
Abstract
Anterior knee pain (AKP) is the most common reason for adolescents, adults, and physically active people to consult with an orthopedic surgeon who specializes in the knee. Despite the high incidence and prevalence of AKP and an abundance of clinical and basic science research, the etiology of this condition is not well-known. This chapter synthesizes a review of the literature and our research and clinical experience on pathophysiology of AKP in the young patient.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
Anterior knee pain (AKP) is the most common reason for adolescents, adults, and physically active people to consult with an orthopedic surgeon who specializes in the knee. Despite the high incidence and prevalence of AKP and an abundance of clinical and basic science research, the etiology of this condition is not well-known. This chapter synthesizes a review of the literature and our research and clinical experience on pathophysiology of AKP in the young patient.
2 Theories on the Genesis of AKP
Until the end of the 1960s, AKP was attributed to chondromalacia patellae, a concept from the early twentieth century [1] that has no clinical value because it offers no specific diagnostic, therapeutic, or prognostic implications. In fact, many authors have failed to find a clear connection between AKP and chondromalacia patellae [2, 3].
In the 1970s AKP was related to the presence of patellar malalignment (PM) [4,5,6,7,8]. For many years, PM has been widely accepted as an explanation for the genesis of AKP in the young patient. Currently, the PM concept is questioned and is not universally accepted as an underlying factor in AKP. An obvious problem with the PM concept is that not all patellar malalignments, even those of significant proportions, are symptomatic (Fig. 1). A person with PM may not experience pain if the joint is never stressed to the extent that the tissues are irritated. Such individuals probably learn early that “my knee hurts when I do sports” and therefore stop being active. Further, only one knee may be symptomatic, even though the underlying patellar malalignment is entirely symmetrical in both knees (Fig. 1). In addition, patients with normal patellar alignment on computed tomography (CT) can also experience AKP. Therefore, although the patellar malalignment theory is biomechanically appealing, it has failed to explain the presence of AKP in many patients. We must also remember that significant differences have been demonstrated between subchondral bone morphology and the geometry of the articular cartilage surface of the patellofemoral joint (PFJ), in both the axial and sagittal planes [9]. Therefore, a radiographical PM may not be real, and realignment surgery to correct the nonexistent problem could lead to a worsening of preoperative symptoms.

Disabling AKP and patellar instability of the left knee. The right knee was asymptomatic in spite of the fact that PM was symmetric in both knees. A Preop CT at 0°, B Postop CT at 6 months of proximal realignment surgery, C CT of the right knee, D CT of the left knee at 13 years of follow-up—the patient is completely asymptomatic in spite of the presence of a visible PM. (A-Reused with permission from Thieme. From: Sanchis-Alfonso V. American Journal of Knee Surgery. Volume 7, Issue 2. Usefulness of computed tomography in evaluating the patellofemoral joint before and after Insall’s realignment. Thieme: New York. 1994, www.thieme.com)
At the end of 1970s, skeletal malalignment of the limb was suggested as the genesis of AKP in some cases [10]. Skeletal malalignment, which is not the same as PM, is the malalignment of the limb measured in the transverse, coronal, and sagittal planes. The presence of excessive femoral anteversion, excessive external tibial torsion, or increased varus or valgus abnormalities has a definite effect on the PFJ [11]. James in 1979 presented a comprehensive review of AKP in which he described the condition of “miserable malalignment”, that is, increased femoral anteversion and increased external tibial torsion [10]. In 1995 he reported on seven patients with miserable malalignment who had been treated with internal rotational tibial osteotomy during an 18-year period [12]. Several years earlier, Cooke and colleagues [13] described internal rotational proximal tibial osteotomy in seven patients presenting with AKP and drew attention to the inwardly pointing knee as an unrecognized cause of AKP. Unlike the concept of PM, however, the concept of skeletal malalignment was almost unnoticed and has had very low influence on orthopedic surgeons. In fact, very few publications refer to skeletal malalignment as a cause of AKP.
In the 1990s, Scott F. Dye and his research group at the University of California, San Francisco, proposed the tissue homeostasis theory [14, 15]. According to this theory, joints are not simply mechanical structures; they are systems that are alive and metabolically active [14]. Pain arises from a physiopathological mosaic of causes, including increased osseous remodeling, increased intraosseous pressure, or peripatellar synovitis leading to a reduced “envelope of function” (or “envelope of load acceptance”) (Fig. 2) [2, 14, 15]. This envelope of function is defined by the range of loading and energy absorption that coexists with normal tissue healing and maintenance (i.e., tissue homeostasis). According to Dye, in the vast majority of AKP cases, the loss of homeostasis of both osseous (Fig. 3) and soft tissue in the peripatellar region is more important than biomechanical/structural issues in the genesis of AKP. He suggests that AKP patients are often symptomatic because of supraphysiologic loading of anatomically normal knee components [2, 14, 15]. In fact, patients with AKP often lack an easily identifiable structural abnormality to account for their symptoms. According to Dye’s theory of envelope of load acceptance, overuse or cyclical overload of soft tissue or bone areas may explain AKP in many patients. However, it should be noted that this biological perspective is compatible with the biomechanical approach. The diagnostic challenge is to find the cause of the loading which is “in excess of the envelope of function or load acceptance”.

The envelope of function theory. (Reused with permission from SAGE. From Sanchis-Alfonso V, Dye SF. “How to Deal with Anterior Knee Pain in the Active Young Patient” Sports Health. 2017; 9(4):346–351)

SPECT-CT in a patient with disabling left AKP due to excessive external tibial torsion showing the loss of osseous homeostasis
Finally, in the 2000s, Chris Powers and his working group conducted weight-bearing studies of the PFJ and suggested that the main factor contributing to patella tilt and lateral displacement during weight-bearing is the internal rotation of the femur [16, 17]. That is to say, the primary contributor to lateral patellar subluxation and patellar tilt is the internal rotation of the femur below the patella. Therefore, control of the rotation of the femur is fundamental to guaranteeing normal patellofemoral kinematics. Thus, a new concept was born. It is the “proximal control” that is currently considered fundamental to understanding the physiotherapeutic treatment of an important subgroup of AKP patients. Lee and colleagues [18] have demonstrated that femoral rotation results in an increase in PFJ contact pressures on the contralateral facet of the patella (i.e., lateral PFJ during internal rotation of the femur and vice versa).
3 A Critical Analysis of Realignment Surgery for PM
After wide usage of certain surgical techniques, surgeons may come to question the basic tenets justifying the procedures and devise clinical research to test the underlying hypotheses. Realignment surgery for treating PM is no exception. In 2005, Sanchis-Alfonso and colleagues [19] retrospectively evaluated 40 Insall’s proximal realignments (IPRs) performed on 29 patients, with an average postsurgical follow-up of 8 years (range: 5–13 years). One of the objectives of this study was to analyze whether a relationship existed between the presence of PM and that of AKP. In this study, IPR was found to provide a satisfactory centralization of the patella into the femoral trochlea in the short-term follow-up and the surgery was associated with resolution of AKP [19, 20]. This outcome appears to support the PM theory; however, the success of realignment surgery may have been due to factors independent of the relative patellofemoral position, such as denervation of the patella, extensive postoperative rest (unload), and postoperative physical therapy. Unfortunately, the satisfactory centralization of the patella observed at the short-term follow-up was lost by the long-term follow-up in almost 57% of the cases, based on CT scans [19]. That is, IPR did not provide a permanent correction of patellofemoral congruence in all cases. Nonetheless, this loss of centralization did not correlate with a worsening of clinical results. In short, a relation between the result (satisfactory versus non-satisfactory) and the presence or absence of postoperative PM was not found in the long term [19].
Out of 29 patients in the study, 12 presented with unilateral symptoms. In nine of these patients, the contralateral asymptomatic knee presented a PM, and there was a satisfactory centralization of the patella into the femoral trochlea in only three cases [19]. If the presence of PM is crucial in the genesis of AKP, how can we account for unilateral symptoms in patients with similar morphologic characteristics between both patellofemoral joints? With regard to unilateral pain in the presence of bilateral PM, patients are known to preferentially load one limb more than the other (usually the dominant limb) in highly demanding activities, such as sports. This loading difference could be enough to cause unilateral pain, but we did not find a relationship between the lateral dominance and the affected side in cases with unilateral pain [21]. Further, in six patients with bilateral symptoms who received surgery on the knee with the most severe symptoms, the contralateral knee was pain-free at follow-up. Therefore, if the presence of PM is crucial in the genesis of AKP, why do symptoms disappear without any change in the patellofemoral alignment? Loss of both tissue and bone homeostasis may be more important than structural characteristics in the genesis of AKP.
