
Abstract
Ultrasound is a mainstay in the diagnostic imaging of the musculoskeletal system in newborns and infants. This chapter focuses on diagnosing hip disorders, particularly developmental dysplasia of the hip in newborns and infants. This is a well-known and familiar challenge for neonatologists as well as paediatricians and paediatric radiologists or paediatric orthopaedics. The chapter gives a brief overview of different approaches and methods of how to assess the neonatal hip—also discussing the different techniques described in the European and the Anglo-American literature. All the respective scanning techniques and findings are described and illustrated in this chapter, with a focus on the Graf method. Additionally, some of the most important disorders of the hip joint in infancy and early childhood are reviewed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


15.1 Introduction and General Remark
Since the first report of “the diagnosis of congenital hip joint dislocation by ultrasound compound treatment” in 1980 by the Austrian orthopaedic surgeon Reinhard Graf, various methods on how to perform hip ultrasound (US) are described. They differ in their systematic approach.
Ultrasound has become the study of choice for evaluating paediatric musculoskeletal disorders and is today well established. It is superior to radiography in neonates and young infants because it can demonstrate the cartilaginous and soft tissue components of the hip joint in addition to the bony structures, which in this age is of tremendous importance.
The methods used for hip US around the world are described and the respective findings are illustrated. Additionally, other applications of US in paediatric hip conditions such as assessing hip effusion are discussed.
The two main queries for performing US of the hip need different examination techniques:
-
1.
In neonates and infants, the goal is to assess developmental dysplasia of the hip (DDH). In this scenario, US is indicated either based on
-
(a)
A clinical suspicion such as typical hip instability, clicks, foetal malposition, impaired mobility, neurological impairment, etc.
-
(b)
Or as a general screening, particularly in regions or countries with high incidence or endemic DDH.
-
(c)
Finally, in some countries and instances a selective screening is preferred, where the indication for a hip US examination is based on risk factors such as familial risk, breach presentation, endemic dysplasia, infants with risk factors, preterm infants, and so forth.
-
(a)
-
2.
The aims of assessment throughout childhood are evaluation for hip joint effusion, capsular thickening, inflammation, or other pathology such as epiphysiolysis and Perthes disease.
15.1.1 Technical Requisites
High-resolution linear array transducers are recommended with a wide frequency range, from as high as 24 MHz, more commonly 18/15 MHz to 5 MHz (potentially “trapezoid/convex mode”—phased linear mode) depending on the age, the size of the infant, and the available equipment.
15.1.2 Other Requisites
Documentation facilities are essential, special positioning devices are helpful in some techniques—particularly the Graf method. Take care to provide a proper environment, swaddling facilities, diapers, and pacifiers. Sometimes charts and material helping to explain findings to parents may be useful.
Furthermore, knowledge and education of the investigator are essential—not only concerning the US technique but also its implications on management with respect to the consequences of over-diagnosis/treatment or, even worse, missing a significant finding.
15.1.3 What About Imaging Techniques Other than US?
For hip queries in neonates, rarely other imaging techniques such as radiographs of the hip, leg, or pelvis are indicated; however, one may find hip pathology in abdominal, pelvis, or leg radiographs performed for other indications (Fig. 15.1a, b). Nevertheless, in older infants and children, a radiograph is sometimes part of the diagnostic work up and irreplaceable.

Incidental findings in the neonatal hip on radiographs. (a) A neonatal pelvic radiograph taken for other reasons shows a split pelvis, sacrococcygeal hypoplasia (in caudal regression syndrome) and incidentally a hip dislocation on the left side. Superimposed is the umbilical clamp. (b) A leg radiograph shows bilateral stippled calcifications in the hip and knee epiphysis in a neonate with chondrodysplasia punctata—although this might be picked on US, the radiograph displays the findings much more convincingly
CT is practically never indicated in neonatal hip queries (except for acute trauma mostly in older infants), and in neonates MRI for hip queries also is a rarity. Only in older infants, MRI may become indicted, e.g. for assessing Perthes disease or a septic hip. Additionally, in these situations (also for tumour queries) and in older infants or children, a scintigraphic study may be an imaging option. These modalities and findings, however, will not be discussed in detail here—it is addressed in Chap. 14.
15.2 Developmental Dysplasia of the Hip (DDH)
Early diagnosis and treatment of DDH are important and irreplaceable for a normal development of the hip joint. The main goal is to prevent and avoid long-term sequelae. Advances in US technology allow for better visualisation and differentiation of osseous and especially non-osseous structures. This led to better understanding of the basics of the pathophysiology for what is now termed “developmental dysplasia of the hip”.
Usually, DDH is a result of a combination of both structural and ligamentous laxity leading to an abnormal incongruent hip. Structural causes are related to primary dysplasia. It has been suggested that only 2% of cases of DDH result from the early phase of joint development within the first trimester of pregnancy. The remaining 98% of cases are caused by changes to a normal hip during the last weeks of pregnancy due to ligamentous laxity related to exposure to maternal hormones, frank breech presentation, oligohydramnios, etc. Postnatal factors are also discussed to play a role in DDH, such as tight swaddling or cradle boards which force the legs into extension and adduction and press the femoral head cephalad. This increased pressure in combination with shearing stress leads to a deformation of the hyaline cartilaginous roof and inhibits the maturation of the bony roof. If treatment is necessary, the age of the infant at the onset of therapy has to be taken into account, and the classification or stage of the DDH must be considered.
Generally, treatment follows a stepwise approach: Sometimes a preparation phase is necessary in late onset treatment before a reduction is possible. After the reduction, the hip joint is still unstable, therefore it is mandatory that a retention phase has to follow for stabilisation—before the final maturation phase can be started. During these stages, the femoral head should be constrained in a secure fixation in squatting position—also known as “human position”—to avoid excessive pressure on the cartilaginous roof, allowing remodelling of the bony roof. Excessive abduction has to be avoided to minimise the risk of avascular necrosis (AVN). Early DDH diagnosis by using US allows early treatment with faster remodelling and maturation of the poorly formed bony roof. Thus, the time of treatment can be considerably shortened.
 Pressure on the cartilaginous roof inhibits the growth and maturation of the bony roof.
Pressure on the cartilaginous roof inhibits the growth and maturation of the bony roof.
The US approach according to Graf’s technique is most commonly and widely used, especially in Europe, partially with the Rosendahl modification. It is also used in the Asian and South American region. It is based on the work of Graf and continuously adapted and optimised from 1980 until now. An alternative—particularly in France—is the femoral head coverage (the Morin and modified Morin–Terjesen method). While centres in North America also primarily use the Graf technique, they also typically add an assessment of the femoral head movement and its displacement from the acetabulum, known as the Harcke method.
15.3 Hip US According to Graf
The aim of the Graf method is to enable a reproducible, reliable, and standardised assessment of the neonatal hip. It consists of a standardised scanning protocol leading to acquisition of scans in a so-called standard plane. It then classifies the findings into four main types by description and angle measurements. A further subtle subclassification additionally takes the shape of the bony acetabulum in proportion to the stability of the cartilaginous acetabulum into account which reflects the coverage of the femoral head within the socket of the hip joint related to the age of the infant. It is important to know that the US appearance of the infant hip changes in the first few months of life, due to the ossification of the initially preformed cartilaginous structures.
The process for a correct and reproducible sonographic image of the newborn and infant hip according to Graf’s criteria follows a stepwise procedure (see below for further details). This acquisition process leads to reproducible images with a high intra- and inter-observer reliability that minimises diagnostic errors.
15.3.1 Standard Plane
Only the defined standard plane must be used for evaluating the hip joint to allow for a reproducible assessment. This necessitates proper imaging of the three following landmarks (Fig. 15.2):
-
The lower margin (also termed as lower limb) of the bony ilium in the depth of the acetabular fossa, which is the border to the triradiate cartilage. It has to be displayed clearly. For US purposes, the lower margin (limb) of the os ilium is the centre of the acetabulum. If this landmark is not depicted precisely on the US image, the sectional plane does not pass through the centre of the acetabulum and therefore no diagnosis can be made in a centred hip joint without this pivotal point.
 “No lower margin (limb), no diagnosis!”
“No lower margin (limb), no diagnosis!” -
The middle of the acetabular roof (= the midportion of the acetabulum). The shape of the iliac bone is seen as a straight line superior to the acetabular bony roof. This is the weight-bearing section of the hip joint when walking in upright position. The middle section is reached when the plane is rotated around the lower margin (limb) of the os ilium until it leaves the concave contour of the gluteal fossa (see below), representing the posterior plane. Then this can easily be identified as the concavity straightens, with a clear border to the cartilaginous acetabular roof and the labrum.
 In the posterior plane or section, the iliac contour is concave and bent, shaped away from the transducer. In the middle section—the standard plane—the iliac silhouette runs straight from the bony rim in cranial direction. “Straight” does not necessarily mean parallel to the edge of the monitor!
In the posterior plane or section, the iliac contour is concave and bent, shaped away from the transducer. In the middle section—the standard plane—the iliac silhouette runs straight from the bony rim in cranial direction. “Straight” does not necessarily mean parallel to the edge of the monitor! -
The acetabular labrum. The labrum on the inner side of the joint capsule is triangular in cross section—with a relatively high echogenicity due to the collagenous fibres. It is part of the cartilaginous roof. The base of the labrum is fixed laterally to the hyaline cartilage; the acetabular roof is displayed with low echogenicity.
 If any one of these three landmarks is missing or not clearly shown, the US examination is worthless and may not be used for diagnosis and angle measurement! Measuring in an incorrectly acquired US image leads to wrong and useless results. Therefore, it is crucial to pay special attention to the proper sequence of identification of the three landmarks. Only if the lower margin of the os ilium is shown one can proceed to check the sectional plane and lastly the acetabular labrum.
If any one of these three landmarks is missing or not clearly shown, the US examination is worthless and may not be used for diagnosis and angle measurement! Measuring in an incorrectly acquired US image leads to wrong and useless results. Therefore, it is crucial to pay special attention to the proper sequence of identification of the three landmarks. Only if the lower margin of the os ilium is shown one can proceed to check the sectional plane and lastly the acetabular labrum. -
Then the hip angle measurement is performed by inserting three lines to define the two angles Alpha (α) and Beta (β) (details see below) (Fig. 15.3).
 “No lower margin (limb), no diagnosis!”
“No lower margin (limb), no diagnosis!” In the posterior plane or section, the iliac contour is concave and bent, shaped away from the transducer. In the middle section—the standard plane—the iliac silhouette runs straight from the bony rim in cranial direction. “Straight” does not necessarily mean parallel to the edge of the monitor!
In the posterior plane or section, the iliac contour is concave and bent, shaped away from the transducer. In the middle section—the standard plane—the iliac silhouette runs straight from the bony rim in cranial direction. “Straight” does not necessarily mean parallel to the edge of the monitor! If any one of these three landmarks is missing or not clearly shown, the US examination is worthless and may not be used for diagnosis and angle measurement! Measuring in an incorrectly acquired US image leads to wrong and useless results. Therefore, it is crucial to pay special attention to the proper sequence of identification of the three landmarks. Only if the lower margin of the os ilium is shown one can proceed to check the sectional plane and lastly the acetabular labrum.
If any one of these three landmarks is missing or not clearly shown, the US examination is worthless and may not be used for diagnosis and angle measurement! Measuring in an incorrectly acquired US image leads to wrong and useless results. Therefore, it is crucial to pay special attention to the proper sequence of identification of the three landmarks. Only if the lower margin of the os ilium is shown one can proceed to check the sectional plane and lastly the acetabular labrum.
(a) Normal US image of a normal hip according to Graf. (b) Same image with landmarks indicated

