
Abstract
Fractures of the extremities are the most common fractures in infancy and childhood, they often occur accidentally making it sometimes difficult to discriminate them from inflicted trauma. In this chapter fractures of both the upper and lower extremity, the epidemiology, the trauma mechanisms, and the differential diagnoses are discussed. The fractures are placed in a clinical and forensic perspective.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Fractures of diaphysis
- Metaphyseal corner fractures
- Salter-Harris fractures
- Fractures of the upper extremities
- Fractures of the lower extremities
- Cause and manner of the fractures of upper and lower extremities
- Epidemiology
- Differential diagnosis
- Growth arrest lines
12.1 General Aspects of Fractures of the Extremities
The bones of the extremities can be categorized according to their shape in long and short bones. Long bones are found in the arms (humerus, radius, ulna), fingers (metacarpals, phalanges), legs (femur, tibia, fibula), and toes (metatarsals, phalanges). The carpals of the wrists and the tarsals of the ankles are short bones (see Sect. 2.4.1.2). Irrespective of their anatomical location, long bones always consist of (Figs. 12.1 and 12.2a–c):
-
Physis: Growth plate.
-
Diaphysis: The shaft; the medulla-containing tubular middle part of a long bone.
-
Epiphysis: The wider parts at both ends of a long bone.
-
Metaphysis: A narrow area between the diaphysis and the epiphysis.

Schematic representation of the anatomy of the long bones

(a) Histological section of the distal femur of a 3-month-old neonate, which shows ossification of the distal epiphysis of the femur (asterisk). (b) Corresponding specimen photo of the distal femur, showing ossification of the epiphysis of the distal femur. (c) Corresponding radiograph of the distal femur, showing ossification of the epiphysis of the distal femur
From an anatomical, physiological, and biomechanical perspective, the skeleton, especially of the extremities, of young children differs from the adult skeleton. Depending on the characteristics of the force of impact, specific fractures will occur in children in specific parts of the long and short bones of the extremities.
12.2 Fractures of the Diaphysis
12.2.1 Cause of Fractures of the Diaphysis
A number of aspects should be considered in the analysis of what long bones are exposed to in either daily life or under the impact of force. These concern:
-
The force or combination of forces exerted on the bone in day-to-day use and when under the impact of force: the load bearing of the bone (‘load’).
-
The force of the bone to resist this load (‘stress’).
-
The changes in shape or size of tissue in reaction to this stress (‘stretch/strain’).
When a fracture is sustained, the three pure forms (load, stress, strain) seldom occur just by themselves, but nearly always a combination of the three is seen (Table 12.1). Three pure forms of strain can be distinguished: compression, tension, and shearing:
-
Compression: Compression is defined as a perpendicular force that affects a surface in such a manner that it compresses the object. Bone has great resistance to this kind of force. When a fracture is caused by compression, it is usually because the compression is not quite along the central axis of the bone [1]. In such cases, compression will cause the bone to bow, which results in tension on one side, which ultimately determines the nature of the fracture.
-
Tension: Tension is defined as a perpendicular force that affects a surface in such a manner that it pulls an object apart. Bone is less resistant to tension than to compression. In tension the bone is stretched out like a spring: it becomes longer and thinner. Tension exerted on a bone for a limited period of time does not necessarily lead to a fracture. In normal cases it will fully recover; however, as soon as the limit of the elasticity of the bone is exceeded, damage is inflicted. This damage is not necessarily visible on radiographs. Only in cases with prolonged or stronger tension, a fracture will become visible. The fracture line will follow the contours of the weakest areas of the bone, which sometimes causes the fracture to have a zigzag line.
-
Shearing: Shearing is physically equal to compression and tension, but the force is exerted in such a manner that the tissue is distorted and deformed. Bone is not very resistant to shearing.
Furthermore, various combinations may be seen, such as bowing and torque:
-
Bowing: Bowing is caused by a force that causes tension on one side (the convex side) and compression on the opposite side (the concave side). In bowing, the cortex on the tension side will usually be damaged first. When this happens, and the loading stops, it will result in a so-called ‘greenstick fracture’ (Fig. 12.3). When the loading does not stop, the fracture will spread. The most classical expression of this type of loading is the transverse fracture. Depending on the type of bone and the additional forces exerted, other types of fractures may occur. In immature bone, the bone may also yield on the compression side first, which may lead to a buckle fracture (torus fracture) of the compression side (Fig. 12.4).
-
Torque: Torque is the result of forces rotating an object along the longitudinal axis, when the other side is stationary or turned in the opposite direction. When the torque forces are directed to the left, it will cause a spiral fracture that turns to the right, and the other way around (Fig. 12.5).

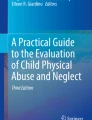
Sixteen-year-old boy who had a painful wrist after romping around with his brother. The lateral side of the distal ulna shows a greenstick fracture (open arrow)

Three-year-old boy with a torus fracture of metatarsal I of the right foot after taking a jump (open arrow)

Spiral fracture of the tibia in an infant as a result of a spoke wheel injury
The growing bone in children reacts differently to subjected forces than the fully developed bone in adults. The presence of larger and more extensive Haversian canals together with increased elasticity make the child’s bone more malleable than adult bone. Consequently, immature bone (in particular the diaphysis of the long bones) can deform more during bending than adult bone without breaking. Finally, the periosteum in children is thicker, stronger, and less firmly attached to the (diaphyseal) bone. It is less frequently torn after trauma and, likewise, can act as a stabilizing factor in case of a fracture. This means that in children specific types of fracture of the shaft are found that are typical for growing bone. This concerns in particular the so-called incomplete fractures:
-
‘Buckle’ fracture or torus fracture (damage to the cortex at the compression side of the bend): In axial compression of a bone that has very limited ability to bow, a child can sustain a torus fracture at the shaft-metaphyseal transition (Fig. 12.6a, b). These fractures are stable by nature and when immobilized will heal within 2–3 weeks.
-
‘Greenstick’ fracture (damage to the cortex at the tension side of the bend): This type of fracture can occur when the bone is bowed past the fracture limit at the tension site. It concerns an incomplete fracture on the tension side of the bone and plastic deformation with an intact cortex and intact periosteum at the compression side. In these cases, the force that caused the damage to the cortex on the tension side is insufficient to cause a complete fracture (Fig. 12.7).
-
‘Bowing’ fractures: In very young children there can be such deformation of the bone that it bows beyond its yield point, the point beyond which deformation becomes permanent (plastic) and no longer spontaneously recoverable (elastic). In these cases, there is no radiologically visible damage in the cortex, neither to the tension nor to the compression side. The fracture will only be visible by the bowing of the diaphyseal segment (Fig. 12.8a, b). These fractures can be very subtle and sometimes comparison with the contralateral bone is helpful. Bowing fractures are common in the forearm.

Two-year-old infant who presented with a painful arm after a fall from a chair. (a) AP radiograph shows an irregularity of the cortex of the distal radius (arrow). (b) on the lateral radiograph shows a clear torus fracture of the distal radius (arrow)

Six-year-old child who sustained a fall onto an outstretched hand (FOOSH)

Five-year-old child who sustained a fall onto an outstretched hand (FOOSH). (a) There is a transverse fracture of the ulna (arrow). (b) The lateral radiograph shows a bowing fracture of the radius
12.2.2 Manner of Fractures of the Diaphysis
In their original publication from 1962 on ‘The battered child syndrome’, Kempe et al. stated that the child’s extremities are ‘the handles for rough handling’ [2]. This may lead to fractures, in particular of the long bones of the extremities. However, in mobile children fractures of arms and legs are also frequently sustained in accidental circumstances. Sometimes their location is an indicator of non-accidental trauma. In other cases, the clinical history and the level of development of the child could help differentiate between accidental and inflicted extremity fractures. The reader is referred to Sects. 12.4–12.9, concerning the more specific aspects of fractures of certain long bones.
12.3 Fractures of the Metaphysis and Epiphysis
12.3.1 Introduction
The most important difference between the still developing skeleton of a child and the fully grown adult skeleton is the presence of growth plates (physeal plates) in the long bones. These growth plates are responsible for the longitudinal growth of a bone in the skeleton of young children by enchondral bone formation, whereas growth in width originates in the periosteum by membranous bone formation.
The epiphyses determine the size and form of the joint ends. Typical long bones, like the humerus, radius, ulna, femur, tibia, and fibula, have two epiphyses (one at both ends) whereas some of the smaller long bones only have one epiphysis.
Growth plates consist of cartilage. This cartilage is among the weakest parts of the child’s skeleton, especially of the long bones. Due to this weakness growth plates are less resistant to forces exerted to the extremities, compared to the joint capsules, tendons, and ligaments [3]. The growth plates also are the most vulnerable places in the growing skeleton when the joint is subjected to force. This vulnerability will remain as long as ligaments and tendons are more resistant to forces than bone. The damage may consist of a fully or partially torn-off metaphysis (resulting in a metaphyseal corner fracture). When the fully grown skeleton is subjected to the same forces, it more likely results in damage to the ligaments around the joint.
Because growth plates are unique for children, all fractures that have some relation to the growth plate are also unique for children. Amongst these fractures are Salter-Harris fractures and the epiphyseal transitional fractures (triplane fractures and Tillaux fractures). All growth plate-related fractures are at risk for premature focal closure of the growth plate.
12.3.2 Metaphyseal Corner Fracture
12.3.2.1 Introduction
The Metaphyseal Corner Fracture (MCF, a.k.a. Classic Metaphyseal Lesion) is a planar fracture through the most immature portion of the metaphysis in the region of the trabecular transition zone (from primary to secondary spongiosa), disrupting the delicate trabeculae composed of central calcified cartilage cores covered by thin layers of newly formed bone [4]. The fracture line passes peripherally to undercut the subperiosteal bone collar [5, 6]. The resultant fracture fragment is made up of subperiosteal bone collar, physis, and a layer of the primary spongiosa of the metaphysis [4, 5]. MCFs can be extensive diffuse (micro) fractures that extend over the entire metaphysis separating a complete rim-like fragment, or localized (incomplete) injuries separating only a portion of this disk [7, 8].
The term classic metaphyseal lesion in fact is a misnomer, because it is a genuine fracture and not only an unspecified lesion. Thompson et al. stated that ‘A classic metaphyseal lesion is a unique type of fracture with specific morphologic characteristics. Therefore, we suggest using the term "classic metaphyseal fracture" in lieu of classic metaphyseal lesion to improve precision of terminology’ [9].
When these fractures are present over the full circumference of the bone, the radiographs will show a detached metaphyseal rim that is smaller in the centre and wider at the edges (a so-called ‘bucket-handle fracture, Fig. 12.9a). Sometimes the radiographs only show the wider edge (the so-called ‘corner fracture’; Fig. 12.9b). The ‘corner fracture’ and ‘bucket-handle fracture’ are simply different radiographic projections of the same fracture. For consistency we will speak of Metaphyseal Corner Fracture throughout this chapter.

(a) Two-month-old girl who died when ‘co-sleeping’. Radiological examination within the scope of the Dutch cot-death protocol shows a bucket-handle fracture of the distal left tibia (open arrow). (b) Radiograph of the same tibia from a different angle shows a corner fracture (see inset)
Metaphyseal corner fractures are almost exclusively seen in children less than 2 years of age. The fracture may be seen in just one bone or around one joint. Hereby should be mentioned that in a MCF of the proximal tibial metaphysis there is often an associated avulsion fracture of the femur (distal metaphysis). Metaphyseal corner fractures are found most frequently in the distal femur and the proximal and distal tibia (Figs. 12.10a and 12.11a, b), making the tibial metaphysis the most prevalent location for MCFs in infants (Fig. 12.12) [5, 10, 11]. There seems to be a tendency for MCFs in the distal tibia to favour the medial margin of the metaphysis (Fig. 12.13) [12, 13]. After the lower extremity locations the proximal humerus is most affected location (Fig. 12.10b) Fractures to the elbow and wrist have been reported less frequently (Figs. 12.10c and 12.14a, b) [7, 13,14,15,16,17,18]. The long-term consequences of MCFs appear to be minimal or even absent [19].

(a) Severely abused 4-month-old girl. The skeletal survey shows healing metaphyseal corner fractures of the distal femurs and the proximal and distal tibias. Reactive sub-periosteal new-bone formation is visible along the greater part of the right tibia shaft. (b) Metaphyseal corner fracture of the right proximal humerus (see inset). (c) Metaphyseal corner fracture of the left distal radius (open arrow) and a distal metaphyseal humerus fracture (arrow)

(a) Four-month-old infant, the skeletal survey showed an irregularity at the medial side of the distal femur metaphysis (arrow). (b) Follow-up radiograph after 14 days shows local sclerosis in keeping with a healing fracture

Previously healthy two-week-old neonate who was admitted because of convulsions. (a) AP radiograph of the ankle shows a metaphyseal corner fracture of the medial tibial metaphysis (arrow). (b) Lateral radiograph shows the MCF located on the anterior side (arrow). (c) CT of the head shows a subdural hematoma (arrows)

Medial metaphyseal corner fracture of the distal tibia metaphysis (arrow)

(a) Extended metaphyseal corner fracture of the distal humerus in a 3-month-old infant (arrow). (b) After one month there is complete healing, note the presence of a healing fracture of the proximal ulna
The rate of healing is variable. Therefore, it is not possible to give a precise timing of injury based on radiographic findings [20,21,22]. Because the periosteum does not have to be disrupted, commonly no healing features are seen at all (Fig. 12.15a, b) [21]. If there is significant displacement and periosteal stripping then sclerosis and subperiosteal new bone formation (SPNBF) may be present [23] (Fig. 12.16a, b). Another feature of healing MCFs is small cartilaginous protrusions from the growth plate into the metaphysis (Fig. 12.17). Based on extensive experience with follow-up skeletal surveys, Kleinman suggests that most healing MCFs become radiographically inconspicuous at 4 weeks and completely healed at 6 weeks [24]. Tsai et al. found subperiosteal new bone formation in an estimated prevalence of 34% on single point-in-time frontal radiographs of distal tibial MCFs [22]. When employing additional radiographs (both initial lateral view and follow-up skeletal survey) detection increased to 71%, but still 29% of distal tibial MCFs failed to demonstrate periosteal reaction. Karmazyn et al. saw subperiosteal new bone formation in only 47% (16/34) of the cases, according to the authors probably due to a higher percentage of acute MCFs in their initial series [20]. In the retrospective cohort study by Barber et al. skeletal surveys and follow-up skeletal surveys of 567 infants and children showed 124 MCFs in 50 cases [10]. On the initial skeletal survey 72 (58%) of the MCFs were healing, including 12 fractures evident only on follow-up survey. Unfortunately, the article did not describe which radiographic healing features were seen.

(a) Metaphyseal corner fracture or the distal femur (arrows). (b) Radiograph after 18 days shows a normalized distal femur without signs of a healing fracture

(a) Radiograph of the right leg shows metaphyseal corner fractures of the distal femur and proximal tibia. (b) Follow-up skeletal survey shows abundant subperiosteal new bone formation along the shaft of the femur and a fully healed proximal tibia

(a) Radiograph of the distal tibia of a 2-week-old infant, who also had skull, rib, and clavicle fractures shows a metaphyseal corner fracture (arrow). (b) Radiograph after 3 weeks shows a cartilaginous protrusion from the growth plate into the metaphysis (arrow)
These studies underscore that, if non-accidental trauma is suspected, the follow-up skeletal survey has important additional value in the detection, confirmation, and dating of fractures. This applies in particular to the determination of MCFs, as others pointed out before [25,26,27,28,29].
Other radiological modalities such as whole-body MRI and PET images have not shown sufficiently successful in the detection of MCFs [30,31,32]. Proisy et al. compared the skeletal survey to whole-body MRI and bone scintigraphy [32]. In their study they found a total of 29 MCF in 13 children on the skeletal survey. Fifteen (51.7%) of these cases were detected by whole-body MRI and nine (31%) were detected by bone scintigraphy. It is suggested that ultrasound may help determine the presence of MCFs whenever radiographs are equivocal [33, 34]. A study on distal tibias of foetal piglets and a study on bone specimens from five fatally abused infants with MCFs both used 3D high-resolution micro-CT coupled with histopathology to depict the region of the chondro-osseous junction (the region of the trabecular transition zone) [4, 35]. The authors concluded that ‘High-resolution CT coupled with histopathology provides elucidation of the morphology of the MCF’ for now the use of micro-CT should be considered for the research domain only. High quality-thin-sliced volume CT scanning is required to make 3D- and multiplanar reconstructions diagnostic.
More research is necessary to determine the diagnostic value of ultrasound and 3D high-resolution computed tomography in the diagnosis of MCF [33, 34].
12.3.2.2 Cause of Metaphyseal Corner Fractures
Metaphyseal corner fractures are thought to be caused by torsional and traction shear strains applied across the metaphysis, for example when an infant’s extremity is pulled or twisted or if the child is ‘shaken’ (Fig. 12.18) [24, 36]. Metaphyseal corner fractures were also experimentally produced in immature porcine pelvic limbs through application of controlled varus and valgus bending [9, 37].

(a) Graphic representation of a shaking incident. (b) Two-month-old boy with inflicted traumatic brain injury. The radiograph of the skeletal survey shows a metaphyseal corner fracture of the right distal femur (open arrow). (c) Four-month-old girl with inflicted traumatic brain injury. The skeletal survey shows a healing posterior fracture of the 9th right rib (see inset) Furthermore, there is an already healed rib fracture visible of the 5th right rib (open arrow). (d) MRI (T2 FLAIR) of this girl (c) shows a bilateral subdural haematoma (asterisk). (e) Cranial ultrasonography of this girl (c) shows the bilateral subdural haematoma (asterisk). Displacement of the arachnoid membrane (open arrow) is distinctly visible. (f) Normal view of the retina of a normal right eye at fundoscopy. (g) Diffuse retinal bleed in a left eye at fundoscopy resulting from inflicted skull/brain injury
Adamsbaum et al. performed a 15-year retrospective study, based on more than 500 cases from French courts, where they selected all children with at least one MCF, this yielded a study population of 67 children with a median age of 3.4 months [11]. Of these children 44 (66%) had multiple MCFs. In 27 cases there was a confessing perpetrator and they described that their actions were abusive, violent, and intentional. With respect to the abuse they stated that they exerted ‘excessive stress on the joints defined as “indirect skeletal forces” with “torsion, traction, violent compression (or crushing), and forced movements (crossing the arms, folding the legs up over the abdomen, separating the thighs’. Diapering was the most common reported circumstance in which violent handling was described by male perpetrators only (44%), followed by dressing/undressing (30%).
12.3.2.3 Manner of Metaphyseal Corner Fractures
Metaphyseal corner fractures can be sustained due to birth trauma and due to trauma after birth. If sustained after birth the fracture may occur due to accidental and non-accidental trauma. Metaphyseal corner fractures may also occur due to medical procedures.
Despite the fact that the fracture may occur due to several circumstances, it is a highly specific fracture for non-accidental trauma in young children, characteristically seen in infants [8, 23, 38,39,40,41]. Caffey was the first to describe a ‘metaphyseal fragment partially or completely separated from the end of the shaft’ [38].
Metaphyseal corner fractures are rarely, if ever, a reason for seeking medical consultation. They are usually found as occult findings on skeletal surveys. Metaphyseal corner fractures can be found in approximately 30% of children under the age of 12 months of whom a skeletal survey was made because of suspected non-accidental trauma [41]. Metaphyseal corner fractures are commonly encountered in infants with high-risk factors for non-accidental trauma (significant intracranial injury, retinal haemorrhages, and skeletal injuries) and are rare in infants with skull fractures associated with falls, but no other risk factors [42].
Kleinman et al. evaluated 31 deceased infants for the presence and distribution of fractures [43]. They found a total of 165 fractures of which there were 72 (44%) long bone fractures, of these the most commonly encountered were metaphyseal corner fractures with 64 fractures (89% of all long bone fractures and 39% of the total amount of fractures. In a large cohort of 2,890 infants evaluated for physical abuse there were 119 (4.1%) with MCFs and of them 84% had at least one non-MCF fractures identified [44].
Although the MCF is commonly seen in high-risk for non-accidental trauma cases, in some cases the occurrence due to medical procedures and accidental circumstances should be considered (Fig. 12.19a, b).

Two-month-old infant who was attacked by a pit bull terrier. (a) AP radiograph after two weeks shows a transverse proximal radius fracture with signs of healing (arrow) and a metaphyseal corner fracture of the distal humerus with callus formation and subperiosteal new bone formation (open arrow). (b) Lateral radiograph obtained at the same time also shows a mid-diaphyseal torus fracture of the ulna (arrow)
MCFs have been reported after vaginal breech delivery and Caesarean section both with or without attempted external cephalic version (Fig. 12.20a, b): Sieswerda-Hoogendoorn et al. report a case of a term neonate who was born via vaginal breech delivery after an unsuccessful external cephalic version (ECV). After birth the baby was admitted to the neonatal intensive care unit (NICU), where irritability was noted during diaper changing and a MCF of the right distal femur was diagnosed on day 6 of life [45].

(a) Term neonate, born at 39 weeks. Physical examination shows abnormal alignment of the left knee after uncomplicated delivery. A radiograph of the knee shows a metaphyseal corner fracture of the distal femur and the proximal tibia (see inset). (b) Term neonate after birth shows a swollen right knee after a complicated breech delivery. A radiograph of the knee shows a metaphyseal corner fracture of the proximal tibia (see inset) and a Salter–Harris type II fracture of the distal femur
There are two other case reports reporting a MCF after ECV. In the first case ECV was performed on a 36-year-old primipara woman [46]. The external version was followed by an emergency Caesarean section because of blood-stained cervical discharge. After birth a swollen right leg with diminished movement was seen. This was also recorded on photographs made in hospital. The parents returned one week after discharge and a radiograph then showed a MCF of the distal right femur.
In the second case, ECV was performed on a 29-year-old primipara, although successful an emergency caesarean section had to be performed due to foetal stress [47]. After birth, the neonate was fussy and showed decreased movement of the left leg, a radiograph three hours after birth showed a corner fracture of the distal femur and a bucket-handle fracture of the proximal tibia. However, in both cases it is questionable whether the MCF was caused by the version or by the emergency caesarean section.
In a retrospective analysis over a period of 22 years, O’ Connell and Donohue identified three neonates born by elective Caesarean section (two breech and one cephalic presentation) with a MCF of a distal femur [48]. Lee et al. reported a MCF of distal tibia following a difficult footling breech delivery [49]. The authors state that the traction and torque placed on the legs during this difficult delivery were a potential mechanism for this injury. Finally, Buonuomo et al. describe a neonate with multiple fractures, among which a metaphyseal fracture of the femur, ultimately resulting in the diagnosis infantile myofibromatosis [50].
MCFs have been described to occur due to medical procedures:
-
Grayev et al. reported the occurrence in serial casting treatment of clubfeet in 7 infants, who were considered not to be victims of child abuse. One child was abused, in this case the skeletal survey also showed 24 rib fractures [51].
-
Burrell et al. reported a 20-day-old infant with a diagnosis of congenital vertical talus who sustained a metaphyseal corner fracture of the distal tibia during manipulation in preparation for intravenous line placement [52]. The event was independently witnessed, including an audible ‘pop’ at the time of the fracture. Prior X-rays showed normal bones.
-
Della Grotta et al. suggested physical therapy with massage, passive range of motion, and positioning techniques of the lower extremities as the circumstances under which a MCF of the right proximal tibia (in combination with a shaft fracture of the right femur) occurred in an infant with a myelomeningocele, hypertonic lower extremities that lacked sensation, as well as bilateral flexion contractures of the knees and club feet [53]. The child remained in the hospital at the time when these fractures occurred and a child abuse evaluation was negative which made the authors conclude that accidental trauma secondary to physical therapy was the likely aetiology of the MCF.
Two cases of motor vehicle collision-related extremity MCF are described by Culotta et al. although they acknowledge that an alternative clinical consideration for each of the babies is that they had the misfortune to suffer both MVC and physical abuse while with their caregivers [54]. In both of the cases, the caregiver reported that the infant was restrained in a rear-facing car seat behind the driver’s seat at the moment of the car accident.
12.3.2.4 Differential Diagnosis
There are several radiological normal variants that may be mistaken for MCFs [55,56,57]:
-
Step-off, an almost 90 degrees angulation in the cortex (Fig. 12.21).
-
Beak, seen in medial projection of the proximal humerus and proximal tibia (Fig. 12.22).
-
Spur, a discrete longitudinal projection of bone that is continuous with the cortex and extends beyond the metaphyseal margin(Figs. 12.23, 12.24, and 12.25).
-
Metaphyseal fragmentation occurs in children of 15 months and older occasionally encountered in healthy children of 15 months and older with physiologic bowing (Fig. 12.26) [58].

The medial side of the distal femur metaphysis shows a physiological step-off (inset). Note that there is also physiological sub-periosteal new bone formation

(a) Pseudoavulsion fracture of the proximal humerus on native axial image (arrow). (b) Coronal reconstruction shows that the pseudoavulsion is caused by breaking of the humerus (arrow)

Radiograph of the wrist shows a spur on the lateral side of the distal ulna (arrow) and a step-off on the medial side of the distal radius (open arrow)

Radiograph of the knee shows a spur on the lateral side of the distal femur (open arrow), a step-off of the medial side of the distal femur (arrow), and physiological sub-periosteal new bone formation along the diaphysis (arrowhead)

More than one normal variant can be seen in a single child. The lateral distal femur metaphysis shows a step-off (arrow) and the lateral proximal tibia metaphysis shows a spur (open arrow)

Metaphyseal fragmentation in a 1-year 9 months-old child with tibia vara
Lesions that can have some similarity to the appearance of MCF can be found in diseases such as rickets, osteomyelitis, congenital syphilis, and spondylometaphyseal dysplasia ‘corner fracture type’ and Menke’s disease (see Chap. 14).
12.3.3 Salter–Harris Fractures
12.3.3.1 Introduction
Trauma during childhood may result in typical fractures with involvement of the growth plate, the so-called Salter–Harris fractures. Salter and Harris described five types of fractures (Table 12.2). These fractures are seen in approximately 18–30% of all trauma-related long bone fractures in children [59].
12.3.3.2 Cause of Salter–Harris Fractures
The Salter–Harris (SH) classification is based on the mechanism of injury (cause) and the relationship of the fracture line to the growing cells of the growth plate and is correlated with the prognosis concerning growth disturbance [3, 60,61,62].
According to Salter and Harris types I–IV are the result of shearing/avulsion forces while type V results from compression of the growth plate. Vertically oriented splitting compression force across the epiphysis, physis, and adjacent metaphysis can cause type IV SH fractures [62, 63].
Because of the lack of epiphyseal ossification in infants, Salter–Harris type II fractures may be missed on conventional radiographs or may appear as dislocations [64, 65]. MRI or ultrasonography may then be of help in diagnosing SH fractures in this age group (Fig. 12.27a, b) [66].

Term neonate born after a complicated breech delivery after premature rupture of membranes. After birth the child was noted to have a slightly swollen knee. (a) Ultrasonography of the knee showed a metaphyseal corner fracture (arrow) (b) AP radiograph confirms the presence of this metaphyseal corner fracture (arrow)
12.3.3.3 Manner of Salter–Harris Fractures
In childhood and adolescence, Salter–Harris fractures mostly are sustained due to accidental trauma. These fractures occur most frequently in young adolescents, aged 11–15 years, except for the humeral physeal fractures (occurring almost twice as often in the distal humerus) which also have peak incidences at ages 4–6 years [67]. The most common sites are the phalanges of the fingers and the distal radius [59, 67]. Salter–Harris type II fractures are the most prevalent (Fig. 12.28) [67]. Humeral and femoral Salter–Harris fractures are also found as birth injuries due to force of labour and obstetric manipulation [68,69,70,71,72,73,74].

Twelve-year-old girl (with unknown trauma) with a Salter–Harris type II fracture of the distal tibia (open arrow). The fracture through the growth plate can be identified by the anterior diastasis (arrow)
Literature on physeal fractures in children with non-accidental trauma is scarce. A few case reports and case series mention physeal fractures in the proximal femur and the distal humerus with proven non-accidental circumstances [65, 75, 76].
Barber performed a large cohort study to define the yield of rigorously performed skeletal surveys in infants with suspected physical abuse [10]. In this study 13 of the 313 (4%) infants diagnosed with a fracture had at least one Salter–Harris fracture (all type II), most frequently of the distal humerus. All SH-fractures were evident on the initial survey and four of the children had other positive findings on the skeletal survey.
12.3.4 Epiphyseal Transitional Fractures
Epiphyseal transitional fractures typically occur in the distal tibia during the 18-month period of closure of the growth plate aged between 12 and 15 years. Closure of the distal tibial growth plate starts centrally and medially before progressing laterally. This partial closure leaves the ankle vulnerable to these types of fractures, especially during external rotation.
The triplane fracture configuration consists of:
-
(1)
A fracture line along the coronal plane through the posterior metaphysis.
-
(2)
A fracture line along the sagittal plane through the epiphysis.
-
(3)
A fracture line along the transverse plane through the growth plate.
The fracture may consist of 2–4 fragments. The triplane fracture appears as a Salter–Harris type II on lateral radiographs and as a Salter-Harris type III on AP radiographs. CT has a definite impact on fracture classification, displacement, and treatment [77]. A gap of 2 mm or more is considered by some authors as the threshold between conservative and surgical treatment. Triplane fractures account for 5–15% of all ankle fractures in adolescents [78]. Growth arrest, although usually insignificant, may occur in 7–21%.
The Tillaux fracture is a SH-type III involving the anterolateral aspect of the distal tibial epiphysis which is seen in adolescents in whom the medial section of the distal tibia metaphysis has started to close. As a result, only the anterolateral part of the growth plate is open and vulnerable to injury and consequently, the Tillaux fracture is seen in adolescents aged between 12 and 15 years. Lateral triplane fractures, just like Tillaux fractures, are caused by supination, combined with external rotation (twisting), while medial triplane fractures are caused by adduction [78]. Epiphyseal transitional fractures have only been reported due to accidental trauma.
12.4 Humerus
12.4.1 General Aspects of Humerus Fractures
Humerus fractures are most frequently seen in children under the age of 3 years and above the age of 12 years [79]. This is irrespective of the circumstances under which the fractures were sustained.
Fractures of the humerus have been described to occur before (very rare), during, or after birth. If sustained after birth, one should differentiate between accidental and non-accidental circumstances. According to Caviglia et al., one should be aware that the circumstances, under which humerus fractures are sustained vary between age groups [79].
12.4.2 Fractures of the Proximal Humerus
12.4.2.1 General Aspects of Fractures of the Proximal Humerus
Fractures of the proximal humerus account for 2–5% of all fractures in paediatric patients [80,81,82,83,84,85,86]. Proximal humeral fractures are 3–4 times more likely to occur in boys than girls and are most common in adolescents with a peak age of 15 years [87]. Chae et al. evaluated the findings in 41 children with proximal humerus fractures (aged 1 month to 15 years; mean age 8.6 years) and found that 56% of this type of fracture occurred in girls and 44% in boys [88].
Proximal humerus fractures include fractures of the proximal metaphysis or the proximal physis [84, 89].
Metaphyseal fractures account for about 70% of the fractures of the proximal humerus in paediatric patients and can be described using the Neer-Horowitz classification based on the amount of angulation and displacement at the fracture site (Table 12.3) [89,90,91]. Fractures at this location typically occur in children aged 5–12 years [87].
Fractures of the physis account for around 30% of proximal humerus fractures and are categorized according to the Salter–Harris classification [91]. SH-type I is most common in children under the age of 5 years, while SH type II is most common in children above the age of 12 years. According to Popkin et al. SH types III and IV are rare in paediatric patients and are usually associated with high-energy trauma [87].
12.4.2.2 Cause and Manner of Fractures of the Proximal Humerus
Fractures of the proximal humerus may occur during and after birth.
12.4.2.2.1 During Birth
Birth-related fractures can be found in all parts of the humerus with midshaft fractures being the most common [92, 93].
The risk of fractures of the proximal humerus is highest in large infants during vaginal delivery (although proximal humerus fractures have also been reported in smaller infants) or during breech delivery (irrespective of the size of the child) [94, 95]. Other known risk factors are labour dystocia and macrosomia (birth weight above 4.5 kg) [87].
Birth-related growth plate injuries have also been described. Varghese et al. presented two neonates with humeral growth plate fractures (Salter–Harris type 1), one at the proximal humerus and one at the distal humerus [96]. Jones et al. described a premature neonate, delivered by caesarean section due to malpresentation, with a Salter–Harris II fracture of the proximal humerus [97].
Popkin et al. stated that a proximal humerus fracture that is diagnosed in the first week of life is considered to be birth-related if no history of a trauma after birth is known: ‘During the descent down the birth canal, the infant’s arm can be placed in a variety of compromised positions that can result in a physeal fracture of the proximal humerus’. According to Popkin et al. birth-related fractures of the proximal humerus are classic physeal separations or SH-type I injuries [87].
12.4.2.2.2 After Birth: Accidental and Non-accidental Circumstances
After birth fractures of the proximal humerus can occur due to direct or indirect trauma in either accidental or non-accidental circumstances.
In children under the age of 3 years one should always consider non-accidental circumstances [87, 91]. There are no radiographic findings on imaging of the shoulder that are suggestive of non-accidental circumstances in case of a proximal fracture. The incidence of proximal humerus fractures due to non-accidental circumstances is not known. Chae et al. evaluated the findings in 41 children with proximal humerus fractures (aged 1 month to 15 years). In only 1 child (age not specified) the circumstances were determined to be non-accidental.
In older children proximal humerus fractures usually are sustained in accidental circumstances due to a moderate-energy trauma, associated with falls, motor vehicle crashes, or sports participation [87].
Fractures may be due to a direct trauma (blunt force trauma) to the shoulder/proximal arm, usually to the posterior shoulder. This can be a direct blow/strike to the shoulder/proximal arm or a fall on the posterolateral part of the shoulder. They may also occur due to an indirect trauma, like a fall (backwards) on an outstretched hand, with the arm in abduction and external rotation, the hand in dorsiflexion, and the elbow in hyperextension. These fractures often occur during traffic accidents, sporting activities (contact sports, like hockey and soccer, horseback riding, gymnastics) and during play (Fig. 12.29) [81, 87, 98]. Popkin et al. also mentioned the occurrence of overuse injuries due to repetitive throwing in baseball (little league shoulder, due to overthrowing, mainly in baseball players aged 11–14 years). Another example given by Popkin et al. is the occurrence of an avulsion fracture of the lesser tuberosity in throwing athletes aged 12–15 years and in fly fishermen [87].

