
Abstract
Although athletic muscle injuries are very frequent, a consistent and comprehensive classification system as well as a clear terminology were so far missing. In order to facilitate effective communication among medical practitioners and to support the development of systematic treatment strategies, we developed practical and systematic definitions of muscle injuries as well as a new and comprehensive classification system, both based on an international consensus meeting.
The classification system differentiates basically between (A) indirect and (B) direct muscle injuries and within the indirect muscle injuries between (1) functional muscle disorders, describing disorders without macroscopic evidence of fiber tear, and (2) structural muscle injuries with macroscopic evidence of fiber tear, i.e., structural damage. Subclassifications are presented for each type.
This comprehensive classification system is proven in the daily practice and scientifically validated. It will help to improve clarity of communication for diagnostic and therapeutic purposes and can serve as the basis for future comparative studies to address the continued lack of systematic information on muscle injuries in the literature.
NOTE: Since this book chapter is based on consensus statements published not before October 2012 (Epub ahead of print), the new nomenclature and classification used in this chapter is not yet reflected consistently in all chapters of this book.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1.1 Introduction
Muscle injuries are a substantial problem for athletes. They constitute 31 % of all injuries in elite football (soccer) [12]; thigh muscle injuries are the most common diagnosis in track and field athletes with 16 % [24, 25]. Their relevance has also been documented in many other sports like rugby (10.4 %) [23], basketball (17.7 %) [5], and American football (46/22 % practice/games) [14].
Muscles that are frequently involved in injuries are often biarticular [19] or have a more complex architecture (e.g., adductor longus). They usually undergo eccentric contraction and contain primarily fast-twitch type 2 muscle fibers [1, 30]. Ninety-two percent of all muscle injuries affect the four major muscle groups of the lower limbs: hamstrings (37 %), adductors (23 %), quadriceps (19 %), and calf muscles (13 %) [12]. Sixteen percent of muscle injuries in soccer are reinjuries and cause significantly longer absence times than the initial injuries [12].
Particularly in elite athletes, where decisions regarding return to play and player availability have significant financial or strategic consequences for the player and the team, there is an enormous interest in optimizing the diagnostic, therapeutic, and rehabilitation process after muscle injuries in order to minimize the absence from sport and to reduce recurrence rates.
However, little information is available in the international literature about muscle injury definitions and classification systems. Since injury definitions are not standardized and guidelines are missing, proper assessment of muscle injury and communication between practitioners are often difficult to achieve [29]. Moreover, it has been documented that variability between definitions creates significant differences in study results and conclusions [7, 17, 20]. Thus, it is critically important to establish a standardization. Muscle strain, for example, presents one of the most frequently used terms to describe athletic muscle injury, but this term is still without clear definition and used with high variability [29].
The aim of this book chapter is to present a standardized English terminology for muscle injuries in order to improve diagnostic, therapeutic, and scientific communication. The standardized definitions were established in a consensus meeting of international sports medicine experts working in the field of muscle injuries.
In addition, an empirically based comprehensive and practical classification system is presented that reflects the differentiated spectrum of muscle injuries seen in athletes. This classification was recently published as a consensus statement [29]. It is based on an extensive, long-term experience and has been used successfully in the daily management of athletic muscle injuries.
It has to be pointed out that this book chapter is mainly based on the 2013 publication by Mueller-Wohlfahrt et al. in British Journal of Sports Medicine.
1. Terminology
Even among sports experts, considerable inconsistency exists in the use of muscle injury terminology. There is no clear definition, differentiation, and use of several terms like strain, tear, pulled muscle. To evaluate the currently used English terminology of athletic muscle injuries, a survey of sports medicine experts was conducted by the authors. The results confirmed that even among experts working frequently with athletic muscle injuries at the elite level, considerable inconsistency exists in the use of muscle injury terminology.
After this survey, a consensus meeting of 15 international experts on the basic science of muscle injury as well as sports medicine specialists involved in the daily care of premier professional sports and national teams was established. The meeting was endorsed by the International Olympic Committee (IOC) and the Union of European Football Associations (UEFA).
