muscle tumors. Luciferase activity, indicating gene expression, did not diminish during tumor growth and suggested plasmid replication during tumor expansion (Fig. 12.8) (Li et al. 2009).

Demonstration of prolonged luciferase activity in mouse hind leg muscle tumors after delivery of luciferase reporter, pEIP-1-Luc, following ultrasound-mediated and MB101®-assisted transfection in vivo. (a) The signal obtained from an animal at day 4 following transfection and (b) the same animal at day 20 following transfection. (c and d) The luminescent signal generated by the skin overlying the tumor and excised tumor, respectively. Reprinted with permission from Elsevier (Li et al. 2009)
Short interfering RNA (siRNA) are double stranded RNA oligonucleotides of approximately 20–25 kb in length and are complementary in sequence to an area of a gene of interest. siRNA bind to a protein called RISC (RNA-induced silencing complex) which uses RNase to cleave mRNA strands that match the complementary siRNA strand (Martinez et al. 2002). Delivery of siRNA targeted to oncogenes can be used to stop expression of key proteins and reduce tumor sizes (Urban-Klein et al. 2005). Using a GFP expressing rat C166 cell line, Kinoshita and Hynynen showed that 11 % of cells showed reduced GFP expression 48 h post-sonoporation with continuous wave ultrasound (Kinoshita and Hynynen 2005). Delivery of microbubbles loaded with epidermal growth factor receptor (EGFR) directed siRNA to murine squamous carcinoma cells in vivo resulted in three to fivefold increase in the doubling time of treated tumors compared with controls (Carson et al. 2012). No EGFR knockdown was observed in non-sonoporated tissues (i.e., heat, lungs, etc.), and there was no detectable increase of cytokines 24 h post-injection, demonstrating selectivity of the treatment to the targeted area. While the types of tumors suitable for targeting by siRNA/microbubble therapy can be limited due to US scattering by various tissues, further effectiveness of siRNA transfection may be achieved through optimization of acoustic parameters and bubble response.
5.4 Protein Therapy
Even though the majority of the literature using microbubble delivery of a payload pertains to drugs smaller than 2,000 Da or genetic material, there are several studies using microbubbles for protein delivery by exploiting their unique ultrasound-responsive property. Bekeredjian et al. incorporated luciferase enzyme as a model protein drug into the lipid shell of a microbubble for ultrasound-mediated delivery to the heart (Bekeredjian et al. 2005) or testes (Bekeredjian et al. 2007). They showed that protein delivery into the organ is augmented due to ultrasonic destruction via in vivo studies.
5.4.1 Therapeutic Protein Loading
Because of their size and availability of potential linkages, protein loading commonly involves covalent attachment between protein and the surface of microbubble. An amide bond between an amino group on the protein ligand can be formed between a carboxyl group or a maleimide on the microbubble shell with a protein thiol group to load the microbubble surface. The required moieties on the microbubble shell are generally incorporated via functionalized end groups of poly(ethylene glycol).
5.4.2 Current Protein Therapy Uses
As an alternative to traditional drug action, protein-conjugated microbubbles can act to modulate cell activity. For antigen delivery during vaccination, adjuvants are required to promote immunogenicity. Microbubbles coated with surface proteins can act as an antigen delivery system without the need for ultrasound application. Bioley et al. (2012) used covalent bonds between maleimide molecules on the microbubbles and thiol groups from the antigen to coat the microbubble surface. Microbubbles could have a direct effect on structural and immune cells of the lymph node, which are primary sites of adaptive immunity induction, because they have been shown to directly drain from peripheral administration sites to afferent lymph node (Sever et al. 2012).
6 Targeted Therapies Using Microbubbles
Microbubbles have been used in the clinic as ultrasound imaging contrast agents for echocardiography since 1997 in the United States. In combination with ultrasound, microbubbles have shown potential for molecular level imaging and delivery of drugs or genes to cells or tissue. While these advances are promising, microbubbles for molecular imaging or therapeutic purposes for the most part remain in the preclinical stage of development.
