
Abstract
Central neuraxial techniques are among the most reliable regional anesthesia techniques at the disposal of the anesthesiologist. Although they are relatively simple to perform, a thorough knowledge of underlying neuraxial anatomy and factors determining the spread and duration of anesthesia is critical to their success. Also, an understanding of the physiological effects and potential complications of these neuraxial techniques is paramount to ensure safe application of these methods.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Central neuraxial techniques are among the most reliable regional anesthesia techniques at the disposal of the anesthesiologist. Although they are relatively simple to perform, a thorough knowledge of underlying neuraxial anatomy and factors determining the spread and duration of anesthesia is critical to their success. Also, an understanding of the physiological effects and potential complications of these neuraxial techniques is paramount to ensure safe application of these methods.
Subarachnoid block or spinal anesthesia is the administration of an appropriate dose of local anesthetic into the cerebrospinal fluid and the subarachnoid space, which results in rapid onset of dense sensory and motor block that is suitable for surgical anesthesia. Epidural anesthesia, on the other hand, involves instillation of local anesthetic into the fat-filled epidural space and results in slower onset and a less-dense sensory and motor block, which is most often used to provide analgesia rather than surgical anesthesia. Spinal anesthesia is generally only performed at the lower lumbar intervertebral levels in order to avoid spinal cord injury; epidural anesthesia may however be performed at the lumbar, thoracic, or cervical levels depending upon the desired area of sensory blockade.
Applied Anatomy
A thorough, three-dimensional knowledge of spinal anatomy, including the vertebral column, the vertebral curves, the spinal ligaments, the meninges, and the spinal cord, is essential for performing spinal and epidural anesthesia and is particularly helpful when technical difficulty is encountered. The concept of spinal cord segments, the segmental spinal nerves, and respective dermatomes is also important in understanding the physiological effects of neuraxial techniques.
Surface Anatomy
Surface landmarks are generally used to locate a particular vertebral level. These include the vertebra prominens which is the spinous process of the C7 vertebra, the root of the spine of the scapula corresponding to the T3 vertebra, and the inferior angle of the scapula corresponding to the T7 vertebra. The inferior margin of the 12th rib lies at the level of the L1 vertebra, Tuffier’s line (the line connecting the iliac crests) crosses the vertebral column at the level of the L4 vertebra, while the posterior superior iliac spine lies at level with S2 (Fig. 41.1a, b) [1, 2]. However, it is important to note that these are only estimations and various factors including normal anatomic variation, subcutaneous fat, and patient position can render these surface landmarks inaccurate in any given individual [3–5]. This may be overcome to some extent by the use of ultrasound which can improve the correct identification of intervertebral space levels [5–7].

(a) The common surface landmarks of the vertebral column. (b) The common surface landmarks of the vertebral column (With permission from Danilo Jankovic)
The spinous processes are angled caudally at the thoracic levels. However, they are nearly horizontal at cervical and lumbar levels (Fig. 41.2a–c) [8–10]. As a result, cranial angulation of the needle is required when performing a thoracic epidural, while needle insertion perpendicular to the skin usually suffices in the lumbar spine.

Cervical, thoracic, and lumbar spinous processes (With permission from Danilo Jankovic). (a) C7 cervical vertebra (vertebra prominens, nuchal tubercle). (b) T8 thoracic vertebra. (c) L3 lumbar vertebra
The kyphotic thoracic curve and the lordotic lumbar spine determine the spread of subarachnoid local anesthetic in a supine adult. An injection of hyperbaric local anesthetic placed at the height of the lumbar lordosis will spread both caudad and cephalad to a variable extent (Fig. 41.3a, b). The cephalad extent of this spread is limited by the pooling of the solution at the mid-thoracic concavity [11].

(a) Anatomy: cervical, thoracic, and lumbar spine (With permission from Danilo Jankovic). (b) Paramedian sagittal section. Cervical, thoracic, and lumbar spine (With permission from Danilo Jankovic)
The three meningeal layers cover the spinal cord and protect it. The dura mater (Fig. 41.4) is the outermost meningeal layer and extends from the base of the skull to the second sacral vertebra. It is thickest in the posterior midline and thinner in the lumbar area than the thoracic or cervical levels [12, 13]. The epidural space is superficial to this layer and is the target for epidural anesthesia. The subdural space lies deep to this layer but superficial to the arachnoid mater.

Meninges. (1) Spinal dura mater, (2) arachnoid mater, (3) pia mater, (4) spinal nerve, (5) dorsal (posterior) nerve root, (6) ventral (anterior) nerve root, and (7) internal vertebral venous plexus (With permission from Danilo Jankovic)
The arachnoid mater lies deep to the dura mater and encloses the subarachnoid space and the cerebrospinal fluid (Fig. 41.4). Both spinal cord and spinal nerve roots are exposed to cerebrospinal fluid and thus are the sites of action of local anesthetic deposited in the subarachnoid space during a spinal anesthetic. Cysts in the subarachnoid space have been reported and may be a potential cause of inadequate spinal anesthesia [14, 15].
The pia mater is the innermost meningeal layer and covers the spinal cord (Fig. 41.4). The pia mater extends to the tip of the spinal cord and continues as the filum terminale, anchoring the spinal cord to the sacrum.
A needle inserted in the midline will traverse the skin, subcutaneous tissue, supraspinous ligament, interspinous ligament, ligamentum flavum, epidural space, dura mater, subdural space, and arachnoid mater to access the subarachnoid space (Fig. 41.5a, b). A paramedian insertion of the needle, on the other hand, bypasses the supraspinous and interspinous ligaments and can be useful in the older patient with degenerative spine disease and narrowed interspinous spaces.

(a) Sagittal section of the vertebral column illustrating the ligaments of the spinal cord. (1) Supraspinous ligament, (2) interspinous ligament, (3) ligamentum flavum, (4) posterior longitudinal ligament, (5) intervertebral disc, and (6) anterior longitudinal ligament (With permission from Danilo Jankovic). (b) Transverse dissection at the level of T9. (1) Ligamentum flavum, (2) posterior epidural space with fat, (3) anterior epidural space with veins, (4) spinal dura mater, (5) subarachnoid space with spinal cord, (6) posterior longitudinal ligament, (7) anterior longitudinal ligament, (8) zygapophysial joint, (9) aorta, and (10) sympathetic ganglion (With permission from Danilo Jankovic)
The length of the spinal cord varies with age. In the fetus, the spinal cord extends to the end of the vertebral column. However, by birth, the terminal end of the cord, the conus medullaris, extends only until L3 due to a faster growth of the vertebrae than the spinal cord. In the majority of adults, the conus ends at L1. Spinal anesthetics must therefore be performed at the L2–L3 intervertebral space or lower to avoid the risk of spinal cord injury [16]. The portion of the spinal cord that gives rise to the dorsal nerve root, ventral nerve root, and paired spinal nerves is called the spinal cord segment. The area of the skin supplied by a given cord segment and its spinal nerve is termed a dermatome. Qualitative assessment of sensory changes within the dermatomes allows rapid estimation of the spread of the local anesthetic within the subarachnoid or epidural space and is used to assess and document the extent of spinal or epidural anesthesia. Table 41.1 lists the most clinically relevant dermatomal levels and their corresponding surface landmarks.
The ligamentum flavum and interspinous ligaments are not continuous (Fig. 41.5a). While the interspinous ligament extends from the spinous process above to the spinous process below, the ligamentum flavum extends from the lamina superior to a given intervertebral space to the lamina inferior to it. Failure of the left- and the right-sided ligamentum flavum to fuse in the midline has been described and may result in difficulty in localizing epidural space using a midline “loss-of-resistance” technique [17].
The epidural space is not a continuous space, but segmented along its length (Fig. 41.6) [18]. Cryomicrotome sectioning and imaging has shown that the various compartments of the epidural space are segmented by areas where the dura is directly fused with the bone. The lateral epidural compartment is divided by intervening pedicles which are in contact with the dura, while the posterior epidural compartment is divided by dural contact with bone beneath the cephalad half of each lamina. The anterior epidural compartment is divided by the attachment of the posterior longitudinal ligament to the intervertebral disc at each level. These posterior, lateral, and anterior compartments of the epidural space may impede the movement of injectate and may explain the unpredictable epidural drug spread that is occasionally seen [19].

Cross section of the epidural space. (1) Ligamentum flavum, (2) epidural space, (3) spinal ganglion, (4) spinous process, (5) body of vertebra, (6) dorsal branch of spinal nerve, and (7) ventral branch of spinal nerve (With permission from Danilo Jankovic)

Location of the procedure and required sensory spread of local anesthetic (With permission from Danilo Jankovic)
Epidural fat in the epidural space (see also Fig. 41.5b) may play an important role in the pharmacokinetics of epidurally administered lipophilic drugs by acting as a reservoir. This may result in a delayed onset and a longer duration of action [20, 21]. A reduction in the epidural fat with age may partly explain the age-related changes in epidural dose requirements [22].
The depth of the epidural space from the skin varies with body habitus, being less in a thin individual and more in an obese or pregnant individual [23, 24]. Ultrasound is a useful tool for measuring this depth and has been shown to correlate well with the actual depth [25].
Physiological Effects of Neuraxial Block
The physiological effects of both subarachnoid and an epidural block are quite similar. However, the effects of an epidural block have a slower onset and are usually segmental in nature, due to the segmental spread of local anesthetic in the epidural space. These effects are summarized below.
Neurological Blockade
The injection of local anesthetic within the intrathecal or epidural space produces nerve blockade. This blockade first affects the smaller-diameter sympathetic fibers, before the larger myelinated sensory–motor fibers [26, 27]. As a result, autonomic block manifests before sensory block, which in turn precedes the motor block. Among the sensory modalities, the sequence of blockade is temperature, pain, touch, pressure, and finally proprioception.
Block dissipation occurs in the reverse manner with autonomic fibers being the last to recover. In general, more dilute solutions affect the sensory fibers preferentially, while higher concentration is needed to block the motor fibers. Sensory block extends two to four segments higher than motor block, and the sympathetic block extends two to four segments higher than the sensory block. This is termed differential block [28].
Cardiovascular Effects
Blockade of the thoracolumbar sympathetic nerves manifests as the cardiovascular effects that follow a neuraxial block, including hypotension and bradycardia. These effects are in proportion to the extent of the block produced and may be exaggerated in a hypovolemic patient. Hypotension is a result of arteriolar vasodilatation and venous pooling which diminishes preload. Bradycardia is partially due to blockade of cardiac accelerator fibers (T1–T5) [29] but is more often a result of decreased preload which activates cardiac reflexes involving intracardiac stretch receptors [30]. The Bezold–Jarisch reflex in particular is often invoked as an explanation for severe bradycardia and asystole following spinal anesthesia in young healthy adults [31].
In general, the sympathetic block following a spinal anesthetic is more rapid and greater in extent compared to an epidural. Thus, a gradually dosed epidural may be useful in providing hemodynamic stability. Additionally, a high thoracic epidural block (T1–T4) provides coronary vasodilatation and reduces work of the myocardium by reducing afterload and reducing the heart rate [32]. However, this unopposed vagal tone has been thought to contribute to bradycardia, asystole, or laryngospasm [33, 34].
Respiratory Effects
In a patient with normal lung function, neuraxial blocks produce a clinically insignificant impact on respiratory function [35]. However, in high thoracic blockade or in a patient with preexisting respiratory compromise, this effect may be significant. The paralysis of abdominal and intercostal muscles negatively impacts expiratory function causing a reduction in peak expiratory flows, expiratory reserve volume, and maximal minute ventilation. This may manifest as dyspnea. However, these effects are negligible in comparison to the pain relief obtained following thoracic or abdominal surgery, and overall improvement in postoperative outcome and a reduction in postoperative pulmonary complications are observed [36].
Spread of the local anesthetics to cervical segments can affect inspiration by blocking the phrenic nerve and diaphragmatic function. Respiratory arrest following a total spinal may be due to medullary hypoperfusion rather than an effect of local anesthetics per se [35].
Gastrointestinal Function
The splanchnic blockade (T6–L2) produced following a neuraxial block leads to unopposed parasympathetic activity. This results in increased gastrointestinal secretions, increased intestinal motility, and relaxation of sphincters. This contracts the bowel and allows better access during abdominal surgery. Also, improved visceral perfusion due to vasodilation may improve healing and contribute to an earlier return of bowel function following surgery [37, 38].
Nausea and vomiting, if observed, are usually secondary to increased vagal tone and hypotension. A higher block (above T5), accompanying hypotension, use of opioids, and a history of motion sickness are risk factors for developing nausea and vomiting [39].
Genitourinary
Neuraxial anesthesia does not affect renal blood flow since it is autoregulated. Sacral blockade produces an atonic bladder and an increased bladder sphincter tone. This may result in urinary retention until the resolution of the block.
Thermoregulation
Redistribution of heat following sympathetic block results in mild hypothermia. This induces thermoregulatory vasoconstriction and shivering above the level of the neuraxial block [40]. Epidural fentanyl may be used to abolish shivering during anesthesia [41].
Neuroendocrinal Effects
Neuraxial block effectively blocks the afferent innervation from the surgical site and is responsible for the inhibition of the surgical stress response that involves release of a variety of mediators (including catecholamines, vasopressin, growth hormone, renin, angiotensin, glucose, antidiuretic hormone, and thyroid-stimulating hormone). This effect is greater for a lumbar epidural than a thoracic epidural [42]. The magnitude of the stress response correlates with postoperative morbidity, and thus, its attenuation should be of benefit [43].
Indications
Spinal Versus Epidural Anesthetic
Neuraxial techniques (spinal and epidural anesthesia) at the lumbar levels allow for a temporary blockade of nerve conduction in the autonomic, sensory, and the motor fibers. However, it is important to recognize differences between the two. These are summarized in Table 41.2.
Comparison to General Anesthesia
When compared to a general anesthetic, the central neuraxial techniques offer the following advantages:
-
Avoidance of airway manipulation
-
Avoidance of side effects of a general anesthetic (sore throat, nausea and vomiting, dental damage, malignant hyperthermia, aspiration of gastric contents, etc.)
-
Simple and reliable block
-
Predictable physiologic changes
-
Minimal metabolic disturbances (in hepatic or renal disease)
-
Preservation of consciousness
-
Extension into postoperative analgesia
When compared to general anesthesia, neuraxial techniques have been associated with a reduction in cardiovascular adverse events, perioperative pulmonary complications, thromboembolic events, preserved gastrointestinal motility, development of chronic pain, surgical stress response, immune dysfunction, and morbidity and mortality [44–48].
However, general anesthesia is advantageous over neuraxial block when better control over hemodynamics is desired (such as in severe or critical aortic stenosis). It offers definitive control of the airway and allows for immediate postoperative pain assessment.
Indications
The application of neuraxial anesthesia depends on the following factors:
-
The area of surgery
-
The type and expected duration of the procedure
-
The degree of muscle relaxation required
-
The presence of concomitant disease
-
The expected blood loss
The relevant indications for spinal and epidural anesthetic are considered in Table 41.3.
Contraindications
These are summarized in Table 41.4.
Coagulopathy, whether iatrogenic or idiopathic, is now considered a relative contraindication. According to the consensus statements by the American Society of Regional Anesthesia and Pain Medicine (2010), epidural block can be placed 4 h after the last dose of heparin. NSAIDs including aspirin are not a contraindication to epidural placement provided that catheter placement is uncomplicated (one or two attempts). LMWH should be held at least 12 h before placement of catheter and 2 h after its removal. Epidural placement is relatively safe with international normalized ratio (INR) <1.5. If an epidural vein is punctured, subcutaneous heparin administration should be held at least 2 h and LMWH held at least 24 h. GIIa/IIIb inhibitors should be withheld for at least 4 weeks after epidural placement. Epidural placement is best avoided for 7 days after clopidogrel and 14 days after ticlopidine. For a further review on the use of neuraxial techniques in anticoagulated patients, patients on antiplatelet drugs, or patients with coagulopathy, please refer to the “Executive summary: regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition)” [49].
Performing a Spinal Anesthetic
Before performing a spinal anesthetic, a full discussion of the risk–benefit and informed consent should take place.
Preparation and Materials
-
Check that the emergency equipment is complete and in working order (intubation kit, emergency drugs); sterile precautions, intravenous access, and anesthetic machine.
-
Start an intravenous infusion and ensure adequate volume loading (250–500 ml of a balanced electrolyte solution).
-
Vasopressors such as ephedrine, phenylephrine, or metaraminol should be readily available.
-
ECG, noninvasive blood pressure, and pulse oximetry monitoring are essential.
-
Skin prep using an alcohol, iodine, or chlorhexidine. Note that if chlorhexidine is used, extreme care must be taken to prevent its inadvertent introduction into the neuraxis, as it has been implicated in chemical arachnoiditis [50, 51].
-
Local anesthetic for skin infiltration and intrathecal injection.
-
Spinal needles (Fig. 41.8a–c) are commonly of the following two types:
Fig. 41.8 
(a–c) Spinal needles. (a) Pencil-point, 25 G. (b) Quincke tip, 27 G. (c) Atraucan Special Cut, 26 G (With permission from Danilo Jankovic)
-
25–27-G spinal needles with conical tip (pencil-point)—e.g., Sprotte, Pencan, and Whitacre—in current standard use. When the dura is penetrated with these needles, the dural fibers are separated and then closed together again. This reduces the risk of post-dural puncture headache [52, 53].
-
25–27-G spinal needles with Quincke tip. The needle bevel should be directed laterally during the puncture in order to pass through the dura in a longitudinal direction [54]. A 22-G needle may be used where increased stiffness is desired to facilitate needle redirection—e.g., in older patients with narrowed interlaminar spaces or when there are difficulties with positioning.
-