In the consensus meeting, practical and systematic scientific terms of muscle injuries were defined. In addition, a new comprehensive classification system was developed.
The following consensus definitions were established:
1.1 Functional (=non-structural) Muscle Disorder
“Acute indirect muscle disorder without macroscopic evidence (in MRI or ultrasound) of muscular tear.
Often associated with circumscribed increase of muscle tone (muscle firmness) in varying dimensions and predisposing to tears. Based on the etiology several subcategories of functional muscle disorders exist.”
According to Fuller et al., a sports injury is defined as “any physical complaint sustained by an athlete that results from a match/competition or training, irrespective of the need for medical attention or time loss from sportive activities” [15]. That means also irrespective of a structural damage. By this definition, functional muscle disorders, irrespective of any structural muscle damage, are injuries as well. However, the term disorder better differentiates functional disorders from structural injuries. Thus, the term functional muscle disorder was specifically chosen by the consensus conference.
Functional muscle disorders are indirect injuries, i.e., not caused by external force, and present a distinct clinical entity. They result in a functional limitation for the athlete, e.g., painful increase of the muscle tone which can represent a risk factor for structural injury. However, they are not readily diagnosed with standard diagnostic methods such as MRI since they are without macroscopic evidence of structural damage, defined as absence of fiber tear on MRI.
A recent UEFA muscle injury study has demonstrated the relevance of functional muscle disorders in football/soccer [13]. This study included data from a 4-year observation period of MRI obtained within 24–48 h after injury and demonstrated that the majority of injuries (70 %) were without signs of fiber tear. However, these injuries caused more than 50 % of the absence of players in the clubs [13].
1.2 Structural Muscle Injury
“Any acute indirect muscle injury with macroscopic evidence (in MRI or ultrasound) of muscle tear.”
It must be pointed out that MRI is usually precise enough to determine if there is a relevant tear or not. However, MRI alone is not appropriate to determine the diagnosis and extent of a muscle injury. Careful combination of diagnostic modalities including medical history, inspection, clinical examination, and imaging will most likely lead to an accurate diagnosis, not imaging alone.
For example, the history of a sharp acute onset of pain, experience of a snap, and a well-defined localized pain with positive MRI for edema but indecisive for fiber tear strongly suggest a minor partial muscle tear, below the detection sensitivity of the MRI. Edema, or better the increased fluid signal on MRI, would be observed with a localized hematoma and would be consistent with the working diagnosis in this case. The diagnosis of a small tear (structural defect) that is below the MRI detection limit is important in our eyes, since even a small tear is relevant because it can further disrupt, e.g., when the athlete sprints.
1.3 Strain and Tear
Strain represents certainly one of the most frequently used terms to describe athletic muscle injury. Hägglund et al. defined it as “acute distraction injury of muscles and tendons” [17]. However, this definition is rarely used in the literature and in the day-to-day management of athletic muscle injuries.
Strain is a biomechanical term which is not defined and used indiscriminately for anatomically and functionally different muscle injuries. Some authors use strain exclusively as a term for “grade I injuries” or “minor muscle injuries” involving only a few muscle fibers [9], whereas others subsume different grades of injuries ranging from mild to severe [25, 30]. Again other authors differentiate strain from ruptures.
Thus, we do not recommend the use of this term. Instead, we propose to use the term tear (which has the same meaning like rupture) for structural injuries of muscle fibers/bundles leading to loss of continuity and contractile properties. Tear better reflects structural characteristics as opposed to a mechanism of injury.
The following terms are without specific recommendation:
-
Strain – See above.
-
Pulled muscle – A lay term for different, undefined types or grades of muscle injuries and cannot be recommended as a scientific term.
(Further recommended consensus definitions are presented below together with the new classification system.)
1.2 Classification
Usually, researchers compare the results from their study with results from other published studies. But comparisons of different muscle injuries and layoff times can only be made between studies with essentially the same injury definitions and classification system. Since so far no universal and comprehensive classification existed that includes all types of athletic muscle injuries, the significant methodological differences between studies do not allow for comparison between study results [10].