Subcapital humerus fracture in a 4-year-old girl who fell from a swing
Fractures at this location may result from complications of underlying diseases such as tumours, metabolic diseases, and secondary neuropathies [81, 91, 99,100,101]. Proximal humerus fractures have also been described resulting from aneurysmal and unicameral bone cysts and can be associated with complications of radiation therapy [87].
12.4.3 Fractures of the Humerus Shaft
12.4.3.1 General Aspects of Humeral Shaft Fractures
The reported incidence of humeral shaft fractures in paediatric patients under the age of 16 years varies greatly. According to Caviglia et al. humeral shaft fractures account for around 0.75%, according to Marengo et al. for around 2–5% and according to Shrader for up to 10% of all fractures in paediatric patients [79, 84, 102]. Shaft fractures account for approximately 20% of all humerus fractures in children with an estimated incidence of 12–30 per 100.000 paediatric patients per year [103]. Shaft fractures seem to be more common in children under the age of 3 years and above the age of 12 years [79, 103]. Boys to girls ratio is around 2:1 [85].
Shaft fractures are described by [79, 104]:
-
Anatomical location: proximal, middle, or distal third part of the shaft
-
Fracture pattern: spiral, oblique, transverse, or comminuted
-
Degree of displacement and angulation
-
Presence of soft tissue damage: open or closed fracture
12.4.3.2 Cause and Manner of Humeral Shaft Fractures
Fractures of the humeral shaft have been described to occur before (very rare), during, or after birth. If sustained after birth, one should differentiate between accidental and non-accidental circumstances. According to Caviglia et al. one should be aware that the circumstances, under which humeral shaft fractures are sustained vary between age groups [79]. In neonates, e.g. shaft fractures are seen mainly within the scope of birth trauma in macrosomic babies (Figs. 12.30 and 12.31a, b), while in children under the age of 3 years, non-accidental trauma should always be considered. In children above the age of 10 years, shaft fractures are often the result of direct or indirect blunt force accidental trauma (Fig. 12.29) [79].

Birth-related humerus fracture after a complicated delivery due to shoulder dystocia

Neonate born at 40 weeks gestational age, birthweight 4060 g (P89), vaginal delivery was complicated by a shoulder dystocia. During delivery the gynaecologist heard a ‘crack’. (a) Radiography showed a mid-diaphyseal humerus fracture (arrow). (b) Follow-up radiography shows callus formation around the fracture
12.4.3.2.1 Before Birth
Prenatally acquired shaft fractures are probably very rare and almost always found in children with severe congenital bone disease, e.g. osteogenesis imperfecta type II (see Chap. 14) [105]. One of the first reports on bilateral intrauterine humeral shaft fractures was by Barker in 1857 [106]. Barker described the findings in a newborn, who died within minutes after birth. The girl had numerous long bone fractures (humerus, radius, ulna, femur, tibia, fibula) and extensive skull abnormalities (absent frontal bone, absent parietal bone, abnormal occipital bone) (Fig. 12.32). Although no diagnosis was given in the article, one may suspect that the child today would probably be diagnosed with perinatal lethal type II osteogenesis imperfecta. Barker referred to several other case reports, in which numerous prenatally acquired fractures, including humerus fractures, had been described. In a follow-up article Barker stated: ‘P.S. It may be worthy of remark that the lady, Mrs. L., who in September, 1856, gave birth to the foetus, the subject of the foregoing remarks, was yesterday (September 27th) delivered of a healthy and well formed female child at the full period’ [106].

Drawing of the newborn, who died within minutes after birth, described by Barker [106]. The girl had numerous long bone fractures
12.4.3.2.2 During Birth
Birth-related humeral fractures can be found in all parts of the humerus (shaft, proximal, and distal humerus) with midshaft fractures being the most common [107, 108]. Shaft fractures may occur due to trauma during vaginal birth (Fig. 12.33), but also, although less common, in caesarean section (sometimes even bilaterally), due to limb extraction [92, 93, 108]. Shaft fractures are caused by hyperextension or rotation of the arm during passage through the birth canal [109,110,111]. Shaft fractures are often seen as birth trauma in infants due to obstetric manoeuvres during a breech delivery [112], but may also occur in vaginal delivery with shoulder dystocia [113,114,115].

Humerus shaft fracture in a one-day-old neonate after an uncomplicated vaginal delivery
The typical birth-related shaft fracture is a complete, transverse midshaft fracture (Fig. 12.34) [116].

One-month-old infant girl who, according to the parents, had fallen from a bed. The spiral fracture of the humerus does not correspond with the trauma description
Humeral (shaft) fractures are the second most common birth-related long bone fractures in the neonate after clavicular fractures [116]. Their exact incidence is not known and is estimated to be up to 0.6/1000 live births (Table 12.4) [107, 117,118,119,120,121]. Von Heideken et al. found that the occurrence of a birth-related shaft fracture was associated with maternal obesity, labour dystocia, shoulder dystocia, vacuum-assisted delivery, male sex, multiple birth, breech, preterm, large-for-gestational age, birth weight over 4000 g, and injury of brachial plexus [117]. A bone fragility diagnosis was recorded in 1% of the neonates birth-related humerus shaft fractures.
12.4.3.2.3 After Birth: Accidental or Non-accidental Circumstances
Transverse shaft fractures are caused by a direct trauma, a blunt force trauma, directly impacting the shaft (e.g. a blow). The more energy is transferred during the impact (the harder the blow hits the upper arm), the more likely the fracture is to be comminuted [122]. Spiral/oblique fractures are caused by an indirect trauma from a fall or another incident with humeral rotation or twisting, as may happen in arm wrestling (Fig. 12.34) [116, 122].
Concerning the occurrence of humeral shaft fractures after birth, Von Heideken et al. found an incidence after birth of 0.073 per 1000 children under the age of 1 year (142 children in a nationwide study in 1,855,267 infants under the age of 12 months). In 56% of these children falls were reported. In 14% of the shaft fractures were determined to have occurred in non-accidental circumstances. This concerned mainly children under the age of 6 months.
Some authors state that humerus fractures (including fractures at locations other than the shaft) are the most common fractures in young children under the age of 3 years due to non-accidental trauma [96, 123]. Loder and Bookout found that shaft fractures were the second most common long bone fracture due to non-accidental trauma after tibial fractures [39]. Others report that most humerus fractures (46–81%, five different studies), especially in young children outside the neonatal period and under the age of 3 years occur due to non-accidental trauma. In children under the age of 15 months, the reported percentage of non-accidental trauma ranges from 67% to 100% [40, 124,125,126,127]. The most common locations in non-accidental trauma are midshaft and metaphyseal [96, 123].
Williams and Hardcastle published a ‘best evidence topic report’ on the relation between humeral shaft fractures and non-accidental trauma in children [128]. Their study comprised 44 articles, of which two were able to provide an indication regarding the formulated query: ‘What is the specificity of an isolated proximal humerus fracture in children who are suspected of being abused’ [123, 129]. Their analysis provided the following clinical bottom line: ‘Although a humerus fracture cannot be seen as pathognomonic for child abuse, such a fracture in a young child should always be followed up with a closer look into its origin’ (Fig. 12.35). Williams and Hardcastle maintain that both included studies tried to define the specificity of the various types of humerus fracture in relation to child abuse, but that in both studies there was no ‘golden standard’. Consequently, it is feasible that in both studies children have been overlooked or that it was falsely concluded that non-accidental trauma was involved. Yet, it appears that the incidence of non-accidental trauma in this type of fracture is high. In particular in children under the age of 3 years, spiral and oblique fractures were more often the result of non-accidental trauma than of anything else.

(a) Seven-month-old girl suspected of being abused. Slightly abnormal alignment of the upper arm is visible (open arrow). (b) Radiograph shows a distal oblique humerus fracture
Shaw et al. did a retrospective study on 34 children under the age of 3 years with a humeral shaft fracture [129]. The authors excluded children with a humerus fracture at a different places (supracondylar, epicondylar, condylar, proximal epiphyseal, and metaphyseal). From a revision of the clinical data and data from the county child protective services the authors established whether or not the child had probably sustained the fracture in non-accidental circumstances (defined as probable child abuse). Cases were reviewed independently by four physicians and were classified as probable abuse (non-accidental trauma), probable not abuse, and indeterminate. Shaw et al. concluded that most fractures of the humerus shaft were accidental. After evaluation, only 18% were classified as ‘probable abuse’. Neither age nor fracture pattern was conclusive in differentiating between accidental and non-accidental circumstances. The history and findings other than the fracture itself were critical in establishing the circumstances. Based on these findings, the authors concluded that six factors can be essential in establishing whether non-accidental trauma should be suspected:
-
1.
The presence of simultaneous or older injuries (Fig. 12.36).
-
2.
Delay in seeking medical treatment.
-
3.
Differences in or contradicting stories regarding the incident.
-
4.
The child is accompanied by a person other than the one present at the incident.
-
5.
The lack of metabolic or genetic bone diseases.
-
6.
The parent shows lack of involvement or unusual behaviour.

Right distal metaphyseal humerus fracture in a 3-month-old boy. The mid-axillar rib fractures on the right are clearly visible in this view (open arrows)
Pandya et al. performed a large retrospective study, in children under the age of 4 years, in an urban level I paediatric trauma centre [130]. In the period 1998–2007, a total of 1485 children, 500 non-accidental (377 <18 months), and 985 accidental (425 <18 months) cases, were included. In the non-accidental group there were 43 (8.6%) humerus fractures and in the accidental group 102 (10.3%, p=0.28). In the under 18 months group this was, respectively, 37 (9.8%) versus 19 (4.5%, p<0.001). Based on their findings the authors concluded that in the under 18 months group ‘the odds of a humerus fracture (2.3 times) were found to be significantly higher in the child abuse group than in the control group’. For the whole study population the odds ratio for abuse was 0.8 (95% CI: 0.6–1.2).
In another study from the same group the authors compared 36 children (representing 39 humerus fractures) under the age of 4 years in whom the cause of the fracture was recorded as abuse with 95 children with an accidental humerus fracture [131]. Based on univariate logistic regression the authors showed that the odds of being a victim of non-accidental injury in children with an age below 18 months was 31.54 times greater, in children with any additional fractures or injuries to another body system it was 65.1 times greater, and in children with physical and/or radiographic evidence of prior injuries it was 131.60 times greater.
If non-accidental trauma cannot be ruled out in a child younger than 2 years with a humerus fracture a skeletal survey should be performed according to the guideline of the Royal College of Radiology and the Society and College of Radiographers (See Chap. 3) [29].
In older children shaft fractures usually occur in accidental circumstances, due to either indirect trauma, like a fall on an outstretched hand, or direct trauma, usually with a high transfer of energy, e.g. a direct blow to the upper arm, e.g. in traffic accidents, falls or sporting activities [116]. Accidental shaft fractures occur more frequently in children that have been victims of a serious accident [132]. In contact sports (martial arts), there is also a possibility of direct trauma, due to a direct blow (e.g. a karate blow) or indirect trauma, due to falling in a judo throw. Other circumstances are skateboarding, mountain biking, downhill skiing, and trampoline jumping [133, 134].
12.4.3.2.4 After Birth: The ‘Hymel manoeuvre’
A rare trauma mechanism that can lead to fractures in the humerus shaft in non-mobile infants is the so-called ‘Hymel manoeuvre’ (Figs. 12.37, 12.38, and 12.39) [135].

Graphic representation of the mechanism as described by Hymel and Jenny

Two-month-old infant, father turned the infant from prone to supine position holding the right arm. During this manoeuvre he heard a ‘crack’ and the infant started to cry. Radiography showed an oblique fracture of the left humerus. A skeletal survey, CT of the head, and a follow-up survey all were negative. The reported history is in keeping with the publication by Hymel and Jenny [135]

Three-month-old infant who was positioned in a prone position on a duvet. He was found on his back, crying and upon inspection did not use his arm. Radiography showed a fracture of the right humerus (arrow). A skeletal survey, CT of the head, and a follow-up survey all were negative. After extensive evaluation it was concluded that the reported history was in keeping with the publication by Somers et al. [136]
Hymel and Jenny presented two cases, one of which was videotaped, in which a parent unintentionally fractured the humerus of their infant by turning the infant from a prone to a supine position. In the second case, the father gave a similar clinical history and subsequent evaluation ruled out non-accidental injury.
In 2014, Somers et al. published a paper describing 7 infants (aged 4–7 months) who were presented with only a humerus shaft fracture [136]. In none of the cases, a videotape was available as a source of evidence, but the clinical histories were independently obtained as part of court hearings. In three cases the parents stated that they witnessed that their child tried to roll from prone to supine, where he/she was initially obstructed from doing so by the dependent arm. After several attempts, the infant gained sufficient momentum to roll over and as a result the dependent arm got overloaded and broke. In the other 4 cases, the infant was placed in a prone position and found in a supine position. The authors agree that, given the lack of an actual video of the event, they cannot state with certainty that this is a valid trauma mechanism. However, given the Hymel video, one should at least consider this as a potential trauma mechanism which of course can only be in the differential diagnosis if all other evaluations and examinations are negative.
In 2020, Altai et al. casted doubt on this proposed mechanism by performing a CT-based finite element study [137]. According to their data, the highest predicted strain is around 20% of the predicted elastic limit of humerus during an infant rolling over.
12.4.3.2.5 After Birth: Underlying Medical Conditions
Shaft fractures may also occur as a complication of underlying medical conditions, e.g. unicameral benign bone cysts or other benign lesions (pathological fracture) [79, 116]. Pathological fractures may also occur in disorders with increased bone fragility, like osteogenesis imperfecta, fibrous dysplasia, scurvy, and osteopetrosis [134]. Von Heideken et al. found among infants with birth-related humerus shaft fractures, that 1% had a bone fragility diagnosis (n = 2; osteogenesis imperfecta and rickets/vitamin D deficiency). Among children with a later humeral shaft fracture 6% had a bone fragility disorder (n = 8; 7× osteogenesis imperfecta and 1× rickets/vitamin D deficiency).
One should consider a pathological shaft fracture if the fracture occurs after a mild trauma. Pathological fractures occur most commonly in children aged between 3 and 12 years [104].
12.4.4 Fractures of the Distal Humerus
12.4.4.1 General Aspects of Fractures of the Distal Humerus
Fractures of the distal humerus account for over 10% of all paediatric fractures [138]. Several fracture patterns of the distal humerus can be found, which include [138, 139]:
-
Supracondylar fractures
-
Lateral condyle fractures
-
Medial condyle fractures
-
Medial epicondyle fractures
-
Transphyseal fractures
-
Capitellum fractures
When evaluating the distal humerus, the ossification centres of the epiphysis should be taken into account. These ossify according to a set order (Fig. 12.40 and Table 12.5) [140]. Although CRITOE (see Fig. 12.40 and Table 12.5) is generally applicable variation does occur, in a study by Goodwin et al. in 212 of 221 children (96%) the order was according to the general rule [141]. In seven cases, the internal epicondyle was visible before the radial head and in two cases the olecranon was visible before the trochlear centre.

Ossification of the elbow follows a set sequence that is described in the acronym CRITOE (see Table 12.5)
Avulsion fractures of growth centres have been found after accidental trauma (Fig. 12.41).

Avulsion fracture of the medial epicondyle of the humerus (open arrow) in a 9-year-old girl who had fallen from a skateboard. There is considerable soft-tissue swelling present (asterisk)
With respect to metaphyseal corner fractures of the distal humerus the reader is referred to Sect. 12.3.2.
12.4.4.2 Supracondylar Fractures: Epidemiology, Cause, and Manner
Supracondylar fractures are common fractures in paediatric patients. In some studies, the incidence is estimated at 10–16% of all paediatric fractures [138, 142]. Supracondylar fractures are the most common fractures of the distal humerus/elbow fractures and account for 60–75% of all distal humerus fractures/elbow fractures [138, 139]. This type of fracture is much more common in skeletally immature children aged between 3 and 7 years than in adults, with a peak age between 5 and 7 years [142,143,144]. Ninety percent of all subcondylar fractures are found in children under the age of 10 years and are more common in boys than in girls [145].
Over 95% of supracondylar fractures are of the extension type due to a fall on the outstretched hand, e.g. a fall from a moderate height, like from a bed or a monkey bar [145]. In the extension type the distal part is displaced posteriorly.
Flexion-type fractures are uncommon and account for less than 5% of all supracondylar fractures. Flexion-type fractures are much more common in older adult patients and are caused by direct impact on the flexed elbow, e.g. in a fall directly on the flexed elbow [139, 146]. In this type, the distal part of the fractures is displaced posteriorly.
In children over the age of 18 months, supracondylar fractures and dislocations most commonly occur in accidental circumstances and are only rarely reported due to non-accidental circumstances (Fig. 12.42) [123, 130, 131, 147,148,149]. In younger children and certainly in non-mobile/non-ambulatory children non-accidental circumstances should always be excluded [123, 149].

Ten-year-old girl with a supracondylar humerus fracture after a fall
Thomas et al. evaluated the medical records and radiographs of 39 children under the age of 3 years with either humeral or femoral fractures [125]. Fourteen of them had humeral fractures. In 11 children the circumstances were determined to be non-accidental. In 3 children, all 3 with supracondylar fractures the circumstances were determined to be accidental (fall from a tricycle, a rocking horse, or a fall downstairs). Humerus fractures other than supracondylar fractures were all found to be due to abuse. The clinical history usually shows that the (mobile) child fell on the extended arm (hand in dorsiflexion and elbow in hyperextension) or directly on the bent elbow [125, 147].
Strait et al. evaluated retrospectively the findings in 124 children under the age of 3 years with humerus fractures, concerning the circumstances of the occurrence (inflicted, undetermined, not-inflicted) [123]. In 9 out of 25 children under the age of 15 months (36%) the fractures were determined to be inflicted and in only 1 of 99 children over the age of 15 months (73%). Non-accidental circumstances were excluded in 91 of 124 children (73%). In 23 of 124 children the circumstances were undetermined (18.5%). Ten children under the age of 15 months had supracondylar fractures. In 2 of these 10 children the circumstances were determined to be non-accidental. In these children the clinical history and the moment that medical help was sought were conclusive [150]. Twelve children had spiral/oblique fractures. In 7 of them (58%) the circumstances were determined to be non-accidental. According to Strait et al. non-accidental circumstances should be considered in children under the age of 15 months with humeral fractures, including children with supracondylar fractures.
Rosado et al. evaluated the findings in 97 children under the age of 18 months with a total of 100 humerus fractures [149]. The most common fracture location was the distal humerus (65%) and the most common fracture type was supracondylar (48%). Child Protection evaluated 44 children (45%) and determined that in 24 of these children, with a total of 25 humerus fractures, the fractures were sustained in non-accidental circumstances (25% of the total study population). The most common fracture location, in children determined to have been sustained in non-accidental circumstances, was the distal humerus (50%) and the most common types were transverse and oblique (25% each). However, transverse and oblique fractures were also seen in patients whose injuries were determined to have been due to accidental circumstances. Children with non-accidental fractures were younger and non-ambulatory than children with accidental fractures. Children with non-accidental fractures also had more often additional injuries, suspected to be inflicted.
Rinaldi and Hennrikus reviewed the findings in 75 children with displaced supracondylar elbow fractures: 42 boys, 33 girls with an average age of 6 years (range: 1 year 4 months to 12 years 4 months; 70 children older than 3 years) [151]. Forty-seven percent of the fractures occurred at home. Only one child (the youngest child in the evaluated population), aged 1 year and 4 months was reported because of suspected non-accidental circumstances. The child supposedly was injured from a fall at home. The evaluation did not confirm the suspicion of non-accidental circumstances. Rinaldi and Hennrikus concluded that paediatric supracondylar elbow fractures in their study only occurred due to accidental falls while children were at play. The mechanisms involved were fall on the outstretched hand and hyperextension of the elbow.
12.4.4.3 Fractures of the Lateral Condyle: Epidemiology, Cause, and Manner
Fractures of the lateral condyle are the second most common fractures of the distal humerus and account for up to 20% of all paediatric elbow fractures [138, 139, 152]. This fracture is most commonly found in children aged between 4 and 10 years with a peak at 6 years of age, these fractures are most commonly a Salter–Harris-type IV fracture [139, 152].
This fracture occurs after a fall on an outstretched hand (FOOSH) (Fig. 12.43). Two theories exist concerning the cause of the fracture (mechanism) [152,153,154]:
-
A push-off mechanism: This theory postulates that the fracture is the result of a force directed upward and outward along the radius. If the radial head impacts the distal humerus, this may cause the fracture of the lateral condyle. This typically occurs due to a fall on an outstretched hand (axial loading).
-
A pull-off mechanism: This theory postulates that the pull of the tendons of the extensor carpi radialis longus, extensor carpi radialis brevis, and brachioradialis, that are attached to the lateral condyle, may result in an avulsion fracture of the lateral humeral condyle.

Fourteen-month-old child who was seen in the emergency department after a fall onto an outstretched hand (FOOSH). AP radiograph of the left elbow shows an avulsion fracture of the lateral condyle (arrow)
According to Tewjani et al., the most likely cause is a combination of push- and pull-off mechanisms [153]. Reports on fractures of the lateral condyle only describe the occurrence due to accidental circumstances. No case reports (series or single) were found concerning the occurrence of fractures of the lateral condyle due to non-accidental circumstances, although Kleinman states that fractures of the lateral condyle may occur due to non-accidental circumstances and Offiah and Hall are of the opinion that a fracture at this location has a medium specificity concerning non-accidental circumstances [155].
12.4.4.4 Fractures of the Medial Condyle: Epidemiology, Cause, and Manner
According to Walsh ‘medial condyle fractures involve a fracture line that extends through and separates the medial metaphysis and epicondyle from the rest of the humerus; by definition, the fracture line must involve the trochlear articular surface. Medial condyle fractures must be distinguished from medial epicondyle fractures that involve the medial column but are extraarticular’ [156]. Isolated fractures of the medial condyle are very rare and probably account for less than 1–2% of all distal humerus fractures [156, 157]. This type of fracture is most common in children, aged 7–14 years [156]. Concerning the cause of a fracture of the medial condyle (mechanism) 3 theories exist [156, 157]:
-
A fall on the palm of an outstretched arm, with the elbow forced into valgus (axial loading).
-
A fall on the point of the elbow (apex of the flexed elbow), with the olecranon driving the medial condyle proximally and medially (direct impact).
-
An avulsion fracture, due to violent contraction of the flexor and pronator muscles that attach to the medial epicondyle, such as that which occurs in arm wrestling.
Because this type of fracture is so rare, hardly any (if any) epidemiological data concerning the circumstances of the occurrence in paediatric patients are known. Kleinman reports an unusual SH-type III medial condylar fracture of the distal humerus in a 23-month-old girl, which was determined to be inflicted [158].
12.4.4.5 Fractures of the Medial Epicondyle: Epidemiology, Cause, and Manner
As stated in Sect. 12.4.4.4 fractures of the medial epicondyle should be distinguished from fracture of the medial condyle. Fractures of the medial epicondyle are much more common than fractures of the medial condyle and account for 10–20% of all elbow fractures in children and adolescents [139]. In up to 60% of these fractures are associated with elbow dislocation [159]. Bauer et al. described the simultaneous occurrence of bilateral elbow dislocation with bilateral medial epicondyle fractures in a 13-year-old female gymnast (trampoline gymnastics) with hyperlaxity [160].
Most occur in paediatric patients aged between 11 and 14 years (peak ages 11 and 12 years) [156]. According to Smithuis 80% of these fractures occur in boys with a peak age in early adolescence [139].
Walsh mentions three theories concerning the cause of fractures of the medial epicondyle:
-
A direct blow on the posterior medial aspect of the epicondyle.
-
An avulsion mechanism, due to activity of the flexor muscles of the forearm. This may occur when a child falls on the extended arm and hyperextends wrist and fingers, placing more stress on the forearm flexors. This avulsion mechanism may also in arm-wrestling and throwing a baseball (‘little league elbow’).
-
An avulsion mechanism in which, due to dislocation of the elbow, the ulnar collateral ligament (UCL) provides an avulsion force that causes the medial epicondyle to fail.
Irrespective of the theory in a fracture of the medial epicondyle the apophyseal fragment is partially or completely separated from the rest of the humerus.
Most of the fractures of the medial epicondyle will occur in older children and adolescents, due to accidental circumstances or sporting activities [161]. No reports were found concerning the occurrence due to non-accidental circumstances. Sperry and Pfalzgraf described the occurrence of healing symmetrical clavicular fractures and a healing left medial humeral epicondyle fracture in a 9-month-old child [162]. The child was found unresponsive in his crib, five hours after his last feeding. During the autopsy no physical signs, suggesting non-accidental trauma, were found. Only a few visceral pleural and epicardial petechiae were found, which were determined to be consistent with the sudden infant death syndrome (SIDS). The healing fractures were found on post-mortem total body radiographs. The parents had no explanation for these injuries and denied causing any harm to the child. The case was reported to the police and the district attorney's office as suspected non-accidental trauma. During the investigation the parents stated that the child had undergone ‘chiropractic’ manipulations by an unlicensed therapist, between three and four weeks prior to death, to correct supposed ‘shoulder dislocations’. This time interval correlated with the histologic age of the injuries, and the history explained their unusual bilateral location and appearance.
12.4.4.6 Transphyseal Fractures: Epidemiology, Cause, and Manner
Transphyseal fractures (a.k.a. transcondylar fractures or distal humerus physeal separation) are fractures through the distal humeral physis, in which the entire distal humeral epiphysis is separated from the metaphysis. According to Shore the physis is biomechanically the weakest location in distal humerus in skeletally immature children [163]. This type of fracture most commonly occurs in children under the age of 3 years [164, 165].
Transphyseal fractures can be classified according to the Salter–Harris classification (see Sect. 12.3.2) [165]:
-
SH-type I (pure physeal injury) is seen most commonly in children under the age of 3 years.
-
SH-type II (metaphyseal fragment attached to distal fragment) is most common in children over the age of 3 years.
-
SH-types III and IV (intra-articular extension) occur, but are rare.
Transphyseal fractures have been described to occur during and after birth [64, 165, 166]:
-
In vaginal delivery fractures may happen due to the force of labour or due to obstetric manoeuvres. Shoulder dystocia and traumatic delivery are known risk factors. It may also occur during a caesarean section, due to excessive traction. Usually, birth-related transphyseal fractures are recognized before the age of 2 weeks.
-
Transphyseal fractures have also been described to occur after birth, either in accidental or in non-accidental circumstances.
Gigante et al. described 5 cases of birth-related distal humeral growth plate fractures [69]. During a 30-month follow-up 4 cases showed an excellent clinical and radiological outcome with conservative treatment, in one case surgical intervention with stabilization using a K-wire was needed. On conventional radiographs the diagnosis may, due to the non-ossified epiphysis, be difficult (Fig. 12.44a, c). In several case reports the use of ultrasound in the diagnosis is propagated as a problem-solving modality (Fig. 12.44b) [68, 167, 168]. Although birth-related humerus fractures are usually diagnosed during the first day of life delayed presentation of several days is not uncommon and thus a delayed presentation should not rule out birth trauma [169].

Neonate born after an uneventful vaginal delivery. Two days after birth the nurse noted a lack of motion of the left arm. (a) Radiography showed an abnormal relation in the elbow, which was suspect for a humerus epiphysiolysis. (b) Ultrasonography clearly shows the displaced epiphysis (asterisk). (c) Radiography on day 22 of life shows callus formation along the distal humerus metaphysis. Long-term follow-up showed a normal development of the elbow joint
Supakil et al. reviewed the findings in 16 children with transphyseal fractures (distal humeral epiphyseal separation) under the age of 36 months (mean age 8.6 months; 10 boys, 6 girls) [166]. In 10 (63%) children, one or more additional humeral fractures were found (bucket-handle fractures in 5 and condylar avulsion fractures in 6 children). Six children (38%) were under the age of 2 weeks. In these children, the fracture was determined to be secondary to birth trauma. In 4 children the fracture occurred in a vaginal delivery (breech delivery with footling presentation 1×, nuchal cord wrapped around right upper extremity 1×, shoulder dystocia 1× after uncomplicated). In two children the fractures occurred in an uncomplicated caesarean section. In 4 of the 10 children above the age of 14 days (3 boys, aged 3.3 months, 8.1 months, 2.3 years; 1 girl; aged 3.3 months), the fracture was determined to have occurred in non-accidental circumstances. In the remaining 6 children the fracture occurred due to accidental circumstances (sibling jumping on child twice, falls downstairs twice, falls from chair twice). In the same publication the occurrence of a transphyseal fracture in a 1-month-old neonate was reported. Because a relevant obstetrical history of a history of a preceding trauma was lacking, it was suspected that the fracture occurred due to non-accidental circumstances.
The supposed mechanism in non-accidental trauma is a rotational force (twisting) and in accidental trauma a fall on outstretched hand with an extended elbow [165]. According to Shore in infants extension forces may more likely cause a transphyseal fracture, while in older children comparable forces may more likely cause a supracondylar fracture [163].
12.4.4.7 Capitellum Fracture: Epidemiology, Cause, and Manner
Capitellum fractures are very rare in children and adolescents, accounting for less than 1% of all elbow fractures. Murthy et al. evaluated 32 paediatric patients with capitellum fractures (22 boys, 10 girls) [170]. Although Ertl states that capitellum fractures do not occur in children under the age of 10 years, the mean age in the series of Murthy et al. was 11.8 years, with an age range of 6–16 years [170, 171]. Fractures at this location result from a low-energy fall on outstretched hand (axial compression with the elbow in a semi-flexed position) or a fall or blow directly onto the elbow (direct impact) [171, 172]. No data are found concerning the occurrence of capitellum fractures due to non-accidental circumstances.
12.5 Radius and Ulna
12.5.1 General Aspects of Fractures of the Radius and Ulna
In children, fractures of the forearm are probably the most common fractures of the long bones, with an estimation of up to 40% to 50% of all paediatric fractures [81, 147, 173,174,175]. This is irrespective of type (complete, incomplete, or plastic deformation) or location (proximal, middle, or distal third) of the fractures. Forearm fractures are more common in boys than in girls [176].
Distal radius (and ulna) fractures are the most common forearm fractures in children under the age of 16 years and account for around 75% of all forearm fractures and 20–25% of all paediatric fractures (Fig. 12.45) [40, 81, 82, 174, 177,178,179]. Distal forearm fractures may be incomplete fractures (buckle/torus fractures and greenstick fractures), complete fractures (metaphyseal corner fractures or Salter-Harris fractures), or bowing fractures [61].

Distal fracture of the radius and ulna in a 6-year-old girl after a fall
Fractures of the distal radial and ulnar growth plate are often Salter–Harris I or II fractures (Fig. 12.46a, b). Although distal forearm fractures (excluding MCF) may occur at any age, they are predominantly seen during the growth spurt in puberty with peak ages in girls between 10 and 12 years and in boys between 12 and 14 years [180, 181]. Distal forearm fractures are 2–3 times more common in boys than in girls [181].

