
Abstract
For individuals with mental illnesses, contact with the criminal justice system often begins a cycle of arrest, incarceration, release, supervision, and rearrest that poses recovery challenges. Jail and prison environments may worsen many symptoms and outcomes. This chapter focuses on integrations between components of mental health and criminal justice systems in an effort to reduce the prevalence of persons with mental illnesses behind bars and under supervision. It focuses on the factors that increase risk of incarceration for persons with mental illnesses and the role of community psychiatry providers in mediating that risk by participating in comprehensive care coordination.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
I am dismayed to be “forced to authorize the confinement of persons with mental illness in the Williamsburg jail, against both my conscience and the law” because of lack of appropriate services. (Deutsch 1937)
Introduction and Background
Through mass incarceration, the United States has a higher number and rate of people incarcerated than anywhere else in the world. At their bloated peaks, 4.7 million people were on probation in 2008; in 2018, there were upwards of 875,000 people on parole; in 2010, there were more than 2.3 million people behind bars (Barboriak 2017). Persons with mental illnesses are vastly overrepresented in the criminal justice system (Wilson et al. 2020). Estimates vary by definitions, time, and mode of inquiry. Researchers have documented mental health problems in upwards half of inmates in federal and state prisons as well as in local jails – the highest proportion being 73% of women in state prisons (James and Glaze 2006). Serious mental illness has been reported in 14.5% of male jail inmates and 31% of female jail inmates in Maryland and New York (Steadman et al. 2009), which are approximately three to six times the rates found in the general population (Pratt et al. 2006). Schizophrenia, bipolar disorder, and major depressive disorder are themselves two to three times more prevalent in jails than the community (Dvoskin et al. 2003). Conservative estimates indicate that 10–15% of people would benefit from treatment of a primary mental health problem and that 7–9% of persons on probation or parole have serious mental illness (Pinals 2017). The presence of so many people with mental illnesses in criminal justice settings represents an enormous burden on correctional and behavioral health systems of care, communities, families, and those with mental illnesses. There are many factors that contribute to this problem, and understanding these factors is crucial to providing relief throughout the system.
The majority of individuals with mental illnesses who wind up in jails have committed nonviolent misdemeanors (Ventura et al. 1998). The crimes of persons with mental health problems are often related to undertreatment (Allison et al. 2017), which is the basis of the concept of criminalization of mental illness. Nonetheless, even adequate treatment would not significantly prevent crime, and it is also important to be mindful that people with mental illnesses will commit crimes for which legal remedies are appropriate (Draine et al. 2010; JLI 2010). Safety must remain emphasized. Persons with mental illnesses who commit crimes can be held responsible for their actions while relevant effects of illness on their behavior are simultaneously taken into account. In fact, appropriate intervention for persons with mental illness also seeks to reduce characteristics of criminality, as will be later discussed.
For individuals with mental illnesses, contact with the criminal justice system often begins a cycle of arrest, incarceration, release, supervision, and rearrest that can pose nearly insurmountable challenges to recover. However, jail and prison environments are not the best setting for individuals with mental illnesses and in fact may worsen many symptoms and outcomes (Anestis and Carbonell 2014). This chapter focuses on integrations between components of mental health and criminal justice systems in an effort to reduce the prevalence of persons with mental illnesses behind bars and under supervision. The following pages focus on the factors that increase the risk of incarceration for persons with mental illnesses and the role of community psychiatry providers in mediating that risk by participating in comprehensive care coordination.
The incarceration of high numbers of persons with mental illnesses has been taking place in the context of expanding incarcerated populations in general. Until 2008, the nation’s prison and jail population continued to skyrocket to an all-time high of over two million people incarcerated and over five million under some form of correctional supervision (Kaeble et al. 2016). Around that time, the United States reached the dubious landmark of having over 1 in every 100 adults in the nation behind bars (Rich et al. 2011). Beyond the considerable human cost, correctional spending is also important to recognize. Although the correctional population decreased between 2007 and 2016 (Kaeble and Cowhig 2018), state spending on corrections accounted for 2.9% of expenditures in 2020, amounting to $65.9 billion – an increase of $20 billion annually since the first edition of this chapter was published (2012). Continued reduction of the number of persons with mental illnesses under correctional supervision should be a shared goal for behavioral health and criminal justice systems, as well as anyone who cares about human dignity.
Involvement in the criminal justice system should be a public health opportunity rather than the setback it often becomes. Jails and prisons are obligated to provide general and mental health care (Cohen 2008); in fact, incarcerated individuals are the only US citizens with constitutionally protected access to health care. The US Supreme Court, in Estelle v. Gamble [429 U.S. 97 (1976)], found that deliberate indifference to prisoners with “serious medical needs” constitutes a violation of the 8th Amendment of the Constitution and is thus cruel and unusual punishment. In Estelle v. Ruiz [503 F.Supp. 1265 (S.D. Tex. 1980)] and subsequent cases, “serious medical needs” were extended to include mental illness by the Fifth Circuit. The American Psychiatric Association (Weinstein et al. 2000), the National Commission on Correctional Health Care (Care 2008), and the National Institute of Correction (Hills et al. 2004) have all recommended that all jails provide the following, at a minimum: (a) mental health screening, referral, and evaluation, (b) crisis intervention and short-term treatment (most often medication), and (c) discharge and prerelease planning.
There have been concerted efforts by criminal justice systems to identify persons with mental illnesses at the earliest possible moments and to develop mechanisms to leverage legal authority to improve their connection to treatment. Innovative police-based responses, specialty courts, and jail, prison, and community corrections programs have been developed for persons with psychiatric problems. The shared goal for all systems is to reduce the frequency of contacts and absolute numbers of justice-involved persons with mental illnesses in criminal justice settings. At the heart of this approach lies the continuity of effective mental health care in the community and in corrections.
Why Are There So Many People with Mental Illnesses in Jail and Prison?
To develop appropriate interventions, it is important to understand the various factors that contribute the presence of persons with mental illness behind bars. A public misconception is that people who struggle with mental illness are inherently violent (Rozel and Mulvey 2017). Most crime is instead related to socioeconomic circumstances intersecting with demographics (Stuart 2003). For example, due to social determinants and structural factors including institutional racism, young, poor, Black men are much more likely to be incarcerated than other populations (Massoglia and Remster 2019). By disrupting these communities and families with incarceration, they are often pushed further into poverty, increasing odds of future arrest in a multigenerational manner.