Hip US—Graf standard plane. (a) Schematic drawing of relevant structures, lines, and angles for hip US according to Graf. (b) Typical corresponding US image (standardised projection—upright position, always projected as right sided). Note the blurred acetabular rim
15.3.2 Device Presets
Images with relatively strong contrast (e.g. hard post-processing with low dynamic range) are preferred. This allows a good discrimination of interfaces and better identification of the anatomic structures. The focus should be positioned at the level of the hip joint; there is no need for a multi-focus scan (this might slow the scan and thus make the investigation more cumbersome).
The image orientation is defined: cranial is on the right side of the monitor image. Some turn the monitor by 90° (up = cranial) as originally introduced to reflect a somewhat anatomic projection similar to a radiograph (as shown in most figures in this chapter).
-
Some devices allow for flipping the image on the display into this above-mentioned orientation.
-
Rarely (not consistent with general recommendations) the cranial position is defined as in an abdominal US (the left side of the monitor is cranial), for example if the hip scan is performed after an abdominal US.
-
Both hips are displayed on the screen in the same way as right sided joint, similar as in radiography. So, for documentation it is necessary to insert a marker or pictogram for side identification.
 Make sure that with this orientation the system’s angle measurement software is not confused—as it may happen in some US systems; this may also happen if you use the left-right inversion button in some devices!
Make sure that with this orientation the system’s angle measurement software is not confused—as it may happen in some US systems; this may also happen if you use the left-right inversion button in some devices!
15.3.3 Examination Technique
15.3.3.1 Positioning the Infant for Sonographic DDH Assessment
When using Graf’s technique, the infant is positioned in lateral decubitus position with a slightly bent hip and rotated inward. An extreme extension as well as flexion should be avoided.
Specific devices for placing the infant and stabilising the transducer may be helpful. It is noteworthy that they are recommended by some examiners, but not mandatory. These devices can help to reduce angulation artefacts and can also notably increase the precision of the scan—independent from the skill and experience of the examiner.
After the static examination, an additional stress test for dynamic assessment is performed in the same position and maintaining the standard section.
 The stress test is mandatory in all hips which are not within the physiological range or have a clinical abnormality/risk factor.
The stress test is mandatory in all hips which are not within the physiological range or have a clinical abnormality/risk factor.
The French approach for femoral head coverage assessment and the Graf’s modified approach according to Rosendahl use a similar examination technique.
For hip US according to Harcke, the infant is placed in supine or lateral decubitus position during the dynamic examination, and the hips are scanned in coronal and transverse planes—with the legs in a neutral position and flexed (details see below).
15.3.3.2 Access from Lateral in Coronal Section
The goal is the acquisition of an image in the reproducible standard plane in the mid portion of the acetabulum according to Graf (Figs. 15.2 and 15.3).
The transducer is placed over the major trochanter in a cranio-caudal coronal direction.
Then the transducer is carefully moved to parallel sections and rotated on the acetabular axis without tilting—thus imaging the standard plane essential for diagnosis and measurement. It is important that the lower margin (lower limb) of the os ilium is clearly seen and identified. Then the transducer is rotated from the bowed concave silhouette of the gluteal fossa until it straightens into the standard plane (Fig. 15.4a, b).

(a) Hip US according to Graf, dorsal plane—gluteal fossa. Note the concave shape of the os ilium bent away from the transducer. (b) Rotation to the standard plane: The contour of the os ilium becomes straight
The structures are then identified on an adequate view of the acetabular mid portion and the landmarks are checked.
15.3.3.3 Dynamic Assessment in the Graf Technique
A dynamic assessment is advisable even in normal-appearing newborn hips. The femoral head can be mobile due to laxity of the joint capsule after birth induced by maternal hormones. In a normal joint, an elastic whipping of the cartilaginous roof with the labrum may be seen. This may not be confused with the dislocation or provocable dislocation of the femoral head in instable and decentred hips.
Dynamic assessment is mandatory with suspicious clinical examination results or if any suspicious findings in the standard section are noted, also in neonates with other risk factors (see above).
The technique is rather simple: push the leg softly in cranial and slight dorsal direction for assessment of stability whilst stabilising the back of the infant. If a positioning device is used, the buckles serve as abutment.
In a stable hip joint, the femoral head stays well positioned within the socket and the cartilaginous roof exhibits only subtle movements (“whipping”).
In an instable hip joint, the displacement of femoral head is seen—out of the dysplastic acetabular fossa superiorly; the acetabular labrum is displaced in cranial direction without losing contact to the femoral head. In dislocated or luxated hips reducibility into a normal human position is checked, paying attention to probable reposition obstacles. This is achieved by a soft pulling and abducting manoeuvre under US surveillance.
15.3.4 Documentation
At least two individually acquired images must be recorded per hip joint; these are taken in the standard plane with a pictogram or any other clearly evident side identification for documentation. One of these two images must contain the correct measurement lines (see Fig. 15.5).