Viewing AKP as being necessarily tied to PM is an oversimplification that has impeded progress toward better diagnosis and treatment. The great danger in using PM as a diagnosis is that the unsophisticated or unwary orthopedic surgeon may think that he or she can correct it with surgical procedures. Pursuing this misguided path very often makes the patients’ pain worse. The worst cases of AKP, at least in my series (V.S-A), occur in patients that have had multiple PM-oriented operative procedures for symptoms that initially were only mild and intermittent. We have observed that not all patellofemoral malaligned knees show symptoms, which is not surprising, because asymptomatic anatomic variations are not uncommon. Moreover, we have demonstrated that PM is not a sufficient condition for the onset of symptoms, given that many patients with AKP do not have PM. We can conclude that the pain does not arise from the PM. That is, pain does not arise from the malposition of the patella on the trochlea. Thus, no imaging study should give us an indication for surgery. PM diagnosed with plain x-ray, CT or MRI is only an instant in time and does not describe the dynamics of motion. Moreover, we do not have adequate proof of the definition of normal alignment. History, physical exam, and differential injection must point towards surgery, with imaging only being used to confirm clinical impression.
4 The Key Question: Is There a Mechanical Overload of the PFJ Behind AKP and What is the Role of Patellofemoral Imbalance in the Genesis of AKP?
Multiple approaches have been taken to determine the genesis of AKP, from the more traditional structural/biomechanical view to the newer tissue homeostasis perspective. Despite their differences, all potential explanations include joint loading as an important factor. This commonality is not surprising because the PFJ is very sensitive to stress.
Certain activities that highly load the PFJ, such as going down stairs or inclines or experiencing prolonged flexion while a person is sitting, kneeling, or squatting, are strongly associated with the genesis and persistence of AKP. In addition, a direct blow to the patella in a fall to the ground or with dashboard contact in an automobile accident can also cause pain that may persist for an extended time, even without an overt radiographically identifiable fracture. How can pain be explained in such cases by the tissue homeostasis perspective? The PFJ is one of the most highly loaded joints in the human body [22] as well as one of the most difficult musculoskeletal systems in terms of restoration of functionality after an injury and the subsequent loss of tissue homeostasis [23]. Joint reaction forces that are created within the PFJ with certain activities can be many times the body weight [24]. These high loads have been estimated to be 3.3 times the body weight with activities such as climbing up or down stairs, 7.6 times the body weight with squatting, and in excess of 20 times the body weight with jumping activities [25, 26]. In addition to the load applied to the joint, the actual stresses generated within the PFJ also depend on the surface areas of the patella and femur that may be in contact at any given moment [19]. Such high forces can easily result in loads that may exceed the safe load acceptance capacity of musculoskeletal tissues, leading to symptomatic damage and inducing a mosaic of pathophysiologic processes causing AKP [2, 15]. Further, patellofemoral overload could be secondary to inappropriate physiotherapy in some cases of AKP. Attempting to strengthen the quadriceps through open kinetic chain exercises will unacceptably overload the PFJ if the exercises are performed between 0 and 45 degrees of flexion [27]. Likewise, closed kinetic chain exercises performed between 45 and 90 degrees of flexion will also overload the PFJ [27]. Although there may be no obvious structural alteration, the PFJ can be overloaded and AKP can be triggered.
In some cases, PFJ overloading is secondary to structural anomalies, such as trochlear dysplasia [28]. Patients with AKP are more likely to have trochlear dysplasia compared to pain-free individuals [29]. Moreover, in patients with a trochlear bump (severe trochlear dysplasia) and AKP, both hydrostatic pressure and water content increase in the patella [30]. Such increases potentially provoke episodes of tissular ischemia and mechanical stimulation of nociceptors, which are both associated with pain [31]. Along these lines, Barton and colleagues [32] have demonstrated that the patella contains an intraosseous nerve network that is the densest in the medial and central portions of the patella and significantly sparser laterally. Moreover, growing evidence shows that in the subgroup of patients with patellofemoral chondral lesions, some of their pain is related to such lesions due to the overload of the richly innervated subchondral bone interface [31]. Such subchondral bone overload is secondary to damaged cartilage and the loss of its capacity as a shock absorber.
However, of all the structural factors that can cause an overload of the PFJ, the most powerful is the skeletal malalignment of the lower limb (limb alignment in the three planes), specifically torsional alterations (femoral anteversion and/or external tibial torsion) [33, 34]. With regard to malalignment, Albert van Kampen [35] has demonstrated that patellar tracking is highly susceptible to tibial rotations. Therefore, patellar tracking biomechanical studies must take tibial rotation into account. However, the classic PM theory does not take tibial and femoral torsion into consideration, which represents another weak point in the PM theory.
Limb alignment appears to very strongly influence the quadriceps vector [33, 34]. An abnormal quadriceps vector is an important contributor to AKP, and abnormal limb alignment is the underlying cause of the incorrect quadriceps vector [33, 34]. The direction of the quadriceps vector is likely more important than its magnitude [33, 34]. It should be noted that skeletal malalignment is not an abnormal Q-angle or an increased TT-TG distance, nor is it an increased tilt or increased shift of the patella. It instead involves the alignment of the limb in all three spatial planes—coronal, sagittal, and transverse. During a normal gait, the knee joint axis moves straight forward with minimal amounts of internal or external rotation, and the quadriceps force is directed posteriorly, compressing the patella into the trochlea. With abnormal limb torsion, the knee joint axis often moves forward in a manner that is oblique to the direction of motion. Such movement generates abnormal shear forces between the patella and the femur that will eventually cause tissue failure. If the force is not perfectly aligned, it can lead to an unbalanced distortion of the soft tissues surrounding the patella. It is very likely that one of the sources of AKP is in the peripatellar soft tissues due to the stress that the soft tissues undergo. However, we do not know the strain levels that must be reached to trigger the pain.
Some patients with torsional deformities have unilateral AKP, despite the deformity being symmetric. Why one side is symptomatic and the other is not remains an enigma. It is probable that most people limit their activity to avoid overuse or injury to the PFJ and thus AKP. Many of these patients are symptomatic only when they attempt an activity that causes increased loading; therefore, many select their activities based on what is comfortable. Once an injury (soft tissue lesion) or overuse (soft tissue strain) develops, quick recovery does not occur because of the underlying mechanical inefficiency. This situation may explain why disabling pain may occur on one side, while the opposite side remains asymptomatic. Moreover, the lack of symptoms on one side may be relative. In some cases, patients have asked for surgery on the asymptomatic side after the symptomatic side has been corrected because “they never knew what it was like to feel normal”.
In short, according to Robert A. Teitge, it is the excess of force in the PFJ that exceeds tissue homeostasis which is responsible for AKP. However, the problem is not a question of leaving the load acceptance envelope, but rather knowing what the envelope size limits are and why the excess force is excessive. If this is true, then the problem in diagnosing AKP is determining the source of the excess force. Robert A. Teitge puts forward a simile to understand the etiopathogenesis of AKP. To build a bridge, one must be knowledgeable of several factors. They include: (a) the required load limit, meaning the envelope; (b) the design of the bridge parts, which is the skeletal alignment; and (c) what materials the bridge is made of, connoting the response of those materials to the load. In the following sections, we will look at the biological response to a mechanical stimulus. The question we must ask ourselves is whether it is possible that all the neuroanatomical factors that we are going to discuss below are secondary to an excess of force. In other words, is the excess force the precipitating event? We do not have an answer to these questions.
