
Abstract
Vestibular migraine is an increasingly recognized cause of recurrent vertigo. It may present at any age with attacks of spontaneous or positional vertigo, head motion-induced vertigo and visual vertigo lasting minutes to days. Since headache is often absent during acute attacks, other migrainous features such as photophobia, phonophobia or auras have to be specifically inquired about. The recent classification of vestibular migraine allows identification of vestibular migraine and probable vestibular migraine on the basis of explicit criteria. The diagnosis of VM is based on recurrent vestibular symptoms, a history of migraine, temporal association of vestibular symptoms with migraine symptoms and exclusion of other causes. Vestibular symptoms must be of moderate or severe intensity. Duration of acute episodes is limited to a window between 5 min and 72 h. Common triggers include stress, sleep deprivation and hormonal changes. During acute attacks one may find central spontaneous or positional nystagmus and, less commonly, signs of unilateral vestibular hypofunction. In the asymptomatic interval, the neuro-otological examination is mostly normal. Some patients have mild ocular motor abnormalities including persistent positional nystagmus.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Hearing Loss
- International Headache Society
- Benign Paroxysmal Positional Vertigo
- Vestibular Disorder
- Vestibular Migraine
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
6.1 Introduction
The interrelations of vertigo and migraine are increasingly recognized by the medical community. The number of published papers on vestibular migraine (VM) has rocketed in the last decades. A PubMed search using the term “migraine” and “vestibular” yields 10 hits before 1980, 70 between 1980 and 2000 and 310 since then. That migraine may present with attacks of vertigo has been noted from the early days of neurology [1]. Starting with Kayan and Hood’s classical paper [2], the clinical features of VM have been well elucidated in several large case series [3–9]. Various terms have been used to designate vertigo caused by a migraine mechanism including migraine-associated vertigo, migraine-associated dizziness, migraine-related vestibulopathy, migrainous vertigo, benign recurrent vertigo and basilar migraine. Vestibular migraine has been convincingly advocated as a term that stresses the particular vestibular manifestation of migraine and thus best avoids confounding with non-vestibular dizziness associated with migraine [10]. Therefore, the Bárány Society and the International Headache Society (IHS) have opted for vestibular migraine in their recent joint paper on the classification of the disorder [11].
6.2 Diagnostic Criteria for Vestibular Migraine
In the previous International Classification of Headache Disorders (ICHD-2), vertigo was not included as a migraine symptom in adults except in the framework of basilar-type migraine [12], which leads to vertigo in more than 60 % of the patients [13]. As an aura symptom of basilar-type migraine, vertigo should last between 5 and 60 min and should be followed by migraine headaches. In addition, at least one more aura symptom from the posterior circulation is required. Less than 10 % of patients with VM fulfilled the criteria for basilar-type migraine [5–8], which makes basilar-type migraine an inappropriate category for most of these patients.
Therefore, the Bárány Society, which represents the international community of basic scientists, otolaryngologists and neurologists committed to vestibular research, mandated a classification group to develop diagnostic criteria for VM. The draught of the classification was extensively discussed with the Migraine Classification Committee of the International Headache Society, which resulted in a joint document defining vestibular migraine and probable vestibular migraine [11]. These criteria have been included in the third edition of the International Classification of Headache Disorders (ICHD-3), published in 2013 [14]. VM appears in the appendix for new disorders that need further research for validation. In addition, the classification of vestibular migraine is part of the evolving Classification of Vestibular Disorders of the Bárány Society. The new ICHD-3 includes only vestibular migraine, while the Bárány classification also contains probable vestibular migraine (Table 6.1).
6.3 Prevalence of Vestibular Migraine
Vestibular migraine was diagnosed in 7 % in a group of 200 dizziness clinic patients and in 9 % of 200 migraine clinic patients [8]. In a population-based study (n = 4,869) with screening interviews followed by expert telephone interviews, the lifetime prevalence of VM was estimated at 0.98 % (95 % CI 0.7–1.37) [18]. Of note, VM accounted for only a third of migraine patients with a history of vertigo, which indicates the need for a thorough neuro-otological workup for exclusion of other diagnoses [18]. In a community-based sample of middle-aged women in Taiwan, VM was identified in 5 % and in 30 % of those with migraine [19]. VM is still widely underdiagnosed, as shown by a study from a dizziness clinic in Switzerland, where VM accounted for 20 % of the diagnoses in young patients, but was suspected by the referring doctors in only 2 % [20] (for an extensive review on epidemiology of VM, see Chap. 5 in this volume).