It is critical to acknowledge that most people with mental illnesses are not violent, and most people who commit violent crimes do not have mental illnesses. Only about 4% of criminal violence can be linked to individuals with mental health problems (Rozel and Mulvey 2017). People with mental illnesses who are in fact violent often have untreated symptoms of psychosis and/or co-occurring substance use disorders, with stimulant abuse being particularly problematic (Miles et al. 2003). Furthermore, people with mental illness are three times more likely to be the victims of crime than perpetrators (Rozel and Mulvey 2017), and those with serious mental illness (SMI) are 11 times more likely to be victims of crime than the general population (Teplin et al. 2005). Nonetheless, while hard to predict and relatively infrequent, psychiatric symptoms do at times contribute to the commission of criminal offenses (Skeem et al. 2014). The risk of violence by persons with mental illness increases with being a previous victim or perpetrator of crime, lack of treatment, poverty, and unstable housing, as well as substance use, which is discussed below (Swanson et al. 2015).
There is an established link between substance abuse and crime, including violence (Rozel and Mulvey 2017). As a consequence of the failed War on Drugs, rates of substance use disorders are overrepresented in correctional settings – rates in the community are around 9% and prisons around 50% (including 20% with a history of injection drug use) – and affect nearly two-thirds of persons in jail (Peters et al. 2015; Rich et al. 2011). As the number of people incarcerated in the United States quadrupled between 1982 and 2007 (Swanson et al. 2013), drug-related arrests also tripled – nearly half of which were for marijuana (Mauer and King 2007). In general, people with substance use disorders also have a mental health diagnosis around 40–50% of the time (Kessler 2004). So it stands that incarcerating people with substance use problems will also lead to imprisonment of those with other psychiatric difficulties.
There are layered interrelationships between mental health problems, poverty, substance abuse, trauma, housing instability, and arrest (Osher 2013; Swanson et al. 2015). Being homeless and some symptoms of serious mental illness each make a person visible in the community and frequently result in calls to law enforcement; they can also make treatment engagement difficult. Recent homelessness is very common among incarcerated people; in fact, it is 7.5–11.3 times more common than in the general population (Greenberg and Rosenheck 2008). In addition, incarcerated persons with mental illness are more likely to have been homeless at the time of their arrest than those without mental illness. In jails, 30.3% of inmates with mental illness were homeless in the year prior to arrest compared to 17.3% of other inmates (Stephan 2001). This relationship has been tied to the closure of state hospitals beginning in the 1970s, leaving people without structured housing and treatment. The same population then ended up incarcerated through a process called trans-institutionalization (Lamb and Weinberger 2017). On the other hand, not having a stable place to live severely complicates the reentry of a person with mental illness following release from prison. In fact, a detailed home plan is required for supervised release through parole, and absence of an adequate residence can effectively lengthen time behind bars.
A third factor that contributes to the incarceration of people with mental illness is harsh correctional conditions that can have harmful effects on a person’s mental health. Compounding past histories of extensive trauma, the overcrowding, witnessed violence, and sexual and violent victimization behind bars often make the experience of incarceration a prolonged distressing event (Sindicich et al. 2014). The deleterious effects of these circumstances on persons with serious mental illnesses are predictable: despair, worsened symptoms, and acting out. There is also an association between experiencing trauma and having a mental illness in this population (Karlsson and Zielinski 2020).
Most – but not all – studies find that people with mental illness tend to be incarcerated for longer periods of time and are less likely to be placed on probation or parole than others charged with similar offenses (Leifman and Coffey 2020). Inmates who have psychotic illnesses are often profoundly impacted by these timelines. Parole board members may lack knowledge about community resources for individuals with mental illnesses, have misconceptions about their risk, or fear negative public reactions; prisoners with MI are also more likely to forgo parole and “max out” their sentences (Matejkowski and Ostermann 2020). As a result, people with mental illness have their releases delayed and more frequently serve the maximum sentence allowed by law (2002). The trend also worsens overcrowding, destabilizes the milieu, and increases the potential for violence overall (Houser and Welsh 2014).
Fifth, once released, former incarcerees with mental illnesses are significantly more likely to recidivate, with serious mental illness, substance use disorders, and lack of treatment associated with higher levels of risk for return to incarceration (Zgoba et al. 2020). Cuts in mental health services have an impact on the prevalence of mental illnesses in jails and prisons insofar as they make it more difficult for treatment providers to dedicate resources to this population. Compared to their counterparts, probationers and parolees with mental illness are significantly more likely to have their probation or parole term suspended or revoked, resulting in reincarceration (Meredith et al. 2020). Stigma of supervision officers should be considered to be a potential factor in these trends (Eno Louden et al. 2018).
What Can Be Done to Reduce the Likelihood that They Will End Up There?
There are programmatic responses that can identify persons with mental illnesses in the criminal justice system, divert them from jail and prison, and reduce the likelihood of return. All of these programmatic efforts are dependent upon communication and integration between the mental health and criminal justice systems. Both linkage to effective treatment in the community and reverse communication with providers in incarceration settings are important (Lamberti 2016). The next section discusses evidence-based practices (EBPs) and program models intended to reduce criminal engagement of persons struggling with mental health problems.
The broad set of responses to behavioral needs of citizens within a community is shaped by local, state, and federal regulations and policy. When this focus is narrowed to a specific target population defined by its participation in criminal activity, the need for mental health leadership to incorporate the perspectives of law enforcement, courts, and local and state corrections personnel is imperative, as is the perspective of individuals with lived experience in these systems. Clarity in the goals and objectives for initiatives is critical to determine the range, format, and intensity of partnerships. At the outset, stakeholders may be convened as a strategic planning committee, but more collaborative partners will emerge as goals are formulated. Additional partners may include other treatment providers, housing officials, private funders, elected officials, peer supports, crime victims, family members, academic partners, advocates, or other community representatives.
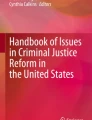
The sequential intercept model (SIM) creates a framework around which to organize responses to assist justice-involved individuals with mental illnesses (Munetz and Griffin 2006). The model diagrams the various stages at which an individual may come in contact with the criminal justice system. The five intercept points identified in the model are: (1) law enforcement, (2) initial detention and hearings, (3) jails/courts, (4) reentry from jail or prison, and (5) community corrections. The US Substance Abuse and Mental Health Services Administration (SAMHSA) offers SIM training for communities (Center 2020a). See Fig. 1.

Sequential intercept model (SAMHSA 2021)
The SIM focuses on a series of intercepts where interventions can prevent individuals from penetrating further into the criminal justice system. At each of these intercept points, there is an opportunity to develop programs tailored to the needs of persons with mental illnesses and subpopulations within this group. The hope is that the further upstream a person can be redirected, the fewer legal consequences will obstruct their path to recovery. The ultimate and most effective intercept has been described as accessible, comprehensive, and effective community-based services (Munetz and Griffin 2006).