5 Neuroanatomical Bases for AKP in the Young Patient: Neural Model
Sanchis-Alfonso and colleagues have developed the neural model as an explanation for the genesis of AKP in young patients [36]. The origin of AKP can be in the lateral retinaculum (LR), medial retinaculum, infrapatellar fat pad, synovium, or subchondral bone [37,38,39]. Studies by Sanchis-Alfonso and colleagues on AKP pathophysiology have mainly focused on the LR retrieved during patellofemoral realignment surgery in patients with a diagnosis of PM [40,41,42,43].
5.1 Morphologic Neural Changes in the Lateral Retinaculum
Some studies have implicated neural damage in the LR as a possible source of AKP in the young patient. In 1985, Fulkerson and colleagues described for the first time, nerve damage (demyelination and fibrosis) in the LR of patients with intractable patellofemoral pain requiring lateral retinacular release or realignment of the PFJ [44]. The changes in the retinacular nerves observed by these authors resembled the histopathologic picture of Morton's interdigital neuroma. Later, in 1991, Mori and colleagues found degenerative neuropathy in the LR in AKP patients [45].
Sanchis-Alfonso and colleagues have also observed nonspecific, chronic degenerative changes in nerve fibers, including myxoid degeneration of the endoneurium, retraction of the axonal component, and perineural fibrosis, in the LR in many cases (Fig. 4A) [42, 43]. Moreover, Sanchis-Alfonso and colleagues have found that a smaller group of specimens presented nerve fibers mimicking amputation neuromas seen elsewhere in the body (Fig. 4B) [42, 43]. A clear relationship has been demonstrated between the presence of neuromas and AKP; however, a similar relationship between neural myxoid degeneration and pain has not been found [43].

A Myxoid degeneration in the nerve fibers. No inflammatory cells are seen, B Microneuroma next to a rich vascular area (HE). (B-Reused with permission from SAGE. From: “Quantitative analysis of nerve changes in the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment” Am J Sports Med. 1998; 26:703–709)
Nerve damage occurs diffusely in the affected LR, and one must therefore consider the possibility of multiple neurologic sequelae in the peripatellar region. A possible consequence of such damage could be an altered proprioceptive innervation [43]. For example, Baker and colleagues observed an abnormal sense of the knee joint position (proprioception) in subjects with AKP [46]. Current research shows the importance of proprioceptive information from joint mechanoreceptors for proper knee function. Connective tissues, in addition to their mechanical function, play an important role in transmitting specific somatosensory afferent signals to the spinal and cerebral regulatory systems. Thus, the giving-way in AKP patients can be explained, at least in part, by the alteration or loss of joint afferent information with regard to proprioception due to nerve damage in the ascendant proprioception pathway or a decrease of healthy nerve fibers capable of transmitting proprioceptory stimuli. It seems likely that, to a certain degree, the instability of the PFJ in patients with AKP arises not only from mechanical factors but also neural factors [47, 48]. Such factors center on a proprioceptive deficit both in the sense of position and in the slowing or diminution of stabilizing and protective reflexes. In addition, Jensen and colleagues reported abnormal sensory function in the painful and nonpainful knee in some subjects with long-term unilateral AKP [49].
5.2 Hyperinnervation into the Lateral Retinaculum and AKP
Several studies have implicated hyperinnervation of the LR as a possible source of AKP in the young patient, with higher innervation in those with severe pain compared with those with moderate or mild pain [43]. Moreover, the LR of patients with pain as the predominant symptom has been shown to have a higher innervation pattern than the medial retinaculum or the LR of patients with patellar instability [43]. This nerve ingrowth consisted of myelinated and unmyelinated nerve fibers with a predominant nociceptive component (Fig. 5) [40].

A Free nerve endings immersed in the connective tissue, B Hot spot of free nerve endings forming a microneuroma, C Nerve endings entering the arterial wall. (Neurofilament NF). (Reused with permission from SAGE. From: “Immunohistochemical analysis for neural markers of the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment” Am J Sports Med. 2000; 28: 725–731)
The nociceptive properties of at least some of these nerves were shown by their substance P (SP) immunoreactivity (Fig. 6) [40]. SP, which is found in primary sensory neurons and C fibers (slow-chronic pain pathway), is involved in the neurotransmission pathways of nociceptive signals [50,51,52,53,54,55,56,57,58,59,60,61,62]. SP was detected in the axons of big nerve fibers, in free nerve endings, and in the vessel walls in some patients with pain as the predominant symptom [40]. Nociceptive fibers (i.e., neural fibers with intraaxonal SP) were fewer in number than NF fibers, indicating that not all the tiny perivascular or interstitial nerves were nociceptive [40]. Interestingly, the finding that SP fibers are more abundant in the LR than in its medial counterpart reinforces the role of the LR as the main source of pain in some AKP patients. Moreover, the number of these nociceptive fibers has been observed to be higher in patients experiencing pain as the main symptom relative to those with instability as the predominant symptom (with little or no pain between instability episodes) [40].

A Substance P, a marker of sensory fibers, is expressed in the nerve fibers in a granular pattern, B Neuromas are rich in nociceptive axons, as can be demonstrated studying substance P. (Reused with permission from SAGE. From: “Immunohistochemical analysis for neural markers of the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment” Am J Sports Med. 2000; 28: 725–731)
Nerve ingrowth, is mostly located within and around blood vessels (Fig. 7) [40, 43]. Thus, within the LR of AKP patients, S-100 positive fibers in the adventitia and within the muscular layer of medium and small arteries resemble a necklace. S-100 protein is a good marker of nerves because it permits identification of the Schwann cells in the myelinated parts of axons. Myelinated fibers typically lose their myelin sheath before they enter the muscular arterial wall, but this was found to not be the case in AKP patients. In a study of myelinated fibers by S-100 immunostaining, we were surprised by the identification of S-100-positive fibers within the muscular layer of medium and small arteries given that the myelin sheath was expected to be lost before the nerve entered the muscular arterial wall [43]. Vascular innervation has been demonstrated to be more prominent (94%) in patients with severe pain, whereas this type of hyperinnervation has been found in only 30% of the patients with light or moderate pain [42]. These findings are in agreement with the statement of Byers, who postulated in 1968 that pain in an osteoid osteoma could be generated and transmitted by vascular pressure-sensitive autonomic nerves [63]. In reviewing the literature, we have seen that hyperinnervation is also a factor implicated in the pathophysiology of pain in other orthopedic abnormalities, such as chronic back pain and jumper’s knee [54, 55, 64, 65]. On the other hand, pain has also been related with vascular innervation in some pathologies, as is the case in osteoid osteoma, in which an increase in perivascular innervations has been found in all the cases, leading the authors to postulate that pain was more closely related to this innervation than to the release of prostaglandin E2 [66]. Grönblad and colleagues have reported similar findings in the lumbar pain of facet syndrome [67]. Finally, Alfredson and colleagues related pain in Achilles tendinosis with vasculo-neural ingrowth [64].

Lateral retinaculum vessels are richly innervated in some of our patients. The myelinated innervation enters the muscular wall from the adventitial tissue, forming a necklace. (S-100). (Reused with permission from SAGE. From: “Quantitative analysis of nerve changes in the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment” Am J Sports Med. 1998; 26:703–709)
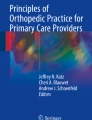
Hyperinnervation has been demonstrated to be associated with the release of neural growth factor (NGF), a polypeptide that stimulates axonogenesis [41]. NGF has two biologically active precursors: a long form with a molecular weight of approximately 34 kD and a short form of 27 kD [68]. The 34 kD precursor has been found in the LR of AKP patients [41]. Since some of the nerve fibers of the LR express NGF, these nerve fibers must still be in a proliferative phase. As expected, NGF expression is higher in PM patients with pain that in those with instability as the main symptom (Fig. 8) [41]. Gigante and colleagues [69] have also found NGF and TrkA (the NGF receptor) expression in the LR of patients with PM, but not in patients with jumper’s knee or meniscal tears. Interestingly, NGF is related not only to neural proliferation in vessels and perivascular tissue but also to the release of neuroceptive transmitters, such as SP [70].

