
Abstract
In this chapter we will explore the normal anatomy and physiology of the gastrointestinal system, and how its functions can alter in the presence of disease and consider what the consequences of this means for the patient.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Learning Outcomes-
Reflect upon the structure of the bowel layers itself and describe the role each of these layers has in relation to peristalsis
-
Consider how understanding the function of the Gastro-intestinal (GI) tract is useful in the care of patients with surgical changes for example the formation of an ileostomy.
-
Reflect on the function of the small intestine and how having a high faecal output stoma might impact the patient.
The gastrointestinaI (GI) tract runs from mouth to anus, consisting of mouth, pharynx, oesophagus, stomach, small bowel (duodenum, jejunum, and ileum) and large bowel (colon) rectum and anus. In total it is thought to be approximately 9 m in length [1]. The primary function of the GI tract is digestion. Digestion is a mechanical and chemical process, that is made up of six key stages;
-
1.
Ingestion
-
2.
Secretion
-
3.
Propulsion
-
4.
Digestion
-
5.
Absorption
-
6.
Defaecation
Each stage will be further discussed as the chapter progresses.
Ingestion is the first stage to occur when food enters the mouth, the food is then chewed or masticated by the teeth, moistened by saliva and broken down by enzymes. This process forms a food bolus, which consequently goes down the pharynx and triggers a swallowing reflex. The food bolus then travels through the oesophagus, where two sphincters situated at the base of the oesophagus prevent its regurgitation into the pharynx and mouth, and also prevents acidic gastric juices from being regurgitated into the oesophagus.
The Bowel Wall
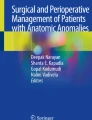
It is important when reviewing the GI tract to consider the structure of the bowel itself. The bowel wall consists of four layers; serosa (Adventitia), muscularis, submucosa and mucosa [1] (See Fig. 4.1).

Layers of the bowel (courtesy of A Perrin)
The serosa is the outer layer and consists of a serous membrane made up of connective tissue and epithelial cells that allows the bowel to receive its blood supply, lymph vessels and nerves. The serosa (adventitia) is only present where there is a mesentery surrounding or suspending the bowel [1].
The muscularis essentially consists of two layers of smooth muscle, that contract in wavelike movements. The movement of smooth muscle is under involuntary control, unlike straited muscle which is voluntary. The two muscle layers are made up of longitudinal fibres and circular fibres, the contraction of these two layers of muscles is known as peristalsis and is present from mid-oesophagus to anus. Peristaltic (or propulsive) movement looks like a wave being propelled through the muscle, as the muscle constricts it then forces anything in front of the narrowed portion forward.
The submucosal layer consists of numerous plexuses of blood vessels, tissue, nerves and lymph vessels including the submucosal or Meissner’s plexus, consequently it is extremely vascular.
The mucosa is the layer closest to the bowel lumen. It secretes mucus, hormones and digestive enzymes, it offers protection and facilitates absorption into the blood. It consists of a mucous membrane creating the inner lining of the GI tract.
The mucosa has three layers: the epithelium, lamina propria and muscularis mucosa.
The epithelium acts as a protective layer in the mouth and oesophagus, and has a secretory and absorptive function throughout the remaining GI tract. Epithelial cells are continuously renewed every 4–5 days eventually being shed off and passed into the faeces [2].
The lamina propria supports the epithelium by binding it to the muscularis mucosa and consists of loose connective tissue containing blood and lymph vessels [1]. The muscularis mucosa consists of very thin, smooth muscle fibres which accommodates movement and expansion of the bowel surface.
The Blood Supply
Blood supply to the abdominal organs is provided by three major vessels originating from the abdominal aorta, the coeliac trunk and the superior and inferior mesenteric arteries (SMA and IMA). This is known as the splanchnic circulation. The SMA and IMA supply oxygenated blood to the complete GI tract. The SMA supplies the jejunum and ileum via a series of intercommunicating paths which travel through the mesentery [3]. The splenic vein joins with the superior mesenteric vein to form the hepatic portal vein which takes blood from these organs to the liver.
Stomach
The stomach is located in the upper left quadrant of the abdomen, is a J-shaped organ composed predominantly of involuntary smooth muscle [4].
