
Abstract
Despite major advances in the management of ischemic heart disease, it remains a leading cause of morbidity and mortality worldwide. To overcome this epidemiological issue, among different treatment options, there has been interest in applying cellular therapy to reduce the acute injury secondary to acute myocardial infarction and to restore cardiac function in chronic ischemic heart disease. Preclinical cell-based therapy has proved to be effective and has yielded encouraging results, which involve preventing or reducing myocardial cell death, inhibiting scar formation, promoting angiogenesis, and improving cardiac function. However, clinical studies have not yet achieved a desired outcome, with several clinical trials showing paradoxical results in terms of cardiac function and remodeling. With this chapter, we aimed to present current preclinical and clinical evidence with stem cells use in the treatment of acute and chronic ischemic heart disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
With more than 17 million deaths worldwide each year, IHD caused by coronary artery disease is the most common cause of death and a major cause of hospital admission in developed countries. In Europe, IHD is the main cause of death among women >50 years of age and men [1, 2].
Conventional therapies have significantly reduced mortality of acute IHD, leaving an increasing number of patients with chronic IHD and/or HF without further treatment options. An increasing morbidity rate of this nature in an aging population is a huge burden for current society. HF is an expensive disease, both in terms of financial burden ($30 billion/year in medical expenditures in the US) and reduced quality of life and workdays lost [3]. Although HF survival has improved since 1979, the death rate remains very high, with more people dying of cardiac disease than cancer and chronic lower respiratory disease combined. Therapies aimed at restoring the billions of cardiomyocytes lost during myocardial infarction or damaged by nonischemic cardiomyopathies are sorely needed.
Among different medical strategies developed in the last decades to relieve symptoms, prevent disease progression, and improve survival and quality of life, stem cells therapy has emerged as a promising therapeutic approach to promote myocardial repair and regeneration. Cardiovascular disease is perhaps the field with the most clinical research on cell-based therapeutics, with over 200 clinical trials since 2001 examining multiple stem cell products for a diverse array of cardiac syndromes. Despite this extensive body of research, stem cell therapy has yet to transition from research to practice, as there is no definitive evidence of an efficacious cell product.
With this chapter, we aim to overview the biology of stem cell types used in cardiovascular research, and current preclinical and clinical applications regarding stem cells use in acute and chronic IHD.
2 Stem Cells Source
Stem cells are undifferentiated cells defined by their capacity for both self-renewal and ability to differentiate into other mature cell types. While embryonic stem cells are the prototypical pluripotent stem cells, capable of becoming any other cell type in an embryo, there are numerous stem cells populations found in adult tissues. These adult stem cells have a more limited differentiation potential and generally exist to maintain tissue homeostasis and replenish lost cells from that particular tissue. Some of these adult stem cells can naturally (albeit rarely) transdifferentiate to form cells outside of their original tissue of origin.
Several studies have shown that various cell types exerted beneficial effects on cardiac repair. Overall stem cells effect is summarized in Fig. 1.
-
Skeletal myoblast was the first cell type to be clinically tested, but the efficacy was unsatisfactory mainly due to the high incidence of arrhythmias [4].
-
Bone marrow-derived mononuclear cell contains the undifferentiated HSC and MSC as well as other committed cells in various stages of maturation. Its abundance and easy accessibility allow for autologous implantation without expansion in tissue culture, which avoids the decline of stem cell differentiation and migration ability, and reduces the incidence of immune rejection. Preclinical studies show discordant results in terms of angiogenesis and left ventricle function among different animal models [5,6,7,8,9,10]. Clinically, BMMNCs have been evaluated both for AMI and ischemic heart failure. In AMI, intracoronary delivery of autologous BMMNCs were evaluated in the REPAIR-AMI clinical trial: this was a large, phase III, double-blinded, placebo-controlled study designed to determine the therapeutic efficacy of BMMNCs. There were 204 patients randomized to receive either cells or placebo 3–7 days following AMI. Initial results at 4-months were encouraging, with LVEF significantly improved in the BMMNC-treated group by 5.5% on average, whereas the placebo-treated group exhibited a 3.0% in increase in LVEF. At 1-year, there were some encouraging signs. There were fewer myocardial infarctions, less need for repeat revascularization and fewer incidences of death in the BMMNC compared to the placebo group [11]. However, a longer follow-up analysis (5-year follow-up) found out that, despite a preserved benefit on mortality, improvement in LVEF was not maintained [12]. These mid-term results were also highlighted by other clinical experiences which did not find any significant improvement of myocardial function after BMMNCs administration in AMI (e.g., TIME trial [13], LateTIME trial [14], SWISS AMI trial [15], BOOST-2 trial [16], MiHeart/AMI trial [17]). In patients with post-ischemic HF, results have been more promising: in fact, a recent meta-analysis reports a mean improvement of 4.33% in LVEF as well as reductions in left ventricle volumes after MBBNCs injection in patients with post-ischemic HF [18]. This analysis suggested that overall BMMNCs for post-ischemic cardiomyopathy appear to produce positive effects on cardiac function and remodeling.