Immunoblotting detection of NGF showing a thicker band in cases with AKP (4,5,6,7) compared with cases of instability without pain (1,2,3)
In short, in symptomatic PM patients with pain as the main symptom, there are detectable levels of NGF that cause hyperinnervation and stimulate SP release, whereas in patients with instability as the predominant symptom, there are lower levels of local NGF release, less neural proliferation, and less nociceptive stimulus [41]. Consequently, there must be some factors acting on a PM that make the patient has pain or instability as the main symptom. PM may in fact not have anything to do with the presence of pain. In other words, symptoms appear to be related to multiple factors with variable clinical expression, and our imperfect understanding of these factors may explain the all-too-frequent failure to achieve adequate symptom relief with the use of realignment procedures. The question is, what are the mechanisms that stimulate NGF release in these patients? We hypothesize that periodic short episodes of ischemia could be the primary mechanism of NGF release and hyperinnervation, and therefore could be implicated in pain, at least in a subgroup of AKP patients.
5.3 Role of Ischemia in the Genesis of AKP: Loss of Vascular Homeostasis
Despite numerous publications on AKP, the mechanism underlying the pain is controversial. The loss of vascular homeostasis has been proposed as an intrinsic pain mechanism in a subgroup of AKP patients.
5.3.1 Basic Science
According to some authors, ischemia can induce NGF synthesis [70,71,72]. Moreover, NGF has been shown to stimulate neural sprouting and hasten neural proliferation in blood vessel walls [73, 74], which is the same pattern of hyperinnervation that is seen in the LR of some AKP patients [40, 42, 43]. Similar changes have been studied in animal models and are present in the coronary innervation of patients with myocardial infarcts and brain ischemia [71, 72, 74]. Thus, short episodes of tissular ischemia due to vascular torsion or vascular bending have been hypothesized as the main problem in painful patellofemoral imbalance [40, 42]. Vascular bending could be induced mechanically by medial traction over the retracted LR with knee flexion [38].
Sanchis-Alfonso and colleagues have demonstrated histologic retinacular changes associated with hypoxia in painful PM [42]. They have found lesions that can lead to tissular anoxia, such as arterial vessels with obliterated lumina and thick muscular walls, and other lesions that can arise from ischemia, such as infarcted foci of the connective tissue, myxoid stromal degeneration, and ultrastructural findings related with anoxia (degenerated fibroblasts with autophagic intracytoplasmic vacuoles, endothelial cells with reduplication of the basal lamina, young vessels with endothelial cells containing active nuclei and conspicuous nucleoli, and neural sprouting) (Fig. 9) [75].

A Arterial vessel in the retinacular tissue can show a prominent and irregular endothelium and thick muscular walls or even an irregular reduction of the vascular lumen. (Hematoxylin–Eosin stain). B Infarcted foci in the connective tissue showing a degenerative pattern of the collagen fibers, with loss of the fibrillar component and accumulation of myxoid material in the interstitium, (Masson’s Trichrome stain). C Myxoid stromal degeneration in the middle of the fibrous retinacular tissue (Hematoxylin–Eosin stain). D Degenerative changes in fibroblasts (increased autophagic vacuoles—asterisk–) secondary to hypoxia (TEM). E Young vessels with endothelial cells containing active nuclei and conspicuous nucleoli. F Neural sprouting is detected ultrastructurally as a bunch of tiny axons immersed in the Schwann cell cytoplasm. G Neural sprouting detail
Another phenomenon related to ischemia is angiogenesis. Chronic ischemia leads to release of vascular endothelial growth factor (VEGF), a potent hypoxia-inducible angiogenic factor that causes hypervascularization [76]. This hypervascularization creates blood vessels to supply the nutrient needs of the tissue. Sanchis-Alfonso and colleagues have performed a quantitative analysis of vascularization in the LR excised during surgical patellofemoral realignments, using a pan-vascular marker, anti-Factor VIII-related antigen [42]. They have found an increase in the number of blood vessels in the LR of patients with painful PM, with the severe pain group having greater numbers compared with those of moderate or mild pain group [42]. Moreover, as expected, they found a positive linear correlation between the number of blood vessels and number of nerves [42]. Tissular ischemia induces VEGF release by fibroblasts, synovial cells, mast cells, or even endothelial cells [77,78,79,80]. Based on these principles, Sanchis-Alfonso and colleagues performed a study of VEGF expression in the LR of patients with PM, using immunohistochemistry and immunoblot analysis [42]. VEGF release begins 8 h after hypoxia, and the peptide disappears in 24 h if the ischemic crisis has ended [42]. Therefore, VEGF positivity reflects the presence of an ischemic process, or better said, 8–24 h has elapsed since the onset of the transitory ischemic episode. However, given that the average duration of VEGF is very short, its absence has no significance regarding whether a transitory ischemic process is occurring. Although this process has been well documented in joints affected by rheumatoid arthritis and osteoarthritis [79,80,81], it has never been documented in AKP until the study by Sanchis-Alfonso and colleagues [42]. They have shown VEGF production in stromal fibroblasts, vessel walls, certain endothelial cells, and even nerve fibers, including similar levels in axons as in perineurium (Fig. 10) [42]. Their immunohistochemical findings were confirmed by immunoblot analysis. VEGF levels were higher in patients with severe pain than in those with mild to moderate pain; the protein was barely detectable in two cases with mild pain (Fig. 11) [42]. VEGF expression is absent in normal joints, although inflammatory processes can stimulate its release [81, 82]. In such cases, synovial hypoxia secondary to articular inflammation is assumed to trigger VEGF production [82]. However, inflammatory changes have not been observed in the LR of AKP patients [42, 43]. Furthermore, peripheral nervous system hypoxia has been reported to be able to simultaneously trigger VEGF and NGF synthesis via neurons [83], or inflammatory or stromal cells [71, 72]. VEGF induces hypervascularization, and NGF induces hyperinnervation. Both occurrences have been observed in AKP patients [42, 43]. In conclusion, ischemia could be the main trigger for pain in at least a subgroup of AKP patients.

A VEGF, the factor promoting vascular proliferation, is present in smalls vessels (wall and endothelium) and in perivascular fibroblasts. B Some cases have VEGF expression in the perineural shift and inside the axons (VEGF)

Immunoblotting detection of VEGF showing a thicker band in cases with severe AKP (2,3,10) compared with cases with moderate pain (1,5,8) or light pain (4,6,7,9)
5.3.2 Clinical Studies
The role of vascular insufficiency in AKP has not been studied extensively from a clinical point of view. In fact, only a few clinical papers have alluded to the possibility of hypoxia as a factor in the pathogenesis of AKP.
Sandow and Goodfellow [84] investigated the natural history of AKP in adolescents. In a study sample of 54 adolescent girls, the researchers observed that 9 out of 54 (16.7%) had pain that was aggravated by cold weather. According to Selfe and colleagues [85] the proximal part of the rete patellae is very superficial and is therefore vulnerable to thermal environmental stress, resulting in greater hypoxia during cold weather. More recently, Selfe and colleagues [86] studied clinical outcomes in a sample of AKP patients categorized as hypoxic, that is to say, with “cold knees” (his or her legs felt cold even in warm surroundings). Fourteen out of 77 (18.2%) of the patients were categorized as “cold sufferers,” a percentage very similar to that reported by Sandow and Goodfellow [84]. Selfe and colleagues [86] studied local hypothermia by means of infrared thermography and concluded that patients categorized as hypoxic reported greater pain levels and had poorer response to an exercise-based treatment than non-hypoxic patients. Gelfer and colleagues [87], using single photon emission computed tomography (SPECT), also found a relationship between transient patellar ischemia after total knee replacement and the clinical symptoms of AKP. Similarly, using photoplethysmography, which is a reliable technique for estimating blood flow in bone tissue, Naslund also observed that an ischemic mechanism (decreased blood flow in the patellar bone) is involved in the pathogenesis of AKP [88]. Moreover, in half of the AKP studied patients, Naslund observed accelerated bone remodeling in bony compartments of the knee joint, which may have been due to a dysfunctioning sympathetic nervous system and caused intermittent ischemia and pain. Selfe and colleagues [85] classified AKP patients into three groups: hypoxic, inflammatory, and mechanical. However, ischemia may be the pain-provoking factor in all three groups, given that inflammatory changes can develop not only after ischemia but also after mechanical damage to the vascular system. Ischemia could be caused by higher intraosseous pressure, redundant axial loading, or decreased arterial blood flow.
