
Abstract
Cerebellar structure and function have intrigued investigators and clinicians for millennia. Major anatomic features were recognized early, and the role of the cerebellum in coordinating movements was established two centuries ago. Cerebellar involvement in nonmotor functions was described in clinical and experimental observations starting around the same time, but attention to their importance rose to the fore only recently. Functional localization was first derived from comparative morphology. Ablation degeneration and physiological studies in animals and neurological observations in patients with focal injury led to the lobular theory of organization. This was refined by delineation of the mediolateral parasagittal zonal organization of cerebellar connections. Histological studies date back to Cajal, with descriptions of additional neuronal elements and circuitry evolving over the years. Recognition of the cerebellar cognitive affective syndrome and the neuropsychiatry of the cerebellum, observations from connectional neuroanatomy, and advances in anatomic, task-based, and functional connectivity magnetic resonance neuroimaging provide contemporary support for the earliest notions that the cerebellum is engaged in a wide range of neurological functions. Together with new theories of cerebellar function, and elucidation of the genetic basis of inherited or sporadic ataxias and neurobehavioral disorders, the cerebellum has become increasingly relevant to contemporary clinical neurology and neuropsychiatry.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
The cerebellum has been recognized since antiquity. Notions regarding its functions included the belief that it imparted strength to the motor nerves (Galen A.D. 129/130–200/201), was a center for memory (Nemesius, c.A.D. 390, and Albert von Bollstädt/Albertus Magnus 1193–1280), controlled sensory functions including unconscious sensibility (Co(n)stanzo Varolio/Variolus 1543–1575), was involved with involuntary activity including the functions of the heart and respiration (Thomas Willis 1621–1675), and was the seat of amative love (Franz Joseph Gall 1758–1828) (Neuburger 1897/1981; Clarke and O’Malley 1996; Schmahmann and Pandya 2006). As is apparent from the historical account below, the conclusions of these pioneers, although based on flimsy or fanciful evidence, were rather prescient.
1 Early and Evolving Views of Cerebellar Organization and Function
Rolando (1809) first demonstrated that ablation of the cerebellum results in disturbances of posture and voluntary movement. Fodéra (1823) showed the release of postural mechanisms, and extensor hypotonia following acute cerebellar injury in pigeons, guinea pigs, and rabbits. Flourens (1824) showed in pigeons that the cerebellum is responsible for the coordination, rather than generation, of voluntary movement and gait, a concept that has remained the guiding principle of cerebellar function. François Magendie’s (1824) lesion studies led to the understanding that the cerebellum is essential for equilibrium. Disturbances of motor control following focal cerebellar lesions in monkeys were demonstrated by Luciani (1891), Ferrier and Turner (1893), and Russell (1894).
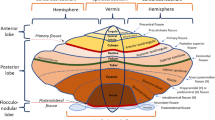
Comparative anatomists such as Lodewijk “Louis” Bolk (Bolk 1902; Glickstein and Voogd 1995) derived structure–function correlations by comparing the size of a cerebellar region with the characteristics of the species to which it belonged. They concluded that the vermis coordinates bilateral symmetrical movements, the cerebellar hemispheres coordinate unilateral movements of the limbs, and the development of manual dexterity corresponded with the expansion of the lateral cerebellar hemispheres. The lobular theory (Fulton and Dow 1937; Larsell 1970; Brodal 1967; see Angevine et al. 1961) held that the cerebellum is functionally organized into lobes. The flocculonodular lobe, archicerebellum, and vestibulocerebellum became synonymous. The anterior lobe, pyramis, and uvula in the vermis of the posterior lobe, and the paraflocculus were termed the paleocerebellum or spinocerebellum. The lateral parts of the cerebellar hemispheres and the middle portion of the vermis were termed the neocerebellum or pontocerebellum.
Ablation-degeneration studies in animals (Jansen and Brodal 1940; Chambers and Sprague 1955a, b) introduced the concept of the organization of the cerebellum into three bilaterally symmetrical longitudinal corticonuclear zones. These studies (see Dow and Moruzzi 1958 for review) showed that the medial zone (vermis and fastigial nucleus) regulates vestibular function and the tone, posture, locomotion, and equilibrium of the body, with somatotopic localization in the vermal cortex – the head, neck, and eyes at the posterior vermis, the tail and lower limbs at the rostral aspect of the anterior vermis, and the upper limbs situated in between. The intermediate zone (paravermal cortex and nucleus interpositus) regulates spatially organized and skilled movements and the tone and posture associated with these movements of the ipsilateral limb, and lesions in the intermediate zone produced motor deficits including tremor, ataxia, and postural instability. The lateral zone (hemispheral cortex and dentate nucleus) was thought to be involved in skilled and spatially organized movements of the ipsilateral limbs, although lateral hemispheres or dentate nucleus lesions produced only minor impairments of the distal extremities, without clear somatotopic organization. Dow (1942, 1974) identified the dentate nucleus in man and anthropoid apes as consisting of two parts, a dorsomedial microgyric, magnocellular older part homologous to the dentate nucleus of lower forms, and an expanded new part comprising the bulk of the dentate nucleus, the ventrolateral macrogyric parvicellular part. He postulated that the newer “neodentate” expanded in concert with, and was connected to, the frontal, temporal, and parietal association areas of higher primates and man, an idea he later expanded upon with Leiner et al. (1986).
The study of the cerebellar role in nonmotor functions has a rich history (see Schmahmann 1991, 1997a, b, 2010 for review and citations). Physiological and ablation studies demonstrated cerebellum to be engaged in autonomic functions such as pupil diameter, blood pressure, and sleep wake cycle. Cerebellar stimulation influenced the size of stroke following middle cerebral artery ligation in rats, produced generalized arousal of the electroencephalogram, evoked hyperactivity in monkeys and cats, and produced complex behaviors including grooming, predatory attack, aggression, and sham rage. Studies also showed the cerebellum to be essential for conditional associative learning including fear-conditioned bradycardia in the rat and the nictitating membrane response in rabbits, in addition to its role in spatial navigation and visual-spatial learning.
