
Abstract
Cuba is a developing country at an advanced stage of ageing, with a population growth rate around zero since 2006. The Cuban population shows a high life expectancy (77 years in 2007) and low infant mortality (below 5 per thousand births). Nonetheless, it has maintained a small sex gap (around 4 years) in life expectancy at birth over the last century. This paper examines the evolution of life expectancy at birth, and trends in specific causes of death. The differentials in life expectancy by sex and across time are examined in order to shed light on the narrower sex gap that Cuba shows compared to other countries. Data on population and specific death rates published by the National Statistics and Information Office and Public Health Ministry of Cuba are used. We decompose the mortality rates to determine the impact of age- and cause- specific death rates on the sex differential at three points in time; and on the life expectancy of each sex, from 1987 to 1995, and 1995 to 2007. Our results show that Cuba presents a mix of mortality patterns, with most of the deaths attributable to chronic or degenerative diseases. However, there is also a sizeable proportion of avoidable deaths such as those due to external causes, respiratory diseases or diabetes. Differences between periods are clear. During the economic crisis, male survivorship was seriously constrained while females barely kept their advantage of half of a year; but, in the recovery period, males recovered faster than females.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
11.1 Introduction
During the last century, most of the developed world experienced a steady increase in life expectancy at birth. From the beginning of the Twentieth century until the sixties, when it was overtaken by Sweden, the record life expectancy was held by the Netherlands. Since the end of the seventies Japan has been in the lead, with a life expectancy reaching 83 years in 2009 (Human Mortality Database: www.mortality.org). This substantial increase in longevity has been accompanied by a widening of the gap in life expectancy between males and females: females have consistently had a life expectancy advantage of between 3 and 8 years.
These two phenomena have been extensively studied. The first one, the increase in life expectancy at birth, depends directly on mortality patterns. The rise of this indicator was due to the mortality decline, firstly for age group 1–4, and then an overall decline in infant mortality. As life expectancy at birth is a measure of mortality averaged over all ages, once infant mortality reaches very low levels, the gains in life expectancy depend more on mortality rates at older ages (Christensen et al. 2009). Moreover, whenever there is an abrupt increase or decrease in mortality, we need to turn to an analysis of its components, that is, mortality at various ages, in order to understand the changes (Bongaarts and Feeney 2002; Oeppen and Vaupel 2002).
Epidemiological Transition Theory elaborates upon the changes in mortality patterns, and affirms that mortality shows several stages in its evolution: from an early stage characterized by infections and parasitic diseases it has evolved into one where chronic and degenerative conditions predominate (Omran 1971). Other studies (Nathanson 1984; Rogers and Hackenbert 1987) have emphasized that risk behaviour and lifestyle are linked to death in contemporary high income countries. This implies a mix of mortality patterns from different stages, as has also been argued in the convergence-divergence approach on countries’ life expectancies (Meslé and Vallin 2004).
The second phenomenon, the increase of the sex differential in life expectancy at birth, has been observed all over the world, although developed countries account for its highest growth. Nevertheless, in some of these countries such as Sweden, Spain and France, the sex gap stagnated or even declined at the end of the century. Trovato (2005) has shown that the decline in the sex gap is due to convergence in the main causes of death. There have been fewer men’s deaths due to accidents, violence, lung cancer and suicide, with a consequent improvement in male’s survival. Moreover, this narrowing of the sex gap has also been associated with changes in life style, education and, in general, with the convergence of attitudes and behaviours of both sexes (Annandale and Hunt 2000).
Although this pattern of increasing life expectancy was first observed in the developed world, it has extended to other, less developed countries. According to United Nations Prospect 2007, developed regions had 76.5 years of life expectancy at birth in 2005–2010, while the less developed regions had 65.4 years (11 years less). Most developing countries follow this pattern but, nonetheless, there are some that are already catching up with the group of developed countries. For instance, Barbados, Brunei, Chile, Costa Rica, Cuba and Kuwait are developing countries with more than 77 years of life expectancy at birth in 2005–2010.
Cuban life expectancy increased rapidly until it reached 70 years in 1970. Subsequently, the improvement in life expectancy slowed down but has continued to rise, reaching 77 years in 2000 (30 years later), and 77.97 in the last period for which data is available (2005–2007). Hernández (1986) and Albizu-Campos (2002) have described this evolution as steady over time, but with two periods of slowdown: first during the first two decades of Twentieth century, and between 1985 and 1995.
The improvement in life expectancy over the Twentieth century has been linked to several factors. In particular, there has been a change in mortality patterns, from predominantly infectious diseases (higher for women), to non-infectious diseases, especially since the mid-twentieth century. It is noteworthy that, despite the high life expectancy at birth observed in Cuba, the difference between male and female life expectancies at birth has never exceeded 4 years (González and Ramos 1996).
The focus of our paper is on the changes in life expectancy at birth in Cuba, describing the mortality transformations that have shaped this indicator and the differences between males and females. Cuba’s life expectancy stagnated at the end of the Twentieth century and beginning of the Twenty-First century, with growth being lowest during the nineties (which coincided with an economic crisis in Cuba after the fall of the Soviet Union). We analyse the changes in life expectancy in Cuba at three points in time (1987, 1995 and 2007) looking at the contribution of mortality patterns by age and sex to the sex differential in life expectancy at birth. We also look at trends for each sex through the period 1987–1995 and 1995–2007. In particular, we ask if the narrowing of the sex gap in this period was because males were doing better and catching up with females, or because females were doing worse.
We structure the contents of this article as follows: after describing the data and methods used in the analysis (Sect. 2), the evolution of life expectancy for several countries over the Twentieth century will be analysed in Sect. 3. Section 4 describes the main characteristics of Cuban population and mortality patterns during the three periods. We finish our analysis by decomposing the effect of age-specific causes of death over the sex differential in life expectancy at birth, looking at changes in time and also for each sex (Sect. 5). The final sections present the conclusions, references and annex (Sects. 6 to 8).
11.2 Data and Method
Data on population were acquired from the National Statistic and Information Office of Cuba (Demographic Yearbooks: 2006, 2008 and 2010). Deaths by age, sex, year of death and cause of death come from the Public Health Ministry of Cuba. Mortality data is on a yearly basis and correspond to years 1987, 1995 and 2007. Official Life Tables calculated by the National Statistic Office are used in this study, using those nearest to the years selected, which are: 1986–1987, 1994–1995 and 2005–2007. As we are working with official data, and did not have access to the primary databases, we could not use the corresponding yearly life tables that match the mortality rates. Moreover, for the trends in life expectancy and sex differentials in Cuba, we only have data grouped for 3 or 5 years, so the comparison with yearly data of other countries should be treated with caution.
During the time period covered, deaths were classified according to the International Classifications of Diseases (ICD), ICD-9 until year 2000 and ICD-10 from 2001 onwards. Changes in cause-of-death classification did not have any significant effect on the mortality trend of the relevant causes of death used in our research. Selected causes of death and corresponding ICD codes are given in Annex 1.
To understand the changes in life expectancy and the sex gap we need to look deeply into the mortality patterns and particularly into the contribution of the different causes of death over the life span of each sex. In order to do that, we will apply the decomposition method of Shkolnikov et al. (2001) to determine the impact of age and cause specific death rates on the difference in male and female life expectancy at three points in time, and for each sex at two periods in time.
The difference between two life expectancies may be expressed as:
where \(\varepsilon \) is the contribution to the difference between the life expectancies of population 2 and population 1 produced by the difference in mortality in age groups y to y + n. \(\varepsilon \) is obtained from:
where x is the initial age group; y are exact ages; n is the length of the age interval; W the last age and lx are the survivors at each age. Cause-specific mortality rates (j) are also decomposed and multiplied by equation [11.2], resulting in a matrix with the contribution of ages (rows) and causes of death (columns):
where \({}_{\rm{n}}{{\rm{M}}_{{\rm{y,j}}}}\) is the central death rate in the population (1 or 2) for the age group y, y + n and the cause of death j; and \({}_{\text{n}}{{\text{M}}_{\text{y}}}\) is the central death rates for the total causes of death in the age group y, y + n.
The method allows us to divide up the difference between life expectancies. In our case, we are going to analyse differences between females and males for 1987, 1995 and 2007; and differences between 1987–1995 and 1995–2007 for each sex.
11.3 Trends in Life Expectancy Over the Past Century
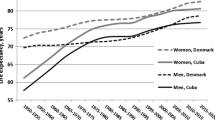
Trends in life expectancy during the twentieth century for specific countries are shown in Fig. 11.1. Although data for different countries do not always coincide in time the overall trends are clear. In the case of Japan, Spain and The Netherlands figures are expressed on a yearly basis, while for Costa Rica, Uruguay, Chile and Cuba they are in five-year intervals, with the exception of the last three years for Cuba that are in a three-year average.