6.1 Targeting Methods
Tissue and cell specificity can be achieved by using passively or actively targeted microbubbles. Passive targeting refers to taking advantage of the body’s intrinsic mechanism, phagocytosis, and inherent properties of the microbubble shell to use their affinity for a specific cell type or tissue. For example, albumin-shelled microbubbles were shown to bind to adherent leukocytes via cell-surface integrins or complement-mediated opsonization solely due to their shell composition (Ferrara et al. 2007; Kiessling et al. 2009; Deshpande et al. 2010). On the other hand, active targeting refers to covalent or noncovalent attachment of specific targeting moieties to the microbubble shell, to allow for binding to specific receptors. Most microbubble shell composition consists of lipid; thus, by using polymer-attached lipid, targeting moieties can be tethered at the end of the polymer brush. The polymer brush plays a role as a spacer between the ligand and monolayer shell for the ligand to bind its receptor efficiently (Kim et al. 2000). The method of linking targeting agents to the polymer brush is analogous to tethering of drug-carrying particles, which we discussed in the previous sections. For non-covalent attachment of ligand, the biotin–avidin linkage is the most widely used technique (Fig. 12.9).

Targeted drug-loaded microbubbles via noncovalent biotin–avidin linkage
Covalent attachment includes creating an amide bond between an amino group on the ligand and a carboxyl group on the microbubbles or, alternatively, using a maleimide on the microbubble shell to react with a thiol group on the ligand.
6.2 Preclinical Applications of Targeted Microbubbles
There are 52 targeted ultrasound agents up to date (June 27, 2013) in the Molecular Imaging and Contrast Agent Database (MICAD) collected by the National Center for Biotechnology Information (NCBI), at the National Institutes of Health (NIH). Twenty-one of these have been developed for diagnosing and treating tumor angiogenesis, while 18 have been developed for inflammation in preclinical models. Table 12.1 summarizes targeted microbubbles that are currently involved in clinical trials. The most used molecular markers for assessment of tumor angiogenesis are vascular endothelial growth factor receptor 2 (VEGFR2) and αvβ3 integrin. Willmann et al. (2008) studied the effect of VEGFR2-targeted microbubbles on quantitative video intensity of ultrasound contrast enhanced molecular imaging in angiosarcoma and malignant glioma mice models. The average video intensity was significantly higher when using VEGFR2 targeted microbubbles vs. control immunoglobulin G2 antibody microbubbles (p < 0.001).
Commonly used targets for detecting and treating diseases by inflammation, such as atherosclerosis or myocardial ischemia, are VCAM-1 (vascular cell adhesion molecule 1), ICAM-1 (intercellular adhesion molecule 1), E-selectin, and P-selectin. Yan et al. studied the degree of myocardial inflammation and levels of ICAM-1 protein using ultrasound molecular imaging with ICAM-1 targeted microbubbles, as well as routine non-invasive methods including electrocardiography, echocardiography, and plasma troponin I levels (Yan et al. 2011). The video intensity of ICAM-1 molecular images of the ischemic anterior wall was almost three times greater than that in the non-ischemic posterior wall during the late phase (8–24 h) of reperfusion. In contrast, routine methods yielded only weak evidence of ischemia, suggesting the ultrasound molecular imaging with targeted microbubbles provides reliable evidence of a recent myocardial ischemic event in the late phase of reperfusion. Also they investigated binding efficiency and rate of ICAM-1-targeted microbubbles in vitro (Fig. 12.8). In preclinical research, ligands are predominantly coupled to microbubbles via an avidin–biotin linkage. However, this can be problematic because of inherent immunogenicity of avidin in humans. Biotin-conjugated lipopolymer present on microbubbles activates the complement system in humans and mice (Borden et al. 2008). The first formulation for clinical application is BR55, that is, avidin–biotin-free soft shell microbubbles that target mouse and human VEGFR2. BR55 was found to strongly bind to the tumor endothelium of breast (Pochon et al. 2010) and prostate cancer xenografts in rodents (Tardy et al. 2010).
