
Abstract
Diffuse pulmonary lymphangiomatosis (DPL) is a rare, often fatal condition characterized by extensive proliferation of lymphatic vessels throughout the lungs. This condition typically manifests in young adults, with a broad spectrum of clinical findings, ranging from dyspnea and cough to chylothorax and severe respiratory failure. From a clinical standpoint, these findings significantly overlap with lymphangiomyomatosis (LAM), another rare condition with predilection for women of reproductive age. From an imaging perspective, the findings in DPL and LAM are useful to differentiate these two entities, with the form being characterized by septal and peribronchovascular thickening, following the pattern of lymphatic proliferation, while LAM is typically characterized by cystic lung disease. Histologically, DPL consists of anastomosing lymphatic vessels of varying caliber following a lymphangitic distribution. Although the lesions in LAM tend to follow a similar anatomic distribution, they typically contain a proliferation of myoid perivascular epithelioid cells (PEC), which express HMB-45 and/or hormone receptors. Another important consideration in the diagnosis of DPL includes other lymphatic vascular abnormalities, such as lymphangiectasia and solitary lymphangiomas; the distinction between DPL and these lesions may be difficult in small biopsies and requires correlation with clinical and imaging findings.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Case Presentation
A 26-year-old woman presented to the emergency room after a motor vehicle collision. Chest computed tomography (CT) performed at that time demonstrated a large pleural effusion, associated with a right upper lobe mass. A wedge excision and pleural decortication demonstrated multiple subpleural and septal lesions composed of prominent, variably dilated and anastomosing lymphatic channels, associated with fibrosis and patchy lymphocytic infiltrates.
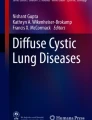
On follow-up, the patient had progressive dyspnea associated with restrictive lung disease. Chest CT studies demonstrated bilateral ground-glass opacities, septal and pleural thickening, and recurrent chylous pleural and pericardial effusions (Fig. 59.1). Four years after the initial diagnosis, the patient had a pregnancy during which her pulmonary function severely deteriorated, requiring a cesarean section at 29 weeks. Postoperatively, her respiratory status continued to worsen, ultimately leading to respiratory failure and death.

CT imaging findings of diffuse pulmonary lymphangiomatosis commonly include extensive peribronchial/perivascular thickening, scattered ground-glass opacities, and pleural and pericardial effusion. (a) Axial view; (b) coronal view
Autopsy revealed markedly enlarged lungs bilaterally, with extensive areas of pleural scarring. Other findings included marked ascites and additional lesions composed of similarly arranged lymphatic vessels involving the lungs (Fig. 59.2a–c), as well as the mediastinal and retroperitoneal soft tissues (Fig. 59.2d).

(a, b) Histologic features of diffuse pulmonary lymphangiomatosis include multiple lesions composed of variably dilated lymphatics with a lymphangitic distribution, accompanied by fibrosis and variable lymphocytic aggregates (H&E, 40×). (c) The lesional vessels are lined by cytologically bland lymphatic endothelium (H&E, 200×). (d) Extrapulmonary lesions may be seen in DPL; in this particular case in the retroperitoneum, it is associated with lymph nodes (H&E, 40×)
Her cause of death was attributed to respiratory failure due to diffuse pulmonary lymphangiomatosis.
Final Diagnosis: Diffuse Pulmonary Lymphangiomatosis
What Are the Clinical Features of Diffuse Pulmonary Lymphangiomatosis (DPL) and How Do They Differ from Lymphangioleiomyomatosis (LAM)?
Diffuse pulmonary lymphangiomatosis (DPL) is a rare condition characterized by diffuse prominence of lymphatic vessels within the lung parenchyma (lymphangiomas) [1]. It typically arises in children and young adults, with no significant difference between sexes [1, 2]. Rare cases of DPL have been reported in middle-aged adults [3, 4]. DPL is a typically aggressive disease which presents with a wide variety of clinical manifestations; these range from mild wheezing and productive cough to severe respiratory failure associated with infiltrative disease and recurrent pleural effusions [1]. The content of the expectoration and pleural effusion are often chylous [1, 2]. DPL is often associated with other lymphatic abnormalities and involvement of other organs in up to 75% of cases [5]. The clinical prognosis of DPL is poor, and death by respiratory failure is common [2, 6, 7].