Evolution of Life Expectancy at Birth (in Years) in selected countries. 1900–2008. (Sources: Human Mortality Database (HMD); Latin American and Caribbean Demographic Centre (CELADE); National Statistics Office (ONE), Cuba. *Five-year averages, †Three-year averages for the last 3 years)
As shown in Fig. 11.1, life expectancy at birth experienced the largest improvements during the first half of the twentieth century (with the exception of the World War periods, when it showed a strong drop). For instance, life expectancy in The Netherlands increased by 23 years, while in countries like Spain and Cuba the increase reached around 20 years. This progress was mainly due to scientific discoveries such as antibiotics, sulphas, etc., along with advances in the health and living conditions of the population. It enabled the control and eradication of many infectious and parasitic diseases, and increased infant and children’s survival.
In the second half of the twentieth century, there was a slowdown in the increase of survival in many industrialized countries. Some countries experienced large improvements (around 20 years), catching up with those in the group with the highest levels, like Spain and even surpassing them, like Japan, which has held the record life expectancy at birth since 1972. Furthermore, some developing countries such as Chile, Costa Rica, Uruguay and Cuba had significant increases in this period. From the last part of the twentieth century until the present the indicators have been converging, so that the gap between the countries with the highest and lowest levels, which was almost 20 years in 1950, had been reduced to less than 10 years by 2008.
In the case of Cuba, the trend shows a continuous increase in life expectancy at birth, with the largest improvements between the 1930s and late seventies, when it was very close to that of the countries with the highest levels. However, during the eighties and nineties there was a slowdown in the pace of improvements, which did not recover until the beginning of the twenty-first century. It is this change in the trend of life expectancy that we address in the present paper. By analysing the evolution of mortality differences between and within sexes, we will address the issue of increases in life expectancy, as well as the observed decrease in the pace of improvements.
As life expectancy at birth is markedly different for each sex, we first look at them by analysing the sex differential of life expectancy for selected countries in 1990, 2000 and 2006. We grouped them according to three different behaviours of the sex gap: those that show a continuous decline; a second group where the gap fluctuates; and a third group where the gap first rises and then levels off (Fig. 11.2).

Sex differential of life expectancy at birth for selected countries in 1990, 2000 and 2006. (Sources: Human Mortality Database (HMD); Latin American and Caribbean Demographic Centre (CELADE); National Statistics Office (ONE), Cuba. *Closest life table: 1986–1987, 1998–2000 and 2005–2007)
In the first group (formed by Argentina, USA, The Netherlands and Mexico) the gap ranges from 6 to 7 years in the first observation, and then declines between 4 and 6 years. The second group (Costa Rica and Uruguay) shows a rise and afterwards a drop. Note that although both are developing countries, the sex gap in life expectancy in Uruguay is almost double that in Costa Rica. The last group includes Japan and Cuba. Despite being at different levels, they experienced a similar development: an increment in the gap followed by a levelling off, at around 4 years in the case of Cuba and almost 7 years for Japan.
11.4 The Case of Cuba
11.4.1 Population Trend
According to the classification of Latin-American countries presented by Chackiel (2004), Cuba has been in the Third Stage of the Demographic Transition since 1985–1990. Death rates have remained almost constant (varying within a narrow range of 5 to 7 per thousand), the population growth rate has started to decline and aging has become a major concern. In Fig. 11.3 we show the evolution of the natural growth rate and its components. The first four observations correspond to the initial 50 years of the century (only 5-year grouped data were available), so although there is a decline in the birth and death rates, it is not as steep as it seems due to this fact. Births increased during the sixties, corresponding to the baby boom but, by 1978, Cuban fertility fell below replacement level (less than 2.1 children per woman). This indicator has not recovered the replacement level, achieving the lowest levels in the nineties with a Total Fertility of 1.30, and then slightly increasing to 1.59 in 2008.

Regarding mortality, we observe that death rates declined until the beginning of the sixties, when they levelled off at very low levels (around 8 per thousand inhabitants). The mortality trend from 1902 (after the war and the establishment of the Republic of Cuba) starts to decline, especially due to improvements in health and economic and political conditions, but this did not reach the entire society (in particular not the lowest classes and rural areas). Different studies (Albizu-Campos 2003; Riverón and Azcuy 2001; UNICEF 1995) pointed out the impact of the Revolution in 1959, when health and education programmes were universalized in Cuba , spreading the supply of health care to all areas (urban and rural) and without limitations, and thus increasing the health and living conditions of the population.
Since the last two decades of the twentieth century there has been a steady but slow increase in mortality, which is due to the population’s age structure. As the Cuban population ages, and mortality becomes concentrated at older ages, it is expected that this trend will continue. The combination of mortality and fertility results in a declining rate of population growth, which depends markedly on what occurs with births and migration, but mortality has less impact given its steady trend. Thus, as a result, in 2006 the total growth rate fell below zero and has been fluctuating around that level until the present.
This evolution has led to a change in the structure of the population. With fewer new-borns and people living longer, the population has aged, as can be seen in the population pyramids (Fig. 11.4). Pyramids of 2008 and the projection for 2030 were calculated in single ages, from 0 to 110 and above. Although they appear unnaturally symmetric for both sexes, possibly due to data management, we can see the transformation of the pyramid’s structure. The 2008 pyramid has a considerably reduced base at age 0 (compared to what had been in the past, for instance in 1966, people aged 42 years in 2008) as a result of the decline in fertility (since 1978, TFR dropped from 1.98 to 1.30). In the projections of 2030 the large generations of the past are gradually increasing the weight of every age they pass through, and therefore shrinking the base. We can also see the abrupt discontinuities between cohorts due to the impact of migration. Particularly important were the four outmigration waves which occurred during the second half of the 20th century in Cuba: 1959–1962; 1965–1972; 1980 and 1994, with a total population loss in these periods of 703,900 people, making up 65 % of the total migration for the period 1959–1999 (Aja 2000, 2002).

Population pyramids for Cuba in 2008 and 2030* (Source: Data of population for 2008 comes from Oficina Nacional de Estadísticas (2009), Cuba. *Own projection of 2030 assuming fertility, mortality and migration constant based on 2008 official data; Total Fertility Rate (TFR): 1.59)
An extraordinary example of this impact can be seen in the pyramid of 2008, at ages 49 to 57 (those born between 1951 and 1959), where, instead of a gap, it looks like a vertical cut of the population. One of the reasons for this shape (apart from the effect of subsequent migration waves) is a particular migration pattern experienced by this generation in the period 1960–1962, when 14,000 children (5 % of total migrants of the period) migrated to the United States without their parents, a migration flow called the Peter Pan Operation (Torreira and Buajasan 2000). Another important aspect of the change in the population structure is the increase in the proportion of people over age 60. According to the population projection, by 2030 the elderly population will reach 31 %, twice the percentage in 2008.
Cuba began the twentieth century with a total life expectancy of 37.7 years (1900–1904) and a differential by sex of 3.96 years (González and Ramos 1996; López et al. 2005). For the second half of the century, the sex gap fluctuated between 3 to 4 years (Table 11.1). Several factors, biological, socio-economic and behavioural, affected this trend. After the Cuban Revolution in 1959 women took an active role in the transformation of society, increasing their labour force participation and educational attainment, among others. These changes led women to share similar behaviours and risk factors with men, for instance smoking tobacco (which increased especially among women until 2006, with 16 and 14 % of women and men smoking, respectively). These factors could possibly lead to a worsening in female’s survival for causes that previously did not affect them, while at the same time, the improvements in the health system could have a positive effect on men’s survival. Results from López et al. (2005) support this interpretation. They show that there was more progress in males’ survival compared to females until the nineties, which helped to maintain the lower sex differential observed before. We shall check, below, whether this trend holds into the first decade of the twenty-first century, and what causes of death are responsible for it.
11.4.2 The Evolution of Mortality in Recent Decades
The age schedule of mortality in Cuba has changed considerably in the past 20 years (Fig. 11.5), from 1987, represented by the darkest blue line, until 2007, the lime colour. There is a marked drop in mortality below age one and for younger adults there is a flat peak around age 25, followed by a decline in the number deaths in the surrounding ages until 2007. Later there is an appreciable increase in the number of deaths after age 70, with a peak around age 81 which is the modal age at death in 1987 (first line in dark blue). The modal age at death continues to shift to the right and the number of deaths around the mode increases until 2007 (upper line in lime colour). This shift towards older ages at death supports the idea that the Cuban population is extending its lifespan by delaying mortality at older ages.

Number of deaths by age from 1987 to 2007, Cuba. (Source: Taken from Esperanza de vida Cuba y provincias, 2005–2007. Cálculos por sexo y edades. Pp. 22, Gráfico 2. Cuba. 1987–2007. Número de defunciones por edad. Oficina Nacional de Estadísticas, (2008)
Before analysing the effect of different causes of death on the differences in life expectancy , we will describe the pattern of mortality for the specific years that will be used later on. Mortality curves follow the regular U shape, describing a low infant mortality (reduced over time); a slight hump at younger adult ages (from age group 15–19 to 30–35); and an increment in mortality rates as age increases (Fig. 11.6). The differences by sex can also be seen, with lower mortality rates for females over all ages, although the smallest differences by sex are before age 5, and at older ages. The most significant changes over time can be seen at age 0, with an important reduction of mortality, and at younger ages (15–30), where the hump has been considerably reduced.