Patient Positioning
Optimal patient positioning during puncture and during the fixation phase of the local anesthetic is a prerequisite for successful spinal anesthesia. The following positions may be used:
-
Lateral decubitus position
-
Sitting
-
Prone
In all three positions, it is important to locate the midline and to follow it during the entire injection procedure. Lumbar lordosis must be minimized.
Lateral Decubitus Position
The assistant stands in front of the patient. If the anesthetist is right-handed, the patient is placed in the left lateral position. The patient is asked to adopt a hunchback position (legs flexed up against the abdomen and chin flexed down onto the chest) in order to flex the lumbar spine and allow optimal expansion of the intervertebral spaces. It is important here for the spine to be parallel and for the intercristal line and the line connecting the two scapular tips to be perpendicular to the operating table (Fig. 41.9).

Position: lateral decubitus (With permission from Danilo Jankovic)
Advantages
-
More comfortable for the patient and thus particularly suitable for frail patients (risk of collapse).
-
The reduction in blood pressure is less marked [55].
-
When hyperbaric solutions are used, unilateral anesthesia is more easily obtained.
-
Can be used in pregnant patients (since the lateral tilt or lateral decubitus position reduces the extent of aortocaval compression) [56].
Disadvantages
-
Difficulty may arise in the correct identification of the midline, especially if the pelvis is tilted too anteriorly.
Sitting Position
The patient is seated on the edge of the operating table and is supported by an assistant standing in front of him or her (Fig. 41.10). It may also be helpful to provide a padded Mayo stand, an adjustable table, or a similar device for the patient to lean on for additional support.

Position: sitting (With permission from Danilo Jankovic)
Advantages
-
When palpation of the spinous processes is difficult (e.g., in obese patients or those with spinal deformities), it is easier to locate the midline in the sitting position.
-
Facilitates the performance of a saddle block with hyperbaric local anesthetic when anesthesia in only the perineal or perianal region is required.
Disadvantages
-
This position may lead to orthostatic hypotension (and risk of collapse) and should be avoided in frail and heavily sedated patients [55].
-
More support and assistance may be required to keep patient upright.
Prone Jackknife
This position is only used in the very rarely practiced hypobaric technique for spinal anesthesia (procedures in the rectum, perineum, sacrum, lower spine) [57]. An assistant and subsequent repositioning of the patient are not required (Fig. 41.11).

Position: prone (“jackknife” position) (With permission from Danilo Jankovic)
Injection Technique
The subarachnoid space may be accessed using a midline approach, a paramedian approach, or a Taylor’s approach. These are discussed below.
Median Approach (Midline)
Landmarks
The injection is carried out in the midline below the L2 segment (conus medullaris), usually between the spinous processes of L2/L3 or L3/L4 (depending on the desired level of anesthesia). The patient is asked to draw the legs tightly up to the abdomen and to place the chin on the chest. A line is drawn from one iliac crest to the other. This connection (Tuffier’s line) crosses either the spinous process of L4 (50 %) or the intervertebral space of segments L4/L5. However, this palpatory method alone may be unreliable, and ultrasound may help to correctly identify the vertebral levels [7].
The spinous processes and intervertebral spaces are palpated to identify the midline, which is the important landmark. It is recommended that the index and middle fingers of the nondominant hand be used to palpate and identify the chosen interspace, as they can be subsequently used to fix the overlying skin, which is important for precision and accuracy in needle insertion (Fig. 41.12).

Palpation of the intervertebral space (With permission from Danilo Jankovic)
Strict Asepsis
Thorough, repeated, and wide skin prep and drying and covering of the injection site with a drape.
Local Anesthesia
The skin and supraspinous and interspinous ligaments are anesthetized with 1–1.5 ml of a local anesthetic (e.g., 1 % lignocaine). The injection is carried out between the spread index and middle fingers of the left hand (Fig. 41.13). In the patient with less-distinct surface landmarks, the local anesthetic needle may be used to explore the underlying anatomy. Bony contact at a relatively shallow depth indicates contact with the tip of the spinous process and the location of the midline. Firm resistance to further injection of local anesthetic indicates that the needle tip lies within the interspinous ligament in the midline and not in the paraspinous muscles on either side.

Local anesthesia (With permission from Danilo Jankovic)
Injection
Advancing the Introducer
Without moving the spread index and middle finger of the left hand away from the intervertebral space (which prevents inadvertent movement of the skin overlying the chosen interspace), the introducer is grasped between the thumb and index finger of the right hand and advanced parallel to the operating table and slightly cranially (10°) deep enough for it to sit firmly in the interspinous ligament (Fig. 41.14). It should be ensured that the midline position is maintained. After this, the introducer is fixed with the thumb and index finger of the left hand, with the dorsum of the hand lying firmly on the patient’s back.

Advancing the guiding cannula (With permission from Danilo Jankovic)
Introducing the Spinal Needle, Puncture of the Subarachnoid Space
The spinal needle, held between the thumb and index finger (or middle finger) of the right hand, is introduced through the interspinous ligament, ligamentum flavum, epidural space, and dura/arachnoid as far as the subarachnoid space. Penetration of the ligamentum flavum is usually evident by the “rubbery” resistance to needle advancement. A characteristic “dural click” may be felt when the subarachnoid space is reached; however, this does not always occur (Fig. 41.15). When a Quincke needle is used, it should be ensured that the needle bevel is directed laterally, so that the dura is punctured in a longitudinal direction.

Introducing the spinal needle. Puncture of subarachnoid space (With permission from Danilo Jankovic)
Removing the Stylet
The following may occur here:
-
CSF flows freely
The injection needle is advanced 1 mm and fixed between the thumb and index finger of the left hand, which is supported on the patient’s back. The desired amount of local anesthetic can now be injected (Figs. 41.16 and 41.17a, b).
Fig. 41.16 
Removing the stylet. Subarachnoid injection (With permission from Danilo Jankovic)
Fig. 41.17 
(a) Subarachnoid position of the needle (With permission from Danilo Jankovic). (b) Transverse dissection at the level of L4/L5. (1) Posterior epidural space with fat, (2) anterior epidural space with veins, (3) spinal dura mater, (4) subarachnoid space and cauda equina, (5) zygapophysial joint, (6) anterior longitudinal ligament, and (7) posterior longitudinal ligament (With permission from Danilo Jankovic)
With the single-injection technique, aspiration of CSF (0.1 ml) should be attempted immediately before and after injection of local anesthetic. The subarachnoid injection is made at the rate of 1 ml per 5 s.
-
Blood in the CSF
Slightly bloody CSF which clears quickly (spontaneously or after aspiration) usually occurs after penetration of an epidural vein on the way into the subarachnoid space. The local anesthetic can be injected.
However, backflow of frank blood indicates that the injection needle is likely positioned within a vein. A new attempt at puncture must be made and possibly in a different intervertebral space.
-
No CSF flow
Rotation of the needle to all four quadrants and careful aspiration may help. The needle may also be advanced slightly with the stylet in place.
If no CSF flows in spite of all these measures, the needle should be removed and the procedure repeated with a different needle direction or at a different interspace.
Unexpectedly deep bone contact suggests that the posterior side of the vertebra or an intervertebral disc has been reached. CSF appears in most cases after the needle has been slightly withdrawn and aspiration has been repeated.
-
Pain or paresthesias during puncture
Pain or paresthesia prior to entry into the epidural or intrathecal space is most often due to needle contact with the facet joint, which forms the lateral border of the interlaminar space. The needle should be directed slightly more medially, away from the side on which the pain or paresthesia occurred. It is not uncommon for a transient paresthesia radiating down one leg to occur upon needle entry into the intrathecal space; this signals contact with the cauda equina. If it persists, the needle must be withdrawn slightly or repositioned. When paresthesias occur during the injection, the needle must be repositioned before any further drug is injected.
The local anesthetic must never be injected without evidence of CSF! The location and distribution of paresthesias arising during the puncture procedure must be recorded.
Experience shows that failure is usually due to deviation of the needle from the midline or excessive cranial angulation of the needle.


Paramedian Approach (Lateral, Paraspinal)
In this technique (Figs. 41.18 and 41.20), the supraspinous and interspinous ligaments are avoided, so that the ligamentum flavum is the primary target on the way to the subarachnoid space.

