
Abstract
There is a growing awareness that radiation dose originating from medical diagnostic procedures in radiology is contributing an increasing proportion of the total population dose, especially for examinations using computed tomography (CT). In response to the heightened awareness of the importance of patient dose contributed by radiology procedures, there has been a general trend to optimise CT examinations to obtain the required diagnostic outcome while minimising the dose to the patient. This chapter describes various options for dose optimisation in CT colonography (CTC). These techniques are not necessarily unique to CTC and can be applied for optimisation of CT scan protocols for other sites as well. Dose reduction tools discussed include: tube current reduction and automatic tube current modulation, tube voltage, iterative reconstruction, filtration, active collimation, CT detectors, shielding, and other factors such as pitch and slice thickness.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
6.1 Introduction
The publications 103 and 105 of the International Commission on Radiological Protection (ICRP) clearly identify two key elements in radiation protection in medicine: justification and optimisation [1, 2]. In one sentence, these principles could be summarised as ‘doing the right procedure’ and ‘doing the procedure right’, respectively.
In 2012, the International Atomic Energy Agency (IAEA) held a conference on radiation protection in medicine in Bonn, Germany. The conference was co-sponsored by the World Health Organisation (WHO): the specific outcome of the conference was the Bonn Call-For-Action [3]. The aims of the Bonn Call-For-Action include: to strengthen the radiation protection of patients and health workers; to attain the highest possible benefit with the least possible risk by the safe and appropriate use of ionising radiation in medicine; and to enhance the safety and quality of radiological procedures in medicine. Ten main actions were identified as being essential. They include enhancing the principle of justification; the implementation of the principle of optimisation; strengthening radiation protection education and training of health professionals; increase access to information on medical exposure globally; and foster an improved radiation-risk-dialogue.
6.2 Justification
There are three levels of justification for a procedure in medicine [1]. The use of radiation in medicine, at the most general level, is accepted as doing more good than harm. At the second level, a specified procedure with a specified objective is defined and justified; for example, a CTC study to detect polyps. The aim of this generic justification is to determine whether the procedure will improve the diagnosis or treatment. At the third level, the application of the procedure to an individual must be justified and judged to do more good than harm to that particular patient.
6.3 Optimisation
Optimisation is the process of determining how to obtain the required diagnostic outcome for a patient from a procedure while minimising factors that cause patient detriment, with economic and societal factors being taken into account. Optimisation is intended for those situations that have been deemed to be justified [1]. Optimisation involves input from a radiologist, radiographer, and medical physicist. It also includes the concept of maximising the benefit of the use of radiation while minimising the risk of detriment. Therefore, a knowledge of risk estimation may be important in optimisation in clinical practice. The concept of ALARA (as low as reasonably achievable) should be applied whenever possible.
6.3.1 Risk
Radiation exposure from CT is associated with an increase in risk for fatal cancer, especially in paediatric CT scanning [4,5,6]. The lifetime cancer mortality risk for a 1-year-old patient attributable to the radiation exposure from an abdominal CT is estimated to be 0.18%, which is about an order of magnitude higher than for adults [7]. An estimate for the absolute lifetime cancer risk associated with the radiation exposure from CTC is about 0.14% for paired CTC scans for a 50-year-old, and about half of that for a 70-year-old [8]. Most of the quantitative data regarding the risk of radiation-induced cancer comes from studies of the atomic bomb survivors from Japan [9]. According to the BEIR VII Phase 2 report [9] approximately 42 of 100 people will be diagnosed with cancer from causes unrelated to radiation; a single exposure of 100 mSv of X-ray radiation could result in approximately one additional cancer in 100 people. The risk depends on age and sex, with a higher risk for females and those exposed at younger ages. Typical CT exposures result in doses substantially smaller than that; nonetheless, some argue that the risks of medical radiation should form part of an informed consent process [10] (see Chaps. 2 and 3). While the increased risk of a radiation-induced cancer is small for any one individual, the risk to the population as a whole is considerable, given the large number of CT scans performed worldwide [5]. A risk-benefit analysis to estimate the ratio of cancers prevented to induced for CTC screening every 5 years from age 50 to 80 showed that the benefits from such screening outweighs the risk substantially; the estimated number of radiation-related cancers from CTC screening every 5 years in that age bracket was 150 cases/100,000 individuals, while the estimated number of colorectal cancers prevented ranged from 3580 to 5190/100,000, yielding a benefit-risk ratio that varied from 24:1 to 35:1 [11].