Different classification systems are published in the literature (Table 1.1), but no system is consistently used within studies and in daily practice [8]. Most of the grading systems classify acute muscle injuries as grade 1, 2, and 3. However, this does not accurately reflect the occurrence of muscle injuries in athletes. Previous systems are either based upon clinical signs or upon imaging.
All previous grading systems lack subclassifications within the grades or types. In consequence, injuries with a different etiology, treatment pathway, and prognostic relevance are categorized in the same group. Moreover, no terminology or grading system (sub)classified disorders without macroscopic evidence of structural damage, even though a muscle injury study of the Union of European Football Associations (UEFA) has emphasized their high clinical relevance in professional athletes, as mentioned above [13].
The most recently published classification system by Chan et al. is imaging based, even though many authors have stated that diagnosis and prognosis of muscular injuries are normally mainly based on clinical findings and radiological methods such as MRI or ultrasound are used for additional information in order to confirm a diagnosis [13, 22].
1.2.1 Diagnosis
Our approach is to include the combination of the currently best available diagnostic tools. Careful combination of diagnostic modalities including medical history, inspection, clinical examination, and imaging will most likely lead to an accurate diagnosis, rather than relying on imaging alone.
In accordance with Askling et al. and Järvinen et al., we recommend to start with a precise history of occurrence, circumstances, symptoms, and previous problems, followed by a careful clinical examination with inspection, palpation of the injured area, comparison to the other side, and testing of the function of the muscles [2, 19]. Palpation serves to detect (more superficial and larger) tears, perimuscular edema, and increased muscle tone. An early post-injury ultrasound provides helpful information about any existing disturbance of the muscle structure and reveals if further MR imaging is needed.
1.2.2 Imaging
Imaging (ultrasound and MRI) definitely provides additional information about a muscle injury. It helps to localize the site of injury to reveal if there is any hematoma and a defect/tear including its approximate size in the muscle tissue and if the tendon is involved. Especially MRI is helpful to determine edema incidence and pattern. However, diagnosis based only on imaging is not appropriate. Even the best imaging reveals no information about the muscle tone, pain, functional loss, and other information such as previous injuries, which has significant relevance for the management of the athlete.
In daily practice ultrasound is sufficient in many cases to localize the site of injury and to exclude higher grade of injury. Ultrasound is easily available and cost-effective which makes it superior to MRI for follow-up examinations. However, it must be pointed out that examination of skeletal muscle takes time. With a little practice, the examiner can distinguish a functional muscle disorder without evidence of structural damage from a structural injury with a tissue defect. We recommend to use a 7.5 or 10.0 MHz transducer and to start with a transversal section. A complete scan through the muscle should be performed to obtain anatomical orientation. The longitudinal section is added on locations where a disturbance of the muscle structure or a gap is suspected. Ultrasound can also assess the need for further investigation by MRI. We recommend MRI in every case that is suspicious for structural injury.
High-resolution imaging is required for precise diagnosis. However, quality of MR imaging differs a lot since many radiologists choose a large field of view demonstrating, for example, both thighs including the pelvis in one examination (even though the clinical question is, e.g., only to search for a partial muscle tear in the biceps femoris muscle). Combination with clinical examination is critical to make MRI more sensitive.
The argument that large field-of-view MRI is the best initial test in order not to miss some muscle injuries is only relevant if no clinical and ultrasound examination was done before MRI, what usually should not happen. With clinical examination, the field of view can easily be limited. This will lead to a much higher spatial resolution.
We recommend a high field strength with a minimum of 1.5 or better 3 T, the use of surface coils, a limited field of view based on clinical examination and ultrasound, the use of skin markers to localize the center of injury, and a multiplanar orientation. Three millimeter slices must be postulated for MR imaging in muscle injuries. Otherwise smaller tears could be missed. With a limited field of view in MRI, this does not cause additional examination time.
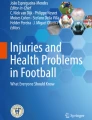
But even in best quality, MRI alone is not sensitive enough to measure the extent of muscle tissue damage accurately. For example, it is not possible to judge from the scans where edema/hemorrhage (seen as high signal) is obscuring muscle tissue that has not been structurally damaged (Figs. 1.1 and 1.2).