2 Cerebellar Cortex
Jan Evangelista Purkynĕ (1787–1869) described the cell that would come to bear his name (Purkinyě 1837), and Ramón y Cajal (1909) provided the first detailed description of the neuronal architecture of the cerebellar cortex, including mossy fibers, granule cell glomeruli, and parallel and climbing fibers (Eccles et al. 1967; Palay and Chan-Palay 1974; Brodal et al. 1975) (Fig. 2.1). Later investigators described Lugaro cells (Fox 1959; Palay and Chan-Palay 1974) and unipolar brush cells in the vestibulocerebellum (Mugnaini and Floris 1994). Using acetylcholinesterase, Voogd and colleagues (Voogd 1967, 1969; Marani and Voogd 1977) demonstrated parasagittal zonal organization in cerebellar white matter: zones A and B at the vermis, paravermal zones C1, 2, and 3, and zones D1 and 2 in the hemispheres. Hawkes and colleagues (Gravel and Hawkes 1990) demonstrated this zonal pattern in the cortex using monoclonal antibodies. Histochemical markers confirmed these parasagittal zones, each with topographically arranged connections with the deep cerebellar nuclei (Haines 1981) and inferior olive (Groenewegen and Voogd 1977; Hoddevik and Brodal 1977; Groenewegen et al. 1979). The demonstration of fractured somatotopy in sensory projections to cerebellum (Shambes et al. 1978; Bower and Kassel 1990) is consistent with the observation that Purkinje cells (PCs) can be activated by the ascending axons of granule cells (Llinas 1984; Cohen and Yarom 1998) as well as by beams of parallel fibers.

General organization of the cerebellar cortex. (a) Santiago Ramón y Cajal (1911/1995) diagram of the neurons in the cerebellar cortex-oriented perpendicular to the long axis of the folium, as well as fibers and glial cells. A molecular layer, a Purkinje cell, B granular layer, b basket cell, C white matter of the folium, d pericellular baskets around the PC soma formed by the basket cell axon, e superficial stellate cell, f Golgi cell, g granule cell, h mossy fiber, i ascending axon of granule cell, j Bergmann glial cell, m astroglial cell, n climbing fiber, o recurrent collateral branches of a PC. (b) Diagram redrawn from Eccles et al. (1967) in Gray’s Anatomy (1995). A single cerebellar folium is shown sectioned in its longitudinal axis (diagram right) and transversely (left). Purkinje cells are red; superficial and deep stellate, basket and Golgi cells are black; granule cells and ascending axons and parallel fibers are yellow; mossy and climbing fibers are blue. Also shown are the glomeruli with mossy fiber rosettes, claw-like dendrites of granule cells, and Golgi axons. Lugaro and unipolar brush cells are not shown (Figures reproduced with permission)
3 Connectional Anatomy
Myelin and degeneration studies in the nineteenth and early twentieth centuries revealed that cerebellar connections with spinal cord, vestibular system, brainstem, and cerebral cortex are topographically arranged. Bechterew (1888) showed that the caudal pons is linked with the cerebellar anterior lobe, but rostral pons is linked with the cerebellar posterior lobe. Sherrington’s (1906) physiological studies showed cerebellar afferents from the proprioceptive system (he viewed cerebellum as the “head ganglion of the proprioceptive system”), and others showed topographically arranged inputs to cerebellum following proprioceptive, cutaneous (Dow and Anderson 1942; Snider and Stowell 1942; Hampson et al. 1952) vagal, visual, and auditory stimulation (Snider and Stowell 1942; Dow and Moruzzi 1958).
Cerebellar somatotopy was subsequently confirmed in anatomical and physiological investigations of afferents to the cerebellum from the spinal cord (Chambers and Sprague 1955a, b; Grant 1962a, b; Oscarsson 1965), with spinocerebellar tracts terminating exclusively in the anterior lobe and lobule VIII (sensorimotor areas of cerebellum). Spinal-recipient olivary nuclei project to sensorimotor cerebellum (anterior lobe and lobule VIII), whereas most of the principal olive (devoid of spinal afferents) projects to the cerebellar posterior lobe (Oscarsson 1980; Ruigrok et al. 1992; Groenewegen et al. 1979).
Anatomical studies of the feedforward loop of the cerebrocerebellar system (Brodal 1978; Glickstein et al. 1985; see Schmahmann 2004), and electrophysiological experiments of the cerebrocerebellar system (Henneman et al. 1952; Sasaki et al. 1975; Allen and Tsukuhara 1974) demonstrated predominantly motor connections of cerebellum in a topographically precise manner. Studies also linked cerebellum with limbic structures – hippocampus, septum, and amygdala (Maiti and Snider 1975; Heath and Harper 1974), the hypothalamus (Haines et al. 1997), and the ventral tegmental area (Snider and Maiti 1976) that gives rise to the mesolimbic dopaminergic system critical for behavioral modulation (Carta et al. 2019). Anterograde isotope studies of corticopontine pathways demonstrated precisely arranged inputs from motor and supplementary motor areas (Schmahmann et al. 2004), and also from associative and paralimbic regions of the prefrontal, posterior parietal, superior temporal, and parastriate cortices concerned with higher order functions (Schmahmann and Pandya 1997a, 1997b; see Schmahmann 2010). Trans-synaptic viral tracing studies revealed that cerebellar linkage with association areas is reciprocal – cerebral areas that project via pons to cerebellum in turn receive projections back via thalamus from the cerebellum (Middleton and Strick 1994). They also showed that cerebellar anterior lobe and dorsal dentate nucleus are linked with motor cortices, whereas cerebellar posterior lobe and ventral dentate nucleus are linked with prefrontal and posterior parietal regions (Clower et al. 2001; Dum and Strick 2003).
4 The Cerebellar Motor Syndrome
Early studies in patients with Friedreich’s ataxia, cerebellar cortical atrophy, and penetrating gunshot injuries of the cerebellum (Brown 1892; Marie 1893; Babinski 1899; Holmes 1907) established the critical role of cerebellum in coordination of extremity movement, gait, posture, equilibrium, and speech. Holmes (1939) later analyzed the motor and speech deficits resulting from focal cerebellar injury. Much of Holmes’ terminology and neurologic examination remain in contemporary use (see Chap. 3). These clinical studies confirmed in human that the vestibular cerebellum was important for posture and equilibrium, the spinocerebellum for locomotion and extremity movement, and they suggested that the neocerebellum was important for manual dexterity. The anterior superior cerebellar vermis was particularly important for gait. Hypotonicity was a frequent accompaniment of bilateral cerebellar lesions. Lesions involving both cerebellar hemispheres produced characteristic cerebellar dysarthria. More than a century of clinical neurology has further refined the understanding of the cerebellar motor syndrome, and now clinical rating scales are helpful in defining the nature and severity of the motor incapacity.