Increasing concerns about radiation dose have led CT manufacturers to develop dose reduction tools for their CT scanners [12]. It was shown that specifically for CTC large dose reductions are possible without losing diagnostic quality [13]. Effective doses from low-dose CTC are lower than those from a double-contrast barium enema [14, 15].
6.4 Patient Dose in CT: Controllable and Built-in Factors
A number of controllable and built-in factors influencing patient dose in CT are discussed below.
6.4.1 Tube Current
The most straightforward way to reduce radiation dose is to reduce the tube current (mAs). There is a linear relationship between dose and mAs; decreasing mAs will however result in increased image noise and thus decreased image quality. There is a wide tolerance for image noise in CTC [16]. A number of studies [17,18,19,20] have shown that decreases in the tube current can still maintain accuracy for the purposes of polyp detection in CTC.
6.4.2 Automatic Tube Current Modulation
For most patients, the anterior–posterior (AP) dimension is smaller than the lateral dimension. This means there is a larger attenuation of radiation in the lateral projections when compared to the AP projections. Less radiation will reach the detectors to produce an image for the lateral projections. The tube current can therefore be reduced for the AP projections while still maintaining the same noise level as the lateral projections [21]. The tube current may be modulated according to patient attenuation or using a sinusoidal-type function. The modulation may be fully pre-programmed, implemented in near-real time using a feedback mechanism, or achieved using a combination of pre-programming with a feedback loop [22]. As shown in Fig. 6.1, the smaller patient thickness in the AP direction (and thus less attenuation of the X-ray beam) allows for a reduction in tube current for those projections.

Tube current modulation
Automatic dose modulation can occur in the X–Y axis as described above, and also along the Z-axis [23] where the dose can be reduced in more radiolucent parts of the body (e.g. over the lungs). Both approaches are now also commonly combined resulting in an X–Y–Z axis dose modulation [16]. These approaches typically use the AP and lateral CT scout images to predict the amount of dose modulation in the scan. In a CTC screening population, the dose to patients was significantly lower (at least 33%) when tube current modulation was applied with X-, Y-, and Z-axis tube modulation, when compared to X- and Y-axis tube current modulation only [24].
Another approach for dose reduction is an organ-based tube-current modulation [25] to reduce the radiation dose to superficial radiosensitive organs: the lens of the eye, thyroid, and breast, for example. This is done by decreasing the tube current when the tube passes closest to these organs: to maintain the same noise level, the dose is increased for the opposing projections.
It has been shown in CTC [26] that the amount of stool and fluid tagging, using tagging agents such as iodine and barium, does not significantly affect the radiation exposure when using automatic exposure control.
6.4.3 Tube Voltage
Decreasing the X-ray tube voltage from 140 to 80 kVp decreases the CTDIvol (computed tomography dose index) by about a factor of 4 [27], while a tube voltage reduction in CTC from 120 to 100 kVp resulted in a 20% decrease in CTDIvol in one study, but with only a minimal decrease in 3D image quality at all patient sizes [28]. The CTDI is measured in a phantom and not in a patient, but the dose reduction potential remains with a reduction in tube voltage. A reduction in kVp will result in a less penetrative beam and an increase in image noise. Therefore, reducing the kVp for large patients should be done with caution because conventional dose modulation approaches will increase the tube current to make up for the increased noise in the image, which in turn can reverse any dose savings. It has been shown that at a constant kVp, increasing the patient weight from 10 kg (kilogram) to 120 kg reduces the transmission of X-ray intensity for abdominal CT scanning by about a factor of 100 [29]. One approach is to set the kVp according to patient weight [16], whereas another approach takes into account the patient size and diagnostic task [30].
The ability to automatically select the tube potential can also be an effective approach for dose reduction [31]. This has been implemented on some CT scanners using the topogram, which provides information about the attenuation in the patient along the patient length axis and, on the basis of that information, the required tube current is calculated for the different kVs to obtain a specified image quality. An overall dose reduction of over 25% was reported for 40 patients undergoing abdominal CT angiography (CTA) compared with a standard protocol using 120 kVp [32].