Paramedian approach (With permission from Danilo Jankovic)

Taylor’s approach (With permission from Danilo Jankovic)

Puncture of the subarachnoid space: (1) median, (2) paramedian, (3) Taylor (With permission from Danilo Jankovic)
Procedure
This technique can be used in all the patient positions mentioned above. Flexion of the spine is not essential. The caudal edge of the spinous process is marked. The injection site is located 1–1.5 cm lateral and caudal to this. The puncture is carried out in a cranio-medial direction, at an angle of about 10–15°. The dura is reached after about 4–6 cm. Most mistakes arise when the needle is angled too cranially or when the needle entry point is too lateral.
This technique can be used in:
-
Degenerative changes in the spine
-
Older patients with marked calcification of the supraspinous and interspinous ligaments [58]
-
Obesity
-
Fractures or other pathological conditions in which pain makes it impossible to flex the spine
Taylor’s Approach
This lumbosacral approach (Figs. 41.19 and 41.20) is a paramedian injection via the intervertebral space of L5 and S1, the largest interlaminar space in the spinal region.
Procedure
The injection site is located about 1 cm medial and about 1 cm caudal to the posterior superior iliac crest. The injection needle is advanced in a cranio-medial direction and at an angle of about 55°. If it touches the periosteum (sacrum), the needle must be withdrawn and its direction must be corrected.
The indications for this access route include procedures in the perineal and perianal region, as spread to the higher spinal levels may not always reliably occur.
Unilateral Spinal Anesthesia
Unilateral spinal anesthesia is intended to block only the anterior and posterior spinal nerve roots on the side being operated on, while the contralateral side—and particularly its sympathetic fibers—remains unblocked. This leads to a reduced incidence of hypotension.
Indications
-
Surgical and orthopedic procedures on the lower extremities
Procedure
-
Patient positioning: lateral decubitus position, lying on the side that is to be operated on.
-
Injection technique: this is the same as for conventional spinal anesthesia. The opening of the pencil-point needle is rotated to the operating side, and the desired amount of local anesthetic is slowly injected [59]. A hyperbaric solution of local anesthetic such as bupivacaine should always be used for maximum effectiveness.
-
Patient position after the injection: the patient remains lying on the side that is to be operated on for about 20 min.
Advantages
-
Reduction in the extent of the sympathetic block (by about 70 %), since smaller volumes and slower injection of the local anesthetic mean that fewer spinal segments are involved [60]
-
Hemodynamic stability (hypotension is only observed in 5 % of patients)
-
Faster recovery from anesthesia
-
Suitable for outpatient procedures [61]
-
Greater acceptance by patients
Disadvantage
-
Strict unilateral anesthesia is only achieved if adequate time is allowed for the local anesthetic to settle on the operative side. However, a differential block of some degree can almost always be achieved.
Continuous Spinal Anesthesia
The insertion of a catheter into the subarachnoid space allows a continuous or repeated intermittent dosing of local anesthetic.
Indications
-
Lower abdominal and lower limb surgery in elderly patients and high-risk patients [62]
-
Postoperative pain relief
-
Chronic pain relief (in cancer patients)
Procedure
-
The procedure is similar to a standard spinal anesthetic. However, usually a 20–22-G spinal needle is used to gain access to the subarachnoid space, and a 25–27-G catheter is threaded (usually 2–3 cm) into the subarachnoid space (Fig. 41.21).
Fig. 41.21 
Introducing the catheter in the subarachnoid space (With permission from Danilo Jankovic)

Advantages
-
A smaller initial dose of local anesthetic can be injected without concern about inadequate block height or duration. This helps prevent hypotension due to excessive sympathetic block caused by large doses or greater spread of local anesthetic [62].
-
Ability to prolong spinal anesthetic as needed.
Disadvantages
-
Higher risk of post-dural puncture headache in younger population [63].
-
Use of small micro-catheters (less than 24 G) may predispose to sacral pooling of local anesthetic leading to cauda equina syndrome and is therefore not recommended [64].
Management of the Patient After Intrathecal Injection
Patient Positioning
The level of the anesthetic spread is controlled by patient positioning measures and checked with cold tests at intervals of 2–5 min.
Hyperbaric Spinal Anesthesia
-
Lateral decubitus position: the patient remains on the side of surgery for 10–15 min if unilateral anesthesia is desired. The patient is laid supine if bilateral anesthesia is required.
-
Sitting position: the patient is immediately laid supine to allow the anesthetic to spread cephalad. The patient remains sitting if sacral spread is desired.
Hypobaric Technique
-
Hypobaric spinal anesthesia is ideal for perineal and perirectal surgeries requiring a prone “jackknife” position, so that the patient does not need to be repositioned (Fig. 41.11).
-
The hypobaric technique has also gained popularity in major hip surgery, which is performed in the lateral position. Thus, repositioning of the patient is often not needed when the spinal is placed in the lateral decubitus position, with the operative side nondependent. Compared to isobaric bupivacaine, a hypobaric solution demonstrated a significant delayed block recession and time until analgesia, for total hip arthroplasty [65].
Isobaric Spinal Anesthesia
-
Horizontal positioning is adequate; other positions have no significant influence on the spread of the anesthesia.
Fixation Phase
-
The phase immediately after injection of the local anesthetic is particularly critical and requires precise monitoring. The fixation phase lasts about 10–15 min.
Patient Monitoring
-
Sympathetic block following a spinal anesthetic results in a drop in the blood pressure and heart rate. This may be profound in elderly and volume-depleted patients. Bradycardia may occur after the peak of sympathetic block is achieved (30–60 min after spinal injection) due to the blockade of cardiac accelerator fibers. Unexpected bradycardia and cardiac arrest may occur in young healthy patients [66]. Thus, frequent monitoring of the vitals (heart rate, blood pressure, and oxygen saturation) is advocated during and after the conduct of a spinal anesthetic.
-
Supplemental oxygen administration is recommended after a spinal anesthetic, especially if sedation is used for patient comfort.
-
End-tidal carbon dioxide monitoring is also used to monitor the respiratory rate.
-
Postoperatively, the patient should be monitored until the effects of spinal anesthetic have receded.
Block Assessment
-
Injecting a local anesthetic into the subarachnoid space blocks autonomic, sensory, and motor function. The main targets of local anesthesia are the posterior roots with the ganglia, the anterior roots of the spinal nerves, the autonomic nerve fibers, and mixed neural trunks.
-
The spread of the anesthesia should be checked at short intervals (2–5 min) and confirmed (with a cold spray or pinprick) shortly before the start of the operation [67, 68]. The first sign of an effect on the spinal nerve roots is a subjective sensation of warmth in the feet. The further development of the block encompasses touch, deep pressure, motor function, vibration sensitivity, and positional sense.
-
Motor function is completely blocked at the site of the greatest concentration of the local anesthetic. Sensory block extends two to four segments higher than motor block, and the sympathetic block extends for a further two to four segments higher than the sensory block.
-
Resolution of the block is marked by a return of motor function, followed by the sensory modalities. The autonomic function is the last to recover [28].
Performing an Epidural Anesthetic
Preparation and Materials
Preparation for an epidural anesthetic is similar to that for a spinal block. This has already been discussed in Sect. Patient Positioning.
Epidural needles: The epidural needles required to perform an epidural block are generally larger in gauge than spinal needles. Additionally, they may have distinct tip design to facilitate entry into the epidural space and introduction of the catheter. Some of these are already discussed in Sect. Patient Positioning. Of these, Tuohy-tip epidural needles are most commonly used.

(a–d) Epidural needles. (a) Tuohy, (b) Hustead, (c) Crawford, (d) Weiss (With permission from Danilo Jankovic)
Positioning of the Patient
An epidural block can be performed with the patient in lateral decubitus or sitting position. While the former is commonly used in obstetric patients, the latter is preferred in other patient groups. Prone position is rarely used. The pros and cons of these positions have been already discussed on p. 514 (Patient Positioning).
Performing a Lumbar Epidural
Lumbar epidural space may be accessed using a midline approach which is most commonly used or using a paramedian approach. These are discussed below.
Midline Approach
Landmarks
The injection is carried out in the midline below the L2 segment (conus medullaris) (Fig. 41.23a, b), usually between the spinous processes of L2/L3 or L3/L4. The intervertebral space is palpated, and the midline is located to serve as the most important signpost. In the midline, the ligamentum flavum is at its thickest, the epidural space is widest, and the blood vessels are at their smallest [69].

(a) Conus medullaris (lower edge of the first lumbar vertebra). (1) Conus medullaris, (2) cauda equina, (3) dural sac, (4) L1 segment (With permission from Danilo Jankovic). (b) Cauda equina at the level of L2–L5. Paramedian sagittal section. (1) Spinal dura mater, (2) epidural space (With permission from Danilo Jankovic)
Strict Asepsis
Thorough, repeated, and wide skin prep is done. After drying, the injection site is covered using a sterile drape.
Local Anesthesia
The skin and supraspinous and interspinous ligaments are anesthetized with 1–1.5 ml of a local anesthetic (e.g., 1 % lignocaine). The injection is carried out between the spread index and middle fingers of the left hand (Fig. 41.24).

Local anesthesia (With permission from Danilo Jankovic)
Needle Insertion
Without moving the spread index and middle fingers of the left hand from the intervertebral space, an epidural needle is fixed between the thumb of the right hand (hub) and the index and middle finger (shaft) and advanced through the skin (Fig. 41.25). After passing the supraspinous ligament, which is about 1-cm thick, the needle, with its bevel directed cephalad or caudad, is slowly advanced a further 2–3 cm (depending on the anatomy), until it rests firmly in the interspinous ligament. This often results in a “gritty” sensation. The trocar is removed and a low-friction (loss of resistance) syringe is attached (Fig. 41.26).

Introducing the epidural needle (With permission from Danilo Jankovic)

Removing the stylet and attaching a low-friction syringe (With permission from Danilo Jankovic)
Care should be taken to ensure that the needle is kept in the midline. Inadvertent deviation from the midline leads to the needle passing the supraspinous ligament, with an angled entry into the interspinous ligament with only brief resistance and a subsequent false loss of resistance. This type of puncture ends in the paravertebral musculature and is accompanied by local pain.
After passing the interspinous ligament, the needle must be advanced carefully, millimeter by millimeter, in the direction of the ligamentum flavum.
Puncturing the Epidural Space
The thumb and index finger of the left hand, which is resting with the back of the hand firmly against the patient’s back, secure the needle, advance it millimeter by millimeter, and at the same time serve as a “brake” to prevent inadvertent forward movement. The thumb of the right hand applies pressure on the syringe plunger. Loss of resistance indicates that the epidural space has been reached. The contents of the syringe are easily injected.
Identification of the epidural space is carried out using the loss-of-resistance technique (Fig. 41.27). The following variations on this technique can be applied:

Identifying the epidural space (loss of resistance) (With permission from Danilo Jankovic)
-
(a)
Saline with an air bubble: after the interspinous ligament has been reached, the stylet is removed, and a low-friction syringe filled with a saline solution and with a small air bubble in it, serving as a visual indicator, is attached. When the ligamentum flavum is encountered, the air bubble is compressed by pressure on the syringe plunger (Fig. 41.28a); when the epidural space is reached, the bubble returns to its normal, larger shape (Fig. 41.28b). This technique is the most common choice as it provides a good identification of the epidural space and an idea of the force being applied (by the compression of the air bubble).
Fig. 41.28 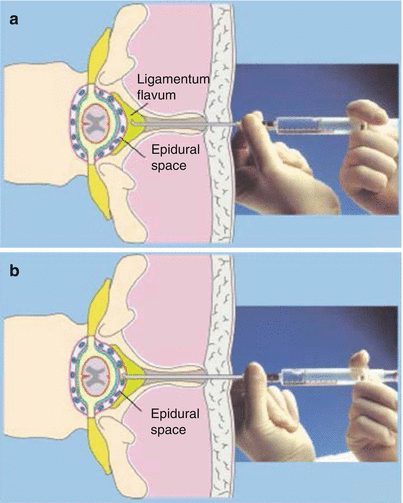
(a) Loss-of-resistance technique with saline. The air bubble is compressed by pressure on the syringe plunger (With permission from Danilo Jankovic). (b) Loss-of-resistance technique with saline. The epidural space has been reached. The air bubble has returned to its normal, loose shape (With permission from Danilo Jankovic)
-
(b)
Saline-only technique: since the introduction of air in the epidural space may lead to “patchy” block, some clinicians prefer to use only saline. The disadvantage of doing so is the inability to objectively judge the amount of force being applied on the plunger.
-
(c)
Air-only technique: this technique allows for a more subjective “feel” while identifying the epidural space. It also allows clearer identification of an accidental dural puncture as any fluid that emerges from the hub of the needle must be CSF. However, using air to locate epidural space has been associated with patchy blocks, venous air embolism, and pneumocephalus [70].
-
(d)
Hanging drop technique: in this technique, after the interspinous ligament has been reached, a drop of saline is placed within the hub of the needle (Fig. 41.29a). After the ligamentum flavum has been passed and the epidural space has been reached, the drop is “sucked in” due to the negative pressure in the epidural space (Fig. 41.29b) [71].
Fig. 41.29 
(a) “Hanging drop” technique. The epidural needle is positioned in the ligamentum flavum (With permission from Danilo Jankovic). (b) “Hanging drop” technique. The epidural space has been reached. The drop is sucked back in (With permission from Danilo Jankovic)


Aspiration and Injection of a Test Dose
Having reached the epidural space, a careful aspiration is carried out to detect CSF or blood while the needle continues to be secured by the thumb and index finger of the left hand, resting with the back of the hand firmly against the patient’s back (Fig. 41.30).

Aspiration test (With permission from Danilo Jankovic)
After a negative aspiration, a test dose of 3–4 ml of local anesthetic (usually 1.5 % lignocaine) and 15 mcg epinephrine can be injected. This allows detection of intrathecal injection (rapid development of spinal block) or intravascular injection (tachycardia).
The addition of epinephrine can lead to unreliable results in patients taking beta-blockers, patients under general anesthesia, and pregnant patients. Due caution must be exercised while adding epinephrine in pregnant patients (may cause transient fetal bradycardia due to reduced uterine blood flow), older patients with coronary artery disease, and hypertensive patients. The use of epinephrine is best avoided in patients with closed-angle glaucoma and tachyarrhythmia [72].
Maintaining constant verbal contact with the patient and careful cardiovascular monitoring after a test dose is recommended. If all is well, a further dose of the local anesthetic can be injected.
Drug Administration
The epidural injection may be performed as a single-shot injection or as a catheter technique (allowing further dosing).
-
(a)
Single-injection technique: incremental administration of a local anesthetic is carried out in aliquots of 3–5 ml, waiting 15–20 s between each dose, with intermittent aspiration (Fig. 41.31). After aspiration has been repeated shortly before the end of the injection, the needle is withdrawn and the patient is placed in the desired position.
Fig. 41.31 
Incremental injection of local anesthetic (With permission from Danilo Jankovic)
-
(b)
Catheter technique: upon confirmation of the epidural space and negative aspiration, a catheter may be introduced. For this, the thumb and index finger of the left hand secure the epidural needle, with the back of the hand lying firmly on the patient’s back. The catheter is advanced cranially, using the thumb and index finger of the right hand, to a maximum of 3–4 cm beyond the tip of the needle (Fig. 41.32). Advancing it further than this can lead to lateral deviation of the catheter, with accompanying paresthesias. After placement of the catheter in the desired position, the needle is slowly withdrawn (Fig. 41.33), while at the same time the thumb and index finger of the left hand secure the catheter at the injection site (Fig. 41.34).
Fig. 41.32 
Introducing the catheter (With permission from Danilo Jankovic)
Fig. 41.33 
Withdrawing the injection needle (With permission from Danilo Jankovic)
Fig. 41.34 
The catheter is secured at the injection site with the thumb and index finger (With permission from Danilo Jankovic)




An adapter is attached to the end of the catheter. The patency of the catheter is tested by injecting 1–2-ml saline (Fig. 41.35). After aspiration, the syringe is disconnected, and the open end of the catheter is placed on a sterile drape below the puncture site. Attention must be given to any escaping fluid (CSF or blood) (Fig. 41.36). A bacterial filter is then attached (Fig. 41.37), and the catheter is secured and dressed to prevent dislodgement and ensure sterility (Fig. 41.38). Fixation of the catheter can be accomplished in a variety of ways, including skin suture or proprietary dressings.