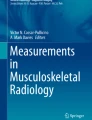
Hip US according to Graf: Relevant structures, one of hip US image according to Graf without (a) and one with (b) angle measurements. Patient identification and side mandatory, (gestational) age helpful. (a) 1 transition zone of osseous to cartilaginous part of femur, 2 femoral head, 3 fold, 4 capsule, 5 cartilaginous labrum, 6 cartilaginous roof, 7 osseous contour of ilium bone, 8 bony rim, 9 lower margin (limb). (b) 1 base line, 2 bony roof line, 3 cartilaginous coverage line, α (between line 1 and 2) 60°, β (between lines 1 and 3) 71°
Recommendations for documentation in unstable hips include a series of images—or better—a video-clip/cine-loop showing all respective changes, particularly also during the stress manoeuvre.
15.3.5 (Normal) US Anatomy of the Newborn and Infant Hip (Fig. 15.5)
To identify all relevant structures in the standard plane, it is helpful to follow a structured and stepwise assessment. This avoids misinterpretation and incorrect findings.
-
Femoral head: The hyaline cartilaginous femoral head is roundish, with a low echogenicity and scattered internal echoes representing vascular sinusoids. Later the central echogenic ossification centre appears, termed the nucleus. Its size varies depending on age. It is not round nor necessarily in the centre of the femoral head and only its outer border is visible.
 On US, the nucleus cannot be used as on radiographs for assessing the position of the femoral head in relation to the acetabulum. It is important to note that the size of the ossified part of the femoral head is the limiting factor for hip US performance, which therefore has no clear age limit. When the ossified nucleus becomes large, it blocks the US beam producing a broad acoustic shadow. This inhibits the visualisation of the lower margin (limb) of the os ilium in the mid portion of the acetabular fossa.
On US, the nucleus cannot be used as on radiographs for assessing the position of the femoral head in relation to the acetabulum. It is important to note that the size of the ossified part of the femoral head is the limiting factor for hip US performance, which therefore has no clear age limit. When the ossified nucleus becomes large, it blocks the US beam producing a broad acoustic shadow. This inhibits the visualisation of the lower margin (limb) of the os ilium in the mid portion of the acetabular fossa. -
Ossified femoral neck: It is the border zone between the ossified part of the femur and the cartilaginous femoral head termed osseocartilaginous junction.
-
Joint capsule: The capsule runs from the femoral neck to the acetabulum and inserts into the periosteum of the os ilium.
-
Cartilaginous acetabular roof: It is composed of two components. The lateral portion is the fibrocartilaginous acetabular labrum, a hyperechoic triangular structure between the joint capsule and the femoral head. The labrum is laterally fixed at the hyaline cartilage roof. This is the second portion, which is normally hypoechoic, with the same echogenicity as the femoral head.
-
The osseous os ilium: The lateral contour of the iliac bone is seen as a straight line that runs cranially with a clear border to the cartilaginous acetabular roof and allows a good osseous definition. In caudal direction, the bony rim and the osseous roof complete the roof of the femoral head.
-
The socket or acetabular roof is composed of both the osseous and the cartilaginous roof.
 On US, the nucleus cannot be used as on radiographs for assessing the position of the femoral head in relation to the acetabulum. It is important to note that the size of the ossified part of the femoral head is the limiting factor for hip US performance, which therefore has no clear age limit. When the ossified nucleus becomes large, it blocks the US beam producing a broad acoustic shadow. This inhibits the visualisation of the lower margin (limb) of the os ilium in the mid portion of the acetabular fossa.
On US, the nucleus cannot be used as on radiographs for assessing the position of the femoral head in relation to the acetabulum. It is important to note that the size of the ossified part of the femoral head is the limiting factor for hip US performance, which therefore has no clear age limit. When the ossified nucleus becomes large, it blocks the US beam producing a broad acoustic shadow. This inhibits the visualisation of the lower margin (limb) of the os ilium in the mid portion of the acetabular fossa. The strong echoes of the os ilium are produced by total reflection and absorption of parallel US beams with acoustic shadowing, mimicking an outer and inner wall. Only the lateral surface artefact is seen in the US image.
The strong echoes of the os ilium are produced by total reflection and absorption of parallel US beams with acoustic shadowing, mimicking an outer and inner wall. Only the lateral surface artefact is seen in the US image.
15.3.6 US Criteria in Graf’s Technique (Landmarks) (Fig. 15.2)
Only US images taken in the standard plane with the three obligatory landmarks are allowed to be used for diagnosis and measurements. These must contain:
-
The lower margin of the bony ilium in the depth of the acetabular fossa representing the physis, the iliac growth plate (as part of the triradiate cartilage).
-
The midportion of the acetabular roof with a straight iliac bone line running cranially.
-
The triangular acetabular labrum.
If any one of these three points is missing or not clearly shown, the US is inadequate and therefore angle measurements are unreliable and can even worsen the diagnosis.
15.3.7 Findings in DDH
Sonographic criteria vary depending on the method applied (Graf, Harcke, adapted Graf by Rosendahl, femoral head coverage according to Morin and Terjesen, pubo-femoral distance).
Comment
There is a general agreement that it is important to diagnose DDH early in order to avoid long-term sequelae with immense healthcare costs and even individual morbidity, e.g. by repeated surgery and even early joint replacement. Hence, early detection by US is seen as an advantage allowing for an early start of treatment. Then the treatment duration can be considerably shortened and outcome is improved, also reducing the need for invasive procedures. Nevertheless, the debate on the role of general versus selected US screening (or even only individual US indications based on some sort of clinical screening) is ongoing in the Anglo-American literature, whilst in most of the middle European Countries, a general US screening is established; a similar approach is discussed in some Asian and South American countries.
 Hip US for detection DDH is called a “final” investigation indicating the risk that if one misses an endangered hip, the patient will only come back after years or decades when he/she is symptomatic. Therefore, strict and consistent adherence to all quality criteria is essential. In addition, although clinical investigations and anamnestic data are a mandatory part of every examination, these are not sufficient to detect subtle changes and should not be used as exclusive screening tools particularly in (preterm) neonates or neonates at risk.
Hip US for detection DDH is called a “final” investigation indicating the risk that if one misses an endangered hip, the patient will only come back after years or decades when he/she is symptomatic. Therefore, strict and consistent adherence to all quality criteria is essential. In addition, although clinical investigations and anamnestic data are a mandatory part of every examination, these are not sufficient to detect subtle changes and should not be used as exclusive screening tools particularly in (preterm) neonates or neonates at risk.
15.3.8 Angle Measurement: Measured Between the Three Lines
Three lines form the two angles alpha (α) and beta (β):
-
Base line: It is drawn from the most upper portion of the hyaline cartilage as pivot point caudally, tangential to the echo of the os ilium where the proximal perichondrium inserts to the periosteum of the os ilium (Fig. 15.6a).
 The baseline is not necessarily paralleling the near field border of the US image (the transducer).
The baseline is not necessarily paralleling the near field border of the US image (the transducer). -
Bony roof line or acetabular roof line: It is drawn from the inferior margin (lower limb) of the acetabulum as pivot point tangential to the bony roof (Fig. 15.6b). This definition implies the outer border of the os ilium.
-
Cartilage roof line: It is drawn from the bony rim through the centre of acetabular labrum (Fig. 15.6c). The bony rim is defined as the transition point where the convexity of the osseous acetabulum changes into its concavity. This is the most outer point of the osseous socket.
 These three lines do not necessarily intersect in one point!
These three lines do not necessarily intersect in one point! -
The bony angle alpha (α) is formed between the base line and the bony roof line (Fig. 15.6d, e); it reflects the osseous coverage and quantifies the bony socket.
-
The cartilage angle beta (β) is formed between the base line and the cartilaginous roof line (Fig. 15.6d, e); it quantifies the cartilaginous acetabular roof.
 The baseline is not necessarily paralleling the near field border of the US image (the transducer).
The baseline is not necessarily paralleling the near field border of the US image (the transducer). These three lines do not necessarily intersect in one point!
These three lines do not necessarily intersect in one point!
Angle measurements and lines in hip US according to Graf (a–f). (a) How the baseline is defined. (b) Definition of acetabular roof line. (c) Cartilaginous roof line added, (d) with normal angle α and β—upright standard view, increasingly used for practicability and device restrictions; (e) Hip US with integrated calculation software: the software automatically indicates angles (α 54°, β 75°) (f) not an upright standard view, cranial on this image is displayed on right-hand side: increasingly used for practicability and device restrictions; sonometer software indicates hip type (full line) after manual definition of respective lines (immature type II hip, sufficient or suboptimal coverage, dynamic assessment shows elastic whipping)
With these two angles, the entire socket with its bony and cartilaginous parts can be accurately assigned to a specific hip type. This measurement system is independent of the position of the infant, the projection, and the presence of an ossified centre of the femoral head. Additional measurement lines and calculations were shown not to improve results or precision.
 The angle measurement system is only valid in correctly performed exams (see above). It is used to determine the presence of hip dysplasia and to categorise its severity using the most widely accepted Graf classification. A correct section through the hip joint with sufficient depiction of all three landmarks is mandatory for judging hip maturity and for performing angle measurements—if a section is taken angulated or too ventrally or dorsally (usually recognisable by a bent shape of iliac line or incorrect/missing identification of the bony fossa definition), measurements are always wrong and therefore diagnostically useless. So NEVER use these images to try to make a diagnosis!
The angle measurement system is only valid in correctly performed exams (see above). It is used to determine the presence of hip dysplasia and to categorise its severity using the most widely accepted Graf classification. A correct section through the hip joint with sufficient depiction of all three landmarks is mandatory for judging hip maturity and for performing angle measurements—if a section is taken angulated or too ventrally or dorsally (usually recognisable by a bent shape of iliac line or incorrect/missing identification of the bony fossa definition), measurements are always wrong and therefore diagnostically useless. So NEVER use these images to try to make a diagnosis!
An α-angle of 60° or greater is considered normal in any age and implies a mature hip joint.
Smaller α-angles indicate poorer coverage and at least immaturity (in infants younger than 3 months) or dysplasia in infants older than 3 months. The soft cartilaginous roof must compensate the ossification deficit and cannot resist the pressure of the femoral head in cranial direction. The β-angle indicates the risk of instability—the higher the angle, the worse the risk.
15.3.9 Classification of the Hip According to Graf
The strict classification not only differentiates between normal hips, dysplasia, and luxation. It also takes into account the age-dependent maturation and thus allows for differentiation between physiologic immaturity and a maturation deficit (Table 15.1).
The US grading correlates with the pathological changes in the hip joint. In cases with dislocation, the femoral head was initially positioned within the socket, but biomechanical factors caused cessation of the normal development and the femoral head started to slide out of the socket thus deforming the acetabulum (developing dislocation of the hip).
The classification is composed by description and measurement.
 Description and measurement must be consistent!
Description and measurement must be consistent!
15.3.9.1 Type I: Normal or Mature Hip (Figs. 15.2, 15.4, and 15.5)
This hip type is considered mature at any age and can therefore be present already at birth. Maturation should be completed at the age of 3 months.
The degree of the ossification of the bony acetabular roof is appropriate for a hip joint of an infant at the age of 3 months. The bony socket is well developed with normal position of a well-covered femoral head in the acetabular fossa. The bony rim is angular or slightly blunt, but well defined. The cartilaginous acetabular roof covers well the femoral head, holding it firmly in the socket (the cartilage “covers” the head) (Fig. 15.7).