6.4.4 Iterative Reconstruction
Iterative reconstruction is well established in nuclear medicine. It is becoming more popular for CT image reconstruction. The concept of iterative reconstruction was used in the first transmission CT efforts in the early 1970s, but was not practical for fast high-resolution CT [33]. The increase in computing power, and the ongoing efforts for lower doses in CT, have changed the situation: the first CT vendor introduced iterative reconstruction in 2008 [33]. Familiar vendor names include iDose (Philips Healthcare), IRIS and SAFIRE (Siemens), AIDR 3D or ADMIRE (Toshiba/Canon), and ASIR or VEO MBIR (GE Healthcare).
All iterative reconstruction methods consist of three major steps, which are repeated iteratively (i.e., repeatedly). In the first step, a set of projections from an estimated volumetric object is generated to create artificial raw data. This data is then compared to the real measured raw data in the second step and a correction term is computed, which is then applied to the volumetric object in the third step. This becomes the new estimate and the process is repeated until a fixed number of iterations is reached or until the updates/correction terms between the various projections are considered small enough. The initial guess for the volumetric object can be an empty image, or an image estimate that uses prior information; a standard filtered back-projection image, for example. The iterative reconstruction methods differ mainly in how the actual and estimated projections are compared and how the correction term is computed [33].
Projections might be examined for points likely to result from noisy projections. Noisy data are penalised and edges are preserved during reconstruction. An added benefit of iterative reconstruction is that beam hardening artefacts can potentially be reduced [34] and that incomplete or noisy data can still be reconstructed [35,36,37].
Iterative reconstruction techniques can allow scanner-specific models and statistical noise models to be included in the reconstruction to help eliminate noise and so bring the dose down [38]. Iterative reconstruction has allowed large dose reductions (32% or more) when compared to filtered back projection without the loss of diagnostic information [39, 40]. Iterative reconstruction allowed for a dose reduction of 10–24% in abdominopelvic multidetector CT examinations in one study and an average abdominal CT radiation dose decrease of 25.1% in another study [41] when compared to filtered backprojection image reconstruction [42]. Another pilot study [43] showed that the radiation dose during CTC can be reduced 50% below currently accepted low-dose techniques without significantly affecting image quality when an adaptive statistical iterative reconstruction technique was used for image reconstruction. While there is some variation in the amount of dose saving, there is a significant dose reduction in all cases.
6.4.4.1 Use of Artificial Intelligence in CT Image Reconstruction
Artificial intelligence (AI) is an emerging technique in CT image reconstruction [44]. These types of techniques can be used to improve image quality, or conversely reduce patient dose, in computed tomography [45]. The first commercial algorithms are already FDA approved in the United States. Image denoising is often the first step in CT image processing, and several deep learning methods are available for this step [46] and show promise in reducing image noise, without a loss of spatial resolution [47, 48]. Alternatively, deep learning (a subset of AI) can be used to aid the iterative reconstruction process by producing high-dose images from lower dose data, or by “learning” how to differentiate noise from signal.
Deep learning will also have a significant role to play in sparse-sampling CT, where the number of acquired image projections are reduced and dose reductions of over 50% are reported [46]. Deep learning-based reconstruction algorithms have certain limitations: large and applicable training datasets are required, as well as ground-truth data. The reduced noise or improved contrast-to-noise ratio may make for pretty viewing, but there is limited data on direct comparisons of diagnostic accuracy between different reconstruction methods [44]. The principles of AI are presented in Chap. 25.
6.4.5 Pre-patient Beam Filter
Since the cross-section of patients is well approximated by an oval shape, special bowtie filters are nowadays common in CT systems for attenuating the beam at the periphery, while keeping the intensity in the central portion of the beam [31]. Different filters can be used for different fields-of-view (FOV) or patient sizes [49] to reduce the radiation dose to the patient, especially the skin dose [50].
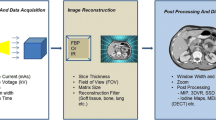
6.4.6 Active Collimators: Over-Ranging
In helical scanning exposure is needed before the start and after the end of the planned scan range in order to reconstruct images at these positions [51]. This over-ranging requires at least one extra gantry rotation, even though only a small portion of this data is utilised for image reconstruction.