6 The Role of the Peripheral and/or Central Nervous System in the Pathophysiology of AKP—“Central Sensitization”—“The Neuromatrix Model”
AKP is a paradigm of chronic pain. Chronic pain is a multidimensional phenomenon composed of sensitive, cognitive-evaluative and affective-motivational domains. The central nervous system, both the brain and spinal cord, is where pain is produced and modulated. Several brain and spinal cord areas work together (the pain neuromatrix) in response to corporal stimuli to create the multidimensional experience of pain. Interestingly, Damasio and colleagues [89] observed an overlap between the cerebral activity areas related to chronic pain and those related to cognition and emotions. This finding suggests that chronic pain, cognition, and emotions are interrelated. Moreover, it has been shown that AKP is not only related to structural anomalies but also to altered central neural processes along with alterations in central nociceptive processing [90, 91]. Slutsky-Ganesh and colleagues [92] indicate that the posterior cerebellum could be a key modulator in cognitive assessment of pain in patellofemoral pain across the cortico-cerebellar loops, possibly leading to consequences on motor function downstream.
As we will see in chapter “Evaluation of Psychological Factors Affecting Anterior Knee Pain Patients: The Implications for Clinicians Who Treat these Patients”, AKP patients have a high incidence of anxiety, depression, kinesiophobia (the belief that movement will create additional injury or re-injury and pain) and catastrophizing (the belief that pain will worsen, and one is helpless to deal with it) [93,94,95]. Psychological factors play an important role as pain modulators. Even in cases with clear structural findings that justify pain, psychological factors influence and modify pain sensation as well as subsequent impairment. Therefore, they can be barriers to recovery after the appropriate surgical treatment. Catastrophizing is not only responsible for the chronification of pain due to a psychological mechanism but may also influence the neurophysiology of pain modulation. In a functional MRI study of patients with chronic pain, Gracely and colleagues [96] showed that catastrophizing ideas were associated with a higher degree of brain activity not only in the pain regions but also in the cortical regions associated with attention, anticipation of pain and emotional aspects of pain. Catastrophizing may play a role as a facilitator of the pain perception process. It also has been suggested that pain catastrophizing interfere with descending pain-inhibitory systems and may facilitate neuroplastic changes in the spinal cord during repeated painful stimulation, thereby promoting sensitization in the central nervous system.
Impaired “conditioned pain modulation,” defined as the endogenous pain inhibition ability of a subject, has been demonstrated in young women with long-standing AKP [97]. Central sensitization (CS) has been defined by the International Association for the Study of Pain (IASP) as “increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold input” [98]. In other words, there is ineffective pain modulation-inhibition in the central nervous system. That is to say, there is a process of amplification of the afferent signal that arrives from the periphery. For all that, the malfunctioning of the descending pain-inhibiting mechanisms is another of the mechanisms involved in CS. From a clinical standpoint, we can suspect that there is CS when the patient presents with allodynia or hyperalgesia. A significant number AKP patients present more signs of CS when compared to healthy pain-free individuals. Interestingly, it has been demonstrated that pain sensitization may be amenable to treatment through exercises, pharmacological therapy, and surgery [99]. In AKP patients, there is “central sensitization,” meaning an increased responsiveness of the central nervous system to a variety of stimuli [100,101,102]. Rathleff and colleagues [101] suggested that adolescent females with AKP have both localized and distal hyperalgesia (a reduced pressure pain threshold), which can be determined through pressure algometry. This hyperalgesia may signal altered central processing of nociceptive information.
Jensen and colleagues [49] have shown that some patients with unilateral AKP have neuropathic pain, which suggests damage in the peripheral and/or central nervous system that causes pain signals without a specific cause. In this way, many AKP patients have alterations in the central nervous system that might play an important role both in the magnitude and persistence of pain after suitable conservative or surgical treatment. Lefaucheur and colleagues [103] found a link between chronic neuropathic pain and motor cortex disinhibition. The current data suggest that repetitive transcranial magnetic stimulation of the motor cortex corresponding to the patient’s site of pain may be a complementary treatment modality for patients with chronic neuropathic AKP [104]. Motor cortex stimulation may produce analgesic effects by restoring missing or impaired intracortical inhibitory processes [103].
As we can see in chapter “Brain Network Functional Connectivity Clinical Relevance and Predictive Diagnostic Models in Anterior Knee Pain Patients”, AKP patients have brain functional connectivity changes compared to healthy controls. That is especially the case between the brain areas involved in cognitive stimulus processing and the regions involved in pain modulation. This widespread impact on overall brain function could play an important role in explaining the magnitude, experience and persistence of pain after suitable conservative or surgical treatment.
7 Authors’ Proposed AKP Pathophysiology
A subgroup of patients with AKP have a skeletal malalignment of the limb, especially in the transverse plane (femoral and/or tibial rotational malalignment) [33, 34]. This malalignment of the lower limb could provoke pain due to the abnormal stress on tissue which is not of sufficient magnitude or direction to result in instability. It is likely that nerve changes or ischemia may be due to chronic repetitive stretch of soft tissue (retinaculum). Moreover, skeletal malalignment could provoke patellofemoral instability due to a failure of the ligaments that stabilize the PFJ, and it will also lead to the development of patellofemoral cartilage lesions due to the increased patellofemoral compression forces (Fig. 12). However, in most cases, the abnormal femoral rotation is functional due to a deficit of the proximal control [105]. This situation will lead to a patellofemoral imbalance as it occurs in the structural skeletal malalignment of the lower limb.

Pathways to pain in patients with torsional abnormalities. Force out of balance is the culprit, and force out of the balance is due to the limb out of alignment
We hypothesize that short and repetitive episodes of tissular ischemia, potentially due vascular torsion or vascular bending induced by a patellofemoral imbalance, could trigger release of NGF and VEGF in the peripatellar soft tissues. Once NGF is present in the tissues, it induces hyperinnervation, attracts mastocytes, and triggers substance P release by free nerve endings (Fig. 13) [70]. In addition, VEGF induces hypervascularization and plays a role in increasing neural proliferation.

Pathophysiology of AKP
Free nerve endings, slowly adapting receptors that mediate nociception, are activated in response to deformation of tissues. In the knee, such deformation results from abnormal tensile and compressive forces generated during flexo-extension of the joint or in response to chemical agents such as histamine, bradykinin, prostaglandins, and leukotrienes [57, 106, 107]. Therefore, SP is released from peripheral endings of nociceptive afferents as a result of noxious chemical or mechanical stimulation. The nociceptive information relayed by these free nerve endings is responsible, at least in part, for the pain.
Once SP is liberated in the connective tissue, it induces the release of prostaglandin E2, one of the biochemical agents known to stimulate nociceptors (Fig. 13) [50]. The activation of nociceptive pathways by prostaglandins could be one of the many mechanisms involved in the transmission of pain in AKP patients. Moreover, SP stimulates mast cells, facilitating a degranulation process that can liberate histamine, another non-neurogenic pain mediator (Fig. 14) [56]. Numerous mast cells have been identified in the LR of AKP patients [19]. Mast cells are also associated with the release of NGF [40, 108], contributing to the hyperinnervation and indirectly provoking more pain. Furthermore, SP has been shown to induce the release of collagenase, interleukin-1, and tumor necrosis factor-alpha (TNF-α) from synoviocytes, fibroblasts, and macrophages [50, 52]. These factors could contribute to the genesis of patellar instability through degradation of soft tissues. SP, NGF and mast cells have also recently been implicated in bone resorption in both in vitro and in vivo experiments, which could explain, at least in part, the osteoporosis found in many cases of AKP [109]. Finally, SP and VEGF stimulate endothelial cell proliferation and migration [53], which are essential to the development of a new vascular network that may promote tissue repair, but indirectly maintain a vicious cycle.