Mortality pattern by sex and age groups. Years 1987, 1995 and 2007. (Source: Calculations based on data from National Statistic Office and Public Health Ministry of Cuba)
As previously mentioned, the first three principal causes of death in Cuba are non-infectious diseases. As early as 1970, heart disease, cancer (lung, colon and lymphoma) and cerebrovascular disease were the leading causes of death (Fernández 2006; Oficina Nacional de Estadísticas 2010). In this study, we will use the following 11 causes of death groups:
-
1.
Heart diseases
-
2.
Cancer
-
3.
Cerebrovascular diseases
-
4.
External causes (Accidents, Violent deaths and Suicide)
-
5.
Respiratory diseases (including Influenza)
-
6.
Artery and arterioles
-
7.
Diabetes
-
8.
Liver, Kidney and Obstruction
-
9.
Congenital Malformation
-
10.
Mental disorders (including Alzheimer disease)
-
11.
Other causes
Given the impact of these causes in specific age groups and their evolution over time, we have grouped them into 6 patterns of mortality. Below are shown patterns of mortality due to Cancer, External Causes, Respiratory Diseases, Other Causes and Diabetes (other causes can be found in the Annex, sects. 2 to 7).
The first pattern of mortality affects especially adult life (cancer; heart diseases and liver, kidney and obstruction). Mortality due to cancer is depicted in Fig. 11.7. Over time the number of deaths below age 30 declines, but they increase appreciably above that age. Between the ages of 30 and 50 there are more female than male deaths, while men have more deaths at older age. Over the period studied, 1987 to 2007, the mortality rate for men increases faster with age than does the rate for women.

Number of deaths and age-specific death rates of Cancer in 1987, 1995 and 2007, Cuba. (Source: Calculations based on data from Public Health Ministry of Cuba)
Figure 11.8 depicts the second pattern of mortality, that of external causes, one which affects all ages, especially younger adults. It shows a minimum at younger ages (0–14) and a maximum at young adult ages (20–30). By sex, males have a disadvantage at almost all ages and there is an increase of deaths in 1995 compared to 1987, particularly for younger adults, and then a decrease, especially for women. It is worth noting the rise in mortality rates at older ages and, in particular for the last two age-groups, the rise in the number of female deaths and rates, which surpass those of males.

Number of deaths and age-specific death rates of External Causes in 1987, 1995 and 2007, Cuba. (Source: Calculations based on data from Public Health Ministry of Cuba)
The third pattern of mortality corresponds to the impact of respiratory diseases (also cerebrovascular diseases; and artery and arterioles), showing a gradual increase in mortality from agke forty onwards. Both sexes experienced an increase in the number of deaths over time; however, the mortality rates of women decreased (Fig. 11.9).

Number of deaths and age-specific death rates of Respiratory Diseases in 1987, 1995 and 2007, Cuba. (Source: Calculations based on data from Public Health Ministry of Cuba)
The fourth pattern of mortality can be observed only for diabetes, where mortality is higher for females at almost all ages (Fig. 11.10). It affects mainly adult and older ages, and female deaths are almost double those of males. Over time, there was an increase in 1995, but the number of deaths then fell to its previous level, while mortality rates decreased, particularly for females, falling to half their value in previous observations.

Number of deaths and age-specific death rates of Diabetes Mellitus in 1987, 1995 and 2007, Cuba. (Source: Calculations based on data from Public Health Ministry of Cuba)
The fifth pattern describes the effect of mortality at two opposite ends of the life cycle: congenital malformations (Annex 6) which account for the majority of deaths in the first year of life, and which show a considerable decrease over time; and mental disorders (Annex 7), concentrated at the end of life, in particular after age 75, which affect females in particular, and which have been increasing over time.

Number of deaths and age-specific death rates of Other Causes in 1987, 1995 and 2007, Cuba. (Source: Calculations based on data from Public Health Ministry of Cuba)
The rest of the causes of death are grouped into other causes, forming the last pattern of mortality (Fig. 11.11). This group affects all ages, although there has been a considerable reduction from infancy through to young adult ages over time. In 2007, for age group 85 and above, females had more deaths from other causes than did males, but also with a reduction in death rates for both sexes.
11.5 Decomposition of Life Expectancy Differences at Birth
So far, we have shown that Cuba is at an advanced stage of the demographic transition, with low levels of fertility and mortality, and a death distribution that is concentrated at older ages. We now decompose the effect of age and specific-causes of death which account for differentials in life expectancy at birth. This will be done firstly for the sex differential in 1987, 1995 and 2007; and then, for each sex, to see the changes between the two periods (1987–1995 and 1995–2007).
The evolution of mortality trends has led to an increasing life expectancy at birth over time, and this improvement now depends mainly on gains in terms of survival at older ages. Furthermore, there are clear differences by sex in the mortality patterns, as was shown in the last section. The changing sex gap in life expectancy is made up of the relative age- and cause-specific gains and losses of each sex, and of the distinct way in which different causes of death affect each sex. In this section we will address the following questions: To what extent are these gains higher for females or males? What causes of deaths are responsible for gains or losses in survival?
11.5.1 Sex Differential in Life Expectancy at Birth
Figure 11.12 depicts the contribution of each age group to the sex-difference in life expectancy for the three years of observation. As we can see, all contributions are positive, meaning that at all ages, females gain more years of life than males. The life expectancy differential between females and males was 3.60 years in favour of females in 1986–1987 (green bars). There is a large contribution of infant mortality and a very low contribution at younger adult ages. The difference starts to increase from age group 20–24 onwards, with the highest contributions being at age groups 60–64 and 70–74.

Decomposition of Sex Differential in life expectancy at birth, by age. (Source: Calculations based on data from the National Statistic Office, Cuba)
In 1994–1995 (yellow bars), the differential was 3.96, higher than before, but contributions by age were different. Infant mortality decreased in importance, given the small proportions of deaths that occurred at age 0 in this period, but there was a significant increase in the contributions of young adult ages (15–19 to 35–39 age groups). As we saw previously, in Fig. 11.8, in this period male mortality from external causes increased, but this was not the case for females, hence the abrupt increase in contributions observed in this period and not in the previous or the following one.
For the last period 2005–2007 (red bars), the differential in life expectancy was 4.01 years, slightly higher than in the previous period. Infant mortality continued to drop in importance, and the female advantage became concentrated even more at older ages, especially at ages 70–74. For age-group 85 and above the contribution is double that of the first period.
The overall reading of Fig. 11.12 is that female life expectancy has been higher than that of males for all 3 years in the study, and the major contributions to the sex-gap in life expectancy shift to the right as infant and childhood mortality lose their importance. However, there is also an important increase in contributions at young adult ages as a result of the increase in male mortality for the period 1994–1995. This could be related to the economic crisis and the deterioration in living conditions that shocked Cuban society after 1989.
We now split these contributions according to the corresponding causes of death implicated in the changes in life expectancy. This means that each bar will be divided according to the weight of each cause with respect to: the total difference in the sex gap and the total difference in time by each sex. Data used to build graphs 13, 14 and 15 are in Annex sections 8 to 14. The results should be interpreted with caution, given that the detailed information we are using for the analysis (splitting by cause of death) could lead to some inconsistencies, for instance, the irregularity by age of the contributions (bars nearby often didn’t follow a consistent increase or decrease), especially when the sexes are analysed separately.
Figure 11.13 presents the decomposition for the years 1987, 1995 and 2007. For the year 1987, it shows a predominantly greater female survival for almost all age groups. The few disadvantages (negative contributions), especially at adult ages (35–54), are due to cancer and diabetes, as well as a strong negative effect of cancer, at 85 years and over. On the other hand, females are doing better in terms of survival than males, especially for other causes at age 0 (at that time, still significant gains are found at this age); external causes, heart diseases and cancer. For 1995, some differences with respect to the previous period can be observed: firstly, the growth of the contribution due to external causes; secondly, the share of infant mortality is considerably reduced in size; and thirdly, for all age groups there were some causes with small negative contributions (males advantage over females), which are concentrated at adult ages. For 2007, the contrast with respect to the other 2 years is the concentration at older ages of the majority of contributions, the reduction in the infant mortality effect and the reduction in external causes at younger ages.

Decomposition of the difference in Life Expectancy at birth between females and males by causes of death and age, 1987, 1995 and 2007. (Source: Calculations based on data from the National Statistic Office and the Public Health Ministry of Cuba)
Taking a general overview of the period shown in Fig. 11.13, we see that the importance of infant mortality declined over time; external causes increased in 1995 but then declined again, but still remained the foremost cause of death at young ages and adults before age 50, for the entire period. Females’ advantages are mainly due to cancer, external causes and heart diseases. At older ages, cancer leads the higher gains in women’s survival, followed by heart diseases, and respiratory diseases. Male advantage is mainly concentrated in their lower mortality from cancer at younger adult ages (30–49), and from diabetes at older ages.
11.5.2 Time Differential in Life Expectancy at Birth
The second part of the analysis will allow us to illustrate the behaviour of each sex separately, between two periods: 1987–1995 and 1995–2007. Starting with males (Fig. 11.14), they improved their life expectancy at birth by 3.26 years over the 20 years of the study (1987–2007). Only 0.2 of that gain was achieved in the first period 1987–1995. During this period, important improvements of infant mortality due to congenital malformation and other causes took place.