-
Hematopoietic stem cell has multiple differentiation potentials and can be autologously transplanted, but they are limited in abundance, which leads to poor efficacy [19].
-
Endothelial progenitor cells are isolated from peripheral blood and bone marrow and can give rise to vascular cells. Clinical application of EPC transplantation is expected to increase the capillary density and subsequently improve the microcirculation around the transplanted sites in infarcted heart. Studies have showed that EPC transplantation can also improve heart function, but its effect is restricted, which may result from its weak differentiation ability [20].
-
Embryonic stem cells have strong proliferation and differentiation capabilities, but it has ethical controversies and high risks of teratoma formation, which create hurdles to its clinical translation [21].
-
Induced pluripotent stem cells can differentiate into multiple cell types, are anti-inflammatory, and have therapeutic potential to repair tissues following ischemic disease. They have great proliferative capacity and might have the potential to be a major source for cardiac repair, but preclinical studies are needed to assess potential tumor formation and other safety issues [22, 23].
-
Cardiosphere-derived cells: The discovery of small clusters of heart cells expressing stem cell antigens (originally called “side population”—SP) capable of symmetric (self to identical self) or asymmetric (self to differentiated daughter progeny) division prompted the enthusiastic declaration that in situ, adult stem cells exist and such cells might have therapeutic potential. These in situ stem cells have been obtained by cardiac biopsies and then expanded in particular cultures to generate the CDCs (Fig. 2), which have clonogenic potential and express markers indicative of progenitor/stem cell identity [24]. To date, several trials have already tested this new population of cells. The CADUCEUS trial was the first to determine if intracoronary injection of autologous CDCs to patients soon after myocardial infarction was safe [25]. At 1 year of follow-up, CDC-treated patients had smaller scar sizes, increased viable myocardium, and improved regional function compared to control patients. A subsequent study using allogenic CDCs also confirmed the positive outcomes in terms of ventricular function improvement (even if no difference was found in terms of scar size) [26]. These results are hypothesized to be caused by the paracrine anti-inflammatory, immunomodulatory, and anti-fibrotic effect of these cells on the injured area rather than a CDC differentiation into local new myocardial cells [27].
-
Mesenchymal stem cells are isolates by multiple tissues (e.g., bone marrow, adipose tissue, dental pulp, umbilical cord) and can be expanded in vitro. Among the different cells studied for these purposes, MSCs are the most widely studied because of their abundancy, their easy retrieval and their immune exemption [28]. This type of cell is known since early 70s, and it has been called with different names (osteogenic stromal cell, stromal stem cell, mesenchymal stem cell, mesenchymal progenitor/precursor cell, multipotent mesenchymal stromal cell). It is now called MSC because of the hypothesis that postnatal MSC might generate all mesoderm-derived tissues (including myocardium). However, the formation of similar differentiated similar cells is still a point of controversy. The main and most studied source of MSCs for cardiac regeneration is bone marrow (Fig. 3 summarizes the process to obtain bone marrow MSCs); however, further studies have demonstrated favorable results in terms of LVEF improvement, perfusion, and remodeling for MSCs isolated from adipose tissue and umbilical cord in large-animal models [29, 30]. Particularly, adipose-derived MSCs can differentiate into cardiomyocytes, endothelial cells, and vascular smooth muscle cells and exhibit immunomodulatory properties that can protect other cell types (e.g., endothelial progenitor cells) from rejection.