At the first three intercepts, the processes are referred to as jail diversion which is defined as:
A community-based, collaborative criminal justice-mental health response for justice-involved people with mental illnesses where jail time is reduced or avoided, and the individual is linked to comprehensive and appropriate services. (JLI 2010)
Police-Based Responses
The earliest and most prevalent prebooking diversion programs exist within the community and often rely on law enforcement officers interacting with people in psychiatric crisis. Law enforcement officers have become the de facto first-line responders to deal with persons with mental health emergencies or criminal activity. How law enforcement personnel react to these individuals can have a huge impact on their outcomes and determine whether a person is linked to treatment and/or enters the criminal justice system (see chapter “Community Education”). A well-recognized program is the Crisis Intervention Team (CIT) through which officers receive training in how to recognize mental health problems and deescalate crises. CITs are associated with increased confidence and decreased stigma in law enforcement as well as more referrals to treatment (Pinals 2017). Another intervention relies on mental health specialists who provide consultation to law enforcement and often located within the department. A third prebooking approach is a specialized community mental health response, which includes mental health mobile crisis teams that work in partnership with police to deescalate emergencies and link individuals to services. Appropriate recognition of mental health crises, with deescalation and other nonaggressive techniques, also works towards decreasing the risk of violence in police encounters (Watson et al. 2008).
Jail- and Court-Based Strategies
Postbooking diversion programs at intercept 2 involve jail- and court-based strategies. In these programs, individuals identified as having mental health needs are linked to treatment with leveraged conditions of release. These interventions may consist of teams of mental health providers that operate within the jail and are available to assess individuals and to provide recommendations on diagnoses, treatment needs, and the possibility of alternative dispositions in the community. Identification of arrested persons with mental illnesses in some communities has been improved by the matching of jail rosters to public mental health rosters. A one-way flow of information is then generated to the mental health provider informing them that their client is in custody. The mental health provider can then attempt to engage their client and coordinate care within the jail, helping to promote alternatives to incarceration.
Specialized Courts
At intercept 3, specialized courts have been developed in jurisdictions across the country. Broadly characterized, mental health courts have been shown to reduce recidivism (Loong et al. 2019). The Honorable Steve Leifman established the foundation for the Miami Model in 2000, which continues to successfully function in its aims to divert individuals with serious mental illness away from the courts and into a full spectrum of treatment options (Leifman and Coffey 2020). Participants are identified by CIT-trained officers as well as postbooking screening and are then linked with comprehensive treatment and supports in the community. Most engagement is voluntary, but some participation may be actualized through civil commitment (Iglehart 2016). Legal consequences can be lowered or dropped with treatment adherence, resulting in fewer incarcerated people with SMI, reduced recidivism, cost savings, improved health and safety, and less homelessness (Leifman and Coffey 2020).
Transition Planning
With the constitutional obligation to provide health care comes an opportunity to identify and begin treatment for mental illnesses within jails and prisons. Despite chronic staffing shortages and limited formularies, critical treatment can take place behind bars. Assuring continuity from the community to the jail or prison and back to the community is imperative for effective mental health care. Almost all jail inmates, including those with mental illnesses will leave correctional settings and return to the community. Thoughtful transition planning from jails and prisons can reduce the possibility of return to criminal justice systems (Skeem et al. 2011).
At intercept 4, inadequate transition planning can put individuals who entered jail in a crisis state back on the street in the middle of the same crisis. Individuals were often released without Medicaid benefits or medical insurance (though this improved somewhat with that passage of the Affordable Care Act in 2010) (Heiss et al. 2016). Enrollment in Medicaid should be a focus of intervention. Inadequate treatment upon release increases the risks for repeat offenses, psychiatric instability, hospitalization, homelessness, rearrest, and death from overdose (Binswanger et al. 2007). We follow the suggestion of the American Association of Community Psychiatrists (AACP) by using the term transition planning, rather than discharge planning or reentry planning, in order to imply bidirectional responsibility and collaboration among providers (Sowers and Rohland 2004). It is understood that some ex-offenders will return to custody and as such reentry can be seen as part of a cycle of care, though with attempts to decrease recidivism. Transition planning is a process and not an event. The APIC model – assess, plan, identify, and coordinate – describes elements of transition planning associated with successful integration back into the community (Osher et al. 2003). The model pays attention to biopsychosocial strengths and needs, short- and long-term projections, and coordination of support. Such planning can serve as an investment in public health by reducing future costs associated with reincarceration (Wolff 2005).
Specialized Community Supervision
At intercept 5, there are significant opportunities to reduce the prevalence of persons with mental illnesses in jail and prison. The number of people with mental illness under correctional supervision reached unprecedented levels in the mid-aughts, with the vast majority of persons supervised in the community (Glaze and Bonczar 2010). Probation and parole officers are often left with revocation to jail or prison as a punishment for failing to meet conditions of release. These technical violations, where a new crime has not been committed, are a principal contributor to ballooning correctional populations (White et al. 2011). In this context, specialized community caseloads have been developed to improve outcomes for persons with mental illnesses under community correctional supervision. The key features of such programs are closer supervision and support of persons with mental illness, officer training on psychiatric issues, and collaboration with community-based providers (Prins and Draper 2009). Studies support this model as effective in improving the well-being and reducing the reincarceration risk of people with mental illness on probation and parole (Skeem and Louden 2006). However, with states facing the grim reality of enormous budget constraints, the resources to fund effective, specialized transition resources are difficult to come by.
Comprehensive, Effective Community-Based Care: The Ultimate Intercept
It has been said that any effort to keep people with mental illnesses out of the criminal justice system will only be as good as the community treatment and supports available – the ultimate intercept. Towards that end, this chapter now discusses linkage to community treatment. There are several EBPs that have the potential to reduce jail days for persons with mental illnesses. In discussing justice-involved persons with mental illnesses, it is important to keep in mind the heterogeneity of this group. They differ in terms of the seriousness of their mental illnesses, charge levels, criminogenic risks, demographics, and access to community supports. Unfortunately, many inmates are un- or undertreated at the time of their arrests (Wilper et al. 2009). The community mental health system also rarely assesses the nature of criminal justice involvement or criminogenic risk. Almost one-half of the clients seen for the first time at community mental health centers have had contact with the criminal justice system and that nearly one-third of them had been sentenced to jail (Theriot and Segal 2005). Lumping justice-involved persons with mental illnesses into a single class does not allow for prioritization of scarce resources to those with highest need or who might benefit most. There is a great need for valid, reliable screening and assessment processes that can drive the development of effective, integrated treatment and supervision plans. What follows are recommended services to reduce criminal justice involvement in persons with mental illnesses.
