
Abstract
Since the year 2000, eight major disease outbreaks, including COVID-19 involving zoonosis of viruses, have occurred. Increasing population density, high mobility and economic activity make cities hotspots for the spread of infectious diseases. COVID-19 has exposed the vulnerability of nations regardless of the development index. This paper reviews and analyses the literature on the effect of population density on the morbidity and mortality of COVID-19 since the outbreak of COVID-19. Literature reveals that 7 months into COVID-19, 95% of the infections came from urban centres around the world (Mizutori and Sharif, OPINION: COVID-19 demonstrates urgent need for cities to prepare for pandemics. UN-Habitat. https://news.trust.org/item/20200615120207-y321f, 2020). This could be because of a skewed economic model in which 55% of the world’s population resides in cities which occupy 1–3% of the landmass while concentrating 85% of the world’s economic activity. Cities are a constant magnet for huge numbers of people, making the chances of spreading disease relatively high. Current studies reveal a significant correlation between population density and the number of infections. The paper recommends a health reform plan centred on decongesting cities and a systematic reorganisation of settlement patterns, recognising efficient social distancing to limit illicit human-wildlife interactions. This should ensure less vulnerability to disease pathogens while guaranteeing environmental, food security, and good health for all.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The COVID-19 pandemic has to date infected about 562 million people (17 July 2022) (John Hopkins University, 2022) and killed nearly 15 million (World Health Organization, 2022). Scientists admit to the unprecedented nature of the spread of COVID-19 (Jefferson et al., 2020). Within a few months of the outbreak, questions were already being asked about the role population density has on the spread of the pandemic (Carozzi et al., 2020). Seven months into the pandemic, it was also observed that 95% of cases emanated from the urban centres (Mizutori & Sharif, 2020). Notably, 55% of the world’s population now resides in cities which occupy up to 3% of the entire land mass (Lucertini & Musco, 2020). As such cities which concentrate 85% of economic activity have become global hotspots of all kinds of pollution including pandemic diseases (Landrigan et al., 2017).
Population density is one of the major variables which determine the duration of impact of a pandemic (Reyes et al., 2013). Density has historically always been contentious when referencing the spread of infectious airborne diseases because of the dichotomy of thought among scholars. Modelling studies published early into the pandemic suggested how population density affects the basic reproduction number, Ro, through the number of contacts in crowded areas (Joacim Rocklöv & Sjödin, 2021). This is reflected in the raft of protocols of social distancing measures which have been implemented globally to reduce human contact since the outbreak (Yin et al., 2021).
At least 4.5 billion of the world’s population were put on lockdown by decrees from various governments acting in concert (Cresswell et al., 2020; Sheikh et al., 2020). A study of 49 countries has shown that lockdowns effectively reduce the spread of the COVID-19 (Atalan, 2020). A physical separating distance of at least 1 meter is associated with lower transmission of SARS-CoV-2 with better protection accorded when the distance is increased (Chu et al., 2020).
However, being able to social distance is also a function of population density (Wong & Li, 2020). The built environment is known to promote crowding (Sharifi & Khavarian-Garmsir, 2020) which leads to more contacts between persons and hence the spreading of infectious diseases. The debate on the role of cities spreading of COVID-19 as they attract large numbers of residents has meant that some have questioned the sustainability of the sanitation particularly so, the dense model for development. Both sides have weighed in on the ‘compact versus sprawl’ debates (Sahasranaman & Jensen, 2021). This paper uses an integrative and semi-systematic literature review approach with the aim of analysing the current correlation between COVID-19 infections and mortality as a function of population density.
2 Literature Review
2.1 Cities and Outbreaks of Pandemics in the Twenty-First Century
The rate at which disease outbreaks are happening has been alarming in the past few years, while crowded cities have acted as chambers for global spread. In the twenty-first century alone, the world has experienced at least eight major disease outbreaks beginning with SARS of 2002 (Cherry & Krogstad, 2004; LeDu & Barry, 2004). Coronavirus are known to undergo a zoonotic spill over into secondary hosts such as civet cats for SARS-CoV-1 (Parashar & Anderson, 2004; Widagdo et al., 2017), dromedary camels for MERS (Sharif-Yakan & Kanj, 2014), (Ji, 2020) and pangolins for SARS-CoV-2 (Liao et al., 2020) (T. Zhang et al., 2020). A 22.8% incidence of MERS-CoV in camels is regarded as an occupational hazard (Ji, 2020). Figure 9.1 shows some of the outbreaks which have happened with increasing frequency and severity during the past 20 years. Table 9.1 also provides more detail on the epidemiology of these infectious diseases of the past 20 years.

The trajectory, frequency and prevalence of major disease outbreaks since 2000. (Source: Authors)
Concomitantly with the outbreak of polio (Akil & Ahmad, 2016; Okiror et al., 2021), Ebola Virus Disease (EVD) spread globally from West Africa with a case fatality rate of more than 40% (Cenciarelli et al., 2015; Gatherer, 2014). The African bats have been implicated as primary hosts in the spread of Ebola (Letko et al., 2020). Before the emergency of COVID-19 in December 2019, the world had been grappling with containing another Ebola epidemic which started in West Africa (see Fig. 9.1) and spread to a host of countries in the West (Kalenga et al., 2019; Rugarabamu et al., 2020). Most of the diseases have had their epicentres in urban areas.
Despite the outbreaks occurring in distant countries, the spread of these diseases to become global epidemics and pandemics has been facilitated by global connectivity and population density associated with some jurisdictions especially the mega cities of the world.
2.2 COVID-19 and the City Connection
Many cities with large population densities have particularly borne the brunt of COVID-19 and there is a tacit realisation of the need to reconfigure the way the city is designed (Sharifi & Khavarian-Garmsir, 2020). Authors such as Hazarie et al. (2021) have posited the existence of a strong interaction between mobility and population density and spread of infectious diseases. An indictment of the city has always been that in extraordinary circumstances such as pandemics, there is the so-called (urban) death penalty associated with urban development (Martínez & Short, 2021).