7 Mechanisms for Delivery of Therapeutic Agents Using Microbubbles and Ultrasound
As discussed previously, drug-loaded microbubbles are more effective when in combination with US. Therefore, optimization of the mechanical response for stable microbubble cavitation under sonoporation is a key factor in increasing the potential of therapeutic delivery. Traditional systemic drug delivery of small molecules and passive drug delivery particles rely on tumor enhanced permeability and retention (EPR) effect to perfuse tumor tissues (Maeda 2001). Due to increased angiogenesis and nutrient demand of tumor aggregates, high molecular weight molecules and particles are trapped in the defective vascular architecture near the tumor and remain there due to impaired lymphatic drainage/recovery system. This effect is commonly referred to as the EPR effect. However, small molecules are able to diffuse away from the tumor site and are unaffected by EPR (Maeda et al. 2000). Additionally, some tumors are as far as 100 μm from vasculature or are located in hypoxic regions, which remain difficult to reach from systemic delivery (Helmlinger et al. 1997). Stable microbubble cavitation is able to increase extravasation of small molecules from the vasculature to tumor sites. Using a flow-through tissue-mimicking phantom composed of a biocompatible hydrogel with embedded tumor cells, luciferase expression was shown to increase by 60-fold even for modest microbubble concentrations undergoing inertial cavitation (bubble collapse) when delivering a non-replicating luciferase-expressing adenovirus (Arvanitis et al. 2011). Using commercially available SonoVue, none of the insonation conditions induced cell death under ultrasound alone. However, extravasation from the tissue phantom vessel was shown to exhibit short-range vessel disruption during stable cavitation and formation of micro-channels during inertial cavitation. The findings suggest that enhanced drug delivery extravasation of anticancer agents through the use of microbubbles is possible.
Sonoporation alone has been shown to increase therapeutic retention in cells, indicating the role of acoustic energy in effecting cell permeability. In gene therapy, sonoporation of various cancer cell lines (U937, HeLa, PC-3, Meth-A, and T-24) in the presence of a reporter gene was shown to significantly increase reporter gene expression over both electrotransfection and liposomal transfection without ultrasound (Feril et al. 2006). In vivo ultrasound stimulation of prostate tumor cells implanted subcutaneously in rats induced a tenfold increase of a β-galactosidase reporter measured via histology and a 15-fold increase of β-galactosidase protein expression via ELISA (Huber and Pfisterer 2000). However, at these low frequencies (<20 kHz), prolonged ultrasound exposure has been demonstrated to result in cell death and tissue damage (Miller et al. 2002). Furthermore, these low frequencies are not in the range of clinical use ultrasound. Increasing the applied frequency to the clinical range of 1–3 MHz or using pulse-mode ultrasound reduces tissue damage but also results in lowered transfection (Hallow et al. 2006). One way to increase the efficiency of high frequency ultrasound sonoporation is through combination with microbubbles.
Furthermore, US and microbubbles have been used as tools to increase blood–brain-barrier permeability of drugs and drug delivery vehicles. Sheikov et al. showed that when US is applied in the presence of microbubbles, the acoustic energies stimulate active vesicular transport and temporarily disrupt tight junctions to allow previously size occluded drugs to pass and treat the diseased areas (Sheikov et al. 2004, 2008). Treat et al. (2012) used liposomal doxorubicin and focused US to increase permeability of the blood–brain barrier and showed a greater decrease in brain tumor size when compared with administration of free doxorubicin alone. Some groups have even used the microbubble cavitation phenomenon to accelerate lysis of thrombus and blood clots (Porter and Xie 2001; Porter et al. 1996; Culp et al. 2003).
8 Summary
There is a large body of literature for use of various microbubble formulations in imaging and treatment of oncological diseases. The purpose of this chapter was to introduce the reader to the basic form and function of microbubbles and to discuss current work that have laid the foundation for the use of microbubbles as contrast agents, drug delivery vehicles, and theranostic particles. The articles reviewed here only constitute a small fraction of the literature on this topic, and there is still work being done in order to move these technologies toward clinical use. More advanced studies in vivo need to be performed, and methods of optimization of acoustic parameters of the ultrasound contrast agents in vivo are being developed to aid in truly realizing the full potential of microbubbles in the clinic. Through the combination of these hybrid drug-loaded contrast agents and molecular targeting, a complete theranostic tool may be developed that would allow a clinician to potentially image, locate, and treat localized tumors with just one injection of these multipurpose particles. Furthermore, the spatial control given to clinicians over the delivery of therapeutic agents directly to the tumor site will minimize damage done to surrounding healthy tissues and has the potential to prevent side effects that currently plague chemotherapy. Using specific targeting agents and combination of multi-image modalities, microbubble platforms may one day have the capability of reaching the tumor site regardless of its location in the body. The further development of these systems could have a considerable impact on treatment and diagnosis of not only cancer but also on numerous other diseases and disorders.