Integrated Mental Health and Substance Use Services
Since the majority of justice-involved persons with mental illnesses will have co-occurring addictive disorders, effective and integrated treatments must be available. The structure of services as well as the treatments themselves can be integrated. There are a number of evidence-based, integrated practices for correctional implementation, though gaps in service delivery remain (Peters et al. 2017). These interventions include integrated dual disorder treatment (IDDT), cognitive-behavioral therapy (CBT), modified therapeutic community (MTC), and the risk-need-responsivity (RNR) model. Integrated treatment for justice-involved persons has been associated with improved criminal justice and mental health outcomes, including reduced criminal activity, substance abuse, arrest, and reincarceration (Osher 2013; see chapters “Integrated Care and Community Psychiatry”, and “Social and Political Determinants of Health and Mental Health”, for more detailed discussion). Given the high correlation of substance use disorders with crime, they should be the primary target of treatment. It is also associated with significant cost-saving for correctional systems (BEM 2009).
Supportive Housing
High rates of homelessness among justice-involved persons with mental illnesses must be considered in comprehensive treatment planning (Osher and Steadman 2007). Housing needs range from owning their own homes or living in independent rental units to institutional care. Supportive housing can significantly decrease the chance of recidivism as well as time spent in shelters or hospitals and is less costly on a daily basis than time spent in institutions (Salem et al. 2015). Supportive housing includes a variety of residential settings with on-site or easily accessible services, including case management, peer support, medical care, mental health and substance abuse treatment, vocational training, cognitive skills groups, and assistance in obtaining income supports and entitlements. Unfortunately, affordable housing is in short supply in many communities, and persons with criminal records often have trouble accessing public housing assistance (For greater detail, please refer to chapters “Psychiatric Care for People Experiencing Homelessness” concerning homelessness and “Housing First and the Role of Psychiatry in Supported Housing” for a discussion of housing).
Trauma Interventions
Incarceration is closely linked with trauma in myriad ways. Almost all categories of adverse childhood experiences (ACEs) are associated with future incarceration, as well as with later victimization, drug use, and homelessness (Eaves et al. 2020). Evidence also indicates that treatment for those with a history of ACEs may need to be substantially different than for those without such experiences. Rates of physical and sexual abuse in jail and prison populations have been found to be at least twice as high as in the general population (Teplin et al. 1996) and are associated with having a mental illness (Karlsson and Zielinski 2020). Among some inmate populations, such as previously homeless women with co-occurring mental and substance use disorders, histories of violent victimization are extremely high (Anderson et al. 2016). Studies indicate that posttraumatic stress disorder (PTSD) may exist in nearly 50% of inmates, as compared to less than 10% of the general population (Anderson et al. 2016). Moreover, the very experience of incarceration is one of trauma, coercion, injury, invasiveness, violence, and dehumanization (Piper and Berle 2019). In particular, solitary confinement is highly associated with the development of PTSD. Having posttraumatic stress disorder is then associated with negative post-release experiences including self-harm and suicide, additional trauma, homelessness, and reincarceration (Piper and Berle 2019).
Because of the pervasiveness and profound consequences of trauma, criminal justice system programs must integrate sensitivity to trauma into service delivery (Levenson and Willis 2019) (a detailed discussion of trauma-informed care is present in chapter “Traumatic Stress in the Community: Identificationand Intervention”). Training correctional treatment staff in this approach can work towards creating a calmer and safer environment for inmates as well as employees. Both rehabilitative efforts (intended to reduce criminality) and mental health treatment (framed for diagnoses and symptoms) can specifically address trauma. SAMHSA offers training for trauma-informed responses to court personnel, law enforcement, community corrections, and providers (Center 2020a, b). Trauma-focused models that fit the correctional setting focus on the present, use cognitive behavioral approaches, provide education, and emphasize coping skills; one example would be the seeking safety approach (Miller and Najavits 2012). Various models have been shown to reduce violence and recidivism in youth and adolescents, including trauma-focused cognitive-behavioral therapy (TF-CBT), family functional therapy (FFT), and multisystemic therapy (MST), though more research is needed for these and other populations (Zettler 2020).
Supported Employment
Given that some criminal activity is driven by the need for money, successful employment is expected to mitigate contact with the criminal justice system. In fact, many studies have shown that employment of returning citizens is associated with lower chances of recidivism (Bunting et al. 2019). As detailed in chapter “Supported Employment”, over the past 30 years, supported employment has become an important tool for improving the well-being of persons with serious mental illness (Drake et al. 2016). Such programs should be modified to accommodate conditions of release, allowing community correctional obligations to exist concurrently with employment responsibilities. A number of successful community reintegration programs include supported employment, but more research is needed on the efficacy of this component in reducing recidivism (Leifman and Coffey 2020). Individual placement and support (IPS) is an employment model that may be particularly effective for justice-involved individuals with serious mental illness, particularly when coupled with dual diagnosis treatment (Bond 2013).
Illness Management and Recovery
Illness management and recovery comprise a group of EBPs that teach skills required to manage a person’s own mental illness in collaboration with health care professionals and other supports (see chapter “Health Self-Management: The Emerging Importance of Trauma and Resilience” for details). These EBPs have been demonstrated to promote recovery in functional, personal, and clinical domains (Roosenschoon et al. 2019). There are several illness management and recovery programs, including the Wellness Recovery and Action Plan (WRAP) and Social and Independent Living Skills (SILS).
When these programs have been implemented for persons with mental illnesses and co-occurring disorders within correctional settings, they produce the expected social and coping skill gains (Black et al. 2019). The common application of psychoeducational and cognitive components within illness management and recovery programs makes them well-suited for adaptations that could address criminogenic thinking and antisocial tendencies. Using WRAP with homeless individuals has been shown to reduce recidivism (Listwan et al. 2018), but more evidence is needed.
Case Management and Forensic Assertive Community Treatment
Access to case management services is important for individuals with complex mental health and legal needs. Assertive community treatment (ACT) is a well-validated EBP that combines treatment, rehabilitation, and support services within a multidisciplinary team (Dixon 2000). It is a high-intensity, high-cost package that is typically reserved for the topmost utilizers of acute and emergency mental health services (see chapter “Case Management and Assertive Community Treatment” for a detailed discussion). Particularly when combined with the provision of low-demand housing, it has been associated with less criminal justice involvement (Hirschtritt and Binder 2017).