6.3.1 Demographic Aspects
VM may occur at any age [4, 5, 7]. It is more common in women with a reported female to male ratio between 1.5 and 5 to 1 [5–8]. Familial clustering may occur, probably based on an autosomal dominant pattern of inheritance with decreased penetrance in men [21]. In most patients, migraine begins earlier in life than VM [7, 8]. Some patients have been free from migraine attacks for years when VM first manifests itself [7]. Not infrequently, vertigo attacks replace migraine headaches in women around menopause.
6.4 Vestibular Migraine in Children
Benign paroxysmal vertigo of childhood is an early manifestation of VM which is recognized by the ICHD [14]. It is characterized by brief attacks of vertigo or disequilibrium, anxiety and often nystagmus or vomiting, recurring for months or years in otherwise healthy young children [22]. Many of these children later develop migraine, often years after vertigo attacks have ceased [23]. A family history of migraine in first-degree relatives is twofold increased compared to controls [24]. The prevalence of recurrent vertigo probably related to migraine was estimated at 2.8 % in children between 6 and 12 years in a population-based study [24].
6.4.1 Symptoms
6.4.1.1 Types of Vertigo
Patients with VM typically report spontaneous or positional vertigo. Some experience a sequence of spontaneous vertigo transforming into positional vertigo after several hours or days. This positional vertigo is distinct from benign paroxysmal positional vertigo (BPPV) with regard to duration of individual attacks (often as long as the head position is maintained in VM versus seconds only in BPPV), duration of symptomatic episodes (minutes to days in VM versus weeks in BPPV) and nystagmus findings [25]. Altogether, 40–70 % of patients experience positional vertigo in the course of the disease, but not necessarily with every attack. A frequent additional symptom is head motion intolerance, i.e. imbalance, illusory motion and nausea aggravated or provoked by head movements [5, 26]. Visually induced vertigo, i.e. vertigo provoked by moving visual scenes such as traffic or movies, can be another prominent feature of VM [5, 27]. Nausea and imbalance are frequent but nonspecific accompaniments of acute VM. The combination of different types of vertigo distinguishes VM from other neuro-otological disorders such as benign paroxysmal positional vertigo or Menière’s disease, which typically present with monosymptomatic vertigo. Patients with VM are often affected by motion sensitivity even in-between attacks [28], which may lead to a chronic type of vestibular dizziness [25]. Another factor contributing to chronic vestibular migraine is secondary psychiatric morbidity, particularly anxiety disorders [29, 30]. These two components of interictal dizziness may not be easily discriminated in individual patients [31].
6.4.1.2 Relation to Headaches
VM often misses not only the duration criterion for an aura as defined by the ICHD but also the temporal relationship to migraine headaches: vertigo can precede headache as would be typical for an aura, may begin with headache or may appear late in the headache phase. Many patients experience attacks both with and without headache [4, 6, 7]. Quite frequently, patients have an attenuated headache with their vertigo as compared to their usual migraine [3, 6]. In some patients, vertigo and headache never occur together [4, 6, 8]. Misdiagnosis of VM as “cervical vertigo” may occur when accompanying pain is mainly or exclusively localized in the neck, which is quite common in patients with migraine [32].
6.4.1.3 Other Symptoms
Along with the vertigo, patients may experience photophobia, phonophobia, osmophobia and visual or other auras. These phenomena are of diagnostic importance, since they may represent the only apparent connection of vertigo and migraine. Patients need to be asked specifically about these migraine symptoms since they often do not volunteer them. A dizziness diary can be useful for prospective recording of associated features.
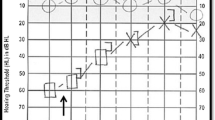
Auditory symptoms, including hearing loss, tinnitus and aural pressure, have been reported in up to 38 % of patients with VM [2, 5, 6, 33, 34]. Hearing loss is usually mild and transient, without or with only minor progression in the course of the disease [6]. About 20 % develop mild bilateral downsloping hearing loss over the years [35]. In contrast, unilateral moderate to severe hearing loss starting in the low-frequency range would rather favour a diagnosis of Menière’s disease.
