
Abstract
The classical blocks of the brachial plexus using Hirschel’s [1] (axillary approach) and Kulenkampff’s [2] (supraclavicular block) anesthesia have been continuously developed and supplemented with additional access routes. As representative techniques for a multitude of clinical procedures for plexus anesthesia, the axillary perivascular block [3–5], subclavian perivascular block using the Winnie and Collins technique [6], Winnie’s interscalene block [5, 7], and Raj’s infraclavicular approach [8] may be mentioned. All of the blocks of the brachial plexus are based on the concept that the nerve plexus lies within a perivascular and perineural space in its course from the transverse processes to the axilla. Like the epidural space, this space limits the spread of the local anesthetic and conducts it to the various trunks and roots. Within the connective-tissue sheath, the concentration and volume of the local anesthetic used determine the extent of the block’s spread.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
The classical blocks of the brachial plexus using Hirschel’s [1] (axillary approach) and Kulenkampff’s [2] (supraclavicular block) anesthesia have been continuously developed and supplemented with additional access routes. As representative techniques for a multitude of clinical procedures for plexus anesthesia, the axillary perivascular block [3–5], subclavian perivascular block using the Winnie and Collins technique [6], Winnie’s interscalene block [5, 7], and Raj’s infraclavicular approach [8] may be mentioned. All of the blocks of the brachial plexus are based on the concept that the nerve plexus lies within a perivascular and perineural space in its course from the transverse processes to the axilla. Like the epidural space, this space limits the spread of the local anesthetic and conducts it to the various trunks and roots. Within the connective-tissue sheath, the concentration and volume of the local anesthetic used determine the extent of the block’s spread.
The presence of a well defined sheath varies along the course of the brachial plexus. For example, there is not evidence of a substantial sheath on cryomicrotome sections of the supraclavicular region [9].
The axillary sheath is a collection of connective tissue surrounding the neurovascular structures of the brachial plexus. It is a continuation of the prevertebral fascia separating the anterior and middle scalene muscle. Original descriptions of the sheath considered it to be a dense tubular structure extending from above the first rib to a point distal in the axilla. It was believed that the axillary vessels and nerves were all lying loose within its center, implying that conduction anesthesia of the upper extremity could be performed with a single injection at any site along the sheath, with local anesthetic volume being the primary determinant for successful block [5, 6, 10, 11].
However several investigators have since challenged the concept of a tubular axillary sheath proposing instead that the sheath is a multicompartmental structure formed by thin layers of fibrous tissue surrounding the plexus in firmly membranes and extending inward to create discrete fascial septae. Nerves are thus enmeshed in this tissue rather than lying separate and distinct. As a result, individual fascial compartments are created for each nerve and define the anatomic limits for that neural structure. These compartments could functionally limit the circumferential spread of injected solutions, thereby requiring separate injections into each compartment for maximal nerve blockade. However, proximal connections between compartments have been identified, which may account for the success of single injection techniques. Certain clinical observations may be interpreted as offering support or non-support for the existence of a functional tubular sheath [12–15].
Although the clinical significance of these septa remains controversial, it makes sense to inject local anesthetic in divided doses at several locations within the sheath.
Apart from technical aspects, the main differences between the various block procedures are that the injection is made into the interscalene space, the subclavian space, the infraclavicular space, or the axillary space – leading to different focuses for the block.
In this chapter, four techniques that are among the standard methods for plexus anesthesia will be described: the interscalene, supraclavicular, infraclavicular, and axillary blocks of the brachial plexus.
All of these procedures have well-known advantages in contrast with general anesthesia:
-
They can be used on an outpatient basis.
-
Use in patients with a full stomach, high-risk and emergency patients, and patients who are anxious about general anesthesia.
-
Absence of side effects such as nausea and vomiting.
-
Absence of postoperative pulmonary complications.
-
Excellent postoperative pain control, particularly with the use of long-term local anesthetics (continuous procedures).
-
Sympathetic block with vasodilation, better perfusion and faster recovery of traumatized extremities.
Certain points should always be observed when preparing for this procedure:
-
Contraindications must be excluded.
-
The anatomic relationships in each patient must be precisely studied and studied again for repeated blocks.
-
Neurological abnormalities must be excluded.
-
The procedure must be explained to the patient in detail in order to ensure cooperation.
-
The patient must be placed in a comfortable position during the intervention.
-
All patients should be informed of possible side effects and complications; outpatients in particular must also be advised of what they should and should not do after anesthesia or pain treatment.
Anatomy [12–14, 16, 17]
The brachial plexus arises from the union of the spinal nerve roots of C5, C6, C7, C8, and T1, and it often also contains fine fibers from the fourth cervical nerve and second thoracic nerve.
After they have left their intervertebral foramina, the roots of the plexus appear in the interscalene groove between the scalenus anterior and scalenus medius muscles and they join together there to form the primary cords or trunks (Fig. 28.1). The upper roots (C5, C6) form the superior trunk, the roots of C7 continue as the middle trunk, and the inferior trunk arises from the roots of C8 and T1. After passing through the interscalene groove, the primary cords of the plexus, lying close together, move toward the first rib (Fig. 28.2). The suprascapular nerve and subclavian nerve already branch off from the superior trunk here, in the posterior triangle of the neck above the clavicle. When crossing the first rib, the trunks of the plexus lie dorsolateral to the subclavian artery and are enclosed along with the artery by a connective-tissue sheath. The plexus runs through under the middle of the clavicle, following the course of the subclavian artery, into the tip of the axilla (Fig. 28.3). As it does so, each of the primary cords divides into the anterior (ventral) divisions and posterior (dorsal) divisions. These supply the ventral flexor muscles and the dorsal extensor muscles of the upper extremity.