More recently, ACT services have been augmented by specifically focusing on justice-involved populations and training team members to be responsive to criminal justice partners (Weisman et al. 2004). These forensic ACT teams, also known as FACT teams, aim to specifically reduce recidivism, are integrated into the legal system, and include additional forms of supervision; substance use treatment is highly recommended for their success (Kelly et al. 2017). Some studies show FACT involvement to be associated with reduced time spent behind bars, yet to effectively realize such goals, the teams should be part of an overall forensic continuum of care (Cuddeback et al. 2020).
The development of forensic intensive case management (FICM) teams is another effort to coordinate criminal justice and treatment services. FICM focuses on arranging access to services rather than direct provision of care and, without requiring a large team, is less costly to implement (Lee and Cain 2020). The bottom line for many justice-involved persons with mental illness is that any case management team must have a sound understanding of legal issues. With “criminal justice savvy” case management, teams can be expected to reduce recidivism and have been found to have better success than regular ACT teams (Cuddeback et al. 2020).
Cognitive-Behavioral Interventions
Critical to a more complete understanding of these patterns of incarceration are the concepts of criminogenic risk factors and criminogenic needs. Criminogenic risk factors are those associated with criminal conduct and arrest. According to the risk-need-responsivity (RNR) model, the primary risk factors are antisocial personality, substance use, antisocial behavior, family circumstances, low levels of employment and education, antisocial peers, antisocial cognition, and how one spends leisure time (Wilson et al. 2020). While originally describing a more general population, studies have shown that the same factors are associated with criminal recidivism in those with mental illness (Wilson et al. 2020). In our support of and advocacy for persons with mental illness, we cannot overlook the (often times, even higher) levels of criminogenic risk factors present in people with mental illness who are justice-involved (Wilson et al. 2020); to do so would be a missed opportunity for intervention. The intensity of mental health symptoms covaries with higher criminogenic risk (Van Deinse et al. 2021), though shared criminogenic risk factors largely predict recidivism independently of mental illness (Skeem et al. 2014).
The four risk factors that are often portrayed to be the most amenable to improvement are a person’s criminal thinking, behavior, personality, and associates (Abracen et al. 2016). Cognitive-based correctional programming tends to target antisocial personality and behavior and focuses more on interpersonal expression than, as typical, on individual distress (Rotter and Carr 2010). Unfortunately, relatively simple approaches for substance use and other risk factors are often neglected. Criminogenic needs are individual characteristics associated with risk factors; those associated with criminal personality and behavior include risk-taking, hostility, anger, irritability, and cold-heartedness. While a time-limited correctional program may address anger in a meaningful way, other needs such as emotional callousness might be harder to intervene upon. Furthermore, research has found inmates with serious mental illness to have low levels of employment and education, substance abuse, and maladaptive recreational endeavors, which are usually not addressed by the justice system (Wilson et al. 2020). Unfortunately, incarceration can also increase contact with criminal- minded peers and call for certain behaviors intended to protect oneself, in effect working against a stated goal of criminal rehabilitation.
The more criminogenic needs that are addressed by treatment and supports in general, the bigger the expected impact on recidivism (Latessa and Lowenkamp 2005). Addressing the criminogenic needs of incarcerated or formerly incarcerated people with SMI can be specifically adapted to increase chances of success (Wilson et al. 2018). Given the prevalence of social and neurocognitive difficulties, effective programs will include actively involved staff who frequently repeat and summarize information using concrete language. The format should allow for accessible participation.
Accessible and Appropriate Medication
Psychiatric medication is a critical tool, and for many individuals, treatment is disrupted when they enter and exit the criminal justice system. Having access to appropriate medication at suitable doses, for sufficient lengths of time, is imperative. It is clear that effective psychopharmacology is important for the personal recovery of many people as well as for fulfillment of criminal justice requirements (by being able to function better with a reduced symptom burden) (Skeem et al. 2014).
Research points towards more specific associations, as well. Some findings indicate that mood stabilizers and antipsychotic medications (particularly long-acting injectables) are associated with reduced violent crime (Fazel et al. 2014), and data indicates that medication nonadherence, in concert with substance use, is associated with increased rates of violence in those with SMI (Swartz et al. 1998). Populations with attention-deficit hyperactivity disorder (ADHD) are also less likely to engage in crime when appropriately medicated (Lichtenstein et al. 2012). On the other hand, population-level prescriptions of selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs) have been recently associated with having no effect on violent crime (Osler et al. 2019) as well as with an increased risk of violent crime in past offenders and youth (Lengvenyte and Vieta 2020).
Conclusion
As for other persons with serious mental illnesses, access to prescribers, funding for medications, supports for adherence, and fluid continuity across systems are challenges for those involved in the criminal justice system. These programs are components of a comprehensive strategy to reduce the overrepresentation of persons with mental illnesses in the justice system. Few communities have all components and none have sufficient capacity, yet inroads are being made. Financing these EBPs relies on a patchwork of block grant funding, public and private insurance, and uncompensated care. Advocacy for investments in these services is essential. At the time of publication of the previous edition of this chapter, the passage of the Patient Protection and Affordable Care and Health Care and Education Reconciliation Acts held promise for this population. Ten years later, however, significantly increased insurance coverage has not been associated with improved access to mental health care for formerly incarcerated patients, reinforcing that there are no simple solutions for addressing the complex needs of this population (Howell et al. 2019).
Community psychiatrists are working, and will continue to work, with persons who have criminal justice histories. They should develop familiarity with the system and how it intersects with their patient’s lives and future trajectories. Recovery-oriented practices are as germane to justice-involved persons as any. Community psychiatrists must understand the literature and work with their patients towards a vision of what is likely to work, for whom, and under what circumstances. Gaining this expertise can be achieved through formal training (such as a forensic and/or community psychiatry fellowship program) as well as through other routine methods of lifelong learning. If we are to avoid being a society where punishment inappropriately substitutes for care, a shared commitment to our patients’ dignity and our communities’ safety is of paramount importance.
References
(2002) Criminal Justice/Mental Health Consensus Project Report. New York, NY, Council of State Governments Justice Center.
(2008) One in 100: Behind bars in America 2008. Washington, DC, Pew Center on the States.
(2020) State Expenditure Report (Fiscal 2018-2020 Data). Washington, DC, National Association of State Budget Officers.
Abracen, J., Gallo, A., Looman, J. & , Goodwill, A. (2016). Individual community-based treatment of offenders with mental illness: Relationship to recidivism. Journal of Interpersonal Violence, 31(10), 1842–1858.
Allison, S., Bastiampillai, T., & Fuller, D. A. (2017). Mass incarceration and severe mental illness in the USA. The Lancet, 390(10089), 25.
Anderson, R. E., Geier, T. J., & Cahil, S. P. (2016). Epidemiological associations between posttraumatic stress disorder and incarceration in the National Survey of American Life. Criminal Behaviour and Mental Health, 26(2), 110–123.