Stem cells effect on cardiac remodeling and function

Laboratory pathway to obtain cardiosphere-derived cells

Isolation of bone marrow mesenchymal stem cells
3 MSCs Mechanisms of Action
MSCs favor cardiac repair by means of fibrosis reduction (Fig. 4), angiogenesis stimulation, and ventricular function improvement. The mechanism of action is heterogenous and includes engraftment and heterocellular coupling (stem and somatic cell intercommunication) [31] and paracrine mediated signaling [32]. Figure 5 summarizes all the mechanisms of action. The initial idea that MSCs differentiate and directly remuscularize a scarred myocardial area has been disconfirmed since multiple studies have shown that cardiomyocyte replacement by MSCs is low and does not represent a therapeutically meaningful mechanism of MSC action [33, 34]. Regarding paracrine signaling, MSCs release a variety of growth factors, with variability according to MSC tissue source. Besides, MSC secretion also includes exosomes and extracellular vesicles containing mRNA, miRNA and non-protein encoding RNA, peptides, and other bioactive compounds, which produce a wide variety of effects on target tissues (e.g., angiogenesis, reduction of infarct size, cardiac function preservation, and anti-arrhythmic effect) [35]. Further studies are required to determine the extent and duration of these effects. Heterocellular coupling through gap junctions allows for the transfer of small molecules and plays a role in coordinating activities between neighboring cells during tissue function. Mitochondrial transfer is also allowed through these gap junctions, and it is involved in rescuing damaged cells, reducing the ischemia-reperfusion injury [36].

Cardiac magnetic resonance showing mesenchymal stem cells effect on myocardial fibrosis on short-axis view (a) and long-axis 2-chamber view (b)

Mesenchymal stem cells mechanism of action
Regarding the immunomodulatory action, MSCs lack surface molecules which can activate the immune system. Furthermore, they reduce the expression of proinflammatory cytokines and lymphocytes proliferation.
4 MSCs Preliminary Clinical Outcomes: Acute Myocardial Infarction and Post-ischemic Heart Failure
Given the promising preclinical data on MSCs in IHD, multiple studies have investigated the clinical application of MSCs in humans. In AMI patients, autologous MSCs were first used. Two different trials demonstrated that intracoronary infusion of MSCs (before autologous bone marrow MSCs expansion and after percutaneous coronary intervention) showed better LVEF and ventricular volumes at mid-term follow-up [37, 38]. However, other studies did not find any superiority in the autologous MSCs group in terms of ventricular function improvement in patients with coronary artery disease [39]. This discrepancy might be due to different MSCs injection protocols used. Given the absence of MSCs immunogenicity and the disadvantages of using autologous cells, allogenic MSCs from healthy donors were tested. First clinical experiences show better results in terms of arrhythmias reduction [40], but trials are still ongoing.
Clinical experience with MSCs in ischemic HF has been obtained by means of several studies. Phase I [41] and Phase II studies [42, 43] using MSCs directly injected into the myocardium have demonstrated functional cardiac improvement, reverse remodeling, and improved exercise capacity and quality of life. Other studies have also analyzed MSCs effect after epicardial injection at the time of other surgical interventions (providing a unique opportunity to include cell-based therapies as an adjunct to open surgical procedures), showing an improvement in terms of scar size reduction, perfusion, and contractility [33]. When comparing autologous vs. allogenic MSCs in ischemic HF, both types showed a significant reduction in scar size at 1 year of follow-up as well as a ventricular reverse remodeling [34]. However discordant data are available regarding the dose-dependent effect.
5 Stem Cells Delivery: How and When to Do It
Delivery routes in cardiac cell therapy mainly include thoracotomy injection, system infusion, and imaging guide mini-invasive injection (Fig. 6).
-
1.
Thoracotomy injection: Through this access, cells can be delivered in a trans-epicardial intramyocardial fashion directly into the targeted area. Even if this method reduces the cells loss, unfortunately it requires anesthesia and a surgical approach. For this reason, this delivery might be limited to patients undergoing cardiac surgery (e.g., coronary artery bypass grafting). Potential complications are left ventricle perforation, bleeding from the myocardium and unbalanced ventricular motion caused by the uneven distribution of cells after injection.
-
2.
System infusion: It includes intracoronary and intravenous injection. Intracoronary has the advantage of increasing the number of cells homing to the ischemia area of the myocardium, while avoiding the damage caused by direct injection in the myocardium. This approach does not require chest opening and can be done at the time of PCI directly [44]. Complications can be cell loss through coronary circulation, and overdose of cell injection that can cause coronary artery occlusion. Intravenous injection is the easiest and the most economical way of infusing stem cells. Even if some researchers argued the real efficacy of this method (primarily due to pulmonary first-pass effect) [45], other studies combining intravenous and intracoronary injection demonstrated improved cardiac function, increased perfusion, and alleviated ventricular remodeling in preclinical ischemia settings [30].
-
3.
Imaging-guided mini-invasive injection: This strategy includes trans-endocardial intramyocardial and trans-epicardial intramyocardial injection. These injections are performed under echo or cardiac magnetic resonance guidance. Advantages are less trauma, fewer complications, and multiple transplantation at different time points [46].