Mast cells are abundant in the stroma (arrow), mainly in a perivascular disposition. Some of them show a degranulation process (activated mast cells) (A), (Giemsa stain). Ultrastructural image of a mast cell of the lateral retinaculum with its cytoplasm full of chemotactic granules, (TEM) (B). (A)-(Reused with permission from SAGE. From: “Immunohistochemical analysis for neural markers of the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment” Am J Sports Med. 2000; 28: 725–731)
Woolf [110] described four types of pain from a clinical point of view: (1) nociceptive pain, which is transient pain in response to noxious stimulus; (2) homeostatic pain, which is pain that promotes the healing of injured tissue (i.e., the cascade of events toward re-establishing homeostasis); (3) neuropathic pain, which is spontaneous pain and hypersensitivity to stimulus in association with damage to the nervous system; and (4) functional pain, which is pain resulting from abnormal central processing of normal input. All these mechanisms appear to be involved in the pathophysiology of pain in AKP patients.
8 Take Home Messagess
-
Currently, much remains to be learned about the cause of AKP. Our understanding is limited. AKP is one of the most intriguing orthopedic pathologies from a clinical point of view.
-
AKP obliges us to “think out of the box”, to look deeper into the anatomy, biomechanics, biology, anatomic pathology, physiopathology, and psychology. AKP is a great stimulus for orthopedic intellectual development.
-
Chondromalacia patellae is not synonymous with AKP. It is not the underlying problem.
-
Very often, patellofemoral malalignment (patellar tilt/lateral patellar subluxation) is not the problem.
-
In a subgroup of AKP patients, skeletal malalignment of the limb is responsible for disabling AKP due to both patellofemoral overload and patellofemoral imbalance. Understanding the biomechanics is crucial—orthopedic surgery is very much a mechanical engineering discipline. At this time, from the biomechanical viewpoint, the most powerful treatment effect in treating AKP comes from limb re-alignment.
-
In the vast majority of AKP cases, the loss of both soft tissue (peripatellar synovitis and others soft tissue impingements such as synovial hypertrophy around the inferior pole of the patella) and osseous (intraosseous edema, osseous hypertension) homeostasis is more important in the genesis of AKP than local structural anomalies (patellar till, lateral patellar displacement, and patellofemoral chondropathy). However, we do not know how often is AKP present in a structurally perfect limb, except for overtraining. It is likely that the loss of homeostasis can be mechanical with an as yet unrecognized structural anomaly.
-
There is a neuroanatomical basis for AKP in the young patient. A dysfunction of the peripheral and/or the central nervous system may cause neuropathic pain in some individuals with AKP.
-
Periodic short episodes of ischemia, secondary to a mechanical stimulus, could be implicated in the pathogenesis of AKP by triggering neural proliferation of nociceptive axons (SP-positive nerves), mainly in a perivascular location. These findings are in line with the homeostasis perspective. Loss of vascular homeostasis in the knee region (e.g., hypervascularity, ischemia, osseous hypertension) may be associated with AKP.
-
It is possible that all of the neuroanatomical factors involved in the genesis of AKP and the loss of vascular homeostasis are due to an excess of force that would be the precipitating event.
-
Chronic pain is a multidimensional phenomenon composed by sensitive, cognitive-evaluative and affective-motivational domains. The neuromatrix model can explain the multidimensional pain experience in AKP patients.
9 Key Message
-
We hypothesize that it is the force (magnitude or direction) which determines whether one is in or out of Dye’s envelope. In short, the diagnostic challenge is determining the source of excess force which overcomes tissue homeostasis. We are a long way from determining why excess force is excess.
References
Büdinger K. Üeber ablösung von gelenkteilen und verwandte prozesse. Dtsch Z Chir. 1906;84:311–65.
Dye SF. The pathophysiology of patellofemoral pain: a tissue homeostasis perspective. Clin Orthop Relat Res. 2005;436:100–10.
Royle SG, Noble J, Davies DR, et al. The significance of chondromalacic changes on the patella. Arthroscopy. 1991;7:158–60.
Ficat P, Ficat C, Bailleux A. Syndrome d’hyperpression externe de la rotule (S.H.P.E). Rev Chir Orthop. 1975;61:39–59.
Ficat P, Hungerford DS. Disorders of the Patello-Femoral Joint. Baltimore: Williams & Wilkins; 1977.
Hughston JC. Subluxation of the patella. J Bone Joint Surg. 1968;50–A:1003–1026.
Insall J. “Chondromalacia Patellae”: Patellar malalignment syndrome. Orthop Clin North Am. 1979;10:117–27.
Merchant AC, Mercer RL. Lateral release of the patella: a preliminary report. Clin Orthop Relat Res. 1974;103:40.
Staeubli HU, Bosshard C, Porcellini P, et al. Magnetic resonance imaging for articular cartilage: cartilage-bone mismatch. Clin Sports Med. 2002;21:417–33.
James SL. Chondromalacia of the Patella in the adolescent. In: Kennedy JC. editor. The injured adolescent knee. Baltimore: The Williams & Wilkins Company, 1979.
Orthopaedic Knowledge Update 3 Home Study Syllabus Published by American Academy of Orthopaedic Surgeons, Park Ridge, Illinois, January 1990, pp 563–567.
Meister K, James SL. Proximal tibial derotation osteotomy for anterior knee pain in the miserably malaligned extremity. Am J Orthop (Belle Mead NJ). 1995;24:149–55.
Cooke TD, Price N, Fisher B, et al. The inwardly pointing knee. An unrecognized problem of external rotational malalignment. Clin Orthop Relat Res. 1990;56–60.
Dye SF. The knee as a biologic transmission with an envelope of function: a theory. Clin Orthop Relat Res. 1996;325:10–8.
Dye SF, Staubli HU, Biedert RM, et al. The mosaic of pathophysiology causing patellofemoral pain: therapeutic implications. Oper Techni Sports Med. 1999;7:46–54.
Powers CM, Ward SR, Fredericson M, et al. Patellofemoral kinematics during weightbearing and non-weightbearing knee extension in persons with patellar subluxation: a preliminary study. J Orthop Sports Phys Ther. 2003;33:677–85.
Souza RB, Draper CE, Fredericson M, et al. Femur rotation and patellofemoral joint kinematics: a weight-bearing MRI analysis. J Orthop Sports Phys Ther. 2010;40:277–85.
Lee TQ, Morris G, Csintalan RP. The influence of tibial and femoral rotation on patellofemoral contact area and pressure. J Orthop Sports Phys Ther. 2003;33:686–93.
Sanchis-Alfonso V. Anterior Knee Pain and Patellar Instability. London: Springer; 2011.
Sanchis-Alfonso V, Gastaldi-Orquín E, Martinez-SanJuan V. Usefulness of computed tomography in evaluating the patellofemoral joint before and after Insall’s realignment. Correlation with short-term clinical results. Am J Knee Surg. 1994;7:65–72.
Sanchis-Alfonso V, Roselló-Sastre E, Martinez-SanJuan V. Pathogenesis of anterior knee pain syndrome and functional patellofemoral instability in the active young. A review Am J Knee Surg. 1999;12:29–40.
Dye SF. Functional anatomy and biomechanics of the patellofemoral joint. In: Scott WN, editor. The Knee. St. Louis: Mosby; 1994. p. 381–9.
Dye SF. Forward. In Fulkerson JP. Disorders of the Patellofemoral Joint. Ed 4. Philadelphia, Lippincott Williams and Wilkins xi–xii, 2004.
Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop. 1979;144:9–15.
Reilly DT, Martens M. Experimental analysis of the quadriceps muscle force and patellofemoral joint reaction force for various activities. Acta Orthop Scand. 1972;73:146–137.
Smith AJ. Estimates of muscle and joint force at the knee and ankle during jumping activities. J Hum Movement Stud. 1975;1:78–86.
Steinkamp LA, Dillinghan MF, Markel MD, et al. Biomechanical considerations in patellofemoral joint rehabilitation. Am J Sports Med. 1993;21:438–44.
Van Haver A, De Roo K, De Beule M, et al. The effect of trochlear dysplasia on patellofemoral biomechanics: a cadaveric study with simulated trochlear deformities. Am J Sports Med. 2015;43(6):1354–61.
Powers CM. Patellar kinematics, part II: the influence of the depth of the trochlear groove in subjects with and without patellofemoral pain. Phys Ther. 2000;80(10):965–78.