Anestis, J. C., & Carbonell, J.L. (2014). Stopping the revolving door: Effectiveness of mental health court in reducing recidivism by mentally ill offenders. Psychiatric Services, 65(9), 1105–1112.
Barboriak, P.N. (2017). The history of correctional psychiatry in the United States. Principles and Practice of Forensic Psychiatry, 3rd edition. Edited by Rosner R, Scott CL, New York, CRC Press. 511–520.
BEM, M. D. F. (2009). Providing chemical dependency treatment to low-income adults results in significant public safety benefits, Olympia (WA), Washington State Department of Social and Health Services.
Binswanger, I. A., Stern, M. F., Deyo, R. A., Heagerty, P. J., Cheadle, A., Elmore, J. G. & , Koepsell, T.D. (2007). Release from prison--a high risk of death for former inmates. N Engl J Med, 356(2), 157–165.
Black, A et al. (2019). The treatment of people with mental illness in the criminal justice system: The example of Oneida County, New York, Clinton, NY, Levitt Center for Public Affairs, Hamilton College. https://digitalcommons.hamilton.edu/student_scholarship/6/.
Bond, G.R. (2013). Supported employment for justice-involved people with mental illness. SAHSA GAINS Center for Behavioral Health and Justice Transformation. http://gainscenter.samhsa.gov.
Bunting, A.M., Staton, M., Winston, E., & Pangburn, K. (2019). Beyond the employment dichotomy: An examination of recidivism and days remaining in the community by post-release employment status. International Journal of Offender Therapy and Comparative Criminology,. 63(5), 12–733.
Care, N. (2008). Standards for Mental Health Services in Correctional Facilities. National Commission on Correctional Health Care.
Center, S. (2020a). Training Opportunities. Retrieved 12/20/2020, from https://www.samhsa.gov/gains-center/trauma-training-criminal-justice-professionals/training-opportunities.
Center, S. (2020b). Trauma Training for Criminal Justice Professionals. Retrieved 12/20/2020, from https://www.samhsa.gov/gains-center/trauma-training-criminal-justice-professionals.
Cohen, F. (2008). The Mentally Disordered Inmate and the Law: Cumulative Supplement. Kingston, NJ, Civic Research Institute, Inc.
Cuddeback, G. S., Simpson, J.M., & Wu, J. C. (2020). A comprehensive literature review of Forensic Assertive Community Treatment (FACT): Directions for practice, policy and research. International Journal of Mental Health, 49, 106–127.
Deutsch, A. (1937). Mental Illness in America: A History of Their Care and Treatment from Colonial Times. New York, Columbia University Press.
Dixon, L. (2000). Assertive community treatment: Twenty-five years of gold. Psychiatric Service, 51(6), 759–765.
Draine, J., A. Blank Wilson, S. Metraux, T. Hadley & A. C. Evans (2010). The impact of mental illness status on the length of jail detention and the legal mechanism of jail release. Psychiatric Services, 61(5), 458–462.
Drake, R. E., Bond, G. R., Goldman, H. H., Hogan, M. F., & Karakus, K. M. (2016). Individual placement and support services boost employment for people with serious mental illnesses, but funding is lacking. Health Affairs, 35(6), 1098–1105.
Dvoskin, J. A., Spiers, E. M., Metzner, J. L., & Pitt, SE. (2003). The structure of correctional mental health services. In Principles and Practice of Forensic Psychiatry, 2Ed. Boca Raton, FL, CRC Press, 511–526.
Eaves, E. R., Camplain, R.L., Lininge, M.R., & Trotter II, R. T. (2020). Adverse childhood experiences in relation to drug and alcohol use in 30 days prior to incarceration in a county jail. International Journal of Prisoner Health, 17, 142–155.
Eno Louden, J., Manchak, S. M., Ricks, E. P., & Kennealy, P. K. (2018). The role of stigma toward mental illness in probation officers’ perceptions of risk and case management decisions. Criminal Justice and Behavior, 45(5), 573–588.
Fazel, S., Zetterqvist, J., Larsson, H., Långström, N., & Lichtenstein, P. (2014). Antipsychotics, mood stabilisers, and risk of violent crime. The Lancet, 384(9949), 1206–1214.
Glaze, L. E. & Bonczar, T. P. (2010). Probation and parole in the United States, 2006. Washington, DC, Bureau of Justice Statistics.
Greenberg, G. A. & Rosenheck, R. A. (2008). Jail incarceration, homelessness, and mental health: A national study. Psychiatric services, 59(2), 170–177.
Heiss, C., Somers, S. A., & Larson, M. (2016). Coordinating Access to Services for Justice-Involved Populations. Center for Health Care Strategies. New York, Milbank Memorial Fund. 1–21.
Hills, H., Sigfried, C., & Ickowitz, A. (2004). Effective prison mental health services: Guidelines to expand and improve treatment. Washington, DC, US Department of Justice, National Institute of Corrections.
Hirschtritt, M. E., & Binder, R. L. (2017). Interrupting the mental illness–incarceration-recidivism cycle. Jama, 317(7), 695–696.
Houser, K. A., & Welsh, W. (2014). Examining the association between co-occurring disorders and seriousness of misconduct by female prison inmates. Criminal Justice and Behavior, 41(5), 650–666.
Howell, B. A., Wang, E. A., & Winkelman, T. N. (2019). Mental health treatment among individuals involved in the criminal justice system after implementation of the Affordable Care Act. Psychiatric Services, 70(9), 765–771.
Iglehart, J. K. (2016). Decriminalizing mental illness—the Miami model. New England Journal of Medicine, 374(18), 1701–1703.
James, D. J. and L. E. Glaze (2006). Mental health problems of prison and jail inmates. US Department of Justice/Office of Justice Programs. Washington, DC, Bureau of Statistics.
JLI (Judges’ Criminal Justice/Mental Health Leadership Initiative). (2010). Judges’ guide to mental health diversion: A reference for justice system practitioners. Delmar, NY, Policy Research Associates, CMHS National GAINS Center.
Kaeble, D., Glaze, L., Tsoutis, A., & Minton, T. (2016). Correctional populations in the United States, 2014. Washington, DC, Bureau of Justice Statistics, 1–19.
Kaeble, D. and M. Cowhig (2018). Correctional Populations in the United States, 2016. Washington, DC, Bureau of Justice Statistics, 1–13.
Karlsson, M. E., & Zielinski, M. J. (2020). Sexual victimization and mental illness prevalence rates among incarcerated women: A literature review. Trauma, Violence, & Abuse, 21(2), 326–349.