6.4.1.4 Precipitating Factors
Asking for migraine-specific precipitants of vertigo attacks may provide valuable diagnostic information, e.g. provocation by menstruation, deficient sleep, excessive stress, skipped meals, lack of fluid and exposure to sensory stimuli, such as bright or scintillating lights, intense smells or noise. The influence of specific foods and weather conditions is probably overestimated. Sometimes, migraine accompaniments and typical precipitants may be missing, but VM is still considered the most likely diagnosis after other potential causes have been investigated and appear unlikely. In this case, a favourable response to antimigraine drugs may support the suspicion of an underlying migraine mechanism. However, apparent efficacy of a drug should not be regarded as a definite confirmation of the diagnosis, since spontaneous improvement, placebo response and additional drug effects (e.g. anxiolytic or antidepressant) have to be taken into account.
6.5 Findings on Clinical Examination
In most patients, the general neurologic and otologic examination is normal in the symptom-free interval [4]. Neuro-ophthalmological evaluation may reveal mild central ocular motor deficits such as persistent positional nystagmus and saccadic pursuit, particularly in patients with a long history of VM [7, 35, 36]. Interictal head-shaking nystagmus was observed in 50 % of VM patients [37]. In one study, patients with VM became nauseous after caloric testing four times more often than migraine patients with other vestibular disorders [38]. A neuro-otologic study of 20 patients during the acute phase of VM showed pathological nystagmus in 14 patients, mostly central spontaneous or positional nystagmus. Three patients had a peripheral type of spontaneous nystagmus and a unilateral deficit of the horizontal vestibuloocular reflex. Imbalance was observed in all patients except one [39]. Another study confirmed the high prevalence of persistent positional nystagmus, which was often horizontal and direction changing, but could also beat in the vertical or torsional plane [40].
Vestibular testing in the interval can be useful to reassure patient and doctor that there is no severe abnormality, such as a complete canal paresis which would rather suggest another diagnosis. MRI is required in patients presenting with central abnormalities and no previous history of similar attacks. Audiometry helps to differentiate VM from Menière’s disease. In clinical practice, history will usually provide more clues for the diagnosis than vestibular testing, since there are no abnormalities which are specific for VM. Therefore, in patients with a clear-cut history, no additional vestibular tests are required (for details on vestibular testing abnormalities, see Chap. 7 in this volume).
6.6 Differential Diagnosis
The differential diagnosis of vestibular migraine includes other disorders causing spontaneous and positional vertigo. Again, history taking provides more valuable clues than technical procedures, which rather serve to provide further evidence for or against a clinical working diagnosis.
6.6.1 Menière’s Disease
The interrelation of migraine with Menière’s disease may cause particular diagnostic problems. Migraine is more common in patients with Menière’s disease than in healthy controls [41]. Patients with features of both Menière’s disease and vestibular migraine have been repeatedly reported [41, 42]. In fact, migraine and Menière’s disease can be inherited as a symptom cluster [43]. Fluctuating hearing loss, tinnitus and aural pressure may occur in vestibular migraine, but hearing loss does not progress to profound levels [6, 44]. Similarly, migraine headaches, photophobia and even migraine auras are common during Menière’s attacks [41, 45]. The pathophysiological relationship between vestibular migraine and Menière’s disease remains uncertain. In the first year after onset of symptoms, differentiation of vestibular migraine from Menière’s disease may be challenging, as Menière’s disease can be monosymptomatic with vestibular symptoms only in the early stages of the disease. When the criteria for Menière’s disease [46] are met, particularly hearing loss as documented by audiometry, Menière’s disease should be diagnosed, even if migraine symptoms occur during the vestibular attacks. Only patients who have two different types of attacks, one fulfilling the criteria for vestibular migraine and the other for Menière’s disease, should be diagnosed with the two disorders. A future classification of VM may include a vestibular migraine/Menière’s disease overlap syndrome [34].
6.6.2 Benign Paroxysmal Positional Vertigo (BPPV)
VM may present with purely positional vertigo, thus mimicking BPPV. Direct nystagmus observation during the acute phase may be required for differentiation. In vestibular migraine, positional nystagmus is usually persistent and not aligned with a single semicircular canal. Symptomatic episodes tend to be shorter with vestibular migraine (minutes to days rather than weeks) and more frequent (several times per year with VM rather than once every few years with BPPV) [25].
6.6.3 Transient Ischemic Attacks (TIAs)
A differential diagnosis of vertebrobasilar TIAs must be considered particularly in elderly patients. Suggestive features include vascular risk factors, coronary or peripheral atherosclerosis, sudden onset of symptoms, total history of attacks of less than 1 year and angiographic or Doppler ultrasound evidence for vascular pathology in the vertebral or proximal basilar artery.