For a given beam collimation, the observed Z-over-ranging depends on slice width and pitch [52]. Z-over-ranging increases with increasing cone angle of large Z-axis coverage multidetector CT scanners [53]. Active collimation synchronises the width of the X-ray beam at the ends of the scan range to the clinically useful area needed for image reconstruction. The pre-patient collimator asymmetrically opens and closes at the beginning and end of each spiral scan, temporarily blocking those parts of the X-ray beam that are not used for image reconstruction. Percentage dose reductions, when using active collimation, are larger for short scan lengths and greater pitch values [54]. Figure 6.2(i) shows the concept of over-ranging, with the first and last full rotation of the gantry shown in a darker shade of grey. Figure 6.2(ii) explains how dose is deposited outside of the planned scan length because of over-ranging. Active collimation (Fig. 6.2(iii)) reduces the dose outside of the planned scan length by opening and closing the collimator asymmetrically.

(i), (ii) Over-ranging— the deposition of dose outside of the planned scan length. (iii) Active collimation to block parts of the beam that are not used for image reconstruction at the beginning and end of each spiral scan
6.4.7 Detector Material
The X-ray detector is a very important determinant of the dose performance of a CT system [49]. Two dose-relevant characteristics of a detector are quantum detection efficiency and geometrical efficiency, which together describe the effectiveness of the detector in converting X-rays to a signal. Solid state or ceramic scintillators with a fast response, low electronic noise, and a high light output are preferred over and more efficient than the xenon gas detectors that were common in the 1980s [55]. To improve radiation dose efficiency, advances in the detector material and system electronics are needed. For example, integrating detector components to reduce electronic noise or minimising detector to detector cross-talk [31]. In one study, CTC images acquired using an integrated circuit detector had significantly lower noise than images acquired using the conventional detector, which allowed for a dose reduction of approximately 20% to result in similar levels of image noise [56]. Some advances in detector materials are also described in Chap. 26.
6.4.8 Shielding
External shielding may be useful in reducing radiation exposure to parts of the body that are not in the examination field [57]. Use of shielding for radiation-sensitive tissues and organs in the examination field is generally not recommended [58] because of an increase in noise and beam-hardening artefacts.
6.4.9 Pitch
In single slice CT scanning, pitch is defined as the patient couch movement per rotation divided by the slice thickness. In multislice CT, this definition is altered slightly to patient couch movement per rotation divided by the beam width [59]. A pitch of less than 1, i.e. small couch increments, yields an improved spatial resolution along the Z-axis (along the length of the patient), but also results in higher patient doses because of overscanning (like in Fig. 6.3(i)). For pitches >1 patient dose is less, but data must be interpolated to preserve spatial resolution along the Z-axis (like in Fig. 6.3(ii)) [60]. By increasing the pitch, with a fixed scan length and mA, the radiation dose is reduced. The detectability of small lesions may be reduced due to a lower dose and an increase in image noise.

(i), (ii) Explanation of pitch
6.4.10 Slice Thickness
Thinner slices mean an increase in noise if all the other scanning parameters remain the same. The noise is increased because the number of X-rays used to form an image is reduced in proportion to the slice thickness [60]. A decrease in slice thickness by 50% will necessitate a dose increase by a factor of 2 to fully compensate.
6.4.11 Matrix Size
Choosing a larger matrix (more pixels) will increase the noise per pixel and will decrease the contrast if all other scanning parameters remain the same. Care must be taken to choose an appropriate matrix size.
6.5 Other Practical Dose Saving Approaches
The most obvious dose saving approach is to limit multiple scans and to perform only indicated CTC examinations. Another approach to reduce overall dose is to minimize the number of scan phases and limit the scan volume to the colon only [16]. Correct patient positioning is very important for the proper functioning of the automatic dose modulation and to optimise the image quality; bowtie filters work most efficiently when a patient is positioned in the gantry isocentre. If this is not the case, then the X-ray beam is not attenuated appropriately, which can lead to an increased patient dose. Additionally, because of the lower tube currents with automatic exposure control, unintentional X-ray beam attenuation can cause an unwanted increase in image noise or beam-hardening artefacts [61].
6.6 Diagnostic Reference Levels as an Optimisation Tool
Diagnostic reference levels (DRLs) are dose levels for typical examinations of groups of standard-sized patients [62]. The ICRP states in publication 105 [2] that it is inappropriate to set dose limits or dose constraints for patient exposures because the medical condition is more significant than the potential for radiation harm arising from any justified exposure. Dose management is implicit in dose optimisation, and the patient doses can only be managed if the magnitude and range of doses encountered for a study are known. Diagnostic reference levels (DRLs) can then be set using this data and local practice can be improved by comparing the institution’s data with appropriate DRLs. Radiology department should set local DRLs by taking into account appropriate national or international DRLs [62].