Kelly, B. L., Barrenger, S. L., Watson, A. C., & Angell, B. (2017). Forensic assertive community treatment: Recidivism, hospitalization, and the role of housing and support. Social Work in Mental Health, 15(5), 567–587.
Kessler, R. C. (2004). The epidemiology of dual diagnosis. Biological Psychiatry, 56(10), 730–737.
Lamb, H. R., & Weinberger, L.E. (2017). Understanding and treating offenders with serious mental illness in public sector mental health. Behavioral Sciences & the Law, 35(4), 303–318.
Lamberti, J. S. (2016). Preventing criminal recidivism through mental health and criminal justice collaboration. Psychiatric Services, 67(11), 1206–1212.
Latessa, E. J., & Lowenkamp, J. (2005). What are criminogenic needs and why are they important. For the Record, 4, 15–16.
Lee, L. H., & Cain, D. S. (2020). Mental Health Policy for Justice-Involved Persons: Exploring History, Perspectives, and Models in the United States. Best Practices in Mental Health, 16(2), 55–68.
Leifman, S., & Coffey, T. (2020). Jail diversion: the Miami model. In Decriminalizing Mental Illness, K. Warburton and S. Stahl (eds), Cambridge, UK, Cambridge University Press, 97–105.
Lengvenyte, A., & Vieta, E. (2020). Association between selective serotonin reuptake inhibitors and violent crime - could underlying psychopathology be the cause? Eur Neuropsychopharmacol 36, 151–153.
Levenson, J. S., & Willis, G. M. (2019). Implementing trauma-informed care in correctional treatment and supervision. Journal of Aggression, Maltreatment & Trauma, 28(4), 481–501.
Lichtenstein, P., Halldner, L., Zetterqvist, J., Sjölander,A., Serlachius, E., Fazel, S., Långström, N., & Larsson, H. (2012). Medication for attention deficit–hyperactivity disorder and criminality. New England Journal of Medicine, 367(21), 2006–2014.
Listwan, S. J., Hartman, J. L., & LaCourse, A. (2018). Impact of the MeckFUSE Pilot Project: Recidivism among the chronically homeless. Justice Evaluation Journal, 1(1), 96–108.
Loong, D., Bonato,S., Barnsley, J., & Dewa, C. S. (2019). The effectiveness of mental health courts in reducing recidivism and police contact: a systematic review. Community Mental Health Journal, 55(7), 1073–1098.
Massoglia, M., & Remster, B. (2019). Linkages between incarceration and health. Public Health Reports, 134(1_suppl), 8S–14S.
Matejkowski, J., & Ostermann, M. (2020). The Waiving of Parole Consideration by Inmates With Mental Illness and Recidivism Outcomes. Criminal Justice and Behavior, 48 (8), 1052–1071.
Mauer, M., & King, R. K. (2007). 25-Year Quagmire: The “War On Drugs” and Its Impact on American Society, Washington, DC, Sentencing Project.
Meredith, T., Hawk, S. R., Johnson, S., Prevost, J. P., & Braucht, G. (2020). What Happens in Home Visits? Examining a Key Parole Activity. Criminal Justice and Behavior 47(5), 601–623.
Miles, H., Johnson, S., Amponsah-Afuwape, S., Finch, E., Leese, M., & Thornicroft, G. (2003). Characteristics of subgroups of individuals with psychotic illness and a comorbid substance use disorder. Psychiatric Services, 54(4), 554–561.
Miller, N. A., & Najavits, L. M. (2012). Creating trauma-informed correctional care: A balance of goals and environment. European Journal of Psychotraumatology, 3(1), 17246, https://doi.org/10.3402/ejpt.v3i0.17246.
Munetz, M. R., & P. A. Griffin (2006). Use of the sequential intercept model as an approach to decriminalization of people with serious mental illness. Psychiatric Services, 57(4), 544–549.
Osher, F., Steadman, H. J., & Barr, H. (2003). A best practice approach to community reentry from jails for inmates with co-occurring disorders: The APIC model. Crime & Delinquency, 49(1), 79–96.
Osher, F. C. (2013). Integrating mental health and substance abuse services for justice-involved persons with co-occurring disorders. Delmar, NY: SAMHSA’s GAINS Center for Behavioral Health and Justice Transformation.
Osher, F. C., & Steadman, H. J. (2007). Adapting evidence-based practices for persons with mental illness involved with the criminal justice system. Psychiatric Services 58(11), 1472–1478.
Osler, M., Wium-Andersen, M. K., Wium-Andersen, I. K., Gronemann, F. S., Jørgensen, M. B., & Rozing, M. P. (2019). Incidence of suicidal behaviour and violent crime following antidepressant medication: a Danish cohort study. Acta Psychiatrica Scandinavica, 140(6), 522–531.
Peters, R. H., Wexler, H. K., & Lurigio, A. J. (2015). Co-occurring substance use and mental disorders in the criminal justice system: A new frontier of clinical practice and research. Psychiatric Rehabilitation Journal, 38(1), 1–6.
Peters, R. H., Young, M. S., Rojas, E. C., & Gorey, C. M. (2017). Evidence-based treatment and supervision practices for co-occurring mental and substance use disorders in the criminal justice system. The American Journal of Drug and Alcohol Abuse, 43(4), 475–488.
Pinals, D. A. (2017). Jail diversion, specialty court, and reentry services: Partnerships between behavioral health and justice systems. Principles and Practice of Forensic Psychiatry, 3rd edition. Edited by Rosner R., Scott C. L., New York, CRC Press, 237–246.
Piper, A., Berle, D. (2019). The association between trauma experienced during incarceration and PTSD outcomes:A systematic review and meta-analysis. J Forensic Psychiatry & Psychology, 30(5), 854–875.
Pratt, S. I., Mueser, K. T., Driscoll, M. R., et al. (2006). Medication nonadherence in older people with serious mental illness: Prevalence and correlates. Psychiatric Rehab J 29(4), 299–310.
Prins, S. J., & Draper, L (2009). Improving Outcomes For People with Mental Illness Under Community Corrections Supervision: A Guide to Research-Informed Policy and Practice. New York City, NY, Council of State Governments Justice Center.
Rich, J. D., Wakeman, S. E., Dickman, S. L. (2011). Medicine and the epidemic of incarceration in the United States. NEJM, 364(22), 2081–2083.
Roosenschoon, B. J., Kamperman, A. M., Deen, M. L., van Weeeghel, J., et al. (2019). Determinants of clinical, functional and personal recovery for people with schizophrenia and other severe mental illnesses: A cross-sectional analysis. PloS One 14(9), e0222378.