Demonstrates clearly how important resolution and field of view are for interpreting MR imaging (Reprinted with permission of UEFA [41]). In (a) it is not possible to judge from the images if there is a structural defect or not, due to overlaying bright signal. (b) Performed in high-resolution technique (3 T, coil, limited field of view, 3 mm slice, etc.) demonstrating more clearly the actual defect in the muscle structure

Demonstrates that contrast and brightness (adjustable on the radiological monitors) play a crucial role for interpretation of muscle injuries (Reprinted with permission of UEFA [41]). (a) High brightness and little contrast demonstrating a large muscle tear. (b) After adjusting contrast and brightness, the actual defect in the muscle appears much smaller
Imaging technology to detect muscle injuries continues to evolve, and future techniques may allow for more sensitive and specific visualization of muscle injury and pathology.
1.2.3 New Comprehensive Classification System
The presented muscle injury classification is based on an extensive, long-term experience and has been used successfully in the daily management of athletic muscle injuries. The classification is empirically based and includes several original aspects of athletic muscle injuries that have not yet been described in the literature, specifically the frequently observed functional muscle disorders. Distinguishing these injuries as separate clinical entities has great relevance for the successful management of the athlete with muscle injury and represents the basis for future comparative studies since scientific data are limited for muscle injury in general.
This advanced comprehensive classification system differentiates between indirect and direct muscle injuries. Indirect muscle injuries are divided into functional and structural ones. Functional muscle disorders (type 1, overexertion-related, and type 2, neuromuscular muscle disorders) describe disorders without macroscopic evidence of fiber tear. Structural muscle injuries (type 3, partial tears, and type 4, (sub)total tears/tendinous avulsions) are injuries with macroscopic evidence of fiber tear, i.e., structural damage. Subclassifications are presented for each type.
1.2.3.1 Functional (=non-structural) Muscle Disorders
Functional muscle disorders are multifactorial. They can be grouped into subgroups reflecting their clinical origin: “overexertional” and “neuromuscular” muscle disorders. This is important since the origin of muscle disorder influences their treatment pathway. A spine-related muscle disorder associated with a spine problem (e.g., spondylolysis) will respond better to treatment by addressing not only the muscle disorder itself but also the original back problem. One could argue that this presents mainly a back problem with a secondary muscle disorder. However, this secondary muscular disorder prevents the athlete from sports participation and will require comprehensive treatment that includes the primary problem as well in order to facilitate return to sport. Thus, a differentiation is important not only because of the different pathogenesis but more importantly because of different therapeutic implications.
1.2.3.1.1 Overexertion-Related Muscle Disorders
Weakened or fatigued muscles absorb less energy and are therefore more likely to get injured [16]. Previous data has shown that muscle fatigue predisposes the athlete to muscle injury [33, Wilson AJ and Myers PT, 2005, unpublished data]. Thus, muscle fatigue due to overexertion and other factors, which frequently presents as firmness of a muscle (bundle or part), must be recognized and treated.
Delayed onset muscle soreness has to be differentiated from fatigue-induced muscle injury [4]. DOMS occurs several hours after unaccustomed deceleration movements while the muscle is stretched by external forces (eccentric contractions), whereas fatigue-induced muscle disorder can also occur during athletic activity. DOMS resolves spontaneously usually within a week. In contrast, fatigue-induced muscle disorder can – if unrecognized and untreated – persist over a longer time and may cause structural injuries such as partial tears.
1.2.3.1.2 Neuromuscular Muscle Disorders
The term neuromuscular was chosen by the consensus group to describe the specific pathogenesis of these muscle disorders. Two different types of neuromuscular disorders can be differentiated: a spinal or spinal nerve-related (central) and a neuromuscular end plate-related (peripheral) type.