Trunks: (a) superior trunk, (b) medial trunk, (c) inferior trunk, divisions and cords of the brachial plexus. (1) Suprascapular nerve, (2) musculocutaneous nerve, (3) axillary nerve, (4) radial nerve, (5) median nerve, (6) ulnar nerve, (7) medial antebrachial cutaneous nerve, (8) medial brachial cutaneous nerve (With permission from Danilo Jankovic)

Interscalene region. (1) Scalenus anterior muscle, (2) scalenus medius muscle, (3) trunks of the brachial plexus with subclavian artery, (4) proximal supraclavicular plexus sheath, (5) phrenic nerve, (6) ascendent cervical artery, (7) clavicle (With permission from Danilo Jankovic)

Brachial plexus sheath extending from interscalene to subclavian and axillary region. Pectoralis muscle separated. (1) Middle and anterior scalene muscles, (2) trunks of the brachial plexus, (3) sternocleidomastoid muscle, (4) clavicle, (5) infraclavicular region, (6) axillary part of the brachial plexus, (7) deltoid muscle (With permission from Danilo Jankovic)
In the axilla itself, the nerve cords regroup and separate into the individual nerves (Fig. 28.4).

Regrouping of the nerve cords in the area of the axilla and their distal distribution. (1) Lateral cord, (2) musculocutaneous nerve, (3) posterior cord, (4) medial cord, (5) median nerve, (6) radial nerve, (7) ulnar nerve (With permission from Danilo Jankovic)
The ventral branches of the superior and middle trunk combine to form the lateral cord (fasciculus lateralis, C5, C6, C7) (Figs. 28.5, 28.6, and 28.9).

Fascicles (Cords) of the brachial plexus. Lateral cord (white), posterior cord (blue), medial cord (green), axillary artery (red). (1) Trunks of the brachial plexus above the clavicle (2), deltoid muscle (3). Pectoralis major muscle separated (With permission from Danilo Jankovic)

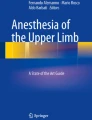
Musculocutaneous nerve (yellow), and median nerve (green), axillary artery (red). (1) deltoid muscle, (2) biceps brachii muscle and coracobrachialis muscle, (3) latissimus dorsi muscle, (4) clavicle (With permission from Danilo Jankovic)
The following nerves emerge from this:
All of the dorsal branches of the three trunks form the posterior cord (fasciculus posterior, C5–8, T1). The end branches of this (Figs. 28.4, 28.5, and 28.9) are the:
-
Radial nerve (Fig. 28.7)
Fig. 28.7 
Radial nerve (green) and axillary nerve (yellow) (With permission from Danilo Jankovic)
-
Axillary nerve (Fig. 28.7)
-
Thoracodorsal nerve (Fig. 28.8)
Fig. 28.8 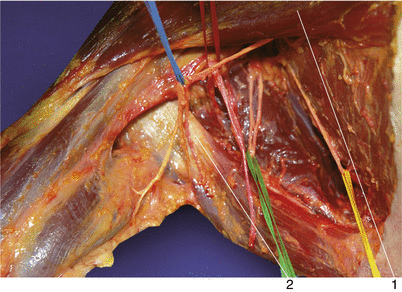
Thoracodorsal nerve (green), thoracicus longus nerve (yellow), intercostobrachial nerve (blue), thoracodorsal artery (red). (1) pectoralis major muscle, (2) latissimus dorsi muscle (With permission from Danilo Jankovic)
-
Inferior subscapular nerve
-
Superior subscapular nerve