There are ongoing efforts to tally the CT dose metrics, in particular the CTDIvol and dose-length product (DLP), for various studies for the purpose of comparing dose levels. In the European Union, DRLs are required by law [62]. DRLs do not represent a dose constraint for individual patients but give an indication of the boundary between good or normal and bad practice. The DRL is usually set at the 75th percentile of the distribution of doses for a particular examination. If the typical average dose for a given procedure is consistently high compared to the set DRL, this could point to the necessity for dose optimisation and adaptation of local practice [62].
A search for published data on DRLs in CTC yielded very few results. One paper [63] referenced the 2016 UK data [64], which proposed a DRL of the CTDI of 11 mGy and of the DLP of 950 mGy cm. This data was updated in 2019 [65]. The 2019 dataset contained 16,842 patients from 92 hospitals and reported a third quartile DLP of the medians of the submitted datasets of 685 mGy cm, while the CTDI was reported at 6 mGy. This is an indication that an awareness of the patient doses can result in significant dose savings.
6.7 Ethics in Radiology Imaging
A 2022 publication of the WHO underscores the importance of ethics in imaging in terms of justification, optimisation and dose limitation in medical imaging [66]. The WHO also issued six guiding principles with respect to the design and use of AI in health [67] (the principles of AI are discussed in Chap. 25). These aspects with respect to dose optimisation should be considered in CTC clinical audits. The principles of the latter are presented in Chap. 27.
Key Messages
-
Justification means ordering the right procedure for a specific clinical indication; optimisation means obtaining the required diagnostic information with a minimum detriment to the patient, taking into account economic and societal factors.
-
An increase in the use of ionising radiation in medicine has led to a higher dose awareness and thus to increased pressure to optimise the procedures to keep the doses as low as reasonably achievable, while still maintaining diagnostic quality of images.
-
CT vendors have introduced many dose-saving features, like automatic tube current modulation, new detectors, filters, or iterative reconstruction algorithms. Many of the newer innovations come at a premium and will have to be specified before the purchase of a CT scanner.
-
However, the CT operator still has a number of variables to adjust to try and reduce the dose while maintaining image quality. These include the tube voltage and current, the slice thickness, and the pitch.
-
Multiple and repeat scans should be limited as far as possible. Proper patient positioning on the CT couch is vital and often overlooked as a dose-saving feature.
-
Diagnostic reference levels (DRLs) are not a dose-limiting tool in any given patient examination. They do however provide a good indication whether the radiological practice is operating at reasonable dose levels.
6.8 Conclusion
In response to the awareness of an increased population radiation burden, campaigns such as Image Gently (the alliance for radiation safety in paediatric imaging) and Image Wisely (radiation safety in adult medical imaging) were started. Their goal is to raise awareness of the opportunities to lower radiation dose in the imaging of children and adults, respectively, by providing information and free educational materials. Any imaging procedure that uses ionising radiation should be justified, and once it has been justified it should be optimised.
Optimised protocols are essential in any dose reduction programme. It does not matter how sophisticated the dose reduction hardware and software is if it is not fully utilised. Dose reduction techniques often remain underused, but CTC is an imaging examination that can tolerate a relatively high level of noise compared to most other abdominal CT protocols. This allows for aggressive attempts at dose optimisation while preserving the diagnostic image quality. In addition, it is essential to promote and facilitate the implementation of a quality assurance programme, which includes appropriate training, use of well-designed and maintained equipment that is in proper operating condition, suitable and optimised examination protocols, and adequate viewing conditions for image interpretation.
References
ICRP. The 2007 Recommendations of the international commission on radiological protection, vol. 103. Vienna: ICRP Publication; 2007.
ICRP. Radiological protection in medicine, vol. 105. Vienna: ICRP Publication; 2007.
World Health Organization. Bonn call-for-action: joint position statement by IAEA and WHO. Geneva: World Health Organization; 2013.
Chodick G, Ronckers CM, Shalev V, Ron E. Excess lifetime cancer mortality risk attributable to radiation exposure from computed tomography examinations in children. Isr Med Assoc J. 2007;9(8):584.