Muscles act as a target organ and their state of tension is modulated by electrical information from the motor component of the corresponding spinal nerve. Thus, irritation of a spinal nerve root can cause an increase in muscle tone. It is known that back injuries are very frequent in elite athletes [32] and lumbar pathology such as disc prolapse at the L5/S1 level may present with hamstring and/or calf pain and limitations in flexibility, which may result in or mimic a muscle injury [34]. It is logical that this type of injury would require variable forms of treatment beyond simple treatment of the muscle–tendon injuries [18]. Thus, it is important that assessment of muscle injury should include a thorough biomechanical evaluation, especially that of the lumbar spine, pelvis, and sacrum. Negative structural findings on the lumbar spine do not exclude nerve root irritation. Functional lumbar dysfunctions, like lumbar or iliosacral blocking, can also cause spine-related muscle disorders [28]. The diagnosis is then established through precise clinical functional examination. The spine-related muscle disorder is usually MRI negative or shows muscle edema only [34]. Verrall et al. showed that footballers with a history of lumbar spine injury had a higher rate of MRI-negative posterior thigh injury, but not of actual structural hamstring injury [42].
We differentiate muscle-related neuromuscular disorders from the spine-related ones because of different treatment pathways. Dysfunction of neuromuscular control mechanisms can result in a painful muscle firmness which can prevent an athlete from sportive activities, when inhibition of antagonistic muscles is disturbed and agonistic muscles over-contract to compensate this [6].
It has to be stated that it remains an area for future research to definitely describe the functional muscle disorders and other risk factors for muscle injuries.
1.2.3.2 Structural Injuries
1.2.3.2.1 Partial Muscle Tears
Most indirect structural injuries are partial muscle tears. Clinical experience clearly shows that most partial injuries can be assigned to one of two types, either a minor or a moderate partial muscle tear, which ultimately has consequences for therapy and absence time from sports. Thus, indirect structural injuries should be subclassified. Since previous graduation systems refer to the complete muscle size, they are relative and not consistently measurable. In addition to this, there is no differentiation of grade 3 injuries with the consequence that many structural injuries with different prognostic consequences are subsumed as grade 3.
Anatomical facts should be considered while discussing muscle injury and classification: The individual muscle fiber presents a microscopic structure with an average diameter of 60 μm [38]. Therefore, an isolated tear of a single muscle fiber remains without clinical relevance. Muscle fibers are anatomically organized into primary and secondary muscle fascicles/bundles. Multiple secondary bundles constitute the muscle.
The extent of the injury to the anatomic landmarks determines the difference between minor and moderate partial muscle tear. However, it definitely remains a challenge for future studies to determine the exact cutoff.
Besides size, the involvement of adjacent connective tissue (endomysium, perimysium, epimysium, and fascia) distinguishes partial muscle tears from each other. Concomitant injury of the external perimysium seems to play a special role: This connective tissue structure somehow has an intramuscular barrier function in case of bleeding. It may be the injury to this structure (with optional involvement of the muscle fascia) that differentiates a moderate from a minor partial muscle tear.
However, drawing a clear differentiation between partial muscle tears seems difficult because of the heterogeneity of the muscles that can be structured very differently. Technical diagnostic tools today (MRI and ultrasound) are not precise enough to ultimately determine and prove the effective muscular defect within the injury zone of hematoma and/or liquid seen in MRI, which can [19] lead to overestimation of the actual damage. It will remain a challenge for future studies to exactly define the size of the injury which describes the distinction between a minor and a moderate partial muscle tear.
The great majority of muscle injuries heal without formation of scar tissue. However, greater muscle tears can result in a defective healing with scar formation [19] which has to be considered in the diagnosis and prognosis of a muscle injury. Our experience is that partial tears of less than a muscle fascicle usually heal completely, while moderate partial tears can result in a fibrous scar.
1.2.3.2.2 (Sub)Total Muscle Tears and Tendinous Avulsions
Complete muscle tears with a discontinuity of the whole muscle are very rare. Subtotal muscle tears and tendinous avulsions are more frequent. Clinical experience shows that injuries involving more than 50 % of the muscle diameter (subtotal tears) usually have a similar healing time compared with complete tears.
Tendinous avulsions are included in the classification system since they are biomechanically complete tears of the origin or insertion of the muscle. The most frequently involved locations are the proximal rectus femoris, the proximal hamstrings, the proximal adductor longus, and the distal semitendinosus.