On the other hand, LAM shows a marked preference for women of reproductive age. Somewhat similarly to DPL, LAM typically presents with dyspnea, spontaneous pneumothorax, and ultimately respiratory failure. Involvement of venous and lymphatic vessels can lead to other less common clinical manifestations, such as hemoptysis, pulmonary hypertension, and chylothorax [8,9,10]. This entity is also discussed in Chap. 58 (Lymphangioleiomyomatosis versus Benign Metastasizing Leiomyoma).
How Can Radiologic Studies be Used to Distinguish DPL from LAM?
The most common radiologic manifestations of DPL are distinctive, although not entirely specific. The most CT findings are smooth septal and peribronchovascular thickening and diffusely increased attenuation of mediastinal fat. Other common findings include bilateral patchy ground-glass opacities, pleural and pericardial effusion, pleural thickening, and lymphadenopathy [6, 11]. Representative CT images are seen in Fig. 59.1.
In contrast, the CT imaging appearance of LAM typically consists of multiple air-filled cysts of variable size, distributed throughout the entirety of the lung parenchyma (Fig. 59.3). Other common pulmonary findings include reticulated opacities, pneumothorax, increased lung volumes, and pleural effusions [12,13,14].

CT imaging findings of lymphangioleiomyomatosis are typically characterized by the variable presence of thin-walled pulmonary cysts, without a predilection for a specific region, and often distributed in a homogeneous manner throughout the lungs. (a) Axial view; (b) coronal view
What Are the Pathologic Features of DPL and LAM? How Can Immunohistochemistry be Used to Distinguish These Two Entities?
DPL is histologically characterized by the presence of complex anastomosing thin-walled lymphatic vessels, which are present throughout the lung parenchyma and pleura, with a subpleural, septal, and peribronchovascular distribution (Fig. 59.2a, b). The lesional vessels are lined by cytologically bland endothelial cells (Fig. 59.2c) and may be associated with fibrosis and increased hemosiderin-laden macrophages. True infiltration of the lung parenchyma is usually not seen in DPL [5, 7, 15].
On the other hand, LAM is characterized by the presence of solid nodules or multiple cysts throughout the lung parenchyma, lined by cytologically bland spindled to epithelioid perivascular cells (PEC) (Fig. 59.4). These lesions show a similar anatomic distribution to lymphangiomatosis, given their close association with lymphatic structures, with a peribronchial, septal, and subpleural location [8, 16].

Histologic findings in LAM. (a) Notice the presence of myoid cells within the cyst lining (H&E, 100×), which show focal expression of (b) HMB-45 and (c) variable progesterone receptor (PR) (IHC DAB, 100×)
Immunohistochemical stains can be useful to further differentiate DPL from LAM, since the latter has a characteristic immunophenotype, with expression of smooth muscle actin, HMB45 (Fig. 59.4), and estrogen and progesterone receptors (Fig. 59.4) (PR more commonly than ER) in a majority of cases [17,18,19]. In addition, immunoreactivity for β-catenin in a membranous and cytoplasmic pattern has been described in a majority of cases of LAM [17].
What Other Lesions Should I Consider in the Differential Diagnosis of DPL?
Other lymphatic vascular lesions may be histologically difficult to distinguish from DPL. These include solitary lymphangiomas and lymphangiectasis. The former consist of solitary, typically well-circumscribed lesions composed of abundant lymphatic vessels, lined by cytologically bland endothelial cells, and containing lymph within their lumen. These lesions may be solid or cystic, with capillary and/or cavernous architecture, and are commonly associated with prominent lymphoid aggregates [5]. In small biopsies, and in the absence of clinical and imaging correlation, these lesions may be histologically indistinguishable from DPL.
References
Kadakia KC, Patel SM, Yi ES, Limper AH. Diffuse pulmonary lymphangiomatosis. Can Respir J. 2013;20(1):52–4.
Ernotte C, Medart L, Collignon L. Diffuse pulmonary lymphangiomatosis. J Belg Soc Radiol. 2018;102(1):64.
Lim HJ, Han J, Kim HK, Kim TS. A rare case of diffuse pulmonary lymphangiomatosis in a middle-aged woman. Korean J Radiol. 2014;15(2):295–9.