5 The Cerebellar Cognitive Affective Syndrome
From the earliest days of clinical case reporting, at least since 1831 (Combette 1831), instances of mental and intellectual dysfunction were described in the setting of cerebellar pathology (Schmahmann 1991). Sizable posterior lobe strokes may produce only nausea and vertigo at the onset, and gait impairment subsides once the vestibular syndrome improves (Duncan et al. 1975; Schmahmann et al. 2009). Surgically induced dentate nucleus lesions in humans do not produce motor disability (Zervas et al. 1967). Cerebellar abnormalities have been identified in autism (Bauman and Kemper 1985), schizophrenia (Moriguchi 1981; Snider 1982), and attention-deficit disorder (Berquin et al. 1998). Cognitive impairments were noted in patients with cerebellar stroke (Botez-Marquard et al. 1994; Silveri et al. 1994), cerebellar cortical atrophy (Grafman et al. 1992), and in those with cerebellar developmental disorders (Joubert et al. 1969; see Schmahmann 1991, 1997a). The spinocerebellar ataxias have changes in cognition to varying degrees throughout the course of the illness (Manto 2014); and in children, mutism and subsequent dysarthria occur following excision of cerebellar tumors (Wisoff and Epstein 1984), often accompanied by regressive personality changes, emotional lability, and poor initiation of voluntary movement (Pollack et al. 1995; Levisohn et al. 2000; Gudrunardottir et al. 2016).
Schmahmann and Sherman (1998) described the cerebellar cognitive affective syndrome (CCAS) in patients with acquired cerebellar lesions characterized by impairment of executive functions such as planning, set-shifting, verbal fluency, abstract reasoning, and working memory; difficulties with spatial cognition including visual-spatial organization and memory; personality change with blunting of affect or disinhibited and inappropriate behavior; and language deficits including agrammatism and dysprosodia. The CCAS occurred following lesions of the cerebellar posterior lobe, and the vermis was usually involved when there was a prominent affective component. The CCAS was then described in children (Levisohn et al. 2000) with a similar pattern of cognitive deficits, the affective changes reflecting damage to the vermis, and it has been replicated widely (e.g., Neau et al. 2000; Riva and Giorgi 2000; Tedesco et al. 2011). Metalinguistic deficits (Guell et al. 2015) are related to impaired social cognition (Hoche et al. 2015), and neuropsychiatric symptoms occur in the domains of attention, mood, social cognition, autism, and psychosis spectrum behaviors (Schmahmann et al. 2007). It is now apparent that there is a double dissociation in the motor vs cognitive dichotomy of cerebellar clinical neurology. Holmes’ (1917) cerebellar motor syndrome of ataxia, dysmetria, and dysarthria arises following lesions of the sensorimotor anterior lobe but not the posterior lobe; the CCAS/Schmahmann syndrome (Manto and Mariën 2015) arises from the cognitive – affective posterior lobe, but not the anterior lobe (Schmahmann and Sherman 1998; Levisohn et al. 2000; Schmahmann et al. 2009). The cognitive and limbic consequences of cerebellar injury and the underlying neurobiology and theory of the putative cerebellar role in cognition were crystallized in the 1997 monograph on this topic (Schmahmann 1997b).
6 Atlases and Functional Neuroimaging
Vincenzo Malacarne provided the first detailed description of the cerebellum (Malacarne 1776), naming the vermis, lingula, and tonsil. The atlas of Vicq-d’Azyr (1786) showed the structure of the cerebellum. Depictions of cerebellum and brainstem were included in drawings by Franz Joseph Gall (Gall and Spurzheim 1810) and Herbert Mayo (1827), and in numerous volumes on cerebellum (Bolk 1906; Edinger 1909; Ingvar 1918; Riley 1929; Ziehen 1934; Larsell and Jansen 1972) (Fig. 2.2). The most detailed human atlas available was that of Angevine et al. (1961), until the introduction of the three-dimensional MRI Atlas of the Human Cerebellum (Schmahmann et al. 2000) for use with anatomic and functional neuroimaging. It depicted cerebellum in the three cardinal planes in Montreal Neurologic Institute stereotaxic space, included histological specimens with cerebellar nuclei, and revised Larsell’s nomenclature. This atlas facilitated the development of the on-line SUIT atlas (Diedrichsen 2006) for functional neuroimaging.

Depictions of the cerebellum by early anatomists. (a) Image from the atlas of Vicq-d’Azyr (1786). His Plate IV includes the cerebellum. The image is flipped vertically, as in the atlas the cerebellum is shown at the top. (b) Images from the atlas of Gall and Spurzheim (Gall and Spurzheim 1810). i Gall and Spurzheim’s Plate IV, shows the base of the brain with cerebral hemispheres, cerebellum and brainstem. ii Plate XIII, shows dissections of the cerebral hemisphere and cerebellum. iii Plate X shows cerebral and cerebellar hemispheres partially dissected in the sagittal plane. (c) Depictions of white matter dissections of the cerebral hemisphere, cerebellum, and brainstem by Mayo (1827). i Plate III shows dissection of the middle cerebellar peduncle. In ii Plate IV, brainstem and cerebellar dissection with removal of the MCP reveals the inferior and superior cerebellar peduncles
Magnetic resonance imaging (MRI) revolutionized the ability to visualize posterior fossa structures and lesions. Task-based functional MRI reliably shows cerebellar activation by motor (Fox et al. 1985) and nonmotor tasks (Petersen et al. 1989; Gao et al. 1996). The topography of functions in cerebellum is exemplified in fMRI meta-analyses and prospective studies showing areas of cerebellum dedicated to motor control, cognition, and emotion (Stoodley and Schmahmann 2009; Stoodley et al. 2012; Guell et al. 2018; King et al. 2019). Resting state functional connectivity MRI has added physiological connectivity evidence to the connectional data from non-human primates, showing functionally and anatomically distinct cerebrocerebellar circuits (Buckner et al. 2011; Habas et al. 2009; O’Reilly et al. 2010).
