
Abstract
The Declaration of Alma-Ata in 1978 crystallized a global vision of justice in health, regardless of income, gender, ethnicity, or education, and called for “health for all by the year 2000” through primary health care (PHC). While much progress has been made since the declaration, more than 40 years later and in the midst of the global pandemic of COVID-19, much remains to be done to achieve health for all. This chapter outlines the important values and principles that underlie PHC, with attention to how global health policy has evolved and country trajectories have differed with respect to PHC since its historic debut in 1978. The chapter then identifies the current strategies for PHC in the global context of a pandemic and other challenges and opportunities, to outline an agenda for the renewal of primary health care allied to the movement to achieve universal health coverage.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Primary Health Care and Its Evolution over Four Decades in Global Health
The International Conference on Primary Health Care in Alma-Ata in 1978 represented through its declaration the first articulation of a unifying global vision and strategy for health. The shared outcome of “health for all by the year 2000” was fueled by the strategy of primary health care (PHC). The strategy’s emphasis on primary care reflected widespread concern that recently independent low and middle-income countries were following an inequitable, high-tech, high-cost, hospital-based, urban-focused approach to their health systems as in many high-income countries. Importantly, the PHC strategy extended beyond personal health care services to identifying the importance of engaging other sectoral assets for health such as education, water and sanitation, mobilizing the participation of communities in health systems, and ensuring the development and use of technology that was appropriate in terms of setting and cost.
Progress was made in many low- and middle-income countries, however, the target of “health for all by the year 2000” was missed by a large margin. The reasons were complex but partly entailed a general failure to implement all aspects of the primary health care approach, particularly work across sectors to address social and economic factors that affect health and the mobilization of critical systems inputs including health workers and government financing. Furthermore, despite the consensus in Alma-Ata in 1978, the global health community rapidly became fractured in its commitment to the far-reaching measures called for by the declaration. Economic recession tempered enthusiasm for PHC, and momentum shifted to programs concentrating on a few priority measures for child survival such as growth monitoring, oral rehydration, breast-feeding and immunization leading to calls for more modest and focused efforts around “selective primary health care” [1].
Growing momentum with these initiatives supported the continued movement of health development efforts away from the comprehensive approach of PHC primary health care and toward programs that targeted specific public health priorities. By the 1990s, PHC had fallen out of favor in many global health policy circles reinforced by structural adjustment policies of multi-lateral development banks recommending cuts to public sector spending as a stimulus for economic growth [2]. Consequently, many low- and middle-income countries slashed public sector spending on health and were encouraged to get more health for the money by selecting a package of “best-buy services” [3].
Concerns about losing ground in child immunization and the emergence of the HIV/AIDS pandemic alongside longstanding scourges of tuberculosis and malaria, led to the establishment of the first-ever billion-dollar global funds (GAVI and GFATM) at the turn of the millennium and their inclusion as specific goals in the Millennium Development Goals (MDGs). Despite these focused priorities and unprecedented amounts of development assistance, slower than expected progress in equitable coverage of immunization and treatment for HIV, TB and malaria drew attention to dimensions of the health and social systems in countries that were holding back progress. This led WHO to re-direct global health policy towards PHC with the issuance of a triumvirate of publications on the 30th anniversary of Alma-Ata: (i) the report of the commission on the social determinants of health [4], (ii) a WHO framework to understand the core functions of health systems [5]; and (iii) a World Health Report titled “PHC: now more than ever” [6].
2 Primary Health Care in the Twenty-First Century
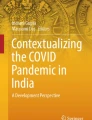
The renewal of PHC advocated four major reforms (see Fig. 41.1. WHR 2008) that would help to remediate three pervasive barriers to progress including: (i) shortfalls in systems performance; (ii) stratifying social conditions; and (iii) skews in science [7]. The first of these recommended reforms gave rise to renewed policy interest in Universal Health Coverage (UHC) [8] and its inclusion as a target under the health goal of Sustainable Development Goals (SDGs) in 2015. Subsequently, the global policy discourse has embraced the synergy between PHC and UHC in the mantra “no UHC without PHC”. In 2018, at the Astana conference to celebrate the 40th anniversary of Alma-Ata, a Declaration reframed PHC as three components: (i) primary care and essential public health functions as the core of integrated health services; (ii) empowered people and communities; and (iii) multisectoral policy and action.

The four reforms of primary health care renewal. (Source: World Health Organization: Primary Health Care: Now More Than Ever. World Health Report 2008)
3 The Bumpy Road to Primary Health Care
Despite this array of global health policy convergence around PHC, the road ahead for all countries regardless of their levels of wealth looks anything but certain [9]. Traditional public financing systems for health and other social sectors are under extreme pressure not only in the wake of the pandemic and in the clutches of widespread inflation but also due to underlying trends towards a gig economy alongside persistently high levels of informal economic transactions that elude taxation. And while mobilization of development assistance and replenishments of global funds remain critical, the total envelope of development assistance ($37 Billion) represents such a small fraction of total health spending in LMICs ($2 trillion) that it must be more effectively deployed as a catalyst to greater domestic financing for health.