References
Arvanitis CD et al (2011) Cavitation-enhanced extravasation for drug delivery. Ultrasound Med Biol 37(11):1838–1852
Bekeredjian R et al (2005) Augmentation of cardiac protein delivery using ultrasound targeted microbubble destruction. Ultrasound Med Biol 31(5):687–691
Bekeredjian R et al (2007) Ultrasound-targeted microbubble destruction augments proteins delivery into testes. Urology 69(2):386–389
Bioley G et al (2012) Gas-filled microbubble-mediated delivery of antigen and the induction of immune responses. Biomaterials 33(25):5935–5946
Blomley MJ et al (2001) Microbubble contrast agents: a new era in ultrasound. BMJ 322(7296):1222–1225
Borden MA et al (2007) DNA and polylysine adsorption and multilayer construction onto cationic lipid-coated microbubbles. Langmuir 23(18):9401–9408
Borden MA et al (2008) A stimulus-responsive contrast agent for ultrasound molecular imaging. Biomaterials 29(5):597–606
Carson AR et al (2011) Gene therapy of carcinoma using ultrasound-targeted microbubble destruction. Ultrasound Med Biol 37(3):393–402
Carson AR et al (2012) Ultrasound-targeted microbubble destruction to deliver siRNA cancer therapy. Cancer Res 72(23):6191–6199
Castle J et al (2013) Ultrasound-mediated targeted drug delivery: recent success and remaining challenges. Am J Physiol Heart Circ Physiol 304(3):H350–H357
Castro-Hernandez E et al (2011) Microbubble generation in a co-flow device operated in a new regime. Lab Chip 11(12):2023–2029
Chen SY et al (2006) Efficient gene delivery to pancreatic islets with ultrasonic microbubble destruction technology. Proc Natl Acad Sci U S A 103(22):8469–8474
Cochran MC et al (2011) Doxorubicin and paclitaxel loaded microbubbles for ultrasound triggered drug delivery. Int J Pharm 414(1–2):161–170
Cosgrove D (2004) The advances are significant improvements in both the microbubbles used as contrast agents and in the software that allows their selective detection. Eur Radiol 14(Suppl 8): P1–P3
Cosgrove D (2006) Ultrasound contrast agents: an overview. Eur J Radiol 60(3):324–330
Cui W et al (2005) Preparation and evaluation of poly(l-lactide-co-glycolide) (PLGA) microbubbles as a contrast agent for myocardial contrast echocardiography. J Biomed Mater Res B Appl Biomater 73(1):171–178
Culp WC et al (2003) Microbubble-augmented ultrasound declotting of thrombosed arteriovenous dialysis grafts in dogs. J Vasc Interv Radiol 14(3):343–347
Deshpande N, Needles A, Willmann JK (2010) Molecular ultrasound imaging: current status and future directions. Clin Radiol 65(7):567–581
Dove JD, Murray TW, Borden MA (2013) Enhanced photoacoustic response with plasmonic nanoparticle-templated microbubbles. Soft Matter 9(32):7743–7750
Duncanson WJ et al (2010) Targeted binding of PEG-lipid modified polymer ultrasound contrast agents with tiered surface architecture. Biotechnol Bioeng 106(3):501–506
El-Aneed A (2004) An overview of current delivery systems in cancer gene therapy. J Control Release 94(1):1–14
Fabiilli ML et al (2010) Delivery of water-soluble drugs using acoustically triggered perfluorocarbon double emulsions. Pharm Res 27(12):2753–2765
Fang JY et al (2007) A study of the formulation design of acoustically active lipospheres as carriers for drug delivery. Eur J Pharm Biopharm 67(1):67–75
Feril LB et al (2006) Optimized ultrasound-mediated gene transfection in cancer cells. Cancer Sci 97(10):1111–1114
Ferrara K, Pollard R, Borden M (2007) Ultrasound microbubble contrast agents: fundamentals and application to gene and drug delivery. Annu Rev Biomed Eng 9:415–447
Ganan-Calvo AM, Gordillo JM (2001) Perfectly monodisperse microbubbling by capillary flow focusing. Phys Rev Lett 87(27 Pt 1):274501
Geers B et al (2011) Self-assembled liposome-loaded microbubbles: the missing link for safe and efficient ultrasound triggered drug-delivery. J Control Release 152(2):249–256
Gunduz O et al (2012) Bioinspired bubble design for particle generation. J R Soc Interface 9(67):389–395