Schematic drawing (a) and US image (b) of hip US according to Graf showing findings in Type I
The bony angle (α) between base line and bony roof line is >60°.
The cartilaginous angle (β) is <55°.
 In newborns, β-angles are shown to be higher, even in static examinations (see Sect. 15.3.3—“Dynamic Assessment in the Graf Technique”).
In newborns, β-angles are shown to be higher, even in static examinations (see Sect. 15.3.3—“Dynamic Assessment in the Graf Technique”).
15.3.9.2 Type II: Immaturity
The physiologic hip maturation of an immature hip tends to be rapid in the first few weeks (namely 4–6 weeks) after birth, with a normal hip development expected within the first 12 weeks of age. So, these hips are termed as “physiologically immature” and are labelled as “Type IIa”. These type IIa hips are further subclassified into hips that show appropriate development at or after the sixth week. This finding is classified as a normal/physiological immature hip joint with favourable outcome and most probably normal maturation to a mature hip joint (Type IIa+).
Hips with persistent immaturity after the sixth week are classified as hips with delayed maturation (Type IIa−) remaining at higher risk for a maturation/ossification deficit by the time the infant reaches the age of 12 weeks.
 The age of the infant with physiologic maturation has to be taken into consideration. Depending on the subtype, the rounded bony roof is defined from sufficient (or adequate/satisfactory) to deficient. The cartilaginous acetabular roof still covers more than half of the femoral head, but appears much wider than the osseous acetabulum due to poorer ossification.
The age of the infant with physiologic maturation has to be taken into consideration. Depending on the subtype, the rounded bony roof is defined from sufficient (or adequate/satisfactory) to deficient. The cartilaginous acetabular roof still covers more than half of the femoral head, but appears much wider than the osseous acetabulum due to poorer ossification.
-
Subtypes of hip Type II:
-
IIa +: physiologic immaturity. Spontaneous maturation is expected
-
IIa−: maturation deficit within the first 3 months of life. Follow-up exams are recommended because of the risk of potentially delayed ossification (Fig. 15.8).
-

Schematic drawing (a) and US image (b) of hip US according to Graf showing findings in Type II. (c) Image Type D. Note the insufficiently covered femoral head in (c) opposite to (b) where the femoral head is centred. The arrow (in a) indicates the acetabular rim/y-suture
15.3.9.3 Type IIb: Ossification Deficit
After the age of 3 months, a Type II hip is described as Type IIb and classified to have an ossification deficit and be dysplastic. In Type IIb hips, the labelling “b” underlines the importance to state the age. Hips with ossification deficits are at risk for residual dysplasia.
Follow-up examinations and eventually treatment are recommended.
Measurements in Type IIa and Type IIb hips:
α-angle ranges between 50° and 59°, β-angle is > 77° (exception: newborns have higher β-angles).
15.3.9.4 Type IIc
This hip type is termed “critical hip” or “hip at risk”. It describes a developmentally dysplastic hip that is definitely endangered for residual dysplasia and even decentration. This type needs treatment.
On US, it exhibits a very rounded bony rim which is severely deficient, with a cartilaginous roof that still covers the femoral head. In some hips, the cartilaginous roof can be displaced upwards during the mandatory dynamic stress manoeuvre (this allows the discrimination between Type IIc = stable, and an unstable hip).
Measurements in Type IIc hips:
α-angle = 43°–49°, β < 77° (stable in the stress test).
α-angle = 43°–49°, β > 77° (unstable in the stress test).
15.3.9.5 Decentred Hips
15.3.9.5.1 Type D (Formerly IId)
This type defines an unstable hip with beginning decentration. On US it exhibits a very rounded bony rim with already initially displaced cartilaginous acetabulum that is pressed upwards by the femoral head.
Treatment with fixation of the femoral head in the socket is recommended.
Measurements in Type D hips:
α angle = 43°–49°, β > 77°.
15.3.9.5.2 Type III: Decentred Hip
This type shows an insufficient osseous containment with a flat bony rim. The bony as well as cartilaginous coverage is poor. The femoral head is decentred, and the cartilaginous acetabulum is displaced upwards because the femoral head has pushed the cartilaginous acetabular roof in cranial and dorsal direction.
This type needs treatment by repositioning and secure fixation.
On US, the following features are seen:
-
Type IIIa: The cephalad displaced hyaline cartilage is hypoechoic.
-
Type IIIb: Due to a long-standing pressure of the femoral head on the cartilaginous acetabulum, structural anomalies occur and the echogenicity increases and becomes higher than the cartilage of the femoral head. This is a sign of severe damage with poor outcome of the joint and occurs only in untreated hips which have been dislocated for a long time or in neglected cases (very uncommon in middle Europe) (Fig. 15.9).

Schematic drawing (a) and US image (b) of hip US according to Graf showing findings in Type III. The arrow in (a) demonstrates the displacement of the cartilagenous roof and the contour of the joint capsule running cephalead
Measurements in Type III hips:
α angle = <43°, β-angle > 77°.
15.3.9.5.3 Type IV: Luxated Hip (Fig. 15.10)
In this most severe form of DDH, the femoral head is displaced from the joint space and luxated into a cranial and dorsal position. The cartilaginous acetabulum is herniated, displaced caudally, and compressed between the femoral head and the iliac bone.