Stem cells delivery
Regarding the optimal timing of cell therapy in AMI, there is evidence that myocardial microenvironment at different time points after infarction has profound influences on stem cells survival, homing, and differentiation [47]. In acute infarct stage, the microenvironment is not conducive to the survival and growth of stem cells because of the overwhelming inflammatory response in the myocardial injury area. It was found that inflammatory reaction peaks at 1–4 days, some cytokines (such as VEGF) which were favorable to stem cells migration reached the peak of secretion at 7 days, and scars began to form at about 14 days after AMI. A recent systematic review found that cardiac function parameters (e.g., diameters, volumes, and LVEF) were significantly improved when stem cells were transplanted between 7 and 10 days after infarction [14]. For chronic IHD, there is no obvious time window problem, so we can select the time when the patients are in good condition (such as no angina attack and general physical activity without discomfort, which denotes that the heart blood supply and heart function are still good), suggesting that the patients’ internal environment and myocardial microenvironment are relatively favorable for transplantation, so as to facilitate the survival, homing, and differentiation of implanted cells.
6 Future Perspectives
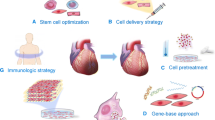
Current research is oriented toward different new strategies. First, a novel approach is trying to direct MSCs to a cardiopoietic phenotype (by means of a recombinant mix of growth factors, hormones and cytokines which favor the expression of pro-cardiogenic transcription factors). Preclinical and clinical studies are available and have already showed their efficacy and safety [48, 49], but still need to be evaluated in larger cohorts. Analogously, cell combination therapy with different types of stem cells might promote cardiac repair through synergistic interaction [50]. Additional strategies will include: MSC “secretome” including factors within exosomes; bioengineered cellular and acellular matrices and patches that can increase cell/factor retention; repeated injections of stem cells.
References
Timmis A, Townsend N, Gale CP, Torbica A, Lettino M, Petersen SE, et al.; European Society of Cardiology. European Society of Cardiology: cardiovascular disease statistics 2019. Eur Heart J. 2020;41(1):12–85. https://doi.org/10.1093/eurheartj/ehz859. Erratum in: Eur Heart J. 2020;41(47):4507. PMID: 31820000.
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al.; GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. https://doi.org/10.1016/j.jacc.2020.11.010. Erratum in: J Am Coll Cardiol. 2021;77(15):1958–9. PMID: 33309175; PMCID: PMC7755038.
Echouffo-Tcheugui JB, Bishu KG, Fonarow GC, Egede LE. Trends in health care expenditure among US adults with heart failure: the Medical Expenditure Panel Survey 2002–2011. Am Heart J. 2017;186:63–72. https://doi.org/10.1016/j.ahj.2017.01.003. Epub 2017 Jan 13. PMID: 28454834; PMCID: PMC5439297
Suzuki K, Smolenski RT, Jayakumar J, Murtuza B, Brand NJ, Yacoub MH. Heat shock treatment enhances graft cell survival in skeletal myoblast transplantation to the heart. Circulation. 2000;102(19 Suppl 3):III216–21. https://doi.org/10.1161/01.cir.102.suppl_3.iii-216. PMID: 11082390
Kobayashi T, Hamano K, Li TS, Katoh T, Kobayashi S, Matsuzaki M, et al. Enhancement of angiogenesis by the implantation of self bone marrow cells in a rat ischemic heart model. J Surg Res. 2000;89(2):189–95. https://doi.org/10.1006/jsre.2000.5828. PMID: 10729249
Kamihata H, Matsubara H, Nishiue T, Fujiyama S, Tsutsumi Y, Ozono R, et al. Implantation of bone marrow mononuclear cells into ischemic myocardium enhances collateral perfusion and regional function via side supply of angioblasts, angiogenic ligands, and cytokines. Circulation. 2001;104(9):1046–52. https://doi.org/10.1161/hc3501.093817. PMID: 11524400