Hallow DM et al (2006) Measurement and correlation of acoustic cavitation with cellular bioeffects. Ultrasound Med Biol 32(7):1111–1122
Harvey CJ et al (2001) Developments in ultrasound contrast media. Eur Radiol 11(4):675–689
Hashimoto M et al (2008) Formation of bubbles and droplets in parallel, coupled flow-focusing geometries. Small 4(10):1795–1805
Helmlinger G et al (1997) Interstitial pH and pO(2) gradients in solid tumors in vivo: high-resolution measurements reveal a lack of correlation. Nat Med 3(2):177–182
Hettiarachchi K et al (2007) On-chip generation of microbubbles as a practical technology for manufacturing contrast agents for ultrasonic imaging. Lab Chip 7(4):463–468
Hettiarachchi K et al (2009) Controllable microfluidic synthesis of multiphase drug-carrying lipospheres for site-targeted therapy. Biotechnol Prog 25(4):938–945
Huber PE, Pfisterer P (2000) In vitro and in vivo transfection of plasmid DNA in the Dunning prostate tumor R3327-AT1 is enhanced by focused ultrasound. Gene Ther 7(17):1516–1525
Hynynen K et al (2001) Noninvasive MR imaging-guided focal opening of the blood–brain barrier in rabbits. Radiology 220(3):640–646
Janib SM, Moses AS, MacKay JA (2010) Imaging and drug delivery using theranostic nanoparticles. Adv Drug Deliv Rev 62(11):1052–1063
Kang J et al (2010) Antitumor effect of docetaxel-loaded lipid microbubbles combined with ultrasound-targeted microbubble activation on VX2 rabbit liver tumors. J Ultrasound Med 29(1):61–70
Kendall MR et al (2012) Scaled-up production of monodisperse, dual layer microbubbles using multi-array microfluidic module for medical imaging and drug delivery. Bubble Sci Eng Technol 4(1):12–20
Kiessling F, Huppert J, Palmowski M (2009) Functional and molecular ultrasound imaging: concepts and contrast agents. Curr Med Chem 16(5):627–642
Kiessling F et al (2012) Ultrasound microbubbles for molecular diagnosis, therapy, and theranostics. J Nucl Med 53(3):345–348
Kim DH, Klibanov AL, Needham D (2000) The influence of tiered layers of surface-grafted poly(ethylene glycol) on receptor-ligand-mediated adhesion between phospholipid monolayer-stabilized microbubbles and coated class beads. Langmuir 16(6):2808–2817
Kinoshita M, Hynynen K (2005) A novel method for the intracellular delivery of siRNA using microbubble-enhanced focused ultrasound. Biochem Biophys Res Commun 335(2): 393–399
Klibanov AL (1999) Targeted delivery of gas-filled microspheres, contrast agents for ultrasound imaging. Adv Drug Deliv Rev 37(1–3):139–157
Kwan JJ, Borden MA (2010) Microbubble dissolution in a multigas environment. Langmuir 26(9):6542–6548
Kwan JJ, Borden MA (2012) Lipid monolayer collapse and microbubble stability. Adv Colloid Interface Sci 183:82–99
Laurent S et al (2008) Magnetic iron oxide nanoparticles: synthesis, stabilization, vectorization, physicochemical characterizations, and biological applications. Chem Rev 108(6):2064–2110
Lee MH, Lee D (2010) Elastic instability of polymer-shelled bubbles formed from air-in-oil-in-water compound bubbles. Soft Matter 6(18):4326–4330
Lee H et al (2006) Antibiofouling polymer-coated superparamagnetic iron oxide nanoparticles as potential magnetic resonance contrast agents for in vivo cancer imaging. J Am Chem Soc 128(22):7383–7389
Lentacker I et al (2006) Microbubbles which bind and protect DNA against nucleases. J Control Release 116(2):E73–E75
Lentacker I et al (2007) Lipoplex-loaded microbubbles for gene delivery: a Trojan horse controlled by ultrasound. Adv Funct Mate 17(12):1910–1916
Lentacker I et al (2010) Design and evaluation of doxorubicin-containing microbubbles for ultrasound-triggered doxorubicin delivery: cytotoxicity and mechanisms involved. Mol Ther 18(1):101–108
Leong-Poi H et al (2007) Therapeutic arteriogenesis by ultrasound-mediated VEGF165 plasmid gene delivery to chronically ischemic skeletal muscle. Circ Res 101(3):295–303
Li YS et al (2009) Optimising ultrasound-mediated gene transfer (sonoporation) in vitro and prolonged expression of a transgene in vivo: potential applications for gene therapy of cancer. Cancer Lett 273(1):62–69