Schematic drawing (a) and US image (b) in hip US according to Graf showing findings in Type IV. Note the shape of the joint capsule arrow in (a) demonstrates the contour of the caudally pressed joint capsule
 In decentred hips, measurements are not necessarily required and often impossible, because the displaced femoral head has left the standard plane when moving in cranio-dorsal direction, out of the dysplastic socket. This is why the bony rim is often not displayed on the US image.The dynamic assessment helps to evaluate for reducibility and to rule out reposition obstacles, such as, for example some intraarticular fibro-fatty tissue (pulvinar), constriction of the elongated joint capsule, or a tight iliopsoas tendon.
In decentred hips, measurements are not necessarily required and often impossible, because the displaced femoral head has left the standard plane when moving in cranio-dorsal direction, out of the dysplastic socket. This is why the bony rim is often not displayed on the US image.The dynamic assessment helps to evaluate for reducibility and to rule out reposition obstacles, such as, for example some intraarticular fibro-fatty tissue (pulvinar), constriction of the elongated joint capsule, or a tight iliopsoas tendon.
 Also note that wrong angulation will cause wrong results—dedicated devices are available to reduce the probability of this common pitfall (Fig. 15.11).
Also note that wrong angulation will cause wrong results—dedicated devices are available to reduce the probability of this common pitfall (Fig. 15.11).

(a–c) Common pitfall in hips US: wrong angulation with respective implication on angle measurements in the Graf and modified Rosendahl method: As demonstrated in schematic drawing of a table corner, the angle will appear different depending on the viewing angle and perspective (a), influencing angle measurements on US (b)—where the correct angle measurement is only given on the lower hip US image, whereas the upper image exhibits wrong angle measurements; the malposition is recognisable by missing femoral structures (e.g. osseocartilaginous junction) on the respective upper hip US image. Note that the measurement lines do not have to cross in one point to be correct. (c) shows a technical device that may help to avoid accidental tilting of the transducer
The discussion about the necessity of follow-up US exams in immature hips is still ongoing. In the Anglo-American countries, the costs to the health care system are strongly taken into account. The screening policies also differ in different countries, because multicentre prospective randomised controlled trials are lacking. There is consensus that these studies are judged to be unfeasible from the ethical point of view. To stratify newborns or infants to the control group without follow-up or even treatment might cause unpredictable harm to this group of study members. Furthermore, if properly done the study must be performed over decades to determine late sequelae of a missed dysplasia, whilst there is consensus that a missed and untreated displacement of the hip is deleterious to the joint (Fig. 15.12a, b).

Schematic drawing of the different hip types with angle measurement helpful for classification (“Sonometer”)
There is consensus that a radiograph should be performed in infants with treated hips after the onset of walking. So-called residual dysplasias and missed dysplasias as a result of maturation deficit are not detectable solely by clinical examination. Children with residual and late dysplasias are at higher risk for earlier and prolonged orthopaedic problems, even resulting in hip replacement. Furthermore, secondary hip dislocation may occur in, e.g. neurologically impaired infants and children then necessitating a radiograph.
 Comment on “How to perform hip US according to Graf’s technique”: There is consensus that the examination should be performed by appropriately trained health professionals. The training should be offered in standardised and approved training programmes and taught by certified and approved trainers and instructors—with accreditation by organisations that guarantee and survey the quality of the content of the training programme. A learning by doing, e.g. as by bed-side teaching only, was proven not to be sufficient. An ongoing quality assurance programme with respective audits is valuable to ensure persisting quality even after years.
Comment on “How to perform hip US according to Graf’s technique”: There is consensus that the examination should be performed by appropriately trained health professionals. The training should be offered in standardised and approved training programmes and taught by certified and approved trainers and instructors—with accreditation by organisations that guarantee and survey the quality of the content of the training programme. A learning by doing, e.g. as by bed-side teaching only, was proven not to be sufficient. An ongoing quality assurance programme with respective audits is valuable to ensure persisting quality even after years.
15.4 Modified Graf Classification (Rosendahl)
In the imaging approach, there is no essential difference from the Graf technique, but with addition of a compulsory stress test (similar to Graf’s “dynamic examination”). But this classification further aims at simplifying the grading. According to the morphology (using Graf’s angle discrimination), one categorises hips into immature, mildly dysplastic, or severely dysplastic. Using stability for discrimination hips are classified as stable, dislocatable, or dislocated, thus it classifies hip morphology and stability separately and offers a simpler and less subtle grading. The age of the infant is not taken into account, but the system is more easily and consistently applicable—although with a lower fine-tuning.
-
Technique: The hip morphology (α-angle) is assessed in standard coronal view (Graf) with a centred femoral head. If the hip is decentring, eccentric, or dislocated (Graf types 2c, D, 3, 4), an attempt is made to relocate the femoral head by mild traction, and thereafter hip morphology is reassessed. If the hip is irreducible, the morphology is assessed with dislocated femoral head.
 Always an additional Barlow manoeuvre is performed to assess for coexisting instability even in morphologically normal hips. The stability is classified as above.
Always an additional Barlow manoeuvre is performed to assess for coexisting instability even in morphologically normal hips. The stability is classified as above.
15.5 Hip US According to Harcke
In North America, hip US with the dynamic manoeuvre according to Harcke has become widely used. The exact study protocol varies among institutions and it relies on the sonographer’s skill in performing the examination and interpreting the result of the images without angle measurements.
This technique parallels the clinical manoeuvres of Barlow and Ortolani during the physical examination of the hip. It attempts also to detect a subtle instability, which eluded the clinical examination. Thus, the objective is to classify hip stability.
15.5.1 Technique
The infant is placed in supine or lateral decubitus position, and the transducer is positioned over the lateral or posterolateral aspect of the hip. The position of the femoral head at rest is noted in a neutral position. Then the stability of the hip is assessed with motion and gentle stress by pushing the femoral head posteriorly as in Barlow’s manoeuvre. Then the development and configuration of both the bony and cartilaginous acetabulum are assessed.
Usually the examination has four steps:
-
Coronal images with the hip in neutral position (similar to Graf’s method).
-
Coronal images with the hip in flexion, plus a posterior lip view.
-
Then transducer is rotated to obtain transverse images with the hip flexed, with passive abduction and adduction.
-
This is finally followed by transverse images in neutral position and with posterior stress—to evaluate hip stability.
15.5.2 Normal Findings During Harcke Investigation
On coronal extension and flexion views, the cartilaginous femoral head is contained within the acetabulum defined by the triradiate cartilage centrally and the posterior ischium, with the femoral metaphysis seen anteriorly. Approximately half of the diameter of the femoral head lies on either side of the ilium. On the transverse extension view, the femoral head is seated in the centre of a V-shaped acetabulum formed by the ischium posteriorly, the pubic bone anteriorly, and the triradiate cartilage centrally.
When the Barlow manoeuvre is performed, no displacement is seen with stress and the image remains the same, with the head centred in fossa (see Fig. 15.13a).

(a) Obvious dislocation of both hips on a pelvic radiograph in an infant—this imaging however is not the standard first step when assessing hip dislocation or DHD, (b) Dislocation of the left hip. Note the severe defect of the bony rim, the smaller centre of the femoral head that is displaced cephalad
15.5.3 DDH According to Harcke
The position and stability of the femoral head at rest and with stress are reported as normal, subluxatable with stress, subluxed or dislocated (see Fig. 15.14b). With the abduction manoeuvres the formerly displaced femoral head with no contact or coverage to the acetabulum is shown to return to the acetabulum. The coronal neutral image has traditionally been used to evaluate the degree of femoral head coverage and the acetabular shape. Respective images must document all findings and need to be labelled appropriately (Fig. 15.14a).