While the conclusion of population density as driver of infection may be considered intuitive (Federgruen & Naha, 2021), empirical studies have demonstrated that under forced circumstances, population densities are ‘quite pathogenic’ (Levy & Herzog, 1974). A countrywide study conducted in the USA concluded that counties with larger population densities produced greater reproductive numbers (Ro) hence greater rates of transmission of COVID-19 and as such larger infection cases. Evidence from other studies in the USA reached similar conclusions suggesting a 0.14 increase of Ro with every unit log increase in population density. There are further arguments by the researchers that the value of Ro was not mediated by transportation (Sy et al., 2021) which contradicts the observations in New York (Hamidi et al., 2020; Hamidi & Hamidi, 2021). The evidence of density as a persistent predictor of COVID-19 severity and death appears overwhelming from most of the studies conducted in the USA (Desmet & Wacziarg, 2021)
A study conducted in Brazil revealed that initially smaller cities were impacted more by COVID-19 infections. However, this trend called an urban advantage is reversed in the long term with major cities showing that a 1% increase in the susceptible population being associated with 0.14% increase in infections (Ribeiro et al., 2020). With some of the largest population densities, the difficulty to contain the virus has been compromised by the prevalence of slum urban development with as many as 205,415 people /km2 in Bangladesh (Islam & Kibria, 2020). Further studies of environmental factors in Bangladesh also reveal a positive correlation between the number of cases and the population density (Alam, 2021). Research done in Malaysia showed that districts with greater population densities were more affected by the COVID-19 pandemic (Ganasegeran et al., 2021). In India where large population densities are realised through very close contact between individuals in public spaces also gave positive correlations between population density and infections (Bhadra et al., 2021). Concerns were expressed at the beginning of the pandemic for cities such as Manila which are known to have very high densities as much as 71,263 persons/km2 (Salva et al., 2021). Moderate positive correlations have been observed in some Indian cities contrary to the information released by John Hopkins University (Bhadra et al., 2021).
Researchers investigating the effect of household size among other parameters have observed a positive correlation between the size of the household and the rate of infection (Federgruen & Naha, 2021). While one Italian study showed that COVID-19 exhibited more severity in households with single occupancies for people aged more than 80 years (53.1% of the 25 million Italian families in Italy are composed of less than two people) (Liotta et al., 2020), other research done in Italy showed a positive correlation between population density as a function of the number of infections and deaths further indicating how the proximity of household exacerbates the spread of COVID-19 (Ilardi et al., 2021). An IZA Institute of Labour Economics report often quoted in the debate on population density versus COVID-19 spread categorically finds no evidence that greater population density is linked with more COVID-19 cases and deaths (Carozzi et al., 2020). This demonstrates the divergent views and positions among scholars, and as such the need for further investigation into population density as risk factor of COVID-19.
On the other hand, a largely rural community (Diop et al., 2020) and a younger population in Africa (Chitungo et al., 2020) are some of the reasons proffered for the lesser number of infections and mortalities in Africa compared to West. The United Nations has thus far realised and deplored the roles cities have played in the spread of the COVID-19 pandemic especially as they have been heavily impacted on by the outbreak (UN-Habitat, 2021). There is also a realisation of the need for reconfiguration of the settlement patterns especially in urban centres to a model which provides social and economic equity (Sharifi & Khavarian-Garmsir, 2020).
3 Methodology
In this paper, we mostly surveyed literature which has been published since the outbreak of COVID-19 and how the spread of the disease has been influenced by population density. A combination of integrative and semi-systematic literature review approach (Snyder, 2019) is used to search for literature and provide an overhead review and qualitative analysis of information available regarding the influence of population density versus COVID-19 infections and fatalities. A continuous search of literature was done on databases such as PubMed, Google Scholar using search criteria using words such as ‘COVID-19 and population density’. Other literature relating to similar infectious diseases such as, SARS, H1N1, Ebola, polio and ZIKA was also consulted. A number of ‘cause and effect’ or correlation models used by various authors globally were identified. Fifteen studies which provide various models showing the correlation between population densities against the total number of infections and in some cases the number of fatalities due to COVID-19 were selected within the last 2 years of published data. A compilation was done of the model used, the place or cities studied, the correlation coefficients obtained and the time limits within which the study was considered and conducted. Table 9.2 shows the different models which have been used to arrive at the correlation between population density and the number of infections and fatalities around the world.
4 Results
Researchers have used various tests of goodness of fit and statistical significance to assess the validity of the claims of population density as a function of morbidity and mortality. These models range from the simple standard linear regression, and the Quantile regression which is an extension of linear regression method. Others have applied multiple linear regression and cluster analysis to derive Pearson coefficients to measure levels of correlation or association. The other models captured in Table 9.2 are spatial regression models, spatial lag models, the Susceptible-Infected-Recovered-Deceased (SIRD) epidemiological model, the Ordinary Least Squares (OLS), and Negative Binomial Regression (NBR) models, Extreme Bounds Analysis (EBA), Variable Addition Tests (VAT), nonparametric Spearman’s correlation and negative binomial regression (NBR). Each of these models have been used to calculate the corresponding correlation coefficient or another size effect parameter such as extreme values coefficients (β) to measure the effectiveness of population density in influencing the COVID-19 epidemiology. Other methods used including econometric methodologies such as random-effects models and Hausman–Taylor models (Kaicker et al., 2020) and the Generalised Linear Model (GLM) combined with the Geographically Weighted Regression (GWR). It is not the scope of this paper to exhaust all the models which have been utilised but highlight how several tools have been utilised to measure the size effect of population density on COVID-19 severity. The heterogeneity of the models makes it difficult for comparisons to be made between the various models. However, what is clear is that from most (about 80%) of the models which have been sampled for this paper, a statistically significant correlation has been established between population density and with the number of infections.
What is also clear is that a number of researchers have predicted that population density including other parameters such as the total country population, the age of the population and family sizes living within the same households correlate strongly with the quick diffusion of COVID-19 within countries (Sigler et al., 2021). In Malaysia, the strongest correlation was observed in the central region of the country, being greater in urbanised districts and cities (Ganasegeran et al., 2021). A study in the Gauteng region of South Africa assessed that the ‘ward’ areas which have more than average risk to COVID-19 and more than average population density were in the so-called townships with denser settlements patterns (Maree & Ballard, 2020).
In studying the disparate jurisdictions, researchers chose a variety of approaches which include the investigation of many countries grouped together such as the 172 country study by Moosa and Khatatbeh (2021) or the 84 country quantile regression analysis by Sigler et al. (2021). An analysis of data from 140 countries undertaken by Murányi et al. (2021) between 18 April and 4 July 2020 quantitatively reveals very high infection rates as a function of population density after ranking the 140 countries into four categories according to infection rates of very high, high, medium, and low (Murányi et al., 2021).