7 Theories
Snider (1952) proposed that cerebellum is the great modulator of neurologic function, and Heath (1977) regarded it as an emotional pacemaker for the brain. Gilbert and Thach (1977) confirmed the hypothesis of Marr (1969) and Albus (1971) that cerebellar climbing fibers and mossy fibers work in collaboration to facilitate a cerebellar role in motor learning. Ito used the model of the vestibular ocular reflex (Lisberger and Fuchs 1978) to suggest that the cerebellum engages in error correction in the realms both of movement (Ito 1984) and of thought (Ito 1993). Leiner et al. (1986) and Leiner and Leiner (1997) drew on evolutionary considerations of the dentate nucleus expanding in concert with cerebral association areas to propose that cerebellum serves as a multipurpose computer designed to smooth out performance of mental operations. Thach (1996) suggested that the cerebellum uses the mechanism of context-response linkage for motor adaptation, motor learning, and higher function. Llinas and Welsh (1993) highlighted the role of the olivocerebellar system in entraining cerebellar neuronal firing, focusing on the cerebellar role in movement. Other ideas include the view that the cerebellum is critical for timing (Ivry and Keele 1989), sensory perception (Bower 1995), anticipation and prediction (Courchesne and Allen 1997), and sequence learning (Molinari et al. 1997). Schmahmann’s dysmetria of thought theory (Schmahmann 1991, 2000, 2010) holds that there is a universal cerebellar transform that maintains function around a homeostatic baseline according to context; information being modulated is determined by topographically arranged anatomical circuits; the universal cerebellar impairment is dysmetria – resulting in the motor ataxia syndrome when the motor cerebellum is damaged, the CCAS when the cognitive-limbic cerebellum is damaged.
8 Evolving Techniques and Therapies
Walker (1938) showed that stimulation of the cerebellum alters electrical activity of the motor cortex. Cerebellar stimulation in patients produced amelioration of aggression (Heath 1977) and reduced the frequency of seizures (Riklan et al. 1974). The recognition of the cerebellar incorporation into the distributed neural circuits subserving cognition and emotion as well as motor control has opened the way to brain modulation using transcranial magnetic stimulation and transcranial direct current stimulation of the cerebellum. These approaches have been used to study cerebrocerebellar interactions in health (Hashimoto and Ohtsuka 1995; Schutter and van Honk 2006; Halko et al. 2014) and disease (e.g., Wessel et al. 1996; Brady Jr et al. 2019). They have also been used to treat motor and cognitive/emotional manifestations in individuals with cerebellar disorders, and to improve motor learning, stroke recovery, speech and language functions, and non-ataxic neuropsychiatric and movement disorders (Demirtas-Tatlidede et al. 2010; Grimaldi et al. 2014; Cattaneo et al. 2021; Manto et al. 2021). Magnetoencephalography (MEG) can record activity in the human cerebellum (Tesche and Karhu 1997) and provides a temporal dimension to the study of cerebellar circuitry and function.
Magnetic resonance spectroscopy (MRS) is sensitive to metabolic changes (Ross and Michaelis 1996), is abnormal in patients with cerebellar degeneration (Tedeschi et al. 1996), and together with morphometric studies of volumetric change may be useful as a biomarker of cerebellar dysfunction in the spinocerebellar and other ataxias (Őz et al. 2011, 2020). Diffusion tensor MRI (Takahashi et al. 2014) and optical coherence tomography (Liu et al. 2021) also now enable novel insights into cerebellar anatomy, connections, and disease.
Physical, occupational, and speech rehabilitation strategies have long been the mainstay of therapy for ataxia. Therapeutic nihilism has given way to the appreciation that many symptoms experienced by ataxia patients can be treated successfully with medications. Rest tremor, spasticity, camps, dystonia, neuropathic pain, dysphagia, urogenital symptoms, orthostasis, fatigue, mood and attention, among others symptoms, can all be effectively managed by repurposing medications from other neurological disorders, mandating that ataxia clinicians be more proactive in the care of these patients (Stephen et al. 2019; Perlman 2020). Medications are also being repurposed or newly developed for the treatment of kinetic ataxia that address the underlying molecular and physiological defects that produce cerebellar motor, cognitive, and other syndromes.
Since the discovery of the genetic basis of Friedreich’s ataxia (Campuzano et al. 1996), the understanding of autosomal dominant spinocerebellar ataxias and recessive ataxias has produced a paradigm shift in the care of patients and families with heritable cerebellar disorders. Exome sequencing and genome analysis have catapulted this further forward. Advances in understanding the genetics of the ataxias and the development of novel approaches to gene-related therapies such as the introduction of antisense oligonucleotides, modulation of downstream common pathway mechanisms, and direct implantation of genes using viral vectors (Ashizawa et al. 2018) hold out real promise for amelioration, cessation, and perhaps even prevention of the phenotypic manifestations of the genetic ataxias.
References
Albus JS (1971) A theory of cerebellar function. Math Biosci 10:25–61
Allen GI, Tsukuhara N (1974) Cerebrocerebellar communication systems. Physiol Rev 54:957–1008
Angevine JB, Mancall EL, Yakovlev PI (1961) The human cerebellum: an atlas of gross topography in serial sections. Little Brown and Company, Boston
Ashizawa T, Öz G, Paulson HL (2018) Spinocerebellar ataxias: prospects and challenges for therapy development. Nat Rev Neurol 14(10):590–605
Babinski JFF (1899) De l’asynergie cerebelleuse. Rev Neurol 7:806–816
Bauman M, Kemper TL (1985) Histoanatomic observations of the brain in early infantile autism. Neurology 35:866–874
Bechterew W (1888) Zur frage über die secundären degenerationen des hirnschenkels. Arch Psychiatr Nervenkr 19:1–17