Decomposition of the difference in male life expectancy at birth between 1987–1995 and 1995–2007, by age and causes of death, Cuba. (Source: Calculations based on data from the National Statistic Office and the Public Health Ministry of Cuba)
At young ages there were almost no signs of improvements; on the contrary, for age groups 1–4, 20–29 and 35–50, there was actually a decline. At older ages the intensity of the effects was greater, but also with an overall negative contribution to the indicator. In fact, the ages between 55–59 and 75–79 experienced both the highest improvements and deteriorations in the same age groups, with heart diseases and cerebrovascular diseases leading the negative contributions.
There was a greater improvement in male survival during the period 1995–2007 and life expectancy at birth increased by 3.06 years. This was due to improvements at almost all ages and from almost all causes of death. The reduction in external causes contributed most to the positive changes at younger ages, while at older ages these were mainly due to heart diseases and cerebrovascular diseases and, to a lesser extent, diabetes and external causes. At older ages, deterioration (negative contribution) was mainly due to cancer and mental disorders.
For females, life expectancy at birth increased by 3.68 years over the entire period and the trends were similar to those for males. In the first period (1987–1995) there was little improvement, around half a year, and the major advances took place in the second period (1995–2007), with more than 3 years of improvement (Fig. 11.15). During the first period the female improvement was more than double that for males (0.56 compared with 0.20); in the second period both show almost the same progress, which was only 0.06 of a year higher for females (3.12 and 3.06 respectively).

Decomposition of the difference in female life expectancy at birth between 1987–1995 and 1995–2007, by age and causes of death, Cuba. (Source: Calculations based on data from the National Statistic Office and the Public Health Ministry of Cuba)
In the first period infant mortality showed improvements (reductions in other causes and congenital malformation) as did mortality at younger adult ages, from age 15 to 34, largely owing to the reduction in external causes. Mortality at ages 1–4 made an overall negative contribution, while at older ages, there was a concentration of both losses and of increments in life expectancy. Positive shares were mainly due to heart and cerebrovascular diseases, and external causes.
The second period shows greater improvements, with a gain of 3.12 years in life expectancy. Females improved their survival on account of all causes of deaths, except for cancer, mental disorders, and respiratory diseases at ages older than 55 (excluding age groups 60–64 and 80–84). Slightly negative contributions were also found at younger ages (0 to 14) due to: cancer; congenital malformation; other causes; cerebrovascular diseases; liver, kidney and obstruction and arteries and arterioles.
11.6 Conclusions
One of the great successes of society in the twentieth century has been the control of infectious and parasitic diseases, leading to a decline in mortality and a remarkable increase in life expectancy especially in the first half of the century. However, sex differences in life expectancy also widened, meaning that the mortality decline did not affect both sexes in the same way. As has been argued in previous studies, survival is affected by biological factors, but also by behavioural and sociological differences. These differences have been decreasing over time, leading to a reduction or stagnation in the sex gap, especially over the last three decades.
As we have shown in this study, Cuban life expectancy at birth has been increasing since the beginning of the twentieth century, reaching 80 years of life expectancy for females and 76 years for males at the last available record (2005–2007). This has been possible as a result of the changes experienced by the Cuban population: a rapid progression into the demographic transition (it stands now at the last stage, with low levels of mortality and fertility); and by the changes inherent in the epidemiologic transition , showing in Cuba a mixture of mortality patterns and a co-existence of endogenous and exogenous causes of death among the leading causes of death in the country.
However, unlike other countries, in Cuba this increase in life expectancy has not been translated into a growing mortality difference between males and females. In the 20 years analysed here, this is particularly true for the first period (1987–1995) in which life expectancy increased around half a year for females, and even less for males; in the subsequent period (1995–2007) both sexes increased their life expectancy by more than 3 years.
In this research, we have focussed our attention on the impact of changes in the mortality patterns on male and female life expectancy in Cuba . We summarise our findings concerning the improvements in survival over time by looking at the three aspects analysed: age; causes of death; and sex. Results by specific age-group contributions show that despite the fact that mortality is now concentrated at older ages (50 per cent of years gained are due to mortality reductions above age 60), mid-adult mortality is still important, particularly for 1987 and 1995. Furthermore, even though infant mortality shows very low and decreasing contributions, other causes remain important in this age group, indicating deaths which could have been prevented.
In terms of causes of death, there are four main causes of death which contribute the most to the higher female survival compared to that of males: heart disease, external causes, cancer and cerebrovascular diseases. However, males do enjoy an advantage with respect to some causes, mainly diabetes, and cancer at younger adult ages.
When comparing within each sex, females show higher gains for both periods. For 1987–1995 these were mainly due to a decrease in infant mortality, while the small gains at other ages were counterbalanced by losses at age group 1–4 and age 40 and over. In the following period (1995–2007), females experienced higher gains of life expectancy. In this period, both higher positive and negative contributions were found, and these were substantially greater at 55 years and over. In this case, females experienced losses at older ages mainly due to cancer, mental disorders and respiratory diseases.
Males’ advantage in the first period of analysis is concentrated in childhood and between ages 55 and 80. The gains in survival at older ages were accompanied by opposite effects that exceeded the positive contributions. For other ages, there were only changes towards a slight deterioration. The second period shows an important increase in male survival. Almost all ages showed positive contributions, in particular for: other causes in childhood ; external causes at young adult ages, and heart diseases at older ages. Negative contributions were found principally for cancer at old ages .
Our results suggest that there is a mix of mortality patterns in Cuba, where most deaths are attributable to chronic or degenerative diseases, but there are a sizeable proportion of avoidable deaths (for instance external causes, respiratory diseases or diabetes). Although effects by sex are different, with females having higher survival, this difference is less than might otherwise be expected. The evidence suggests that life expectancy can still increase for the Cuban population, particularly by reducing the impact of external causes, respiratory diseases, heart diseases and other causes.
The differences between the periods are clear. The first one was the period when increases in life expectancy were at their lowest. The second period shows a recuperation of the positive trend in life expectancy. During the economic crisis, male survival was seriously constrained while females kept their advantage of half of a year; in the recovery period, males recovered faster than females, almost catching up with them.
11.7 Annex
11.7.1 Annex 1. Groups of causes of death used in the analysis, according to ICD-10 and ICD-9
Group of Causes of death | CIE-9 | CIE-10 |
|---|---|---|
01 Cancer | 140–208 | C00-C97 |
02 Diabetes mellitus | 250 | E10-E14 |
03 Mental disorders (including Alzheimer) | 290 310 | F01-F03 G30 |
04 Heart diseases | 393–429 | I05-I52 |
05 Cerebrovascular diseases | 430–438 | I60-I69 |
06 Artery and arterioles | 440–444 447–448 | I70-I79 |
07 Respiratory disease (including Influenza) | 490–496 | J40-J47 |
08 Liver, Kidney and Obstruction | 550–553 560 | K40-K46 K56 |
09 Congenital Malformation | 740–759 | Q00-Q99 |
10 External causes (Accidents, Violent deaths and Suicide) | 800–949 | V01-X59 Y85-Y86 |
11.7.2 Annex 2. Number of deaths and age-specific death rates of Heart Diseases. Cuba, 1987, 1995 and 2007

11.7.3 Annex 3. Number of deaths and age-specific death rates of Liver, Kidney and Obstruction. Cuba, 1987, 1995 and 2007