6.6.4 Vestibular Paroxysmia
Vestibular paroxysmia is a controversial disorder, presumably caused by vascular compression of the vestibular nerve. The presenting feature is brief attacks of vertigo, lasting from one to several seconds, which recur many times per day. Successful prevention of attacks with carbamazepine supports the diagnosis.
6.6.5 Psychiatric Dizziness Syndromes
Anxiety and depression may cause dizziness and likewise complicate a vestibular disorder. Anxiety-related dizziness is characterized by situational provocation, intense autonomic activation, catastrophic thinking and avoidance behaviour. More than 50 % of patients with VM have comorbid psychiatric disorders [47].
References
Liveing E (1873) On megrim: sick headache and some allied health disorders: a contribution to the pathology of nerve storms. Churchill, London, pp 129–148
Kayan A, Hood JD (1984) Neuro-otological manifestations of migraine. Brain 107:1123–1142
Behan PO, Carlin J (1982) Benign recurrent vertigo. Raven, New York
Cutrer FM, Baloh RW (1992) Migraine-associated dizziness. Headache 32:300–304
Cass SP, Ankerstjerne JKP, Yetiser S, Furman JM, Balaban C, Aydogan B (1997) Migraine-related vestibulopathy. Ann Otol Rhinol Laryngol 106:182–189
Johnson GD (1998) Medical management of migraine-related dizziness and vertigo. Laryngoscope 108:1–28
Dieterich M, Brandt T (1999) Episodic vertigo related to migraine (90 cases): vestibular migraine? J Neurol 246:883–892
Neuhauser H, Leopold M, von Brevern M, Arnold G, Lempert T (2001) The interrelations of migraine, vertigo, and migrainous vertigo. Neurology 56:436–441
Reploeg MD, Goebel JA (2002) Migraine-associated dizziness: patient characteristics and management options. Otol Neurotol 23:364–371
Brandt T, Strupp M (2006) Migraine and vertigo: classification, clinical features, and special treatment considerations. Headache Currents 3:12–19
Lempert T, Olesen J, Furman J et al (2012) Vestibular migraine: diagnostic criteria. Consensus document of the Bárány Society and the International Headache Society. J Vestib Res 22:167–172
International Headache Society Classification Subcommittee (2004) International classification of headache disorders. 2nd edition. Cephalalgia 24(Suppl 1):1–160
Sturzenegger MH, Meienberg O (1985) Basilar artery migraine: a follow-up study of 82 cases. Headache 25:408–415
Headache Classification Subcommittee of the International Headache Society (2013) The international classification of headache disorders: 3rd edition. Cephalalgia 33:629–808
Bisdorff A, von Brevern M, Lempert T, Newman-Toker DE (2009) Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res 19:1–13
Versino M, Sances G, Anghileri E et al (2003) Dizziness and migraine: a causal relationship? Funct Neurol 18:97–101
Murdin L, Davies RA, Bronstein AM (2009) Vertigo as a migraine trigger. Neurology 73:638–642
Neuhauser HK, Radtke A, von Brevern M et al (2006) Migrainous vertigo. Prevalence and impact on quality of life. Neurology 67:1028–1033
Hsu LC, Wang SJ, Fuh JL (2011) Prevalence and impact of migrainous vertigo in midlife women. A community-based study. Cephalalgia 31:77–83
Geser R, Straumann D (2012) Referral and final diagnoses of patients assessed in an academic vertigo center. Front Neurol 3:Article 169. www.frontiersin.org
Oh AK, Lee H, Jen JC, Baloh RW (2001) Familial benign recurrent vertigo. Am J Med Genet 100:287–291
Basser LS (1964) Benign paroxysmal vertigo of childhood (a variety of vestibular neuronitis). Brain 87:141–152
Krams B, Echenne B, Leydet J, Rivier F, Roubertie A (2011) Benign paroxysmal vertigo of childhood: long-term outcome. Cephalalgia 31:439–443
Abu-Arafeh I, Russell G (1995) Paroxysmal vertigo as a migraine equivalent in children: a population-based study. Cephalalgia 15:22–25