Bilateral Salter–Harris type II fracture (a and b) of the distal radius in a 13-year-old boy after a fall while skating
Fractures of the forearm shaft (transverse, oblique, or spiral) are the third most common fracture in children, after distal radius and supracondylar humerus fractures, and may account for around 15% of all paediatric fractures [177]. In other studies, lower percentages are mentioned, namely 3–6% of all paediatric fractures and around 20% of forearm fractures [82, 176]. Midshaft fractures are more frequently seen in young children [182].
Isolated fractures of the ulnar shaft are rare in children. A Parry or ‘nightstick’ fracture is a specific type of isolated fracture of the ulnar shaft which fulfils the following criteria: absence of radial involvement, transverse fracture line, distal from midshaft, and minimal displacement [183].
Olecranon fractures are uncommon in childhood and account for around 4% of paediatric elbow fractures (Fig. 12.47a, b). Olecranon fractures have been found in children between 5 and 17 years of age with a boy to girl ratio of 3.5:1 [176, 184, 185].

Five-year-old child who presented with pain in the elbow and limited range of motion after a fall onto an outstretched hand (FOOSH). (a) AP radiograph shows a fracture of the proximal radius head (arrow). (b) Lateral radiograph shows a fracture of the olecranon
Radial head and neck fractures account for around 1% of all paediatric fractures and for 5–10% of all elbow fractures. The median age of children with these fractures is 9–10 years of age and the boys to girls ratio is 1:1 [186].
Galeazzi fractures are distal radius fractures at the distal metaphyseal–diaphyseal junction with concomitant disruption of the distal radio-ulnar joint. This type is rare, compared to other distal forearm fractures, ranging from 0.3% to 3% of the distal radius fractures, with a peak incidence between 9 and 13 years [61, 187, 188].
A Monteggia’s fracture is a proximal ulna fracture or plastic deformation of the ulna with an associated radial head dislocation (Fig. 12.48). Just like the Galeazzi fracture, this type is rare and may account for 0.4% of all forearm fractures. The peak incidence is between 4 and 10 years [187, 189,190,191]. Combined Monteggia and Galeazzi fractures have been described to occur [192, 193].

Monteggia fracture, with the characteristic midshaft fracture of the ulna and dislocation of the head of the radius (open arrow), in a 2-year-old child after a fall from the couch (Courtesy of J. Davis, fellow Chadwick Center for Children and Families, San Diego, CA, USA)
Bowing fractures due to plastic deformation have been described to occur in all long bones (Sect. 12.2.1). The radius and ulna, followed by the fibula, are the most commonly affected bones [194].
The clinical signs of a forearm fracture, and in particular of a shaft fracture, are pain, pain at pressure, swelling, crunching (crepitus), restricted movement in wrist and hand, and possibly an aberrant alignment or the arm. This is seen mainly in complete fractures. In ‘bowing’ fractures and minimal greenstick fractures an aberrant position is seen (may be minimal), there is sensitivity when touched and restricted movement of the lower arm. Pain and swelling may be minimal, while crepitus may not be present at all [195].
12.5.2 Cause of Fractures of the Radius and Ulna
In children fractures of the forearm most commonly are caused by an indirect trauma, usually in a fall on the outstretched hand (FOOSH) (Table 12.6). This may happen when a child tries to break his/her fall by outstretching the arm and hand. As soon as the child lands on the extended arm, the main deforming force is transferred to the radius. Consequently, a fracture in the forearm may occur first in the radius, and then in the ulna. Often these are incomplete fractures, either greenstick or torus fractures. Fractures of the forearm are less commonly caused by a direct blow to the forearm, which is perpendicular to the forearm.
12.5.3 Manner of Fractures of the Radius and Ulna
Fractures of the forearm (radius and/or ulna), including MCF, have been described to occur before, during, or after birth. If sustained after birth, forearm fractures can occur due to accidental and non-accidental circumstances.
12.5.3.1 Before Birth
Fractures of the forearm, occurring in utero, have only very rarely been reported in the medical literature.
Onimus et al. reported the case of a patient (second pregnancy, first birth) who had been involved in a motor vehicle accident (frontal impact) when she was 7 months pregnant [196]. She was driving and wearing her seatbelt. Because of recurring metrorrhagia and uterine contractions in the period after the accident, a caesarean section was done. The neonate showed angulation of the left forearm. On X-ray a fracture line was seen with a callous already formed.
In 2 neonates the forearm fractures were related to the presence of an amniotic constriction band of the forearm:
-
Ho et al. described increased swelling to the right forearm distal to a congenital fibrous band in a 1-day-old neonate who was born at 28 3/7 weeks of gestational age [197]. The band was associated with underlying mid-shaft fractures of the right arm with pseudoarthrosis.
-
Angelis et al. described a 2-day-old preterm male, who was born at 31 weeks by caesarean section [198]. His left hand was swollen due to a constriction band with severe swelling and vascular compromise of the hand. Radiography showed a displaced fracture of the radius and ulna at the level of the band on the distal third of the forearm with pseudoarthrosis.
12.5.3.2 During Birth
In Sect. 2.6.2 and Table 2.9 an overview is given of fractures, that were sustained during birth. Only 1 dislocation of the elbow was reported by Bhat et al. [121]. No fractures of the forearm due to birth trauma are mentioned in the epidemiological studies, shown in Sect. 2.6.2. Only one case report concerning a birth-related radius fracture was found. Thompson et al. described a spiral fracture of the radius in a neonate after a complicated delivery due to shoulder dystocia. The child had a birth weight of 4,610 g [199]. The physical examination after the delivery showed bilateral cephalhaematomas, bruising of the face and forehead, a markedly oedematous left upper arm, and bruising of the right forearm. On X-ray, a spiral fracture of the right radius and a fracture of the left midhumeral shaft were seen.
12.5.3.3 After Birth: Accidental Circumstances
In mobile children, fractures of the radius and ulna are usually the result of accidental trauma, most commonly due to a fall on the outstretched hand (FOOSH) [81, 82]. Ryan et al. reviewed the findings in 929 paediatric patients, aged 0–17 years (mean age 8.4 years; male to female ratio 2:1) with isolated forearm fractures (2003–2006) [200]. They classified the circumstances as major trauma (motor vehicle collision; pedestrian or bicyclist struck by a moving vehicle; fall greater than patient height), minor trauma (Fall less than patient height; fall equal to patient height; other mechanisms not meeting criteria for major trauma severity classification), and unknown (unable to determine severity of trauma from documentation). Most fractures were determined to have occurred due to a minor trauma (58%), followed by unknown trauma (36.2%) and major trauma (5.8%). In the group of children aged 0–4 years (n = 150; 16%) falls from furniture were most common, in the 5–9 years group (n = 410; 44%) falls from monkey bars and in the 10–17 years group (n = 369; 40%) injuries due to organized sporting activities. Most fractures were fall-related (83%), while only 10% of the forearm fractures were caused by a direct blow to the forearm.
Other circumstances of forearm fractures, described in the medical literature are falls from high chairs (Sect. 13.3.5.5) [201] from shopping carts (Sect. 13.3.5.10) [202], and with baby-walkers (Sect. 13.3.5.8) [203].
12.5.3.4 After Birth: Non-accidental Circumstances
Fractures of the forearm occur frequently in non-accidental trauma. In several studies describing a series of children with non-accidental fractures, the radius and/or ulna belong to the most commonly affected bones:
-
Worlock et al. compared the findings in 35 children (28 children under the age of 18 months; 7 children between 19 and 60 months; 0 children above the age of 60 months) with non-accidental fractures to the findings in 826 children (19 children under the age of 18 months; 97 children between 19 and 60 months; 710 children above the age of 60 months) with accidental fractures [40]. Worlock et al. found non-accidental forearm fractures only in children under the age of 5 years. They found metaphyseal corner fractures of the forearm only in infants under the age of 18 months. Other non-accidental fractures in this group were 4 fractures of the shaft: 2 greenstick fractures, 1 transverse fracture, and 1 healing fracture (periosteal reaction). In the toddlers (19–60 months) 2 shaft fractures (1 oblique fracture and 1 healing fracture) and one distal fracture (greenstick fracture) were found.
-
Leventhal et al. evaluated the findings in 215 children under the age of 3 years with a total of 253 fractures [124]. The fractures were sustained in 24.2% in non-accidental circumstances and in 67.4% in accidental circumstances. In 8.4% the circumstances were not known. Concerning forearm fractures (n = 17) they found that 4 (23%) were due to non-accidental trauma and 12 (71%) to accidental trauma. In one child the circumstances were unknown. According to the authors non-accidental trauma should be suspected in a child under the age of 1 year with a fracture of the radius and/or ulna.
-
Loder et al. reviewed the findings in 1794 patients under the age of 20 years with injuries due to non-accidental trauma [204]. They found a total of 1053 fractures, of which 83 were fractures of radius and/or ulna. Of these 51 were found in children under the age of 1 year, 17 between 1 and 2 years, 13 between 3 and 12 years, and 2 between 13 and 20 years.
-
Van As et al. evaluated the physical findings in 1,037 children between 1 month and 13 years (median age 16.5 months, average age 44.8 months; male to female ratio 2:1) with injuries due to non-accidental trauma [205]. Of these children 121 had a total of 149 fractures (21 had multiple fractures). 15 children had fractures of the radius and/or ulna.
-
Pandya et al. did a large retrospective study, in children under the age of 4 years, in an urban level I paediatric trauma centre [130]. In the period 1998–2007 a total of 1485 children, 500 non-accidental (377 <18 months) and 985 accidental (425 <18 months) cases, were included. In the non-accidental group there were 23 (4.6%) radius and/or ulna fractures and in the accidental group 7 (0.7%) (p<0.001). In the under 18 months group this was, respectively, 19 (5.0%) versus 3 (0.7%). In the over 18 months group this was, respectively, 4 (3.3%) versus 4 (0.7%). Based on their findings the authors concluded that radius and/or ulna fractures were more common in the non-accidental group than in the accidental group, irrespective of the age of the child (p<0.001).
-
Ryznar et al. evaluated the findings in 135 children under the age of 18 months with a total of 216 forearm fractures. Most fractures were torus fractures (57%), followed by transverse fractures (26%), irrespective of the circumstances (accidental or non-accidental). Children whose only forearm fracture was a metaphyseal corner fracture were excluded from the study. Forty-seven (35%) children were evaluated by child protection teams. In 11 children (23%) it was concluded that the fractures were sustained in non-accidental circumstances. Children with non-accidental fractures were significantly younger than children with accidental fractures (7 months versus 12 months; p < 0.0001). Next to age, additional injuries, and an absent or inconsistent explanation were found more often in the children with non-accidental forearm fractures. The most common causing mechanism in accidental fractures was a fall (82%). Ryznar et al. also concluded that no particular type of forearm fracture was specific for non-accidental trauma.
-
Hermans et al analyzed the findings in 36 paediatric patients, between 2 and 16 years (mean age 8.9 years; range between 2.3 and 15.4 years) with isolated fractures of the ulna (a.k.a. ‘nightstick’ fracture) [183]. Only in 6 patients the fracture was caused by a direct trauma (2× kicked by another kid; 1× kicked by pony; 1× other kid fell on arm; 2× other kid stepped on arm). No association between the occurrence of an isolated ulna fracture and non-accidental trauma could be established by the authors.
Based on the findings in the foregoing literature one can conclude the following concerning fractures of the forearm:
-
The younger the child, the more likely a forearm fracture is sustained in non-accidental circumstances.
-
Metaphyseal corner fractures of the forearm most commonly occur in infants under the age of 18 months and are highly suggestive of non-accidental circumstances.
-
Except for metaphyseal corner fractures, differentiation between accidental and non-accidental circumstances is not possible, based on the type of forearm fracture.
-
In children under the age of 5 years radius and/or ulna fractures seem to be more commonly sustained in non-accidental than in accidental circumstances.
-
In forearm fractures one should always consider non-accidental trauma in non-mobile children/children who do not (yet) walk.
-
One should also consider non-accidental circumstances if the explanation of how the fracture occurred does not match the known trauma mechanism(s) (inconsistent history) or when other physical findings are found, which are suggestive of non-accidental circumstances (concomitant injuries).
12.5.4 ‘Nursemaid’s Elbow’
12.5.4.1 General Aspects of the ‘Nursemaid’s elbow’
‘Nursemaid’s elbow’, or pulled elbow syndrome, is the popular name for what initially was known as radius head subluxation (RHS), but at the moment as annular ligament displacement (ALD) [206]. It is one of the most common paediatric joint injuries, which accounts for over 20% of upper extremity orthopaedic injuries in children [207]. The recurrence rate is about 25% [208]. Bilateral occurrence of the nursemaid’s elbow has been described but is very rare [209, 210]. A nursemaid’s elbow typically occurs in children between 1 and 4 years of age [211]. The youngest child, reported in the medical literature is an infant of 2 months, with several reports of children under the age of 6 months [208, 212, 213]. Nursemaid’s elbow is also seen in older children, although seldom in children over the age of 7 years [212]. In older children subluxation is prevented by a thicker and stronger distal attachment of the annular ligament [214].
Rudloe et al. evaluated the findings in 3170 children (median age 2.1 years; 50% between 1.5 and 2.8 years) with a nursemaid’s elbow. Girls to boys ratio was 3:2 [215]. In almost 60% of the children the left arm was involved.
Vitello et al. reviewed the findings in 1,228 children under the age of 6 years (mean age 28.6 months; 44% between 18 and 29 months), who visited an emergency department and were diagnosed with a nursemaid’s elbow [211]. 137 children visited the ED more than 1 time (up to 7 times in one child) because of a nursemaid’s elbow. Girls to boys ratio was 3:2. Most of the included children were over the 75th percentile for weight and more than one quarter were over the 95th percentile in each gender. 60% of the subluxations were found in the left elbow.
The radiological examination, which is usually not required due to the obvious clinical history, generally shows no dislocation. When the radiograph is taken, positioning of the arm by the radiographer will usually reduce the nursemaid’s elbow.
12.5.4.2 Cause and Manner of the ‘Nursemaid’s elbow’
‘Imagine a parent innocently swinging around a toddler ... a yank on an outstretched arm to keep a preschooler from falling ... a caregiver attempting to move a reluctant child by dragging the child by the hand ... a helping hand to lift a young child up over the curb or a high step. None of these activities is ever intended to hurt a child, yet the result of these specific activities send many children with anxious parents and caregivers to emergency departments and unscheduled pediatrician appointments each year’ [216].
Nursemaid’s elbow is caused by traction along the longitudinal axis of the arm or a sudden pull of the extended pronated arm. Initially, it was assumed that due to the traction/pulling the radial head moves out of the weak annular ligament and capitellum, resulting in slipping over and subluxation of the radial head into the supinator muscle and annular ligament [212, 217]. According to Browner, however, it is not a subluxation of the radius head that is responsible for the nursemaid’s elbow, but a displacement of the annular ligament (Fig. 12.49) [206]. The traction/pulling causes the annular ligament to slip over the head of the radius and come to rest in the radial–humeral joint between the radius and capitellum, where it becomes entrapped.

Subluxation of the annular ligament due to a sudden longitudinal traction
It is not clear how much force is needed to cause a nursemaid’s elbow. According to the Pediatric Society of North America (POSNA) only very little force is needed to pull the bones of the elbow partially out of place which explains why, according to POSNA, the nursemaid’s elbow is so common. Others, however, are of the opinion that it needs pulling the child’s arm with great force to cause a nursemaid’s elbow [212]. Concerning the causing mechanisms, it does not matter whether a nursemaid’s elbow is the result of a subluxation of the radius head or of a displacement of the annular ligament.
Rudloe et al. analyzed the causing mechanisms in 3,170 children (median age 2.1 years, with 50% of the children between 1.5 and 2.8 years) [215]. They found that the nursemaid’s elbow in 63% was due to traction and in 17% due to non-traction. In 19% the causing mechanism was unknown or undocumented. In the traction group (n = 2011) several traction/pulling mechanisms were identified:
-
Lifting the child by one arm or both arms (28.3%)
-
‘Wrestling’ or ‘roughhousing’ (12.3%)
-
Swinging the child by one arm or both arms (9.2%)
-
Placing the child into and out of a seat (4.3%)
Male caregivers were more likely to be involved when a child was swung by the arms, lifted or ‘wrestled’/’roughhousing’ with. Mechanisms more common for female caregivers included the child pulling away from the parent, tripping (the child tumbling while being held by the hand or wrist), and getting the child dressed (e.g. pulling a child’s arm through a coat sleeve with too much force).
In the non-traction group (n = 547) the majority occurred during a fall. In 30 children the nursemaid’s elbow occurred due to rolling over in the bed, while the arm was caught under the body. Most of these 30 children were under the age of 1 year and 22 of them were girls.
Li et al. analyzed the findings in 69 children (median age 2.4 years; 50% between 1.5 and 3.6 years) with nursemaid’s elbow due to non-axial traction mechanisms [218]. The most commonly reported causing mechanisms were falls (57%), direct hits to the elbow (16%), and rolling over (7%).
The predominance of the nursemaid’s elbow in the left arm can most probably be explained by the fact that most adults are right-handed holding the child’s left hand or wrist [207].
‘Rolling over’ is probably the most common mechanism in infants under the age of 1 year. The ‘rolling over’ mechanism was first described by Newman, who reported 4 infants under the age of 6 months with the ‘rolling over’ mechanism [213]. In 3 of these 4 infants it was not a spontaneous ‘rolling over’, but a forced ‘rolling over’, in which the child was rolled over by another (once an older sister and two times the mother). Newman also reported 1 infant under the age of 6 months who had been lifted by the arm and another infant whose arm was pulled by a sibling.
Newman stated about the ‘rolling over’ mechanism in infants: ‘Although child abuse should always be kept in mind when there is unusual trauma in the young baby, none of the instances described was thought to represent abuse’. In other words, knowing the causing mechanism of a nursemaid’s elbow (e.g. traction/pulling or rolling over) does not imply knowing whether the nursemaid’s elbow was sustained due to accidental or non-accidental circumstances.
12.6 Fractures of the Hand
12.6.1 General Aspects of Fractures of the Hand
Approximately one-fifth of all hand injuries in children are fractures [219]. Fractures of the hand are common injuries in children and adolescents and account for 15% of all paediatric fractures and for 2.3% of all paediatric ER visits [220, 221]. Boys sustain hand fractures more often than girls in an almost 3:1 ratio [220]. The incidence of hand fractures is low in infants, but increases with age.
Vadivelu et al. found that hand fractures occurred in toddlers in 34 per 100.000 per year, while hand fractures in children aged 11–18 years increased up to 663 per 100.000 per year [222].
Kreutz-Rodrigues et al. did a review of frequency and pattern of paediatric hand fractures in a 27-year period [223]. The data of 4356 hand fractures in patients under the age of 18 years (mean age 12.2 years) (categorized in 3 age groups: 0–5, 6–11, and 12–17 years) were evaluated. Most hand fractures were found in the 12–17 years group (n = 2775, 64%), followed by the 6–11 years group (n = 1347, 31%) and finally the group of children under the age of 5 years (n = 234, 5%). Most hand fractures were found in the proximal/middle phalanx (48%), followed by metacarpal (33%), distal phalangeal (12%), and intra-articular metacarpophalangeal/proximal interphalangeal/distal interphalangeal joints (7%). Proximal/middle phalangeal fractures were the most common in all age groups.
Chung and Spilson found that in children, aged 5–14 years, the overall incidence of hand fractures was 546 per 100,000 per year [224]. The incidence of carpal fractures was 131 per 100.000 per year, of metacarpal fractures 250 per 100.000 per year, and of phalangeal fractures 165.6 per 100.000 per year. According to Chung and Spilson the highest incidence of phalangeal fractures occurs in the 0–4 year age group (around 0.2% of children in that age group. Metacarpal fractures and carpal fractures occur slightly more rarely, at a rate of approximately 0.1% of children overall.
12.6.2 Cause and Manner of Fractures of the Hand
Fractures of the hand are usually caused by a direct impact, either by being hit with an object or by punching, or by crushing with a heavy object. Fractures may also occur due to hyperextension or hyperflexion [225].
Fractures of the hand can be sustained in accidental and in non-accidental circumstances.
In young children accidental crush injuries to the digits are common, e.g. after getting stuck in the door (Fig. 12.50) [226]. In older children, hand fractures usually are sustained in accidental circumstances, e.g. in sports and play-related trauma (Figs. 12.51, 12.52a–c and 12.53) [220, 226]. In adolescents fractures of the hands are often described to occur in non-accidental circumstances, e.g. in fights, and can be the result of self-defence and/or fighting back [220].

Four-year-old child whose finger got caught in the door opening. Radiography shows a crush fracture of the distal phalanx of the second digit (inset)

Fracture of the proximal phalanx (open arrow) of a 4-year-old girl who had a television topple on her hand

(a) Two-year-old girl who had a drawer fall on her hand while playing. Radiological examination revealed a fracture of the capitate bone (Reprinted with permission [465]) (b) Postero-anterior view of the hand shows the fracture of the capitate bone. (c) Coronal STIR-weighted MRI shows bone oedema at the location of earlier-mentioned capitate fracture (open arrow); however, also of the hamate bone (arrow)

Five-year-old child who sustained a trauma, a heavy object fell on his hand, while playing in the schoolyard. Radiograph shows an intra-articular communitive fracture of the head of the proximal phalanx of the 5th finger (inset)
Although the hand is the second most frequently injured part of the body in older children and adolescents, the number of studies on fractures of the hands in children, especially in association with non-accidental trauma, is limited compared to other bony injuries [224, 227,228,229,230,231,232].
According to Johnson et al. in the paediatric population the hands can be considered to be a target organ in case of non-accidental trauma (child abuse) [233]. They evaluated the findings in 944 reports of non-accidental trauma. Injuries involving the hands were found in 94 children. Of the 94 children 18 (20%) were admitted to hospital, because of burn injuries (17), apnoea (2—once combined with a bite mark and once with bruising), fractures (2), bruising (2), crushing injury (1—fingers slammed in a door). In 19 children (2%) the hands were the only location with inflicted injuries: burns (8), bruises (2), human bite marks (2), erythema (2), fractures (2), swelling (2), and laceration (1). The fractures were found in a 5-year-old girl after being hit on the hand and in an 11-year-old girl with an unknown history. Despite the fact that the hand may be a target organ, hand fractures seem to be relatively rare compared to other hand injuries (Table 12.7). Of the ‘hand only’ group 5 children were admitted to hospital.
Unexplained or unexplainable fractures of the hands in children under the age of one year are thought to have a strong association with non-accidental trauma (Figs. 12.54a–e, 12.55a, b and 12.56a, b) [10, 234,235,236].

Four-month-old sibling of an abused index case. (a) Radiograph of the left hand shows slight irregularity and subperiosteal new bone formation at the base of MC-III (inset). (b) AP radiograph of the right knee shows a metaphyseal corner fracture of the proximal tibia (arrow). (c) Lateral radiograph shows the posterior location of the fracture (arrow). Repeat skeletal survey shows (d) a healing fracture of the base of MC-III (inset) and (e) a healed metaphyseal corner fracture of the proximal tibia

(a) One-and-a-half month old girl was found dead in her crib. Radiological examination of the hands revealed a torus fracture at the base of the proximal phalanx of the third finger of the right hand (see inset). (b) Radiograph of the finger, sampled at autopsy. The radiograph has been taken with a mammography system, because of its high resolution

Four-month-old infant suspected of being a victim of child abuse. (a) Radiograph of the right hand shows a buckle fracture of the base of MC-I (inset). (b) Radiograph after 2 weeks clearly shows callus formation (inset)
Nimkin et al. evaluated 11 infants under the age of 10 months with fractures of hands and feet, due to non-accidental trauma [235]. A total of 22 fractures were noted. Six infants had a total of 15 fractures of the hands (6× metacarpal and 9× proximal phalangeal fractures). The authors found predominantly torus fractures, which according to the authors are consistent with forced hyperflexion. Seven infants had three or more additional fractures of long bones of the upper and lower extremities, and seven infants had additional fractures of the ipsilateral extremity. Only one child showed clinical symptoms.
Despite the supposed strong association with non-accidental trauma Pandya et al. reported in a comparative study an OR of 0.3 to find these fractures due to accidental circumstances compared to non-accidental circumstances in infants younger than 18 months old and an OR of 0.5 in children older than 18 months [130]. The inclusion by the authors of children aged 0–18 months means the inclusion of both pre-mobile and mobile children in the same group. The findings in pre-mobile and mobile children were not split. Because of this it is not possible to draw definitive conclusions concerning the circumstances under which hand fractures were sustained in the pre-mobile group.
Hand fractures have only rarely been reported in studies, concerning infants and children who underwent a skeletal survey for the evaluation of suspected non-accidental trauma [10, 236,237,238]. Barber et al. reported on a study on 567 children, of whom 313 suffered a total of 1,029 fractures [10]. Seven (2.2%) children had fractures of the hand. In the study by Kleinman et al. 225 out of 365 children had one or more fractures on the skeletal survey. Five (2.2%) children had a total of 10 fractures of the hand [236]. Karmazyn et al. studied 930 children of whom 317 had a total of 899 fractures. One infant had 6 (0.7%) fractures of the hand [237]. In the, by far largest, the study of Lindberg et al. out of 2890 children 1208 had one or more fractures. Fifteen of them (1.1%) had a total of 20 fractures of the hand [238]. In this study, there were 7 children with either a fracture to the hand or foot, but it was not possible to discriminate as the report spoke of, e.g. a digital fracture.
12.7 Femur
12.7.1 General Aspects of Femur Fractures
The femur is the largest and strongest bone in the body. The proximal part of the femur (caput femoris—head of the femur) articulates with the acetabulum of the pelvis to form the hip joint and the collum femoris (neck of the femur) connects the caput with the shaft. The distal end of the femur is characterized by the presence of the medial and lateral condyles, which articulate with the tibia and patella to form the knee joint.
Fractures of the femur are relatively rare in paediatric patients and account for around 2% of all paediatric fractures. Fractures of the shaft are much more common than fractures of the proximal or distal femur. The first peak of occurrence is found in the first 2–3 years of life and the second peak is in adolescence [239].
Buess et al. analyzed the findings in 100 consecutive children (0–18 years; mean age 7.3 months) with femoral fractures [240]. Boys to girls ratio was 1.85:1. Only one patient was older than 16 years, a severely handicapped spastic child with cerebral palsy with a pathological fracture. Buess et al. found 3 peaks: 0–4 years, 6–10 years, and 13–15 years. Fractures in the youngest children most likely occurred due to accidental falls (usually low energy trauma). Traffic accidents (high energy trauma) were seen mainly in the group of school children, whereas sports-related fractures were seen mainly in adolescents. Pathological fractures were found in 8 children: spastic cerebral palsy in four children, achondroplasia, bone cyst, poliomyelitis, and posttraumatic osteoporosis each in one child. In two children in the youngest group the femur was due to non-accidental trauma.
Brown and Fisher evaluated the occurrence of femur fractures in 2753 children under the age of 6 years by using the ‘1997 Kids’ Inpatient Database’ [241]. They did not differentiate between fractures of the proximal femur, shaft, and distal femur. They found that the occurrence of femur fractures was highest in the first year (especially during the 3rd month of life, slightly decreasing between the 4th and 11th months) and between the ages of 20–40 months. In the children under 1 year of age the boys to girls ratio was 1:1, whereas in the older children more boys than girls sustained femur fractures. According to Brown and Fisher their findings suggest that an infant has as great a chance of sustaining a femur fracture due to non-accidental trauma as an older child dominantly does due to accidental trauma because of their increasing motoric abilities, e.g. climbing, and their increasing mobility.
Loder et al. evaluated the characteristics of femur fractures in 9963 children and adolescents under the age of 18 years: 1076 fractures between 0 and 2 years (11%), 2119 between 2 and 5 years (21%), 3237 between 6 and 12 years (33%) and 3528 between 13 and 18 years (35%) [242]. Boy to girl ratio was almost 2.5:1. Of the 9963 fractures, 9458 were closed. Of the closed fractures 70% were shaft fractures, 12% were proximal and 18% were distal fractures. Shaft fractures occurred in 2493 (81%) of 3096 closed fractures in children under the age of 6 years compared to 3940 (65%) of 6080 in children aged 6–18 years (P< 0.001). Fractures of the proximal femur occurred twice as often in the 2 older age groups (aged 6–18 years) compared with younger children under the age of 6 years. The fewest fractures of the distal femur were found in the 2–5 years old group. Open fractures were found in 505 cases. 70% of the open fractures occurred in the adolescent group. Fractures in younger children most likely occur due to accidental falls (usually low energy trauma), whereas those in older children most commonly occur as a result of motor vehicle accidents (high energy trauma). Approximately 2% of all children sustained the fracture (location not further specified) due to non-accidental trauma. Nearly all of these children were under the age of 2 years. In these age group 15% of all femoral fractures were due to non-accidental trauma.
Petković et al. evaluated the findings in 143 children (average age 8.6 years) with femur fractures [243]. Sixty-five percent were shaft fractures, 21% were fractures of the proximal fracture and 14% of the distal fracture. Boys to girls ratio was 3.2:1. The fractures occurred during play and sport activities in 67 children and in traffic accidents in 64 children. Pathological fractures were found in 12 children.
Baldwin et al. compared the findings in 70 children with non-accidental femur fractures to 139 children with accidental femur fractures [244]. Children with accidental femur fractures more often had shaft fractures (46% versus 66%), children with non-accidental femur fractures more often had distal femur fractures (37% versus 20%). No difference was found between both groups concerning proximal femur fractures. They identified 3 risk factors that could be helpful in differentiating non-accidental from accidental femur fractures (Fig. 12.57):
-
Age younger than 18 months.
-
Physical and/or radiographic evidence of prior trauma.
-
History suspicious for non-accidental trauma.

Algorithm for determining whether a femur fracture stems from abuse or accidental trauma as presented by Baldwin et al. [244]. Percentages refer to the risk of an abusive femur fracture, the Odds Ratio is the result of a multiple logistic regression model with a number of risk factors (risk factors: age younger than 18 months, physical and/or radiologic evidence of prior trauma, and suspicious history)
Volkman reviewed the findings in 228 children under 2 years of age with a total of 235 femoral fractures (including 6 bilateral fractures and 1 case with 2 fractures in the same limb). Volkman found that the overall percentage of non-accidental femur fractures was 10.9% (25 of 228 children). In children under the age of 6 months, 25.8% (15 of 58 infants) of the fractures were the result of non-accidental trauma, under the age of 1 year, 16.4% (20 of 122 infants) and over 1 year, 4.7% (5 of 106 children). The percentage of suspicious or indeterminate cases was 25.8% (59 of 228 cases) and of accidental cases 74.2% (169 of 228 cases). Proximal femur fractures were found in 36 children, midshaft fractures in 134 children, distal femur fractures in 65 children:
-
Of the proximal fractures 6 were the result of non-accidental trauma, and 26 of accidental trauma. In four children the circumstances were not known.
-
Of the midshaft fractures 15 were the result of non-accidental trauma, and 97 of accidental trauma. In 22 children the circumstances were not known.
-
Of the distal femur fractures 10 were the result of non-accidental trauma, and 46 of accidental trauma. In nine children the circumstances were not known.
Volkman concluded that several factors could help differentiate between non-accidental and accidental femur fracture, namely age under 12 months, non-ambulatory status, delayed presentation, concurrent injuries, bilateral fractures, and unknown/inconsistent history of mechanism of injury.
Engström et al. evaluated the occurrence of femur fractures in Swedish paediatric patients under the age of 16 years (n = 709) [245]. Most fractures were located in the shaft (64%), followed by the distal femur (27%) and the proximal femur (9%). Boys to girls ratio was almost 2:1. Most fractures were observed in boys aged 2–3 years and in adolescent boys, while in girls the fractures were evenly distributed. In younger children the fractures were most commonly sustained in falls, whereas in adolescents traffic-related accidents were the most common.
Rokaya et al. evaluated the findings in 104 children (mean age 5.5 years; boys to girls ratio 1.6:1) with femur fractures [246]. 65.3% were fractures of the shaft, 18.2% of the proximal femur and 16.3% of the distal femur. Most occurred due to accidental falls from varying heights (ladder, rooftop, cliff, horse, bicycle) or during sporting activities. In 4 children the fracture occurred in non-accidental circumstances (physical assault).
Valaikaite et al. reviewed the findings in 348 children with a total of 353 femur fractures [247]. The mean age was 7.5 years, ranging from 0 to 15 years. 37 children were under the age of 1 year, 112 between 1 and 5 years of age, 125 between 6 and 11 years, and 74 between 12 and 15 years. Except for children under the age of 1 year, most fractures occurred in male patients (69%), with boys to girls ratio of 2.2:1. In the group of children under 1 year of age 68% were girls (girls to boys 2.2 to 1). Fractures of the shaft were most common in all ages (72.2%), followed by fractures of the distal femur (17.9%) and the proximal femur (8.2%). In 1.7% the location was not reported in the medical records. Femoral fractures were mainly due to low-energy trauma in neonates and infants, to road accidents and low-energy trauma in preschool children, to sports accidents (especially skiing) in school-age children, and to road traffic accidents in teenagers. 94.9% were closed fractures. Pathological fractures were found in 29 cases (13× shaft, 6× distal femur, 10× proximal femur).
12.7.2 Fractures of the Proximal Femur
12.7.2.1 General Aspects of Fractures of the Proximal Femur
Fractures of the proximal femur are uncommon in children. They account for less than 1% of all paediatric fractures [239, 248,249,250]. Boy to girl ratio is 2.5:1 [251].
Fractures of the proximal femur and hip fractures are sometimes used as synonyms [252]. This can be confusing because hip fractures can also be defined as fractures in 1 or more of the bones, that form the hip joint (proximal femur and pelvis, especially the acetabulum—see also Chap. 11).
Proximal femur fractures are classified as transepiphyseal, transcervical, cervicotrochanteric, and intertrochanteric fractures (Fig. 12.58) [248, 250, 252, 253]:
-
Transcervical fractures (Delbet type II) are fractures through the mid-portion of the femoral neck. This is the most common type in children and adolescents, accounting for 40–50% of fractures of the proximal femur in paediatric patients. Miller identified three peak ages for type II fractures: 2–4 years of age, 8 and 9 years of age, and 12 and 13 years of age [248, 254].
-
Cervicotrochanteric fractures (Delbet type III) are fractures through the base of the femoral neck and are found in 25–35%.
-
Intertrochanteric fractures (Delbet type IV) are fractures between the greater and the lesser trochanters and account for 6–15%.
-
Transepiphyseal fractures (Delbet type I) are fractures through the proximal femoral physis, representing a Salter–Harris type I of the proximal femur. This type may occur with or without dislocation of the femoral head. This is the least common type (less than 10%). However, in infants and young children under the age of 2 years and in children aged 5–10 years this type is more common than in children between 2 and 5 years and above 10 years.