El Hajj L, Mazieres J, Rouquette I, Mittaine M, Bolduc JP, Didier A, et al. Diagnostic value of bronchoscopy, CT and transbronchial biopsies in diffuse pulmonary lymphangiomatosis: case report and review of the literature. Clin Radiol. 2005;60(8):921–5.
Faul JL, Berry GJ, Colby TV, Ruoss SJ, Walter MB, Rosen GD, et al. Thoracic lymphangiomas, lymphangiectasis, lymphangiomatosis, and lymphatic dysplasia syndrome. Am J Respir Crit Care Med. 2000;161(3 Pt 1):1037–46.
Swensen SJ, Hartman TE, Mayo JR, Colby TV, Tazelaar HD, Muller NL. Diffuse pulmonary lymphangiomatosis: CT findings. J Comput Assist Tomogr. 1995;19(3):348–52.
Zhao J, Wu R, Gu Y. Pathology analysis of a rare case of diffuse pulmonary lymphangiomatosis. Ann Transl Med. 2016;4(6):114.
Johnson SR, Taveira-DaSilva AM, Moss J. Lymphangioleiomyomatosis. Clin Chest Med. 2016;37(3):389–403.
Moir LM. Lymphangioleiomyomatosis: current understanding and potential treatments. Pharmacol Ther. 2016;158:114–24.
Taylor JR, Ryu J, Colby TV, Raffin TA. Lymphangioleiomyomatosis. Clinical course in 32 patients. N Engl J Med. 1990;323(18):1254–60.
Yekeler E, Dursun M, Yildirim A, Tunaci M. Diffuse pulmonary lymphangiomatosis: imaging findings. Diagn Interv Radiol. 2005;11(1):31–4.
Ferrans VJ, Yu ZX, Nelson WK, Valencia JC, Tatsuguchi A, Avila NA, et al. Lymphangioleiomyomatosis (LAM): a review of clinical and morphological features. J Nippon Med Sch. 2000;67(5):311–29.
Pallisa E, Sanz P, Roman A, Majo J, Andreu J, Caceres J. Lymphangioleiomyomatosis: pulmonary and abdominal findings with pathologic correlation. Radiographics. 2002;22:S185–98.
Abbott GF, Rosado-de-Christenson ML, Frazier AA, Franks TJ, Pugatch RD, Galvin JR. From the archives of the AFIP: lymphangioleiomyomatosis: radiologic-pathologic correlation. Radiographics. 2005;25(3):803–28.
Tazelaar HD, Kerr D, Yousem SA, Saldana MJ, Langston C, Colby TV. Diffuse pulmonary lymphangiomatosis. Hum Pathol. 1993;24(12):1313–22.
Thway K, Fisher C. PEComa: morphology and genetics of a complex tumor family. Ann Diagn Pathol. 2015;19(5):359–68.
Flavin RJ, Cook J, Fiorentino M, Bailey D, Brown M, Loda MF. Beta-catenin is a useful adjunct immunohistochemical marker for the diagnosis of pulmonary lymphangioleiomyomatosis. Am J Clin Pathol. 2011;135(5):776–82.
Grzegorek I, Lenze D, Chabowski M, Janczak D, Szolkowska M, Langfort R, et al. Immunohistochemical evaluation of pulmonary lymphangioleiomyomatosis. Anticancer Res. 2015;35(6):3353–60.
Gao L, Yue MM, Davis J, Hyjek E, Schuger L. In pulmonary lymphangioleiomyomatosis expression of progesterone receptor is frequently higher than that of estrogen receptor. Virchows Arch. 2014;464(4):495–503.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Mantilla, J.G. (2022). Diffuse Pulmonary Lymphangiomatosis Versus Lymphangioleiomyomatosis. In: Xu, H., Ricciotti, R.W., Mantilla, J.G. (eds) Practical Lung Pathology. Practical Anatomic Pathology. Springer, Cham. https://doi.org/10.1007/978-3-031-14402-8_59
Download citation
DOI: https://doi.org/10.1007/978-3-031-14402-8_59
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-14401-1
Online ISBN: 978-3-031-14402-8
eBook Packages: MedicineMedicine (R0)