Berquin PC, Giedd JN, Jacobsen LK, Hamburger SD, Krain AL, Rapoport JL, Castellanos FX (1998) Cerebellum in attention-deficit hyperactivity disorder: a morphometric MRI study. Neurology 50:1087–1093
Bolk L (1902) Hauptzüge der vergleichenden anatomie des cerebellums der säugetiere mit besonderer berüksichtigung des menschlichen kleinhirns. Monatschr f Psychiat Neurol 12:432–467
Bolk L (1906) Das cerebellum der säugetiere. De Erven F Bohn, Haarlem
Botez-Marquard T, Léveillé J, Botez MI (1994) Neuropsychological functioning in unilateral cerebellar damage. Can J Neurol Sci 21:353–357
Bower JM (1995) The cerebellum as sensory acquisition controller. Hum Brain Mapp 2:12–13
Bower JM, Kassel J (1990) Variability in tactile projection patterns to cerebellar folia crus IIA of the Norway rat. J Comp Neurol 302:768–778
Brady RO Jr, Gonsalvez I, Lee I et al (2019) Cerebellar-prefrontal network connectivity and negative symptoms in schizophrenia. Am J Psychiatry. 176(7):512–520
Brodal A (1967) Anatomical studies of cerebellar fibre connections with special reference to problems of functional localization. In: Schade JP (ed) The cerebellum, progress in brain research. Elsevier, Amsterdam, pp 135–173
Brodal P (1978) The corticopontine projection in the rhesus monkey. Origin and principles of organization. Brain 101(2):251–283
Brodal A, Walberg F, Hoddevik GH (1975) The olivocerebellar projection in the cat studied with the method of retrograde axonal transport of horseradish peroxidase. J Comp Neurol 164(4):449–469
Brown S (1892) On hereditary ataxia, with a series of twenty-one cases. Brain 15:250–282
Buckner RL, Krienen FM, Castellanos A, Diaz JC, Yeo BT (2011) The organization of the human cerebellum estimated by intrinsic functional connectivity. J Neurophysiol 106(5):2322–2345
Campuzano V, Montermini L, Moltò MD et al (1996) Friedreich’s ataxia: autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science 271(5254):1423–1427
Carta I, Chen CH, Schott AL, Dorizan S, Khodakhah K (2019) Cerebellar modulation of the reward circuitry and social behavior. Science 363(6424):eaav0581
Cattaneo Z, Ferrari C, Ciricugno A et al (2021) New horizons on non-invasive brain stimulation of the social and affective cerebellum. Cerebellum 21(3):482–496. https://doi.org/10.1007/s12311-021-01300-4
Chambers WW, Sprague JM (1955a) Functional localization in the cerebellum. I. Organization in longitudinal corticonuclear zones and their contribution to the control of posture, both extrapyramidal and pyramidal. J Comp Neurol 103:105–130
Chambers WW, Sprague JM (1955b) Functional localization in the cerebellum. II. Somatotopic organization in cortex and nuclei. Arch Neurol Psychiatr 74:653–780
Clarke E, O’Malley CD (1996) The human brain and spinal cord. A historical study illustrated by writings from antiquity to the twentieth century, 2nd edn. Norman Publishing, San Francisco
Clower DM, West RA, Lynch JC, Strick PL (2001) The inferior parietal lobule is the target of output from the superior colliculus, hippocampus, and cerebellum. J Neurosci 21(16):6283–6291
Cohen D, Yarom Y (1998) Patches of synchronized activity in the cerebellar cortex evoked by mossy-fiber stimulation: questioning the role of parallel fibers. Proc Natl Acad Sci U S A 95:15032–15036
Combette M (1831) Absence compléte du cervelet, des pedoncules posterieurs et de la protuberance cerebrale chez une jeune fille morte dans sa onziéme annee. Bull Soc Anat de Paris 5:148–157
Courchesne E, Allen G (1997) Prediction and preparation, fundamental functions of the cerebellum. Learn Mem 4(1):1–35
Demirtas-Tatlidede A, Freitas C, Cromer JR, Safar L, Ongur D, Stone WS, Seidman LJ, Schmahmann JD, Pascual-Leone A (2010) Safety and proof of principle study of cerebellar vermal theta burst stimulation in refractory schizophrenia. Schizophr Res 124(1–3):91–100
Diedrichsen J (2006) A spatially unbiased atlas template of the human cerebellum. Neuroimage 33(1):127–138
Dow RS (1942) The evolution and anatomy of the cerebellum. Biol Rev 17:179–220
Dow RS (1974) Some novel concepts of cerebellar physiology. Mt Sinai J Med 41:103–119
Dow RS, Anderson R (1942) Cerebellar action potentials in response to stimulation of proprioceptors and exteroceptors in the rat. J Neurophysiol 5:363–372
Dow RS, Moruzzi G (1958) The physiology and pathology of the cerebellum. University of Minnesota Press, Minneapolis
Dum RP, Strick PL (2003) An unfolded map of the cerebellar dentate nucleus and its projections to the cerebral cortex. J Neurophysiol 89(1):634–639
Duncan GW, Parker SW, Fisher CM (1975) Acute cerebellar infarction in the PICA territory. Arch Neurol 32(6):364–368
Eccles JC, Ito M, Szentagothai J (1967) The cerebellum as a neuronal machine. Springer, New York
Edinger L (1909) Uber die enteilung des cerebellums. Anat Anz 35:319–323
Ferrier D, Turner WA (1893) A record of experiments illustrative of the symptomatology and degenerations following lesions of the cerebellum and its peduncles and related structures in monkeys. Philos Trans R Soc B 185:719–778
Flourens P (1824) Recherches exprimentales sur les proprietes et les fonctions du systeme nerveux dons les animaux vertebres, 1st edn. Crevot, Paris
Fodéra M (1823) Recherches expérimentales sur le système nerveux. J Physiol Exp Pathol 3:191–217
Fox CA (1959) The intermediate cells of Lugaro in the cerebellar cortex of the monkey. J Comp Neurol 112:39–53
Fox PT, Raichle ME, Thach WT (1985) Functional mapping of the human cerebellum with positron emission tomography. Proc Natl Acad Sci U S A 82:7462–7466
Fulton JF, Dow RS (1937) The cerebellum: a summary of functional localization. Yale J Biol Med 10:89–119
Gall FJ, Spurzheim G (1810) Anatomie et physiologie du système nerveux en général, et du cerveau en particulier. Chez F. Schoell, Paris
Gao J-H, Parsons LM, Bower JM, Xiong J, Li J, Fox PT (1996) Cerebellum implicated in sensory acquisition and discrimination rather than motor control. Science 272:545–547
Gilbert PFC, Thach WT (1977) Purkinje cell activity during motor learning. Brain Res 128:309–328
Glickstein M, Voogd J (1995) Lodewijk Bolk and the comparative anatomy of the cerebellum. Trends Neurosci 18:206–210
Glickstein M, May JG 3rd, Mercier BE (1985) Corticopontine projection in the macaque: the distribution of labelled cortical cells after large injections of horseradish peroxidase in the pontine nuclei. J Comp Neurol 235(3):343–359