Intratendinous lesions of the free or intramuscular tendon also occur. Pure intratendinous lesions are rare. The most frequent type is a tear near the musculotendinous junction (e.g., of the intramuscular tendon of the rectus femoris muscle). Tendinous injuries are either consistent with the partial (type 3) or (sub)total (type 4) tear in our classification system and can be included in that aspect of the classification.
1.2.3.2.3 Muscle Contusions
In contrast to indirect injuries (caused by internal forces), lacerations or contusions are caused by external forces [3, 21] like a direct blow from an opponent’s knee. Thus, muscle contusions are classified as acute direct muscle injuries (Tables 1.1 and 1.2).
Contusion injuries are common in athletes and present a complex injury that includes defined blunt trauma of the muscular tissue and associated hematoma [3, 21]. The severity of the injury depends on the contact force, the contraction state of the affected muscle at the moment of injury, and other factors. Contusions can be graded into mild, moderate, and severe [37]. The most frequently injured muscles are the exposed rectus femoris and the intermediate vastus, lying next to the bone, with limited space for movement when exposed to a direct blunt blow. Contusion injury can lead to either diffuse or circumscribed bleeding that displaces or compresses muscle fibers causing pain and loss of motion. It happens that muscle fibers are torn off by the impact or by shear forces, but muscle fibers are not typically torn by longitudinal distraction. Therefore, contusions are not necessarily accompanied by a structural damage of muscle tissue. For this reason athletes, even with more severe contusions, can often continue playing for a long time, whereas even a smaller indirect structural injury often forces the player to stop at once. However, contusions may lead to persistent intramuscular bleeding and hematoma formation with the potential for severe complications such as acute or delayed compartment syndrome and possible resultant long-term functional limitation [26, 27].
1.3 Conclusion
Consensus definitions of the English terminology of athletic muscle injuries as well as a new comprehensive and empirical classification system for acute muscle injuries are presented. Both will help to improve effective communication among medical practitioners and development of systematic treatment strategies and can serve as the basis for future comparative studies to address the continued lack of systematic information on muscle injuries in the literature.
Key component of the new classification system is the differentiation between indirect and direct muscle injuries and within the indirect injuries between functional muscle disorders from structural injuries. The use of the term strain is no longer recommended, since it is a biomechanical term, not well defined, and used indiscriminately for anatomically and functionally different muscle injuries. Instead, we propose the term tear for structural injuries, graded into (minor and moderate) partial and (sub)total tears, used only for muscle injuries with macroscopic evidence of muscle damage (structural injuries). While this classification is most applicable to lower limb muscle injuries, it can be translated also to the upper limb.
Scientific data supporting the presented classification system can be found in the publication “Return to play after thigh muscle injury in elite football players: implementation and validation of the Munich muscle injury classification” by Ekstrand J, Askling C, Magnusson H, and Mithoefer K in the British Journal of Sport Medicine [11]. Further scientific data are still missing. We hope that the suggested standardized terminology and the new classification system will stimulate research to prospectively evaluate the prognostic and therapeutic implications of the new classification. Furthermore, future studies have to define the exact size threshold between a minor and a moderate partial muscle tear.
Note: Further information about the consensus definitions and the new classification system can be found in
Mueller-Wohlfahrt HW, Haensel L, Mithoefer K, Ekstrand J, English B, McNally S, Orchard J, van Dijk N, Kerkhoffs G, Schamasch P, Blottner D, Swaerd L, Goedhart E, Ueblacker P. Terminology and classification of muscle injuries in sport. A consensus statement. Br J Sports Med. 2013;47(6):342–50.
References
Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001;29(4):521–33.
Askling CM, Tengvar M, Saartok T, Thorstensson A. Acute first-time hamstring strains during high-speed running: a longitudinal study including clinical and magnetic resonance imaging findings. Am J Sports Med. 2007;35:197–206.
Beiner JM, Jokl P. Muscle contusion injuries: current treatment options. J Am Acad Orthop Surg. 2001;9:227–37.