Harcke hip US (a) Normal hip: normal position of the femoral head on this transverse flexion view. Note the cup-like appearance formed by the metaphysis and the ischium. No change with stress manoeuvre. (b) Coronal flexion view. (c, d) Abnormal hip: transverse view of the hip with stress showing subluxation of the femoral head from its normal position and disruption of its cup-like configuration. This hip was reducible. Abbreviations: F femoral head, M femoral metaphysic, I ischium, T triradiate cartilage. Arrow: cartilaginous labrum. (Courtesy of Dr. B. Coley, Cincinnati/Ohio, USA)
In abnormal decentred hips, either Harcke’s or Graf’s method can be applied additionally for treatment decisions.
A similar approach is used for the “femoral head coverage” assessment (French approach).
 The method is more subjective, but it also includes description of hip stability. Neither accuracy nor population-based rates of pathological hips have been published based on this technique.
The method is more subjective, but it also includes description of hip stability. Neither accuracy nor population-based rates of pathological hips have been published based on this technique.
15.6 Femoral Head Coverage According to Morin (and Modified Morin = Terjesen, Also Called the French approach)
This method assesses the degree of lateralisation of the femoral head based on Graf’s standard plane or Harcke’s coronal flexion view—with the child placed in supine position. The Graf standard plane is recommended, but not mandatory.
A modified Graf’s baseline is drawn through the lateral bony rim of the acetabulum parallel to the long axis of the transducer. Then two additional lines parallel to this iliac line are added—one indicates the lateral border of the femoral head in the near field of the transducer and the other the medial part (i.e. the junction of the femoral head in the depth of the acetabular fossa).
The distance between medial and iliac line (a) and between medial and lateral line (b) is measured.
The ratio is multiplied by 100 which gives the coverage degree as a percentage of the femoral head covered by the bony acetabulum (Fig. 15.15).

Femoral head coverage (a) Scheme (b) modified Graf standard plane. Child placed in supine position
15.6.1 Modified Morin (Terjesen)
The hip is assessed in Graf’s standard plane, but instead of the baseline according to Graf a line through the lateral bony rim of the acetabulum parallel to the long axis of the transducer is drawn. Then the “bony rim percentage”, later named “femoral head coverage” is assessed as above.
-
Anatomic landmarks and normal limits for measuring the femoral head coverage:
The lateral part of femoral head, the contour of the bony os ilium, and the medial junction of the head in the acetabular fossa are used, additionally if required the pubic bone.
15.6.2 Hip Assessment Based on Femoral Head Coverage
All results outside of the accepted limits (see below) reflect DDH. But this classification has less potential for grading, and can only be used as an initial screening tool to assess for normal or abnormal hips. Further grading (if necessary for treatment decisions) is then often performed using Graf’s or the modified Graf method.
-
Coverage degree
Normal: | >55% |
Lower normal limits: Male Female | −47% −45% |
Undetermined: | 45–54% |
Altered: | <45% |
15.6.3 Pubo-Femoral Distance
This parameter is sometimes also assessed. For being able to achieve this, the centre of the pubic bone needs to be displayed as a roundish hyperechoic cup on the US image.
The distance between the medial border of the femoral head and the ossified portion of the pubic bone is measured.
Distances ≤6 mm or a difference of less than 0.15 cm between both sides are considered normal.
15.7 Three-Dimensional US (3DUS) for DDH Assessment
Several attempts have been made to use (semi-)automated 3DUS reconstruction algorithms for presenting the hip in a standardised fashion after 3DUS acquisitions (usually using the Graf or Rosendahl approach) and for automated angle measurements. However, 3DUS is currently not introduced into daily clinical practice—in part also because of the equipment (and cost) implications and its restricted availability.
There are some potential advantages: possibly 3DUS may offer a better standardisation if the acquisition is done properly, particularly less dependent on possible angling and tilting errors.
Disadvantages are that 3DUS has a higher risk of motion artefacts during acquisition. Furthermore, no dynamic scanning is possible at present (so-called real time 4DUS) for this application, particularly visualisation of these changes in rendered views is difficult. And the available linear or curved-array 3DUS transducers are rather clumsy—the much smaller and handier available 3DUS sector transducers should not be used for hip US, as these may impair measurement accuracy.
15.8 Ultrasound and Imaging of Other Hip Conditions
There are a number of conditions which more commonly affect older infants and children. However, some may also occur in neonates and as such are briefly addressed. A more detailed description of all other applicable imaging methods with illustration of respective findings can be found in the respective chapters of the books such as Chap. 14 on imaging the neonatal musculoskeletal system or Chap. 17 on imaging in neonatal trauma.
The queries for these other sonographic hip assessments throughout childhood are a painful hip mainly caused by hip effusion, which may be accompanied by capsular thickening (Fig. 15.16). Others, but much rarer aspects depictable by US are irregularity of bony structures and other pathologic features like disruption of the osseous contour.

Hip US in simple hip effusion (transient synovitis, extended field of view): echo-free fluid in widened joint space, thickened capsule
15.8.1 Indications and Technique
The sonographically targeted features are joint effusion, capsular thickening in inflammatory conditions, a slipped (capital femoral) epiphysis, proximal femoral deficiency, and others such as rare tumours or Perthes disease, trauma, or other joint haemorrhage.
For all these queries, the US approach is different from the classical DDH scanning technique: Ultrasound should be performed in a supine position leaving the leg in a resting position, which is typically slightly flexed and externally rotated (important also for pain relief). Manipulation can cause discomfort and stress induced defense with a restless child, leading to prolonged examination time and poorer result. A support under the popliteal fossa may be helpful to relax the leg and make the examination less painful.
 It is highly recommended to start the examination with the contralateral, not affected, healthy side. This is also helpful for intraindividual comparison to become familiar with the individual normal anatomy. This approach is recommended for every musculoskeletal examination performed on the extremities.
It is highly recommended to start the examination with the contralateral, not affected, healthy side. This is also helpful for intraindividual comparison to become familiar with the individual normal anatomy. This approach is recommended for every musculoskeletal examination performed on the extremities.
The use of a linear transducer is preferred. A trapezoid or virtual convex mode widens the view and may allow for a better overview. Sometime a panoramic mode (e.g. extended-field-of-view) is useful to demonstrate large soft tissue masses or longer segments of bony structures. The range of the chosen beam frequency depends on the age and size of the infant; the selection of the transducers varies—one may also need lower frequencies in older children or for deep structures (frequency range 14/10–3 MHz); also curved arrays may be used in such situations. Sometimes the split-screen/dual image function may be helpful for direct comparison of affected and unaffected side.
The transducer is positioned longitudinally on the groin—anteriorly along the femoral neck, usually slightly lateral to the course of the femoral vessels. By this sagittal and parasagittal sections are acquired. Cross sectional/axial views are rarely helpful, but can be acquired in selected cases.
15.8.2 The Normal Hip Joint
Typical US findings in normal hip joints performed in longitudinal sections with a frontal sagittal view show the ossified femoral head, the femoral neck connected by non-ossified physis (= an anechoic line). The visible contours of the acetabulum and the femoral head and neck appear continuous, without disruption, smooth and with a clearly defined non-interrupted surface (Fig. 15.17b). Osseous defects can also be seen. The anterior part of the joint capsule parallels the anterior cortex of the femoral neck and has a concave shape. The fibrous joint capsule is normally displayed with two small layers, separated by the small apposed synovial lining—producing an acoustic artefact presenting as a linear echogenic reflection or a small amount of anechoic fluid within the joint space that separates the two capsule layers.