Femoral neck classification according to Delbet
Due to the vascular anatomy and the active growth plate, specifically in skeletally immature young children, fractures of the proximal femur can be associated with severe complications such as premature physeal closure, coxa vara or valga, avascular osteonecrosis, mal- or non-union, limb shortening, and arthritic changes [253, 255,256,257,258,259].
12.7.2.2 Cause of Fractures of the Proximal Femur in Normal Bone
Because of the high bone mineral density the proximal femur in children is very strong (except for the physis). A severe high-energy trauma will be necessary to fracture the proximal femur [259, 260]. Up to 90% of all fractures of the proximal femur are caused by a high-energy trauma [248, 250]. In children 30–85% of the proximal femur fractures are associated with other often major injuries, reflecting the severity of the trauma [248]. Associated injuries are head and/or facial injuries, abdominal injuries (splenic lacerations, retroperitoneal haemorrhage), intra-pelvic visceral injuries, perineal injury, and other skeletal injuries, e.g. pelvic ring or acetabular fractures, hip dislocation, or other femur fractures [248, 251, 256, 261, 262].
Several mechanisms, resulting in a high-energy trauma to the proximal femur, can be deduced from the literature. These may result from direct trauma, e.g. due to a direct blow to the hip, or from indirect trauma, e.g. due to axial loading, hyperabduction, or torsion (see Sect. 12.7.2.3). According to Ogden et al. birth-related fractures of the proximal femur in neonates most probably are due to a combination of hyperextension, abduction, and rotation during forceful traction [70].
If it is suspected that a fracture of the proximal femur resulted from a low-energy trauma, (e.g. a fall from standing height or a twisting mechanism) one must consider the presence of an underlying disorder with weakened bone, e.g. metabolic bone diseases, benign and malignant bone tumours, or non-accidental trauma (see also Sect. 12.7.3.3.4) [250, 251, 263].
12.7.2.3 Manner of Fractures of the Proximal Femur
12.7.2.3.1 Before Birth
No reports concerning proximal femur fractures, sustained before birth, were found.
12.7.2.3.2 During Birth
Birth-related injuries of the proximal femur are probably rare, and have only been described in single case reports or small series of cases.
The majority of these studies focus on proximal femoral epiphysiolysis of the femur (= Delbet I, transepiphyseal fracture) [264,265,266,267,268,269,270,271] [70, 248, 252]. This most commonly occurs due to a difficult and traumatic breech delivery and is caused by a combination of hyperextension, abduction, and rotation during forceful traction of the leg [70]. ‘Large for date’ neonate probably are more at risk [272]. Clinically it is usually diagnosed soon after birth as the neonate tends to keep the extremity limp in a position of flexion, abduction, and external rotation. Clinically passive motion is painful and swelling can be present.
12.7.2.3.3 After Birth: Accidental or Non-accidental Trauma
After birth fractures of the proximal femur may occur in accidental and in non-accidental circumstances. There are two peaks of occurrence: children under the age of 2–3 years, and older children above the age of 11 years and in adolescents [251, 253].
Non-accidental fractures of the proximal femur are less common than non-accidental fractures of the shaft and the distal femur. According to Baldwin et al. diaphyseal femur fractures are found more often in children with accidental trauma than in children with non-accidental trauma, while distal femur fractures were more common in children with non-accidental trauma than in children with accidental trauma [244]. They found no difference in the occurrence of proximal femur fractures between both groups.
In children under the age of 2–3 years non-accidental circumstances should always be considered in case of fractures of the proximal femur, especially if a history of a plausible accident is lacking or if the described accident can be considered to be a minor trauma with insufficient force to explain the fracture [75, 244, 252, 273,274,275].
-
Jones et al. reported two girls with hip problems [76]. The first girl was seen at the age of 9 months at a well-child check-up and the mother stated that she was not rolling over or bearing weight on her legs, which she did before. A radiograph showed that the femoral head was seated in a normal acetabulum, but that the neck was displaced cranially and laterally. A skeletal survey showed healing metaphyseal corner fractures of the proximal humerus bilaterally, a healing metaphyseal corner fracture of the right distal humerus and a metaphyseal corner fracture of the left proximal tibia. Several rib fractures were also found. Her mother’s boyfriend eventually admitted that he forcefully pulled the arms backward in anger and that he caused the hip injury during a frustrated diapering attempt by abducting the child’s thigh and then pushing the shaft towards her acetabulum. The second girl was seen at the age of 2 months. It was suspected that she had a displaced hip. On X-ray, it was seen that her left proximal femur was displaced cranially and laterally. There were signs of early callus. At the age of 4 months proximal and distal parts of both femurs had periosteal layering. There were also healing rib fractures visible and healing fractures of the distal right radius and healing metaphyseal corner fractures of the distal right and left femur, both proximal tibias and possibly the distal tibias. No indication was found for a primary skeletal abnormality. Jones et al. noted that this type of injury can look identical to epiphyseal separations due to birth trauma.
-
According to Beaty non-accidental trauma should always be excluded if a Delbet type 1 fracture is found in an infant [248].
-
Gholve et al. described a 3-year-old girl with a femoral neck fracture, which occurred due to non-accidental circumstances [275]. The authors stated that femoral neck fractures usually are sustained in a high-energy trauma or, less common due to pathological conditions (Sect. 12.7.3.3.4). However, the possibility of non-accidental circumstances should be considered if there is no indication of one of these.
-
Pastor et al. presented a 5-month-old boy with a 4-day history of diagnosed upper respiratory illness and a new 2-day history of decreased left hip motion and pain [274]. The decreased movement and pain were caused by a fracture of the femoral neck. A full skeletal survey indicated a metaphyseal corner fracture of the right distal femur and a periosteal reaction of the right fibula shaft. The boy also had evidence of fractures of the left distal femur and the left proximal fibula in various stages of healing. Externally visible injuries were not described.
-
Kembhavi and James described the findings in a 4-year-old girl with bilateral intertrochanteric fractures [273]. Initially, it was thought that the fractures were due to a fall from height. However, the child had multiple fractures in different stages of healing: relatively minimal vertebral wedge compression fractures, combined with older fractures (right-sided supracondylar humerus fracture, left proximal ulna fracture, and right-sided proximal tibial metaphyseal fracture with physeal injury). It was concluded that the fractures were sustained due to non-accidental circumstances. The child had no externally visible injuries.
-
Shalaby-Rana et al. reported eight children, aged 2.5–26 months (mean age 10 months) with a total of 10 fractures of the proximal femur physis [75]. All children showed lateral displacement of the proximal femur. Two children, aged 3 and 8 months, had bilateral fractures of the proximal femur. In seven of the eight children non-accidental trauma was confirmed. Six of them, aged 2.5–10 months, had other fractures, most commonly rib fractures or metaphyseal corner fractures. In two children no other fractures were found. One child, aged 13 months, was disciplined by his father by slapping his thigh. Eighteen days before presentation the father had punched the child’s left thigh, after which the child stopped bearing weight. In one child, aged 26 months, it was concluded that the child was medically neglected, because the parents did not seek medical care until 2 weeks after the child stopped bearing weight.
In children above the age of 11 years and in adolescents up to 90% of all proximal femur fractures occur in accidental circumstances, usually a high energy trauma with a high-energy transfer, like motor vehicle accidents, falls from great heights, or high-impact sports trauma [250, 259, 260]. Transcervical fractures (Delbet type II fractures) most commonly occur due to severe trauma with a high-energy transfer/high-velocity accidents involving a direct impact, such as motor vehicle accidents, or pedestrian-vehicle accidents. Delbet type II fractures may also occur due to falls from height [248, 253]. Three peak ages can be identified for type II fractures: 2–4 years of age, 8 and 9 years of age, and 12 and 13 years of age [248].
Cervicotrochanteric fractures (Delbet type III) and intertrochanteric fractures (Delbet type IV) also demand trauma with a high energy transfer [248].
According to Beaty, a severe trauma is needed to sustain a trans(epi)physeal fractures (Delbet type I fracture). This may occur during birth (see Sect. 12.7.2.3.2) and after birth due to an accidental trauma with a high-energy trauma or in seizures [248, 276]. Two peak ages have been described: infants and young children under the age of 2 years and children between 5 and 10 years of age.
In healthy, mobile children, usually young athletic adolescents, stress fractures of the proximal femur due to repetitive activity such as running, jumping, and during sports have been described. These children typically present with ongoing pain, increasing with physical activity. Because they are so rare, a broad differential diagnosis has to be considered, and it can be hard to diagnose these stress fractures [277,278,279,280,281,282,283,284,285,286,287,288,289,290].
Rinat et al. described the occurrence of fractures of the proximal femur (Delbet type II and III) in two girls aged 10 and 12 years, due to a trauma caused by (suspected) hyperabduction while sliding on a water slide [291].
The occurrence of Delbet-type I fractures has been described to occur during attempted closed reduction of a traumatic hip dislocation with a nondisplaced physeal fracture in adolescents [292,293,294].
12.7.2.3.4 After Birth: Diseases with an Increased Risk of Fractures of the Proximal Femur
Pathological fractures of the proximal femur are very rare in paediatric patients but may occur in malignant and in benign medical conditions [263]. Physicians should consider a pathological fracture in a child in case of a (confirmed) history of a minor or insignificant trauma (a trauma with a low transfer of energy), or in case of the suspected presence of abnormal findings on radiological imaging.
Pathological fractures of the proximal femur in children, caused by a minor trauma can be found due to generalized changes in mineral density of the bone (e.g. osteogenesis imperfecta) or due to localized changes in density (e.g. in infections, bone cysts, bone tumours, and tumour-like lesions) [263, 295,296,297,298,299,300]. The proximal femur is one of the most common locations for benign bone tumours in children.
Shrader et al. identified pathologic femoral neck fractures, including two basicervical fractures, in 15 children (9 boys, 6 girls) ranging in age from 18 months to 15 years (mean age, 9 years) between 1960 and 2000: fibrous dysplasia (n = 5 children), unicameral bone cyst (n=2), Ewing's sarcoma (n = 2), osteomyelitis (n = 2), leukaemia (n = 1), rhabdomyosarcoma (n = 1), osteogenesis imperfecta (n = 1), and osteopetrosis (n = 1) [263]. According to authors paediatric patients with pathologic fractures of the proximal femur are at significant risk for complications.
Femoral neck fractures may also occur in children with osteopenia secondary to other conditions, e.g. cerebral palsy or muscular dystrophy.
12.7.3 Fractures of the Femoral Shaft
12.7.3.1 General Aspects of Fractures of the Femoral Shaft
Shaft fractures are the most common femur fractures in children, especially midshaft fractures, accounting for over 60% of all paediatric femur fractures [301]. They account for almost 2% of the fractures in children [242, 245, 302,303,304,305,306]. This includes subtrochanteric and supracondylar fractures (fractures of the upper and lower third of the shaft) [302].
Femoral shaft fractures are more common in boys compared to girls with a ratio of approximately 2.6:1 [307]. Two peak ages can be distinguished, especially in boys: toddlers aged 2–4 years and adolescents above the age of 12 years [242, 245, 304, 308, 309].
The incidence of femoral shaft fractures in children is estimated to be between 11 and 20 per 100.000 children worldwide. In 1999 Hinton et al. reported an annual incidence of 19.15 per 100,000 children [304]. The incidence of femoral shaft fractures seems to have decreased in the last decades. Based on data from the Swedish National Hospital Discharge Registry (SNHDR) von Heideken et al. reported that from 1987 to 2005 a total of 4984 children, aged 0–14 years, had a diagnosis of a femur shaft fracture [303]. They found an overall annual incidence of 16.4 cases (95% CI, 15.9–16.8) per 100,000 children, where during the observed period, the annual incidence of femur shaft fractures declined on average with 3% per year with a total decrease of 42%. The authors do not give an explanation for this decrease but similar findings have been reported in the United Kingdom by Bridgman and in the United States by Wilson and Mooney and Forbes [306, 310]. The authors do suggest that it might be related to the fact that children tend to be less physically active, the increased role of injury prevention research, and safety education campaigns.
In the United Kingdom, Talbot et al. identified in 2018 a total of 1852 isolated, closed fractures of the femoral shaft in children from birth to 15 years of age, indicating a mean annual incidence was 5.82 per 100 000 children (95% confidence interval (CI) 5.20–6.44). The age of peak incidence was two years for both boys and girls; this decreased with increasing age [311].
12.7.3.2 Cause of Fractures of the Femoral Shaft
As stated before, the femur is the largest and strongest bone in the body. Above that, the femoral shaft is protected against blunt force trauma by the surrounding muscles. If a fracture of the shaft is found in a paediatric patient with normal bone, the fracture must have been caused by a trauma with a high energy transfer, either a direct blow to the shaft or an indirect trauma, transmitted at the knee. The protective muscles, however, also are responsible for the displacement, which is often seen in fractures of the femur shaft [312, 313].
The high-energy transfer, which is needed to fracture the femur, can be illustrated by the fact that especially in accidental circumstances (see Sect. 12.7.3.3.3) the fracture often is associated with other injuries, due to a high-energy transfer, e.g. intracranial or intra-abdominal injuries. These injuries regularly result in life-threatening circumstances [313].
Fractures of the femur may also occur in children with bone diseases with an increased risk of fractures (pathological fractures) due to a lesser amount of force (see Sect. 12.7.3.3.5).
12.7.3.3 Manner of Fractures of the Femoral Shaft
Fractures of the femoral shaft can occur before, during, or after birth. If a fracture is sustained after birth, this may have occurred in accidental or in non-accidental circumstances.
12.7.3.3.1 Before Birth
In the literature, several case reports are found concerning intrauterine fractures of the shaft. Multiple intrauterine fractures of long bones, including fractures of the shaft, can be found due to medical conditions with increased fragility of bone-like skeletal dysplasias or due to severe maternal (abdominal) trauma [314, 315]. Maternal trauma may occur in accidental and in non-accidental circumstances. Domestic violence (intimate partner violence) may occur in 3–9% of all pregnancies. Studies in selected populations (low-income, predominantly single women) sometimes even show percentages of up to 50% [316].
According to Christensen and Dietz trauma is the most common cause of non-obstetrical maternal deaths [317]. The fact that pregnant patients frequently are injured in accidents means that unborn children also are risk of being injured in utero. Foetal fractures of almost every bone in the body have been described [317].
Isolated intrauterine fractures of the shaft seem to be extremely rare and are hardly ever diagnosed before birth [314, 318].
Wilkinson (1898) was one of the first to describe the occurrence of an isolated intrauterine fracture of the femur [319]. Concerning the circumstances he stated:
-
‘Professor Gurlt, who has discussed the subject of intra-uterine fractures in an exhaustive paper fortified by cases, published in Berlin in 1857, and later in his classic "Treatise on Fractures," believes that many intra-uterine fractures result from external violence received by the mother during the advanced period of pregnancy’.
Concerning the occurrence of a femur fracture in his case he stated:
-
‘I am unable to assign a positive cause for this fracture. There is a history of an epileptic seizure of the mother in the fourth of fifth month of pregnancy, in which seizure she fell violently over a stove, but aside from the fall no pain followed the accident. Another theory is that the husband, who afterward deserted his wife, owing to a continuance of domestic infidelity, may have abused her, either by striking her or by some other violent means causing the fracture.
-
My other theory, and the one I wish to call your attention to especially is, that during an epileptic seizure, a compression of great severity produced by an abnormal increase of muscular power of the abdominal muscles would be sufficient to squeeze, as in a vise, the pent-up fetus, which would at that time most likely, be raised up against the abdominal walls, consequently being more exposed to the spasmodic contractions of the muscles or walls of the abdomen’.
Bucholz and Moulden reported the occurrence of a fracture of the left midshaft in a male foetus due to, what eventually turned out to be after 5 days a fatal car accident of the mother [318]. The boy was born after an emergency caesarean section, but developed multiple medical problems, including seizures, probably caused by neonatal asphyxia. Christensen and Dietz reported the same case and stated that this case report probably was the first that documented radiographically a fracture prior to delivery [317].
Sometimes an intrauterine fracture of the shaft is reported in single case reports without any indication of a skeletal dysplasia or an evident maternal trauma. These fractures often are labelled as spontaneous fractures [315, 320,321,322]. Forensically seen, the use of the term ‘spontaneous’ is not correct, better terms would be ‘unknown’ or ‘unexplained’.
Despite the fact that usually it is assumed that a severe maternal trauma is needed, a shaft fracture may probably occur in what is considered to be a less severe or even mild maternal trauma. Alonso et al. described the occurrence in a low-speed frontal collision, while the mother was driving (less than 30 mph) [323]. She was wearing a seat belt, but despite that there was a direct impact onto her abdomen with the steering wheel. She attended the Emergency Department. She had no external injuries. The baby was born 4 weeks later after a normal vaginal delivery. The baby had a hard mass on the right femur. The right femur showed on X-ray an almost united fracture with abundant callus formation with no indication of a skeletal dysplasia.
12.7.3.3.2 During Birth
Birth trauma-related fractures of the femur are very rare and may occur both in vaginal deliveries as in caesarean sections [324,325,326]. (Figs. 12.59a, b and 12.60). Most of these are fractures of the shaft, mainly midshaft. Kancherla et al. evaluated 10 neonates with birth-related shaft fractures, of which 8 were midshaft fractures and 2 subtrochanteric fractures [326]. Frik described four neonates with birth trauma-related femoral subtrochanteric fractures, of which three occurred during a caesarean section [327]. Birth trauma-related femoral shaft fractures may occur bilaterally [328].

(a) One-day-old neonate (birth weight 2215 g) with a femur fracture after a complicated delivery with transverse presentation. (b) After 4 months the fracture has healed practically seamless

Oblique left femur after a caesarean section
Four large epidemiological studies, concerning birth-related fractures in over almost 160,000 neonates showed only 11 fractures of the femur, of which 8 were fractures of the shaft [94, 118, 121, 329]. This would mean an incidence of 0.05 femoral shaft fractures in 1,000 live births. Smaller series show comparable low figures (Table 12.8).
Birth trauma-related fractures of the femoral shaft are associated with shoulder dystocia, caesarean section, twin pregnancies, multiple births, breech presentation, preterm and small for age neonates, osteopenia of prematurity, and osteoporosis (e.g. secondary to copper deficiency) [117, 326, 327, 330]. However, these fractures may also occur in neonates with normal weights, uncomplicated pregnancies, and healthy mothers [330].
Not all birth trauma-related fractures are immediately identified after birth. A delay in diagnosis up to a few days after birth has been described, even when children are hospitalized [324,325,326]. Kancherla et al. found a mean delay time of 4 days, before the fracture was diagnosed. Kanai et al. reported a delay in the diagnosis of 9 days in a female neonate with a left spiral femur fracture with associated oedema and hypoaesthesia [331]. The delay was caused by a lack of symptoms and she had a normal physical exam on day 1. On day 1 a whole body X-ray was made which showed on revision a non-displaced fracture of the left femoral shaft. Such a delay may, in theory, lead to a suspicion of non-accidental trauma.
Up to a certain extent, it is possible to differentiate between birth trauma-related femoral shaft fractures and fractures due to trauma after birth (accidental or non-accidental) by evaluating the formation of callus.
Subperiosteal new bone formation and calcification can be found as early as 7 days after birth [332,333,334]. The absence of subperiosteal new bone formation or callus after 11 days should prompt a physician to consider non-accidental injury [332].
Hosokawa et al. evaluated the findings concerning femoral shaft fractures in 7 neonates without underlying disease. Subperiosteal new bone formation (SPNBF) and callus formation were not detected by day 6 on radiographs. SPNBF was first observed on day 14 (14.29 ± 5.35 days; range 9–23 days), soft callus on day 15 (15.85 ± 4.49 days; rage 10–23 days), and hard callus on day 21 (21.43 ± 5.41 days; range 16–32 days). The 7 neonates without an underlying disease showed SPNBF and soft callus formation by day 23. According to Hosokawa et al., an underlying disease (e.g. osteogenesis imperfecta) may be considered, if SPNBF or callus formation is detected within 6 days after birth. The authors also stated that trauma after birth or an underlying diseases may be considered if SPNBF or callus formation is not detected by day 23.
Based on the data presented above reserve is recommended in excluding birth-related trauma if a femoral shaft fracture is found in a neonate, because of the range in days in first radiologically visible SPNBF, soft and hard callus. Above that, Crompton et al. showed that the subperiosteal new bone formation and callus stages of femoral fracture healing in children under the age of 3 years are slower compared to birth-related clavicular fractures [334]. More research (with larger sample sizes) on this topic is needed.
12.7.3.3.3 After Birth: Accidental and Non-accidental Circumstances
The femoral shaft is the most common location in case of femoral fractures. Fractures of the shaft may occur in accidental and in non-accidental circumstances.
In normal bone, a fracture of the shaft usually is caused by a trauma with a high-energy transfer (Sect. 12.7.3.2). After birth this may occur due to a direct blow to the shaft, e.g. in motor vehicle accidents of high-impact sport injuries, or due to an indirect trauma, transmitted at the knee, like in falls from heights and landing on feet [245, 303, 304, 335].
Fractures have also been described to occur due to traditional massage, physiotherapy, or medical procedures, although the occurrence of this type of circumstance is probably extremely rare in paediatric patients (Sect. 12.7.3.3.5). They may also occur due to low-energy trauma, e.g. in diseases with an increased risk of fractures (see Sect. 12.7.3.3.6).
Hinton et al. evaluated the findings of 1,485 paediatric patients under the age of 18 years with acute fractures of the femoral shaft and found that the most common accidental circumstances are age dependent [304]. In children under the age of 6 years falls were the most common accident, in children between 6 to 9 years this was motor vehicle-pedestrian accidents, and in teenagers motor-vehicle accidents. They also found that Firearm-related injuries accounted for 15% of the fractures among black adolescents.
According to Edgington et al. non-accidental trauma should always be considered in young children under the age of 3 years and especially in pre-mobile children [307]. Several large studies describe high rates of non-accidental injury in children under the age of 1 year with a femoral shaft fracture [40, 124, 130, 244, 303, 336,337,338].
In children of 3 years and older shaft fractures are rarely sustained in non-accidental circumstances since bone at this age is significantly stronger in resisting both torque forces and direct blows [339]. In children of 5 years and older and in adolescents, a shaft fracture is hardly ever the result of non-accidental trauma. The most probable circumstances are a high-energy trauma-related, such as sports trauma or motor vehicle accidents [340,341,342]. In the United States, shaft fractures increasingly are sustained due to shot wounds [302].
Most studies concerning shaft fractures in paediatric patients compare the findings in children, who sustained the fracture in accidental circumstances, to children, who sustained the fracture in non-accidental circumstances:
-
Worlock et al. described data from a retrospective study (inclusion period 1976–1982) on 151 children under the age of 5 years [40]. In their study 116 (76.8%) children had an accident as the cause of the fracture and 35 (23.2%) a non-accidental cause. The authors do not provide data on the difference between age groups of mobile versus non-mobile infants and children.
-
Leventhal et al. described a retrospective study (inclusion period 1979–1983) in children under the age of 3 years who were treated for fractures at the Yale-New Haven Hospital [124]. They found that out of 228 children 26 (11.4%) had a femur fracture. Of these 13 (50%) were sustained in accidental circumstances, in 9 (35%) in non-accidental circumstances, and in 4 (15%) the circumstances were unknown. In children under the age of 12 months, 6 of 10 fractures occurred due to non-accidental trauma and children above the age of 23 months none of 10 fractures were the result of non-accidental trauma.
-
Blakemore et al. evaluated data on 42 children aged 1–5 years (mean age 3.1 years) who presented with a femoral fracture between 1979 and 1993 [336]. In this group 16 children were reported to child welfare of which 4 cases went to court. In only 1 case intentional injury was determined to be proven.
-
Schwend et al. performed a retrospective analysis in 139 children, under the age of 4 years, with a femoral shaft fracture [337]. In 126 (91%) children the fracture was sustained in accidental circumstances, and in 13 (9%) the circumstances were determined to be non-accidental. The children in the accidental group were slightly older compared to the non-accidental group: 2.4 ± 1.0 versus 1.1 ± 1.0 years. The strongest predictor for non-accidental trauma was the ability to walk, with 10 (42%) out of 24 non-walking children in the non-accidental group versus 3 (2.6%) out of 116 children in the accidental group.
-
In a large nationwide study based on the 2000 Healthcare Cost and Utilization Project of Kids’ Inpatient Database Loder et al. collected data on 9963 femur fractures [242]. In the vast majority the shaft fracture was sustained either in a fall (35%) (3481 cases, of which 1691 related to sport injuries) or in a motor vehicle accident (33%) (3245 cases). Although the authors not specifically mention the number of fractures, that occurred in non-accidental circumstances, they stated that 15% of all femur fractures under the age of 2 years were inflicted.
-
Hui et al. performed a retrospective study in which they included 127 children under the age of 3 years with a femur fracture [338]. Of the 127 femur fractures 14 (11%) were determined to have occurred in non-accidental circumstances. In children under the age of 1 year this was the case in 10 (17%) out of 60 children. According to Hui et al. non-accidental trauma should be excluded in children with a femur fracture under the age of 12 months, non-ambulatory status, delayed presentation, mechanism of injury unwitnessed or inconsistent, and other associated injuries.
-
Pandya et al. performed a large retrospective study, in children under the age of 4 years, in an urban level I paediatric trauma centre [130]. In the period 1998–2007, a total of 1485 children, 500 non-accidental (377 <18 months), and 985 accidental (425 <18 months) cases, were included. In the non-accidental group there were 73 (14.6%) femur fractures and in the accidental group 140 (14.2%, p = 0.85). In the under 18 months group this was, respectively, 66/377 (17.5%) versus 45/425 (10.6%, p = 0.057). Based on their findings the authors concluded that in the under 18 months group ‘the odds of femur fracture (1.8 times) were found to be significantly higher in the child abuse group than in the control group’. For the whole study population the odds ratio for abuse was 1.0 (95% CI: 08–1.4).
-
In a retrospective study in children under the age of 4 years with femur fracture Baldwin et al. compared 139 control patients (mean age 26.2 months. IQR 34.8, with 44 infants under the age of 18 months) with 70 cases of non-accidental injury (mean age 4.0 months. IQR 8.3, with 63 infants under the age of 18 months, both age and proportion <18 months p < 0.001) [244]. In this study the authors looked at seven risk factors of which three patient characteristics were significant: current polytrauma, physical and/or radiologic evidence of prior trauma, and the history suspicious for abuse. For all three categories there was a significant difference between both groups. Using a multiple logistic regression model the authors calculated odds ratios for the presence of 1, 2, and 3 risk factors these were, respectively, 7.2 (95% CI: 2.2–23.5), 155.5 (95% CI: 41.6–581.0), and 273.0 (95% CI: 28.1–2649.0). Based on a logistic regression equation for each number of risk factors a prediction tool was developed (Fig. 12.57).
-
Shrader et al. evaluated the findings in 137 children under the age of 5 years with a femoral shaft fracture (5-year period) (mean age at the time of injury 2.2 years; range 1 month to 4 years [343]. Forty-three children (mean age 1.8 years) (31%) were determined to have injuries suspicious of non-accidental trauma and were referred to Child Protective Services. Shaft fractures in children under the age of 1 year were a highly significant risk factor for suspected non-accidental trauma. Of the 20 children under the age of 1 year, 18 (90%) were referred to Child Protective Services, comprising 42% of those children suspicious of non-accidental trauma.
-
Mughal et al. evaluated the findings in 759 paediatric patients, aged from 1 day to 12 years (mean age 4.9 years; median age 3.6 years) with a total of 770 femoral shaft fractures [344]. Eleven patients had bilateral fractures. The most common circumstances were falls (39%) (peak age 2–3 years), followed by motor vehicle accidents (33.7%), of which in 88% pedestrians (peak age 4–5 years) were involved. In children under the age of 1 year, 59.3% were due to non-accidental circumstances. Pathological fractures occurred in 39 patients (5.1%) (Sect. 12.7.3.3.6).
-
In a nationwide study of 1,855,267 infants under the age of 12 months, born between 1 January 1997 and 1 December 2004 in Sweden, von Heikeden et al. studied the incidence of femur fractures [117]. From this population 287 infants with a non-birth-related femur fracture were included in the study. Of these fractures 27 (9%) were related to non-accidental trauma, in children under the age of 6 months there were 21 (20%) cases.
Based on the data presented above it is clear that it is imperative that a skeletal survey is performed in non-mobile infants with a shaft fracture without a clear clinical history. This is supported by a study by Cornell et al. which showed that in a series of 19 infants under the age of 12 months who were presented with a femoral fracture 8 (42%) showed occult fractures on the skeletal survey [345].
In young pre-mobile children, an unusual accidental fracture of the distal part of the shaft may occur when a parent falls on the child while the child is carried on the hip of the parent. This can cause a greenstick fracture of the medial distal metaphysis of the femur (Fig. 12.61a, b) due to bowing of the thigh bone, which leads to compression damage to the medial cortex [302].

(a) Five-month-old girl who had sustained a greenstick fracture of the distal femur (open arrow, A-P view). (b) Lateral view of the femur shows a cortical defect (open arrow)
Ali et al. reported the occurrence of femoral shaft fractures in two boys, aged 4 and 6 years, who were playing in a graveyard, due to a tumbling tombstone [346].
Stress fractures of the femoral shaft (and neck) are uncommon, but are increasingly diagnosed in adolescent athletes participating in sporting activities like soccer, basketball, or athletics. These fractures account for 4% of all stress fractures in paediatric patients [339].
In a few studies femoral fractures in sexually abused children are reported. Hobbs and Wynne found fractures in 5% of a group of 130 sexually abused children, as a sign of physical child abuse [347]. According to this study, however, these fractures are seldom or never the result of sexual acts. In three children they did find fractures resulting from sexual acts. A 5-month-old girl sustained a femoral fracture without dislocation as the result of abuse [348]. Johnson et al report on a case of a 4-month-old girl who was thought to have been sexually abused and the follow-up skeletal survey revealed a shaft fracture due to sexual abuse [348].
12.7.3.3.4 After Birth: Differentiating Accidental from Non-accidental Circumstances
Currently, no association has been found between the morphology of the fracture and distinguishing between accidental or non-accidental injury. The systematic review of Kemp et al. showed that the distribution of transverse, spiral, or oblique fractures do not differ significantly between accidental and non-accidental cases [148]. However, high-quality studies with large sample sizes are lacking.
It is often maintained that a spiral fracture of the shaft of one of the long bones, and in particular the femur, is evidence of child abuse. This is incorrect, it is only possible to evaluate such a fracture when the context of the origin of the fracture is also considered [124, 335, 349, 350]. The only conclusion that can be made with certainty when a spiral fracture of the femur is found in a child is that the fracture is the result or applied torque (rotation along the longitudinal axis of the bone). Torque may occur in non-accidental circumstances (Figs. 12.62 and 12.63). In mobile children torque can occur in accidental circumstances, in which the foot takes a more or less stationary position [124, 125, 147, 337, 351]. The fracture may also occur in a fall in which the knee and hip are more or less stationary, and the child turns the lower leg in relation to the stationary joints. This happens regularly, not just to the femur but also to, e.g. the tibia, as in the ‘toddlers’ fracture’ (Sect. 12.8.3.3).