Injection of 1 ml saline (With permission from Danilo Jankovic)

The end of the catheter is placed below the injection site (With permission from Danilo Jankovic)

Placing a bacterial filter (With permission from Danilo Jankovic)

Securing the catheter and dressing (With permission from Danilo Jankovic)
The patient is placed in the desired position and a test dose is administered, as with the single-shot injection. During the waiting period, it is important to maintain verbal contact with the patient and to check the spread of the anesthesia, to exclude the ever-present risk of inadvertent intrathecal injection. After 5 min, the remainder of the dose, adjusted for the individual patient, can be administered on an incremental basis (max. 5 ml each injection) until the desired level of anesthesia is reached.
Troubleshooting
-
(a)
Escaping fluid: after the epidural space has been identified or after administration of the test dose, a few drops of fluid may still drip from the positioned needle. This may be saline from the syringe or CSF if intrathecal space has been punctured. A higher viscosity, higher temperature (Fig. 41.39), near-neutral pH, higher glucose content, and turbidity with thiopentone help identify the fluid as CSF [73]. If the fluid is not CSF, one can proceed with the procedure.
Fig. 41.39 
Escaping fluid: is it cold or warm? (With permission from Danilo Jankovic)
-
(b)
Escaping blood: in this case (Fig. 41.40), it is best to withdraw the needle or the catheter. One may attempt another insertion at a segment higher or lower or abandon the procedure and choose to administer general anesthesia.
Fig. 41.40 
Blood-tinged fluid (With permission from Danilo Jankovic)
-
(c)
Escaping CSF: the options in the event of accidental dural puncture include conversion to a spinal anesthetic by injecting an appropriately reduced dose of local anesthetic or inserting a continuous spinal catheter (this must clearly be labeled as such, to avoid inadvertent overdosing with subsequent top-ups). Another attempt at insertion can also be made keeping in mind the possibility of another dural tap and that an epidural dose of local anesthetic may spread intrathecally through the first dural puncture site and lead to total spinal anesthesia. Finally, one may choose to abandon the procedure and administer general anesthesia. In any case, the patients must be informed about the possibility of post-dural puncture headache.
-
(d)
Inability to thread the catheter: this may happen when a false loss of resistance has been encountered in a superficial tissue plane. Injection of local anesthetic at this point will not be effective. Reattempting the injection is the best course, aiming to obtain a convincing loss of resistance.


Paramedian Approach
This technique, which is independent of lumbar lordosis or the ability of the spine to flex, avoids puncture of the supraspinous ligament and the frequently ossified interspinous ligament. This approach offers a much larger opening into the epidural space than the midline approach.
Indications
-
Patients who cannot be positioned easily or cannot flex the spine (trauma/ arthritic)
-
Calcified ligament (interspinous)
-
Kyphoscoliosis or prior lumbar surgery
Procedure
The puncture site (Fig. 41.41) is located in the selected intervertebral space, about 1.5–2 cm lateral from the upper edge of the lower spinous process. Fan-shaped local anesthesia identifies the depth of the vertebral arches (laminae), which are then marked (4–6 cm). The epidural needle is introduced in a cranio-medial direction at an angle of about 15° to the sagittal level and about 35° to the skin surface, so that it passes the laminae and slides into the interlaminar fissure. The only ligament that needs to be penetrated on the way to the epidural space is the ligamentum flavum. Reaching this is characterized by a rubbery resistance. The most important step in this technique is to identify the depth of the ligamentum flavum. The trocar is then removed from the puncture needle, and identification of the epidural space is carried out in the same way as described for the single-shot technique.

Paramedian puncture (With permission from Danilo Jankovic)
Performance of a Thoracic Epidural
The spinous process of lower thoracic vertebrae is directed horizontally; however, those of the upper to mid-thoracic vertebrae are angulated steeply downward (Fig. 41.42a). Thus, while a midline approach suffices at the lower thoracic levels, a paramedian approach is recommended at the upper to mid-thoracic levels. A cross section of structures at T3 is depicted in Fig. 41.42b.

(a) Angulation of the spinous processes of upper to mid-thoracic vertebrae (With permission from Danilo Jankovic). (b) Transverse dissection at the level of T3. (1) Ligamentum flavum, (2) epidural space, (3) subarachnoid space with spinal cord, (4) spinal dura mater, (5) spinal pia mater, (6) posterior longitudinal ligament, (7) neural foramen with spinal nerves, and (8) zygapophysial joint (With permission from Danilo Jankovic)
Midline Approach for Lower Thoracic Levels
This is similar to the technique used at the lumbar levels. The patient is usually placed in a sitting position, and monitoring is applied. Intravenous access is established before starting. Landmarks are identified by palpating the spinous processes of the lower thoracic vertebrae. Thorough, repeated, and wide skin prep is applied. After drying, the injection site is covered using a sterile drape. The skin and supraspinous and interspinous ligaments are anesthetized with 1–1.5 ml of a local anesthetic as described earlier. A 16-G Tuohy-tip epidural needle is fixed between the thumb of the right hand (hub) and the index and middle finger (shaft) and advanced through the skin, at an angle of 10–15° cephalad (Fig. 41.43). After passing the supraspinous ligament, the needle, with its bevel directed cephalad, is slowly advanced a further 2 cm until it rests firmly in the interspinous ligament. The trocar is removed and a low-friction (loss of resistance) syringe is attached. After passing the interspinous ligament, the needle must be advanced carefully, millimeter by millimeter, in the direction of the ligamentum flavum. The thumb of the right hand applies pressure on the syringe plunger. Loss of resistance indicates that the epidural space has been reached. Extreme care should be exercised at the thoracic level since the spinal cord lies beneath the dura and can be damaged if the needle tip is advanced beyond the epidural space.

Midline approach for thoracic epidural (With permission from Danilo Jankovic)
Paramedian Approach for Upper to Mid-thoracic Levels
At this level, the puncture site is located about 1–1.5 cm lateral from the caudal edge of the lower spinous process. A fan-shaped local anesthesia infiltration is used to anesthetize the skin and also to identify the depth of the vertebral arches (laminae). The epidural needle is introduced in a cranio-medial direction at an angle of about 10–15° to the sagittal level and about 35–45° to the skin surface (Fig. 41.44). The only ligament that needs to be penetrated on the way to the epidural space is the ligamentum flavum. The trocar is then removed from the puncture needle and identification of the epidural space is carried out using a loss-of-resistance syringe. If a bone is contacted, the needle is withdrawn by 0.5 cm, walked off the bone in a medial/cephalad direction until the ligamentum flavum is pierced.