(a, b) Normal longitudinal hip US in an older child: normal joint capsule (synovium) appears prominent, parallels the anterior cortex of the femoral neck and has concave shape as both layers are collapsed schematic drawing (a) and US image (b)
15.8.3 Arthritis and Inflammation of Hip Joint
The most common cause in neonate is (septic) coxitis, in the older infant transient synovitis of hip (toxic synovitis, parainfectious synovitis, “coxitis fugax”).
The irritable hip is a common disorder in childhood characterised by acute onset with refusal to walk. In most cases, the medical history and the physical examination completed with basic laboratory testing (e.g. full blood count, CRP) together with US usually establish the diagnosis. Normally, the clinical symptoms and the joint effusion improve and resolve within a few days. A prolonged or even persisting clinical course and effusion have to attract attention to important differential diagnoses, particularly Perthes disease, Lyme arthritis, or diseases within the rheumatic spectrum. Therefore, it is important to assess and monitor the development of the disease.
A joint effusion leads to accumulation of fluid in the anterior recess of the capsule and consecutive widening of joint capsule (Fig. 15.18). Fluid within the joint will elevate the anterior part of capsule with bulging and widening of the joint space. Thus, the shape of the capsular margin becomes convex. One additionally needs to pay attention at the contour of the femoral head and the congruence between femoral head and neck—not to miss fragmentation or irregularities as seen in Perthes Disease, or step-off formation as in a slipped epiphysis (epiphysiolysis).
-
In simple, uncomplicated cases, a hypo-anechoic clear and uncomplicated effusion is present. The distance between femoral neck and the outer layer of the joint capsule exceeds 5 mm in children under 4 years and 7 mm over 8 years. Measurement should be taken perpendicular to the femoral neck at the vertex of the concavity. An intraindividual difference of >3 mm is judged as abnormal (Fig. 15.18a, b). It is notable that with high-resolution transducers a swelling and thickening of the synovial capsule can be depicted, but grading of the capsular thickness was shown as relatively little helpful. Furthermore, no obvious thickening needs to be present in such an inflammation and the capsule as well as the effusion itself can have varying echogenicity. The appearance is not specific and depends on the kind of inflammation, the age, the duration, the transducer used, etc.
 The measurement of joint distention and thus for quantification of the effusion is taken perpendicular to the femoral neck and includes the outer layer of the joint capsule. Particularly in persisting complaints, a hip radiograph is mandatory; however, it is often already taken at the first visit at the initial presentation of the patient.
The measurement of joint distention and thus for quantification of the effusion is taken perpendicular to the femoral neck and includes the outer layer of the joint capsule. Particularly in persisting complaints, a hip radiograph is mandatory; however, it is often already taken at the first visit at the initial presentation of the patient. -
In complicated cases, one may observe a hyperechoic joint effusion with echogenic particles—in a febrile and severely ill infant this is highly suspicious for septic/bacterial arthritis/coxitis (Figs. 15.18 and 15.19). The synovial reaction is highly sensitive, but lacks specificity. It may also reflect a haematoma/a haemarthros (e.g. in haemophilia, after trauma or in rheumatic conditions). The medical history (and laboratory biochemistry) is crucial and absolutely essential for differentiation. Colour Doppler sonography (CDS) may sometimes show hypervascularity of the potentially significant thickened synovial capsule layer (Fig. 15.19). If increased vascularity is depicted, spectral analysis may show diastolic hyperaemia unless joint pressure increases and diastolic perfusion is impaired. Particularly after long-standing and bacterial arthritis, defects may remain—with poor ossification of the femoral neck and defects in the convexity of the femoral head.
 The measurement of joint distention and thus for quantification of the effusion is taken perpendicular to the femoral neck and includes the outer layer of the joint capsule. Particularly in persisting complaints, a hip radiograph is mandatory; however, it is often already taken at the first visit at the initial presentation of the patient.
The measurement of joint distention and thus for quantification of the effusion is taken perpendicular to the femoral neck and includes the outer layer of the joint capsule. Particularly in persisting complaints, a hip radiograph is mandatory; however, it is often already taken at the first visit at the initial presentation of the patient.
Transient synovitis (a) Thickened synovial capsule and anechoic joint effusion (b) Split image. Note: Measurement perpendicular to the femoral neck includes outer layer of the joint capsule

(a) Power Doppler in septic arthritis: Note impressive hypervascularity of the thickened synovium, complex fluid in the widened joint space (b) massive synovial reaction, measurement (+....+) not useful in establishing diagnosis. Note: this is a sensitive, but unspecific sign
 The assessment of capsule-to-bone distance and the echogenicity of the intraarticular effusion do not permit a differentiation between viral, bacterial/septic, or even rheumatoid arthritis. That means simple effusion does not rule out bacterial/septic arthritis, and complicated effusion does not proof septic arthritis! Establishing a diagnosis solely by US is impossible and may bear the risk of incorrect results and thus delayed start of appropriate therapy. If there is any doubt, further examinations to rule out especially septic arthritis are required. This is usually achieved by clinical data, (possibly US-guided) arthrocentesis, and for some MRI.
The assessment of capsule-to-bone distance and the echogenicity of the intraarticular effusion do not permit a differentiation between viral, bacterial/septic, or even rheumatoid arthritis. That means simple effusion does not rule out bacterial/septic arthritis, and complicated effusion does not proof septic arthritis! Establishing a diagnosis solely by US is impossible and may bear the risk of incorrect results and thus delayed start of appropriate therapy. If there is any doubt, further examinations to rule out especially septic arthritis are required. This is usually achieved by clinical data, (possibly US-guided) arthrocentesis, and for some MRI.
 In particularly septic osteoarthritis of young infants, there may be distention and subsequent luxation and osseous defects. Luxation can be identified by applying DDH US techniques (e.g. using Graf’s criteria)—search for it!
In particularly septic osteoarthritis of young infants, there may be distention and subsequent luxation and osseous defects. Luxation can be identified by applying DDH US techniques (e.g. using Graf’s criteria)—search for it!
15.8.4 (Femoral Head) Epiphysiolysis/Slipped (Capital Femoral) Epiphysis
This is a rare condition. In infants US is judged to be superior to plain radiographs due to its higher sensitivity in detecting disruption of the neck-head continuity and without the restriction of poor ossification of the cartilaginous femoral head in infants, thus improving assessment. The same approach accounts for all other joints with a cartilaginous epiphysis (e.g. shoulder and elbow, namely in/after birth trauma) (Fig. 15.20). Nevertheless, a radiograph is compulsory in the initial assessment and for long-term follow-up.

(a) Ultrasound in haemarthrosis in a child with haemophilia. Note complex fluid representing acute haemorrhage. (b) Hip US in patient with juvenile rheumatoid arthritis. Proliferation of the synovial capsule, only sparse effusion
The US scanning is performed from the anterior approach in a sagittal plane, with the probe parallel to the femur. By this, longitudinal images of the joint should be obtained. In birth trauma, the displacement may occur in any direction, therefore US access from different directions and positions is recommended. Typical US findings are:
The continuity of the bone margin is disrupted at the level of the physis and produces a step-off phenomenon of the femoral head (or the epiphysis in other joints). The anechoic cartilage of the femoral head or the epiphysis (with or without a depictable ossification centre) is slipped off and displaced backwards. One millimetre displacement on US equals approximately 5° displacement on an axial radiograph.
-
Particularly in acute epiphysiolysis the complex joint fluid represents haemorrhagic components in the early phase. The surrounding soft tissues may show nonspecific secondary changes like oedema and subperiosteal bleeding—with elevation of the periosteum.
-
In the chronic form (epiphysiolysis capitis femoris lenta) less joint effusion is seen, which is usually hypoechoic, and often a thickened joint capsule is observed. Periosteal reaction can be noted only in the late stage.
US-guided reposition may be feasible in the neonate. If tolerated, dynamic assessment may reveal pathologic motion at the physis. The same criteria apply to epiphysiolysis of any other joint in neonates and infants (Fig. 15.21).

(a–b) Ultrasound in epiphysiolysis in a newborn after birth trauma. Note the discontinuity between ossified bone and hypoechoic cartilaginous epiphysis indicating dislocation of epiphysis. (c) Radiograph of a left hip with slipped capital femoral epiphysis; note the displacement of the epiphysis in relation to the femoral head
15.8.5 Perthes Disease
This condition is defined as an avascular necrosis of the femoral head of unclear aetiology and unknown origin. Twenty percent of affected children have a history of a transient synovitis of hip.
 In suspicion of Perthes Disease based on a persisting joint effusion, radiographs and (dynamic contrast-enhanced) MRI must be performed.
In suspicion of Perthes Disease based on a persisting joint effusion, radiographs and (dynamic contrast-enhanced) MRI must be performed.
US Findings and Staging
-
Grade I: Potentially only some joint effusion is seen—the contour of the femoral head is maintained. A slight asymmetric reduction of the height of the epiphysis as well as the femoral head on the affected side may be perceivable. These changes are subtle and not always seen on US.
-
Grade II (Fig. 15.22): Sonographically, an irregular disruption of the outer contour of the bony femoral head indicates fragmentation. There may be secondary effusion and capsular thickening.
-
Grade III and IV (Fig. 15.23): Due to reparative mechanisms, the femoral head becomes increasingly homogeneous, with significantly reduced femoral head height.