Comparative and quantitative studies have also been undertaken at country level across the world with a view to recommending the best possible options for in-country containment of COVID-19. In most cases of the literature surveyed, the data reveals a higher severity of the pandemic associated with high population densities. For instance, while studies undertaken in India by Bhadra et al. (2021) reveal a moderate correlation between population density and the number of infections and mortalities (r = 0.58 for infections; r = 0.64 for mortality) for the four major states in India, the authors are careful to mention that the worst effects of the pandemic have been experienced in the megacities of the four states (Bhadra et al., 2021). These studies in India have been corroborated by other researchers who have reached similar conclusions on the spread of COVID-19 in that country (Sengupta et al., 2021; Tamrakar et al., 2021). In the three states of Maharashtra, Jharkhand and Meghalaya, a large association between urban population density as a function of daily and cumulative severity ratios was established (Kaicker et al., 2020).
Multiple linear regression analysis on 2814 US counties done by Zhang and Schwartz (2020) characterises metropolitan cities in the USA as hotspots for COVID-19, although counterintuitively some smaller cities and counties have been similarly affected. This has been attributed to a more aged population found in some of smaller cities. In the US eastern states, a positive association between population density and transmission or fatalities between the 1 March and 16 November 2020 was observed. In this study, New York City leads in the figures (Lee et al., 2021).
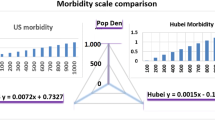
A comparison of 18 cities in the Hubei province of China and 50 states and counties in US arrived at an r = 0.55 for the Chinese cities compared to r = 0.62 for the US when applying simple regression analysis. The assessment and conclusion from this study is that of a positive association between population density and morbidity (Yin et al., 2021). However, the level of analysis seems not as robust to include other parameters such as connectivity, crowdedness, household sizes which could have influenced the spread of the disease. Spatial regression models have predicted correlations as high as 84% for infections in the United States (Wong & Li, 2020). However, Hamidi and Hamidi (2021) have projected contrary results for New York regardless of the large population densities experienced in the city. A globalised world with increased mobility and connectivity between points of interests (POI) has been used to explain the apparent heterogeneity of the associations between density and vulnerability to COVID-19 especially in more developed countries such as the USA (Hazarie et al., 2021). For cities in South Korea which have similar development indices as the United States, connectivity has a greater impact in the spread of COVID-19 (Jo et al., 2021). This is understandable as travelling has the effect of bringing people into more contact with each other and hence increasing the probability of infection to a susceptible population. Despite the mathematical rigor associated with this conclusion, in our opinion this does not override the intuitive effect of population density on the spread of communicable diseases.
A study conducted in Oman using GLM combined with the GWR yielded an adjusted R2 = 78.77% between COVID-19 infection and the population density variable. Other parameters such as the number of households, and spatial interactions have also been used as proxies for population density giving greater effect to the impact of population as a measure of close interaction between individuals during a pandemic leading to infection (Al Kindi et al., 2021).
For the 265,000 cases reported by the end of the August 2020 in Turkey, 60% of these were recorded in Istanbul the capital city with a very strong correlation (r = 0.97) between population density and number of infections (Baser, 2021). Interestingly within a similar timeframe, 60% of infections were also recorded in Dhaka the capital of Bangladesh which has a population density of about 46,997 persons/km2 (compare New York = 34,338.5 persons/km2 (Lee et al., 2021)). In this study, the largest correlation was detected between the population density and number of infections (Sharif & Dey, 2021). Alam also finds a strong positive correlation between population density and infection accounting for 60% countrywide variability in Bangladesh, and similar a strong correlation between COVID-19 and prevalence of urban centres (Alam, 2021). Similarly a Z-score analysis performed for the regions of the Philippines yielded the second highest correlation for population density against COVID-19 infections (0.93) and deaths (0.92) after the number of ICU beds at the regional level (Talabis et al., 2021).
The situation in South Korea, however, offers an interesting middle of the ground position in which both population density and connectivity (both leading to crowdedness) have been observed to be positively correlated to the number of infections in the country. However, there is a greater emphasis on the effect of connectivity rather than density as predictor of the number of infections (Jo et al., 2021).
5 Discussion
There is a clear existential crisis of novel infections and pandemics happening with increasing rapidity and severity. Coupled with the benefits of globalisation these airborne infections are spreading around the world once they have been triggered from a single location. Research has revealed that infectious diseases such as measles and COVID-19 spread more quickly in densely populations areas (Tarwater & Martin, 2001).
The cases of the cruise ships have been investigated over long periods of times as the environments within these confined spaces offer unintended but conducive conditions for disease causation and spread and study (Carling et al., 2009; Kak, 2007). The Diamond Princess cruise ship provided valuable opportunity and information for epidemiologists to analyse the dynamics of COVID-19 (Russell et al., 2020) revealing basic reproduction numbers which were four times higher on the crowded ship than was found in Wuhan (J. Rocklöv et al., 2020). While some studies in countries such as Italy seem to suggests that social connectedness is negatively correlated with spread of COVID-19 (Liotta et al., 2020), high population densities have been observed to catalyse the spread of COVID-19 (Joacim Rocklöv & Sjödin, 2020). A study conducted in China suggests that population density is not a factor in the spread of COVID-19 under strict lockdown conditions (Sun et al., 2020), but observations from Brazilian cities have confirmed a positive correlation between population density with number of cases (Pequeno et al., 2020). Among other reasons, the high population densities in the cities Sao Paolo and Rio de Janeiro are blamed for the higher number of infections of COVID-19 compared to other states in Brazil (Baqui et al., 2020). The increase of infections with population density has been corroborated by other studies within Brazil controlling for metrological factors such as rain, radiation, humidity and radiation (Pequeno et al., 2020). Apparently the number of infections are reduced by lockdowns conditions where there is a greater number of symptomatic cases as observed in an Indian analysis of the spread of the pandemic in its states (Sardar et al., 2020). Observations carried out in US cities from 14 March through 19 March 2020 have also realised that the worse attack rate of COVID-19 is to be expected in cities with larger population sizes (Stier et al., 2020). Regardless of social distance, measures such as lockdowns are more effective where the population density is low among other parameters (Verhagen et al., 2020). In the UK, hospital capacities have been found to be highest along the Cardiff coast, a place with higher levels of population density in the UK (Verhagen et al., 2020).