Shah NB, Platt SL. ALARA: is there a cause for alarm? Reducing radiation risks from computed tomography scanning in children. Curr Opin Pediatr. 2008;20(3):243–7.
Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. N Engl J Med. 2007;357(22):2277–84.
Brenner DJ, Elliston CD, Hall EJ, Berdon WE. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR. 2001;176(2):289–96.
Brenner DJ, Georgsson MA. Mass screening with CT colonography: should the radiation exposure be of concern? Gastroenterology. 2005;129(1):328–37.
National Research Council. BEIR VII phase 2 Report. Health risks from exposure to low levels of ionizing radiation. Washington, DC: The National Academies Press; 2006. p. 2.
Semelka RC, Armao DM, Elias J Jr, Picano E. The information imperative: is it time for an informed consent process explaining the risks of medical radiation? Radiology. 2012;262(1):15–8.
de González AB, Kim KP, Knudsen AB, Lansdorp-Vogelaar I, Rutter CM, Smith-Bindman R, et al. Radiation-related cancer risks from CT colonography screening: a risk-benefit analysis. AJR. 2011;196(4):816.
Raman SP, Johnson PT, Deshmukh S, Mahesh M, Grant KL, Fishman EK. CT dose reduction applications: available tools on the latest generation of CT scanners. J Am Coll Radiol. 2013;10(1):37–41.
Cohnen M, Vogt C, Beck A, Andersen K, Heinen W, vom Dahl S, et al. Feasibility of MDCT colonography in ultra-low-dose technique in the detection of colorectal lesions: comparison with high-resolution video colonoscopy. AJR. 2004;183(5):1355–9.
Neri E, Faggioni L, Cerri F, Turini F, Angeli S, Cini L, et al. CT colonography versus double-contrast barium enema for screening of colorectal cancer: comparison of radiation burden. Abdom Imaging. 2010;35(5):596–601.
Hirofuji Y, Aoyama T, Koyama S, Kawaura C, Fujii K. Evaluation of patient dose for barium enemas and CT colonography in Japan. BJR. 2009;82:219–27.
Chang KJ, Yee J. Dose reduction methods for CT colonography. Abdom Imaging. 2013;38(2):224–32.
Iannaccone R, Laghi A, Catalano C, Brink JA, Mangiapane F, Trenna S, et al. Detection of colorectal lesions: lower-dose multi-detector row helical CT colonography compared with conventional colonoscopy. Radiology. 2003;229:775–81.
Iannaccone R, Catalano C, Mangiapane F, Murakami T, Lamazza A, Fiori E, et al. Colorectal polyps: detection with low-dose multi-detector row helical CT colonography versus two sequential colonoscopies. Radiology. 2005;237(3):927–37.
van Gelder RE, Venema HW, Serlie IW, Nio CY, Determann RM, Tipker CA, et al. CT colonography at different radiation dose levels: feasibility of dose reduction. Radiology. 2002;224(1):25–33.
van Gelder RE, Venema HW, Florie J, Nio CY, Serlie IW, Schutter MP, et al. CT colonography: feasibility of substantial dose reduction—comparison of medium to very low doses in identical patients. Radiology. 2004;232(2):611–20.
Kalender WA, Wolf H, Suess C. Dose reduction in CT by anatomically adapted tube current modulation. II. Phantom measurements. Med Phys. 1999;26(11):2248–53.
McCollough CH, Bruesewitz MR, Kofler JM Jr. CT dose reduction and dose management tools: overview of available options. Radiographics. 2006;26(2):503–12.
Flohr TG, Schaller S, Stierstorfer K, Bruder H, Ohnesorge BM, Schoepf UJ. Multi-detector row CT systems and image-reconstruction techniques. Radiology. 2005;235(3):756–73.
Graser A, Wintersperger B, Suess C, Reiser M, Becker C. Dose reduction and image quality in MDCT colonography using tube current modulation. AJR. 2006;187(3):695–701.
Duan X, Wang J, Christner JA, Leng S, Grant KL, McCollough CH. Dose reduction to anterior surfaces with organ-based tube-current modulation: evaluation of performance in a phantom study. AJR. 2011;197(3):689–95.
Lim HK, Lee KH, Kim SY, Kim KJ, Kim B, Lee H, et al. Does the amount of tagged stool and fluid significantly affect the radiation exposure in low-dose CT colonography performed with an automatic exposure control? Eur Radiol. 2011;21(2):345–52.