Rotter, M., & Carr, C. (2010). Targeting criminal recidivism in justice-involved people with mental illness: structured clinical approaches. Rockville, Md, Substance Abuse and Mental Health Services Administration, GAINS Center for Behavioral Health and Justice Transformation.
Rozel, J.S., & Mulvey, E. P. (2017). The link between mental illness and firearm violence: implications for social policy and clinical practice. Ann Rev Clin Psychol, 13, 445–469.
Salem, L., Crocker, A. G., Charette, Y., et al. (2015). Supportive housing and forensic patient outcomes. Law Hum Behav, 39(3), 311–320.
Substance Abuse and Mental Health Services Administration (2021). The Sequential Intercept Model. Available at https://www.samhsa.gov/criminal-juvenile-justice/sim-overview. Accessed 20 March, 2022.
Sindicich, N., Mills, K. L., Barrett, E. L., et al. (2014). Offenders as victims: Post-traumatic stress disorder and substance use disorder among male prisoners. J Forensic Psychiatry & Psychology, 25(1), 44–60.
Skeem, J. L., & Louden, J. E. (2006). Toward evidence-based practice for probationers and parolees mandated to mental health treatment. Psy Services, 57(3), 333–342.
Skeem, J. L., Manchak, S., Peterson, J. K. (2011). Correctional policy for offenders with mental illness: Creating a new paradigm for recidivism reduction. Law Hum Behav 35(2), 110–126.
Skeem, J. L., Winter, E., Kennealy, P. J., et al. (2014). Offenders with mental illness have criminogenic needs, too: Toward recidivism reduction. Law Hum Behav, 38(3), 212–224.
Sowers, W. E., & Rohland, B. (2004). American Association of Community Psychiatrists’ principles for managing transitions in behavioral health services. Psy Services, 55(11), 1271–1275.
Steadman, H. J., Osher, F. C., Robbins, P. C., et al. (2009). Prevalence of serious mental illness among jail inmates. Psy Services, 60(6), 761–765.
Stephan, J. J. (2001). Census of Jails, 1999. Washington, D. C., Bureau of Justice Statistics.
Stuart, H. (2003). Violence and mental illness: An overview. World Psychiatry, 2(2), 121–124
Swanson, J. W., Frisman, L. K., Robertson, A. G., et al. (2013). Costs of criminal justice involvement among persons with serious mental illness in Connecticut. Psy Services, 64(7), 630–637.
Swanson, J. W., McGinty, E.E., Fazel, S., Mays, V. M. (2015). Mental illness and reduction of gun violence and suicide: Bringing epidemiologic research to policy. Ann Epidemiology, 25(5), 366–376.
Swartz, M. S., Swanson, J. W., Hiday, V. A., et al. (1998). Violence and severe mental illness: the effects of substance abuse and nonadherence to medication. Am J Psychiatry, 155(2), 226–231.
Teplin, L. A., Abram, K. M., McClelland, G. M. (1996). Prevalence of psychiatric disorders among incarcerated women: I. Pretrial jail detainees. Arch Gen Psychiatry, 53(6), 505–512.
Teplin, L. A., McClelland, G. M., Abram, K. M., Weiner, D.A. (2005). Crime victimization in adults with severe mental illness: Comparison with the National Crime Victimization Survey. Arch Gen Psychiatry, 62(8), 911–921.
Theriot, M. T., & Segal, S. P. (2005). Involvement with the criminal justice system among new clients at outpatient mental health agencies. Psy Services, 56(2), 179–185.
Van Deinse, T. B., Cuddeback, G. S., Wilson, A. B., Eswards, D., Jr., et al. (2021). Variation in criminogenic risks by mental health symptom severity: Implications for mental health services and research. Psychiatric Q, 92(1), 73–84.
Ventura, L. A., Cassel, C. A., Jacoby, J. E., Huang, B. (1998). Case management and recidivism of mentally ill persons released from jail. Psy Services, 49(10), 1330–1337.
Watson, A. C., Morabito, M. S., Draine, J., Ottati, V. (2008). Improving police response to persons with mental illness: A multi-level conceptualization of CIT. Int J Law Psychiatry, 31(4), 359–368.
Weinstein, H. C., Burns, K. A., Newkirk, C. S., Zil, J. S., Dvorkin, J. A., Steadman, H. J. (2000). Psychiatric Services in Jails and Prisons: A Task Force Report of the American Psychiatric Association, 2nd Edition. Arlington, VA, American Psychiatric Publishing, Inc.
Weisman, R. L., Lamberti, J., Price, N. (2004). Integrating criminal justice, community healthcare, and support services for adults with severe mental disorders. Psy Quarterly, 75(1), 71–85.
White, M. D., Mellow, J., Englander, K., Ruffinengo, M. (2011). Halfway back: An alternative to revocation for technical parole violators. Crim Justice Policy Rev, 22(2), 140–166.
Wilper, A. P., Woolhandler, S., Boyd, J. W., et al. (2009). The health and health care of US prisoners: Results of a nationwide survey. Am J Public Health, 99(4), 666–672.
Wilson, A. B., Farkas, K., Bonfine, N., Duda-Banwar, J. (2018). Interventions that target criminogenic needs for justice-involved persons with serious mental illnesses: A targeted service delivery approach. Internatl J Offender Therapy Compar Criminol, 62(7), 1838–1853.
Wilson, A. B., Ishler, K. J., Morgan, R., et al. (2020). Examining criminogenic risk levels among people with mental illness incarcerated in U.S. jails and prisons. J Behav Hlth Services & Resch, 1–16 (online). https://doi.org/10.1007/s11414-020-09737-x
Wolff, N. (2005). Community reintegration of prisoners with mental illness: a social investment perspective. Internatl J Law Psychiatry, 28(1), 43–58.
Zettler, H. R. (2020). Much to do about trauma: a systematic review of existing trauma-informed treatments on youth violence and recidivism. Youth Violence Juv Justice, 19(1), 113–134.
Zgoba, K. M., Reeves, R., Tamburello, A., Debilio, L. (2020). Criminal recidivism in Inmates with mental illness and substance use disorders. J Am Acad Psychiatry Law, 48(2), 209–215.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Joy, M., Osher, F.C. (2022). Collaborative Reduction of Criminal Justice Involvement for Persons with Mental Illness. In: Sowers, W.E., McQuistion, H.L., Ranz, J.M., Feldman, J.M., Runnels, P.S. (eds) Textbook of Community Psychiatry. Springer, Cham. https://doi.org/10.1007/978-3-031-10239-4_34
Download citation
DOI: https://doi.org/10.1007/978-3-031-10239-4_34
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-10238-7
Online ISBN: 978-3-031-10239-4
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)