The organization and delivery of comprehensive, essential services from promotion to palliation with continuity and quality according to need faces daunting challenges from both the supply and demand sides. On the supply side many countries are seeing a dramatic shift in disease burden toward chronic diseases together with a rapidly growing menu of personalized and/or precision care services in the setting of pervasive health provider constraints manifested in their insufficient numbers, inequitable distribution, inadequate support and deteriorating morale and burnout. Recent estimates indicate a shortage of >18 million health workers globally, constituting a crisis that is greatly exacerbated by the migration of health workers from low- and middle-income countries to high-income countries. Sub-Saharan Africa carries 24% of the global disease burden but has only 3% of the health workforce [10].
On the demand-side, the expectations of patients for timely access to quality care are rising everywhere alongside growing skepticism and hesitancy with respect to trust in science and public health best buys like vaccines. At the same time, calls to decolonize and democratize global health are redefining the meaning of participation and community empowerment so central to the Alma-Ata declaration in 1978 and placing overdue demands on fair and accountable leadership for health nationally and globally. These demands on leadership are accentuated by the wider global context characterized by more frequent and severe infectious and climate-mediated health emergencies placing unprecedented pressures for coordinated multi-sectoral surge response capacity both within national boundaries and globally.
Despite this dizzying array of challenges that are both longstanding and new, there is ample evidence of remarkable progress and achievement with respect to PHC. Bangladesh, for example, has surged from one of the most impoverished nations on earth at the time of its independence in 1971 to achieve unprecedented health gains and improvements in health equity. The reasons include a society-wide mobilization around PHC inclusive of a focus on the empowerment of poor women through education, access to microcredit and primary care services made available by an army of community health workers [11]. Similar stories of PHC success through mass deployment of community health workers are found in Ethiopia, India and Niger. In middle-income countries like Brazil, Chile and Turkey in the setting of universal health care reforms, multi-disciplinary health teams have been dispatched to the front-lines together with social welfare benefits for disadvantaged groups resulting in accelerated improvements in health amongst those segments of the population previous left behind [12].
Further, recent breakthroughs in information and communication technologies like cell phones and drones are leading to innovative PHC applications that are transcending long standing PHC bottlenecks related to limited health providers and unreliable supply chains. While the primary health care approach has often been sidelined in the initial COVID-19 response, with a focus on hospitals and parallel delivery mechanisms, there have also been encouraging signs of the potential of PHC with dramatic increased uptake of the use of telemedicine and clinical support via digital means.
These and other examples of success, support Nobel Laureate Angus Deaton’s prescient remarks in his World Institute for Development Economics Research annual lecture on September 29, 2006, “People in poor countries are sick not primarily because they are poor but because of other social organizational failures, including health delivery, which are not automatically ameliorated by higher income.” Ensuring social organizational failures and successes are not dismissed as “outliers” and can inform reforms more widely requires re-directing global health policy efforts from the traditional centres of Geneva and Washington to the front-lines of health systems where the most exciting breakthroughs, in the face of overwhelming odds, abound. Primary health care’s future is a bright one in this century provided policy and research move to the front-lines first!
The current COVID-19 pandemic has made the shortfalls in PHC more glaringly visible than ever, but has also mobilized awareness of its importance at the highest levels. Out of this crisis, then, lies an opportunity to recast global and national systems to enable an exciting new chapter to implement primary health care in all countries.
References
Walsh JA, Warren KS. Selective primary health care: an interim strategy for disease control in developing countries. N Engl J Med. 1979;301(18):967–74.
Kim JY. In: Kim JY, Millen JV, Irwin A, Greshman J, editors. Dying for growth: global inequality and the health of the poor. Monroe, ME: Common Courage Press; 2000. p. 604.
World Development Report 1993: Investing in Health. New York: World Bank; 1993. p. 348.
Closing the Gap in a Generation: health equity through action on the social determinants of health—Final report of the commission on social determinants of health. Geneva: World Health Organization; 2008. p. 33https://www.who.int/publications/i/item/WHO-IER-CSDH-08.1
Everybody’s business—strengthening health systems to improve health outcomes: WHO’s framework for action. Geneva: World Health Organization; 2007. p. 44. https://apps.who.int/iris/handle/10665/43918
The World Health Report 2008: Primary Health Care Now More Than Ever. Geneva: World Health Organization; 2008. p. 119.
Evans T, Rasanathan K. Primary care and global health, Chapter 474. In: Harrison’s principles of internal medicine. McGraw Hill; 2022.
Pablos A, Evans T. Universal health coverage and global health, Chapter 42 in this book. Springer Nature; 2023.
World Health Organization 2006 World Health Report 2006, Working Together for Health.
Rasanathan K, Evans TG. Primary health care, the Declaration of Astana and COVID-19. Bull World Health Organ. 2020;98:801–8.
Bangladesh: Innovation for Universal Health Coverage, Lancet Series; November 22, 2013.
Aquino R, de Oliveira NF, Barreto ML. Impact of the family health program on infant mortality in Brazilian municipalities. Am J Public Health. 2009;99(1):87–93. https://doi.org/10.2105/AJPH.2007.127480.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Evans, T.G., Rasanathan, K. (2023). Primary Health Care and Global Health. In: Raviglione, M.C.B., Tediosi, F., Villa, S., Casamitjana, N., Plasència, A. (eds) Global Health Essentials. Sustainable Development Goals Series. Springer, Cham. https://doi.org/10.1007/978-3-031-33851-9_41
Download citation
DOI: https://doi.org/10.1007/978-3-031-33851-9_41
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-33850-2
Online ISBN: 978-3-031-33851-9
eBook Packages: MedicineMedicine (R0)