Lin CY et al (2012) Enhancement of focused ultrasound with microbubbles on the treatments of anticancer nanodrug in mouse tumors. Nanomedicine 8(6):900–907
Liu Z et al (2011) Iron oxide nanoparticle-containing microbubble composites as contrast agents for MR and ultrasound dual-modality imaging. Biomaterials 32(26):6155–6163
Maeda H (2001) The enhanced permeability and retention (EPR) effect in tumor vasculature: the key role of tumor-selective macromolecular drug targeting. Adv Enzyme Regul 41:189–207
Maeda H et al (2000) Tumor vascular permeability and the EPR effect in macromolecular therapeutics: a review. J Control Release 65(1–2):271–284
Martinez J et al (2002) Single-stranded antisense siRNAs guide target RNA cleavage in RNAi. Cell 110(5):563–574
Massoud TF, Gambhir SS (2003) Molecular imaging in living subjects: seeing fundamental biological processes in a new light. Genes Dev 17(5):545–580
Mesiwala AH, Mourad PD (2002) Monitoring of biologic effects of focused ultrasound beams on the brain. Radiology 224(1):294–296, author reply 296–7
Mesiwala AH et al (2002) High-intensity focused ultrasound selectively disrupts the blood–brain barrier in vivo. Ultrasound Med Biol 28(3):389–400
Miller DL, Pislaru SV, Greenleaf JE (2002) Sonoporation: mechanical DNA delivery by ultrasonic cavitation. Somat Cell Mol Genet 27(1–6):115–134
Niidome T, Huang L (2002) Gene therapy progress and prospects: nonviral vectors. Gene Ther 9(24):1647–1652
Nisisako T, Torii T (2008) Microfluidic large-scale integration on a chip for mass production of monodisperse droplets and particles. Lab Chip 8(2):287–293
Panje CM et al (2012) Ultrasound-mediated gene delivery with cationic versus neutral microbubbles: effect of DNA and microbubble dose on in vivo transfection efficiency. Theranostics 2(11):1078–1091
Paradossi G et al (2003) Poly(vinyl alcohol) as versatile biomaterial for potential biomedical applications. J Mater Sci Mater Med 14(8):687–691
Parhizkar M, Edirisinghe M, Stride E (2013) Effect of operating conditions and liquid physical properties on the size of monodisperse microbubbles produced in a capillary embedded T-junction device. Microfluid Nanofluidics 14(5):797–808
Park Y et al (2012) Tunable diacetylene polymerized shell microbubbles as ultrasound contrast agents. Langmuir 28(8):3766–3772
Phillips P, Gardner E (2004) Contrast-agent detection and quantification. Eur Radiol 14(Suppl 8): P4–P10
Pochon S et al (2010) BR55: a lipopeptide-based VEGFR2-targeted ultrasound contrast agent for molecular imaging of angiogenesis. Invest Radiol 45(2):89–95
Porter TR, Xie F (2001) Ultrasound, microbubbles, and thrombolysis. Prog Cardiovasc Dis 44(2):101–110
Porter TR et al (1996) Thrombolytic enhancement with perfluorocarbon-exposed sonicated dextrose albumin microbubbles. Am Heart J 132(5):964–968
Pramanik M et al (2008) Design and evaluation of a novel breast cancer detection system combining both thermoacoustic (TA) and photoacoustic (PA) tomography. Med Phys 35(6):2218–2223
Rapoport N, Gao Z, Kennedy A (2007) Multifunctional nanoparticles for combining ultrasonic tumor imaging and targeted chemotherapy. J Natl Cancer Inst 99(14):1095–1106
Romanowsky MB et al (2012) High throughput production of single core double emulsions in a parallelized microfluidic device. Lab Chip 12(4):802–807
Roth JA, Cristiano RJ (1997) Gene therapy for cancer: what have we done and where are we going? J Natl Cancer Inst 89(1):21–39
Sarkar K, Katiyar A, Jain P (2009) Growth and dissolution of an encapsulated contrast microbubble: effects of encapsulation permeability. Ultrasound Med Biol 35(8):1385–1396
Sciallero C, Trucco A (2013) Ultrasound assessment of polymer-shelled magnetic microbubbles used as dual contrast agents. J Acoust Soc Am 133(6):El478–El484
Sever AR et al (2012) Sentinel node identification using microbubbles and contrast-enhanced ultrasonography. Clin Radiol 67(7):687–694