Healing spiral fracture of the left femur (open arrow) in a 3-week-old infant who, according to the parents, had fallen from the couch. The fracture does not correspond with the described biomechanics

Graphic representation of the possible origin of a non-accidental femur fracture
In a transverse fracture, the fracture line is more or less perpendicular to the long axis of the bone. In an oblique fracture, the fracture line is at an angle of 30–40 degrees to the long axis of the bone. Transverse and oblique fractures may occur due to compression, tension, shearing and bowing, or a combination of these mechanisms (Table 12.1).
Transverse and oblique fractures are frequently seen in accidental and non-accidental circumstances [335]. These fractures may occur as a result of direct blunt force trauma (impact) on the bone (mostly resulting in bowing or shearing, Fig. 12.64), or by indirect trauma, e.g. when a child falls from a significant height and lands on a knee (usually resulting in compression and/or bowing). It may also happen when a parent falls down the stairs while holding the child on an arm and the child lands on the femur (Fig. 12.65) [36]. This is often a trauma with a high-energy transfer.

Oblique femur fracture (open arrow) in a 3-year-old boy who had toppled a television (witnessed trauma)

Four-week-old girl who had sustained a proximal femur fracture after a fall from the arm of her mother who tripped over the family dog
Oblique fractures are usually the result of a combination of various forms of loading, such as compression with some torque, or compression with bowing [36].
While evaluating a shaft fracture, one should realize that it can sometimes be difficult to distinguish radiologically different morphologies, for example a spiral and an oblique fracture, which can look quite similar on different views.
In non-accidental trauma, particularly bowing and shearing are involved. A child may have received a blow or a kick to the upper leg, and the bone bows past the point at which recovery is still possible without a fracture. In younger children, indirectly applied forces may also be involved; for example when a person violently grabs and manipulates the leg, swings the child to and fro, or hits or throws the child against some object [349].
Loos et al. showed that, regardless of working experience, health care professionals in the Netherlands were biased by contextual information towards accidental or non-accidental trauma when assessing images of femur fractures in young children [352]. Context such as low income, single-parent family households, and migrant status may inappropriately influence professionals.
12.7.3.3.5 After Birth: Traditional Massage, Physiotherapy, and Medical Procedures
Mboutol-Mandavo et al. reported two neonates with massage-related fractures: a 17-day-old neonate with a midshaft fracture of the right femur and a 1-month-old infant with a fracture of the right clavicle [353]. In the 17-day-old neonate a crack was heard during the massage, after which the child started crying. The massaging was done at home by a grandmother.
Siddiqui et al. described femoral midshaft fractures in 3 neonates, aged 2–3 weeks, following oil massage, which is common practice in India [354]. The massages took place at home 2–3 times a day and were done by a grandmother. All three grandmothers noted that they felt a crack at the time of the oil massage, after which the babies refused to move the affected lower extremity.
Della Grotto et al. reported an 11-day-old neonate, who was admitted to the hospital at day 1 of life [53]. On day 11, while still in hospital, a swelling of the right leg was noted and on ultrasonography a fracture of the right femoral shaft was diagnosed. Additional radiographs showed an oblique fracture of the right femoral shaft and a metaphyseal corner fracture of the proximal tibia of the same leg. Chart review showed that physiotherapy was provided in the NICU and this was ruled the cause of the fractures.
The medical literature does not report any cases in which a fracture was sustained in a physical examination. However, the authors of this book have been confronted with a 3-day-old neonate with a midshaft femur fracture (Fig. 13.33). According to the mother the child showed pain when she changed the diaper. Patient history and follow-up examination did not show any signs of non-accidental trauma. Post-partum there were no indications for a fracture. On day 3, the paediatric resident performed an examination according to Ortolani. The resident wrote in the dossier that a little snap was heard and that the Ortolani was positive. After this examination the infant showed pain when the diaper was changed. A radiograph of the leg showed a midshaft oblique femur fracture. The successively made skeletal survey did not show any other fractures. The combined facts led to the conclusion that the femur fracture had to be the result of the examination according to Ortolani.
12.7.3.3.6 After Birth: Diseases with an Increased Risk of Femoral Shaft Fractures
Pathological fractures of the femoral shaft are relatively rare in children and account for around 4–5% of all paediatric shaft fractures [239, 344]. A pathological fracture is defined as a fracture that occurs without a significant trauma or with a trauma with a seemingly low-energy transfer, usually in pre-existent pathological bone. Fractures of the shaft in a child should alert physicians to a possible underlying disorder, if there is no history of a significant trauma or if there is a history and/or other findings suggestive of non-accidental trauma.
Bone may be ‘pathological’ due to generalized bone disorders or in disorders with focal manifestations, resulting in an increased fracture risk.
Pathological femoral shaft fractures, due to generalized bone disorders can be seen in children with generalized osteopenia, such as osteogenesis imperfecta (OI) [124, 355]. Other causes of generalized osteopenia in which a fracture of the femoral shaft may occur due to a minor trauma are neurological/neuromuscular disorders, such as cerebral palsy or meningomyocele [239, 356,357,358]. Ju et al. reported the occurrence of shaft fractures in a 14-year-old boy with undiagnosed cystic fibrosis [359]. While playing baseball he sustained a left midshaft femoral fracture while running. Eight months later, he sustained a right midshaft femoral fracture under similar conditions. After the second fracture, further evaluation revealed low bone mineral density and confirmed the diagnosis of cystic fibrosis.
Osteogenesis imperfecta and cerebral palsy are probably the most common underlying disorders. Children with these disorders sustain femoral shaft fractures most commonly between the age of 6 and 12 years, because, according to Murugappan, they start walking late.
Pathological fractures, due to focal lesions, can be seen in paediatric patients with neoplasms. Usually, these are benign lesions such as non-ossifying fibroma, eosinophilic granuloma (unifocal Langerhans cell histiocytosis), fibrous dysplasia, and bone cysts [360,361,362]. Pathological femur fractures are seldom seen in paediatric patients with malignant neoplasms, e.g. osteosarcoma or Ewing sarcoma (see Chap. 14) [302, 363].
Pathological fractures, due to focal lesions, can also be seen in paediatric patients with chronic osteomyelitis of the femoral shaft [364, 365].
12.7.4 Fractures of the Distal Femur
12.7.4.1 General Aspects of Fractures of the Distal Femur
Fractures of the distal femur are rare, accounting for only 7% of all fractures of the lower extremity in children. There is a peak incidence between 10 and 12 years. Boy to girl ratio is estimated around 6:1 [366,367,368]. Distal femur fractures account for approximately 12–19% of all femur fractures in children [242, 301, 369].
Distal femur fractures can be classified as metaphyseal corner fractures, metaphyseal fractures, or physeal fractures [370]:
-
Metaphyseal corner fractures (classical metaphyseal lesions, buckle handle fractures) are almost exclusively seen in children under the age of 2 years of age (Sect. 12.3.2).
-
Metaphyseal fractures of the distal femur (transverse distal metaphyseal fractures, supracondylar femoral fractures) are the most common type of distal femur fracture (excluding MCF) in infants and young children (Fig. 12.66a, b) [370, 371]. These can be complete or incomplete (greenstick or torus) fractures.
-
Physeal fractures of the distal femur are more common in older children and adolescents (Fig. 12.67a, b). These fractures account for around 7% of fractures of the lower extremity and under 1% of all paediatric fractures [372]. Physeal fractures are classified according to the Salter–Harris classification (Sect. 12.3.3) [370]. SH-type II fracture is most common [373, 374]. The epiphysis of the distal femur is particularly prone to growth disturbance due to a fracture, as this is responsible for approximately 70% of the total growth of the femur [375].

Three-year-old child who fell from a climbing frame. (a) AP radiograph shows a supracondylar fracture. (b) Lateral radiograph shows posterior displacement of the distal fracture segment. The anterior humeral line (in white) drawn on a lateral view along the anterior surface of the humerus should pass through the middle third of the capitellum. This is clearly not the case in this child

Nine-year-old paraplegic child with a swollen leg. (a) Radiography shows an osteopenic femur with florid subperiosteal new bone formation along the diaphysis and distal metaphysis. (b) Lateral radiograph shows a SH-I fracture of the distal femur (inset). Most likely the fracture resulted from physical therapy
12.7.4.2 Cause of Fractures of the Distal Femur
‘Older practioners will remember that this injury commonly happened to some young person who was attempting to ‘hook a ride’ by scrambling over the rear dashboard of a high-wheeled horse-drawn vehicle. In swinging his leg over the dashboard, the victim caught his foot in the slowly turning spokes of the wheel. His pelvis being fixed on the dashboard and the foot being fixed in the turning wheel, there resulted a twist with hyperextension of the knee; these factors caused the injury under discussion’ [376].
As long as the growth plates of the distal femur in children and adolescents are open, the distal femoral epiphysis will be less resistant to trauma and therefore more prone to sustain injuries than the knee ligaments. This vulnerability is further increased because of the undulating shape of the distal femur [373].
Fractures of the distal femur are the result of a significant trauma with a high transfer of energy, as may occur in motor vehicle accidents, falls from height, or contact sports. Two mechanisms are most common [368, 374, 377, 378]:
-
A direct blow to the knee joint either from the lateral or the medial side (side impact), causes a valgus or varus bending effect across the joint and on the collateral ligaments. Due to this effect disruption of the ligaments may occur on one side, while compression of bone may occur on the other side. In children with open growth plates, the tensioning of the ligaments at the attachment to the distal femoral epiphysis may result in failure of the bone, eventually leading to fractures of the distal femur. In adolescents, this trauma mechanism can result in the so-called ‘unhappy triad’ consisting of a rupture of the anterior cruciate ligament (ACL), a medial meniscus tear, and a rupture of the tibial (medial) collateral ligament.
-
An indirect trauma due to lateral or medial distortion of the joint, causing a valgus or varus bending effect across the joint and on the collateral ligaments, with comparable consequences as in a direct blow. Indirect trauma may occur in landing on the feet after a fall from height.
Often the bending effect is increased by some degree of rotation/torsion due to twisting the knee on the stable foot.
12.7.4.3 Manner of Fractures of the Distal Femur
12.7.4.3.1 Before Birth
Gowda et al. described the occurrence of a MCF of the distal femur. According to the authors this MCF was sustained in utero due to external cephalic version for a breech presentation with the hips flexed and knees extended [46]. The foetus was successfully manoeuvred into a cephalic presentation, but because of a blood-stained discharge from the cervix, an emergency caesarean section was done.
12.7.4.3.2 During Birth
Injuries related to the femur as a consequence of birth-related trauma are usually found in the shaft and the proximal physis. Few studies have been published on birth-related injuries of the distal femur [71, 72, 109, 379,380,381,382,383]. As for other birth-related long bone fractures, often a complicated vaginal delivery (often in high-birth weight neonates or in breech presentation) or a caesarean section (often secondary to breech presentation) is reported [384].
Eliahou et al. reported a premature neonate with a SH-type 1 fracture of the left distal femur following caesarean section [72]. According to Eliahou et al., the presumed mechanism in caesarean sections is forced traction of the leg with acute angulation or twisting during birth.
Alexander et al. reported the occurrence of metaphyseal fractures in 2 female neonates [385]. The first was born at term after caesarean section because of an extended breech delivery without any progress. She weighed 3.3 kg at birth and was diagnosed on day 6 with metaphyseal fracture of the left distal femur and of the left upper tibia. Skeletal survey otherwise was normal. The second girl was born after caesarean section because of a flexed breech presentation in a primigravida. She weighed 4.14 kg. On day 2 a distal metaphyseal fracture of the right femur was diagnosed.
Bilateral birth-related distal femoral epiphyseal fractures have been reported [386].
Birth-related metaphyseal corner fractures of the distal femur are only very rarely reported. Sieswerda et al. reported the occurrence of an MCF in the distal right femur in a male neonate, born after attempted external version (ECV) and vaginal breech birth [45].
12.7.4.3.3 After Birth: Accidental or Non-accidental Trauma
Fractures of the distal femur can occur in accidental and in non-accidental circumstances [40, 244, 387,388,389].
Metaphyseal and physeal fractures of the distal femur have been described to occur in accidental and in non-accidental circumstances. Metaphyseal fractures (excluding MCF) are the most common type of distal femur fracture in infants and young children, whereas physeal fractures are more common in older children and adolescents.
Fractures of the distal femur usually are sustained due to high-energy trauma, e.g. falls, motor vehicle accidents, or sports-related activities [368]. This especially accounts for children aged 2–11 years [372].
Rex and Kay evaluated the findings, concerning age, site, and fracture patterns, in 14 children with non-accidental femur fractures and compared these with the findings in 33 children with accidental femur fractures. Thirteen of the children with non-accidental fractures of the femur were under the age of 12 months [388]. The authors could not find any specific site or fracture pattern that could allow differentiation between accidental and non-accidental fractures of the femur.
Rewers et al. evaluated epidemiological data concerning femur fractures in 1139 paediatric patients, aged 0–17 years (795 boys and 344 girls) [301]. The most frequent location of femoral fractures was the shaft in 62.5%, followed by the proximal (12.5%) and the distal (11.7%) femur. Almost 1 in 8 fractures involved the shaft in combination with a proximal or distal fracture. Fractures of the shaft, due to non-accidental trauma, were relatively less common, whereas distal fractures and combinations of shaft and distal fractures were more common, compared to fractures due to accidental trauma. Associated injuries were found in 28.6% of the children, more often in older children. Children who sustained femur fractures due to non-accidental trauma, motor vehicle accidents, or car versus pedestrian accidents were 16–20 times more likely to have associated injuries than those with femur fractures as a result of a fall.
Baldwin et al. evaluated the findings in 70 paediatric patients with non-accidental femur fractures and compared these with the findings in 139 paediatric patients with accidental femur fractures [244]. Patients from the accidental group more often had shaft fractures and patients from the non-accidental group more often had fractures of the distal femur. No difference was found between both groups concerning fractures of the proximal femur. The risk of femur fractures due to non-accidental trauma was highest in children under the age of 18 months, in girls (girls to boys ratio 2:1), in polytrauma patients, physical, and/or radiographic evidence of prior trauma and in case of a suspicious history.
In children under the age of 1 year non-accidental trauma should always be considered in case of a fracture of the distal femur. Arkader et al. evaluated the findings in 29 children with complete metaphyseal fractures of the distal femur (two level 1 paediatric trauma centres; 10-year period) [389]. 20 fractures occurred in non-ambulatory infants under the age of 1 year (14 boys, 6 girls; average age 6 months 10 days, with a range of 5 days to 1 year). Non-accidental circumstances were considered confirmed in 10 children and highly suspicious in 5 children. The authors’ advice that in all non-ambulatory infants non-accidental circumstances should always be considered.
Nevertheless, a careful analysis of the medical history, concerning accidental circumstances, is always indicated, in children with distal femur fractures. This also accounts for non-ambulatory infants:
-
Grant et al. described the finding of identical oblique distal femoral metaphyseal fractures extending through the growth plate in two non-ambulatory infants [390]. The fractures supposedly occurred while playing in an infant stationary activity centre (Exersaucer, Sect. 13.3.5.7). According to the authors, the twisting motion provided by the Exersaucer might have generated enough force to cause the fractures.
-
Haney et al. evaluated the findings in 18 children with transverse fractures of the distal femoral metadiaphysis [387]. In 13 children (11 under the age of 1 year; mean age 12 months; median age 8 months) the circumstances were determined to be accidental and in five children (all 5 under the age of 1 year; mean age 8 months; median age 8 months) non-accidental. The authors concluded that impacted transverse fractures of the distal femoral metadiaphysis may occur as a result of accidental short falls of young children. They also were of the opinion that a ‘traditional abuse evaluation’ should be done in all cases, but that in the absence of additional skeletal findings, and a history of a fall, accidental circumstance likely accounts for the occurrence of the fracture.
Fractures of the distal femur may occur due to physiotherapy. Pickett et al. described an ex-premature infant (pregnancy 33 weeks; birth weight 2077 g) in whom multiple defects to both legs were found at age 4 weeks: extensive periosteal reactions around the knees combined with ‘bucket-handle’ fractures of both proximal tibiae [391]. Diaphyseal periosteal new bone formation and metaphyseal fragmentation of both tibiae were present. Diametaphyseal periosteal new bone of the distal end of the left femur was present. The proximal medial femoral metaphyses had corner fractures. The osseous lesions appeared to be limited to joints receiving physical therapy for contractures.
12.7.4.3.4 After Birth: Diseases with an Increased Risk of Fractures of the Distal Femur
Underlying disorders may predispose children to fractures of the distal femur [378]. This has been described in children with spastic cerebral palsy, neonatal osteomyelitis and septic arthritis, and spina bifida (Fig. 12.68) [392,393,394]. In these children fractures may occur due to low-energy trauma, e.g. in ‘twisting’ the leg during physical therapy or while changing diapers or changing the child’s position in bed. Because of disuse osteopenia non-ambulatory children, e.g. with cerebral palsy or spina bifida, are susceptible to fractures due to low-energy trauma. Ambulatory children with spina bifida may develop epiphysiolysis, or a chronic separation of the distal femoral physis, and be unaware of it because of altered sensation.

Ten-year-old paraplegic child with spina bifida. After a puppy jumped on her knee she had a slightly swollen left upper leg. Radiography showed a fracture through a severely osteopenic distal femur
Vander Have et al. described three patients who developed knee stiffness after operative treatment for displaced tibial eminence fractures. The stiffness was treated with manipulation of the knee under anaesthesia [395]. Due to the manipulation the patients sustained distal femoral fractures with subsequent growth arrest.
12.8 Tibia and Fibula
12.8.1 General Aspects of Fractures of the Tibia and Fibula
Tibial fractures are the third most common fractures in childhood, after fractures of the forearm (distal radius and shaft) and the humerus [396]. These fractures occur most frequently in early mobile and older children and in adolescents. In infants fractures of the lower leg are rare. Fractures of the tibia consist of approximately 15% of all paediatric fractures [308], with a yearly incidence of 11 per 1000 children [397]. The average age of occurrence is 8 years. They are more common in boys than in girls [398, 399].
Almost 40% of all tibia fractures are midshaft fractures. Most of these shaft fractures are oblique or transverse and located in the middle or lower third of the shaft, although spiral fractures are regularly found in toddlers (Childhood Accidental Spiral Tibia fractures, Sect. 12.7.3.2). Paediatric patients under the age of 4 years with lower leg fractures most often showed simple oblique fractures of the tibia [400].
About 30% of the tibia shaft fractures are associated with fibular fractures [398]. Isolated tibial fractures with an intact fibula have a lower risk for shortening, but may pose a risk for varus deformity [401, 402]. Isolated fibula fractures are rare [403].
12.8.2 Cause of Fractures of the Tibia and Fibula
The cause of fractures of the lower leg can be divided into low- and high-energy trauma. According to Chapman and Cohen the cause of lower leg fractures varies depending on the age of the patient. In younger children low energy trauma, e.g. a rotational force due to twisting of the lower leg or falls from standing height, will be the more common cause. In older children and in adolescents high-energy trauma will be more common, e.g. due to a direct blow to the lower leg that is perpendicular to the bone shaft (pedestrian versus car accidents) or a long-distance fall (Table 12.9) [397].
12.8.3 Manner of Fractures of the Tibia and Fibula
Fractures of the lower leg (tibia and fibula), including MCF, have been described to occur before, during, or after birth. If sustained after birth, lower leg fractures can occur due to accidental and non-accidental circumstances.
12.8.3.1 Before Birth
Lysack et al. described the occurrence of a MCF in an otherwise healthy newborn in the proximal tibia. The MCF was thought to have occurred due to an external cephalic version for a frank breech presentation, followed by an emergency caesarean section [47].
12.8.3.2 During Birth
Tibial fractures have only sporadically been found as a consequence of birth-related trauma in epidemiological studies [47, 118, 404]:
-
Basha et al. evaluated the findings in a total of 34 519 live births [120]. Long-bone fractures were found in 8 neonates. In one neonate, born after an emergency caesarean delivery due to breech presentation, a transverse non-displaced right tibial shaft fracture was found. The child also had a midshaft spiral fracture of the right femur and an old fracture of the left femur. A diagnosis of osteogenesis imperfecta was made.
-
Dolivet et al. reviewed the findings in 6840 neonates, born after caesarean section (after exclusion of findings in multiple pregnancies and in caesarean sections before 32 weeks) [405]. They found 10 neonates with at least one fracture. One newborn had a fracture of tibia and fibula. The infant was born after a scheduled section because of breech presentation and macrosomia (birth weight of 3510 g).
-
Rehm et al. reviewed the findings in 87,461 consecutive live births. In 66 newborns a fracture was found, of which only one newborn had a tibia fracture [118].
Some descriptions of tibial fractures, sustained during birth, are case based:
-
Kaplan et al. described a term female neonate, delivered by caesarean section [404]. At the age of 1 week, while the girl was still hospitalized, a swelling was noted over the lower third of the infant's left tibia with local tenderness and erythema. Radiographs showed an oblique fracture of the midshaft of the left tibia, and a greenstick fracture at the distal end of the right radius, adjacent to the epiphyseal plate. The authors stated that fractures most likely occurred during the caesarean section.
-
Mileto et al. described the occurrence of a proximal epiphyseal fracture of the right tibia in a newborn following caesarean section [406]. The birth was complicated by a failure to progress after the membranes had been ruptured for 24 h. Four attempts at vacuum assistance were made prior to performing an emergency caesarean section. The newborn showed swelling and bruising of the right lower leg
The occurrence of MCF due to birth trauma probably is extremely rare, only one case report was found. [49]. Lee et al. describe a MCF of the distal tibia that occurred after an urgent and difficult footling breech delivery [49]. According to the authors, their case shows that the traction and torque placed on the distal extremities during this difficult delivery could be a potential mechanism for the occurrence of a MCF.
12.8.3.3 After Birth: Accidental Circumstances
Accidental fractures of the tibia and fibula are very rare in pre-mobile children and have only been reported as case reports:
-
Moineau and Plint described a case of a 9-month-old boy who presented with bilateral buckle fractures of the proximal tibia [407]. Although the authors concluded that in their case the circumstances, under which the fractures were sustained, remained unknown they stated in the discussion of the case ‘the parents could not think of, and the babysitter did not admit to, any potential traumatic event while in their care. When reviewing any possible repetitive stresses occurring on his lower limbs, the parents admitted that he was often in his baby stationary activity center, and the sitter had mentioned that he had been in it for a few hours the day he seemed more irritable’. It thus seems plausible that there is a relation between the use of the exersaucer and the occurrence of fractures.
-
Paddock et al. reported the finding of accidental bilateral fibular fractures in a pre-mobile boy, aged 6 months [408]. The parents reported that the infant repeatedly banged his legs against the metal frame of his playpen. The parents videotaped the ‘banging’, which showed that (according to the instructed radiology expert) the point of impact of the infant's legs against the metal frame was at a similar level to the radiographic abnormalities. The videotaped mechanism was therefore believed to be consistent with the injuries, resulting in a diagnosis of ‘self-inflicted’ bilateral fibular fractures and not of inflicted injury.
Accidental tibial fractures are very commonly reported in mobile children. Probably the most common accidental tibial fractures in mobile children, usually under the age of 8 years, are isolated spiral fractures of the tibia. These fractures are usually the result of a (minor) accident such as a fall while walking/running or a fall in which the child’s body rotates around a fixed foot, often resulting in a spiral or oblique fracture [409,410,411,412]. Often these minor accidents are unwitnessed, which can cause concern for non-accidental injury. In most cases the fracture is a non- or minimally dislocated fracture of the lower two-third of the tibia. These fractures were previously referred to as a toddler’s fracture, however, the term Childhood Accidental Spiral Tibia fractures (CAST) is now preferred because this type of fracture not only occurs in toddlers (Fig. 12.69) [409].

Childhood accidental spiral tibia fracture in a 22-month-old boy
In mobile children and in adolescents simultaneous fractures of the tibia and fibula are usually seen in accidents (Fig. 12.70). Fractures of tibia and fibula may also occur when the child is seated on the backseat of a bike (usually a bike of one of the parents) and the foot gets caught between the frame and the spokes of the wheel (Figs. 12.71 and 12.72) [413,414,415]. These easily avoidable injuries are known as ‘spokes’ injuries and unfortunately, at least in the Netherlands with many cycling parents, these are seen on a regular basis.

Distal fracture of tibia and fibula in a 4-year-old boy after high-energy trauma, car vs pedestrian (radiograph was taken in a vacuum splint)

Graphic representation of a spoke injury

Spoke injury in a 4-month-old girl who was seated at the back of her mother’s bike. The trauma resulted in an oblique fracture of the tibia (open arrow) and a Salter–Harris type II fracture of the fibula (arrow)
Other ‘accidental’ circumstances, resulting in tibial fractures, which are not often reported in the literature, are (see Chap. 13 for additional information):
-
Tibia fracture due to a fall out of bed, crib/cot, or chair, while in hospital (falling distance 30–100 cm) (Sect. 13.3.2).
-
Trampoline related tibial fractures (Fig. 12.73) (Sect. 13.3.5.11).
-
Iatrogenic tibial fractures after the use of an intra-osseous vascular access needle (Sect. 13.4.2.2).
-
MCF of the tibia, during IV line placement [52].
-
Iatrogenic distal tibia/fibula fractures, including metaphyseal corner fractures, due to orthopaedic surgery in clubfoot (Sect. 13.4.2.3).
-
Physiotherapy-related tibial fractures (Sect. 13.4.2.4) [391].
-
Stress injuries (Sect. 13.5.2.2).

Two-year old who fell on a trampoline. Radiography shows transverse fractures of the distal tibia and fibula
12.8.3.4 After Birth: Non-accidental Circumstances
Tibia fractures occur frequently in non-accidental trauma. In several studies describing a series of children with non-accidental fractures, the tibia is one of the most commonly affected bones:
-
Worlock et al. compared the findings in 35 children (28 children under the age of 18 months; 7 children between 19 and 60 months; 0 children above the age of 60 months) with non-accidental fractures to the findings in 826 children (19 children under the age of 18 months; 97 children between 19 and 60 months; 710 children above the age of 60 months) with accidental fractures [40]. Worlock et al. found non-accidental lower leg fractures only in children under the age of 18 months, including 7 tibial metaphyseal corner fractures (5 proximal, 2 distal) and 5 tibial shaft fractures (1 spiral fracture of the tibia, 2 tibial periosteal reactions, and 2 tibial greenstick fractures).
-
King et al. evaluated the findings in 750 children of whom 189 children (age range 1 month to 13 years; median age 7 months) with a total of 429 fractures were considered to have sustained these fractures in non-accidental trauma [96]. They found that fractures of humerus, femur, and tibia were the most common non-accidental fractures and that 26% of the children with non-accidental fractures had non-accidental tibial fractures. Avulsion or metaphyseal corner fractures involving the proximal third of the tibia were most common tibial fractures. Twenty-eight percent of the children had a history of previous fractures.
-
Mellick et al. reviewed 31 tibial fractures in 30 children under the age of 5 years (23 boys, 7 girls; age range from 2 months to 4 years and 10 months; 50% were younger than 36 months) [416]. Non-accidental trauma was suspected in 13 children. The suspicion was confirmed in 7 children. 3 out of 7 children had no other fractures. In only 1 out of 13 children with isolated spiral fractures the fracture occurred in non-accidental circumstances.
-
In 1990, Mellick and Reesor published findings in probably the same 13 children with isolated spiral tibial fractures, as published by Mellick et al. in 1988 [410]. Of these 13 children, 9 were classified as accidental fractures and 4 were classified as non-accidental fractures. The circumstances in the 4 children with, according to Mellick and Reesor, non-accidental fractures were described as:
-
Leg twisted by caretaker in a 9-month-old boy: The parents initially had no explanation for the injury, which they first noticed after the infant was picked up from the babysitter. Shortly afterwards, the babysitter admitted to grabbing and twisting the extremity after becoming angry with the child.
-
‘Slipped of lap’ in a 2-month-old girl: The slipping allegedly occurred while a parent was placing the child into a sitting position on the floor. A subsequent hospital visit, examination, and admission demonstrated rib fractures and bruises on the infant’s back.
-
Fell from bed while playing with a 4-year-old brother in a 19-month-old boy: The boy fell a distance of 3 feet from the bed to the floor. When interviewed alone the older brother gave the same explanation for the injury as was presented by the parents. Although no additional evidence for non-accidental trauma was obtained, it was concluded by a child abuse evaluation that ‘the suspicion of child abuse cannot be ruled out due to the nature of the fracture’.
-
‘Tripped over dog chain’ in a 17-month-old boy: The actual fall was reportedly not observed by either parent. The boy was presented for medical care, 3 days after the reported fall. Because of the delay in seeking medical care and inconsistencies in the history, the fracture was designated to be consistent with non-accidental trauma.
In 3 of these 4 children non-accidental trauma either was confirmed or could not be excluded on plausible grounds. In the 19-month-old boy it is dubious whether non-accidental trauma was maintained as most plausible manner.
-
-
In a third study, Mellick et al. reviewed the data concerning isolated spiral tibial fractures in 55 children under the age of 8 years (age range 12–94 months; mean age 50.7 months; 69% male, 31% female) [409]. In 10 children non-accidental trauma was suspected. In none of these children the suspicion was confirmed after an evaluation by the child protection service.
-
Kowal-Vern et al. evaluated the findings in 124 children with fractures under the age of 3 years to determine the frequency of accidental (motor vehicle accidents, pedestrian accidents, other accidents) versus non-accidental trauma [126]. Fractures due to non-accidental trauma were found in 24 children. The authors found that in only 1 of 8 children with lower leg fractures the fractures were sustained due to non-accidental trauma.
-
Leventhal et al. evaluated the findings in 215 children under the age of 3 years with a total of 253 fractures [124]. The fractures were sustained in 24.2% in non-accidental circumstances and in 67.4% in accidental circumstances. In 8.4% the circumstances were not known. Concerning lower leg fractures (n = 35) they found that 14 (40%) were due to non-accidental trauma and 21 (60%) to accidental trauma. According to the author’s non-accidental trauma should be suspected in a child under the age of 1 year with a fracture of the lower leg.
-
Banaszkiewicz et al. reviewed the medical records of all children, under the age of 1 year of age presenting to an Emergency Department over a 5-year period (1995–1999) with a fracture [417]. Seventy-four children presented with fractures (age range 2 weeks to 1 year; mean age 5 months). 5 children had a tibial fracture. The authors stated that in 1 child the fracture was definitely sustained in non-accidental circumstances and in 1 child likely. In 1 child it was suspected but not confirmed.
-
Coffey et al. found 55 fractures of the lower extremities in 555 children under the age of 18 months [418]. Of these 55 cases 41 were linked to non-accidental trauma. Femur fractures were most common (22 unilateral and 6 bilateral, followed by tibia fractures (14 unilateral and 9 bilateral). Fourteen cases were not linked to non-accidental trauma, 13 femur fractures (12 unilateral and 1 bilateral), and 1 tibia fracture. In other words, Coffey et al. found that 96% (23/24) of all tibial fractures in children under the age of 18 months were due to non-accidental trauma.
-
Loder et al. reviewed the findings in 1794 patients under the age of 20 years with injuries due to non-accidental trauma [204]. They found a total of 1053 fractures, of which 119 were fractures of tibia and/or fibula, and/or ankle. Of these 98 were found in children under the age of 1 year, 15 between 1 and 2 years, 3 between 3 and 12 years, and 3 between 13 and 20 years.
-
Van As et al. evaluated the physical findings in 1037 children between 1 month and 13 years (median age 16.5 months, average age 44.8 months; male to female ratio 2:1) with injuries due to non-accidental trauma [205]. Of these children 121 had a total of 149 fractures (21 had multiple fractures). Eleven children had fractures of the tibia/fibula.
-
Pandya et al. did a large retrospective study, in children under the age of 4 years, in an urban level I paediatric trauma centre [130]. In the period 1998–2007 a total of 1485 children, 500 non-accidental (377 <18 months), and 985 accidental (425 <18 months) cases, were included. In the non-accidental group there were 55 (11.0%) tibia/fibula fractures and in the accidental group 16 (1.6%, p < 0.001). In the under 18 months group this was, respectively, 50 (13.3%) versus 5 (1.2%, p < 0.001). Based on their findings the authors concluded that in the under 18 months group ‘the odds of a humerus fracture (7.5 times) were found to be significantly higher in the child abuse group than in the control group’. For the whole study population the odds ratio for abuse was 7.5 (95% CI: 4.2–13.2).
-
Eren et al. described 16 non-accidental fractures in a pre-mobile 7-month-old girl [419]. Of these 16 fractures 3 were tibial fractures (distal and proximal fractures of right tibia and shaft fracture of the left tibia) and one was a fibular fracture (distal fracture of the right fibula).
Based on the findings in the foregoing literature one can conclude the following concerning fractures of the lower leg:
-
Non-accidental tibial shaft fractures probably are less common than tibial metaphyseal corner fractures or fractures of the apophysis of the proximal tibia (apophyseal ring fractures) [40, 96]. Concerning the meaning of tibial metaphyseal corner fractures the reader is referred to Sect. 12.3.2.
-
Despite the rarity of non-accidental tibial shaft fractures one should always consider non-accidental trauma in non-mobile children/children who do not (yet) walk [409, 418].
-
One should also consider non-accidental circumstances if the explanation of how the fracture occurred does not match the known trauma mechanism(s) (inconsistent history) or when other physical findings are found, which are suggestive of non-accidental circumstances (concomitant injuries) [398, 420].
-
Literature on the association between the type of fracture in the shaft of the tibia (spiral, oblique, or transverse) in association with non-accidental trauma is currently lacking.
-
Literature on fibula fractures in association with non-accidental trauma is very scarce [124, 421, 422]. Compared to tibia fractures, fractures of the fibula are only rarely reported [124, 130]. Usually, a simultaneous fracture of the tibia is seen.
12.9 Fractures of the Foot
12.9.1 General Aspects of Fractures of the Foot
Fractures of the foot account for 5–13% of all paediatric fractures [423]. These fractures are rare in infants and toddlers, but the incidence increases with age [424]. In children fractures of the foot are more common in boys than in girls.
Between 70% and 90% of all foot fractures in children involve the metatarsals and phalanges [425]:
-
Metatarsal fractures are common in older children and adolescents and may account for around 50–70% of all paediatric foot fractures (Fig. 12.74) [424, 426, 427]. The most frequently fractured metatarsal in children under the age of 5 years is the 1st metatarsal and in children above the age of 5 years the 5th metatarsal [426]. Fractures of the 1st and 5th metatarsal can occur isolated, while fractures of the 2nd, 3rd, and 4th metatarsal often occur combined with another metatarsal fracture [426].
-
Phalangeal fractures may account for around 20–30% of all paediatric foot fractures [424, 426, 428,429,430,431]. These fractures usually are Salter–Harris type I or type II fractures [424].
-
Tarsal fractures (fractures of the talus, calcaneus, and of the cuboid, navicular and cuneiform bones) are rare and together account for less than 5–15% of all paediatric foot fractures [427]. Fractures of the calcaneus account for a third of all tarsal fractures. In children the most common talus fracture is a fracture of the neck of the talus [427].