The needle angulation for a mid-thoracic paramedian approach (With permission from Danilo Jankovic)
After accessing the epidural space, a catheter is threaded 3–4 cm in the space akin to that for lumbar levels. However, one should not inject more than 3–4 ml of test dose at a time at thoracic levels as they tend to spread more. Using a larger volume may lead to profound hypotension due to a widespread sympathetic block.
Management of the Patient After an Epidural Block
Patient Positioning
Gravity does not play a clinically significant role in determining the spread of local anesthetic in the epidural space. Thus, the patient is generally placed supine after the block.
Patient Monitoring
-
(a)
The patient should be monitored during and after the placement of epidural block, just like a spinal block. However, the cardiovascular changes seen with an epidural block are in general slower and less profound when compared to a spinal anesthetic. Fluids and vasopressors are used to treat hypotension.
-
(b)
Supplemental oxygen administration is recommended, especially if sedation is used for patient comfort.
-
(c)
End-tidal carbon dioxide monitoring is also used to monitor the respiratory rate.
-
(d)
Postoperatively, the patient should be monitored until the effects of epidural anesthetic have receded or until the epidural catheter is removed.
Troubleshooting an Inadequate or Ineffective Epidural Block
-
(a)
Inadequate sensory block: this may require repeat dosing if the block fails to reach adequate sensory height after 30 min of the initial dose. Addition of opioids (such as fentanyl) to local anesthetic solution may speed the onset and extend the number of segments blocked [74]. An inadequate block in lower segments (L5–S1) may be difficult to troubleshoot in particular.
-
(b)
Missed segments: this may be due to an inadequate volume of initial dose used. A repeat dose often improves this. If the missed segment is unilateral, turning the patient on the spared side before dosing can help [75]. A 2 % lignocaine solution with epinephrine is most effective in dealing with missed segments or an inadequate block.
Assessment of the Block
Similar to the subarachnoid block, an epidural block leads to sensory, autonomic, and motor blockade. These can be assessed as follows:
-
(a)
Sensory block: this can be assessed by testing for loss of touch, temperature, or pinprick. A differential block is noted between the complete loss of cold sensation (being two dermatomes cephalad) and the complete loss of both pinprick and light touch sensation (being caudal) [76].
-
(b)
Autonomic block: this can be subjectively judged by the skin temperature in the involved areas and the degree of blood pressure drop (sympathetic block). Digital plethysmogram and skin conductance are used in research settings to test this objectively.
-
(c)
Motor block: this can be assessed by using the Bromage scale for a lumbar epidural and a RAM (rectus abdominis muscle) test for thoracic epidural [77, 78]. These are summarized in Tables 41.5 and 41.6.
Table 41.5 Bromage scale for assessment of motor block Table 41.6 RAM test of abdominal muscles
Considerations in Patients with Challenging Anatomy
Performing a neuraxial block can be technically challenging in certain patient groups. This includes patients with high body mass index, patients with scoliosis, and those having undergone a spinal surgery. Altered anatomy makes performing the block technically challenging, while spinal stenosis or postoperative epidural fibrosis can impair the spread of spinal anesthetics in the subarachnoid or epidural space, resulting in failed blocks.
Patients with High Body Mass Index
The anthropometric changes associated with obesity make performing a neuraxial block particularly difficult. Difficulty in proper positioning, obscured anatomical landmarks, increased depth of the ligamentum flavum, and the occasional inadequacy of usual equipment (e.g., needle too short) contribute to making neuraxial blocks in obese technically challenging [79]. This can result in a higher incidence of dural punctures while performing epidural anesthesia in morbidly obese patients [80]. Ultrasound helps in the correct identification of midline, intervertebral spaces, and estimates of depth of the ligamentum flavum. It has been successfully used to improve the success rate of epidural placement in obese parturients [81].
Patients with Scoliosis
Lateral deviation of the spine is accompanied by the rotation of the vertebral bodies toward the convex side of the curvature, while the spinous processes are rotated toward the concave side [82]. This makes performing a neuraxial block quite difficult. Ultrasound assists in identifying the lateral curvature and rotation and in its quantifications. The usual approach to this situation is to perform the block using a paramedian injection on the convex side, which provides a more direct access to the neuraxis [83]. Alternatively, if a midline insertion is used, the needle should be directed in a transverse plane, toward the convex side [84].
Patients with Previous Spine Surgery
Epidural fibrosis following spine surgery, altered spine anatomy, and the possibility of worsening neurological symptoms make this patient subset a challenge. Despite this, there have been several reports and reviews of successful neuraxial blocks in patients with previous spine surgery [85–87].
While the absence of spinous process makes it hard to locate intervertebral spaces, laminectomy may actually increase the chances of obtaining a successful dural puncture by increasing the size of the interlaminar gap. However, performing an epidural at the level of previous spinal surgery poses additional challenges due to spinal stenosis immediately above the fusion or decompression and tethering of the dura to the ligamentum flavum by scar formation [88, 89]. The epidural space may also be scarred which reduces the reliability of the loss-of-resistance technique. Thus, performing the epidural injection one or two spaces above or below the level of the surgery is advocated to reduce the chances of accidental dural puncture and ineffective block. Note that scarring of the epidural space may also lead to patchy block.
Ultrasound can help immensely to locate the intervertebral space, identify the interlaminar window, and visualize and estimate the depth of the ligamentum flavum [90].
Pharmacology of Neuraxial Drugs
Many local anesthetics and other adjuvant drugs are used for the conduct of a spinal anesthetic. A reliably rapid onset, adequate distribution and duration, and timely return of the neurological function make spinal anesthesia a good choice for many procedures. However, the successful application of a spinal anesthetic requires a good understanding of the effects of intrathecal drugs and factors that determine them.
Pharmacokinetics of Intrathecal Local Anesthetics
Determinants of Intrathecal Distribution
The local anesthetic deposited within the subarachnoid space spreads to the nerve via bulk flow. Many factors have been proposed to influence the spread of local anesthetics within the subarachnoid space [91, 92]. These may be classified as:
Characteristics of Injected Drug
-
(a)
Baricity: it is defined as the ratio of the density of the local anesthetic solution relative to the patient CSF at 37 ° C. Isobaric, hyperbaric, and hypobaric solutions have same, greater, and less density than the CSF, respectively. While hyperbaric solutions will sink to the most dependent areas within the subarachnoid space, the hypobaric solutions rise upward toward the nondependent areas. In general, hyperbaric solutions will produce a greater spread than isobaric or hypobaric solutions [93].
-
(b)
Mass of the drug: mass, volume, and concentration have been investigated for their effects on the spread of the local anesthetics in the intrathecal compartment. For plain solutions, the effect of drug mass injected is more important than the volume or the concentration [94]. For hyperbaric solutions, this may not always be true, with some studies finding no effect [95].
-
(c)
Effect of additives: while the addition of vasoconstrictors prolong the block duration, the addition of opioids may increase spread and delay block recession [96, 97].
Technical Considerations
-
(a)
Patient position: immediately after, a spinal anesthetic determines the extent of spread under the influence of gravity. This is further influenced by the curvatures of the spine [95, 98].
-
(b)
Level of injection: for an isobaric solution, a higher level of injection results in a greater cephalad spread of the block [99]. This is not consistently observed with hyperbaric solutions where the effect of gravity may be more profound [100].
-
(c)
Needle direction: turning the needle aperture cephalad may result in a higher spread of the drug, with a shorter duration of action and faster resolution of the block [101]. Cephalad angulation of insertion has shown similar results [102].
-
(d)
Speed of injection: has clinically minimal effects.
-
(e)
Barbotage: may shorten the time of onset with hyperbaric solutions [103].
Patient Factors
Individual patient factors such as age, height, body mass index, and sex do not help to predict the spread of intrathecal local anesthetics. However, excessive lordosis in pregnancy may promote cephalad spread, and lowering doses is recommended [104, 105].
Uptake of Local Anesthetics
The local anesthetic deposited in the subarachnoid space spreads within the CSF. It is then taken up by the nerve roots in the cauda equina, resulting in neuronal block. This uptake is affected by the following factors:
-
(a)
Concentration of the local anesthetic in the CSF
-
(b)
The surface area of the nerve root exposed to the CSF [106]
-
(c)
The lipid content of the nerve root (since local anesthetics are lipid soluble)
-
(d)
The blood flow within the nerve
Elimination of Local Anesthetics
The elimination of local anesthetics from the subarachnoid space is determined by the following factors:
-
(a)
Vascular absorption of the local anesthetic (this is the most important route) [107]
-
(b)
Escape of the drug to the epidural space, with subsequent vascular absorption [108]
-
(c)
Lipophilicity of the local anesthetic (highly lipophilic drugs such as bupivacaine have a slower elimination due to greater binding with the neuronal tissue) [109]
Determinants of Duration
Elimination of local anesthetics from the intrathecal space determines the duration of their neural block. The factors influencing this are:
-
(a)
Physicochemical properties of the local anesthetic chosen: while prilocaine and 2-chloroprocaine are short-acting agents, lignocaine and mepivacaine are short- to intermediate-acting local anesthetics. Bupivacaine, levobupivacaine, and ropivacaine are longer-acting agents. However, it must be noted that there is wide inter-patient variability.
-
(b)
Dose injected: in general, the duration of the block is increased with an increase in the dose (or mass) of the local anesthetic injected.
-
(c)
Block spread: for a given dose of the local anesthetic, a block with a greater spread (i.e., higher peak sensory block) will regress faster, thereby shortening the duration of action [110].
-
(d)
Addition of adjuvants: as mentioned above, the addition of vasoconstrictors and opioids may delay the regression of the block [111, 112].
Intrathecal Local Anesthetics
The physicochemical properties of local anesthetics such as lipid solubility and protein binding impact the duration of block. Depending upon this, these local anesthetics may be classified as follows:
Short-Acting Agents
-
(a)
Procaine is an amino ester with a rapid onset (3–5 min) but short duration (50–60 min) of block. This is due to its poor lipid solubility and protein binding. Compared to lignocaine, it has a higher rate of block failure but a lower rate of transient neurologic syndromes (TNS) [113, 114].
-
(b)
2-Chloroprocaine is an amino ester with a rapid onset and short duration (60 min) of spinal block comparable to lignocaine. It has a lower incidence of TNS [115].
-
(c)
Prilocaine is a short-acting amino-amide with a short duration of action (60–120 min). It has been recently used for ambulatory surgery, with shorter recovery times when compared to lignocaine [116, 117].
Short- to Intermediate-Acting Agents
-
(a)
Lignocaine is an amino-amide with a rapid onset and short to intermediate duration of action (60 min, depending upon dose). Its use has dramatically declined due to the higher frequency of TNS observed with its use (15–33 %) [118].
-
(b)
Mepivacaine is an amino-amide with similar profile to lignocaine but lower incidence of TNS (3–6 %).
Long-Acting Agents
-
(a)
Tetracaine is a long-acting (3 h) amino ester with a high lipid solubility. It has been almost entirely replaced by bupivacaine due to poor reliability.
-
(b)
Bupivacaine is a prototypical amino-amide with a long duration of action due to high lipid solubility. It is the most widely used intrathecal local anesthetic. It has an onset time of 10 min and a block duration of 3–4 h. Reducing the doses for unilateral spinal or ambulatory surgery shortens the duration of action but may also increase the incidence of block failures [119].
-
(c)
Levobupivacaine: this less cardiotoxic stereoisomer of bupivacaine is almost identical to bupivacaine in its spinal anesthetic profile [120].
-
(d)
Ropivacaine is a long-acting amino-amide which has gained popularity by virtue of its less cardiotoxic potential. When compared to bupivacaine, it is less potent and produces a block of shorter duration [121].
Dosages and duration of commonly used local anesthetics are summarized in Tables 41.7 and 41.8.
Intrathecal Adjuvants
Additives are often used along with intrathecal local anesthetics to prolong or intensify their block. Although many drugs have been used and evaluated for this, the commonly used intrathecal additives include opioids, vasoconstrictors, and the α2-adrenergic agonists.
Opioids
Opioids act synergistically with local anesthetics by blocking the opioid receptors at the spinal level.
-
(a)
Morphine is the most commonly used hydrophilic opioid. Because of its slow distribution within the CSF and a slow plasma clearance, it has a long duration of action when given intrathecally. Used in the doses of 100–400 mcg, it provides good postoperative analgesia up to 24 h. However, the intrathecal use of morphine has been implicated in delayed respiratory depression due to rostral migration within the CSF [122]. Higher doses of intrathecal morphine are associated with higher incidence of side effects such as nausea, vomiting, pruritus, urinary retention, and respiratory depression [123, 124].
-
(b)
Fentanyl is the most commonly used lipophilic opioid having a rapid onset (5–10 min) and an intermediate duration (1–2 h) of action. In the dose range of 10–25 mcg, it increases the intensity of the block without prolonging it. This makes it a suitable option for ambulatory surgery. It should be noted however that there is a risk of nausea and vomiting and pruritus, especially at higher doses.
-
(c)
Sufentanil is a lipophilic opioid used in the dose range of 2.5–7.5 mcg. It has been used in orthopedic surgery and labor analgesia [125, 126].
Vasoconstrictors
These drugs reduce the vascular uptake of intrathecal local anesthetics, thereby prolonging their duration. However, the significant prolongation is observed when vasoconstrictors are added to tetracaine, when compared with their use along with lignocaine or bupivacaine [127]. The recommended dose range of intrathecal epinephrine is 0.2–0.3 mg and that of phenylephrine is 2–5 mg. Due to delay in return of sacral autonomic function causing delay in the ability to void and increased risk of urinary retention, the use of vasoconstrictors is not recommended in ambulatory surgery [111].
α2-Adrenergic Agonists
α2-Adrenergic agonists such as clonidine and dexmedetomidine act on α2-adrenergic receptors in substantia gelatinosa in the spinal cord, intensifying and prolonging both sensory and motor block produced by intrathecal local anesthetics. Clonidine also prolongs spinal block when given orally or intravenously. This, however, is accompanied by a higher incidence of undesirable side effects such as bradycardia, hypotension, and sedation, when compared with the intrathecal route [128]. The recommended doses of clonidine is 15–150 mcg (but lower doses are advocated), while that of dexmedetomidine is 3 mcg [129, 130].
Pharmacology of Epidurally Administered Drugs
The precise site of action of epidural local anesthetic is not known. However, they are distributed by resorption into the circulation (via the epidural venous plexus), diffuse through the dura into the CSF, and spread laterally through the intervertebral foramina (associated paravertebral block of the spinal nerves) [131].
The local anesthetic spreads both cephalad and caudad in the epidural space. Since the band of anesthesia produced thus cannot be predicted accurately in a given patient, clinicians must be aware of major factors determining this spread. The factors affecting the spread of the local anesthetic within the epidural space are discussed below:
-
(a)
Drug mass, concentration, and volume: both total drug dose and volume are independent determinants of the spread of epidural block. However, they are not linearly related. A higher concentration produces a profound block of both motor and sensory nerves, as opposed to a more selective sensory block produced by using lower concentrations [132].
-
(b)
Site of injection: this is a major determinant of the epidural spread. For example, the same volume of drug in the caudal space covers less dermatomes when compared to the thoracic level [133].
-
(c)
Other technical factors: patient position, needle angulation, direction of needle opening, and the speed of injection are not clinically significant.
-
(d)
Length of catheter in space: threading an epidural catheter more than 5 cm may cause lateral location of the catheter tip, resulting in missed segments or unilateral block.
-
(e)
Patient factors: increasing age, shorter height, and increased body mass index are associated with increased spread, but this is highly variable and cannot be predicted. The epidural spread is not affected by differences in gender.
Epidurally Used Local Anesthetics
Nearly all local anesthetics have been used for epidural block. They are commonly classified by their duration of action. Time for two segment regression is the time taken for the block to recede by two dermatomes from its maximal extent, while the time for complete resolution is the time taken for the recovery from sensory block. While the former helps to time the repeating of an epidural dose intraoperatively, the latter is used to estimate the time for discharge for outpatients. Commonly used agents with doses are mentioned in Table 41.9.
In general, more dilute concentrations suffice for analgesia, while higher concentrations are used for a surgical block. The total dose and volume needed depends upon the surgery and other factors already discussed in section “Management of the patient after an epidural block”.
Epidurally Administered Adjuvants
Similar to spinal anesthetic, many adjuvants have been used to improve the quality of an epidural block. These are summarized below.
Epinephrine
In a concentration of 2.5–5 mcg/ml (1:400,000–1:200,000), epinephrine prolongs both the sensory and motor block when added to short- to intermediate-acting local anesthetics [134]. It reduces the vascular uptake of local anesthetics into the systemic circulation. It may also exert an analgesic effect through α2-adrenergic receptors, reducing pain transmission within the spinal cord [135]. The addition of epinephrine in an epidural block produces a vasodilatation secondary to β2-adrenergic effects in the periphery. This decreases the mean arterial pressure but also increases the cardiac output [136].
Clonidine
Clonidine prolongs the sensory block only, when added to epidural local anesthetics. It is used in doses of 150–300 mcg. Hypotension and sedation are common secondary to systemic uptake.
Opioids
Commonly used epidural opioids include fentanyl (0.5–0.15 mcg/kg), sufentanil (0.3–0.7 mcg/kg), hydromorphone (0.8–1.5 mg), and morphine (4–6 mg) [137].
Bicarbonate
Addition of sodium bicarbonate (0.1 mEq/ml) to local anesthetics has been proposed as a means to hasten the onset of the blocks. While some studies have shown a faster onset, others have found no difference [138].
Complications of Neuraxial Blocks
Complications arising from a spinal or an epidural anesthetic are mostly cardiovascular and neurological. However, practically, they can be classified as early or late.
Early Complications
These include complications seen immediately following a neuraxial block and in the early perioperative period.
Cardiovascular
These are the most prominent complications of a central neuraxial anesthetic and occur as a consequence of profound sympathetic block caused by the intrathecal local anesthetic.
-
(a)
Hypotension: arteriolar dilation and venous pooling lead to hypotension, which is the most frequent complications (16–33 %) observed [139]. A block above T5, emergency surgery, age greater than 40, chronic hypertension, a combined spinal–general anesthetic, and an intrathecal injection above L2–L3 are risk factors for developing hypotension [39]. Although hypotension mostly follows immediately after the neuraxial block, it may be delayed as well. Epidural anesthetic in general is associated with a more gradual fall of blood pressure, making it a better choice in certain circumstances. Prophylactic fluid administration (20 ml/kg) and use of vasopressors such as ephedrine (in 5–10-mg increments) or phenylephrine (50–100-mcg increments) can be used to effectively counteract hypotension.
-
(b)
Bradycardia: results usually from a high block, as a consequence of blockade of the cardiac accelerator fibers (T1–T4) or more commonly from a vagal reflex associated with intracardiac stretch receptors in the presence of decreased cardiac filling. Apart from a high block, a younger age, ASA class 1 status, preoperative use of beta-blockers, and male gender are risk factors for bradycardia [140]. Anticholinergics such as atropine and adrenergics such as ephedrine are commonly used to treat this.
-
(c)
Cardiac collapse: asystole and cardiac arrest following a spinal is a known complication [34]. It is usually preceded by bradycardia resulting from the mechanisms described above.
Nausea and Vomiting
It is associated with hypotension (hypoperfusion of the chemoreceptor trigger zone) and the use of opioids (direct stimulation of chemoreceptor trigger zone). A sympathetic–parasympathetic imbalance may also have a role to play in the causation of nausea. It can be effectively treated by dexamethasone and 5-HT3 antagonists (ondansetron) [141].
Tissue Trauma and Back Pain
Multiple attempts at a neuraxial block lead to trauma to soft tissue and ligaments. This can contribute to persistent backache [142]. However, other factors may have a role to play as well.
Total Spinal Anesthetic
This may result due to inappropriate dosing during a spinal anesthetic, positioning error, or unintended passage of local anesthetic from epidural space to subarachnoid space (secondary to an unrecognized dural tap or catheter migration) [143, 144]. It manifests as a rapidly ascending motor–sensory block, hypotension, bradycardia, and respiratory compromise. Medullary paralysis may result in a respiratory arrest and loss of consciousness. It is life-threatening and requires immediate treatment.
Management: this involves prompt recognition, securing the airway, ventilation, and supporting the hemodynamics till spontaneous recovery of the patient.
-
Immediate tracheal intubation (thiopental 1–2 mg/kg b.w. routinely ca. 150 mg i.v.); succinylcholine if appropriate, since the muscles of mastication are not affected
-
Ventilation with 100 % oxygen
-
Raising the legs
-
Rapid volume administration
-
Atropine
-
Vasopressor
-
Dopamine infusion
-
Careful cardiovascular monitoring
Subdural Anesthetic
This presents as widespread but ineffective patchy anesthesia (Fig. 41.45) [145]. Subdural injection can never be excluded with certainty. It may occur slightly more frequently after spinal anesthesia or myelography than after epidural anesthesia. The subdural space is at its widest in the cervical region, particularly dorsolaterally. It does not end at the great foramen as does the epidural space but continues cranially.