Elojeimy S, Tipnis S, Huda W. Relationship between radiographic techniques (kilovolt and milliampere-second) and CTDIvol. Radiat Prot Dosim. 2010;141(1):43–9.
Chang KJ, Caovan DB, Grand DJ, Huda W, Mayo-Smith WW. Reducing radiation dose at CT colonography: decreasing tube voltage to 100 kVp. Radiology. 2013;266(3):791–800.
Huda W, Scalzetti EM, Levin G. Technique factors and image quality as functions of patient weight at abdominal CT. Radiology. 2000;217(2):430–5.
Yu L, Li H, Fletcher JG, McCollough CH. Automatic selection of tube potential for radiation dose reduction in CT: a general strategy. Med Phys. 2010;37(1):234–43.
Ramirez-Giraldo J, Primak A, Grant K, Schmidt B, Fuld M. Radiation dose optimization technologies in multidetector computed tomography: a review. Med Phys. 2014;2(2):420–30.
Winklehner A, Goetti R, Baumueller S, Karlo C, Schmidt B, Raupach R, et al. Automated attenuation-based tube potential selection for thoraco-abdominal computed tomography angiography: improved dose effectiveness. Investig Radiol. 2011;46(12):767–73.
Beister M, Kolditz D, Kalender WA. Iterative reconstruction methods in X-ray CT. Phys Med. 2012;28(2):94–108.
Elbakri I, Fessler J. Statistical image reconstruction for polyenergetic X-ray computed tomography. IEEE Trans Med Imaging. 2002;21(2):89–99.
Lasio GM, Whiting BR, Williamson JF. Statistical reconstruction for X-ray computed tomography using energy-integrating detectors. PMB. 2007;52(8):2247.
Candès EJ, Romberg J, Tao T. Robust uncertainty principles: exact signal reconstruction from highly incomplete frequency information. IEEE Trans Inf Theory. 2006;52(2):489–509.
Sidky EY, Kao C-M, Pan X. Accurate image reconstruction from few-views and limited-angle data in divergent-beam CT. 2009. https://arxiv.org/abs/0904.4495.
Irwan R, Nakanishi S, Blum A. AIDR 3D-reduces dose and simultaneously improves image quality. Tokyo: Toshiba Medical Systems; 2014. https://www.toshiba-medical.eu/eu/wp-content/uploads/sites/2/2014/10/AIDR-3D-white-paper1.pdf
Pontana F, Duhamel A, Pagniez J, Flohr T, Faivre J-B, Hachulla A-L, et al. Chest computed tomography using iterative reconstruction vs filtered back projection (part 2): image quality of low-dose CT examinations in 80 patients. Eur Radiol. 2011;21(3):636–43.
Hara AK, Paden RG, Silva AC, Kujak JL, Lawder HJ, Pavlicek W. Iterative reconstruction technique for reducing body radiation dose at CT: feasibility study. AJR. 2009;193(3):764–71.
Prakash P, Kalra MK, Kambadakone AK, Pien H, Hsieh J, Blake MA, et al. Reducing abdominal CT radiation dose with adaptive statistical iterative reconstruction technique. Investig Radiol. 2010;45(4):202–10.
Desai G, Thabet A, Elias A, Sahani D. Comparative assessment of three image reconstruction techniques for image quality and radiation dose in patients undergoing abdominopelvic multidetector CT examinations. BJR. 2013;86(1021):20120161.
Flicek KT, Hara AK, Silva AC, Wu Q, Peter MB, Johnson CD. Reducing the radiation dose for CT colonography using adaptive statistical iterative reconstruction: a pilot study. AJR. 2010;195(1):126–31.
Zhang Z, Seeram E. The use of artificial intelligence in computed tomography image reconstruction—a literature review. J Med Imaging Radiat Sci. 2020;51:671–7. https://doi.org/10.1016/j.jmir.2020.09.001.
Lee T, Seeram E. The use of artificial intelligence in computed tomography image reconstruction: a systematic review. Radiology. 2020;4(2):30–8. https://doi.org/10.17140/ROJ-4-129.
Singh R, Wu W, Wang G, Kalra M. Artificial intelligence in image reconstruction: the change is here. Phys Med. 2020;79:113–25.