Sheikov N et al (2004) Cellular mechanisms of the blood–brain barrier opening induced by ultrasound in presence of microbubbles. Ultrasound Med Biol 30(7):979–989
Sheikov N et al (2008) Effect of focused ultrasound applied with an ultrasound contrast agent on the tight junctional integrity of the brain microvascular endothelium. Ultrasound Med Biol 34(7):1093–1104
Shortencarier MJ et al (2004) A method for radiation-force localized drug delivery using gas-filled lipospheres. IEEE Trans Ultrason Ferroelectr Freq Control 51(7):822–831
Stride E, Saffari N (2003) Microbubble ultrasound contrast agents: a review. Proc Inst Mech Eng H 217(6):429–447
Talu E et al (2007) Tailoring the size distribution of ultrasound contrast agents: possible method for improving sensitivity in molecular imaging. Mol Imaging 6(6):384–392
Tardy I et al (2010) Ultrasound molecular imaging of VEGFR2 in a rat prostate tumor model using BR55. Invest Radiol 45(10):573–578
Tinkov S et al (2010a) New doxorubicin-loaded phospholipid microbubbles for targeted tumor therapy: in-vivo characterization. J Control Release 148(3):368–372
Tinkov S et al (2010b) New doxorubicin-loaded phospholipid microbubbles for targeted tumor therapy: Part I – Formulation development and in-vitro characterization. J Control Release 143(1):143–150
Treat LH et al (2012) Improved anti-tumor effect of liposomal doxorubicin after targeted blood–brain barrier disruption by MRI-guided focused ultrasound in rat glioma. Ultrasound Med Biol 38(10):1716–1725
Unger EC et al (1998) Acoustically active lipospheres containing paclitaxel: a new therapeutic ultrasound contrast agent. Invest Radiol 33(12):886–892
Unger EC et al (2001) Local drug and gene delivery through microbubbles. Prog Cardiovasc Dis 44(1):45–54
Unger EC et al (2004) Therapeutic applications of lipid-coated microbubbles. Adv Drug Deliv Rev 56(9):1291–1314
Urban-Klein B et al (2005) RNAi-mediated gene-targeting through systemic application of polyethylenimine (PEI)-complexed siRNA in vivo. Gene Ther 12(5):461–466
Villa R et al (2013) Targeted doxorubicin delivery by chitosan-galactosylated modified polymer microbubbles to hepatocarcinoma cells. Colloids Surf B Biointerfaces 110:434–442
Willmann JK et al (2008) US imaging of tumor angiogenesis with microbubbles targeted to vascular endothelial growth factor receptor type 2 in mice. Radiology 246(2):508–518
Xu MH, Wang LHV (2006) Photoacoustic imaging in biomedicine. Rev Sci Instrum 77(4):1–22
Xu JH et al (2012) Controllable gas/liquid/liquid double emulsions in a dual-coaxial microfluidic device. Lab Chip 12(11):2029–2036
Yan Y et al (2011) Late-phase detection of recent myocardial ischaemia using ultrasound molecular imaging targeted to intercellular adhesion molecule-1. Cardiovasc Res 89(1):175–183
Yan F et al (2013) Paclitaxel-liposome-microbubble complexes as ultrasound-triggered therapeutic drug delivery carriers. J Control Release 166(3):246–255
Yang F et al (2009) Superparamagnetic iron oxide nanoparticle-embedded encapsulated microbubbles as dual contrast agents of magnetic resonance and ultrasound imaging. Biomaterials 30(23–24):3882–3890
Acknowledgments
J. Y. W. acknowledges support from Boston University’s College of Engineering Distinguished Faculty Fellowship, T. P. acknowledges support from the NIH/NIGMS T32 GM008764 and the NIH/NIAID T32 AI089673, and C. B. acknowledges support from the National Science Foundation Graduate Research Fellowship Program.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Controlled Release Society
About this chapter
Cite this chapter
Pham, T., Beigie, C., Park, Y., Wong, J.Y. (2014). Microbubbles as Theranostics Agents. In: Alonso, M., Garcia-Fuentes, M. (eds) Nano-Oncologicals. Advances in Delivery Science and Technology. Springer, Cham. https://doi.org/10.1007/978-3-319-08084-0_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-08084-0_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-08083-3
Online ISBN: 978-3-319-08084-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)