Grafman J, Litvan I, Massaquoi S, Stewart M, Sirigu A, Hallett M (1992) Cognitive planning deficit in patients with cerebellar atrophy. Neurology 42:1493–1496
Grant G (1962a) Spinal course and somatotopically localized termination of the spinocerebellar tracts. An experimental study in the cat. Acta Physiol Scand Suppl 56(193):1–61
Grant G (1962b) Projection of the external cuneate nucleus onto the cerebellum in the cat: an experimental study using silver methods. Exp Neurol 5:179–195
Gravel C, Hawkes R (1990) Parasagittal organization of the rat cerebellar cortex: direct comparison of Purkinje cell compartments and the organization of the spinocerebellar projection. J Comp Neurol 291:79–102
Grimaldi G, Argyropoulos GP, Boehringer A et al (2014) Non-invasive cerebellar stimulation—a consensus paper. Cerebellum 13(1):121–138
Groenewegen HJ, Voogd J (1977) The parasagittal zonation within the olivocerebellar projection. I. Climbing fiber distribution in the vermis of cat cerebellum. J Comp Neurol 174:417–488
Groenewegen HJ, Voogd J, Freedman SL (1979) The parasagittal zonation within the olivocerebellar projection: 2. Climbing fiber distribution in the intermediate and hemispheric parts of cat cerebellum. J Comp Neurol 183:551–602
Gudrunardottir T, Morgan AT, Lux AL et al (2016) Consensus paper on post-operative pediatric cerebellar mutism syndrome: the Iceland Delphi results. Childs Nerv Syst 32(7):1195–1203
Guell X, Hoche F, Schmahmann JD (2015) Metalinguistic deficits in patients with cerebellar dysfunction: empirical support for the dysmetria of thought theory. Cerebellum 14(1):50–58
Guell X, Gabrieli JDE, Schmahmann JD (2018) Triple representation of language, working memory, social and emotion processing in the cerebellum: convergent evidence from task and seed-based resting-state fMRI analyses in a single large cohort. Neuroimage 172:437–449
Habas C, Kamdar N, Nguyen D, Prater K, Beckmann CF, Menon V et al (2009) Distinct cerebellar contributions to intrinsic connectivity networks. J Neurosci 29(26):8586–8594
Haines DE (1981) Zones in the cerebellar cortex. Their organization and potential relevance to cerebellar stimulation. J Neurosurg 55:254–264
Haines DE, Dietrichs E, Mihailoff GA, McDonald EF (1997) The cerebellar-hypothalamic axis: basic circuits and clinical observations. Int Rev Neurobiol 41:83–107
Halko MA, Farzan F, Eldaief MC, Schmahmann JD, Pascual-Leone A (2014) Intermittent theta-burst stimulation of the lateral cerebellum increases functional connectivity of the default network. J Neurosci 34(36):12049–12056
Hampson JL, Harrison CR, Woolsey CN (1952) Cerebro-cerebellar projections and somatotopic localization of motor function in the cerebellum. Res Publ Assoc Nerv Ment Dis 30:299–316
Hashimoto M, Ohtsuka K (1995) Transcranial magnetic stimulation over the posterior cerebellum during visually guided saccades in man. Brain 118:1185–1193
Heath RG (1977) Modulation of emotion with a brain pacemaker. Treatment for intractable psychiatric illness. J Nerv Ment Dis 165:300–317
Heath RG, Harper JW (1974) Ascending projections of the cerebellar fastigial nucleus to the hippocampus, amygdala, and other temporal lobe sites: evoked potential and histological studies in monkeys and cats. Exp Neurol 45:2682–2687
Henneman E, Cooke PM, Snider RS (1952) Cerebellar projections to the cerebral cortex. Res Publ Ass Nerv Ment Dis 30:317–333
Hoche F, Guëll X, Sherman JC, Vangel MG, Schmahmann JD (2015) Cerebellar contribution to social cognition. Cerebellum 15(6):732–743
Hoddevik GH, Brodal A (1977) The olivocerebellar projection studied with the method of retrograde axonal transport of horseradish peroxidase. V. The projection to the flocculonodular lobe and the paraflocculus in the rabbit. J Comp Neurol 176:269–280
Holmes G (1907) A form of familial degeneration of the cerebellum. Brain 30:466–488
Holmes G (1917) The symptoms of acute cerebellar injuries due to gunshot wounds. Brain 40:461–535
Holmes G (1939) The cerebellum of man (Hughlings Jackson memorial lecture). Brain 62:1–30
Ingvar S (1918) Zur Phylo- und ontogenesae des kleinhirns. Folia Neuro-Biol 11:205–495
Ito M (1984) The cerebellum and neural control. Raven Press, New York
Ito M (1993) Movement and thought: identical control mechanisms by the cerebellum. Trends Neurosci 16:448–450
Ivry RB, Keele SW (1989) Timing functions of the cerebellum. J Cogn Neurosci 1:136–152
Jansen J, Brodal A (1940) Experimental studies on the intrinsic fibers of the cerebellum. II. The corticonuclear projection. J Comp Neurol 73:267–321
Joubert M, Eisenring JJ, Robb JP, Andermann F (1969) Familial agenesis of the cerebellar vermis. A syndrome of episodic hyperpnea, abnormal eye movements, ataxia, and retardation. Neurology 19:813–825
King M, Hernandez-Castillo CR, Poldrack RA, Ivry RB, Diedrichsen J (2019) Functional boundaries in the human cerebellum revealed by a multi-domain task battery. Nat Neurosci 22(8):1371–1378
Larsell O (1970) In: Jansen J (ed) The comparative anatomy and histology of the cerebellum from monotremes through apes. The University of Minnesota Press, Minneapolis
Larsell O, Jansen J (1972) The comparative anatomy and histology of the cerebellum. The human cerebellum, cerebellar connections, and cerebellar cortex. The University of Minnesota Press, Minneapolis
Leiner HC, Leiner AL (1997) How fibers subserve computing capabilities: similarities between brains and machines. Int Rev Neurobiol 41:535–553
Leiner HC, Leiner AL, Dow RS (1986) Does the cerebellum contribute to mental skills? Behav Neurosci 100:443–454
Levisohn L, Cronin-Golomb A, Schmahmann JD (2000) Neuropsychological consequences of cerebellar tumour resection in children: cerebellar cognitive affective syndrome in a paediatric population. Brain 123(Pt 5):1041–1050
Lisberger SG, Fuchs AF (1978) Role of primate flocculus during rapid behavioral modification of vestibulo-ocular reflex. I. Purkinje cell activity during visually guided horizontal smooth-pursuit eye movements and passive head rotation. J Neurophysiol 41:733–763