von Brevern M, Radtke A, Clarke AH, Lempert T (2004) Migrainous vertigo presenting as episodic positional vertigo. Neurology 62:469–472
Kuritzky A, Ziegler DK, Hassanein R (1981) Vertigo, motion sickness and migraine. Headache 21:227–231
Waterston J (2004) Chronic migrainous vertigo. J Clin Neurosci 11:384–388
Jeong SH, Oh SY, Kim HJ et al (2010) Vestibular dysfunction in migraine: effects of associated vertigo and motion sickness. J Neurol 257:905–912
Boldingh MI, Ljostadt U, Mygland A, Monstad P (2011) Vestibular sensitivity in vestibular migraine: VEMPs and motion sickness susceptibility. Cephalalgia 31:1211–1219
Eckhardt-Henn A, Best C, Bense S, Breuer P, Diener G, Tschan R, Dieterich M (2008) Psychiatric comorbidity in different organic vertigo syndromes. J Neurol 255:420–428
Furman JM, Balaban CD, Jacab RG, Marcus DA (2005) Migraine-anxiety related dizziness (MARD): a new disorder? J Neurol Neurosurg Psychiatry 76:1–8
Yacovino DA, Hain TC (2013) Clinical characteristics of cervicogenic-related dizziness and vertigo. Semin Neurol 33:244–255
Parker W (1991) Migraine and the vestibular system in adults. Am J Otol 12:25–34
Neff BA, Staab JP, Eggers SD et al (2012) Auditory and vestibular symptoms and chronic subjective dizziness in patients with Ménière’s disease, vestibular migraine and Ménière’s disease with concomitant vestibular migraine. Otol Neurotol 33:1235–1244
Radtke A, von Brevern M, Neuhauser H, Hottenrott T, Lempert T (2012) Vestibular migraine: long-term follow-up of clinical symptoms and vestibulo-cochlear findings. Neurology 79:1607–1614
Neugebauer H, Adrion C, Glaser M, Strupp M (2013) Long-term changes of central ocular motor signs in patients with vestibular migraine. Eur Neurol 69:102–107
Shin JE, Kim CH, Park HJ (2013) Vestibular abnormality in patients with Meniere disease and migrainous vertigo. Acta Otolaryngol 133:154–158
Vitkovic J, Paine M, Rance G (2008) Neuro-otological findings in patients with migraine- and nonmigraine-related dizziness. Audiol Neurootol 13:113–122
von Brevern M, Zeise D, Neuhauser H, Clarke AH, Lempert T (2005) Acute migrainous vertigo: clinical and oculographic findings. Brain 128:365–374
Polensek SH, Tusa RJ (2009) Nystagmus during attacks of vestibular migraine: an aid in diagnosis. Audiol Neurootol 15:241–246
Radtke A, Lempert T, Gresty MA, Brookes GB, Bronstein AM, Neuhauser H (2002) Migraine and Menière’s disease: is there a link? Neurology 59:1700–1704
Cha YH, Brodsky J, Ishiyama G, Sabatti C, Baloh RW (2007) The relevance of migraine in patients with Meńière’s disease. Acta Otolaryngol 127:1241–1245
Cha YH, Kane MJ, Baloh RW (2008) Familial clustering of migraine, episodic vertigo, and Ménière’s disease. Otol Neurotol 29:93–96
Radtke A, Neuhauser H, von Brevern M, Hottenrott T, Lempert T (2011) Vestibular migraine – validity of clinical diagnostic criteria. Cephalalgia 31:906–913
Brantberg K, Baloh RW (2011) Similarity of vertigo attacks due to Meniere’s disease and benign recurrent vertigo both with and without migraine. Acta Otolaryngol 131:722–727
American Academy of Otolaryngology - Head and Neck Foundation (1995) Committee on hearing and equilibrium: guidelines for the diagnosis and evaluation of therapy in Menière’s disease. Otolaryngol Head Neck Surg 113:181–185
Best C, Tschan R, Eckhardt-Henn A, Dieterich M (2009) Who is at risk for ongoing dizziness and psychological strain after a vestibular disorder? Neuroscience 164:1579–1587
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Lempert, T. (2014). Vestibular Migraine: Classification and Clinical Features. In: Colombo, B., Teggi, R. (eds) Vestibular Migraine and Related Syndromes. Springer, Cham. https://doi.org/10.1007/978-3-319-07022-3_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-07022-3_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-07021-6
Online ISBN: 978-3-319-07022-3
eBook Packages: MedicineMedicine (R0)