Alestalo K, Korpi R, Mäkelä J, Lehtonen S, Mäkelä T, Yannopoulos F, et al. High number of transplanted stem cells improves myocardial recovery after AMI in a porcine model. Scand Cardiovasc J. 2015;49(2):82–94. https://doi.org/10.3109/14017431.2015.1018311. Epub 2015 Mar 18. PMID: 25705991
Fuchs S, Baffour R, Zhou YF, Shou M, Pierre A, Tio FO, et al. Transendocardial delivery of autologous bone marrow enhances collateral perfusion and regional function in pigs with chronic experimental myocardial ischemia. J Am Coll Cardiol. 2001;37(6):1726–32. https://doi.org/10.1016/s0735-1097(01)01200-1. PMID: 11345391
Waksman R, Fournadjiev J, Baffour R, Pakala R, Hellinga D, Leborgne L, et al. Transepicardial autologous bone marrow-derived mononuclear cell therapy in a porcine model of chronically infarcted myocardium. Cardiovasc Radiat Med. 2004;5(3):125–31. https://doi.org/10.1016/j.carrad.2004.10.001. PMID: 15721847
Mathieu M, Bartunek J, El Oumeiri B, Touihri K, Hadad I, Thoma P, et al. Cell therapy with autologous bone marrow mononuclear stem cells is associated with superior cardiac recovery compared with use of nonmodified mesenchymal stem cells in a canine model of chronic myocardial infarction. J Thorac Cardiovasc Surg. 2009;138(3):646–53. https://doi.org/10.1016/j.jtcvs.2008.12.031. Epub 2009 Feb 13. PMID: 19698851
Schächinger V, Erbs S, Elsässer A, Haberbosch W, Hambrecht R, Hölschermann H, et al.; REPAIR-AMI Investigators. Improved clinical outcome after intracoronary administration of bone-marrow-derived progenitor cells in acute myocardial infarction: final 1-year results of the REPAIR-AMI trial. Eur Heart J. 2006;27(23):2775–83. https://doi.org/10.1093/eurheartj/ehl388. Epub 2006 Nov 10. PMID: 17098754.
Assmus B, Leistner DM, Schächinger V, Erbs S, Elsässer A, Haberbosch W, et al.; REPAIR-AMI Study Group. Long-term clinical outcome after intracoronary application of bone marrow-derived mononuclear cells for acute myocardial infarction: migratory capacity of administered cells determines event-free survival. Eur Heart J. 2014;35(19):1275–83. https://doi.org/10.1093/eurheartj/ehu062. Epub 2014 Feb 25. PMID: 24569031.
Traverse JH, Henry TD, Pepine CJ, Willerson JT, Zhao DX, Ellis SG, et al.; Cardiovascular Cell Therapy Research Network (CCTRN). Effect of the use and timing of bone marrow mononuclear cell delivery on left ventricular function after acute myocardial infarction: the TIME randomized trial. JAMA. 2012;308(22):2380–9. https://doi.org/10.1001/jama.2012.28726. Erratum in: JAMA. 2013;309(4):343. Erratum in: JAMA. 2015;314(1):86. PMID: 23129008; PMCID: PMC3652242.
Traverse JH, Henry TD, Ellis SG, Pepine CJ, Willerson JT, Zhao DX, et al.; Cardiovascular Cell Therapy Research Network. Effect of intracoronary delivery of autologous bone marrow mononuclear cells 2 to 3 weeks following acute myocardial infarction on left ventricular function: the LateTIME randomized trial. JAMA. 2011;306(19):2110–9. https://doi.org/10.1001/jama.2011.1670. Epub 2011 Nov 14. PMID: 22084195; PMCID: PMC3600981.
Sürder D, Manka R, Moccetti T, Lo Cicero V, Emmert MY, Klersy C, et al. Effect of bone marrow-derived mononuclear cell treatment, early or late after acute myocardial infarction: twelve months CMR and long-term clinical results. Circ Res. 2016;119(3):481–90. https://doi.org/10.1161/CIRCRESAHA.116.308639. Epub 2016 Jun 6. PMID: 27267068
Wollert KC, Meyer GP, Müller-Ehmsen J, Tschöpe C, Bonarjee V, Larsen AI, et al. Intracoronary autologous bone marrow cell transfer after myocardial infarction: the BOOST-2 randomised placebo-controlled clinical trial. Eur Heart J. 2017;38(39):2936–43. https://doi.org/10.1093/eurheartj/ehx188. PMID: 28431003
Nicolau JC, Furtado RHM, Silva SA, Rochitte CE, Rassi A Jr, Moraes JBMC Jr, et al.; MiHeart/AMI Investigators. Stem-cell therapy in ST-segment elevation myocardial infarction with reduced ejection fraction: a multicenter, double-blind randomized trial. Clin Cardiol. 2018;41(3):392–9. https://doi.org/10.1002/clc.22882. Epub 2018 Mar 22. PMID: 29569254; PMCID: PMC6489870.