Liu CJ, Ammon W, Siless V et al (2021) Quantification of volumetric morphometry and optical property in the cortex of human cerebellum at micrometer resolution. Neuroimage 244:118627
Llinas R (1984) Functional significance of the basic cerebellar circuit in motor coordination. In: Bloedel JR (ed) Cerebellar functions. Springer, New York, pp 171–185
Llinas R, Welsh JP (1993) On the cerebellum and motor learning. Curr Opin Neurobiol 3:958–965
Luciani L (1891) Il cerbelletto: Nuovi studi di fisiologia normale e pathologica. Le Monnier, Firenze
Magendie F (1824) Mémoire sur les fonctions de quelques parties du système nerveux. J Physiol Exp Pathol 3:376–407
Maiti A, Snider RS (1975) Cerebellar control of basal forebrain seizures: amygdala and hippocampus. Epilepsia 16:521–533
Malacarne MVG (1776) Nuova esposizione della vera struttura del cerveletto umano. G M Briolo, Torino
Manto M (2014) Cognitive deficits in autosomal dominant ataxias: what did we learn? In: Koziol et al. (ed) Consensus paper: the cerebellum’s role in movement and cognition. Cerebellum 13(1):151–177
Manto M, Mariën P (2015) Schmahmann’s syndrome—identification of the third cornerstone of clinical ataxiology. Cerebellum Ataxias 2:2. https://doi.org/10.1186/s40673-015-0023-1
Manto M, Argyropoulos GPD, Bocci T et al (2021) Consensus paper: novel directions and next steps of non-invasive brain stimulation of the cerebellum in health and disease. Cerebellum 2021:1344. https://doi.org/10.1007/s12311-021-01344-6
Marani E, Voogd J (1977) An acetylcholinesterase band-pattern in the molecular layer of the cat cerebellum. J Anat 124:335–345
Marie P (1893) Sur l’hérédo-ataxie cérébelleuse. Sem Méd 13:444–447
Marr D (1969) A theory of cerebellar cortex. J Physiol 202:437–470
Mayo H (1827) A series of engravings intended to illustrate the structure of the brain and spinal cord in man. Burgess and Hill, London
Middleton FA, Strick PL (1994) Anatomical evidence for cerebellar and basal ganglia involvement in higher cognitive function. Science 266:458–461
Molinari M, Leggio MG, Solida A, Ciorra R, Misciagna S, Silveri MC et al (1997) Cerebellum and procedural learning: evidence from focal cerebellar lesions. Brain 120(Pt 10):1753–1762
Moriguchi I (1981) A study of schizophrenic brains by computerized tomography scans. Folia Psychiatr Neurol Jpn 35:55–72
Mugnaini E, Floris A (1994) The unipolar brush cell: a neglected neuron of the mammalian cerebellar cortex. J Comp Neurol 339(2):174–180
Neau JP, Arroyo-Anllo E, Bonnaud V, Ingrand P, Gil R (2000) Neuropsychological disturbances in cerebellar infarcts. Acta Neurol Scand 102(6):363–370
Neuburger M (1897–1981) Die historische Entwicklung der experimentellen Gehirn- und Rückenmarksphysiologie vor Flourens. Ferdinand Enke Verlag, Stuttgart. Translated and edited, with additional material, by Edwin Clarke. The Historical Development of Experimental Brain and Spinal cord Physiology before Flourens. Johns Hopkins University Press, Baltimore
O’Reilly JX, Beckmann CF, Tomassini V, Ramnani N, Johansen-Berg H (2010) Distinct and overlapping functional zones in the cerebellum defined by resting state functional connectivity. Cereb Cortex 20(4):953–965
Oscarsson O (1965) Functional organization of the spino- and cuneocerebellar tracts. Physiol Rev 45:495–522
Oscarsson O (1980) Functional organization of olivary projection to the cerebellar anterior lobe. In: Courville J, de Montigny C, Lamarre Y (eds) The inferior olivary nucleus: anatomy and physiology. Raven Press, New York, pp 279–289
Őz G, Iltis I, Hutter D, Thomas W, Bushara KO, Gomez CM (2011) Distinct neurochemical profiles of spinocerebellar ataxias 1, 2, 6, and cerebellar multiple system atrophy. Cerebellum 10(2):208–217
Öz G, Harding IH, Krahe J, Reetz K (2020) MR imaging and spectroscopy in degenerative ataxias: toward multimodal, multisite, multistage monitoring of neurodegeneration. Curr Opin Neurol 33(4):451–461
Palay SL, Chan-Palay V (1974) Cerebellar cortex. Springer, New York
Perlman SL (2020) Update on the treatment of ataxia: medication and emerging therapies. Neurotherapeutics 17(4):1660–1664
Petersen SE, Fox PT, Posner MI, Mintum MA, Raichle ME (1989) Positron emission tomographic studies of the processing of single words. J Cogn Neurosci 1:153–170
Pollack IF, Polinko P, Albright AL, Towbin R, Fitz C (1995) Mutism and pseudobulbar symptoms after resection of posterior fossa tumors in children: incidence and pathophysiology. Neurosurgery 37:885–893
Purkinyě JE (1837) Bericht die Versammlung deutscher Naturforscher und Ärzte in Prag im September. Anatomisch-physiologische Verhandlungen 5:3
Ramón y Cajal S (1909–1910) Histologie du système nerveux de l’homme et des vertébrés. Translated into French by L. Azoulay. Translated into English by Swanson N, Swanson LW (1995). Histology of the nervous system of man and vertebrates. New York, Oxford University Press. Maloine, Paris
Riklan M, Marisak I, Cooper IS (1974) Psychological studies of chronic cerebellar stimulation in man. In: Cooper IS, Riklan M, Snider RS (eds) The cerebellum epilepsy and behavior. Plenum Press, New York, pp 285–342
Riley HA (1929) The mammalian cerebellum. A comparative study of the arbor vitae and folial pattern. Res Publ Assoc Res Nerv Ment Dis 6:37–192
Riva D, Giorgi C (2000) The cerebellum contributes to higher functions during development: evidence from a series of children surgically treated for posterior fossa tumours. Brain 123(Pt 5):1051–1061
Rolando L (1809) Saggio sopra la vera struttura del cerbello dell’uome e degli animali e sopra le funzoini del sistema nervosa. Stampeia da S.S.R.M, Sassari
Ross B, Michaelis T (1996) MR spectroscopy of the brain: neurospectroscopy. In: Edelman RR, Hesselink JR, Zlatkin MB (eds) Clinical magnetic resonance imaging, 2nd edn. W.B. Saunders Co, Philadelphia, pp 928–981
Ruigrok TJ, Osse RJ, Voogd J (1992) Organization of inferior olivary projections to the flocculus and ventral paraflocculus of the rat cerebellum. J Comp Neurol 316:129–150
Russell JSR (1894) Experimental researches into the functions of the cerebellum. Philos Trans R Soc Lond B 185:819–861
Sasaki K, Oka H, Matsuda Y, Shimono T, Mizuno N (1975) Electrophysiological studies of the projections from the parietal association area to the cerebellar cortex. Exp Brain Res 23:91–102