Complications. (1) Intravascular injection, (2) subdural injection, (3) subarachnoid injection, (4) catheter shearing, (5) epidural abscess, (6) epidural hematoma, and (7) injury to the spinal cord and nerve roots (With permission from Danilo Jankovic)
-
(a)
Warning signs: an unusually high sensory block, which develops very slowly (even after 20 min) and a much less marked motor block. The clinical picture resembles that of total spinal anesthesia and is characterized by moderate hypotonia, breathing difficulties with retained consciousness, and often involvement of the cranial and cervical nerves.
Trigeminal nerve: trigeminal nerve palsy, with accompanying paresthesias in the area supplied by the nerve and transient weakness of the muscles of mastication with simultaneous Horner’s syndrome, has been observed after high epidural anesthesia or subdural spread [146–148].
Horner’s syndrome: Horner’s syndrome is produced after neuraxial anesthesia with a high spread of the injected local anesthetic and block of very sensitive sympathetic nerve fibers in the areas of segments T4–C8 [148, 149]. Most often, Horner’s syndrome is seen after high spinal or epidural anesthesia in obstetrics and when there is subdural spread of the local anesthetic [150]. Relatively rapid resolution of the symptoms is characteristic.
-
(b)
Differential diagnosis:
Total spinal anesthesia: this has a dramatic course, unrecordable blood pressure and respiratory arrest, and takes a longer time required for symptoms to resolve.
-
(c)
Prophylaxis:
-
Individual dosage and dose reduction in older patients, pregnant patients, obese patients, and those with diabetes mellitus or arteriosclerosis
-
Incremental injection in epidural anesthesia
-
Dural Tap
It presents as a gush of CSF through the epidural needle or upon aspiration through the catheter (Fig. 41.45) [151]. Management options include passing a catheter through the puncture made or reattempting the epidural in another space. In over 75 % of the cases, use of an epidural needle is associated with development of post-dural puncture headache.
Local Anesthetic Toxicity
Inadvertent deposition of drug into a vein or systemic absorption of local anesthetic following infusions may lead to local anesthetic toxicity.
Delayed Complications
These present usually after a few days or weeks of having performed a neuraxial block.
Nerve Injury
These include the following:
-
(a)
Direct needle trauma: this commonly occurs at the time of performance of the block and is associated with sever paresthesia in the dermatomal distribution of the nerve root injured (Fig. 41.45) [152].
-
(b)
Neurotoxicity: all local anesthetics are potentially neurotoxic [153]. Despite this, local anesthetic-induced neural damage is rarely seen clinically.
-
(c)
Transient neurological syndrome: this presents as low back pain that radiates to the lower extremities after a spinal anesthetic. The symptoms last for a week and are treated supportively using simple analgesics. Risk factors such as outpatient procedures, the lithotomy position, obesity, and the use of lignocaine have been implicated in their development [154].
-
(d)
Cauda equina syndrome: this presents as motor weakness and loss of bladder and bowel function, following the use of continuous spinal anesthesia. The pooling of local anesthetic around sacral nerves is thought to be the causative mechanism in its development [155].
Infections
Infections such as localized skin infections, a spinal abscess, an epidural abscess, or meningitis can rarely occur following a neuraxial anesthetic (Fig. 41.45). A spinal or epidural abscess presents a localized back pain and tenderness upon palpation, with sensory or motor deficits and fever. A magnetic resonance imaging of the vertebral canal is considered best for establishing a diagnosis. Intravenous antibiotics and surgical drainage or decompression may be needed.
Post-dural Puncture Headache (PDPH)
It is a relatively common complication of a spinal or an epidural anesthetic. The incidence of PDPH with the use of smaller-gauge spinal needle (25–26G) is 0.5–1 %, while puncture with an epidural needle (17–18G) results in PDPH in over 75 % of cases [44].
-
(a)
Mechanism: the proposed mechanism of the headache is the loss of CSF causing decrease in CSF pressure. This causes sagging of intracranial structure, with consequent traction on pain-sensitive structures (such as meninges, cranial nerves, and veins) [156]. The second hypothesis suggests that decreased CSF pressure leads to intrathecal hypotension and painful vasodilatation of the intracranial blood vessels (known as the “intracranial vascular response”) [157]. Mainly when the patient is in a standing position, painful areas dilate (meninges, tentorium, vessels), and there is further pain transmission via the cerebral nerves and upper cervical nerves.
-
(b)
Clinical presentation: PDPH presents as a positional headache, worse on sitting up, 12–48 h after a dural puncture. PDPH is bilateral, predominantly frontal–temporal, and dull or throbbing in nature. Its severity varies, and it may be accompanied by associated symptoms such as nausea, vomiting, photophobia, diplopia, and hearing impairment. While younger females and parturients are at a higher risk of PDPH, older males are at a lower risk [158].
-
(c)
CSF hypotension syndrome and involvement of the cranial and cervical nerves: all of the cranial nerves, with the exception of the olfactory nerve, glossopharyngeal nerve, and vagus nerve, can be affected by low CSF pressure. The abducent nerve and vestibulocochlear nerve are most frequently affected (Fig. 41.46). The long intracranial course of the abducent nerve leads to traction and consequent irritation of the nerve when there are changes in intracranial pressure. The patient complains of double vision, with parallel horizontal images and difficulties in focusing on objects [150]. When precise audiometric examinations are carried out, unilateral or bilateral hypoacusis (vestibulocochlear nerve involvement) can be observed in 0.4–40 % of patients with CSF hypotension syndrome [150]. The prognosis is good.
Fig. 41.46 
Cranial nerves. (1) Optic nerve, (2) trochlear nerve, (3) trigeminal nerve, (4) vestibulocochlear nerve, (5) glossopharyngeal nerve, (7) vagus nerve, (8) hypoglossal nerve, and (9) abducent nerve (With permission from Danilo Jankovic)
-
(d)
Differential diagnosis: this includes migraine, tension headache, cervical myofascial pain (particularly in the sternocleidomastoid muscle, with what is known as “pseudospinal headache”), CNS infections (bacterial meningitis), sinus thrombosis (in the second half of pregnancy or in the puerperium, frequently in preeclampsia), and pneumocephalus (after accidental dural perforation in attempted epidural anesthesia when using the loss-of-resistance technique with air) [159].
-
(e)
Initial management is conservative and includes simple analgesics and oral hydration. The majority of patients experience marked improvement in the symptoms or complete recovery after 5–7 days with this form of treatment. Other drugs such as caffeine, sumatriptan, and ACTH have been found useful [160–162]. Caffeine produces cerebral vasoconstriction and consequent decrease in cerebral blood flow providing a transient relief from headache. ACTH may stimulate the adrenal gland to increase cerebrospinal fluid production and possibly also increase [beta]-endorphin output [163]. This may thus relieve low CSF pressure and also provide analgesia. Sumatriptan, a serotonin-type 1D receptor agonist, may relieve headache by producing cerebral vasoconstriction [164].
-
(f)
Invasive management: the gold standard for the treatment of PDPH remains an autologous blood patch (Figs. 41.47 and 41.48). Its mechanism appears to be the tamponade of dural leak, with subsequent improvement of CSF pressures [165]. It often produces a dramatic relief of symptoms but may need to be repeated occasionally.
Fig. 41.47 
Sterile withdrawal of blood (With permission from Danilo Jankovic)
Fig. 41.48 
Epidural injection of homologous blood (With permission from Danilo Jankovic)



Spinal or Epidural Hematoma
Although rare, this is the most feared complication of a central neuraxial block (Fig. 41.45). Because the vertebral canal is a confined space, any bleeding may result in compression of the spinal cord resulting in a sensory–motor loss below the level of the compression. Patient with altered hemostasis and ongoing antiplatelet or anticoagulant therapy is at increased risk of developing a spinal or epidural hematoma. This usually presents as a sensory–motor impairment of unusually prolonged duration. Confusing this with an ongoing effect of local anesthetic often delays the correct diagnosis and management. Back pain and bladder or bowel dysfunction may also point toward the possibility of neural damage. Prompt imaging and neurosurgical consultation should be arranged, as the prognosis is poor if the delay between the onset of paralysis and surgical decompression is more than 6–8 h [166]. Guidelines concerning neuraxial anesthesia in anticoagulated patents should be followed to minimize the risks of this devastating complication [167].