Boening D. Delayed-onset muscle soreness (DOMS). Dtsch Arztebl. 2002;99(6):372–7.
Borowski LA, Yard EE, Fields SK, Comstock RD. The epidemiology of US high school basketball injuries, 2005–2007. Am J Sports Med. 2008;36(12):2328–35.
Brenner B, Maassen N. Basic physiology and aspects of exercise. In: Mueller-Wohlfahrt HW, Ueblacker P, Haensel L, editors. Muscle injuries in sports. Stuttgart/New York: Thieme; 2013.
Brooks JH, Fuller CW. The influence of methodological issues on the results and conclusions from epidemiological studies of sports injuries: illustrative examples. Sports Med. 2006;36(6):459–72.
Bryan Dixon J. Gastrocnemius vs. soleus strain: how to differentiate and deal with calf muscle injuries. Curr Rev Musculoskelet Med. 2009;2(2):74–7.
Chan O, Del Buono A, Best TM, Maffulli N. Acute muscle strain injuries: a proposed new classification system. Knee Surg Sports Traumatol Arthrosc. 2012;20(11):2356–62.
Ekstrand J. Epidemiology of muscle injuries in soccer. In: Mueller-Wohlfahrt HW, Ueblacker P, Haensel L, editors. Muscle injuries in sports. Stuttgart/New York: Thieme; 2013.
Ekstrand J, Askling C, Magnusson H, Mithoefer K. Return to play after thigh muscle injury in elite football players: implementation and validation of the Munich muscle injury classification. Br J Sports Med. 2013;47(12):769–74.
Ekstrand J, Hagglund M, Walden M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. 2011;39(6):1226–32.
Ekstrand J, Healy JC, Walden M, Lee JC, English B, Hagglund M. Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play. Br J Sports Med. 2012;46(2):112–7.
Feeley BT, Kennelly S, Barnes RP, Muller MS, Kelly BT, Rodeo SA, Warren RF. Epidemiology of National Football League training camp injuries from 1998 to 2007. Am J Sports Med. 2008;36(8):1597–603.
Fuller CW, Ekstrand J, Junge A, Andersen TE, Bahr R, Dvorak J, Hägglund M, McCrory P, Meeuwisse WH. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Clin J Sport Med. 2006;16(2):97–106.
Gielen JL, Robinson P, van Dyck P, van der Stappen A, Vanhoenacker FM. Muscle injuries. In: Vanhoenacker FL, Maas M, Gielen JL, editors. Imaging of orthopedic and sports injuries. Berlin/Heidelberg/New York: Springer; 2007.
Hagglund M, Walden M, Bahr R, Ekstrand J. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sports Med. 2005;39(6):340–6.
Hoskins WT, Pollard HP. Successful management of hamstring injuries in Australian Rules footballers: two case reports. Chiropr Osteopat. 2005;13(1):4.
Jarvinen TA, Jarvinen TL, Kaariainen M, Kalimo H, Jarvinen M. Muscle injuries: biology and treatment. Am J Sports Med. 2005;33(5):745–64.
Junge A, Dvorak J, Graf-Baumann T, Peterson L. Football injuries during FIFA tournaments and the Olympic Games, 1998–2001: development and implementation of an injury-reporting system. Am J Sports Med. 2004;32(1 Suppl):80S–9.
Kary JM. Diagnosis and management of quadriceps strains and contusions. Curr Rev Musculoskelet Med. 2010;3:26–31.
Kerkhoffs GM, van Es N, Wieldraaijer T, Sierevelt IN, Eksrand J, van Dijk CN. Diagnosis and prognosis of acute hamstring injuries in athletes. Knee Surg Sports Traumatol Arthrosc. 2013;21(2):500–9.
Lopez Jr V, Galano GJ, Black CM, Gupta AT, James DE, Kelleher KM, Allen AA. Profile of an American amateur rugby union sevens series. Am J Sports Med. 2012;40(1):179–84.
Malliaropoulos N, Isinkaye T, Tsitas K, Maffulli N. Reinjury after acute posterior thigh muscle injuries in elite track and field athletes. Am J Sports Med. 2011;39(2):304–10.