Unsanitary conditions emanating from over-crowdedness which induce breeding conditions for pathogens (Amoo et al., 2020) and a high concentration of germs in confined places such as experienced in the Cook County jail in Chicago are examples of how adversely the spread of any infectious disease can be exacerbated by lack of social distance (Reinhart & Chen, 2020). Rural Africa is characterised as sparsely populated, and along with a young population, with fewer comorbidities; this seems to have contributed to a far a smaller number of infections (Oleribe et al., 2021; Wamai et al., 2021) (Diop et al., 2020).
Hamidi et al. have recommended denser urban development as the basis for inducing lower death rates in case of infectious outbreak of disease (Hamidi et al., 2020). This is counter-intuitive to the principles of epidemiology of airborne infections. Unless this is accompanied by the concomitant and commensurate health facilities and adequate infrastructure, a denser model of development becomes a very dangerous proposition especially for countries in the global south. This is because the larger populations residing in the countryside with a better natural phenomenon of social distancing through sparse populations may be encouraged into city dwelling.
Arguments which dismiss the role of population density in large cities appear to have forgotten the importance of this geographical and demographic factor in the spread of infectious diseases (Nathan, 2021). The positions taken by researchers as to whether infectious pandemics spread as function of compactness (dense) or sprawling urban appear to be driven by vested interests amongst scholars of urban planning, with each camp favouring its own theories ahead of intuition and objectivity. Conclusions arrived for compact development in relation to COVID-19 are derived from a persuasion which argues that there is significant reduction in trips to POIs such as grocery stores, pharmacies and transit points during lockdown periods (Hamidi & Zandiatashbar, 2021). As such this would curtail the spread of disease. The data is used to definitively recommend the continued adoption of compact model of development in the face of ever-increasing infections airborne infections (Hamidi et al., 2020). Based on the findings in New York, the question remains to be answered as to whether the significant effect of POIs in the greater proportion of the spread of infections can be positively correlated with bigger population sizes within smaller geographical spaces and hence with an effective population density.
The disparity between the United States, which has a comparatively lower population size and densities, compared to China and yet the US has recorded the largest infections and mortalities to date points to other socio-economic factors between the two countries other than demographic parameters. A greater prevalence of co-morbidities in North America and a larger proportion of an older population has been used to explain the higher cases and fatalities in North America and other western countries (Badawi & Vasileva, 2021). On the other hand, China has implemented a rapid response ‘zero COVID’ policy which is not very popular in the western nations for its seeming harsh stringency (Mallapaty, 2022) and possible violation of individual rights of citizens (Watkins, 2020). However, the Chinese policy has been viewed as success model despite the misgivings (AlTakarli, 2020).
Population size and population density which lead to crowdedness are positively correlated to COVID-19 morbidity and mortality. The effects of these are exacerbated by the ‘benefits’ of globalisation such as better connectivity which unfortunately guarantees the importation of viral infections and their variants from one distant place to another. However, the detrimental effects of higher population densities can be mediated by better health facilities, infrastructure and rapid response governance policies which ensure better chances of survival for a populace. Considering the inequitable distribution of land and the attendant rapid spread of COVID-19 in the urban centres, this paper proposes a calculated and unemotive policy of decongestion of cities as part of a first principles approach to the health reform agenda.
6 Conclusion
This paper sought to establish the role of population density on the spread and severity of COVID-19 by surveying the literature which has been published for the last 2 years. Disparate models have been used by researchers around the world to arrive at several conclusions ranging from positive association to high correlations. In most cases, population density has a significant effect on the proliferation of COVID-19. Two main scenarios emerge as follows: (1) High population densities found in conjunction with inadequate health (and connectivity) infrastructure means population density is found to be significantly positively correlated with more infections and may be deaths. This has been the experience in less developed countries such as Bangladesh, India and the Philippines. This represents the classic scenario in which population density is generally expected to influence the spread of infectious diseases; (2) On the other hand, developed countries with larger metropolitan and better connectivity facilities establishments appear to reverse the effect of population density on the spread of infectious disease. The effect of population density seems to be transferred to crowdedness as encouraged by mobility. As such this becomes a proxy for population density. A typical example is that of North Korea which revealed a similar phenomenon to New York where great neural networks are associated with higher infections and mortality. This situation could be mediated by better medical facilities which help in reducing the impact of COVID-19. However, even the best medical facilities can be overwhelmed as has already been experienced during COVID-19.
References
Akil, L., & Ahmad, H. A. (2016). The recent outbreaks and reemergence of poliovirus in war and conflict-affected areas. International Journal of Infectious Diseases, 49, 40–46. https://doi.org/10.1016/j.ijid.2016.05.025
Al Kindi, K. M., Al-Mawali, A., Akharusi, A., Alshukaili, D., Alnasiri, N., Al-Awadhi, T., Charabi, Y., & El Kenawy, A. M. (2021). Demographic and socioeconomic determinants of COVID-19 across oman-a geospatial modelling approach. Geospatial Health, 16(1), 145–160. https://doi.org/10.4081/gh.2021.985
Alam, M. Z. (2021). Is population density a risk factor for communicable diseases like COVID-19? A case of Bangladesh. Asia-Pacific Journal of Public Health, 33(8), 949–950. https://doi.org/10.1177/1010539521998858
AlTakarli, N. S. (2020). China’s response to the COVID-19 outbreak: A model for epidemic preparedness and management. Dubai Medical Journal, 3(2), 44–49. https://doi.org/10.1159/000508448
Alyami, M. H., Alyami, H. S., & Warraich, A. (2020). Middle East respiratory syndrome (MERS) and novel coronavirus disease-2019 (COVID-19): From causes to preventions in Saudi Arabia. Saudi Pharmaceutical Journal, 28(11), 1481–1491. https://doi.org/10.1016/j.jsps.2020.09.014
Amoo, E. O., Adekeye, O., Olawole-Isaac, A., Fasina, F., Adekola, P. O., Samuel, G. W., Akanbi, M. A., Oladosun, M., & Azuh, D. E. (2020). Nigeria and Italy divergences in coronavirus experience: Impact of population density. Scientific World Journal, 2020, 1. https://doi.org/10.1155/2020/8923036
Atalan, A. (2020). Is the lockdown important to prevent the COVID-9 pandemic? Effects on psychology, environment and economy-perspective. Annals of Medicine and Surgery, 56(June), 38–42. https://doi.org/10.1016/j.amsu.2020.06.010
Badawi, A., & Vasileva, D. (2021). Comparative profile for COVID-19 cases from China and North America: Clinical symptoms, comorbidities and disease biomarkers. World Journal of Clinical Cases, 9(1), 118–132. https://doi.org/10.12998/wjcc.v9.i1.118
Baqui, P., Bica, I., Marra, V., Ercole, A., & van der Schaar, M. (2020). Ethnic and regional variations in hospital mortality from COVID-19 in Brazil: A cross-sectional observational study. The Lancet Global Health, 8(8), e1018–e1026. https://doi.org/10.1016/S2214-109X(20)30285-0
Barbiero, V. K. (2020). Ebola: A hyperinflated emergency. Global Health Science and Practice, 8(2), 178–182. https://doi.org/10.9745/GHSP-D-19-00422
Baser, O. (2021). Population density index and its use for distribution of Covid-19: A case study using Turkish data. Health Policy, 125(January), 148–154.