Ultrasound in Perthes disease. (a) Scattered epiphysis of femoral head in early Perthes disease (stage II). (b) Both hips imaged for comparison (split image technique)

(a) Ultrasound in Perthes disease. Scattered epiphysis of femoral head in early Perthes disease (stage IV). Both hips imaged for comparison (split image technique). Note the reduced height of affected left femoral head (Grade IV—US appearance varies with stage); additional imaging compulsory (radiograph and MRI). (b) Radiograph of the pelvis and hip in a patient with Perthes disease: note the condensed left femoral head, which however is still centred. (c) Contrast-enhanced MRI of the hips (coronal T1-weighted view with fat suppression after gadolinium application) in a patient with Perthes disease: note the asymmetric contrast uptake of the femoral head (different patients)
15.9 Summary and Take Away Message
It is has become important for all physicians caring of newborns and infants to have at least basic knowledge about the essentials of US examinations—not only for early diagnosis of musculoskeletal problems, but also for optimising treatment and to help to avoid unnecessary (radiation) burden to the patient. If done properly, US can support decision making in daily clinical setting and is therefore irreplaceable in daily routine. Therefore, it should be part in every education programme and integrated in the medical curriculum of health care professionals.
With respect to hip US, one needs to state that it has become the mainstay for DDH assessment, with different techniques throughout the world—in Europe the Graf method including dynamic assessment (or the modified Graf technique according to Rosendahl) is most often used, whereas in North America, the Harcke technique is also used. The indication varies too—some only perform US as a selected screening in risk patients, other countries have a well-established general screening programme. This is recommended particularly in regions with high DDH incidence. Whichever approach is chosen, one needs to remember that this US for DDH is a so-called final investigation: if one misses pathology, the patient will only come back after years or even decades with severe complaints and high morbidity, also causing high health care costs. As a missed pathology will have potentially disastrous implications, proper scanning technique and the skillful and prudent performance are mandatory by appropriately trained health professionals. The training should be offered in standardised and approved training programmes and taught by certified and approved trainers and instructors to avoid pitfalls and misinterpretation.
The absence of evidence does not necessarily mean the evidence of absence of benefit for the patient, even multicentre prospective double-blinded randomised controlled studies are lacking—therefore the author favours the general US screening approach even if some contradict.
Additionally, US has a high value in the early diagnosis of hip joint effusion and can help to differentiate the most common other pathologies in infants and children such as haemarthrosis, slipped capital epiphysis, and (traumatic) epiphysiolysis or septic coxitis.
This chapter guides through different US techniques in performing US of the hip, mainly focusing on DDH and the method according to Graf. It should help to understand the principles of hip US, address its importance particularly in endemic regions, discuss the indications, illustrate the respective findings, and briefly touch on pitfalls, therapeutic and prognostic implications, but does not replace studying textbooks and consulting current medical literature.
Further Reading
American Institute of Ultrasound in Medicine. AIUM practice guideline for the performance of an ultrasound examination for detection and assessment of developmental dysplasia of the hip. J Ultrasound Med. 2013;32:1307–17, update 2018. https://onlinelibrary.wiley.com/doi/10.1002/jum.14829
Barrera CA, Cohen SA, Sankar WN, et al. Imaging of developmental dysplasia of the hip: ultrasound, radiography and magnetic resonance imaging. Pediatr Radiol. 2019;49:1652–68.
Biedermann R, Eastwood DM. Universal or selective ultrasound screening for developmental dysplasia of the hip? A discussion of the key issues. J Child Orthop. 2018;12:296–301.
De Bruyn R. The musculoskeletal system. In: de Bruyn R, editor. Pediatric ultrasound how, why and when. 2nd ed. Amsterdam: Elsevier; 2010. p. 319–39.
Fröhlich S, Mittelmeier W. Hüftsonografie. In: Robel-Tillig E, editor. Pädiatrische Ultraschalldiagnostik. Ecomed-Storck GmbH; 2021. (In German).
Graf R. The diagnosis of congenital hip joint dislocation by ultrasound compound treatment. Arch Orthop Trauma Surg. 1980;97:117–33.
Graf R. Hip sonography: background; technique and common mistakes; results; debate and politics; challenges. Hip Int. 2017;27(3):215–9.
Graf R, Spiess T. Säuglingshüfte. In: Deeg K-H, Hofmann V, Hoyer PF, editors. Ultraschalldiagnostik in Pädiatrie und Kinderchirurgie. 4th ed; 2014. p. 1076–106. (In German).
Graf R, Lercher K, Baumgartner F, et al. Sonografie der Säuglingshüfte und therapeutische Konsequenzen (In German). 6th ed; 2010.
Graf R, Scott S, Farkas P, et al. Essentials of infant hip sonography according to Graf. Stolzalpe: Edition Stolzalpe Sonocenter; 2014.
Harcke HT. Hip ultrasonography in clinical practice. Pediatr Radiol. 2017;47:1155–9.
Hefti F. Kinderorthopädie. 3rd ed; 2015. p. 216–54; 301–9. (In German).
Merrow AC. Diagnostic imaging pediatrics. 3rd ed; 2017. p. 932–43.
O’Beirne JG, Chlapoutakis K, Alshryda S, et al. International Interdisciplinary Consensus Meeting on the evaluation of developmental dysplasia of the hip. Ultraschall Med. 2019;40:454–64.
OEGUM/DEGUM recommendation: www.OEGUM.at/content/view/506/210 download “Standarddokumentation der Sonografie der Neugeborenen- und Säuglingshüfte” (in German).
Riccabona M, Coley B, Schweintzger G. Small part and hip ultrasound. In: Riccabona M, editor. Pediatric ultrasound. 3rd ed; 2014. p. 397–414.
Rosendahl K, Toma P. Ultrasound in the diagnosis of developmental dysplasia of the hip in newborns. The European approach. A review of methods, accuracy and clinical validity. Eur Radiol. 2007;17:1960–7.
Schwarz Doria A, Babyn P. Arthritis and differential inflammatory joint disorders. In: Coley BD, editor. Caffey’s pediatric diagnostic imaging. 12th ed; 2013. p. 1444–88.
Schweintzger G. Hüftsonografie. In: Feldkamp A, Rech A, editors. Pädiatrische Ultraschalldiagnostik; 2010. (In German).
Schweintzger G. Hüftgelenksdysplasie und postnatales Hüftscreening. In: Hoffman G, Lentze MJ, Spranger J, et al., editors. Pädiatrie. 5th ed; 2020. p. 119–25. (In German).
Servaes S, et al. Developmental dysplasia of the hip. In: Coley BD, editor. Caffey’s pediatric diagnostic imaging. 12th ed; 2013. p. 1437–43.
Siegel MJ. Musculoskeletal system and vascular imaging. In: Siegel MJ, editor. Pediatric sonography. 4th ed; 2011. p. 602–46.
Teixeira SR, Dalto VF, Maranho DA, et al. Comparison between Graf method and pubo-femoral distance in neutral and flexion positions to diagnose developmental dysplasia of the hip. Eur J Radiol. 2015;84:301–6.
Thallinger C, Pospischill R, Ganger R, et al. Long term results of a nationwide general ultrasound screening system for developmental disorders of the hip: the Austrian hip screening Program. J Child Orthop. 2014;8:3–10.
Treguier C, Chapuis M, Branger B, et al. Pubo-femoral distance: an easy sonographic screening test to avoid late diagnosis of developmental dysplasia of the hip. Eur Radiol. 2013;23:836–44.
Tschauner C, Fürntrath F, Saba Y. Developmental dysplasia of the hip: impact of sonographic newborn hip screening on the outcome of early treated decentered hip joints—a single center retrospective comparative cohort study based on Graf’s method of hip ultrasonography. J Child Orthop. 2011;5:415–24.
von Kries R, Ihme N, Oberle D, et al. Effect of ultrasound screening on the rate of first operative procedures for developmental hip dysplasia in Germany. Lancet. 2003;362(9399):1883–7.
Waibel P, Maurer K. The pediatric musculoskeletal system. In: Riccabona M, editor. Pediatric imaging essentials. 1st ed; 2014. p. 229–68.
Yeh RW, Valsdottir LR, Yeh MW, et al. Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial. BMJ. 2018;363:k5094. https://doi.org/10.1136/bmj.k5094.
Acknowledgement
I would like to express my gratitude to my friend and academic teacher Prof. Dr. Reinhard Graf, Stolzalpe, Austria, for the permission to use schematic drawings from his manual, as well as text citations.
I furthermore like to thank Dr. Brian Coley, Cincinnati, Ohio, very much for editing the text and providing some images.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Schweintzger, G., Riccabona, M. (2023). Imaging the Neonatal (and Paediatric) Hip. In: Riccabona, M. (eds) Imaging in Neonates. Springer, Cham. https://doi.org/10.1007/978-3-031-15729-5_15
Download citation
DOI: https://doi.org/10.1007/978-3-031-15729-5_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-15728-8
Online ISBN: 978-3-031-15729-5
eBook Packages: MedicineMedicine (R0)