Radiograph of the foot of a 4-year-old child, he was playing in the house when a door (which was removed from the hinges) fell over and landed on his foot. There are transverse fractures of the 2nd and 3rd metatarsal (inset)
12.9.2 Cause and Manner of Fractures of the Foot
In Table 12.10, an overview is given of the cause and accidental circumstances of fractures of the different bones of the foot.
Fractures of the foot can be sustained in accidental and in non-accidental circumstances. In mobile and increasingly more active children fractures of the foot mostly occur due to accidental circumstances such as direct impact, crush injury, or falls from height. Singer et al. evaluated the findings concerning metatarsal fractures in 125 children (75 boys, 50 girls; average age 8.6 years; range 1–17 years) [426]. Most fractures were sustained outdoors, including backyard and playground (30%). Other sites were indoors (25%), sports facilities (25%), and school and child-care facilities (12%). In 8% the fractures were sustained in traffic accidents. They found that in children under the age of 5 years (n=40) most fractures (>50%) occurred due to a fall from height. Most fractures in these children were sustained either inside the house (43%) or outside the house in the backyard (40%) during leisure activities. In children above that age (n = 85) most fractures (35%) were sustained during sports activities. In these children most fractures occurred due to a fall from standing height on a level surface (including twisting).
Fractures of the feet in children under the age of one year seem to be associated with non-accidental injury (Fig. 12.75). However, they are only rarely reported. Studies on feet fractures in association with non-accidental trauma in children are very limited:
-
In 1977, Jaffe and Lasser reported an infant with multiple metatarsal fractures due to non-accidental trauma [432]. They were the first to make a plea to routinely include imaging of the hands and feet in evaluating suspicions of non-accidental circumstances.
-
Nimkin et al. evaluated 11 infants under the age of 10 months with fractures of hands and feet due to non-accidental trauma [235]. A total of 22 fractures were noted. Five infants had a total of 7 fractures of the feet (6× metatarsal fractures and 1× proximal phalangeal fracture). The authors found predominantly torus fractures. According to the authors torus fractures are consistent with forced hyperflexion.
-
Pandya et al. compared 500 child abuse trauma patients with 985 control (accidental) trauma patients [130]. They found 6-foot fractures in each group, with an OR, adjusted for age and sex, of 3.6 (1.1–12.2) for abuse.

Three-month-old infant who was suspected to be a victim of child abuse. As part of the skeletal survey radiographs of the feet were made, these showed bilateral torus fractures of the base of MT-I (open arrow) and a sub-capital torus fracture of MT-II of the left foot (arrow)
The presence of feet fractures in infants and children who received a skeletal survey for evaluation of suspected non-accidental trauma is low and has been reported in only a few studies (Fig. 12.76) [10, 236,237,238]:
-
Barber et al. reported on a study in 567 children, of whom 313 suffered a total of 1,029 fractures [10]. Eleven children (3.5%) had fractures of the foot. In the study by Kleinman et al. 225 out of 365 children had one or more fractures on the skeletal survey. Six children (2.7%) had a total of 9 fractures of the foot [236].
-
Karmazyn et al. studied 930 children of whom 317 had a total of 899 fractures. Two infants had a total of 4 (0.4%) fractures of the hand [237].
-
In the, by far largest, study of Lindberg et al. out of 2890 children 1208 had one or more fractures. Of these children 21 (1.7%) had a total of 20 fractures of the hand [238]. In this study, there were 7 children with either a fracture to the hand or foot, but it was not possible to discriminate as the report spoke of, e.g. a digit fracture.

Two-month-old infant who was suspected to be a victim of child abuse. As part of the skeletal survey radiographs of the feet were made, these showed a torus fracture of the base of MT-I of the right foot (arrow) and a SH-III fracture of the base of the proximal phalanx of the 5th toe (inset)
12.10 Subperiosteal Haemorrhage and Periosteal Reaction
12.10.1 Traumatic Sub-periosteal Haemorrhage
The periosteum of the young growing bone differs from adult bones on two important points which increase the risk of subperiosteal haemorrhage. First of all, the periosteum of the young growing bone is loosely attached to the underlying cortical bone with much less anchoring collagen fibres than in older children and adults. Secondly, during growth the number of periosteal blood vessels is tremendous and with a strong circulation through them [38].
Traumatic subperiosteal haemorrhage can occur as a result of direct or indirect physical forces acting on the bone. Torsional, tractional, frictional, and blunt impact forces have been described to cause subperiosteal bleeding. Traumatic subperiosteal haemorrhage may be present with or without a visible underlying bone fracture. Extensive subperiosteal hematomas have been described in neurofibromatosis case reports as a rare cause of limb hypertrophy after minor (or no) trauma [433,434,435,436].
Whatever cause it has, a subperiosteal haemorrhage will lift the periosteum from the cortex. The presence of the subperiosteal hematoma causes a periosteal reaction consisting of stimulation of the cells in the cambium layer of the periosteum to form subperiosteal new bone. In children, the cambium is thicker than in adults and it has considerable osteoblastic potential. The process from subperiosteal hematoma to periosteal reaction to subperiosteal new bone formation cannot be detected radiographically until calcification has occurred [437]. From fracture dating studies, it is known that SPNBF in long bone fractures is seen as early as day 5–7 after trauma [438,439,440,441].
Periosteal reaction with subperiosteal new bone formation can be provoked by any condition that irritates or elevates the periosteum.
Subperiosteal haemorrhage and periosteal reaction due to trauma must be distinguished from periosteal reaction seen in medical conditions such as vitamin C deficiency, vitamin A intoxication, infantile cortical hyperostosis (Caffey’s disease), osteomyelitis, malignancies (such as leukaemia), and congenital syphilis [442].
In infants between 1 and 6 months subperiosteal new bone formation of the long bones (tibia, femur, humerus, radius) may represent a normal physiological phenomenon (Fig. 12.77) [443, 444]. Physiological subperiosteal new bone formation tends to be bilateral and with a thickness seldom exceeding 2 millimetres.

Physiological sub-periosteal new bone formation along the diaphysis of the (a) femur and (b) the tibia (arrow)
12.10.2 Periosteum, Periosteal Reaction, and the Healing of Fractures
After a fracture, the periosteum stays intact in children more often than in adults, because in children the periosteum is relatively thicker, stronger, and more biologically active. When the periosteum stays intact, the presence of the subperiosteal hematoma causes a periosteal reaction resulting in subperiosteal new bone (Sect. 12.10.1), leading to a continuity of bony tissue will grow over the location of the fracture. This results in a more stable fracture and reduces the chance of dislocation. Essentially, here the periosteum functions as a natural splint.
Moreover, a child’s periosteum has greater potential to form bone than that of an adult. This adds extra stimulus to the healing process, resulting in faster remodelling of fractures in children than in adults. Low-grade deviations in alignment will be corrected faster, and even in gross deviations in alignment excellent remodelling can occur.
12.11 Growth Arrest Lines
12.11.1 General Aspects of Growth Arrest Lines
Growth arrest lines (a.k.a. Harris lines, Park lines, growth retardation lines, growth recovery lines, and Zebra lines) are symmetrical transverse sclerotic lines, perpendicular to the long axis of long bones. These lines are evidence of a disturbance in longitudinal growth, which takes place in the metaphyses. The lines are formed in periods when longitudinal growth has temporarily been delayed or even ceased. When growing of the bone is resumed, the arrest lines will ‘follow’ the longitudinal growth and ‘migrate’ from the metaphysis towards the diaphysis. They may remain visible for months and may eventually disappear [158, 445].
Radiologically these lines can be recognized by the presence of symmetrical thin white lines in long bones. According to Herring, the lines do not become visible until after normal growth has resumed. The lines are most prominent in rapidly growing ends of bones, e.g. the distal femur and the proximal tibia [445]. Often multiple symmetrical thin white lines are visible, indicating alternating cycles of osseous growth arrest and growth resumption, caused by the occurrence of repetitive pathologic levels of stress during bone development [445, 446].
Growth arrest lines were first described by Harris in 1926/1927 [447, 448]. Park described the influence of nutritional disturbances on the growing bone and on the development of these lines [449].
12.11.2 Growth Arrest Lines Due to Childhood Medical Conditions
Growth arrest lines have been reported in a multitude of childhood medical conditions in which a disturbance (a delay or even a temporary cessation) in growth is seen (causes of ‘organic failure to thrive’).
Growth arrest lines are reported to occur due to malnutrition in children, due to poor diet or starvation [449]. They may also occur in every disease with a severe and/or chronic course of systemic illnesses, e.g. infections, including septicaemia [449, 450], hypothyroidism [451], parahypothyroidism [452], Cushing’s syndrome [453], chronic juvenile arthritis [454], and chemotherapy in children with malignancies and the use of other medication, e.g. bisphosphonates (Figs. 12.78a–c, 12.79, and 12.80) [455,456,457,458].

Ten-year-old infant treated for osteomyelitis of the distal femur. (a) Radiograph shows a mixed permeative sclerotic aspect of the distal femur. (b) Radiograph after 2 months shows a growth retardation line in the proximal tibia (arrow). (c) Radiograph after 8 months shows growth of the tibia resulting in the growth retardation line (arrow) moving away from the growth plate

Child with fibrous dysplasia treated with intravenous bisphosphonates. Each growth retardation line corresponds with a course of treatment