Bhadra, A., Mukherjee, A., & Sarkar, K. (2021). Impact of population density on Covid-19 infected and mortality rate in India. Modeling Earth Systems and Environment, 7(1), 623–629. https://doi.org/10.1007/s40808-020-00984-7
Carling, P. C., Bruno-Murtha, L. A., & Griffiths, J. K. (2009). Cruise ship environmental hygiene and the risk of norovirus infection outbreaks: An objective assessment of 56 vessels over 3 years. Clinical Infectious Diseases, 49(9), 1312–1317. https://doi.org/10.1086/606058
Carozzi, F., Roth, S., & Provenzano, S. (2020). DISCUSSION PAPER SERIES urban density and COVID-19 (Vol. Issue 13440).
Cenciarelli, O., Pietropaoli, S., Malizia, A., Carestia, M., D’Amico, F., Sassolini, A., Di Giovanni, D., Rea, S., Gabbarini, V., Tamburrini, A., Palombi, L., Bellecci, C., & Gaudio, P. (2015). Ebola virus disease 2013-2014 outbreak in West Africa: An analysis of the epidemic spread and response. International Journal of Microbiology, 2015(Figure 1). https://doi.org/10.1155/2015/769121
Chan-Yeung, M., Xu, R., Sinha, M., Pande, B., Sinha, R., Zhou, Y., Macgeorge, E. L., Myrick, J. G., Morin, C. M., Carrier, J., Bastien, C., Godbout, R., Choi, E. P. H., Hui, B. P. H., Wan, E. Y. F., O’Connor, R. C., Wetherall, K., Cleare, S., McClelland, H., et al. (2003). SARS: epidemiology. Respirology, 8, S9–S14.
Cherry, J. D., & Krogstad, P. (2004). SARS: The first pandemic of the 21st century. Pediatric Research, 56(1), 1–5. https://doi.org/10.1203/01.PDR.0000129184.87042.FC
Chitungo, I., Dzobo, M., Hlongwa, M., & Dzinamarira, T. (2020). COVID-19: Unpacking the low number of cases in Africa. Public Health in Practice, 1(January), 100038. https://doi.org/10.1016/j.puhip.2020.100038
Chu, D. K., Akl, E. A., Duda, S., Solo, K., Yaacoub, S., Schünemann, H. J., El-harakeh, A., Bognanni, A., Lotfi, T., Loeb, M., Hajizadeh, A., Bak, A., Izcovich, A., Cuello-Garcia, C. A., Chen, C., Harris, D. J., Borowiack, E., Chamseddine, F., Schünemann, F., et al. (2020). Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. The Lancet, 395(10242), 1973–1987. https://doi.org/10.1016/S0140-6736(20)31142-9
Cresswell, K., Dhami, S., & Sheikh, A. (2020). National COVID-19 lockdown exit strategies need to pay more attention to community engagement and workplace safety, 10(2), 2–5. https://doi.org/10.7189/jogh.10.020323
Desmet, K., & Wacziarg, R. (2021). Understanding spatial variation in COVID-19 across the United States. Journal of Urban Economics, 127. https://doi.org/10.1016/j.jue.2021.103332
Diop, B. Z., Ngom, M., Pougué Biyong, C., & Pougué Biyong, J. N. (2020). The relatively young and rural population may limit the spread and severity of COVID-19 in Africa: A modelling study. BMJ Globalization and Health, 5(5). https://doi.org/10.1136/bmjgh-2020-002699
Federgruen, A., & Naha, S. (2021). Crowding effects dominate demographic attributes in COVID-19 cases. International Journal of Infectious Diseases, 102, 509–516. https://doi.org/10.1016/j.ijid.2020.10.063
Ganasegeran, K., Jamil, M. F. A., Ch’ng, A. S. H., Looi, I., & Peariasamy, K. M. (2021). Influence of population density for covid-19 spread in Malaysia: An ecological study. International Journal of Environmental Research and Public Health, 18(18). https://doi.org/10.3390/ijerph18189866
Gatherer, D. (2014). The 2014 Ebola virus disease outbreak in West Africa. Journal of General Virology, 95(PART 8), 1619–1624. https://doi.org/10.1099/vir.0.067199-0
Hagan, J. E., Wassilak, S. G. F., Craig, A. S., Tangermann, R. H., Diop, O. M., & Burns, C. C. (2015). Progress Toward Polio Eradication — Worldwide , 2014–2015. In Center for Disease Control and Prevention (Vol. 64, Issue 19). https://reliefweb.int/sites/reliefweb.int/files/resources/mm6419.15-19.pdf
Hamidi, S., & Hamidi, I. (2021). Subway ridership, crowding, or population density: Determinants of COVID-19 infection rates in New York City. American Journal of Preventive Medicine, 60(5), 614–620. https://doi.org/10.1016/j.amepre.2020.11.016
Hamidi, S., & Zandiatashbar, A. (2021). Compact development and adherence to stay-at-home order during the COVID-19 pandemic: A longitudinal investigation in the United States. Landscape and Urban Planning, 205(January), 103952. https://doi.org/10.1016/j.landurbplan.2020.103952
Hamidi, S., Sabouri, S., & Ewing, R. (2020). Does density aggravate the COVID-19 pandemic?: Early findings and lessons for planners. Journal of the American Planning Association, 86(4), 495–509. https://doi.org/10.1080/01944363.2020.1777891
Hazarie, S., Soriano-Paños, D., Arenas, A., Gómez-Gardeñes, J., & Ghoshal, G. (2021). Interplay between population density and mobility in determining the spread of epidemics in cities. Communications on Physics, 4(1), 1–10. https://doi.org/10.1038/s42005-021-00679-0
Ilardi, A., Chieffi, S., Iavarone, A., & Ilardi, C. R. (2021). SARS-CoV-2 in Italy: Population density correlates with morbidity and mortality. Japanese Journal of Infectious Diseases, 74, 61.