Ho KY, Hu HH, Colletti PM, et al. Recreational runners with patellofemoral pain exhibit elevated patella water content. Magn Reson Imaging. 2014;32(7):965–8.
Sanchis-Alfonso V. Holistic approach to understanding anterior knee pain. Clinical implications. Knee Surg Sports Traumatol Arthrosc. 2014;22(10):2275–2285.
Barton RS, Ostrowski ML, Anderson TD, et al. Intraosseous innervation of the human patella: a histologic study. Am J Sports Med. 2007;35:307–11.
Teitge RA. Patellofemoral syndrome a paradigm for current surgical strategies. Orthop Clin N Am. 2008;287–311.
Teitge RA. Does lower limb torsion matter? Tech Knee Surg. 2012;11:137–46.
van Kampen A, Huiskes R. The three-dimensional tracking pattern of the human patella. J Orthop Res. 1990;8(3):372–82.
Sanchis-Alfonso V, Roselló-Sastre E. Anterior knee pain in the young patient—what causes the pain? “Neural model.” Acta Orthop Scand. 2003;74:697–703.
Biedert RM, Sanchis-Alfonso V. Sources of anterior knee pain. Clin Sports Med. 2002;21:335–47.
Fulkerson JP. The etiology of patellofemoral pain in young active patients: a prospective study. Clin Orthop Relat Res. 1983;179:129–33.
Kasim N, Fulkerson JP. Resection of clinically localized segments of painful retinaculum in the treatment of selected patients with anterior knee pain. Am J Sports Med. 2000;28:811–4.
Sanchis-Alfonso V, Roselló-Sastre E. Immunohistochemical analysis for neural markers of the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment. A neuroanatomic basis for anterior knee pain in the active young patient. Am J Sports Med. 2000;28:725–731.
Sanchis-Alfonso V, Roselló-Sastre E, Revert F. Neural growth factor expression in the lateral retinaculum in painful patellofemoral malalignment. Acta Orthop Scand. 2001;72:146–9.
Sanchis-Alfonso V, Roselló-Sastre E, Revert F, et al. Histologic retinacular changes associated with ischemia in painful patellofemoral malalignment. Orthopedics. 2005;28:593–9.
Sanchis-Alfonso V, Roselló-Sastre E, Monteagudo-Castro C, et al. Quantitative analysis of nerve changes in the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment. A preliminary study. Am J Sports Med. 1998;26:703–709.
Fulkerson JP, Tennant R, Jaivin JS, et al. Histologic evidence of retinacular nerve injury associated with patellofemoral malalignment. Clin Orthopn Relat Res. 1985;197:196–205.
Mori Y, Fujimoto A, Okumo H, et al. Lateral retinaculum release in adolescent patellofemoral disorders: its relationship to peripheral nerve injury in the lateral retinaculum. Bull Hosp Jt Dis Orthop Inst. 1991;51:218–29.
Baker V, Bennell K, Stillman B, et al. Abnormal knee joint position sense in individuals with patellofemoral pain syndrome. J Orthop Res. 2002;20(2):208–14.
Jerosch J, Prymka M. Knee joint propioception in patients with posttraumatic recurrent patella dislocation. Knee Surg, Sports Traumatol Arthrosc. 1996;4:14–8.
Wilson AS, Lee HB. Hypothesis relevant to defective position sense in a damaged knee. J Neurol Neurosurg Psychiatry. 1986;49:1462–3.
Jensen R, Hystad T, Kvale A, et al. Quantitative sensory testing of patients with long lasting patellofemoral pain síndrome. Eur J Pain. 2007;11:665–76.
Ahmed M, Bergstrom J, Lundblad H, et al. Sensory nerves in the interface membrane of aseptic loose hip prostheses. J Bone Joint Surg. 1998;80-B:151–155.
Ashton IK, Ashton BA, Gibson SJ, et al. Morphological basis for back pain: the demonstration of nerve fibers and neuropeptides in the lumbar facet joint capsule but not in ligamentum flavum. J Orthop Res. 1992;10:72–8.
Ashton IK, Roberts S, Jaffray DC. Neuropeptides in the human intervertebral disc. J Orthop Res. 1994;12:186–92.
Ashton IK, Walsh DA, Polak JM, et al. Substance P in intervertebral discs. Binding sites on vascular endothelium of the human annulus fibrosus. Acta Orthop Scand. 1994;65:635–639.
Coppes MH, Marani E, Thomeer RT, et al. Innervation of “painful” lumbar discs. Spine. 1997;22:2342–9.
Freemont AJ, Peacock TE, Goupille P, et al. Nerve ingrowth into diseased intervertebral disc in chronic back pain. Lancet. 1997;350:178–81.
Grönblad M, Korkala O, Konttinen YT, et al. Silver impregnation and immunohistochemical study of nerves in lumbar facet joint plical tissue. Spine. 1991;16:34–8.
Kocher MS, Fu FH, Harner ChD. Neuropathophysiology. In: Fu FH, Harner ChD, Vince KG, editors. Knee Surgery. Baltimore: Williams and Wilkins; 1994. p. 231–49.
Konttinen YT, Grönblad M, Antti-Poika I, et al. Neuroimmunohistochemical analysis of peridiscal nociceptive neural elements. Spine. 1990;15:383–6.
Korkala O, Grönblad M, Liesi P, et al. Immunohistochemical demonstration of nociceptors in the ligamentous structures of the lumbar spine. Spine. 1985;10:156–7.
Palmgren T, Grönblad M, Virri J, et al. Immunohistochemical demonstration of sensory and autonomic nerve terminals in herniated lumbar disc tissue. Spine. 1996;21:1301–6.
Witonski D, Wagrowska-Danielewicz M. Distribution of substance-P nerve fibers in the knee joint in patients with anterior knee pain syndrome. Knee Surg Sports Traumatol Arthrosc. 1999;7:177–83.
Wojtys EM, Beaman DN, Glover RA, et al. Innervation of the human knee joint by substance-P fibers. Arthroscopy. 1990;6:254–63.
Byers PD. Solitary benign osteoblastic lesions of bone. Osteoid osteoma and benign osteoblastoma Cancer. 1968;22:43–57.
Alfredson H, Ohberg L, Forsgren S. Is vasculo-neural ingrowth the cause of pain in chronic Achilles tendinosis? An investigation using ultrasonography and colour Doppler, immunohistochemistry, and diagnostic injections. Knee Surg Sports Traumatol Arthrosc. 2003;11:334–8.
Sanchis-Alfonso V, Roselló-Sastre E, Subías-López A. Neuroanatomic basis for pain in patellar tendinosis (“jumper’s knee”): A neuroimmunohistochemical study. Am J Knee Surg. 2001;14:174–7.
Hasegawa T, Hirose T, Sakamoto R, et al. Mechanism of pain in osteoid osteomas: an immunohistochemical study. Histopathology. 1993;22:487–91.
Grönblad M, Weinstein JN, Santavirta S. Immunohistochemical observations on spinal tissue innervation. A review of hipothetical mechanisms of back pain. Acta Orthop Scand. 1991;62:614–622.
Dicou E, Pflug B, Magazin M, et al. Two peptides derived from the nerve growth factor precursor are biologically active. J Cell Biol. 1997;136:389–98.
Gigante A, Bevilacqua C, Ricevuto A, et al. Biological aspects in patello-femoral malalignment. 11th Congress European Society of Sports Traumatology, Knee Surgery and Arthroscopy. Book of Abstracts. Athens 5–8 May, 2004.
Malcangio M, Garrett NE, Cruwys S, et al. Nerve growth factor- and neurotrophin-3-induced changes in nociceptive threshold and the release of substance P from the rat isolated spinal cord. J Neurosci. 1997;17:8459–67.
Abe T, Morgan DA, Gutterman DD. Protective role of nerve growth factor against postischemic dysfunction of sympathetic coronary innervation. Circulation. 1997;95:213–20.
Lee TH, Kato H, Kogure K, et al. Temporal profile of nerve growth factor-like immunoreactivity after transient focal cerebral ischemia in rats. Brain Res. 1996;713:199–210.
Isaacson LG, Crutcher KA. The duration of sprouted cerebrovascular axons following intracranial infusion of nerve growth factor. Exp Neurol. 1995;13:174–9.