Growth retardation lines in a 5-year-old girl after treatment with intravenous bisphosphates, due to fibrous dysplasia in the left maxillary sinus
The lines are also found in children that had been immobilized after orthopaedic surgery [459]. Kennedy et al. reported the occurrence in three girls after a localized trauma. In 2 girls a surgical intervention was needed, in 1 girl no surgical intervention was done [450]:
-
Eight-year girl, following a right-sided tibial spine fracture, which required a surgical intervention (open reduction and internal fixation), resulting in growth arrest lines in the right proximal tibia and fibula and in an intra-epiphyseal distal femoral arrest silhouette.
-
Nine-year-old girl, following a hyperflexion injury of the left knee, resulting in avulsions of her anterior and posterior cruciate ligaments, which required a surgical intervention, resulting in left-sided femoral, fibular and tibial growth arrest lines and in an intra-epiphyseal distal femoral epiphyseal ‘arrest silhouette’.
-
Ten-year-old girl, following a comminuted distal tibial fracture after falling from a height, which required an anatomical reduction.
12.11.3 Growth Arrest Lines Due to Non-organic Failure to Thrive
Growth disturbances are not just caused by medical conditions, resulting in a temporary disturbance of longitudinal growth (Sect. 12.11.2). In the Western world, the most common cause of growth and development retardation—in other words, the most common cause of ‘failure to thrive’—is not ‘organic failure to thrive’, but ‘mixed organic and non-organic failure to thrive’, due to neglect and under stimulation. In neglect, the child is offered insufficient calories (malnourishment—organic failure to thrive) and/or insufficient affective stimulation (non-organic failure to thrive).
As early as 1967, Patton and Gardner mentioned growth arrest lines (metaphyseal growth-retardation lines) in their book on maternal deprivation [460]. Maternal deprivation stands for a serious disturbance in the relation between parent (mother) and child, and a lack of bonding between parent (mother) and child. The deprivation consists of neglect, rejection and isolation of the child. Maternal deprivation syndrome leads to serious growth retardation, delayed skeletal maturation, and retarded motor and intellectual development [461]. This multitude of physical symptoms is nowadays summarized in the term ‘non-organic failure to thrive’. Khadilkar et al. confirmed the observation of Patton and Gardner that the origin of these lines may involve psychological factors [462].
Based on a study concerning 241 tibiae from a medieval Swiss skeletal material Papageorgopoulou et al. concluded that the development of these lines is a result of normal growth and growth spurts, rather than a pure outcome of nutritional or pathologic stress. Animal tests, however, suggest that the lines are formed after an initial retardation or cessation in growth, followed by resumed growth [449, 459]. According to Khadilkar et al., in children they seem to occur in similar circumstances [462]. In case the process is cyclic (repeated periods of delayed growth interspersed with periods of resumed growth) a large number of lines may be found. These lines will always remain visible, up to and including puberty.
When multiple growth arrest lines are found in a child, mixed organic and non-organic failure to thrive will be, after exclusion of other merely organic causes, the most probable cause [462].
Thus far, only two studies have evaluated whether growth arrest lines can be an indicator of non-accidental trauma:
-
Zapala et al. reported that growth arrest lines occur more frequently in infants with a high risk of non-accidental trauma (n = 21) compared to infants with a low risk of non-accidental trauma (n = 52) [463]. Infants at high risk had a significant intracranial injury, retinal haemorrhages, other skeletal injuries, and clinical determination of high risk (child protection team/social work assessment). Infants at low risk had a skull fracture without significant intracranial injury, history of a fall and clinical determination of low risk. The authors concluded that growth arrest lines are significantly more present in children with high risk of abuse (71%) compared to the low-risk group (38%) (p < 0.001; odds ratio 4.0, 95% CI: 1.7–9.5). However, this is equal to a likelihood ratio of 1.9, in other words: growth arrest lines are 1.9 times more likely in infants in the high-risk group than in infants in the low-risk group.
-
Spiller et al. describe 135 children, 58 in the low-risk abuse group, 26 in the neglect group, and 51 in the physical abuse group [464]. Children in the neglect group and physical abuse group had 1.73 (p = 0.007) and 1.84 (p < 0.001) times more growth arrest lines respectively, compared to the low-risk group. The most common locations for growth arrest lines in their population were distal radius, proximal tibia, and distal tibia. In the study of Spiller et al., the specificity for maltreatment (child abuse and neglect) in children with at least 10 growth arrest lines in the long bones was greater than 84%, while sensitivity was less than 35%. This means a LR+ of 2.2, in other words the finding of at least 10 growth arrest lines in the long bones is 2.2 times more likely in children in the high-risk group than in the low-risk group.
References
Carter D (1984) The biomechanics of bone. In: Nahum AM, Melvin J (eds) The biomechanics of trauma. Appleton and Lange, pp 15–90
Kempe CH, Silverman FN, Steele BF, Droegenmueller W, Silver HK (1962) The battered-child syndrome. JAMA 181:17–24
Salter RB, Harris WR (1963) Injuries Involving the Epiphyseal Plate. J Bone Joint Surg 45(3):587–622
Tsai A, McDonald AG, Rosenberg AE, Gupta R, Kleinman PK (2014) High-resolution CT with histopathological correlates of the classic metaphyseal lesion of infant abuse. Pediatr Radiol 44(2):124–140
Kleinman PK, Marks SC Jr (1995) Relationship of the subperiostal bone collar to metaphyseal lesions in abused infants. J Bone Joint Surg Am 77A(10):1471–1476
Kepron C, Pollanen MS (2015) Rickets or abuse? A histologic comparison of rickets and child abuse-related fractures. For Sci Med Pathol 11(1):78–87
Kleinman PK, Marks SC, Blackbourne B (1986) The metaphyseal lesion in abused infants: a radiologic-histopathologic study. AJR Am J Roentgenol 146(5):895–905
Kleinman PK, Rosenberg AE, Tsai A (2015) Skeletal trauma: general considerations. In: Kleinman PK (ed) Diagnostic Imaging of child abuse, 3rd edn. Cambridge Publishers, Cambridge, pp 23–52
Thompson A, Bertocci G, Kaczor K, Smalley C, Pierce MC (2015) Biomechanical investigation of the classic metaphyseal lesion using an immature porcine model. AJR Am J Roentgenol 204(5):W503-9
Barber I, Perez-Rossello JM, Wilson CR, Kleinman PK (2015) The yield of high-detail radiographic skeletal surveys in suspected infant abuse. Pediatr Radiol 45(1):69–80
Adamsbaum C, De Boissieu P, Teglas JP, Rey-Salmon C (2019) Classic metaphyseal lesions among victims of abuse. J Pediatr 209:154–9.e2
Tsai A, Johnston PR, Perez-Rossello JM, Breen MA, Kleinman PK (2018) The distal tibial classic metaphyseal lesion: medial versus lateral cortical injury. Pediatr Radiol 48(7):973–978
Kleinman PK, Marks SC Jr (1996) A regional approach to classic metaphyseal lesions in abused infants: the distal tibia. AJR Am J Roentgenol 166(5):1207–1212
Hymel KP, Spivack BS. The biomechanics of physical injury. In: Reece RM, Ludwig S, eds. Child abuse—medical diagnosis and management: Lippincott Williams en Wilkins, 2001; p. 1-22.
Kleinman PK, Marks SC Jr (1996) A regional approach to the classic metaphyseal lesion in abused infants: the proximal humerus. AJR Am J Roentgenol 167(6):1399–1403
Kleinman PK, Marks SC Jr (1996) A regional approach to the classic metaphyseal lesion in abused infants: the proximal tibia. AJR Am J Roentgenol 166(2):421–426
Kleinman PK, Marks SC Jr (1998) A regional approach to the classic metaphyseal lesion in abused infants: the distal femur. AJR Am J Roentgenol 170(1):43–47
Osier LK, Marks SC Jr, Kleinman PK (1993) Metaphyseal extensions of hypertrophied chondrocytes in abused infants indicate healing fractures. J Pediatr Orthop 13(2):249–254
DeLee JC, Wilkins KE, Rogers LF, Rockwood CA (1980) Fracture-separation of the distal humeral epiphysis. J Bone Joint Surg Am 62(1):46–51
Karmazyn B, Marine MB, Wanner MR, Sağlam D, Jennings SG, Hibbard RA (2020) Establishing signs for acute and healing phases of distal tibial classic metaphyseal lesions. Pediatr Radiol. 50(5):715–725
Kleinman PK, Marks SC Jr, Spevak MR, Belanger PL, Richmond JM (1991) Extension of growth-plate cartilage into the metaphysis: a sign of healing fracture in abused infants. AJR Am J Roentgenol 156(4):775–779
Tsai A, Connolly SA, Ecklund K, Johnston PR, Kleinman PK (2019) Subperiosteal new bone formation with the distal tibial classic metaphyseal lesion: prevalence on radiographic skeletal surveys. Pediatr Radiol
Offiah A, van Rijn RR, Perez-Rossello JM, Kleinman PK (2009) Skeletal imaging of child abuse (non-accidental injury). Pediatr Radiol 39(5):461–470
Kleinman PK (2008) Problems in the diagnosis of metaphyseal fractures. Pediatr Radiol 38(Suppl 3):S388–SS94
Kleinman PK, Nimkin K, Spevak MR et al (1996) Follow-up skeletal surveys in suspected child abuse. AJR Am J Roentgenol 167(4):893–896
Harper NS, Eddleman S, Lindberg DM (2013) The utility of follow-up skeletal surveys in child abuse. Pediatrics 131(3):e672-8
Harlan SR, Nixon GW, Campbell KA, Hansen K, Prince JS (2009) Follow-up skeletal surveys for nonaccidental trauma: can a more limited survey be performed? Pediatr Radiol 39(9):962–968
Zimmerman S, Makoroff K, Care M, Thomas A, Shapiro R (2005) Utility of follow-up skeletal surveys in suspected child physical abuse evaluations. Child Abuse Negl 29(10):1075–1083
The Royal College of Radiologists (RCR) and the Society and College of Radiographers (SCoR). The radiological investigation of suspected physical abuse in children. 2017. [05-07-2021]; Available from: https://www.rcr.ac.uk/publication/radiological-investigation-suspected-physical-abuse-children.
Drubach LA, Sapp MV, Laffin S, Kleinman PK (2008) Fluorine-18 NaF PET imaging of child abuse. Pediatr Radiol 38(7):776–779
Perez-Rossello JM, Connolly SA, Newton AW, Zou KH, Kleinman PK (2010) Whole-body MRI in suspected infant abuse. AJR Am J Roentgenol 195(3):744–750
Proisy M, Vivier PH, Morel B et al (2021) Whole-body MR imaging in suspected physical child abuse: comparison with skeletal survey and bone scintigraphy findings from the PEDIMA prospective multicentre study. Eur Radiol
Marine MB, Hibbard RA, Jennings SG, Karmazyn B (2019) Ultrasound findings in classic metaphyseal lesions: emphasis on the metaphyseal bone collar and zone of provisional calcification. Pediatr Radiol 49(7):913–921
Karmazyn B, Marine MB, Wanner MR et al (2020) Accuracy of ultrasound in the diagnosis of classic metaphyseal lesions using radiographs as the gold standard. Pediatr Radiol
Tsai A, McDonald AG, Rosenberg AE, Stamoulis C, Kleinman PK (2013) Discordant radiologic and histological dimensions of the zone of provisional calcification in fetal piglets. Pediatr Radiol 43(12):1606–1614
Pierce MC, Bertocci GE, Vogeley E, Moreland MS (2004) Evaluating long bone fractures in children: a biomechanical approach with illustrative cases. Child Abuse Negl 28(5):505–524
Kleinman PL, Zurakowski D, Strauss KJ et al (2008) Detection of simulated inflicted metaphyseal fractures in a fetal pig model: image optimization and dose reduction with computed radiography. Radiology 247(2):381–390
Caffey J (1957) Some traumatic lesions in growing bones other than fractures and dislocations: clinical and radiological features: The Mackenzie Davidson Memorial Lecture. Br J Radiol 30(353):225–238
Loder RT, Bookout C (1991) Fracture patterns in battered children. J Orthopaed Trauma 5(4):428–433
Worlock P, Stower M, Barbor P (1986) Patterns of fractures in accidental and non-accidental injury in children: a comparative study. BMJ 293:100–102
Lindberg DM, Berger RP, Reynolds MS, Alwan RM, Harper NS (2014) Yield of skeletal survey by age in children referred to abuse specialists. J Pediatr 164(6):1268–73.e1
Kleinman PK, Perez-Rossello JM, Newton AW, Feldman HA, Kleinman PL (2011) Prevalence of the classic metaphyseal lesion in infants at low versus high risk for abuse. AJR Am J Roentgenol 197(4):1005–1008
Kleinman PK, Marks SC Jr, Richmond JM, Blackbourne BD (1995) Inflicted skeletal injury: a postmortem radiologic-histopathologic study in 31 infants. AJR AmJ Roentgenol 165(3):647–650
Thackeray JD, Wannemacher J, Adler BH, Lindberg DM (2016) The classic metaphyseal lesion and traumatic injury. Pediatr Radiol 46(8):1128–1133
Sieswerda-Hoogendoorn T, van Rijn RR, Robben SGF (2014) Classic metaphyseal lesion following vaginal breech birth, a rare birth trauma. JoFRI 2(1):2–4
Gowda SR, Vecsei FA, Fairhurst J, Aarvold A (2018) Metaphyseal corner fracture caused in utero by external cephalic version—a rare presentation. Case Rep Perinatal Med 7:1
Lysack JT, Soboleski D (2003) Classic metaphyseal lesion following external cephalic version and cesarean section. Pediatr Radiol 33(6):422–424
O'Connell A, Donoghue VB (2007) Can classic metaphyseal lesions follow uncomplicated caesarean section? Pediatr Radiol 37(5):488–491
Lee GS, Methratta ST, Frasier LD (2019) Classic metaphyseal lesion of distal tibia following footling breech delivery. Pediatr Radiol 49(13):1840–1842
Buonuomo PS, Ruggiero A, Zampino G, Maurizi P, Attinà G, Riccardi R (2006) A newborn with multiple fractures as first presentation of infantile myofibromatosis. J Perinatol 26(10):653–655
Grayev AM, Boal DK, Wallach DM, Segal LS (2001) Metaphyseal fractures mimicking abuse during treatment for clubfoot. Pediatr Radiol 31(8):559–563
Burrell T, Opfer E, Berglund L, Lowe LH, Anderst J (2015) A witnessed case of a classic metaphyseal fracture caused during IV line placement in a child: Insight into mechanism of injury. J Forensic Leg Med 35:51–53
Della Grotta LM, Marine MB, Harris TL, Karmazyn B (2019) Classic metaphyseal lesion acquired during physical therapy. Clin Imaging 54:100–102
Culotta PA, Burge LR, Bachim AN, Donaruma-Kwoh M (2020) Are classic metaphyseal lesions pathognomonic for child abuse? Two cases of motor vehicle collision-related extremity CML and a review of the literature. J Forensic Leg Med 74:102006
Kleinman PK, Belanger PL, Karellas A, Spevak MR (1991) Normal metaphyseal radiologic variants not to be confused with findings of infant abuse. AJR Am J Roentgenol 156(4):781–783
Quigley AJ, Stafrace S (2014) Skeletal survey normal variants, artefacts and commonly misinterpreted findings not to be confused with non-accidental injury. Pediatr Radiol. 44(1):82–93. quiz 79-81
Norrell K, Hennrikus W (2017) The risk of assuming abuse in an infant with an isolated metaphyseal lesion: a case report. JBJS Case Connect 7(3):e69
Kleinman PK, Sarwar ZU, Newton AW, Perez-Rossello JM, Rebello G, Herliczek TW (2009) Metaphyseal fragmentation with physiologic bowing: a finding not to be confused with the classic metaphyseal lesion. AJR Am J Roentgenol 192(5):1266–1268
Mizuta T, Benson WM, Foster BK, Paterson DC, Morris LL (1987) Statistical analysis of the incidence of physeal injuries. J Pediatr Orthop 7(5):518–523
Cepela DJ, Tartaglione JP, Dooley TP, Patel PN (2016) Classifications in brief: Salter-Harris classification of pediatric physeal fractures. Clin Orthop Relat Res 474(11):2531–2537
Little JT, Klionsky NB, Chaturvedi A, Soral A, Chaturvedi A (2014) Pediatric distal forearm and wrist injury: an imaging review. Radiographics 34(2):472–490
Rogers LF, Poznanski AK (1994) Imaging of epiphyseal injuries. Radiology 191(2):297–308
Kothadia S, Birole U, Ranade A (2017) Paediatric Salter-Harris type IV injury of distal tibia with talus fracture. BMJ Case Rep 2017
Supakul N, Hicks RA, Caltoum CB, Karmazyn B (2015) Distal humeral epiphyseal separation in young children: an often-missed fracture-radiographic signs and ultrasound confirmatory diagnosis. AJR Am J Roentgenol 204(2):W192–W198
Nimkin K, Kleinman PK, Teeger S, Spevak MR (1995) Distal humeral physeal injuries in child abuse: MR imaging and ultrasonography findings. Pediatr Radiol 25(7):562–565
Marine MB, Forbes-Amrhein MM (2021) Fractures of child abuse. Pediatr Radiol 51(6):1003–1013
Peterson HA, Madhok R, Benson JT, Ilstrup DM, Melton LJ 3rd. (1994) Physeal fractures: Part 1. Epidemiology in Olmsted County, Minnesota, 1979-1988. J Pediatr Orthop 14(4):423–430
Tharakan SJ, Lee RJ, White AM, Lawrence JT (2016) Distal humeral epiphyseal separation in a newborn. Orthopedics 39(4):e764-7
Gigante C, Kini SG, Origo C, Volpin A (2017) Transphyseal separation of the distal humerus in newborns. Chin J Traumatol = Zhonghua chuang shang za zhi 20(3):183–186
Ogden JA, Lee KE, Rudicel SA, Pelker RR (1984) Proximal femoral epiphysiolysis in the neonate. J Pediatr Orthop 4(3):285–292
Banagale RC, Kuhns LR (1983) Traumatic separation of the distal femoral epiphysis in the newborn. J Pediatr Orthop. 3(3):396–398
Eliahou R, Simanovsky N, Hiller N, Simanovsky N (2006) Fracture-separation of the distal femoral epiphysis in a premature neonate. J Ultrasound Med 25(12):1603–1605
Baker AM, Methratta ST, Choudhari AK (2012) Transphyseal fracture of the distal humerus in a neonate. West J Emerg Med 12(2):173
Triplet JJ, Samora WP, Balch SJ (2018) Distal humeral physeal separation in a newborn: a case report and review of the literature. Curr Orthop Pract 29(6):611–615
Shalaby-Rana E, Hinds TS, Deye K, Jackson AM (2020) Proximal femoral physeal fractures in children: a rare abusive injury. Pediatr Radiol 50(8):1115–1122
Jones JCW, Feldman KW, Bruckner JD (2004) Child abuse in infants with proximal physeal injuries of the femur. Pediatr Emerg Care 20(3):157–161
Nenopoulos A, Beslikas T, Gigis I, Sayegh F, Christoforidis I, Hatzokos I (2015) The role of CT in diagnosis and treatment of distal tibial fractures with intra-articular involvement in children. Injury 46(11):2177–2180
Ahn L, Williams B (2021) Triplane fractures. Orthobullets. [15-07-2021]; Available from: https://www.orthobullets.com/pediatrics/4029/triplane-fractures
Caviglia H, Garrido CP, Palazzi FF, Meana NV (2005) Pediatric fractures of the humerus. Clin Orthop Relat Res 432:49–56
Hohl JC (1976) Fractures of the humerus in children. Orthop Clin North Am 7(3):557–571
Landin LA (1983) Fracture patterns in children. Analysis of 8, 682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950-1979. Acta Orthop Scand Suppl 202:1–109
Landin LA (1997) Epidemiology of children's fractures. J Pediatr Orthop Part B 6(2):79–83
Rose SH, Melton LJ 3rd, Morrey BF, Ilstrup DM, Riggs BL (1982) Epidemiologic features of humeral fractures. Clin Orthop Relat Res 168:24–30
Shrader MW (2007) Proximal humerus and humeral shaft fractures in children. Hand Clin 23(4):431–435
Hannonen J, Hyvönen H, Korhonen L, Serlo W, Sinikumpu JJ (2019) The incidence and treatment trends of pediatric proximal humerus fractures. BMC Musculoskelet Disord 20(1):571
Watts E, Shirley E, Skaggs DL (2021) Proximal humerus fracture—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4004/proximal-humerus-fracture%2D%2Dpediatric
Popkin CA, Levine WN, Ahmad CS (2015) Evaluation and management of pediatric proximal humerus fractures. J Am Acad Orthop Surg 23(2):77–86
Chae W, Khan A, Abbott S, Assiotis A (2019) Proximal humerus fractures in children: experience from a Central London Paediatric Orthopaedic Service. Open Orthop J 13:202–207
Wimberly RL (n.d.) Proximal humerus fractures. POSNA. [25-11-2021]; Available from: https://posna.org/Physician-Education/Study-Guide/Proximal-Humerus-Fractures
Neer CS 2nd, Horwitz BS (1965) Fractures of the proximal humeral epiphysial plate. Clin Orthop Relat Res 41:24–31
Lefèvre Y, Journeau P, Angelliaume A, Bouty A, Dobremez E (2014) Proximal humerus fractures in children and adolescents. Orthop Traumatol Surg Res 100(1 Suppl):S149-56
Canpolat FE, Köse A, Yurdakök M (2010) Bilateral humerus fracture in a neonate after cesarean delivery. Arch Gynecol Obstet 281(5):967–969
Dias E (2012) Bilateral humerus fracture following birth trauma. J Clin Neonatol 1(1):44–45
Camus M, Lefebvre G, Veron P, Darbois Y (1985) Traumatismes obstétricaux du nouveau-né. Enquête rétrospective à propos de 20409 naissances [Obstetrical injuries of the newborn infant. Retrospective study apropos of 20,409 births]. J Gynecol Obstet Biol Reprod (Paris) 14(8):1033–1043
Gagnaire JC, Thoulon JM, Chappuis JP, Varnier CH, Mered B (1975) Les traumatismes du membre supérieur du noveau-né constatés à la naissance [Injuries to the upper extremities in the newborn diagnosed at birth]. J Gynecol Obstet Biol Reprod 4(2):245–254
King J, Diefendorf D, Apthorp J, Negrete VF, Carlson M (1988) Analysis of 429 fractures in 189 battered children. J Pediatr Orthop 8(5):585–589
Jones GP, Seguin J, Shiels WE 2nd (2003) Salter-Harris II fracture of the proximal humerus in a preterm infant. Am J Perinatol 20(5):249–253
Dalldorf PG, Bryan WJ (1994) Displaced Salter-Harris type I injury in a gymnast. A slipped capital humeral epiphysis? Orthop Rev 23(6):538–541
Ahn JI, Park JS (1994) Pathological fractures secondary to unicameral bone cysts. Int Orthop 18(1):20–22
Barber DB, Janus RB, Wade WH (1996) Neuroarthropathy: an overuse injury of the shoulder in quadriplegia. J Spinal Cord Med 19(1):9–11
Lock TR, Aronson DD (1989) Fractures in patients who have myelomeningocele. J Bone Joint Surg Am. 71(8):1153–1157
Marengo L, Rousset M, Paonessa M et al (2016) Displaced humeral shaft fractures in children and adolescents: results and adverse effects in patients treated by elastic stable intramedullary nailing. Eur J Orthop Surg Traumatol Orthop Traumatol 26(5):453–459
Rush J. Scapula fractures. POSNA (Pediatric Orthopaedic Society of North America); [29-07-20]; Available from: https://posna.org/Physician-Education/Study-Guide/Scapula-Fractures.
Whooley PJ. Humeral shaft injuries. 2021. [25-11-2021]; Available from: https://dontforgetthebubbles.com/humeral-shaft-injuries/.
Bayram S, Mert L, Anarat FB, Chodza M, Ergin ÖN (2018) A Newborn with Multiple Fractures in Osteogenesis Imperfecta: A Case Report. J Orthop Case Rep 8(3):71–73
Barker TH (1857) On intrauterine fractures: with an illustrative case. Br Med J 2(39):806–809
Madsen ET (1955) Fractures of the extremities in the newborn. Acta Obstet Gynecol Scand 34(1):41–74
Sherr-Lurie N, Bialik GM, Ganel A, Schindler A, Givon U (2011) Fractures of the humerus in the neonatal period. Isr Med Assoc J 13(6):363–365
Shulman BH, Terhune CB (1951) Epiphyseal injuries in breech delivery. Pediatrics 8(5):693–700
Dameron TB Jr, Reibel DB (1969) Fractures involving the proximal humeral epiphyseal plate. J Bone Joint Surg Am 51(2):289–297
Lemperg R, Liliequist B (1970) Dislocation of the proximal epiphysis of the humerus in newborns. Acta Paediatr Scand 59(4):377–380
Reed MH, Letts RM, Pollock AN (1994) Birth fractures. In: Letts RM (ed) Management of pediatric fractures. Churchill Livingstone, pp 1049–1061
Kaya B, Daglar K, Kirbas A, Tüten A (2015) Humerus diaphysis fracture in a newborn during vaginal breech delivery. Case Rep Obstet Gynecol 2015:489108
Hamilçıkan Ş, Yılmaz K, Can E (2018) Humeral diaphysis fracture in a neonate after vaginal delivery. Sisli Etfal Hastan Tip Bul 52(1):51–53
Tan TS, Mohamed A, Dharmaraj S (2016) Bilateral fractures in a shoulder dystocia delivery. BMJ Case Rep 2016
Ryan LM (2011) Midshaft humeral fractures in children. UpToDate. [25-11-2021]; Available from: https://somepomed.org/articulos/contents/mobipreview.htm?40/18/41262
von Heideken J, Thiblin I, Högberg U (2020) The epidemiology of infant shaft fractures of femur or humerus by incidence, birth, accidents, and other causes. BMC Musculoskelet Disord 21(1):840
Rehm A, Promod P, Ogilvy-Stuart A (2020) Neonatal birth fractures: a retrospective tertiary maternity hospital review. J Obstet Gynaecol 40(4):485–490
Suleiman FA, Almaaitah AA, Aqrabawi HE (2016) Upper limb birth trauma in a Jordanian population: a prospective study at King Hussein Medical Centre, Amman, Jordan. JPMA J Pak Med Assoc 66(11):1422–1426
Basha A, Amarin Z, Abu-Hassan F (2013) Birth-associated long-bone fractures. Int J Gynaecol Obstet 123(2):127–130
Bhat BV, Kumar A, Oumachigui A (1994) Bone injuries during delivery. Indian J Pediatr 61(4):401–405
Carter S (2021) Humeral shaft fracture. Radiopaedia. Available from: https://radiopaedia.org/articles/humeral-shaft-fracture-1
Strait RT, Siegel RM, Shapiro RA (1995) Humeral fractures without obvious etiologies in children less than 3 years of age: when is it abuse? Pediatrics 96(4 Pt 1):667–671
Leventhal JM, Thomas SA, Rosenfield NS, Markowitz RI (1993) Fractures in young children. Distinguishing child abuse from unintentional injuries. Am J Dis Child 147:87–92
Thomas SA, Rosenfield NS, Leventhal JM, Markowitz RI (1991) Long-bone fractures in young children: distinguishing accidental injuries from child abuse. Pediatrics 88(3):471–476
Kowal-Vern A, Paxton TP, Ros SP, Lietz H, Fitzgerald M, Gamelli RL (1992) Fractures in the under-3-year-old age cohort. Clin Pediatr (Phila). 31(11):653–659
Rosenberg N, Bottenfield G (1982) Fractures in infants: a sign of child abuse. Ann Emerg Med 11(4):178–180
Williams R, Hardcastle N (2005) Best evidence topic report. Humeral fractures and non-accidental injury in children. Emerg Med J 22(2):124–125
Shaw BA, Murphy KM, Shaw A, Oppenheim WL, Myracle MR (1997) Humerus shaft fractures in young children: accident or abuse? J Pediatr Orthop. 17(3):293–297
Pandya NK, Baldwin K, Wolfgruber H, Christian CW, Drummond DS, Hosalkar HS (2009) Child abuse and orthopaedic injury patterns: analysis at a level I pediatric trauma center. J Pediatr Orthop 29(6):618–625
Pandya NK, Baldwin KD, Wolfgruber H, Drummond DS, Hosalkar HS (2010) Humerus fractures in the pediatric population: an algorithm to identify abuse. J Pediatr Orthop Part B. 19(6):535–541
Samardzić M, Grujicić D, Milinković ZB (1990) Radial nerve lesions associated with fractures of the humeral shaft. Injury 21(4):220–222
Hannonen J, Sassi E, Hyvönen H, Sinikumpu JJ (2020) A shift from non-operative care to surgical fixation of pediatric humeral shaft fractures even though their severity has not changed. Front Pediatr 8:580272
Raza M, Anestis I (2021) Paediatric humeral shaft fractures: an overview and modern management approach. Int J Orthop 8(2):1443–1146
Hymel KP, Jenny C (1996) Abusive spiral fractures of the humerus: a videotaped exception. Arch Pediatr Adolesc Med 150(2):226–227
Somers JM, Halliday KE, Chapman S (2014) Humeral fracture in non-ambulant infants-a possible accidental mechanism. Pediatr Radiol 44(10):1219–1223
Altai Z, Viceconti M, Li X, Offiah AC (2020) Investigating rolling as mechanism for humeral fractures in non-ambulant infants: a preliminary finite element study. Clin Radiol 75(1):78.e9-.e16
Silverio L (2018) Distal hymerus fracture in children – emergency management. DynaMed. [25-11-2021]; Available from: https://www.dynamed.com/management/distal-humerus-fracture-in-children-emergency-management
Smithuis R (2008) Elbow fractures in children. Radiology Assistant. [25-11-2021]; Available from: https://radiologyassistant.nl/pediatrics/hip/fractures-in-children-1
Patel B, Reed M, Patel S (2009) Gender-specific pattern differences of the ossification centers in the pediatric elbow. Pediatr Radiol 39(3):226–231
Goodwin SJ, Irwin LJ, Irwin GJ (2019) Gender differences in the order of appearance of elbow ossification centres. Scott Med J 64(1):2–9
Brubacher JW, Dodds SD (2008) Pediatric supracondylar fractures of the distal humerus. Curr Rev Musculoskelet Med 1(3-4):190–196
Holt JB, Glass NA, Shah AS (2018) Understanding the epidemiology of pediatric supracondylar humeral fractures in the United States: identifying opportunities for intervention. J Pediatr Orthop 38(5):e245–ee51
Woon C, Souder C, Skaggs D (2021) Supracondylar fracture—pediatric. Orthobullets. [cited 25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4007/supracondylar-fracture%2D%2Dpediatric
Knipe H (2021) Supracondylar humeral fracture. Radiopaedia. [25-11-2021]; Available from: https://radiopaedia.org/articles/supracondylar-humeral-fracture-2
Carter S (2021) Flexion supracondylar fracture. Radiopaedia. [25-11-2021]; Available from: https://radiopaedia.org/articles/flexion-supracondylar-fracture?lang=us
Reisdorff EJ, Roberts MR, Wiegenstein JG (1993) Pediatric emergency medicine. WB Saunders Co
Kemp AM, Dunstan F, Harrison S et al (2008) Patterns of skeletal fractures in child abuse: systematic review. BMJ 337:a1518
Rosado N, Ryznar E, Flaherty EG (2017) Understanding humerus fractures in young children: abuse or not abuse? Child Abuse Negl 73:1–7
Lawton L (1994) Fractures of the distal radius and ulna. In: Letts RM (ed) Management of pediatric fractures. Churchill-Livingstone, pp 345–368
Rinaldi JM, Hennrikus WL (2018) Are supracondylar fractures of the elbow in children caused by child abuse? Pediatrics 141(1 Meeting Abstract):300
Shaath K, Souder C, Skaggs DL (2021) Lateral condyle fracture. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4009/lateral-condyle-fracture%2D%2Dpediatric
Tejwani N, Phillips D, Goldstein RY (2011) Management of lateral humeral condylar fracture in children. J Am Acad Orthop Surg 19(6):350–358
Carter S (2021) Lateral humeral condyle fracture. Radiopaedia. [25-11-2021]; Available from: https://radiopaedia.org/articles/lateral-humeral-condyle-fracture-1
Offiah AC, Hall CM (2009) Diaphyseal fractures. In: Offiah AC, Hall CM (eds) Radiological atlas of child abuse. Radcliff Publishing Ltd, London, pp 81–117
Walsh JJ (2020) Medial humeral condyle fracture. Medscape. [25-11-2021]; Available from: https://emedicine.medscape.com/article/1231290-overview#showall
Tepeneu NF (2018) Fractures of the humeral condyles in children—a review. J Med Psych Trauma 1(1):3–13
Kleinman PK (2015) Upper extremity trauma. In: Kleinman PK (ed) Diagnostic imaging of child abuse, 3rd edn. Cambridge University Press, Cambridge, pp 121–163
Gottschalk HP, Eisner E, Hosalkar HS (2012) Medial epicondyle fractures in the pediatric population. J Am Acad Orthop Surg 20(4):223–232
Bauer S, Dunne B, Whitewood C (2012) Simultaneous bilateral elbow dislocation with bilateral medial epicondyle fractures in a 13-year-old female gymnast with hyperlaxity. BMJ Case Rep 2012
DeFroda S, McGlone P, Levins J, O'Donnell R, Cruz AI, Kriz PK (2020) Shoulder and elbow injuries in the adolescent throwing athlete. R I Med J (2013) 103(7):21–29
Sperry K, Pfalzgraf R (1990) Inadvertent clavicular fractures caused by "chiropractic" manipulations in an infant: an unusual form of pseudoabuse. J Forensic Sci 35(5):1211–1216
Shore RM (2018) What are pediatric transphyseal fractures. Medscape. [25-11-2021]; Available from: https://www.medscape.com/answers/415822-185743/what-are-pediatric-transphyseal-fractures
Abzug JM, Ho CA, Ritzman TF, Brighton BK (2016) Transphyseal fracture of the distal humerus. J Am Acad Orthop Surg 24(2):e39–e44
Makanji H, Glotzbecker M (2021) Distal humerus physeal separation—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4006/distal-humerus-physeal-separation%2D%2Dpediatric
McLoughlin E, Stanhope B, Johnson K (2017) The answer is not always in black and white: a frequently missed diagnosis in a child presenting with elbow pain. Emerg Med J 34(8):524–525
Patil MN, Palled E (2015) Epihyseal separation of lower end humerus in a neonate-diagnostic and management difficulty. J Orthop Case Rep 5(4):7–9
Navallas M, Díaz-Ledo F, Ares J et al (2013) Distal humeral epiphysiolysis in the newborn: utility of sonography and differential diagnosis. Clin Imaging 37(1):180–184
Mane PP, Challawar NS, Shah H (2016) Late presented case of distal humerus epiphyseal separation in a newborn. BMJ Case Rep 2016
Murthy PG, Vuillermin C, Naqvi MN, Waters PM, Bae DS (2017) Capitellar fractures in children and adolescents: classification and early results of treatment. J Bone Joint Surg Am 99(15):1282–1290
Ertl JP (2020) Capitellar fractures. Medscape. [25-11-2021]; Available from: https://emedicine.medscape.com/article/1238203-overview#showall
Yoon R, Sanchez-Sotelo J, on behalf of ‘American Shoulder and Elbow Surgeons’ (2021) Capitellum fractures. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/trauma/1023/capitellum-fractures
Thomas EM, Tuson KW, Browne PS (1975) Fractures of the radius and ulna in children. Injury 7(2):120–124
Schweich P (2021) Distal forearm fractures in children: diagnosis and assessment. UpToDate. [25-11-2021]; Available from: https://www.uptodate.com/contents/distal-forearm-fractures-in-children-diagnosis-and-assessment
Wolfe JA, Wolfe H, Banaag A, Tintle S, Perez Koehlmoos T (2019) Early pediatric fractures in a universally insured population within the United States. BMC Pediatr 19(1):343
Edgington J, Glotzbecker M (2021) Both bone forearm fracture—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4126/both-bone-forearm-fracture%2D%2Dpediatric
Cheng JC, Shen WY (1993) Limb fracture pattern in different pediatric age groups: a study of 3,350 children. J Orthop Trauma 7(1):15–22
Johnson PG, Szabo RM (1993) Angle measurements of the distal radius: a cadaver study. Skeletal Radiol 22(4):243–246
Reed MH (1977) Fractures and dislocations of the extremities in children. J Trauma 17(5):351–354
Bailey DA, Wedge JH, McCulloch RG, Martin AD, Bernhardson SC (1989) Epidemiology of fractures of the distal end of the radius in children as associated with growth. J Bone Joint Surg Am 71(8):1225–1231
Qudsi R, Souder C (2021) Distal radius fractures—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4014/distal-radius-fractures%2D%2Dpediatric
Tredwell SJ, Van Peteghem K, Clough M (1984) Pattern of forearm fractures in children. J Pediatr Orthop 4(5):604–608
Hermans K, Fransz D, Walbeehm-Hol L, Hustinx P, Staal H (2021) Is a Parry Fracture-an isolated fracture of the ulnar shaft-associated with the probability of abuse in children between 2 and 16 years old? Children (Basel). 8:8
Perkins CA, Busch MT, Christino MA et al (2018) Olecranon fractures in children and adolescents: outcomes based on fracture fixation. J Children's Orthop 12(5):497–501
Holme TJ, Karbowiak M, Arnander M, Gelfer Y (2020) Paediatric olecranon fractures: a systematic review. EFORT Open Rev 5(5):280–288
Edgington J, Andras L (2021) Radial head and neck fractures—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4011/radial-head-and-neck-fractures%2D%2Dpediatric
Perron AD, Hersh RE, Brady WJ, Keats TE (2001) Orthopedic pitfalls in the ED: Galeazzi and Monteggia fracture-dislocation. Am J Emerg Med 19(3):225–228
Berger R, Souder C (2021) Galeazzi fracture—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4016/galeazzi-fracture%2D%2Dpediatric
Allen D (2021) Monteggia fracture—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4015/monteggia-fracture%2D%2Dpediatric
Hupin Debeurme M, Powers J (2021) Monteggia fracture. POSNA. [25-11-2021]; Available from: https://posna.org/Physician-Education/Study-Guide/Monteggia-Fracture
Korner J, Hansen M, Weinberg A, Hessmann M, Rommens P (2004) Monteggia fractures in childhood diagnosis and management in acute and chronic cases. Eur J Trauma 30:361–370
Shonnard PY, DeCoster TA (1994) Combined Monteggia and Galeazzi fractures in a child's forearm. A case report. Orthop Rev 23(9):755–759
Maeda H, Yoshida K, Doi R, Omori O (2003) Combined Monteggia and Galeazzi fractures in a child: a case report and review of the literature. J Orthop Trauma 17(2):128–131
Knipe H, Jones J (2021) Bowing fracture. Radiopedia. [25-11-2021]; Available from: https://radiopaedia.org/articles/bowing-fracture?lang=us
Price CT, Mencio GA (2001) Injuries to the shafts of the radius and ulna. In: Beatty JH, Kasser JR (eds) Rockwood and Wilkins’ Fractures in Children, 5th edn. Lippincott Williams en Wilkins, pp 433–482
Onimus M, Lebrat J, Scherrer M, Weber R, Cousin J, Samaki M (1991) Pregnancy and traffic accident. A case report [Grossesse et accident de la voie publique. A propos d'un cas]. Rev Fr Gynecol Obstet 86(4):315–317
Ho CA, Richards BS, Ezaki M (2014) Congenital band syndrome with pseudarthrosis of the radius and ulna and impending vascular compromise: a case report. J Pediatr Orthop. 34(6):e14–e18
Angelis S, Vynichakis G, Trellopoulos A, Mirtsios H, Michelarakis J (2019) Strangling congenital constriction ring band of the forearm with fracture: a rare case report. Cureus 11(3):e4189
Thompson KA, Satin AJ, Gherman RB (2003) Spiral fracture of the radius: an unusual case of shoulder dystocia-associated morbidity. Obstet Gynecol 102(1):36–38
Ryan LM, Teach SJ, Searcy K et al (2010) Epidemiology of pediatric forearm fractures in Washington, DC. J Trauma 69(4 Suppl):S200-5
Watson WL, Ozanne-Smith J (1993) The use of child safety restraints with nursery furniture. J Paediatr Child Health 29(3):228–232
Smith GA, Dietrich AM, Garcia CT, Shields BJ (1996) Injuries to children related to shopping carts. Pediatrics 97(2):161–165
Smith GA, Bowman MJ, Luria JW, Shields BJ (1997) Babywalker-related injuries continue despite warning labels and public education. Pediatrics 100(2):E1
Loder RT, Feinberg JR (2007) Orthopaedic injuries in children with nonaccidental trauma: demographics and incidence from the 2000 kids' inpatient database. J Pediatr Orthop 27(4):421–426
Van As AB, Naidoo S, Craig R, Franklin J (2007) Fracture patterns in non-accidentally injured children at Red Cross Children’s Hospital. SAJCH. 1(3):102–105
Browner EA (2013) Nursemaid's elbow (annular ligament displacement). Pediatr Rev 34(8):366–367. discussion 7
Campo TM (2011) A case of subluxation of the radial head: nursemaids' elbow. Adv Emerg Nurs J 33(1):8–14
Schunk JE (1990) Radial head subluxation: epidemiology and treatment of 87 episodes. Ann Emerg Med 19(9):1019–1023
Michaels MG (1989) A case of bilateral nursemaid's elbow. Pediatr Emerg Care 5(4):226–227
Meiner EM, Sama AE, Lee DC, Nelson M, Katz DS, Trope A (2004) Bilateral nursemaid's elbow. Am J Emerg Med 22(6):502–503
Vitello S, Dvorkin R, Sattler S, Levy D, Ung L (2014) Epidemiology of nursemaid's elbow. West J Emerg Med 15(4):554–557
Thompson GH (2001) Dislocations of the elbow. In: Beaty JH, Kasser JR (eds) Rockwood and Wilkins’ fractures in children, 5th edn. Lippincott Williams en Wilkins, pp 705–739
Newman J (1985) "Nursemaid's elbow" in infants six months and under. J Emerg Med 2(6):403–404
Shaath K, Shirley E (2021) Nursemaid's elbow. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4012/nursemaids-elbow
Rudloe TF, Schutzman S, Lee LK, Kimia AA (2012) No longer a "nursemaid's" elbow: mechanisms, caregivers, and prevention. Pediatr Emerg Care 28(8):771–774
Kunkler CE (2000) Did you check your nursemaid's elbow? Orthop Nurs 19(4):49–52. quiz 3-5
Yamanaka S, Goldman RD (2018) Pulled elbow in children. Can Fam Physician 64(6):439–441
Li N, Khoo B, Brown L, Young T (2021) Nonaxial traction mechanisms of nursemaid's elbow. Pediatr Emerg Care 37(6):e292–e2e4
Shah SS, Rochette LM, Smith GA (2012) Epidemiology of pediatric hand injuries presenting to United States emergency departments, 1990 to 2009. J Trauma Acute Care Surg 72(6):1688–1694