Islam, T., & Kibria, M. G. (2020). Correspondence: Challenges to the prevention of COVID-19 spread in slums of Bangladesh. Journal of Public Health, 42(3), 637–638. https://doi.org/10.1093/pubmed/fdaa088
Jefferson, T., Plüddemann, A., Spencer, E., Roberts, N., & Heneghan, C. (2020). Analysis of the evidence of transmission dynamics of COVID-19 protocol for a scoping evidence review. Centre for Evidence Based Medicine. https://www.cebm.net/wp-content/uploads/2020/07/Protocol-Analysis-of-Transmission-Dynamics-of-COVID-2.pdf.
Ji, J. S. (2020). Origins of MERS-CoV, and lessons for 2019-nCoV. The Lancet Planetary Health, 4(3), e93. https://doi.org/10.1016/S2542-5196(20)30032-2
Jo, Y., Hong, A., & Sung, H. (2021). Density or connectivity: What are the main causes of the spatial proliferation of covid-19 in Korea? International Journal of Environmental Research and Public Health, 18(10). https://doi.org/10.3390/ijerph18105084
John Hopkins University. (2022). Global Cases, Global Death. John Hopkins University. https://coronavirus.jhu.edu/map.html
Kaicker, N., Imai, K. S., & Gaiha, R. (2020). Global development severity of the Covid-19 pandemic in India. In The case of three states: Maharashtra, Jharkhand and Meghalaya.
Kak, V. (2007). Infections in confined spaces: Cruise Ships, Military Barracks, and College Dormitories. Infectious Disease Clinics of North America, 21(3), 773–784. https://doi.org/10.1016/j.idc.2007.06.004
Kalenga, O. I., Moeti, M., Sparrow, A., Lucey, D., & Ghebreyesus, T. A. (2019). Spe ci a l R e p or t the ongoing Ebola epidemic in the Democratic Republic of Congo, 2018–2019. The New England Journal of Medicine, 381(4), 373–383.
Lam, W. K., Zhong, N. S., & Tan, W. C. (2003). Overview on SARS in Asia and the World. Respirology, 8(July), 29–32. https://doi.org/10.1046/j.1440-1843.2003.00516.x
Landrigan, P. J., Fuller, R., Acosta, N. J. R., Adeyi, O., Arnold, R., Basu, N. (Nil), Baldé, A. B., Bertollini, R., Bose-O’Reilly, S., Boufford, J. I., Breysse, P. N., Chiles, T., Mahidol, C., Coll-Seck, A. M., Cropper, M. L., Fobil, J., Fuster, V., Greenstone, M., Haines, A., et al. (2017). The lancet commission on pollution and health. The Lancet, 6736(17), 462. https://doi.org/10.1016/S0140-6736(17)32345-0
LeDu, J. W., & Barry, M. A. (2004). SARS, the first pandemic of the 21st century. Emerging Infectious Diseases, 10(11), e26. https://doi.org/10.3201/eid1011.040797_02
Lee, W., Kim, H., Michelle, H., Heo, S., Fong, K. C., Yang, J., Park, C., Kim, H., & Bell, M. L. (2021). Urban environments and COVID-19 in three Eastern states of the United States. Science of the Total Environment, 779(146334).
Letko, M., Seifert, S. N., Olival, K. J., Plowright, R. K., & Munster, V. J. (2020). Bat-borne virus diversity, spillover and emergence. Nature Reviews Microbiology, 18(8), 461–471. https://doi.org/10.1038/s41579-020-0394-z
Levy, L., & Herzog, A. N. (1974). Effects of population density and crowding on health and social adaptation in the Netherlands. Journal of Health and Social Behavior, 15(3), 228–240.
Liao, Y., Wei, W., Cheung, W. Y., Li, W., Li, L., Leung, G. M., Holmes, E. C., Hu, Y., & Guan, Y. (2020). Identifying SARS-CoV-2 related coronaviruses in Malayan pangolins. Nature, 1–19.
Liotta, G., Marazzi, M. C., Orlando, S., & Palombi, L. (2020). Is social connectedness a risk factor for the spreading of COVID-19 among older adults? The Italian paradox. PLoS ONE, 15(5), 1–7. https://doi.org/10.1371/journal.pone.0233329
Lucertini, G., & Musco, F. (2020). Circular urban metabolism framework. One Earth, 2(2), 138–142. https://doi.org/10.1016/j.oneear.2020.02.004
Mallapaty, S. (2022). China’s zero-COVID strategy: What happens next? Nature. https://www.nature.com/articles/d41586-022-00191-7, 602, 15.
Maree, R. G., & Ballard, R. (2020). Relating COVID-19 risk indices to population density in Gauteng (issue April).
Martínez, L., & Short, J. R. (2021). The pandemic city: Urban issues in the time of covid-19. Sustainability (Switzerland), 13(6), 1–10. https://doi.org/10.3390/su13063295
Martins-Filho, P. R. (2021). Relationship between population density and COVID-19 incidence and mortality estimates: A county-level analysis. Journal of Infection and Public Health, 14(8), 1087–1088. https://doi.org/10.1016/j.jiph.2021.06.018
Mizutori, M., & Sharif, M. M. (2020). OPINION: COVID-19 demonstrates urgent need for cities to prepare for pandemics. UN-Habitat. https://news.trust.org/item/20200615120207-y321f
Monamele, C. G., Njifon, H. L. M., Vernet, M. A., Njankouo, M. R., Kenmoe, S., Yahaya, A. A., Deweerdt, L., Nono, R., Mbacham, W., Anong, D. N., Akoachere, J. F., & Njouom, R. (2019). Molecular characterization of influenza A(H1N1)pdm09 in Cameroon during the 2014-2016 influenza seasons. PLoS One, 14(1), 1–11. https://doi.org/10.1371/journal.pone.0210119
Moosa, I. A., & Khatatbeh, I. N. (2021). The density paradox: Are densely-populated regions more vulnerable to Covid-19? International Journal of Health Planning and Management, 36(5), 1575–1588. https://doi.org/10.1002/hpm.3189
Murányi, A., Varga, B., & Ward, P. R. (2021). Relationship between the COVID-19 pandemic and ecological. Economic, and Social Conditions, 9(July), 1–10. https://doi.org/10.3389/fpubh.2021.694191
Nathan, M. (2021). The city and the virus. Urban Studies, November 2020, 004209802110583. https://doi.org/10.1177/00420980211058383.