McCollough C, Leng S. Use of artificial intelligence in computed tomography dose optimisation. Ann ICRP. 2020;49(1):113–25. https://doi.org/10.1177/0146645320940827.
Missert A, Yu L, Leng S, Fletcher J, McCollough C. Synthesizing images from multiple kernels using a deep convolutional network. Med Phys. 2020;2:422–30. https://doi.org/10.1002/mp.13918.
Toth TL, Cesmeli E, Ikhlef A, Horiuchi T. Image quality and dose optimization using novel X-ray source filters tailored to patient size. Int Soc Opt Eng. 2005;5745:283–91.
Yu L, Liu X, Leng S, Kofler JM, Ramirez-Giraldo JC, Qu M, et al. Radiation dose reduction in computed tomography: techniques and future perspective. Imaging Med. 2009;1(1):65–84.
Nicholson R, Fetherston S. Primary radiation outside the imaged volume of a multislice helical CT scan. BJR. 2002;75(894):518–22.
Tzedakis A, Damilakis J, Perisinakis K, Stratakis J, Gourtsoyiannis N. The effect of z overscanning on patient effective dose from multidetector helical computed tomography examinations. Med Phys. 2005;32(6):1621–9.
Walker MJ, Olszewski ME, Desai MY, Halliburton SS, Flamm SD. New radiation dose saving technologies for 256-slice cardiac computed tomography angiography. Int J Cardiovasc Imaging. 2009;25(2):189–99.
Christner JA, Zavaletta VA, Eusemann CD, Walz-Flannigan AI, McCollough CH. Dose reduction in helical CT: dynamically adjustable z-axis X-ray beam collimation. AJR. 2010;194(1):W49–55.
Von der Haar T, Klingenbeck-Regn K, Hupke R. Improvement of CT performance by UFC detector technology. Advances in CT IV. Berlin: Springer; 1998. p. 9–15.
Liu Y, Leng S, Michalak GJ, Vrieze TJ, Duan X, Qu M, et al. Reducing image noise in computed tomography (CT) colonography: effect of an integrated circuit CT detector. J Comput Assist Tomogr. 2014;38(3):398–403.
Kalra MK, Maher MM, Toth TL, Hamberg LM, Blake MA, Shepard J-A, et al. Strategies for CT radiation dose optimization. Radiology. 2004;230(3):619–28.
McCollough CH, Primak AN, Braun N, Kofler J, Yu L, Christner J. Strategies for reducing radiation dose in CT. Radiol Clin N Am. 2009;47(1):27–40.
Hendee WR, Ritenour ER. Medical imaging physics. New York: Wiley; 2002.
Bushberg JT, Boone JM. The essential physics of medical imaging. Philadelphia: Lippincott Williams & Wilkins; 2011.
Li J, Udayasankar UK, Toth TL, Seamans J, Small WC, Kalra MK. Automatic patient centering for MDCT: effect on radiation dose. AJR. 2007;188(2):547–52.
Dance DR, Christofides S, Maidment ADA, McLean ID, Ng KH. Diagnostic radiology physics—a handbook for teachers and students. Vienna: IAEA; 2014.
Paulo G, Damilakis J, Tsapaki V, Schegerer A, Repussard J, Jaschke W, Frija G. Diagnostic reference levels based on clinical indications in computed tomography: a literature review. Insights Imaging. 2020;11:96. https://doi.org/10.1186/s13244-020-00899-y.
Public Health England. National Diagnostic Reference Levels (NDRLs). London: Public Health England; 2016.
UKHSA-RCE-1: doses from computed tomography (CT) exams in the UK: 2019 review. 2022.
World Health Organization. Ethics and medical radiological imaging. A policy brief for health-care providers. Geneva: World Health Organization; 2022. https://www.who.int/publications/i/item/9789240047785
World Health Organization. Ethics and governance of artificial intelligence for health. Geneva: World Health Organization; 2021. https://www.who.int/publications/i/item/9789240029200
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Trauernicht, C.J. (2023). Dose Optimisation in CT Colonography. In: Bortz, J.H., Ramlaul, A., Munro, L. (eds) CT Colonography for Radiographers. Springer, Cham. https://doi.org/10.1007/978-3-031-30866-6_6
Download citation
DOI: https://doi.org/10.1007/978-3-031-30866-6_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-30865-9
Online ISBN: 978-3-031-30866-6
eBook Packages: MedicineMedicine (R0)