Nellans KW, Chung KC (2013) Pediatric hand fractures. Hand Clin 29(4):569–578
Wahba G, Cheung K (2018) Pediatric hand injuries: practical approach for primary care physicians. Can Fam Physician 64(11):803–810
Vadivelu R, Dias JJ, Burke FD, Stanton J (2006) Hand injuries in children: a prospective study. J Pediatr Orthop 26(1):29–35
Kreutz-Rodrigues L, Gibreel W, Moran SL, Carlsen BT, Bakri K (2020) Frequency, pattern, and treatment of hand fractures in children and adolescents: a 27-year review of 4356 pediatric hand fractures. Hand (N Y):1558944719900565
Chung KC, Spilson SV (2001) The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am 26(5):908–915
Brodeur AE, Monteleone JA (1994) Child maltreatment. A clinical guide and reference. GW Med:32
Bauer A (n.d.) Study guide: hand trauma. POSNA (Pediatr Orthop Soc North Am). [25-11-2021]; Available from: https://posna.org/Physician-Education/Study-Guide/Hand-Trauma
Worlock PH, Stower MJ (1986) The incidence and pattern of hand fractures in children. J Hand Surg Br. 11(2):198–200
Barton NJ (1979) Fractures of the phalanges of the hand in children. Hand 11(2):134–143
Hastings H 2nd, Simmons BP (1984) Hand fractures in children. A statistical analysis. Clin Orthop Relat Res 188:120–130
Liu EH, Alqahtani S, Alsaaran RN, Ho ES, Zuker RM, Borschel GH (2014) A prospective study of pediatric hand fractures and review of the literature. Pediatr Emerg Care 30(5):299–304
Rajesh A, Basu AK, Vaidhyanath R, Finlay D (2001) Hand fractures: a study of their site and type in childhood. Clin Radiol 56(8):667–669
Mahabir RC, Kazemi AR, Cannon WG, Courtemanche DJ (2001) Pediatric hand fractures: a review. Pediatr Emerg Care 17(3):153–156
Johnson CF, Kaufman KL, Callendar C (1990) The hand as a target organ in child abuse. Clin Pediatr (Phila). 29(2):66–72
McClelland CQ, Heiple KG (1982) Fractures in the first year of life. A diagnostic dilemma. Am J Dis Child 136(1):26–29
Nimkin K, Spevak MR, Kleinman PK (1997) Fractures of the hands and feet in child abuse: imaging and pathologic features. Radiology 203(1):233–236
Kleinman PK, Morris NB, Makris J, Moles RL, Kleinman PL (2013) Yield of radiographic skeletal surveys for detection of hand, foot, and spine fractures in suspected child abuse. AJR Am J Roentgenol 200(3):641–644
Karmazyn B, Lewis ME, Jennings SG, Hibbard RA, Hicks RA (2011) The prevalence of uncommon fractures on skeletal surveys performed to evaluate for suspected abuse in 930 children: should practice guidelines change? AJR Am J Roentgenol 197(1):W159–W163
Lindberg DM, Harper NS, Laskey AL, Berger RP (2013) Prevalence of abusive fractures of the hands, feet, spine, or pelvis on skeletal survey: perhaps "uncommon" is more common than suggested. Pediatr Emerg Care 29(1):26–29
Murugappan KS (2019) Pediatric femur fractures. Medscape. [25-11-2021]; Available from: https://emedicine.medscape.com/article/1246915-overview#a4
Buess E, Kaelin A (1998) One hundred pediatric femoral fractures: epidemiology, treatment attitudes, and early complications. J Pediatr Orthop Part B. 7(3):186–192
Brown D, Fisher E (2004) Femur fractures in infants and young children. Am J Public Health 94(4):558–560
Loder RT, O'Donnell PW, Feinberg JR (2006) Epidemiology and mechanisms of femur fractures in children. J Pediatr Orthop 26:561–566
Petković L, Djan I, Gajdobranski D, Marić D, Petković M (2011) Pediatric femur fractures, epidemiology and treatment. Vojnosanit Pregl 68(1):9–14
Baldwin K, Pandya NK, Wolfgruber H, Drummond DS, Hosalkar HS (2011) Femur fractures in the pediatric population: abuse or accidental trauma? Clini Orthop Relat Res 469(3):798–804
Engström Z, Wolf O, Hailer YD (2020) Epidemiology of pediatric femur fractures in children: the Swedish Fracture Register. BMC Musculoskelet Disord 21(1):796
Rokaya PK, Karki DB, Rawal M, Limbu D, Acharya BD, Bhandari PB (2020) Epidemiology of Femur fractures in children: a descriptive cross sectional study based on a rural population of Nepal. JNMA J Nepal Med Assoc 58(228):574–579
Valaikaite R, Tabard-Fougère A, Steiger C, Samara E, Dayer R, Ceroni D (2020) A retrospective epidemiological study of paediatric femoral fractures. Swiss Med Wkly 150:w20360
Beaty JH (2006) Fractures of the hip in children. Orthop Clin North Am 37(2):223–232. vii
Boardman MJ, Herman MJ, Buck B, Pizzutillo PD (2009) Hip fractures in children. J Am Acad Orthop Surg 17(3):162–173
Dial BL, Lark RK (2018) Pediatric proximal femur fractures. J Orthop 15(2):529–535
Ahn L, Andras L, Shirley E (2021) Proximal femur fractures—pediatric. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4018/proximal-femur-fractures%2D%2Dpediatric
Stone KP, White K (2021) Hip fractures in children. UpToDate. [25-11-2021]; Available from: https://www.uptodate.com/contents/hip-fractures-in-children
Bimmel R, Bakker A, Bosma B, Michielsen J (2010) Paediatric hip fractures: a systematic review of incidence, treatment options and complications. Acta Orthop Belg 76(1):7–13
Miller WE (1973) Fractures of the hip in children from birth to adolescence. Clin Orthop Relat Res 92:155–188
Pape HC, Krettek C, Friedrich A, Pohlemann T, Simon R, Tscherne H (1999) Long-term outcome in children with fractures of the proximal femur after high-energy trauma. J Trauma 46(1):58–64
Davison BL, Weinstein SL (1992) Hip fractures in children: a long-term follow-up study. J Pediatr Orthop. 12(3):355–358
Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC (1993) Types and complications of femoral neck fractures in children. Pediatr Radiol 23(6):415–420
Togrul E, Bayram H, Gulsen M, Kalaci A, Ozbarlas S (2005) Fractures of the femoral neck in children: long-term follow-up in 62 hip fractures. Injury 36(1):123–130
Shrader MW, Jacofsky DJ, Stans AA, Shaughnessy WJ, Haidukewych GJ (2007) Femoral neck fractures in pediatric patients: 30 years experience at a level 1 trauma center. Clin Orthop Relat Res 454:169–173
Currey JD, Butler G (1975) The mechanical properties of bone tissue in children. J Bone Joint Surg Am 57(6):810–814
Ratliff AH (1962) Fractures of the neck of the femur in children. J Bone Joint Surg Br 44-b:528–542
Bali K, Sudesh P, Patel S, Kumar V, Saini U, Dhillon MS (2011) Pediatric femoral neck fractures: our 10 years of experience. Clin Orthop Surg 3(4):302–308
Shrader MW, Schwab JH, Shaughnessy WJ, Jacofsky DJ (2009) Pathologic femoral neck fractures in children. Am J Orthop (Belle Mead, NJ) 38(2):83–86. discussion 6
Wojtowycz M, Starshak RJ, Sty JR (1980) Neonatal proximal femoral epiphysiolysis. Radiology 136(3):647–648
Prevot J, Lascombes P, Blanquart D, Gagneux E (1989) Labor trauma-induced epiphysiolysis of the proximal femur. 4 cases. ZKinderchir. 44(5):289–292
Towbin R, Crawford AH (1979) Neonatal traumatic proximal femoral epiphysiolysis. Pediatrics 63(3):456–459
Milgram JW, Lyne ED (1975) Epiphysiolysis of the proximal femur in very young children. Clin Orthop Relat Res 110:146–153
Michail JP, Theodorou S, Houliaras K, Siatis N (1958) Two cases of obstetrical separation (epiphysiolysis) of the upper femoral epiphysis: appearance of ossification centre of the femoral head fifteen-day-old child. J Bone Joint Surg Br Volume 40-b(3):477–482
Kennedy PC (1944) Traumatic separation of the upper femoral epiphysis. Am I Roentgenol 51:707
Lindseth RE, Rosene HA Jr (1971) Traumatic separation of the upper femoral epiphysis in a new born infant. J Bone Joint Surg Am 53(8):1641–1644
Mortens J, Christensen P (1964) Traumatic separation of the upper femoral epiphysis as an obstetric lesion. Acta Orthop Scand 34:238–250
Theodorou SD, Ierodiaconou MN, Mitsou A (1982) Obstetrical fracture-separation of the upper femoral epiphysis. Acta Orthop Scand 53(2):239–243
Kembhavi RS, James B (2015) A rare case report on bilateral intertrochanteric fractures in a child following child abuse. J Clin Diagnostic Res 9(10):Rd03-5
Pastor AJ, Gupta A, Press CM, Gourineni P (2012) Femoral neck fracture as the sentinel sign of child abuse in an infant: a case report. J Pediatr Orthop Part B. 21(6):587–591
Gholve P, Arkader A, Gaugler R, Wells L (2008) Femoral neck fracture as an atypical presentation of child abuse. Orthopedics 31(3):271
Paris N, Journeau P, Moh Ello N et al (2008) Bilateral upper femoral physis injury in a case of epilepsy in a young child [Décollement épiphysaire fémoral proximal bilatéral chez un nourrisson atteint d'épilepsie généralisée. A propos d'une observation]. Revue de chirurgie orthopedique et reparatrice de l'appareil moteur 94(4):403–406
Hayyun MF, Jamil K, Abd-Rashid AH, Ibrahim S (2021) Subcapital femoral neck tension stress fracture—a rare injury in a child: a case report. Malays Orthop J 15(1):132–134
Papadimitriou NG, Christophorides J, Papadimitriou A, Beslikas TA, Ventouris TN, Goulios BA (2007) Stress fractures in children: a review of 37 cases. Eur J Orthop Surg Traumatol Orthop Traumatol 17:131–137
Er MS, Eroglu M, Altinel L (2014) Femoral neck stress fracture in children: a case report, up-to-date review, and diagnostic algorithm. J Pediatr Orthop Part B 23(2):117–121
Lehman RA Jr, Shah SA (2004) Tension-sided femoral neck stress fracture in a skeletally immature patient. A case report. J Bone Joint Surg Am 86(6):1292–1295
Boyle MJ, Hogue GD, Heyworth BE, Ackerman K, Quinn B, Yen YM (2017) Femoral neck stress fractures in children younger than 10 years of age. J Pediatr Orthop 37(2):e96–ee9
Meaney JE, Carty H (1992) Femoral stress fractures in children. Skeletal Radiol 21(3):173–176
St Pierre P, Staheli LT, Smith JB, Green NE (1995) Femoral neck stress fractures in children and adolescents. J Pediatr Orthop 15(4):470–473
Walker RN, Green NE, Spindler KP (1996) Stress fractures in skeletally immature patients. J Pediatr Orthop 16(5):578–584
Scheerlinck T, De Boeck H (1998) Bilateral stress fractures of the femoral neck complicated by unilateral displacement in a child. J Pediatr Orthop Part B 7(3):246–248
Román M, Recio R, Moreno JC, Fuentes S, Collantes F (2001) Stress fracture of the femoral neck in a child. Case report and review of the literature. Acta Orthop Belg 67(3):286–289
Fiévez EF, Hanssen NM, Schotanus MG, van Haaren EH, Kort NP (2013) Stress fracture of the femoral neck in a child: a case report. J Pediatr Orthop Part B 22(1):45–48
Maezawa K, Nozawa M, Sugimoto M, Sano M, Shitoto K, Kurosawa H (2004) Stress fractures of the femoral neck in child with open capital femoral epiphysis. J Pediatr Orthop Part B 13(6):407–411
Lee GW, Park KS, Yoon TR, Eshnazarovich EK (2016) Bilateral femoral neck stress fracture in child: a case report. Hip Pelvis 28(3):169–172
Miller F, Wenger DR (1979) Femoral neck stress fracture in a hyperactive child. A case report. J Bone Joint Surg Am 61(3):435–437
Rinat B, Bor N, Dujovny E, Rozen N, Rubin G (2021) Pediatric femoral neck fractures after sliding in a water slide: a case report of two patients. J Orthop Case Rep 11(5):68–71
Blaiser RD, Hughes LO (2001) Fractures and traumatic dislocations of the hip in children. In: Beaty JH, Kasser JR (eds) Rockwood and Wilkins’ fractures in children, 5th edn. Lippincott, Philadelphia, pp 913–914
Gaudinez RF, Heinrich SD (1989) Transphyseal fracture of the capital femoral epiphysis. Orthopedics 12(12):1599–1602
Swischuk LE (1997) Irritable infant and left lower extremity pain. Pediatr Emerg Care 13(2):147–148
De Mattos CB, Binitie O, Dormans JP (2012) Pathological fractures in children. Bone Joint Res 1(10):272–280
Miu A (2015) Pathological fractures of the proximal femur due to solitary bone cyst: classification, methods of treatment. J Med Life 8(4):536–543
Vynichakis G, Angelis S, Chandrinos M et al (2019) Pathological hip fractures in children and adolescents due to benign tumor or tumor-like lesions. J Long Term Eff Med Implants 29(2):91–99
Swiontkowski MF, Winquist RA (1986) Displaced hip fractures in children and adolescents. J Trauma. 26(4):384–388
Ortiz EJ, Isler MH, Navia JE, Canosa R (2005) Pathologic fractures in children. Clin Orthop Relat Res 432:116–126
Morcos MW, Hamdy RC, Fassier F, Saran N (2019) Treatment of Femur neck fracture in children with osteogenesis imperfecta: two case reports. JBJS Case Connect 9(4):e0449
Rewers A, Hedegaard H, Lezotte D et al (2005) Childhood femur fractures, associated injuries, and sociodemographic risk factors: a population-based study. Pediatrics 115(5):e543-52
Kasser JR, Beaty JH (2001) Femoral shaft fractures. In: Beaty JH, Kasser JR (eds) Rockwood and Wilkins’ Fractures in children, 5th edn. Lippincott Williams and Wilkins, pp 941–980
von Heideken J, Svensson T, Blomqvist P, Haglund-Åkerlind Y, Janarv PM (2011) Incidence and trends in femur shaft fractures in Swedish children between 1987 and 2005. J Pediatr Orthop 31(5):512–519
Hinton RY, Lincoln A, Crockett MM, Sponseller P, Smith G (1999) Fractures of the femoral shaft in children. Incidence, mechanisms, and sociodemographic risk factors. J Bone Joint Surg Am 81(4):500–509
Rennie L, Court-Brown CM, Mok JY, Beattie TF (2007) The epidemiology of fractures in children. Injury 38(8):913–922
Bridgman S, Wilson R (2004) Epidemiology of femoral fractures in children in the West Midlands region of England 1991 to 2001. J Bone Joint Surg Br Volume 86(8):1152–1157
Edgington J, Shirley E, Sink E (2021) Femoral shaft fractures—pediatric. Orthobullets. [26-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4019/femoral-shaft-fractures%2D%2Dpediatric
Galano GJ, Vitale MA, Kessler MW, Hyman JE, Vitale MG (2005) The most frequent traumatic orthopaedic injuries from a national pediatric inpatient population. J Pediatr Orthop 25(1):39–44
Stone KP, White K. Femoral shaft fractures in children. UpToDate; 2021. [26-11-2021]; Available from: https://www.uptodate.com/contents/femoral-shaft-fractures-in-children.
Mooney DP, Forbes P (2004) Trends in inpatient pediatric trauma care in new England. J Trauma 57(6):1241–1245
Talbot C, Davis N, Majid I et al (2018) Fractures of the femoral shaft in children: national epidemiology and treatment trends in England following activation of major trauma networks. Bone Joint J 100-b(1):109–118
Keany JE, McKeever D (2019) Femoral shaft fractures in emergency medicine. Medscape. [26-11-2021]; Available from: https://emedicine.medscape.com/article/824856-overview
Medda S, Unger T, Halvorson J (2021) Diaphyseal Femur fracture. StatPearls. StatPearls Publishing, Treasure Island (FL)
Arioz DT, Koken GN, Koken R, Kose KC, Cevrioglu AS (2008) Isolated intrauterine femoral fracture in an otherwise normal fetus. J Obstet Gynaecol Res 34(1):92–94
Senanayake H, Anandakumar C, de Silva MV (2003) Mid-trimester fracture of femur in a normal fetus. J Obstet Gynaecol Res 29(3):186–188
Alhusen JL, Ray E, Sharps P, Bullock L (2015) Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Womens Health (Larchmt) 24(1):100–106
Christensen EE, Dietz GW (1978) A radiographically documented intra-uterine femoral fracture. Br J Radiol 51(610):830–831
Bucholz R, Mauldin D (1978) Prenatal diagnosis of intrauterine fetal fracture. A case report. J Bone Joint Surg Am 60(5):712–713
Wilkinson AD (1898) Compound intra-uterine fracture of the femur, with report of a case. JAMA XXXI(10):536
Scheier M, Peter M, Hager C, Lang T, Barvinek A, Marth C (2010) Spontaneous isolated midtrimester fracture of tibia and fibula in a normal fetus with in utero healing and good long-term outcome. Fetal Diagn Ther 28(1):58–60
Yu M, Xu D, Zhang A, Shen J (2018) Spontaneous fetal femoral fracture: a case report and literature review. J Int Med Res 46(3):1282–1287
Raabe E, Dammer U, Kehl S, Beckmann MW, Faschingbauer F. Spontaneous fetal femur fracture. Ultraschall in der Medizin (Stuttgart, Germany : 1980). 2013;34 - KS_CS6_04.
Alonso JA, Wright DM, Sochart DH (2005) Intrauterine femoral fracture diagnosed at birth—maternal abdominal trauma versus non-accidental injury. Injury Extra 36:432–433
Morris S, Cassidy N, Stephens M, McCormack D, McManus F (2002) Birth-associated femoral fractures: incidence and outcome. J Pediatr Orthop 22(1):27–30
Toker A, Perry ZH, Cohen E, Krymko H (2009) Cesarean section and the risk of fractured femur. Isr Med Assoc J 11(7):416–418
Kancherla R, Sankineani SR, Naranje S et al (2012) Birth-related femoral fracture in newborns: risk factors and management. J Child Orthop 6(3):177–180
Frik S (2016) Management of birth-associated subtrochanteric femur fractures. Acta Orthop Belg 82(4):850–853
Cebesoy FB, Cebesoy O, Incebiyik A (2009) Bilateral femur fracture in a newborn: an extreme complication of cesarean delivery. Arch Gynecol Obstet 279(1):73–74
Rubin A (1964) Birth injuries: Incidence, mechanisms and end results. Obstet Gynecol 23:218–221
Barnes AD, Van Geem TA (1985) Fractured femur of the newborn at cesarean section. A case report. J Reprod Med 30(3):203–205
Kanai Y, Honda Y, Honda T, Sanpei M (2018) Delayed birth-related Femur fracture after cesarean section: a case report. AJP Rep 8(3):e158–ee60
Cumming WA (1979) Neonatal skeletal fractures. Birth trauma or child abuse? J Can Assoc Radiol 30(1):30–33
Hosokawa T, Yamada Y, Sato Y, Tanami Y, Oguma E (2017) Subperiosteal new bone and callus formations in neonates with femoral shaft fracture at birth. Emerg Radiol 24(2):143–148
Crompton S, Messina F, Klafkowski G, Hall C, Offiah AC (2021) Validating scoring systems for fracture healing in infants and young children: pilot study. Pediatr Radiol
Scherl SA, Miller L, Lively N, Russinoff S, Sullivan CM, Tornetta P 3rd. (2000) Accidental and nonaccidental femur fractures in children. Clin Orthop Relat Res 376:96–105
Blakemore LC, Loder RT, Hensinger RN (1996) Role of intentional abuse in children 1 to 5 years old with isolated femoral shaft fractures. J Pediatr Orthop. 16(5):585–588
Schwend RM, Werth C, Johnston A (2000) Femur shaft fractures in toddlers and young children: rarely from child abuse. J Pediatr Orthop 20(4):475–481
Hui C, Joughin E, Goldstein S et al (2008) Femoral fractures in children younger than three years: the role of nonaccidental injury. J Pediatr Orthop 28(3):297–302
John R, Sharma S, Raj GN et al (2017) Current concepts in paediatric femoral shaft fractures. Open Orthop J 11:353–368
Hedlund R, Lindgren U (1986) The incidence of femoral shaft fractures in children and adolescents. J Pediatr Orthop 6(1):47–50
Daly KE, Calvert PT (1991) Accidental femoral fracture in infants. Injury 22(4):337–338
Loder RT (1987) Pediatric polytrauma: orthopaedic care and hospital course. J Orthop Trauma 1(1):48–54
Shrader MW, Bernat NM, Segal LS (2011) Suspected nonaccidental trauma and femoral shaft fractures in children. Orthopedics 34(5):360
Mughal MA, Dix-Peek SI, Hoffman EB (2013) The epidemiology of femur shaft fractures in children. SA Orthop J 12(4):23–27
Cornell EM, Powell EC (2018) Skeletal survey yield in young children with Femur fractures. J Emerg Med 55(6):758–763
Ali M, Padhye K, Gauthier L (2021) Pediatric femoral shaft fractures secondary to tombstone uprooting—Two case reports. Trauma Case Rep 32:100416
Hobbs CJ, Wynne JM (1990) The sexually abused battered child. Arch Dis Child 65(4):423–427
Johnson K, Chapman S, Hall CM (2004) Skeletal injuries associated with sexual abuse. Pediatr Radiol 34(8):620–623
Kleinman PK (1998) The lower extremity. In: Kleinman PK (ed) Diagnostic imaging of child abuse. Mosby, pp 26–71
Frasier LD (2003) Child abuse or mimic. Consult Pediatr 2:212–215
Beals RK, Tufts E (1983) Fractured femur in infancy: the role of child abuse. J Pediatr Orthop 3(5):583–586
Loos MHJ, Allema WM, Bakx R, Stoel RD, van Rijn RR, Karst WA (2021) Paediatric femur fractures-the value of contextual information on judgement in possible child abuse cases: are we bias? Eur J Pediatr 180(1):81–90
Mboutol-Mandavo C, N'Dour O, Ouedraogo SF, Missengue-Bosseba R, Ndiaye D, Ngom G (2016) Fractures du nouveau-né et du nourrisson secondaires au massage traditionnel [Newborn and infant fractures secondary to traditional massage]. Arch Pediatr: organe officiel de la Societe francaise de pediatrie 23(9):963–965
Siddiqui SA, Singh MV, Shrivastava A, Maurya M, Gaur VK, Kumar D (2020) Femoral shaft fracture following oil massage in neonates: a single-centre experience. Trop Doct 50(4):387–389
Greeley CS, Donaruma-Kwoh M, Vettimattam M, Lobo C, Williard C, Mazur L (2013) Fractures at diagnosis in infants and children with osteogenesis imperfecta. J Pediatr Orthop 33(1):32–36
Fry K, Hoffer MM, Brink J (1976) Femoral shaft fractures in brain-injured children. J Trauma 16(5):371–373
Torwalt CR, Balachandra AT, Youngson C, de Nanassy J (2002) Spontaneous fractures in the differential diagnosis of fractures in children. J Forensic Sci 47(6):1340–1344
Katz JF (1953) Spontaneous fractures in paraplegic children. J Bone Joint Surg Am 35-a(1):220–226
Ju DG, Mogayzel PJ Jr, Sponseller PD, Familiari F, McFarland EG (2016) Bilateral midshaft femoral fractures in an adolescent baseball player. J Cyst Fibros 15(4):e41–e43
Prince HG, Clay NR (1988) A pathological fracture of the femur through a histiocytic granuloma. Injury 19(2):124–125
Chaib B, Malhotra K, Khoo M, Saifuddin A (2021) Pathological fracture in paediatric bone tumours and tumour-like lesions: A predictor of benign lesions? Br J Radiol 94(1125):20201341
Cherix S, Bildé Y, Becce F, Letovanec I, Rüdiger HA (2014) Multiple non-ossifying fibromas as a cause of pathological femoral fracture in Jaffe-Campanacci syndrome. BMC Musculoskelet Disord 15:218
Srivastava A, Aggarwal AN, Mishra P, Bhateja D (2016) Femoral fracture acting as an "ominous masquerade" in a 7-year-old child. J Clin Orthop Trauma 7(Suppl 1):27–29
Pandey PK, Pawar I, Gupta J (2016) Physeal separation and complete resorption of femoral head associated with chronic osteomyelitis of femoral diaphysis in a young child: rare case report. J Pediatr Orthop Part B 25(6):529–532
Akinyoola AL, Orimolade EA, Yusuf MB (2008) Pathologic fractures of long bones in Nigerian children. J Child Orthop 2(6):475–479
Eid AM, Hafez MA (2002) Traumatic injuries of the distal femoral physis. Retrospective study on 151 cases. Injury 33(3):251–255
Arkader A, Warner WC Jr, Horn BD, Shaw RN, Wells L (2007) Predicting the outcome of physeal fractures of the distal femur. J Pediatr Orthop 27(6):703–708
Duffy S, Gelfer Y, Trompeter A, Clarke A, Monsell F (2021) The clinical features, management options and complications of paediatric femoral fractures. Eur J Orthop Surg Traumatol Orthop Traumatol 31(5):883–892
Bellamy JT, Ward LA, Fletcher ND (2021) Evaluation of pediatric distal femoral physeal fractures and the factors impacting poor outcome requiring further corrective surgery. J Pediatr Orthop Part B 30(1):6–12
Stone KP, White K. Distal femoral fractures in children. UpToDate; 2021 [26-11-2021]; Available from: https://www.uptodate.com/contents/distal-femoral-fractures-in-children.
Smith NC, Parker D, McNicol D (2001) Supracondylar fractures of the femur in children. J Pediatr Orthop 21(5):600–603
Fox S. Distal femoral physeal fractures. Don't Forget the Bubbles; 2021 [26-11-2021]; Available from: https://dontforgetthebubbles.com/distal-femoral-physeal-fractures/.
Neal K (2021) Distal Femur Fractures. POSNA. [26-11-2021]; Available from: https://posna.org/Physician-Education/Study-Guide/Distal-Femur-Fractures
Shaath K, Shirley E, Skaggs DL (2021) Distal femoral physeal fractures—pediatric. Orthobullets. [26-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4020/distal-femoral-physeal-fractures%2D%2Dpediatric
Pritchett JW (1992) Longitudinal growth and growth-plate activity in the lower extremity. Clinical Orthop Relat Res 275:274–279
Leavitt PH (1951) Traumatic separation of the lower-femoral epiphysis. N Engl J Med 245:565–566
El-Zawawy HB, Silva MJ, Sandell LJ, Wright RW (2005) Ligamentous versus physeal failure in murine medial collateral ligament biomechanical testing. J Biomech 38(4):703–706
Price CT (2021) Extra-articular injuries of the knee. TeachMeOrthopedics. [26-11-2021]; Available from: https://teachmeorthopedics.info/extra-articular-injuries-of-the-knee/
Ozturk M, Yurtbay A, Keskin D, Polat AV, Selcuk MB (2019) Subperiosteal hemorrhage due to a distal femoral physeal fracture in a neonate. North Clin Istanb 6(3):312–314
Jain R, Bielski RJ (2001) Fracture of lower femoral epiphysis in an infant at birth: a rare obstetrical injury. J Perinatol 21(8):550–552
Rutherford Y, Fomufod AK, Gopalakrishnan LJ, Beeks EC (1983) Traumatic distal femoral periostitis of the newborn: a breech delivery birth injury. J Natl Med Assoc 75(10):933–935
Clarke TA, Edwards DK, Merritt A, Young LW (1982) Radiological case of the month. Neonatal fracture of the femur: iatrogenic? Am J Dis Child 136(1):69–70
Mangurten HH, Puppala B, Knuth A (2005) Neonatal distal femoral physeal fracture requiring closed reduction and pinning. J Perinatol 25(3):216–219
Trier H (1992) Epiphysiolysis in the distal femur as a birth injury in Cesarean section [Epifysiolyse i distale femur som fødselslaesion ved sectio]. UgeskrLaeger 154(22):1574–1575
Alexander J, Gregg JE, Quinn MW (1987) Femoral fractures at caesarean section. Case reports. Br J Obstet Gynaecol 94(3):273
McCollough FL, McCarthy RE (1988) Bilateral distal femoral epiphyseal fractures following home delivery: a case report. J Ark Med Soc 84(9):364–366
Haney SB, Boos SC, Kutz TJ, Starling SP (2009) Transverse fracture of the distal femoral metadiaphysis: a plausible accidental mechanism. Pediatr Emerg Care 25(12):841–844
Rex C, Kay PR (2000) Features of femoral fractures in nonaccidental injury. J Pediatr Orthop 20(3):411–413
Arkader A, Friedman JE, Warner WC Jr, Wells L (2007) Complete distal femoral metaphyseal fractures: a harbinger of child abuse before walking age. J Pediatr Orthop 27(7):751–753
Grant P, Mata MB, Tidwell M (2001) Femur fracture in infants: a possible accidental etiology. Pediatrics 108(4):1009–1011
Pickett WJ 3rd, Johnson JF, Enzenauer RW (1982) Case report 192. Neonatal fractures mimicking abuse secondary to physical therapy. Skeletal Radiol 8(1):85–86
Aroojis AJ, Gajjar SM, Johari AN (2007) Epiphyseal separations in spastic cerebral palsy. J Pediatr Orthop Part B 16(3):170–174
Aroojis AJ, Johari AN (2000) Epiphyseal separations after neonatal osteomyelitis and septic arthritis. J Pediatr Orthop 20(4):544–549
Parsch K (1991) Origin and treatment of fractures in spina bifida. Eur J Pediatr Surg 1(5):298–305
Vander Have KL, Ganley TJ, Kocher MS, Price CT, Herrera-Soto JA (2010) Arthrofibrosis after surgical fixation of tibial eminence fractures in children and adolescents. Am J Sports Med 38(2):298–301
Cheng JC, Ng BK, Ying SY, Lam PK (1999) A 10-year study of the changes in the pattern and treatment of 6,493 fractures. J Pediatr Orthop 19(3):344–350
Chapman J, Cohen J. Tibial and fibular fractures in children. UpToDate; 2020 [26-11-2021]; Available from: https://www.uptodate.com/contents/tibial-and-fibular-shaft-fractures-in-children.
Mashru RP, Herman MJ, Pizzutillo PD (2005) Tibial shaft fractures in children and adolescents. J Am Acad Orthop Surg 13(5):345–352
Shannak AO (1988) Tibial fractures in children: follow-up study. J Pediatr Orthop 8(3):306–310
Weber B, Kalbitz M, Baur M, Braun CK, Zwingmann J, Pressmar J (2021) Lower leg fractures in children and adolescents-comparison of conservative vs ECMES treatment. Front Pediatr 9:597870
Cruz AI Jr, Raducha JE, Swarup I, Schachne JM, Fabricant PD (2019) Evidence-based update on the surgical treatment of pediatric tibial shaft fractures. Curr Opin Pediatr 31(1):92–102
Sarmiento A, Gersten LM, Sobol PA, Shankwiler JA, Vangsness CT (1989) Tibial shaft fractures treated with functional braces. Experience with 780 fractures. J Bone Joint Surg Br Volume 71(4):602–609
Audigé L, Slongo T, Lutz N, Blumenthal A, Joeris A (2017) The AO pediatric comprehensive classification of long bone fractures (PCCF). Acta Orthop 88(2):133–139
Kaplan M, Dollberg M, Wajntraub G, Itzchaki M (1987) Fractured long bones in a term infant delivered by cesarian section. Pediatr Radiol 17(3):256–257
Dolivet E, Delesalle C, Morello R et al (2018) A case-control study about foetal trauma during caesarean delivery. J Gynecol Obstet Hum Reprod 47(7):325–329
Mileto C, Hashem J, Culbertson MD, Sadeghpour R, Tucci J (2014) Proximal tibial epiphyseal fracture in a newborn following cesarean section: a case report. JBJS Case Connect 4(3):e84
Moineau G, Plint A (2005) Tibial fractures possibly linked to use of a baby stationary activity center. Pediatr Emerg Care 21(3):181–183
Paddock M, Horton D, Offiah AC (2020) Bilateral fibular fractures in a pre-ambulant infant. Pediatr Radiol
Mellick LB, Milker L, Egsieker E (1999) Childhood accidental spiral tibial (CAST) fractures. Pediatr Emerg Care 15(5):307–309
Mellick LB, Reesor K (1990) Spiral tibial fractures of children: a commonly accidental spiral long bone fracture. Am J Emerg Med 8(3):234–237
Tenenbein M, Reed MH, Black GB (1990) The toddler's fracture revisited. Am J Emerg Med 8(3):208–211
Sarmah A (1995) 'Toddler's fracture'? A recognised entity. Arch Dis Child 72(4):376
D'Souza LG, Hynes DE, McManus F, O'Brien TM, Stephens MM, Waide V (1996) The bicycle spoke injury: an avoidable accident? Foot Ankle Int 17(3):170–173
Roffman M, Moshel M, Mendes DG (1980) Bicycle spoke injuries. J Trauma 20(4):325–326
Slaar A, Karsten IH, Beenen LF et al (2015) Plain radiography in children with spoke wheel injury: A retrospective cohort study. Eur J Radiol 84(11):2296–2300
Mellick LB, Reesor K, Demers D, Reinker KA (1988) Tibial fractures of young children. Pediatr Emerg Care 4(2):97–101
Banaszkiewicz PA, Scotland TR, Myerscough EJ (2002) Fractures in children younger than age 1 year: importance of collaboration with child protection services. J Pediatr Orthop 22(6):740–744
Coffey C, Haley K, Hayes J, Groner JI (2005) The risk of child abuse in infants and toddlers with lower extremity injuries. J Pediatr Surg 40(1):120–123
Eren MB, Bilgiç E, Çetin S, Deresoy FA, Öztürk T, Balta O (2021) Sixteen fractures in a seven-month-old child caused by nonaccidental trauma. Case Rep Orthop Res:185–191
Patel NK, Horstman J, Kuester V, Sambandam S, Mounasamy V (2018) Pediatric tibial shaft fractures. Indian J Orthop 52(5):522–528
Taitz J, Moran K, O'Meara M (2004) Long bone fractures in children under 3 years of age: is abuse being missed in Emergency Department presentations? J Paediatr Child Health 40(4):170–174
Clarke NM, Shelton FR, Taylor CC, Khan T, Needhirajan S (2012) The incidence of fractures in children under the age of 24 months—in relation to non-accidental injury. Injury 43(6):762–765
Petnehazy T, Schalamon J, Hartwig C et al (2015) Fractures of the hallux in children. Foot Ankle Int 36(1):60–63
Kay RM, Tang CW (2001) Pediatric foot fractures: evaluation and treatment. J Am Acad Orthop Surg 9(5):308–319
Rammelt S, Godoy-Santos AL, Schneiders W, Fitze G, Zwipp H (2016) Foot and ankle fractures during childhood: review of the literature and scientific evidence for appropriate treatment. Revista brasileira de ortopedia. 51(6):630–639
Singer G, Cichocki M, Schalamon J, Eberl R, Höllwarth ME (2008) A study of metatarsal fractures in children. J Bone Joint Surg Am 90(4):772–776
Ribbans WJ, Natarajan R, Alavala S (2005) Pediatric foot fractures. Clin Orthop Relat Res 432:107–115
Mäyränpää MK, Mäkitie O, Kallio PE (2010) Decreasing incidence and changing pattern of childhood fractures: A population-based study. J Bone Miner Res 25(12):2752–2759
Owen RJ, Hickey FG, Finlay DB (1995) A study of metatarsal fractures in children. Injury 26(8):537–538
Cooper C, Dennison EM, Leufkens HG, Bishop N, van Staa TP (2004) Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res 19(12):1976–1981
Rosendahl K, Myklebust R, Ulriksen KF et al (2021) Incidence, pattern and mechanisms of injuries and fractures in children under two years of age. BMC Musculoskelet Disord 22(1):555
Jaffe AC, Lasser DH (1977) Multiple metatarsal fractures in child abuse. Pediatrics 60(4 Pt 2):642–643
Herrera-Soto JA, Crawford AH, Loveless EA (2005) Ossifying subperiosteal hematoma associated with neurofibromatosis type 1. Diagnostic hesitation: a case report and literature review. J Pediatr Orthop Part B 14(1):51–54
Steenbrugge F, Verstraete K, Poffyn B, Uyttendaele D, Verdonk R (2001) Recurrent massive subperiosteal hematoma in a patient with neurofibromatosis. Eur Radiol 11(3):480–483
Lavell A, Jones CW, Wong D, Counsel P, Carey-Smith R (2017) Plexiform neurofibroma causing an ossifying subperiosteal haematoma: a rare case in the tibia of an 11-year-old girl. Skeletal Radiol 46(10):1405–1413
Blitman NM, Levsky JM, Villanueva-Siles E, Thornhill BA (2007) Spontaneous hemorrhage simulating rapid growth of a benign subperiosteal plexiform neurofibroma. Pediatr Radiol 37(9):925–928
Kenan S, Abdelwahab IF, Klein MJ, Hermann G, Lewis MM (1993) Lesions of juxtacortical origin (surface lesions of bone). Skeletal Radiol 22(5):337–357
Islam O, Soboleski D, Symons S, Davidson LK, Ashworth MA, Babyn P (2000) Development and duration of radiographic signs of bone healing in children. AJR Am J Roentgenol 175(1):75–78
Prosser I, Lawson Z, Evans A et al (2012) A timetable for the radiologic features of fracture healing in young children. AJR Am J Roentgenol 198(5):1014–1020
Prosser I, Maguire S, Harrison SK, Mann M, Sibert JR, Kemp AM (2005) How old is this fracture? Radiologic dating of fractures in children: a systematic review. AJR Am J Roentgenol 184(4):1282–1286
Warner C, Maguire S, Trefan L, Miller A, Weinman J, Fadell M (2017) A study of radiological features of healing in long bone fractures among infants less than a year. Skeletal Radiol 46(3):333–341
Rana RS, Wu JS, Eisenberg RL (2009) Periosteal reaction. AJR Am J Roentgenol 193(4):W259–W272
Ved N, Haller JO (2002) Periosteal reaction with normal-appearing underlying bone: a child abuse mimicker. Emerg Radiol 9(5):278–282
Kwon DS, Spevak MR, Fletcher K, Kleinman PK (2002) Physiologic subperiosteal new bone formation: prevalence, distribution, and thickness in neonates and infants. AJR Am J Roentgenol 179(4):985–988
Herring W. Growth arrest lines. Learning Radiology. Recognizing the basics; 2020 [27-11-2021]; Available from: http://learningradiology.com/archives2008/COW%20334-Growth%20arrest%20lines/growtharrestcorrect.htm.
Bell DJ, Morgan MA (2021) Growth arrest lines. Radiopaedia. [27-11-2021]; Available from: https://radiopaedia.org/articles/growth-arrest-lines
Harris HA (1926) The growth of the long bones in childhood with special reference to certain bony striations of the metaphysis and the role of vitamins. Arch Intern Med 38:785–793
Harris HA (1927) Cessation of growth in long bones in health and disease. Mayo Clin Proc 2:228–229
Park EA (1964) The imprinting of nutrional disturbances on the growing bone. Pediatrics 33(Suppl):815–862
Kennedy JW, Irwin GJ, Huntley JS (2014) Growth arrest lines and intra-epiphyseal silhouettes: a case series. BMC Res Notes 7:27
Boyages SC, Halpern JP, Maberly GF et al (1988) A comparative study of neurological and myxedematous endemic cretinism in western China. J Clin Endocrinol Metab 67(6):1262–1271
Rosen RA, Deshmukh SM (1985) Growth arrest recovery lines in hypoparathyroidism. Radiology 155(1):61–62
Bessler W (1982) Vertebral growth arrest lines after Cushing's syndrome. A case report. Diagn Imaging 51(6):311–315
Fiszman P, Ansell BM, Renton P (1981) Radiological assessment of knees in juvenile chronic arthritis (juvenile rheumatoid arthritis). Scand J Rheumatol 10(2):145–152
Schwartz AM, Leonidas JC (1984) Methotrexate osteopathy. Skeletal Radiol 11(1):13–16
Meister B, Gassner I, Streif W, Dengg K, Fink FM (1994) Methotrexate osteopathy in infants with tumors of the central nervous system. Med Pediatr Oncol 23(6):493–496
Bar-On E, Beckwith JB, Odom LF, Eilert RE (1993) Effect of chemotherapy on human growth plate. J Pediatr Orthop 13(2):220–224
Etxebarria-Foronda I, Gorostiola-Vidaurrazaga L (2013) Zebra lines: Radiological repercussions of the action of bisphosphonates on the immature skeleton. Rev Osteoporos Metab Miner 5(1):39–41
Silverman FN (1994) Variants due to diseases of bone. In: Silverman FN, Kuhn JP (eds) Caffey’s pediatric x-ray diagnosis: an integrated imaging approach, 9th edn. Mosby, pp 1521–1527
Patton RG, Gardner LI (1967) Growth failure in maternal deprivation. Charles C Thomas, Springfield, USA
Patton RG, Gardner LI (1962) Influence of family environment on growth: the syndrome of ‘maternal deprivation’. Pediatrics 30(6):957–962
Khadilkar VV, Frazer FL, Skuse DH, Stanhope R (1998) Metaphyseal growth arrest lines in psychosocial short stature. Arch Dis Child 79(3):260–262
Zapala MA, Tsai A, Kleinman PK (2016) Growth recovery lines are more common in infants at high vs. low risk for abuse. Pediatr Radiol 46(9):1275–1281
Spiller LR, Kellogg ND, Mercado-Deane MG, Zarka AI, Gelfond JAL (2020) Growth recovery lines: a specific indicator of child abuse and neglect? Pediatr Radiol 50(2):207–215
Obdeijn MC, van der Vlies CH, van Rijn RR (2010) Capitate and hamate fracture in a child: the value of MRI imaging. Emerg Radiol 17(2):157–159
UpToDate. Ossification centers of the elbow. UpToDate; 2021 [16-12-2021]; Available from: https://www.uptodate.com/contents/image?imageKey=EM%2F73226&topicKey=EM%2F6537&source=see_link.
Shahareh B (2021) Radius and ulnar shaft fractures. Orthobullets. [25-11-2021]; Available from: https://www.orthobullets.com/trauma/1025/radius-and-ulnar-shaft-fractures
Kanat Pektaş M, Koyuncu H, Kundak AA (2019) Long bone fractures in neonatal intensive care units of Afyonkarahisar: Five-year's experience. Turk J Obstet Gynecol. 16(4):219–223
Gogi N, Deriu L (2017) Common paediatric lower limb injuries. Surgery (Oxford) 35(1):27–32
Norvell JG (2017) Tibia and Fibula fracture in the ED. Medscape. [26-11-2021]; Available from: https://emedicine.medscape.com/article/826304
Macknet D, Yen Y, Joughin E (2021) Tibial eminence fracture. Orthobullets. [26-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4022/tibial-eminence-fracture
Fares A (2021) Tibial plafond fractures. Orthobullets. [26-11-2021]; Available from: https://www.orthobullets.com/trauma/1046/tibial-plafond-fractures
Macknet D, Swarup I, Sink E (2021) Proximal Tibia metaphyseal fractures—pediatric. Orthobullets. [26-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4025/proximal-tibia-metaphyseal-fractures%2D%2Dpediatric
Edgington J, Swarup I, Vitale M (2021) Tibial shaft fractures—pediatric. Orthobullets. [26-11-2021]; Available from: https://www.orthobullets.com/pediatrics/4026/tibial-shaft-fractures%2D%2Dpediatric
Polyzois VD, Vasiliadis E, Zgonis T, Ayazi A, Gkiokas A, Beris AE (2006) Pediatric fractures of the foot and ankle. Clin Podiatr Med Surg 23(2):241–255. v
Chaturvedi A, Mann L, Cain U, Chaturvedi A, Klionsky NB (2020) Acute fractures and dislocations of the ankle and foot in children. Radiographics 40(3):754–774
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Bilo, R.A.C., de Vries, S., Nagtegaal, M., Robben, S.G.F., van Rijn, R.R. (2023). Extremities. In: Bilo, R.A., Robben, S.G.F., van Rijn, R.R. (eds) Forensic Aspects of Paediatric Fractures. Springer, Cham. https://doi.org/10.1007/978-3-031-12041-1_12
Download citation
DOI: https://doi.org/10.1007/978-3-031-12041-1_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-12040-4
Online ISBN: 978-3-031-12041-1
eBook Packages: MedicineMedicine (R0)