Nishiura, H., Klinkenberg, D., Roberts, M., & Heesterbeek, J. A. P. (2009). Early epidemiological assessment of the virulence of emerging infectious diseases: A case study of an influenza pandemic. PLoS One, 4(8), e6852. https://doi.org/10.1371/journal.pone.0006852
Okiror, S., Mulugeta, A., Onuekwusi, I., Braka, F., Malengemi, S., Burton, J., Hydarav, R., Toure, B., Davis, B., Gathenji, C., Nwogu, C., & Okeibunor, J. (2021). Polio outbreak investigation and response in the horn of Africa: 2013-2016. Journal of Immunological Sciences, Special(2), 14–21. https://doi.org/10.29245/2578-3009/2021/s2.1104
Oleribe, O. O., Suliman, A. A. A., Taylor-Robinson, S. D., & Corrah, T. (2021). Possible reasons why sub-saharan africa experienced a less severe COVID-19 pandemic in 2020. Journal of Multidisciplinary Healthcare, 14(July), 3267–3271. https://doi.org/10.2147/JMDH.S331847
Parashar, U. D., & Anderson, L. J. (2004). Severe acute respiratory syndrome: Review and lessons of the 2003 outbreak. International Journal of Epidemiology, 33(4), 628–634. https://doi.org/10.1093/ije/dyh198
Pequeno, P., Mendel, B., Rosa, C., Bosholn, M., Souza, J. L., Baccaro, F., Barbosa, R., & Magnusson, W. (2020). Air transportation, population density and temperature predict the spread of COVID-19 in Brazil. PeerJ, 8, e9322. https://doi.org/10.7717/peerj.9322
Reinhart, E., & Chen, D. L. (2020). Incarceration and its disseminations: COVID-19 pandemic lessons from Chicago’s Cook County Jail. Health Affairs (Project Hope), 39(8), 1412–1418. https://doi.org/10.1377/hlthaff.2020.00652
Reyes, R., Ahn, R., Thurber, K., & Burke, T. F. (2013). Urbanization and infectious diseases: General principles. Historical Perspectives, and Contemporary Challenges, 123–146. https://doi.org/10.1007/978-1-4614-4496-1
Ribeiro, H. V., Sunahara, A. S., Sutton, J., Perc, M., & Hanley, Q. S. (2020). City size and the spreading of COVID-19 in Brazil. PLoS ONE, 15(9 September 2020), 1–12. https://doi.org/10.1371/journal.pone.0239699
Rocklöv, J., & Sjödin, H. (2020). High population densities catalyse the spread of COVID-19. Journal of Travel Medicine, 27(3), 1–2. https://doi.org/10.1093/jtm/taaa038
Rocklöv, J., & Sjödin, H. (2021). High population densities catalyse the spread of COVID-19. Journal of Travel Medicine, 27(3), 1–2. https://doi.org/10.1093/JTM/TAAA038
Rocklöv, J., Sjödin, H., & Wilder-Smith, A. (2020). COVID-19 outbreak on the diamond princess cruise ship: Estimating the epidemic potential and effectiveness of public health countermeasures. Journal of Travel Medicine, 27(3), 1–7. https://doi.org/10.1093/jtm/taaa030
Rugarabamu, S., Mboera, L., Rweyemamu, M., Mwanyika, G., Lutwama, J., Paweska, J., & Misinzo, G. (2020). Two years of responding to Ebola Saharan Africa: Virus outbreaks in sub- – a review, 5, 1–10. https://doi.org/10.1136/bmjgh-2019-001955
Russell, T. W., Hellewell, J., Jarvis, C. I., Van Zandvoort, K., Abbott, S., Ratnayake, R., Flasche, S., Eggo, R. M., Edmunds, W. J., & Kucharski, A. J. (2020). Estimating the infection and case fatality ratio for coronavirus disease (COVID-19) using age-adjusted data from the outbreak on the Diamond Princess cruise ship, February 2020. Eurosurveillance, 25(12), 6–10. https://doi.org/10.2807/1560-7917.ES.2020.25.12.2000256
Sahasranaman, A., & Jensen, H. J. (2021). Spread of COVID-19 in urban neighbourhoods and slums of the developing world: Spread of COVID-19 in urban neighbourhoods and slums of the developing world. Journal of the Royal Society Interface, 18(174), 20200599. https://doi.org/10.1098/rsif.2020.0599
Salva, E. P., Villarama, J. B., Lopez, E. B., Sayo, A. R., Villanueva, A. M. G., Edwards, T., Han, S. M., Suzuki, S., Seposo, X., Ariyoshi, K., & Smith, C. (2021). Correction to: Epidemiological and clinical characteristics of patients with suspected COVID-19 admitted in Metro Manila, Philippines (Tropical Medicine and Health, (2020), 48, 1, (51), 10.1186/s41182-020-00241-8). Tropical Medicine and Health, 49(1), 85. https://doi.org/10.1186/s41182-021-00373-5
Sardar, T., Nadim, S. S., Rana, S., & Chattopadhyay, J. (2020). Assessment of lockdown effect in some states and overall India: A predictive mathematical study on COVID-19 outbreak. Chaos, Solitons and Fractals, 139, 110078. https://doi.org/10.1016/j.chaos.2020.110078
Sengupta, P., Ganguli, B., SenRoy, S., & Chatterjee, A. (2021). An analysis of COVID-19 clusters in India. BMC Public Health, 631, 1–21.