Xiao C, Zhou S, Liu Y, Hu H. Efficacy and safety of bone marrow cell transplantation for chronic ischemic heart disease: a meta-analysis. Med Sci Monit. 2014;20:1768–77. https://doi.org/10.12659/MSM.892047. PMID: 25270584; PMCID: PMC4199404
Garikapati K, Hassan S, Singhvi A, Dania K, Qureshi W. Outcomes of patients with left ventricular diastolic dysfunction in adult hematopoietic stem cell transplantation. Circ Cardiovasc Qual. 2013;6:A72.
Babin-Ebell J, Sievers HH, Charitos EI, Klein HM, Jung F, Hellberg AK, et al. Transmyocardial laser revascularization combined with intramyocardial endothelial progenitor cell transplantation in patients with intractable ischemic heart disease ineligible for conventional revascularization: preliminary results in a highly selected small patient cohort. Thorac Cardiovasc Surg. 2010;58(1):11–6. https://doi.org/10.1055/s-0029-1186199. Epub 2010 Jan 13. PMID: 20072970
Menasché P, Vanneaux V, Hagège A, Bel A, Cholley B, Cacciapuoti I, et al. Human embryonic stem cell-derived cardiac progenitors for severe heart failure treatment: first clinical case report. Eur Heart J. 2015;36(30):2011–7. https://doi.org/10.1093/eurheartj/ehv189. Epub 2015 May 19. PMID: 25990469
Lian Q, Zhang Y, Zhang J, Zhang HK, Wu X, Zhang Y, et al. Functional mesenchymal stem cells derived from human induced pluripotent stem cells attenuate limb ischemia in mice. Circulation. 2010;121(9):1113–23. https://doi.org/10.1161/CIRCULATIONAHA.109.898312. Epub 2010 Feb 22. PMID: 20176987
Jung Y, Bauer G, Nolta JA. Concise review: induced pluripotent stem cell-derived mesenchymal stem cells: progress toward safe clinical products. Stem Cells. 2012;30(1):42–7. https://doi.org/10.1002/stem.727. PMID: 21898694; PMCID: PMC3784250
Messina E, De Angelis L, Frati G, Morrone S, Chimenti S, Fiordaliso F, et al. Isolation and expansion of adult cardiac stem cells from human and murine heart. Circ Res. 2004;95(9):911–21. https://doi.org/10.1161/01.RES.0000147315.71699.51. Epub 2004 Oct 7. PMID: 15472116
Malliaras K, Makkar RR, Smith RR, et al. Intracoronary cardiosphere-derived cells after myocardial infarction: evidence of therapeutic regeneration in the final 1-year results of the CADUCEUS trial (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction). J Am Coll Cardiol. 2014;63:110–22.
Chakravarty T, Makkar RR, Ascheim DD, et al. ALLogeneic heart STem cells to achieve myocardial regeneration (ALLSTAR) trial: rationale and design. Cell Transplant. 2017;26:205–14.
Smith RR, Barile L, Cho HC, Leppo MK, Hare JM, Messina E, et al. Regenerative potential of cardiosphere-derived cells expanded from percutaneous endomyocardial biopsy specimens. Circulation. 2007;115(7):896–908. https://doi.org/10.1161/CIRCULATIONAHA.106.655209. Epub 2007 Feb 5. PMID: 17283259
Shabbir A, Zisa D, Suzuki G, Lee T. Heart failure therapy mediated by the trophic activities of bone marrow mesenchymal stem cells: a noninvasive therapeutic regimen. Am J Physiol Heart Circ Physiol. 2009;296(6):H1888–97. https://doi.org/10.1152/ajpheart.00186.2009. Epub 2009 Apr 24. PMID: 19395555; PMCID: PMC2716100
Vilahur G, Oñate B, Cubedo J, Béjar MT, Arderiu G, Peña E, et al. Allogenic adipose-derived stem cell therapy overcomes ischemia-induced microvessel rarefaction in the myocardium: systems biology study. Stem Cell Res Ther. 2017;8(1):52. https://doi.org/10.1186/s13287-017-0509-2. PMID: 28279225; PMCID: PMC5345145