References
Chakraverty R, Pynsent P, Isaacs K. Which spinal levels are identified by palpation of the iliac crests and the posterior superior iliac spines? J Anat. 2007;210(2):232–6.
Tamakawa S. Comparing the confidence of the 7th cervical spinous process, the inferior angle of the scapula, and Tuffier’s line. Reg Anesth Pain Med. 1999;24(6):585–6.
Kim J-T, Bahk J-H, Sung J. Influence of age and sex on the position of the conus medullaris and Tuffier’s line in adults. Anesthesiology. 2003;99(6):1359–63.
Margarido CB, Mikhael R, Arzola C, Balki M, Carvalho JCA. The intercristal line determined by palpation is not a reliable anatomical landmark for neuraxial anesthesia. Can J Anaesth. 2011;58(3):262–6.
Snider KT, Kribs JW, Snider EJ, Degenhardt BF, Bukowski A, Johnson JC. Reliability of Tuffier’s line as an anatomic landmark. Spine (Phila Pa 1976). 2008;33(6):E161–5.
Furness G, Reilly MP, Kuchi S. An evaluation of ultrasound imaging for identification of lumbar intervertebral level. Anaesthesia. 2002;57(3):277–80.
Pysyk CL, Persaud D, Bryson GL, Lui A. Ultrasound assessment of the vertebral level of the palpated intercristal (Tuffier’s) line. Can J Anaesth. 2010;57(1):46–9.
Panjabi MM, Duranceau J, Goel V, Oxland T, Takata K. Cervical human vertebrae. Quantitative three-dimensional anatomy of the middle and lower regions. Spine (Phila Pa 1976). 1991;16(8):861–9.
Panjabi MM, Takata K, Goel V, Federico D, Oxland T, Duranceau J, et al. Thoracic human vertebrae. Quantitative three-dimensional anatomy. Spine (Phila Pa 1976). 1991;16(8):888–901.
Panjabi MM, Goel V, Oxland T, Takata K, Duranceau J, Krag M, et al. Human lumbar vertebrae. Quantitative three-dimensional anatomy. Spine (Phila Pa 1976). 1992;17(3):299–306.
Barker AE. A report on clinical experiences with spinal analgesia in 100 cases, and some reflections on the procedure. Br Med J. 1907;1(2412):665–74.
Cheng PA. The anatomical and clinical aspects of epidural anesthesia. II. Anesth Analg. 1963;42(4):407–15.
Cheng PA. The anatomical and clinical aspects of epidural anesthesia. I. Anesth Analg. 1963;42(3):398–406.
Hughes G, Ugokwe K, Benzel EC. A review of spinal arachnoid cysts. Cleve Clin J Med. 2008;75(4):311–5.
Stace JD, Gaylard DG. Failed spinal anaesthesia. Anaesthesia. 1996;51(9):892–3.
Bromage PR. Neurological complications of subarachnoid and epidural anaesthesia. Acta Anaesthesiol Scand. 1997;41(4):439–44.
Lirk P, Kolbitsch C, Putz G, Colvin J, Colvin HP, Lorenz I, et al. Cervical and high thoracic ligamentum flavum frequently fails to fuse in the midline. Anesthesiology. 2003;99(6):1387–90.
Hogan QH. Lumbar epidural anatomy. A new look by cryomicrotome section. Anesthesiology. 1991;75(5):767–75.
Hogan Q. Distribution of solution in the epidural space: examination by cryomicrotome section. Reg Anesth Pain Med. 2002;27(2):150–6.
Reina MA, Franco CD, López A, Dé Andrés JA, van Zundert A. Clinical implications of epidural fat in the spinal canal. A scanning electron microscopic study. Acta Anaesthesiol Belg. 2009;60(1):7–17.
Bernards CM, Shen DD, Sterling ES, Adkins JE, Risler L, Phillips B, et al. Epidural, cerebrospinal fluid, and plasma pharmacokinetics of epidural opioids (part 1): differences among opioids. Anesthesiology. 2003;99(2):455–65.
Igarashi T, Hirabayashi Y, Shimizu R, Saitoh K, Fukuda H, Mitsuhata H. The lumbar extradural structure changes with increasing age. Br J Anaesth. 1997;78(2):149–52.
Harrison GR, Clowes NW. The depth of the lumbar epidural space from the skin. Anaesthesia. 1985;40(7):685–7.
Ravi KK, Kaul TK, Kathuria S, Gupta S, Khurana S. Distance from skin to epidural space: correlation with body mass index (BMI). J Anaesthesiol Clin Pharmacol. 2011;27(1):39–42.
Balki M, Lee Y, Halpern S, Carvalho JCA. Ultrasound imaging of the lumbar spine in the transverse plane: the correlation between estimated and actual depth to the epidural space in obese parturients. Anesth Analg. 2009;108(6):1876–81.
Fink BR, Cairns AM. Differential slowing and block of conduction by lidocaine in individual afferent myelinated and unmyelinated axons. Anesthesiology. 1984;60(2):111–20.
Jaffe RA, Rowe MA. Differential nerve block. Direct measurements on individual myelinated and unmyelinated dorsal root axons. Anesthesiology. 1996;84(6):1455–64.
Liu S, Kopacz DJ, Carpenter RL. Quantitative assessment of differential sensory nerve block after lidocaine spinal anesthesia. Anesthesiology. 1995;82(1):60–3.
Neal JM. Hypotension and bradycardia during spinal anesthesia: significance, prevention, and treatment. Tech Reg Anesth Pain Manag. 2000;4(4):148–54.
Crystal GJ, Salem MR. The Bainbridge and the “reverse” Bainbridge reflexes: history, physiology, and clinical relevance. Anesth Analg. 2012;114(3):520–32.
Campagna JA, Carter C. Clinical relevance of the Bezold-Jarisch reflex. Anesthesiology. 2003;98(5):1250–60.
Otton PE, Wilson EJ. The cardiocirculatory effects of upper thoracic epidural analgesia. Can Anaesth Soc J. 1966;13(6):541–9.
Subramani K, Paul A. Laryngospasm during subarachnoid block. Br J Anaesth. 2005;94(5):668–70.
Pollard JB. Cardiac arrest during spinal anesthesia: common mechanisms and strategies for prevention. Anesth Analg. 2001;92(1):252–6.
Steinbrook RA, Concepcion M. Respiratory effects of spinal anesthesia: resting ventilation and single-breath CO2 response. Anesth Analg. 1991;72(2):182–6.
Groeben H. Epidural anesthesia and pulmonary function. J Anesth. 2006;20(4):290–9.
Leslie JB, Viscusi ER, Pergolizzi JV, Panchal SJ. Anesthetic routines: the anesthesiologist’s role in GI recovery and postoperative ileus. Adv Prev Med. 2011;2011:976904.
Shi W-Z, Miao Y-L, Yakoob MY, Cao J-B, Zhang H, Jiang Y-G, et al. Recovery of gastrointestinal function with thoracic epidural vs. systemic analgesia following gastrointestinal surgery. Acta Anaesthesiol Scand. 2014;58(8):923–32.
Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R. Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology. 1992;76(6):906–16.
Sessler DI, Ponte J. Shivering during epidural anesthesia. Anesthesiology. 1990;72(5):816–21.
Shehabi Y, Gatt S, Buckman T, Isert P. Effect of adrenaline, fentanyl and warming of injectate on shivering following extradural analgesia in labour. Anaesth Intensive Care. 1990;18(1):31–7.
Hjortsø NC, Neumann P, Frøsig F, Andersen T, Lindhard A, Rogon E, et al. A controlled study on the effect of epidural analgesia with local anaesthetics and morphine on morbidity after abdominal surgery. Acta Anaesthesiol Scand. 1985;29(8):790–6.
Hosoda R, Hattori M, Shimada Y. Favorable effects of epidural analgesia on hemodynamics, oxygenation and metabolic variables in the immediate post-anesthetic period. Acta Anaesthesiol Scand. 1993;37(5):469–74.
Liu S, Carpenter RL, Neal JM. Epidural anesthesia and analgesia. Their role in postoperative outcome. Anesthesiology. 1995;82(6):1474–506.
Ballantyne J. Does regional anesthesia improve outcome after surgery? Curr Opin Anaesthesiol. 1999;12(5):545–9.
Breivik H, Bang U, Jalonen J, Vigfússon G, Alahuhta S, Lagerkranser M. Nordic guidelines for neuraxial blocks in disturbed haemostasis from the Scandinavian Society of Anaesthesiology and Intensive Care Medicine. Acta Anaesthesiol Scand. 2010;54(1):16–41.
Kettner SC, Willschke H, Marhofer P. Does regional anaesthesia really improve outcome? Br J Anaesth. 2011;107 Suppl 1:i90–5.
Memtsoudis SG, Sun X, Chiu Y-L, Stundner O, Liu SS, Banerjee S, et al. Perioperative comparative effectiveness of anesthetic technique in orthopedic patients. Anesthesiology. 2013;118(5):1046–58.
Horlocker TT, Wedel DJ, Rowlingson JC, Enneking FK. Executive summary: regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med. 2010;35(1):102–5.
Hurst E. Adhesive arachnoiditis and vascular blockage caused by detergents and other chemical irritants: an experimental study. J Pathol Bacteriol. 1955;70(1):167–78.
Cook TM, Counsell D, Wildsmith JAW. Major complications of central neuraxial block: report on the Third National Audit Project of the Royal College of Anaesthetists. Br J Anaesth. 2009;102(2):179–90.
Lambert DH, Hurley RJ, Hertwig L, Datta S. Role of needle gauge and tip configuration in the production of lumbar puncture headache. Reg Anesth. 1997;22(1):66–72.
Parker RK, White PF. A microscopic analysis of cut-bevel versus pencil-point spinal needles. Anesth Analg. 1997;85(5):1101–4.
Richman JM, Joe EM, Cohen SR, Rowlingson AJ, Michaels RK, Jeffries MA, et al. Bevel direction and postdural puncture headache: a meta-analysis. Neurologist. 2006;12(4):224–8.
Obasuyi BI, Fyneface-Ogan S, Mato CN. A comparison of the haemodynamic effects of lateral and sitting positions during induction of spinal anaesthesia for caesarean section. Int J Obstet Anesth. 2013;22(2):124–8.
Kinsella SM, Lohmann G. Supine hypotensive syndrome. Obstet Gynecol. 1994;83(5 Pt 1):774–88.
Edgcombe H, Carter K, Yarrow S. Anaesthesia in the prone position. Br J Anaesth. 2008;100(2):165–83.
Rabinowitz A, Bourdet B, Minville V, Chassery C, Pianezza A, Colombani A, et al. The paramedian technique: a superior initial approach to continuous spinal anesthesia in the elderly. Anesth Analg. 2007;105(6):1855–7.
Enk D, Prien T, Van Aken H, Mertes N, Meyer J, Brüssel T. Success rate of unilateral spinal anesthesia is dependent on injection flow. Reg Anesth Pain Med. 2001;26(5):420–7.
Casati A, Fanelli G. Unilateral spinal anesthesia. State of the art. Minerva Anestesiol. 2001;67(12):855–62.
Kuusniemi KS, Pihlajamäki KK, Pitkänen MT, Korkeila JE. A low-dose hypobaric bupivacaine spinal anesthesia for knee arthroscopies. Reg Anesth. 1997;22(6):534–8.
Denny NM, Selander DE. Continuous spinal anaesthesia. Br J Anaesth. 1998;81(4):590–7.
Gosch UW, Hueppe M, Hallschmid M, Born J, Schmucker P, Meier T. Post-dural puncture headache in young adults: comparison of two small-gauge spinal catheters with different needle design. Br J Anaesth. 2005;94(5):657–61.
Horlocker TT, McGregor DG, Matsushige DK, Chantigian RC, Schroeder DR, Besse JA. Neurologic complications of 603 consecutive continuous spinal anesthetics using macrocatheter and microcatheter techniques. Perioperative Outcomes Group. Anesth Analg. 1997;84(5):1063–70.
Faust A, Fournier R, Van Gessel E, Weber A, Hoffmeyer P, Gamulin Z. Isobaric versus hypobaric spinal bupivacaine for total hip arthroplasty in the lateral position. Anesth Analg. 2003;97(2):589–94, table of contents.
Dyamanna DN, Bs SK, Zacharia BT. Unexpected bradycardia and cardiac arrest under spinal anesthesia: case reports and review of literature. Middle East J Anesthesiol. 2013;22(1):121–5.
Russell IF. A comparison of cold, pinprick and touch for assessing the level of spinal block at caesarean section. Int J Obstet Anesth. 2004;13(3):146–52.
Ousley R, Egan C, Dowling K, Cyna AM. Assessment of block height for satisfactory spinal anaesthesia for caesarean section. Anaesthesia. 2012;67(12):1356–63.
Zarzur E. Anatomic studies of the human ligamentum flavum. Anesth Analg. 1984;63(5):499–502.
Saberski LR, Kondamuri S, Osinubi OY. Identification of the epidural space: is loss of resistance to air a safe technique? A review of the complications related to the use of air. Reg Anesth. 1997;22(1):3–15.
Todorov L, VadeBoncouer T. Etiology and use of the “hanging drop” technique: a review. Pain Res Treat. 2014;2014:Article ID 146750, 10 p.
Guay J. The epidural test dose: a review. Anesth Analg. 2006;102(3):921–9.
Walker DS, Brock-Utne JG. A comparison of simple tests to distinguish cerebrospinal fluid from saline. Can J Anaesth. 1997;44(5 Pt 1):494–7.
Hermanides J, Hollmann MW, Stevens MF, Lirk P. Failed epidural: causes and management. Br J Anaesth. 2012;109(2):144–54.
Arendt K, Segal S. Why epidurals do not always work. Rev Obstet Gynecol. 2008;1(2):49–55.
Camorcia M, Capogna G. Sensory assessment of epidural block for Caesarean section: a systematic comparison of pinprick, cold and touch sensation. Eur J Anaesthesiol. 2006;23(7):611–7.
Graham AC, McClure JH. Quantitative assessment of motor block in labouring women receiving epidural analgesia. Anaesthesia. 2001;56(5):470–6.
Van Zundert A, Vaes L, Van der Aa P, Van der Donck A, Meeuwis H. Motor blockade during epidural anesthesia. Anesth Analg. 1986;65(4):333–6.
Ellinas EH, Eastwood DC, Patel SN, Maitra-D’Cruze AM, Ebert TJ. The effect of obesity on neuraxial technique difficulty in pregnant patients: a prospective, observational study. Anesth Analg. 2009;109(4):1225–31.
Hood DD, Dewan DM. Anesthetic and obstetric outcome in morbidly obese parturients. Anesthesiology. 1993;79(6):1210–8.
Grau T, Leipold RW, Conradi R, Martin E, Motsch J. Efficacy of ultrasound imaging in obstetric epidural anesthesia. J Clin Anesth. 2002;14(3):169–75.
White AA, Panjabi MM. The clinical biomechanics of scoliosis. Clin Orthop Relat Res. 1976;118:100–12.
Boon JM, Prinsloo E, Raath RP. A paramedian approach for epidural block: an anatomic and radiologic description. Reg Anesth Pain Med. 2003;28(3):221–7.
Huang J. Paramedian approach for neuroaxial anesthesia in parturients with scoliosis. Anesth Analg. 2010;111(3):821–2; author reply 822.
Berkowitz S, Gold MI. Spinal anesthesia for surgery in patients with previous lumbar laminectomy. Anesth Analg. 1980;59(11):881–2.
Kim SH, Jeon D-H, Chang CH, Lee S-J, Shin Y-S. Spinal anesthesia with isobaric tetracaine in patients with previous lumbar spinal surgery. Yonsei Med J. 2009;50(2):252–6.
Sharrock NE, Urquhart B, Mineo R. Extradural anaesthesia in patients with previous lumbar spine surgery. Br J Anaesth. 1990;65(2):237–9.