Sharif, N., & Dey, S. K. (2021). Impact of population density and weather on COVID-19 pandemic and SARS-CoV-2 mutation frequency in Bangladesh. Epidemiology and Infection., 149, e16. https://doi.org/10.1017/S0950268821000029
Sharifi, A., & Khavarian-Garmsir, A. R. (2020). The COVID-19 pandemic: Impacts on cities and major lessons for urban planning, design, and management. Science of the Total Environment, 749, 1–3. https://doi.org/10.1016/j.scitotenv.2020.142391
Sharif-Yakan, A., & Kanj, S. S. (2014). Emergence of MERS-CoV in the Middle East: Origins, transmission, treatment, and perspectives. PLoS Pathogens, 10(12), 10–13. https://doi.org/10.1371/journal.ppat.1004457
Sheikh, A., Sheikh, A., Sheikh, Z., Dhami, S., & Sridhar, D. (2020). What’s the way out? Potential exit strategies from the COVID-19 lockdown. Journal of Global Health, 10(1), 1–5. https://doi.org/10.7189/JOGH.10.010370
Sigler, T., Mahmuda, S., Kimpton, A., Loginova, J., Wohland, P., Charles-Edwards, E., & Corcoran, J. (2021). The socio-spatial determinants of COVID-19 diffusion: The impact of globalisation, settlement characteristics and population. Globalization and Health, 17(1), 1–14. https://doi.org/10.1186/s12992-021-00707-2
Snyder, H. (2019). Literature review as a research methodology: An overview and guidelines. Journal of Business Research, 104(August), 333–339. https://doi.org/10.1016/j.jbusres.2019.07.039
Stier, A. J., Berman, M. G., & Bettencourt, L. M. A. (2020). COVID-19 attack rate increases with city size. https://doi.org/10.1101/2020.03.22.20041004
Sun, Z., Zhang, H., Yang, Y., Wan, H., & Wang, Y. (2020). Impacts of geographic factors and population density on the COVID-19 spreading under the lockdown policies of China. Science of the Total Environment, 746(666), 141347. https://doi.org/10.1016/j.scitotenv.2020.141347
Sy, K. T. L., White, L. F., & Nichols, B. E. (2021). Population density and basic reproductive number of COVID-19 across United States counties. PLoS One, 16(4 April), 1–11. https://doi.org/10.1371/journal.pone.0249271
Talabis, D. A. S., Babierra, A. L., Buhat, C. A. H., Lutero, D. S., Iii, K. M. Q., & Rabajante, J. F. (2021). Local government responses for COVID-19 management in the Philippines. BMC Public Health, 21(1711), 1–15.
Tamrakar, V., Srivastava, A., Saikia, N., Parmar, M. C., Shukla, S. K., Shabnam, S., Boro, B., Saha, A., & Debbarma, B. (2021). District level correlates of COVID-19 pandemic in India during March-October 2020. PLoS One, 16(9 Septembe), 1–17. https://doi.org/10.1371/journal.pone.0257533
Tarwater, P. M., & Martin, C. F. (2001). Effects of population density on the spread of disease. Complexity, 6(6), 29–36. https://doi.org/10.1002/cplx.10003
UN-Habitat. (2021). Cities and pandemics : Towards a more just, green and healthy future. https://unhabitat.org/sites/default/files/2021/03/cities_and_pandemics-towards_a_more_just_green_and_healthy_future_un-habitat_2021.pdf
Verhagen, M. D., Brazel, D. M., Dowd, J. B., Kashnitsky, I., Kashnitsky, I., & Mills, M. C. (2020). Forecasting spatial, socioeconomic and demographic variation in COVID-19 health care demand in England and Wales. BMC Medicine, 18(1), 1–11. https://doi.org/10.1186/s12916-020-01646-2
Wamai, R. G., Hirsch, J. L., Van Damme, W., Alnwick, D., Bailey, R. C., Hodgins, S., Alam, U., & Anyona, M. (2021). What could explain the lower covid-19 burden in africa despite considerable circulation of the sars-cov-2 virus? International Journal of Environmental Research and Public Health, 18(16). https://doi.org/10.3390/ijerph18168638
Watkins, J. (2020). Preventing a covid-19 pandemic We need to think beyond containment, 810(February), 1–2. https://doi.org/10.1136/bmj.m810
Widagdo, W., Okba, N. M. A., Stalin Raj, V., & Haagmans, B. L. (2017). MERS-coronavirus: From discovery to intervention. One Health, 3, 11–16. https://doi.org/10.1016/j.onehlt.2016.12.001
Wong, D. W. S., & Li, Y. (2020). Spreading of COVID-19: Density matters. PLoS One, 15(12 December), 1–16. https://doi.org/10.1371/journal.pone.0242398
World Health Organization. (2022). World health statistics 2022. https://cdn.who.int/media/docs/default-source/gho-documents/world-health-statistic-reports/worldhealthstatistics_2022.pdf?sfvrsn=6fbb4d17_3
Yin, H., Sun, T., Yao, L., Jiao, Y., Ma, L., Lin, L., Graff, J. C., Aleya, L., Postlethwaite, A., Gu, W., & Chen, H. (2021). Association between population density and infection rate suggests the importance of social distancing and travel restriction in reducing the COVID-19 pandemic. Environmental Science and Pollution Research, 28(30), 40424–40430. https://doi.org/10.1007/s11356-021-12364-4
Zhang, C. H., & Schwartz, G. G. (2020). Spatial disparities in coronavirus incidence and mortality in the United States: An ecological analysis as of May 2020. Journal of Rural Health, 36(3), 433–445. https://doi.org/10.1111/jrh.12476
Zhang, T., Wu, Q., & Zhang, Z. (2020). Probable pangolin origin of SARS-CoV-2 associated with the COVID-19 outbreak. Current Biology, 30(7), 1346–1351.e2. https://doi.org/10.1016/j.cub.2020.03.022
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Nyambiya, I., Sawunyama , L. (2023). Decongesting Global Cities as Part of Health Reform in the Era of COVID-19: Impacts and Implications for Zimbabwe. In: Chapungu, L., Chikodzi, D., Dube, K. (eds) The COVID-19 - Health Systems Nexus. Global Perspectives on Health Geography. Springer, Cham. https://doi.org/10.1007/978-3-031-21602-2_9
Download citation
DOI: https://doi.org/10.1007/978-3-031-21602-2_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-21601-5
Online ISBN: 978-3-031-21602-2
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)