11.7.4 Annex 4. Number of deaths and age-specific death rates of Cerebrovascular Diseases. Cuba, 1987, 1995 and 2007

11.7.5 Annex 5. Number of deaths and age-specific death rates of Artery and Arterioles. Cuba, 1987, 1995 and 2007

11.7.6 Annex 6. Number of deaths and age-specific death rates of Congenital Malformation. Cuba, 1987, 1995 and 2007

11.7.7 Annex 7. Number of deaths and age-specific death rates of Mental Disorders. Cuba, 1987, 1995 and 2007

11.7.8 Annex 8. Decomposition of the difference in Life Expectancy at birth between females and males by causes of death and age, 1987
Cause specific component of the sex differential 1987 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age groups | Other Causes | Cancer | Diabetes Mellitus | Mental Disorders | Heart Diseases | Cerebrovascular D. | Artery/Arterioles | Respiratory Dis. | Liver/Kidney/Obst | Congenital Malf. | External causes |
< 1 | 0.21337 | − 0.00223 | 0.00000 | 0.00000 | 0.00179 | 0.00094 | 0.00000 | 0.01489 | − 0.00042 | 0.06131 | − 0.00472 |
1–4 | 0.00202 | 0.00482 | 0.00000 | 0.00000 | 0.00029 | 0.00000 | 0.00000 | 0.00144 | − 0.00015 | − 0.00298 | 0.03432 |
5–9 | 0.01124 | − 0.00090 | 0.00000 | 0.00000 | 0.00189 | 0.00189 | 0.00000 | 0.00088 | − 0.00116 | − 0.00260 | 0.02513 |
10–14 | 0.00478 | 0.00759 | 0.00107 | 0.00000 | 0.00426 | 0.00154 | 0.00000 | − 0.00013 | − 0.00391 | 0.00730 | 0.05358 |
15–19 | 0.01402 | − 0.00032 | − 0.00377 | 0.00052 | 0.00433 | − 0.00218 | 0.00000 | − 0.00191 | 0.00348 | − 0.00034 | 0.04030 |
20–24 | 0.00526 | 0.00634 | 0.00042 | 0.00000 | − 0.00070 | 0.00081 | 0.00090 | − 0.00377 | − 0.00195 | − 0.00421 | 0.12226 |
25–29 | − 0.00788 | − 0.00594 | − 0.00465 | 0.00000 | 0.00471 | − 0.00131 | 0.00133 | − 0.00464 | 0.00135 | − 0.00265 | 0.14556 |
30–34 | − 0.00169 | − 0.01132 | − 0.00153 | 0.00001 | 0.00970 | 0.00679 | 0.00056 | 0.00354 | 0.00288 | 0.00442 | 0.14288 |
35–39 | − 0.00416 | − 0.01717 | − 0.00067 | 0.00000 | 0.02828 | 0.00481 | − 0.00003 | − 0.00304 | 0.00100 | − 0.00290 | 0.14229 |
40–44 | 0.01720 | − 0.03592 | − 0.00385 | 0.00000 | 0.04288 | 0.00632 | 0.00247 | − 0.00783 | 0.00111 | 0.00012 | 0.13157 |
45–49 | 0.00856 | − 0.02704 | − 0.01286 | 0.00064 | 0.09710 | 0.00414 | 0.00189 | − 0.01615 | 0.00056 | 0.00126 | 0.11644 |
50–54 | 0.00198 | − 0.02796 | − 0.02003 | 0.00064 | 0.09355 | 0.02554 | 0.00702 | 0.00220 | 0.00529 | 0.00066 | 0.09960 |
55–59 | 0.01858 | 0.00978 | − 0.02587 | 0.00000 | 0.13657 | 0.00994 | 0.00286 | − 0.00100 | 0.01288 | − 0.00096 | 0.07792 |
60–64 | 0.04050 | 0.10790 | − 0.03215 | 0.00151 | 0.16318 | 0.03022 | 0.01209 | 0.02225 | − 0.00403 | − 0.00002 | 0.04682 |
65–69 | 0.02633 | 0.10350 | − 0.02515 | − 0.00255 | 0.13498 | 0.02032 | 0.01772 | 0.02671 | 0.00785 | 0.00110 | 0.03174 |
70–74 | 0.02773 | 0.14918 | − 0.03469 | − 0.00361 | 0.13575 | 0.04268 | 0.02050 | 0.02949 | 0.00034 | − 0.00029 | 0.02640 |
75–79 | 0.01269 | 0.15257 | − 0.03006 | − 0.00116 | 0.08192 | − 0.00275 | 0.01201 | 0.02867 | 0.01797 | 0.00029 | 0.02633 |
80–84 | 0.02055 | 0.13443 | − 0.01863 | − 0.00441 | 0.04153 | 0.00097 | 0.01797 | 0.03106 | 0.00710 | − 0.00026 | 0.00805 |
85 + | − 0.01691 | − 0.17377 | 0.05957 | 0.03161 | 0.16492 | 0.05966 | 0.05389 | − 0.04378 | − 0.00577 | − 0.00066 | 0.00512 |
Sex Δ 1987 | 3.60 | ||||||||||
11.7.9 Annex 9. Decomposition of the difference in Life Expectancy at birth between females and males by causes of death and age, 1995
Cause specific component of the sex differential 1995 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age groups | Other Causes | Cancer | Diabetes Mellitus | Mental Disorders | Heart Diseases | Cerebrovascular D. | Artery/Arterioles | Respiratory Dis. | Liver/Kidney/Obst | Congenital Malf. | External causes |
< 1 | 0.13341 | − 0.00017 | 0.00000 | 0.00000 | − 0.00614 | 0.00000 | 0.00000 | − 0.00410 | 0.00151 | 0.02349 | 0.00876 |
1–4 | 0.00032 | − 0.00048 | 0.00000 | 0.00000 | 0.00004 | − 0.00084 | 0.00000 | 0.00203 | − 0.00005 | 0.01180 | 0.03001 |
5–9 | − 0.00161 | 0.00605 | − 0.00003 | 0.00000 | − 0.00098 | 0.00178 | 0.00000 | − 0.00058 | 0.00082 | 0.00284 | 0.01872 |
10–14 | 0.00831 | 0.01081 | 0.00000 | 0.00000 | 0.00274 | − 0.00113 | 0.00000 | − 0.00014 | − 0.00302 | 0.00038 | 0.03839 |
15–19 | 0.00838 | 0.00290 | − 0.00122 | 0.00000 | 0.00620 | 0.00172 | 0.00000 | 0.00091 | 0.00042 | 0.00378 | 0.10013 |
20–24 | 0.01497 | 0.00462 | − 0.00010 | 0.00000 | 0.01041 | − 0.00058 | 0.00000 | − 0.00330 | − 0.00070 | 0.00340 | 0.15676 |
25–29 | 0.02182 | − 0.00221 | 0.00210 | 0.00000 | 0.00996 | − 0.00094 | 0.00000 | − 0.00058 | 0.00169 | 0.00081 | 0.17243 |
30–34 | 0.02719 | − 0.01223 | 0.00161 | 0.00040 | 0.02193 | 0.00082 | 0.00000 | − 0.00196 | 0.00161 | 0.00161 | 0.15545 |
35–39 | 0.02062 | − 0.04069 | 0.00625 | 0.00185 | 0.03551 | 0.00638 | − 0.00060 | − 0.00154 | 0.00877 | − 0.00117 | 0.16527 |
40–44 | 0.02713 | − 0.03415 | 0.00424 | 0.00051 | 0.05928 | − 0.00555 | 0.00309 | − 0.00826 | 0.00490 | 0.00161 | 0.09663 |
45–49 | 0.03053 | − 0.01378 | 0.00241 | − 0.00045 | 0.07714 | − 0.00049 | 0.00293 | 0.00328 | 0.01671 | 0.00338 | 0.10325 |
50–54 | 0.02849 | − 0.02492 | − 0.00075 | 0.00044 | 0.11240 | 0.00785 | 0.00632 | 0.00338 | 0.00974 | − 0.00123 | 0.10351 |
55–59 | 0.05055 | 0.04738 | − 0.01974 | 0.00224 | 0.12199 | 0.01132 | 0.00495 | 0.00707 | 0.01225 | − 0.00265 | 0.07986 |
60–64 | 0.02981 | 0.06718 | − 0.02285 | − 0.00115 | 0.09339 | − 0.00031 | 0.01342 | 0.00461 | 0.01465 | 0.00079 | 0.05477 |
65–69 | 0.04042 | 0.15213 | − 0.04061 | − 0.00229 | 0.12914 | 0.01183 | 0.02599 | 0.03039 | 0.01771 | 0.00160 | 0.04165 |
70–74 | 0.03845 | 0.13806 | − 0.03616 | − 0.00163 | 0.12328 | 0.01647 | 0.01750 | 0.04203 | 0.00929 | 0.00087 | 0.01824 |
75–79 | 0.03014 | 0.14545 | − 0.02123 | 0.00238 | 0.11628 | 0.00650 | 0.02086 | 0.06970 | 0.00640 | − 0.00060 | 0.01644 |
80–84 | 0.00856 | 0.15344 | − 0.03808 | − 0.00322 | 0.07920 | − 0.01866 | 0.02449 | 0.06790 | 0.00162 | 0.00004 | − 0.01920 |
85 + | 0.01336 | 0.10683 | − 0.02159 | 0.00182 | 0.01994 | − 0.01406 | 0.00331 | 0.05395 | 0.00437 | 0.00002 | − 0.01360 |
Sex Δ 1995 | 3.96 | ||||||||||
11.7.10 Annex 10. Decomposition of the difference in Life Expectancy at birth between females and males by causes of death and age, 2007