Schmahmann J (1991) An emerging concept. The cerebellar contribution to higher function. Arch Neurol 48(11):1178–1187
Schmahmann JD (1997a) Rediscovery of an early concept. Int Rev Neurobiol 41:3–27
Schmahmann JD (1997b) The cerebellum and cognition. Int Rev Neurobiol 41:3–27
Schmahmann JD (2000) The role of the cerebellum in affect and psychosis. J Neurolinguist 13:189–214
Schmahmann JD (2004) Disorders of the cerebellum: ataxia, dysmetria of thought, and the cerebellar cognitive affective syndrome. J Neuropsychiatry Clin Neurosci 16(3):367–378
Schmahmann JD (2010) The role of the cerebellum in cognition and emotion: personal reflections since 1982 on the dysmetria of thought hypothesis, and its historical evolution from theory to therapy. Neuropsychol Rev 20(3):236–260
Schmahmann JD, Pandya DN (1997a) Anatomic organization of the basilar pontine projections from prefrontal cortices in rhesus monkey. J Neurosci 17:438–458
Schmahmann JD, Pandya DN (1997b) The cerebrocerebellar system. Int Rev Neurobiol 41:31–60
Schmahmann JD, Pandya DN (2006) Fiber pathways of the brain. Oxford University Press, New York
Schmahmann JD, Sherman JC (1998) The cerebellar cognitive affective syndrome. Brain 121(Pt 4):561–579
Schmahmann JD, Doyon J, Toga A, Evans A, Petrides M (2000) MRI atlas of the human cerebellum. Academic Press, San Diego
Schmahmann JD, Rosene DL, Pandya DN (2004) Motor projections to the basis pontis in rhesus monkey. J Comp Neurol 478(3):248–268
Schmahmann JD, Weilburg JB, Sherman JC (2007) The neuropsychiatry of the cerebellum—insights from the clinic. Cerebellum 6(3):254–267
Schmahmann JD, MacMore J, Vangel M (2009) Cerebellar stroke without motor deficit: clinical evidence for motor and non-motor domains within the human cerebellum. Neuroscience 162(3):852–861
Schutter DJ, van Honk J (2006) An electrophysiological link between the cerebellum, cognition and emotion: frontal theta EEG activity to single-pulse cerebellar TMS. Neuroimage 33(4):1227–1231
Shambes G, Gibson M, Welker W (1978) Fractured somatotopy in granule cell tactile areas of rat cerebellar hemispheres revealed by micromapping. Brain Behav Evol 15:94–140
Sherrington C (1906) The integrative action of the nervous system. Yale University Press, New Haven
Silveri MC, Leggio MG, Molinari M (1994) The cerebellum contributes to linguistic production: a case of agrammatic speech following a right cerebellar lesion. Neurology 44:2047–2050
Snider RS (1952) Interrelations of cerebellum and brainstem. Res Publ Assoc Nerv Ment Dis 30:267–281
Snider RS (1982) Cerebellar pathology in schizophrenia—cause or consequence? Neurosci Behav Rev 6:47–53
Snider RS, Maiti A (1976) Cerebellar contributions to the Papez circuit. J Neurosci Res 2(2):133–146
Snider RS, Stowell A (1942) Evidence of tactile sensibility in the cerebellum of the cat. Fed Proc 1:82
Stephen CD, Brizzi KT, Bouffard MA et al (2019) The comprehensive management of cerebellar ataxia in adults. Curr Treat Options Neurol 21(3):9
Stoodley CJ, Schmahmann JD (2009) Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuroimage 44(2):489–501
Stoodley CJ, Valera EM, Schmahmann JD (2012) Functional topography of the cerebellum for motor and cognitive tasks: an fMRI study. Neuroimage 59(2):1560–1570
Takahashi E, Hayashi E, Schmahmann JD, Grant PE (2014) Development of cerebellar connectivity in human fetal brains revealed by high angular resolution diffusion tractography. Neuroimage 96:326–333
Tedeschi G, Bertolino A, Massaquoi SG, Campbell G, Patronas NJ, Bonavita S et al (1996) Proton magnetic resonance spectroscopic imaging in patients with cerebellar degeneration. Ann Neurol 39:71–78
Tedesco AM, Chiricozzi FR, Clausi S, Lupo M, Molinari M, Leggio MG (2011) The cerebellar cognitive profile. Brain 134(Pt 12):3672–3686
Tesche CD, Karhu J (1997) Somatosensory evoked magnetic fields arising from sources in the human cerebellum. Brain Res 744:23–31
Thach WT (1996) On the specific role of the cerebellum in motor learning and cognition: clues from PET activation and lesion studies in man. Behav Brain Sci 19:411–433
Vicq-d’Azyr F (1786) Traité d’ anatomie et de physiologie, avec des planches coloriées: Tome premier. Francois Ambrose Didot l’aîné, Paris
Voogd J (1967) Comparative aspects of the structure and fibre connexions of the mammalian cerebellum. In: Fox CA, Snider RS (eds) The cerebellum, vol 25: progress in brain research. Elsevier, Amsterdam, pp 94–135
Voogd J (1969) The importance of fiber connections in the comparative anatomy of the mammalian cerebellum. In: Palay SL, Chan-Palay V (eds) Neurobiology of cerebellar evolution and development. Springer, Berlin, pp 134–161
Walker AE (1938) An oscillographic study of the cerebello–cerebral relationships. J Neurophysiol 1:16–23
Wessel K, Tegenthoff M, Vorgerd M, Otto V, Nitschke MF, Malin JP (1996) Enhancement of inhibitory mechanisms in the motor cortex of patients with cerebellar degeneration: a study with transcranial magnetic brain stimulation. Electroencephalogr Clin Neurophysiol 101:273–280
Wisoff JH, Epstein FJ (1984) Pseudobulbar palsy after posterior fossa operation in children. Neurosurgery 15(5):707–709
Zervas NT, Hoerner GG, Gordy PD (1967) Cerebellar dentatectomy in primates and humans. Trans Am Neurol Assoc 92:27–30
Ziehen T (1934) Central nerves system. Handbuch der anatomie. Verlag von Gustav Fischer, Jena
Acknowledgements
Supported in part by the National Ataxia Foundation, the MINDlink foundation, and Mary Jo Reston. The images in Figs. 2.1 and 2.2 were acquired in the Harvard Medical School Countway Library of Medicine Rare Books and Special Collections Department, and are reproduced from Schmahmann and Pandya (2006).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Schmahmann, J.D. (2023). A Brief History of the Cerebellum. In: Gruol, D.L., Koibuchi, N., Manto, M., Molinari, M., Schmahmann, J.D., Shen, Y. (eds) Essentials of Cerebellum and Cerebellar Disorders. Springer, Cham. https://doi.org/10.1007/978-3-031-15070-8_2
Download citation
DOI: https://doi.org/10.1007/978-3-031-15070-8_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-15069-2
Online ISBN: 978-3-031-15070-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)