The ventral branches of the inferior trunk continue as the medial cord (fasciculus medialis, C8, T1). The following nerves (Figs. 28.4, 28.5, and 28.9) emerge from this:

Brachial plexus, cutaneous innervation (With permission from Danilo Jankovic)
-
Ulnar nerve (Fig. 28.10)
Fig. 28.10 
Ulnar nerve (light blue), median nerve (dark blue), axillary nerve (yellow), radial nerve (green), musculocutaneous nerve (white), axillary artery (red). (1) deltoid muscle, (2) latissimus dorsi muscle, (3) axillary vein (With permission from Danilo Jankovic)
-
Medial pectoral nerve
-
Medial antebrachial cutaneous nerve
-
Medial brachial cutaneous nerve

Suggested Reading
Hirschel G. Anästhesierung des Plexus brachialis bei Operationen an der oberen Extremität. Münchn Med Wschr. 1911;58:1555–6.
Kulenkampf D. Die Anästhesierung des Plexus brachialis. Dtsch med Wschr. 1912;38:1878–80.
Blanchard J, Ramamurthy S. Brachial plexus. In: Benumof LD, editor. Clinical procedures in anesthesia and intensive care. Philadelphia: Lippincott; 1992.
Hickey R, Rogers J, Hoffman J, Ramamurthy S. Comparison of the clinical efficacy of three perivascular techniques for axillary brachial plexus block. Reg Anesth. 1993;18:335–8.
Winnie AP, Radonjic R, Akkineni SR, Durrani Z. Factors influencing distribution of local anesthetics injected into the brachial plexus sheath. Anesth Analg. 1979;58:225–34.
Winnie AP, Collins VJ. The subclavian perivascular technique of brachial plexus anesthesia. Anesthesiology. 1964;25:353–63.
Winnie AP. Interscalene brachial plexus block. Anesth Analg. 1970;49:455–66.
Raj PP, Montgomery SJ, Nettles D, Jenkins MT. Infraclavicular brachial plexus block – a new approach. Anesth Analg. 1973;52:897–904.
Hogan QH, Ericson SJ. MR imaging of the stellate ganglion. Normal appearance. AJR Am J Roentgenol. 1992;158:655–9.
De Jong RH. Axillary block of the brachial plexus. Anesthesiology. 1961;22:215–25.
De Jong RH. Modified axillary block. Anesthesiology. 1965;26:615.
Neal J, Gerancher JC, Hebl J, Ilfeld B, et al. Upper extremity regional anesthesia. Essentials of our current understanding, 2008. Reg Anesth Pain Med. 2009;34(2):134–71.
Pertridge BL, Benirschke F. Functional anatomy of the brachial plexus sheath: implications for anesthesia. Anesthesiology. 1987;66:743–7.
Cornisch PB, Greenfield LJ. Brachial plexus anatomy. Reg Anesth. 1997;22:106–7.
Thompson GE, Rorie DK. Functional anatomy of the brachial plexus sheaths. Anesthesiology. 1983;59:117–22.
Netter FH. Nerve Plexuses and peripheral nerves. In: Netter FH, editor. Nervous system. (Volume 1): neuroanatomy and physiology. The Ciba Collection of Medical Illustrations, 14 Henderson Drive, West Caldwell, NJ 07006. Ciba-Geigy; 1991.
Kahle W. Taschenatlas der Anatomie. Band 3. Nervensystem und Sinnesorgane. Stuttgart/New York: Thieme; 2001.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Jankovic, D. (2015). Brachial Plexus (Introduction and Anatomy). In: Regional Nerve Blocks in Anesthesia and Pain Therapy. Springer, Cham. https://doi.org/10.1007/978-3-319-05131-4_28
Download citation
DOI: https://doi.org/10.1007/978-3-319-05131-4_28
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-05130-7
Online ISBN: 978-3-319-05131-4
eBook Packages: MedicineMedicine (R0)