Liu CB, Huang H, Sun P, Ma SZ, Liu AH, Xue J, et al. Human umbilical cord-derived mesenchymal stromal cells improve left ventricular function, perfusion, and remodeling in a porcine model of chronic myocardial ischemia. Stem Cells Transl Med. 2016;5(8):1004–13. https://doi.org/10.5966/sctm.2015-0298. Epub 2016 Jun 22. PMID: 27334487; PMCID: PMC4954453
Mayourian J, Cashman TJ, Ceholski DK, Johnson BV, Sachs D, Kaji DA, et al. Experimental and computational insight into human mesenchymal stem cell paracrine signaling and heterocellular coupling effects on cardiac contractility and arrhythmogenicity. Circ Res. 2017;121(4):411–23. https://doi.org/10.1161/CIRCRESAHA.117.310796. Epub 2017 Jun 22. PMID: 28642329; PMCID: PMC5899516
Hodgkinson CP, Bareja A, Gomez JA, Dzau VJ. Emerging concepts in paracrine mechanisms in regenerative cardiovascular medicine and biology. Circ Res. 2016;118(1):95–107. https://doi.org/10.1161/CIRCRESAHA.115.305373. PMID: 26837742; PMCID: PMC4874329
Karantalis V, DiFede DL, Gerstenblith G, Pham S, Symes J, Zambrano JP, et al. Autologous mesenchymal stem cells produce concordant improvements in regional function, tissue perfusion, and fibrotic burden when administered to patients undergoing coronary artery bypass grafting: the Prospective Randomized Study of Mesenchymal Stem Cell Therapy in Patients Undergoing Cardiac Surgery (PROMETHEUS) trial. Circ Res. 2014;114(8):1302–10. https://doi.org/10.1161/CIRCRESAHA.114.303180. Epub 2014 Feb 24. PMID: 24565698; PMCID: PMC4104798
Hare JM, Fishman JE, Gerstenblith G, DiFede Velazquez DL, Zambrano JP, et al. Comparison of allogeneic vs autologous bone marrow–derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: the POSEIDON randomized trial. JAMA. 2012;308(22):2369–79. https://doi.org/10.1001/jama.2012.25321. Erratum in: JAMA. 2013;310(7):750. George, Richard [added]; Lardo, Albert [added]. PMID: 23117550; PMCID: PMC4762261
Bian S, Zhang L, Duan L, Wang X, Min Y, Yu H. Extracellular vesicles derived from human bone marrow mesenchymal stem cells promote angiogenesis in a rat myocardial infarction model. J Mol Med (Berl). 2014;92(4):387–97. https://doi.org/10.1007/s00109-013-1110-5. Epub 2013 Dec 14. PMID: 24337504
Liu K, Ji K, Guo L, Wu W, Lu H, Shan P, et al. Mesenchymal stem cells rescue injured endothelial cells in an in vitro ischemia-reperfusion model via tunneling nanotube like structure-mediated mitochondrial transfer. Microvasc Res. 2014;92:10–8. https://doi.org/10.1016/j.mvr.2014.01.008. Epub 2014 Jan 31. PMID: 24486322
Chen SL, Fang WW, Ye F, Liu YH, Qian J, Shan SJ, et al. Effect on left ventricular function of intracoronary transplantation of autologous bone marrow mesenchymal stem cell in patients with acute myocardial infarction. Am J Cardiol. 2004;94(1):92–5. https://doi.org/10.1016/j.amjcard.2004.03.034. PMID: 15219514
Lee JW, Lee SH, Youn YJ, Ahn MS, Kim JY, Yoo BS, et al. A randomized, open-label, multicenter trial for the safety and efficacy of adult mesenchymal stem cells after acute myocardial infarction. J Korean Med Sci. 2014;29(1):23–31. https://doi.org/10.3346/jkms.2014.29.1.23. Epub 2013 Dec 26. PMID: 24431901; PMCID: PMC3890472
Cogle CR, Wise E, Meacham AM, Zierold C, Traverse JH, Henry TD, et al.; Cardiovascular Cell Therapy Research Network (CCTRN). Detailed analysis of bone marrow from patients with ischemic heart disease and left ventricular dysfunction: BM CD34, CD11b, and clonogenic capacity as biomarkers for clinical outcomes. Circ Res. 2014;115(10):867–74. https://doi.org/10.1161/CIRCRESAHA.115.304353. Epub 2014 Aug 18. PMID: 25136078; PMCID: PMC4358751.