Brodsky AE. Post-laminectomy and post-fusion stenosis of the lumbar spine. Clin Orthop Relat Res. 1976;115:130–9.
LaRocca H, Macnab I. The laminectomy membrane. Studies in its evolution, characteristics, effects and prophylaxis in dogs. J Bone Joint Surg Br. 1974;56B(3):545–50.
Yamauchi M, Honma E, Mimura M, Yamamoto H, Takahashi E, Namiki A. Identification of the lumbar intervertebral level using ultrasound imaging in a post-laminectomy patient. J Anesth. 2006;20(3):231–3.
Greene NM. Distribution of local anesthetic solutions within the subarachnoid space. Anesth Analg. 1985;64(7):715–30.
Hocking G, Wildsmith JAW. Intrathecal drug spread. Br J Anaesth. 2004;93(4):568–78.
Stienstra R, van Poorten JF. Plain or hyperbaric bupivacaine for spinal anesthesia. Anesth Analg. 1987;66(2):171–6.
Van Zundert AA, Grouls RJ, Korsten HH, Lambert DH. Spinal anesthesia. Volume or concentration–what matters? Reg Anesth. 1996;21(2):112–8.
Wildsmith JA, McClure JH, Brown DT, Scott DB. Effects of posture on the spread of isobaric and hyperbaric amethocaine. Br J Anaesth. 1981;53(3):273–8.
Kito K, Kato H, Shibata M, Adachi T, Nakao S, Mori K. The effect of varied doses of epinephrine on duration of lidocaine spinal anesthesia in the thoracic and lumbosacral dermatomes. Anesth Analg. 1998;86(5):1018–22.
Singh H, Yang J, Thornton K, Giesecke AH. Intrathecal fentanyl prolongs sensory bupivacaine spinal block. Can J Anaesth. 1995;42(11):987–91.
Hirabayashi Y, Shimizu R, Saitoh K, Fukuda H, Furuse M. Anatomical configuration of the spinal column in the supine position. I. A study using magnetic resonance imaging. Br J Anaesth. 1995;75(1):3–5.
Tuominen M, Taivainen T, Rosenberg PH. Spread of spinal anaesthesia with plain 0.5 % bupivacaine: influence of the vertebral interspace used for injection. Br J Anaesth. 1989;62(4):358–61.
Sakura S, Sumi M, Morimoto N, Yamamori Y, Saito Y. Spinal anesthesia with tetracaine in 0.75 % glucose: influence of the vertebral interspace used for injection. Reg Anesth Pain Med. 1998;23(2):170–5.
Urmey WF, Stanton J, Bassin P, Sharrock NE. The direction of the Whitacre needle aperture affects the extent and duration of isobaric spinal anesthesia. Anesth Analg. 1997;84(2):337–41.
Stienstra R, van Poorten F, Kroon JW. Needle direction affects the sensory level of spinal anesthesia. Anesth Analg. 1989;68(4):497–500.
Janik R, Dick W, Stanton-Hicks MD. Influence of barbotage on block characteristics during spinal anesthesia with hyperbaric tetracaine and bupivacaine. Reg Anesth. 1989;14(1):26–30.
Van Bogaert LJ. Lumbar lordosis and the spread of subarachnoid hyperbaric 0.5 % bupivacaine at cesarean section. Int J Gynaecol Obstet. 2000;71(1):65–6.
Roofthooft E, Van de Velde M. Low-dose spinal anaesthesia for Caesarean section to prevent spinal-induced hypotension. Curr Opin Anaesthesiol. 2008;21(3):259–62.
Cohen EN. Distribution of local anesthetic agents in the neuraxis of the dog. Anesthesiology. 1968;29(5):1002–5.
Burm AG, van Kleef JW, Gladines MP, Spierdijk J, Breimer DD. Plasma concentrations of lidocaine and bupivacaine after subarachnoid administration. Anesthesiology. 1983;59(3):191–5.
Greene NM. Uptake and elimination of local anesthetics during spinal anesthesia. Anesth Analg. 1983;62(11):1013–24.
Burm AG, Van Kleef JW, Vermeulen NP, Olthof G, Breimer DD, Spierdijk J. Pharmacokinetics of lidocaine and bupivacaine following subarachnoid administration in surgical patients: simultaneous investigation of absorption and disposition kinetics using stable isotopes. Anesthesiology. 1988;69(4):584–92.
Kooger Infante NE, Van Gessel E, Forster A, Gamulin Z. Extent of hyperbaric spinal anesthesia influences the duration of spinal block. Anesthesiology. 2000;92(5):1319–23.
Moore JM, Liu SS, Pollock JE, Neal JM, Knab JH. The effect of epinephrine on small-dose hyperbaric bupivacaine spinal anesthesia: clinical implications for ambulatory surgery. Anesth Analg. 1998;86(5):973–7.
Rathmell JP, Lair TR, Nauman B. The role of intrathecal drugs in the treatment of acute pain. Anesth Analg. 2005;101(5 Suppl):S30–43.
Axelrod EH, Alexander GD, Brown M, Schork MA. Procaine spinal anesthesia: a pilot study of the incidence of transient neurologic symptoms. J Clin Anesth. 1998;10(5):404–9.
Le Truong HH, Girard M, Drolet P, Grenier Y, Boucher C, Bergeron L. Spinal anesthesia: a comparison of procaine and lidocaine. Can J Anaesth. 2001;48(5):470–3.
Casati A, Fanelli G, Danelli G, Berti M, Ghisi D, Brivio M, et al. Spinal anesthesia with lidocaine or preservative-free 2-chloroprocaine for outpatient knee arthroscopy: a prospective, randomized, double-blind comparison. Anesth Analg. 2007;104(4):959–64.
Black AS, Newcombe GN, Plummer JL, McLeod DH, Martin DK. Spinal anaesthesia for ambulatory arthroscopic surgery of the knee: a comparison of low-dose prilocaine and fentanyl with bupivacaine and fentanyl. Br J Anaesth. 2011;106(2):183–8.
Gebhardt V, Herold A, Weiss C, Samakas A, Schmittner MD. Dosage finding for low-dose spinal anaesthesia using hyperbaric prilocaine in patients undergoing perianal outpatient surgery. Acta Anaesthesiol Scand. 2013;57(2):249–56.
Zaric D, Pace NL. Transient neurologic symptoms (TNS) following spinal anaesthesia with lidocaine versus other local anaesthetics. Cochrane Database Syst Rev. 2009;2:CD003006.
Nair GS, Abrishami A, Lermitte J, Chung F. Systematic review of spinal anaesthesia using bupivacaine for ambulatory knee arthroscopy. Br J Anaesth. 2009;102(3):307–15.
Alley EA, Kopacz DJ, McDonald SB, Liu SS. Hyperbaric spinal levobupivacaine: a comparison to racemic bupivacaine in volunteers. Anesth Analg. 2002;94(1):188–93, table of contents.
McDonald SB, Liu SS, Kopacz DJ, Stephenson CA. Hyperbaric spinal ropivacaine: a comparison to bupivacaine in volunteers. Anesthesiology. 1999;90(4):971–7.
Gehling M, Tryba M. Risks and side-effects of intrathecal morphine combined with spinal anaesthesia: a meta-analysis. Anaesthesia. 2009;64(6):643–51.
Raffaeli W, Marconi G, Fanelli G, Taddei S, Borghi GB, Casati A. Opioid-related side-effects after intrathecal morphine: a prospective, randomized, double-blind dose-response study. Eur J Anaesthesiol. 2006;23(7):605–10.
Sultan P, Gutierrez MC, Carvalho B. Neuraxial morphine and respiratory depression: finding the right balance. Drugs. 2011;71(14):1807–19.
Motiani P, Chaudhary S, Bahl N, Sethi AK. Intrathecal sufentanil versus fentanyl for lower limb surgeries – a randomized controlled trial. J Anaesthesiol Clin Pharmacol. 2011;27(1):67–73.
Nelson KE, Rauch T, Terebuh V, D’Angelo R. A comparison of intrathecal fentanyl and sufentanil for labor analgesia. Anesthesiology. 2002;96(5):1070–3.
Concepcion M, Maddi R, Francis D, Rocco AG, Murray E, Covino BG. Vasoconstrictors in spinal anesthesia with tetracaine–a comparison of epinephrine and phenylephrine. Anesth Analg. 1984;63(2):134–8.
Dobrydnjov I, Axelsson K, Samarütel J, Holmström B. Postoperative pain relief following intrathecal bupivacaine combined with intrathecal or oral clonidine. Acta Anaesthesiol Scand. 2002;46(7):806–14.
Elia N, Culebras X, Mazza C, Schiffer E, Tramèr MR. Clonidine as an adjuvant to intrathecal local anesthetics for surgery: systematic review of randomized trials. Reg Anesth Pain Med. 2008;33(2):159–67.
Kim JE, Kim NY, Lee HS, Kil HK. Effects of intrathecal dexmedetomidine on low-dose bupivacaine spinal anesthesia in elderly patients undergoing transurethral prostatectomy. Biol Pharm Bull. 2013;36(6):959–65.
Bromage PR. Mechanism of action of extradural analgesia. Br J Anaesth. 1975;47(suppl):199–211.
Duggan J, Bowler GM, McClure JH, Wildsmith JA. Extradural block with bupivacaine: influence of dose, volume, concentration and patient characteristics. Br J Anaesth. 1988;61(3):324–31.
Visser WA, Lee RA, Gielen MJM. Factors affecting the distribution of neural blockade by local anesthetics in epidural anesthesia and a comparison of lumbar versus thoracic epidural anesthesia. Anesth Analg. 2008;107(2):708–21.
Bromage P, Burfoot M, Crowell D, Pettigrew R. Quality of epidural blockade. I. Influence of physical factors. Br J Anaesth. 1964;36:342–52.
Reddy SV, Yaksh TL. Spinal noradrenergic terminal system mediates antinociception. Brain Res. 1980;189(2):391–401.
Bonica JJ, Kennedy WF, Ward RJ, Tolas AG. A comparison of the effects of high subarachnoid and epidural anesthesia. Acta Anaesthesiol Scand Suppl. 1966;23:429–37.
De Leon-Casasola OA, Lema MJ. Postoperative epidural opioid analgesia: what are the choices? Anesth Analg. 1996;83(4):867–75.
Curatolo M, Petersen-Felix S, Arendt-Nielsen L, Lauber R, Högström H, Scaramozzino P, et al. Adding sodium bicarbonate to lidocaine enhances the depth of epidural blockade. Anesth Analg. 1998;86(2):341–7.
Salinas FV, Sueda LA, Liu SS. Physiology of spinal anaesthesia and practical suggestions for successful spinal anaesthesia. Best Pract Res Clin Anaesthesiol. 2003;17(3):289–303.
Lesser JB, Sanborn KV, Valskys R, Kuroda M. Severe bradycardia during spinal and epidural anesthesia recorded by an anesthesia information management system. Anesthesiology. 2003;99(4):859–66.
Nortcliffe S-A, Shah J, Buggy DJ. Prevention of postoperative nausea and vomiting after spinal morphine for Caesarean section: comparison of cyclizine, dexamethasone and placebo. Br J Anaesth. 2003;90(5):665–70.
Butler R, Fuller J. Back pain following epidural anaesthesia in labour. Can J Anaesth. 1998;45(8):724–8.
Chan YK, Gopinathan R, Rajendram R. Loss of consciousness following spinal anaesthesia for Caesarean section. Br J Anaesth. 2000;85(3):474–6.
Palkar NV, Boudreaux RC, Mankad AV. Accidental total spinal block: a complication of an epidural test dose. Can J Anaesth. 1992;39(10):1058–60.
Singh B, Sharma P. Subdural block complicating spinal anesthesia? Anesth Analg. 2002;94(4):1007–9, table of contents.
Dahlgren N, Törnebrandt K. Neurological complications after anaesthesia. A follow-up of 18,000 spinal and epidural anaesthetics performed over three years. Acta Anaesthesiol Scand. 1995;39(7):872–80.
Gazmuri RR, Ricke CA, Dagnino JA. Trigeminal nerve block as a complication of epidural anesthesia. Reg Anesth. 1992;17(1):50–1.
Sprung J, Haddox JD, Maitra-D’Cruze AM. Horner’s syndrome and trigeminal nerve palsy following epidural anaesthesia for obstetrics. Can J Anaesth. 1991;38(6):767–71.
Evans JM, Gauci CA, Watkins G. Horner’s syndrome as a complication of lumbar epidural block. Anaesthesia. 1975;30(6):774–7.
Day CJ, Shutt LE. Auditory, ocular, and facial complications of central neural block. A review of possible mechanisms. Reg Anesth. 1996;21(3):197–201.
Okell RW, Sprigge JS. Unintentional dural puncture. A survey of recognition and management. Anaesthesia. 1987;42(10):1110–3.
Reynolds F. Damage to the conus medullaris following spinal anaesthesia. Anaesthesia. 2001;56(3):238–47.
Radwan IAM, Saito S, Goto F. The neurotoxicity of local anesthetics on growing neurons: a comparative study of lidocaine, bupivacaine, mepivacaine, and ropivacaine. Anesth Analg. 2002;94(2):319–24, table of contents.
Pollock JE. Neurotoxicity of intrathecal local anaesthetics and transient neurological symptoms. Best Pract Res Clin Anaesthesiol. 2003;17(3):471–84.
Rigler ML, Drasner K, Krejcie TC, Yelich SJ, Scholnick FT, DeFontes J, et al. Cauda equina syndrome after continuous spinal anesthesia. Anesth Analg. 1991;72(3):275–81.
Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth. 2003;91(5):718–29.
Camann WR, Murray RS, Mushlin PS, Lambert DH. Effects of oral caffeine on postdural puncture headache. A double-blind, placebo-controlled trial. Anesth Analg. 1990;70(2):181–4.
Evans RW. Complications of lumbar puncture. Neurol Clin. 1998;16(1):83–105.
González-Carrasco FJ, Aguilar JL, Llubiá C, Nogués S, Vidal-López F. Pneumocephalus after accidental dural puncture during epidural anesthesia. Reg Anesth. 1993;18(3):193–5.
Halker RB, Demaerschalk BM, Wellik KE, Wingerchuk DM, Rubin DI, Crum BA, et al. Caffeine for the prevention and treatment of postdural puncture headache: debunking the myth. Neurologist. 2007;13(5):323–7.
Basurto Ona X, Martínez García L, Solà I, Bonfill Cosp X. Drug therapy for treating post-dural puncture headache. Cochrane Database Syst Rev. 2011;8:CD007887.
Ghaleb A, Khorasani A, Mangar D. Post-dural puncture headache. Int J Gen Med. 2012;5:45–51.
Carter BL, Pasupuleti R. Use of intravenous cosyntropin in the treatment of postdural puncture headache. Anesthesiology. 2000;92(1):272–4.
Carp H, Singh PJ, Vadhera R, Jayaram A. Effects of the serotonin-receptor agonist sumatriptan on postdural puncture headache: report of six cases. Anesth Analg. 1994;79(1):180–2.
Gielen M. Post dural puncture headache (PDPH): a review. Reg Anesth. 1989;14(3):101–6.
Lee LA, Posner KL, Domino KB, Caplan RA, Cheney FW. Injuries associated with regional anesthesia in the 1980s and 1990s: a closed claims analysis. Anesthesiology. 2004;101(1):143–52.
Horlocker TT, Wedel DJ, Rowlingson JC, Enneking FK, Kopp SL, Benzon HT, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med. 2010;35(1):64–101.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Sehmbi, H., Chin, K.J. (2015). Neuraxial Blocks: Spinal and Epidural Anesthesia. In: Regional Nerve Blocks in Anesthesia and Pain Therapy. Springer, Cham. https://doi.org/10.1007/978-3-319-05131-4_41
Download citation
DOI: https://doi.org/10.1007/978-3-319-05131-4_41
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-05130-7
Online ISBN: 978-3-319-05131-4
eBook Packages: MedicineMedicine (R0)