Cause specific component of the sex differential 2007 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age groups | Other Causes | Cancer | Diabetes Mellitus | Mental Disorders | Heart Diseases | Cerebrovascular D. | Artery/Arterioles | Respiratory Dis. | Liver/Kidney/Obst | Congenital Malf. | External causes |
< 1 | 0.06817 | 0.00000 | 0.00000 | 0.00000 | − 0.00296 | 0.00111 | 0.00000 | − 0.00243 | − 0.00025 | − 0.00189 | 0.00842 |
1–4 | 0.00953 | 0.03225 | 0.00000 | 0.00000 | − 0.02835 | 0.00380 | 0.00000 | 0.01042 | 0.00000 | − 0.03512 | 0.01911 |
5–9 | 0.00760 | 0.00656 | 0.00000 | 0.00000 | 0.00088 | − 0.00005 | 0.00000 | 0.00186 | − 0.00099 | − 0.00027 | 0.01718 |
10–14 | 0.00365 | 0.00761 | 0.00000 | 0.00000 | − 0.00176 | 0.00077 | 0.00000 | − 0.00090 | 0.00072 | − 0.00266 | 0.03855 |
15–19 | 0.00346 | 0.00044 | − 0.00130 | 0.00000 | 0.00109 | 0.00053 | 0.00119 | 0.00225 | 0.00179 | 0.00348 | 0.06481 |
20–24 | − 0.00392 | 0.00880 | − 0.00010 | 0.00077 | 0.00828 | − 0.00010 | 0.00077 | 0.00511 | − 0.00337 | − 0.00041 | 0.09227 |
25–29 | 0.00616 | 0.00438 | − 0.00208 | 0.00088 | 0.01256 | 0.00425 | 0.00088 | − 0.00214 | 0.00601 | − 0.00309 | 0.09167 |
30–34 | 0.00135 | − 0.02335 | 0.00298 | 0.00359 | 0.01817 | 0.00024 | 0.00000 | 0.00289 | − 0.00070 | 0.00134 | 0.11526 |
35–39 | 0.01945 | − 0.02030 | − 0.00080 | 0.00490 | 0.02382 | 0.00378 | 0.00174 | 0.00125 | 0.00587 | − 0.00078 | 0.09157 |
40–44 | 0.02645 | − 0.02635 | 0.00313 | 0.01531 | 0.04766 | 0.00256 | 0.00103 | − 0.00120 | 0.00384 | 0.00038 | 0.08733 |
45–49 | 0.03309 | − 0.01512 | 0.00117 | 0.01384 | 0.06682 | 0.00794 | 0.00341 | 0.00274 | 0.01871 | 0.00131 | 0.08239 |
50–54 | 0.03612 | 0.03464 | 0.00333 | 0.01194 | 0.09132 | 0.02083 | 0.00335 | − 0.00482 | 0.01988 | 0.00324 | 0.06748 |
55–59 | 0.02291 | 0.08252 | − 0.00495 | 0.01807 | 0.12302 | 0.02588 | 0.01355 | − 0.00302 | 0.00787 | 0.00323 | 0.06809 |
60–64 | 0.04337 | 0.12194 | − 0.02253 | 0.01530 | 0.13384 | 0.03128 | 0.01273 | 0.01451 | 0.00280 | − 0.00020 | 0.05185 |
65–69 | 0.04418 | 0.14245 | − 0.01683 | 0.01220 | 0.12083 | 0.03692 | 0.01852 | 0.01818 | 0.00532 | 0.00011 | 0.04137 |
70–74 | 0.04736 | 0.18423 | − 0.02778 | 0.00708 | 0.08690 | 0.03455 | 0.02774 | 0.04426 | 0.00244 | 0.00133 | 0.03761 |
75–79 | 0.03207 | 0.20807 | − 0.01803 | − 0.00581 | 0.08590 | 0.03709 | 0.01570 | 0.05130 | 0.00380 | 0.00065 | 0.01632 |
80–84 | 0.03003 | 0.16843 | − 0.01245 | − 0.00753 | 0.04893 | − 0.00989 | 0.02402 | 0.07051 | 0.00626 | 0.00134 | − 0.00211 |
85 + | 0.00385 | 0.22282 | − 0.01507 | − 0.02876 | 0.01212 | − 0.02412 | 0.01207 | 0.09434 | 0.00746 | 0.00051 | − 0.03010 |
Sex Δ 2007 | 4.01 | ||||||||||
11.7.11 Annex 11. Males, decomposition of the difference in life expectancy at birth between 1987–1995, by age and causes of death, Cuba
Males cause specific component of the time differential 1987–1995 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age groups | Other Causes | Cancer | Diabetes Mellitus | Mental Disorders | Heart Diseases | Cerebrovascular D. | Artery/Arterioles | Respiratory Dis. | Liver/Kidney/Obst | Congenital Malf. | External causes |
< 1 | 0.18458 | − 0.00087 | 0.00000 | 0.00000 | − 0.00366 | 0.00129 | 0.00000 | 0.03147 | 0.00142 | 0.13108 | 0.00290 |
1–4 | 0.00673 | − 0.00148 | 0.00000 | 0.00000 | 0.02318 | 0.00000 | 0.00000 | 0.03340 | − 0.01140 | − 0.01564 | − 0.06482 |
5–9 | 0.02383 | 0.00005 | − 0.00236 | 0.00000 | 0.00659 | − 0.00285 | 0.00000 | − 0.00049 | − 0.00285 | − 0.00904 | 0.00652 |
10–14 | 0.00532 | 0.00194 | 0.00053 | 0.00000 | 0.00079 | 0.00063 | 0.00000 | 0.00063 | − 0.00032 | 0.00195 | 0.01765 |
15–19 | 0.00007 | − 0.00003 | − 0.00001 | 0.00001 | 0.00000 | − 0.00003 | 0.00000 | − 0.00003 | 0.00001 | − 0.00007 | − 0.00059 |
20–24 | − 0.00695 | 0.00064 | − 0.00128 | 0.00000 | − 0.00427 | 0.00105 | 0.00049 | − 0.00153 | − 0.00100 | − 0.00259 | 0.00479 |
25–29 | 0.00234 | − 0.00092 | − 0.00304 | 0.00000 | 0.00146 | 0.00430 | 0.00068 | 0.00393 | 0.00037 | − 0.00052 | − 0.01920 |
30–34 | − 0.00016 | 0.00000 | 0.00009 | 0.00000 | − 0.00005 | − 0.00026 | − 0.00002 | − 0.00030 | − 0.00006 | − 0.00002 | − 0.00030 |
35–39 | − 0.00018 | − 0.00916 | 0.00563 | 0.00226 | − 0.02457 | − 0.01162 | − 0.00317 | − 0.00417 | 0.00842 | 0.00063 | − 0.01287 |
40–44 | − 0.00541 | − 0.00612 | − 0.00132 | − 0.00016 | − 0.00105 | 0.00506 | − 0.00039 | − 0.00130 | − 0.00207 | − 0.00085 | 0.00300 |
45–49 | − 0.00972 | − 0.00019 | − 0.00526 | 0.00018 | 0.00580 | 0.00376 | − 0.00057 | − 0.00567 | − 0.00494 | − 0.00128 | − 0.00208 |
50–54 | − 0.00122 | − 0.00090 | − 0.00079 | 0.00001 | 0.00044 | 0.00213 | − 0.00012 | − 0.00030 | − 0.00024 | − 0.00007 | − 0.00072 |
55–59 | 0.11302 | 0.09319 | 0.04308 | 0.00718 | − 0.23101 | − 0.09812 | − 0.00320 | 0.06681 | − 0.02809 | − 0.00605 | − 0.00226 |
60–64 | − 0.02585 | 0.02280 | − 0.02289 | − 0.00283 | 0.10597 | 0.06298 | − 0.01432 | 0.01000 | − 0.00554 | − 0.00175 | − 0.03391 |
65–69 | − 0.06441 | − 0.03993 | − 0.02433 | − 0.01283 | 0.11069 | 0.01506 | − 0.01259 | − 0.00997 | − 0.00259 | − 0.00358 | − 0.02396 |
70–74 | − 0.01307 | 0.01341 | 0.00153 | − 0.00589 | 0.02590 | 0.01389 | − 0.00660 | − 0.00628 | 0.00271 | − 0.00039 | − 0.00729 |
75–79 | 0.03834 | − 0.10328 | 0.02888 | 0.08388 | − 0.16453 | − 0.06113 | 0.05548 | 0.04639 | − 0.04141 | − 0.00272 | 0.05419 |
80–84 | 0.00061 | − 0.00218 | 0.00090 | 0.00424 | − 0.00058 | − 0.00044 | 0.00127 | 0.00101 | − 0.00111 | 0.00004 | 0.00401 |
85 + | − 0.00039 | − 0.00052 | − 0.00004 | − 0.00045 | − 0.00078 | − 0.00044 | − 0.00029 | 0.00022 | 0.00002 | 0.00000 | − 0.00043 |
Δ 1987–1995 | 0.20 | ||||||||||
11.7.12 Annex 12. Males, decomposition of the difference in life expectancy at birth between 1995–2007, by age and causes of death, Cuba
Males cause specific component of the time differential 1995–2007 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age groups | Other Causes | Cancer | Diabetes Mellitus | Mental Disorders | Heart Diseases | Cerebrovascular D. | Artery/Arterioles | Respiratory Diseases | Liver/Kidney/Obst | Congenital Malform. | External causes |
< 1 | 0.22458 | 0.00267 | 0.00000 | 0.00000 | 0.01172 | − 0.00339 | 0.00000 | 0.02352 | 0.00016 | 0.07144 | 0.01196 |
1–4 | 0.04867 | 0.00637 | 0.00000 | 0.00000 | 0.01746 | − 0.00132 | 0.00000 | 0.01954 | 0.00103 | 0.02044 | 0.04835 |
5–9 | 0.01040 | − 0.00435 | 0.00073 | 0.00000 | − 0.00109 | 0.00273 | 0.00000 | 0.00109 | 0.00364 | 0.00929 | 0.03789 |