Malliaropoulos N, Papacostas E, Kiritsi O, Papalada A, Gougoulias N, Maffulli N. Posterior thigh muscle injuries in elite track and field athletes. Am J Sports Med. 2010;38(9):1813–9.
Mithoefer K, Lhowe DW, Altman GT. Delayed presentation of acute compartment syndrome after contusion of the thigh. J Orthop Trauma. 2002;16(6):436–8.
Mithoefer K, Lhowe DW, Vrahas MS, Altman DT, Erens V, Altman GT. Functional outcome after acute compartment syndrome of the thigh. J Bone Joint Surg Am. 2006;88(4):729–37.
Mueller-Wohlfahrt HW. Diagnostik und Therapie von Muskelzerrungen und Muskelfaserrissen. Sportorthopaedie-Sporttraumatologie. 2001;17:17–20.
Mueller-Wohlfahrt HW, Haensel L, Mithoefer K, Ekstrand J, English B, McNally S, Orchard J, van Dijk N, Kerkhoffs G, Schamasch P, Blottner D, Swaerd L, Goedhart E, Ueblacker P. Terminology and classification of muscle injuries in sport. A consensus statement. Br J Sports Med. 2013;47(6):342–50.
Noonan TJ, Garrett Jr WE. Muscle strain injury: diagnosis and treatment. J Am Acad Orthop Surg. 1999;7(4):262–9.
O’Donoghue DO, editor. Treatment of injuries to athletes. Philadelphia: WB Saunders; 1962.
Ong A, Anderson J, Roche J. A pilot study of the prevalence of lumbar disc degeneration in elite athletes with lower back pain at the Sydney 2000 Olympic Games. Br J Sports Med. 2003;37(3):263–6.
Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sports Med. 2012;42(3):209–26.
Orchard JW, Farhart P, Leopold C. Lumbar spine region pathology and hamstring and calf injuries in athletes: is there a connection? Br J Sports Med. 2004;38(4):502–4; discussion 502–4.
Peetrons P. Ultrasound of muscles. Eur Radiol. 2002;12(1):35–43.
Ryan AJ. Quadriceps strain, rupture and Charlie horse. Med Sci Sports. 1969;1:106–11.
Ryan JB, Wheeler JH, Hopkinson WJ, Arciero RA, Kolakowski KR. Quadriceps contusion. West Point update. Am J Sports Med. 1991;19:299–304.
Schuenke M, Schulte E, Schumacher U, editors. Atlas of anatomy. Stuttgart/New York: Thieme; 2005.
Stoller DW, editor. MRI in orthopaedics and sports medicine. 3rd ed. Philadelphia: Wolters Kluwer/Lippincott; 2007.
Takebayashi S, Takasawa H, Banzai Y, Miki H, Sasaki R, Itoh Y, Matsubara S. Sonographic findings in muscle strain injury: clinical and MR imaging correlation. J Ultrasound Med. 1995;14(12):899–905.
Ueblacker P, Hänsel L, Müller-Wohlfahrt HW. UEFA Football Doctor Education Programme - Workshop 2 Course Manual “Injury Diagnosis and Treatment”, Chapter 4 “Examination and treatment of muscle injuries”. 2013, www.uefa.org.
Verrall GM, Slavotinek JP, Barnes PG, Fon GT, Spriggins AJ. Clinical risk factors for hamstring muscle strain injury: a prospective study with correlation of injury by magnetic resonance imaging. Br J Sports Med. 2001;35(6):435–9; discussion 440.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Ueblacker, P., Hänsel, L., Müller-Wohlfahrt, HW., Mithoefer, K., Ekstrand, J. (2014). Terminology and Classification of Athletic Muscle Injuries. In: Kerkhoffs, G., Servien, E. (eds) Acute Muscle Injuries. Springer, Cham. https://doi.org/10.1007/978-3-319-03722-6_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-03722-6_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-03721-9
Online ISBN: 978-3-319-03722-6
eBook Packages: MedicineMedicine (R0)