Hare JM, Traverse JH, Henry TD, Dib N, Strumpf RK, Schulman SP, et al. A randomized, double-blind, placebo-controlled, dose-escalation study of intravenous adult human mesenchymal stem cells (prochymal) after acute myocardial infarction. J Am Coll Cardiol. 2009;54(24):2277–86. https://doi.org/10.1016/j.jacc.2009.06.055. PMID: 19958962; PMCID: PMC3580848
Williams AR, Trachtenberg B, Velazquez DL, McNiece I, Altman P, Rouy D, et al. Intramyocardial stem cell injection in patients with ischemic cardiomyopathy: functional recovery and reverse remodeling. Circ Res. 2011;108(7):792–6. https://doi.org/10.1161/CIRCRESAHA.111.242610. Epub 2011 Mar 17. PMID: 21415390; PMCID: PMC3390160
Mathiasen AB, Qayyum AA, Jørgensen E, Helqvist S, Fischer-Nielsen A, Kofoed KF, et al. Bone marrow-derived mesenchymal stromal cell treatment in patients with severe ischaemic heart failure: a randomized placebo-controlled trial (MSC-HF trial). Eur Heart J. 2015;36(27):1744–53. https://doi.org/10.1093/eurheartj/ehv136. Epub 2015 Apr 29. PMID: 25926562
Guijarro D, Lebrin M, Lairez O, Bourin P, Piriou N, Pozzo J, et al. Intramyocardial transplantation of mesenchymal stromal cells for chronic myocardial ischemia and impaired left ventricular function: results of the MESAMI 1 pilot trial. Int J Cardiol. 2016;209:258–65. https://doi.org/10.1016/j.ijcard.2016.02.016. Epub 2016 Feb 2. PMID: 26901787
Diederichsen AC, Møller JE, Thayssen P, Junker AB, Videbaek L, Saekmose SG, et al. Effect of repeated intracoronary injection of bone marrow cells in patients with ischaemic heart failure the Danish stem cell study—congestive heart failure trial (DanCell-CHF). Eur J Heart Fail. 2008;10(7):661–7. https://doi.org/10.1016/j.ejheart.2008.05.010. Epub 2008 Jun 16. PMID: 18555742
Lin L, Gu S, Cheng Y, Ding L. Distribution of adult cardiac stem cells via intravenous cell transplantation in myocardial infarction mouse model. Prog Modern Biomed. 2015;15:7024–7. https://doi.org/10.13241/j.cnki.pmb.2015.36.007.
Freyman T, Polin G, Osman H, Crary J, Lu M, Cheng L, et al. A quantitative, randomized study evaluating three methods of mesenchymal stem cell delivery following myocardial infarction. Eur Heart J. 2006;27(9):1114–22. https://doi.org/10.1093/eurheartj/ehi818. Epub 2006 Mar 1. PMID: 16510464
Khodayari S, Khodayari H, Amiri AZ, Eslami M, Farhud D, Hescheler J, et al. Inflammatory microenvironment of acute myocardial infarction prevents regeneration of heart with stem cells therapy. Cell Physiol Biochem. 2019;53(5):887–909. https://doi.org/10.33594/000000180. PMID: 31749350
Behfar A, Yamada S, Crespo-Diaz R, Nesbitt JJ, Rowe LA, Perez-Terzic C, et al. Guided cardiopoiesis enhances therapeutic benefit of bone marrow human mesenchymal stem cells in chronic myocardial infarction. J Am Coll Cardiol. 2010;56(9):721–34. https://doi.org/10.1016/j.jacc.2010.03.066. PMID: 20723802; PMCID: PMC2932958
Bartunek J, Behfar A, Dolatabadi D, Vanderheyden M, Ostojic M, Dens J, et al. Cardiopoietic stem cell therapy in heart failure: the C-CURE (Cardiopoietic stem Cell therapy in heart failURE) multicenter randomized trial with lineage-specified biologics. J Am Coll Cardiol. 2013;61(23):2329–38. https://doi.org/10.1016/j.jacc.2013.02.071. Epub 2013 Apr 10. Erratum in: J Am Coll Cardiol. 2013 Dec 24;62(25):2457-8. PMID: 23583246
Bolli R, Hare JM, March KL, Pepine CJ, Willerson JT, Perin EC, et al.; Cardiovascular Cell Therapy Research Network (CCTRN). Rationale and design of the CONCERT-HF Trial (Combination of Mesenchymal and c-kit+ Cardiac Stem Cells As Regenerative Therapy for Heart Failure). Circ Res 2018;122(12):1703–15. https://doi.org/10.1161/CIRCRESAHA.118.312978. Epub 2018 Apr 27. PMID: 29703749; PMCID: PMC5993622.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Pradegan, N., Gerosa, G. (2023). Stem Cells Therapy for Ischemic Heart Disease. In: Concistrè, G. (eds) Ischemic Heart Disease. Springer, Cham. https://doi.org/10.1007/978-3-031-25879-4_34
Download citation
DOI: https://doi.org/10.1007/978-3-031-25879-4_34
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-25878-7
Online ISBN: 978-3-031-25879-4
eBook Packages: MedicineMedicine (R0)