10–14 | − 0.00251 | 0.00022 | 0.00000 | 0.00000 | 0.00521 | 0.00110 | 0.00000 | 0.00255 | − 0.00301 | 0.01442 | 0.03876 |
15–19 | 0.01949 | 0.00439 | 0.00008 | 0.00000 | 0.00675 | 0.00024 | − 0.00111 | 0.00255 | 0.00278 | 0.00517 | 0.10489 |
20–24 | 0.02952 | − 0.00114 | 0.00244 | − 0.00057 | 0.00817 | 0.00110 | − 0.00057 | − 0.00008 | 0.00512 | 0.00307 | 0.13518 |
25–29 | 0.02327 | − 0.00097 | 0.00557 | − 0.00063 | 0.00349 | − 0.00219 | − 0.00063 | 0.00382 | − 0.00009 | 0.00195 | 0.13266 |
30–34 | 0.03611 | 0.00284 | 0.00455 | − 0.00327 | 0.00965 | 0.00352 | 0.00000 | 0.00420 | 0.00576 | 0.00148 | 0.10084 |
35–39 | 0.03433 | − 0.00625 | 0.00780 | − 0.00452 | 0.01947 | 0.01500 | − 0.00213 | 0.00991 | 0.00829 | − 0.00127 | 0.10779 |
40–44 | 0.00807 | 0.01535 | 0.00331 | − 0.01180 | 0.02731 | 0.00933 | 0.00178 | 0.00431 | 0.00756 | 0.00212 | 0.05813 |
45–49 | 0.01259 | − 0.01041 | 0.00779 | − 0.01072 | 0.02863 | 0.01149 | 0.00173 | 0.01002 | 0.00205 | 0.00335 | 0.05563 |
50–54 | 0.00812 | − 0.07441 | 0.01294 | − 0.01729 | 0.05423 | 0.01028 | 0.00179 | 0.00168 | 0.00068 | − 0.00386 | 0.06511 |
55–59 | 0.05305 | − 0.14131 | 0.01500 | − 0.03211 | 0.10230 | 0.03269 | − 0.01662 | 0.00156 | 0.02402 | − 0.00831 | 0.08172 |
60–64 | 0.00958 | − 0.01842 | 0.01249 | − 0.01045 | 0.03600 | 0.00574 | 0.00334 | − 0.00792 | 0.01326 | 0.00079 | 0.03095 |
65–69 | 0.02553 | − 0.02555 | 0.00258 | − 0.01615 | 0.09469 | 0.02089 | 0.01474 | 0.00804 | 0.01832 | 0.00160 | 0.02674 |
70–74 | 0.01801 | − 0.00278 | − 0.00171 | − 0.00914 | 0.09147 | 0.01551 | 0.01572 | 0.00740 | 0.00899 | − 0.00033 | 0.01550 |
75–79 | 0.02023 | − 0.05563 | 0.00660 | − 0.00980 | 0.16177 | 0.00668 | 0.04401 | 0.03469 | 0.01794 | − 0.00139 | 0.03360 |
80–84 | 0.00568 | − 0.00218 | 0.00482 | − 0.00631 | 0.08153 | 0.01588 | 0.02201 | 0.00855 | 0.00355 | − 0.00025 | 0.00938 |
85 + | 0.04997 | − 0.09302 | 0.01326 | − 0.07994 | 0.31253 | 0.01818 | 0.14263 | − 0.01708 | 0.00858 | − 0.00109 | 0.02639 |
Δ 1995–2007 | 3.06 | ||||||||||
11.7.13 Annex 13. Females, decomposition of the difference in life expectancy at birth between 1987–1995, by age and causes of death, Cuba
Females cause specific component of the time differential 1987–1995 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age groups | Other Causes | Cancer | Diabetes Mellitus | Mental Disorders | Heart Diseases | Cerebrovascular D. | Artery/Arterioles | Respiratory Diseases | Liver/Kidney/Obst | Congenital Malform | External causes |
< 1 | 0.13502 | 0.00166 | 0.00000 | 0.00000 | − 0.01611 | 0.00000 | 0.00000 | 0.00267 | 0.00440 | 0.08244 | 0.02357 |
1–4 | 0.01368 | 0.02329 | 0.00000 | 0.00000 | 0.02084 | 0.00368 | 0.00000 | 0.02608 | − 0.01015 | − 0.07895 | − 0.02700 |
5–9 | − 0.00414 | 0.00745 | − 0.00054 | 0.00000 | − 0.00094 | 0.00014 | 0.00000 | − 0.00135 | 0.00108 | 0.00299 | 0.00586 |
10–14 | 0.00574 | 0.00183 | 0.00000 | 0.00000 | − 0.00039 | − 0.00051 | 0.00000 | 0.00065 | 0.00059 | − 0.00152 | 0.00413 |
15–19 | 0.00251 | 0.00211 | 0.00120 | 0.00000 | 0.00404 | 0.00261 | 0.00000 | 0.00098 | − 0.00179 | 0.00046 | 0.05792 |
20–24 | − 0.00303 | − 0.00053 | − 0.00323 | 0.00000 | 0.00402 | 0.00057 | 0.00000 | − 0.00270 | − 0.00067 | 0.00337 | 0.05235 |
25–29 | 0.01675 | 0.00094 | 0.00140 | 0.00000 | 0.00912 | 0.00791 | 0.00000 | 0.00333 | 0.00157 | 0.00293 | 0.02502 |
30–34 | 0.01554 | 0.00039 | − 0.00177 | 0.00022 | 0.01153 | 0.00543 | 0.00062 | 0.00230 | 0.00148 | − 0.00247 | 0.00616 |
35–39 | 0.00008 | − 0.00043 | 0.00007 | 0.00000 | 0.00065 | 0.00027 | 0.00004 | − 0.00009 | 0.00002 | 0.00005 | 0.00039 |
40–44 | − 0.00378 | − 0.01216 | 0.00221 | 0.00000 | 0.00958 | 0.00283 | − 0.00027 | − 0.00309 | − 0.00166 | − 0.00073 | − 0.01027 |
45–49 | − 0.00863 | 0.01246 | − 0.00397 | − 0.00069 | 0.02060 | 0.01110 | − 0.00053 | − 0.00033 | 0.00222 | − 0.00228 | − 0.00005 |
50–54 | 0.00749 | − 0.01790 | 0.00478 | 0.00000 | 0.04316 | 0.02493 | − 0.00236 | − 0.00441 | 0.00117 | − 0.00356 | 0.00274 |
55–59 | 0.00251 | 0.00918 | 0.00048 | 0.00039 | 0.00836 | 0.01247 | 0.00137 | − 0.00375 | 0.00203 | − 0.00013 | − 0.00583 |
60–64 | − 0.02677 | − 0.01806 | − 0.01040 | − 0.00532 | 0.01593 | 0.01287 | − 0.00713 | − 0.01167 | 0.01928 | − 0.00028 | − 0.00777 |
65–69 | − 0.00700 | 0.00270 | − 0.00688 | − 0.00172 | 0.00763 | − 0.00135 | − 0.00042 | − 0.00188 | 0.00210 | − 0.00045 | − 0.00242 |
70–74 | 0.00752 | − 0.01337 | 0.00039 | 0.00732 | − 0.03160 | 0.00736 | 0.01363 | − 0.00575 | − 0.01509 | − 0.00075 | 0.02072 |
75–79 | 0.00221 | 0.00456 | 0.00027 | − 0.00256 | 0.01442 | 0.00421 | − 0.00021 | 0.00688 | − 0.00050 | − 0.00007 | − 0.00376 |
80–84 | 0.00532 | 0.00291 | 0.00439 | 0.00578 | − 0.00630 | 0.00395 | 0.00184 | − 0.00453 | 0.00014 | − 0.00003 | 0.01300 |
85 + | 0.01058 | − 0.00103 | 0.00106 | 0.00982 | − 0.01019 | 0.01197 | − 0.00052 | − 0.02533 | − 0.00186 | − 0.00006 | 0.02077 |
Δ 1987–1995 | 0.56 | ||||||||||
11.7.14 Annex 14. Females, decomposition of the difference in life expectancy at birth between 1995–2007, by age and causes of death, Cuba
Females cause specific component of the time differential 1995–2007 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age groups | Other Causes | Cancer | Diabetes Mellitus | Mental Disorders | Heart Diseases | Cerebrovascular D. | Artery/Arterioles | Respiratory Diseases | Liver/Kidney/Obst | Congenital Malform. | External causes |
< 1 | 0.16304 | 0.00334 | 0.00000 | 0.00000 | 0.01852 | − 0.00282 | 0.00000 | 0.03028 | − 0.00201 | 0.05161 | 0.01155 |
1–4 | 0.06494 | 0.02288 | 0.00000 | 0.00000 | 0.00957 | 0.00137 | 0.00000 | 0.02584 | 0.00137 | − 0.00889 | 0.02012 |
5–9 | 0.02917 | − 0.01099 | 0.00110 | 0.00000 | 0.00193 | − 0.00027 | 0.00000 | 0.00550 | 0.00193 | 0.00633 | 0.03494 |
10–14 | − 0.00638 | − 0.00119 | 0.00000 | 0.00000 | − 0.00148 | 0.00335 | 0.00000 | 0.00094 | 0.00209 | 0.00754 | 0.04413 |
15–19 | 0.01792 | 0.00213 | 0.00030 | 0.00000 | 0.00119 | − 0.00157 | 0.00000 | 0.00483 | 0.00531 | 0.00561 | 0.07231 |
20–24 | 0.01563 | 0.00148 | 0.00287 | 0.00000 | 0.00592 | 0.00180 | 0.00000 | 0.00772 | 0.00381 | − 0.00028 | 0.07528 |
25–29 | 0.01047 | 0.00458 | 0.00259 | 0.00000 | 0.00467 | 0.00190 | 0.00000 | 0.00311 | 0.00318 | − 0.00108 | 0.05989 |
30–34 | 0.01083 | − 0.00956 | 0.00752 | − 0.00015 | 0.00561 | 0.00374 | 0.00000 | 0.01188 | 0.00433 | 0.00143 | 0.06421 |
35–39 | 0.03419 | 0.01071 | − 0.00021 | 0.00000 | 0.01089 | 0.01182 | 0.00079 | 0.01212 | 0.00584 | − 0.00092 | 0.04275 |