Kawaja MD. Sympathetic and sensory innervation of the extracerebral vasculature: roles for p75NTR neuronal expression and nerve growth factor. J Neurosci Res. 1998;52:295–306.
Society for Ultrastructural Pathology. Handbook of diagnostic electron microscopy for pathologists-in-training. New York-Tokyo: Igaku-Shoin Medical Publishers Committee; 1995.
Shweiki D, Itin A, Soffer D, et al. Vascular endothelial growth factor induced by hypoxia may mediate hypoxia-initiated angiogenesis. Nature. 1992;359:843–5.
Liu Y, Cox SR, Morita T, et al. Hypoxia regulates vascular endothelial growth factor gene expression in endothelial cells. Identification of a 5’ enhancer. Circ Res. 1995:77:638–643.
Minchenko A, Bauer T, Salceda S, et al. Hypoxic stimulation of vascular endothelial growth factor expression in vitro and in vivo. Lab Invest. 1994;71:374–9.
Nagashima M, Yoshino S, Ishiwata T, et al. Role of vascular endothelial growth factor in angiogenesis of rheumatoid arthritis. J Rheumatol. 1995;22:1624–30.
Yamada T, Sawatsubashi M, Yakushiji H, et al. Localization of vascular endothelial growth factor in synovial membrane mast cells: examination with “multilabelling subtraction immunostaining.” Virchows Arch. 1998;433:567–70.
Pufe T, Petersen W, Tillmann B, et al. The splice variants VEGF121 and VEGF189 of the angiogenic peptide vascular endothelial growth factor are expressed in osteoarthritic cartilage. Arthritis Rheum. 2001;44:1082–8.
Jackson JR, Minton JAL, Ho ML, et al. Expression of vascular endothelial growth factor in synovial fibroblasts is induced by hipoxia and interleukin 1ß. J Rheumatol. 1997;24:1253–9.
Calzà L, Giardino L, Giuliani A, et al. Nerve growth factor control of neuronal expression of angiogenetic and vasoactive factors. Proc Natl Acad Sci USA. 2001;98:4160–5.
Sandow MJ, Goodfellow JW. The natural history of anterior knee pain in adolescents. J Bone Joint Surg. 1985;67-B:36–38.
Selfe J, Karki A, Stevens D. A review of the role of circulatory deficit in the genesis of patellofemoral pain. Phys Therapy Rev. 2002;7:169–72.
Selfe J, Harper L, Pedersen I, et al. Cold legs: a potential indicator of negative outcome in the rehabilitation of patients with patellofemoral pain syndrome. Knee. 2003;10:139–43.
Gelfer Y, Pinkas L, Horne T, et al. Symptomatic transient patellar ischemia following total knee replacement as detected by scintigraphy. A prospective, randomized, double-blind study comparing the mid-vastus to the medial para-patellar approach. Knee. 2003;10:341–345.
Naslund J. Patellofemoral pain syndrome. Clinical and pathophysiological considerations. Thesis. Karolinska Institutet, Stockholm, 2006.
Damasio AR, Grabowky TJ, Bechara A, et al. Subcortical and cortical brain activity during the feeling of self-generated emotions. Nat Neurosci. 2000;3:1049–56.
Diekfuss JA, Grooms DR, Nissen KS, et al. Does central nervous system dysfunction underlie patellofemoral pain in young females? Examining brain functional connectivity in association with patient-reported outcomes. J Orthop Res. 2022;40(5):1083–96.
Foss KDB, Slutsky-Ganesh AB, Diekfuss JA, et al. Brain activity during experimental knee pain and its relationship with kinesiophobia in patients with patellofemoral pain: a preliminary functional magnetic resonance imaging investigation. J Sport Rehabil. 2022;12:1–10. https://doi.org/10.1123/jsr.2021-0236.
Slutsky-Ganesh AB, Diekfuss JA, Grooms DR, et al. A preliminary investigation of the effects of patellar displacement on brain activation and perceived pain in young females with patellofemoral pain. J Sci Med Sport. 2022;31;S1440–2440(22)00030–5. https://doi.org/10.1016/j.jsams.2022.01.006.
Domenech J, Sanchis-Alfonso V, López L, et al. Influence of kinesiophobia and catastrophizing on pain and disability in anterior knee pain patients. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1562–8.
Doménech J, Sanchis-Alfonso V, Espejo B. Changes in catastrophizing and kinesiophobia are predictive of changes in disability and pain after treatment in patients with anterior knee pain. Knee Surg Sports Traumatol Arthrosc. 2014;22(10):2295–300.
Sanchis-Alfonso V, Montesinos-Berry E, Domenech J. Catastrophic thinking is a new puzzle piece in understanding anterior knee pain. Orthopaedics Today Europe Official Newspaper of EFORT. 2014;17(2):44–50.
Gracely RH. Pain catastrophizing and neural responses to pain among persons with fibromyalgia. Brain. 2004;127:835–43.
Rathleff MS, Petersen KK, Arendt-Nielsen L, et al. Impaired conditioned pain modulation in young female adults with long-standing patellofemoral pain: a Single Blinded Cross-Sectional Study. Pain Med. 2016;17(5):980–8.
IASP terminology. International Association for the Study of Pain Web site. https://www.iasp-pain.org/terminology.
Sigmund KJ, Hoeger Bement MK, Earl-Boehm JE. Exploring the pain in patellofemoral pain: a systematic review and meta-analysis examining signs of central sensitization. J Athl Train. 2021;56(8):887–901.
De Oliveira SD, Rathleff MS, Petersen K, et al. Manifestations of pain sensitization across different painful knee disorders: a systematic review including meta-analysis and metaregression. Pain Med. 2019;20(2):335–58.
Rathleff MS, Roos EM, Olesen JL, et al. Lower mechanical pressure pain thresholds in female adolescents with patellofemoral pain syndrome. J Orthop Sports Phys Ther. 2013;43(6):414–21.
Rathleff MS, Roos EM, Olesen JL, et al. Self-reported recovery is associated with improvement in localized hyperalgesia among adolescent females with patellofemoral pain: results from a cluster randomized trial. Clin J Pain. 2016;32(5):428–34.
Lefaucheur JP, Drouot X, Ménard-Lefaucheur I, et al. Motor cortex rTMS restores defective intracortical inhibition in chronic neuropathic pain. Neurology. 2006;67:1568–74.
Young NA, Sharma M, Deogaonkar M. Transcranial magnetic stimulation for chronic pain. Neurosurg Clin N Am. 2014;25(4):819–32.
Powers CM, Bolgla LA, Callaghan MJ, et al. Patellofemoral pain: proximal, distal, and local factors, 2nd International Research Retreat. J Orthop Sports Phys Ther. 2012;42:A1-54.
Soifer TB, Levy HJ, Soifer FM, et al. Neurohistology of the subacromial space. Arthroscopy. 1996;12:182–6.
Solomonow M, D’Ambrosia R. Neural reflex arcs and muscle control of knee stability and motion. In: Scott WN, ed. Ligament and extensor mechanism injuries of the knee: Diagnosis and treatment. St. Louis: Mosby-Year Book, 1991; pp 389–400.
Nilsson G, Forsberg-Nilsson K, Xiang Z, et al. Human mast cells express functional TrkA and are a source of nerve growth factor. Eur J Immunol. 1997;27:2295–301.
Sherman BE, Chole RA. A mechanism for sympathectomy-induced bone resorption in the middle ear. Otolaryngol Head Neck Surg. 1995;113:569–81.
Woolf CJ. Pain: moving from symptom control toward mechanism-specific pharmacologic management. Ann Intern Med. 2004;140:441–51.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Sanchis-Alfonso, V., Roselló-Sastre, E., Dye, S.F., Teitge, R.A. (2023). Pathophysiology of Anterior Knee Pain. In: Sanchis-Alfonso, V. (eds) Anterior Knee Pain and Patellar Instability. Springer, Cham. https://doi.org/10.1007/978-3-031-09767-6_2
Download citation
DOI: https://doi.org/10.1007/978-3-031-09767-6_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-09766-9
Online ISBN: 978-3-031-09767-6
eBook Packages: MedicineMedicine (R0)