40–44 | 0.00737 | 0.02515 | 0.00253 | 0.00000 | 0.01785 | 0.01772 | 0.00003 | 0.01132 | 0.00727 | 0.00120 | 0.05274 |
45–49 | 0.01486 | − 0.01258 | 0.00801 | 0.00046 | 0.01806 | 0.02175 | 0.00228 | 0.01128 | 0.00286 | 0.00181 | 0.03844 |
50–54 | 0.01529 | − 0.00056 | 0.01418 | − 0.00216 | 0.02699 | 0.02131 | − 0.00124 | − 0.00665 | 0.01104 | 0.00133 | 0.02029 |
55–59 | − 0.00427 | − 0.08477 | 0.04588 | − 0.00334 | 0.09129 | 0.05963 | − 0.00145 | − 0.01837 | 0.01482 | 0.00292 | 0.05138 |
60–64 | 0.02298 | 0.01831 | 0.02302 | 0.00220 | 0.07866 | 0.04198 | 0.00172 | − 0.00206 | 0.00432 | − 0.00003 | 0.03247 |
65–69 | 0.02915 | − 0.03414 | 0.02750 | − 0.00034 | 0.08429 | 0.04710 | 0.00660 | − 0.00493 | 0.00480 | − 0.00002 | 0.02603 |
70–74 | 0.02889 | − 0.08206 | 0.03892 | − 0.01544 | 0.11558 | 0.05311 | 0.04329 | − 0.01448 | 0.01005 | − 0.00125 | 0.05295 |
75–79 | 0.02070 | − 0.12186 | 0.04217 | − 0.04256 | 0.18149 | 0.07752 | 0.06663 | − 0.03049 | 0.02807 | 0.00027 | 0.05899 |
80–84 | 0.01449 | − 0.00190 | 0.01685 | − 0.00853 | 0.07478 | 0.02162 | 0.02314 | 0.00801 | 0.00569 | 0.00024 | 0.01780 |
85 + | 0.03344 | − 0.05624 | 0.04815 | − 0.14420 | 0.35051 | 0.02224 | 0.18390 | − 0.01824 | 0.01045 | − 0.00065 | 0.02244 |
Δ 1995–2007 | 3.12 | ||||||||||
References
Aja, A. (2000). La emigración cubana hacia Estados Unidos a la luz de su política inmigratoria. Working Paper, Colección: Centro de Estudios de Migraciones Internacionales—CEMI/UH, La Habana, Cuba. http://biblioteca.clacso.edu.ar/ar/libros/cuba/cemi/laemig.pdf. Zugegriffen: 2. Okt. 2012.
Aja, A. (2002). La emigración cubana. Balance en el Siglo XX. Working Paper, Colección: Centro de Estudios de Migraciones Internacionales—CEMI/UH, La Habana, Cuba. http://biblioteca.clacso.edu.ar/ar/libros/cuba/cemi/laemig.pdf. Zugegriffen: 2. Okt. 2012.
Albizu-Campos, J. C. (2002). Mortalidad y supervivencia en Cuba en los noventa. La Habana: Centro de Estudios Demográficos- Universidad de La Habana.
Albizu-Campos, J. C. (2003). La esperanza de vida en Cuba en los 90. La Habana: Centro de Estudios Demográficos- Universidad de La Habana.
Annandale, E., & Hunt, K. (2000). Gender inequalities in health: research at the crossroads. In Annandale, E. & Hunt, K. (Eds.) Gender Inequalities in Health (pp. 1–35). Buckingham: Open University Press. (http://www.mcgrawhill.co.uk/openup/chapters/0335203647.pdf)
Bongaarts, J., & Feeney, G. (2002). How long do we live? Population and development Review, 28(1):13–29.(http://onlinelibrary.wiley.com/doi/10.1111/j.1728-4457.2002.00013.x/pdf)
Centro de Estudios de Población y Desarrollo. (2008). Envejecimiento de la Población Cubana. La Habana: Oficina Nacional de Estadísticas.
Chackiel, J. (2004). La dinámica demográfica en América Latina. Población y Desarrollo, Series, 52 (CEPAL).
Christensen, K., Doblhammer, G., Rau, R., & Vaupel, J. (2009). Ageing populations: The challenges ahead. The Lancet, 374.
Fernández, J. M. (2006). Principales Causas de mortalidad general en Cuba. Año 2004. Revista Habanera de Ciencias Médicas, 5(2). (La Habana, Cuba).
González, F., & Ramos, O. (1996). Cuba: Balance e indicadores demográficos estimados del período 1900–1959. La Habana: Centro de Estudios Demográficos (CEDEM), National Statistic Office.
Hernández, R. (1986). El Proceso de La Revolución Demográfica en Cuba. La Habana: Editorial Ciencias Sociales.
López, L. M., Albizu-Campos, J. C., & Gran, M. A. (2005). Evolución del diferencial por sexo de la esperanza de vida al nacer. (Cuba, Siglo XX). Revista Cubana de Salud Pública, 31(3):182–191. (http://scielo.sld.cu/pdf/rcsp/v31n3/spu03305.pdf)
Meslé, F., & Vallin, J. (2004). The health transition: Trends and prospects. In G. Caselli, J. Vallin, & G. Wunsch (eds), Demography: Analysis and synthesis, Vol. II. France: INED.
Nathanson, C. (1984). Sex differences in mortality. Annual Review of Sociology, 10:191–213. (http://www.annualreviews.org/doi/pdf/10.1146/annurev.so.10.080184.001203)
Oeppen, J., & Vaupel, J. (2002). Broken limits to life expectancy. Science, 296:1029–1031.
Oficina Nacional de Estadísticas. (2007). Anuario Demográfico de Cuba, 2006. La Habana: Oficina Nacional de Estadísticas.
Oficina Nacional de Estadísticas. (2008). Esperanza de vida Cuba y provincias, 2005–2007. Cálculos por sexo y edades. La Habana: Oficina Nacional de Estadísticas.
Oficina Nacional de Estadísticas. (2009). Anuario Demográfico de Cuba, 2008. La Habana: Oficina Nacional de Estadísticas.
Oficina Nacional de Estadísticas. (2010). Panorama Económico y Social. Cuba 2009. La Habana: Oficina Nacional de Estadísticas e Información.
Oficina Nacional de Estadísticas. (2011). Anuario Demográfico de Cuba, 2010. La Habana: Oficina Nacional de Estadísticas e Información.
Omran, A. B. (1971). The epidemiological transition. A theory of the epidemiology of population change. Milbank Q., 83(4):731–757 (2005).
Riverón, R., & Azcuy, P. (2001). Mortalidad Infantil en Cuba 1959–1999. Revista Cubana de Pediatría, 73 (3):143–157. (http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75312001000300001&lng=es&nrm=iso)
Rogers, A., & Hackenbert, R. (1987). Extending epidemikologic transition theory: A new stage. Social Biology, 34.
Shkolnikov, V. M., Valkonen, T., Begun, A. Z., & Andreev, E. M. (2001). Measuring inter-group inequalities in length of life. Genus, LVII (3–4):33–62. (http://www.jstor.org/stable/29788701)
Torreira, R., & Buajasan, J. (2000). Operación Peter Pan, un caso de la guerra psicológica contra Cuba. La Habana: Editora Política.
Trovato F. (2005). Narrowing sex differential in life expectancy in Canada and Austria: Comparative analysis (pp. 17–52). Vienna Yearbook of Population Research.
UNICEF. (1995). Cuba, Transición de la Fecundidad. Cambio social y conducta reproductiva. La Habana: CEDEM, ONE, MINSAP, FNUAP.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Gómez León, M., León Díaz, E. (2014). Life Expectancy Differences in Cuba: Are Females Losing Their Advantage Over Males?. In: Anson, J., Luy, M. (eds) Mortality in an International Perspective. European Studies of Population, vol 18. Springer, Cham. https://doi.org/10.1007/978-3-319-03029-6_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-03029-6_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-03028-9
Online ISBN: 978-3-319-03029-6
eBook Packages: Humanities, Social Sciences and LawSocial Sciences (R0)