Anatomically, the stomach is divided into four main regions:
-
1.
Cardia – which joins the oesophagus to the stomach
-
2.
Fundic region or fundus – top left, dome-shaped region;
-
3.
Stomach body – the expansive main stomach chamber;
-
4.
Pyloric region or pylorus – funnel-shaped lower region connecting the stomach and duodenum
A typical adult human stomach is around 30 cm long and 15 cm wide with an average capacity of around 1.5 L [4, 5].
The stomach has three main functions; storage of food (about 1500 mls in adults), breakdown of ingested food into chyme and the controlled release of chyme into the small intestine [6]. Depending on the nature of the food consumed, food typically remains in the stomach for 3–6 h. Meals rich in protein and fat, such as a fried breakfast, tend to stay in the stomach for longer periods, [7]. Meals that contain a lot of fluid will leave the stomach faster than dry foods, therefore it is advisable for individuals experiencing a high faecal output to avoid drinking at meal times to help with retaining foodstuff within the stomach [8].
The digestion of protein and absorption of alcohol occur in the stomach [9].
When food is present within the stomach the muscular layer of the stomach wall; known as the muscularis, undergoes regular rhythmic contractions that help mix the food with the gastric secretions to speed up the process of chemical digestion. The muscularis consists of the same circular and longitudinal layers of smooth muscle found in other parts of the bowel within the GI tract. However, it also consists of an additional inner layer of oblique smooth muscle fibres. These layers of muscle allow the stomach to perform the strong churning motions that are vital for efficient mechanical digestion. Slowly solid pieces of food are mechanically and chemically digested, resulting in a semi-solid material called chyme [10].
The gastric secretions are hydrochloric acid, pepsin and intrinsic factor. Hydrochloric acid and intrinsic factor are secreted by Parietal cells. Hydrochloric acid supports chemical digestion, as well as activating the enzyme pepsin. Pepsin is produced at high concentrations, giving the stomach a pH of around 2.5–3.5 [10]; this high acidity helps the stomach sterilise ingested food. Intrinsic factor is a small protein that binds to vitamin B12 and transports it across the wall of the intestine into the blood.
About 3 Litres of gastric juice is produced daily [11] and secreted before and during the ingestion of food [12]. Gastric secretion occurs in three phases: cephalic, gastric, intestinal [8].
In the cephalic phase, gastric juice secretion is stimulated by sight, smell and taste or even the thought of food. This triggers the vagus nerve; facilitated by the parasympathetic nervous system to stimulate the stomach wall to produce gastrin. When a person is hungry, the mere anticipation of food is enough to stimulate gastric juice secretion [13]. The cephalic phase accounts for approximately 30% of gastric juice secretion and primes the stomach for the arrival of food. Chief cells secrete the inactive enzyme precursor pepsinogen, which is converted into the active enzyme pepsin in the presence of hydrochloric acid. Pepsin plays a role in protein digestion and enhances the bacterial killing activity of Hydrochloric acid [14].
The gastric phase is the longest phase of gastric secretion, typically lasting about 2–3 hours it begins when protein foods enter the pyloric area of the stomach. This stimulates the release of gastrin from the bowel mucosa into the blood stream, resulting in a surge of secretions of gastric juice [8]. Additionally, the stomach distends as a consequence of food being present which in turn stimulates the release of gastrin, leading to the activation of local and parasympathetic reflexes in the pylorus [8].
The intestinal phase is a stage in which food continues to pass slowly from stomach to the duodenum. The duodenum responds to arriving chyme and moderates gastric activity through nervous reflexes and the release hormones such as cholecystokinin, secretin and gastric-inhibiting peptide, which gradually reduce the secretion of gastric juice [5].
The Small Bowel/Intestine
The small bowel/intestine comprises of the duodenum, jejunum and ileum. Although the small bowel/intestine is narrower than the large intestine, it is actually the longest section of your digestive tract. The actual length varies considerably from person to person, but it’s thought to range from 3 to 9 metres [15].
Duodenum
Chyme passes from the stomach to the duodenum via the pyloric sphincter to prevent regurgitation [8, 12]. The duodenum is the primary region for chemical digestion. Intermittently, the pyloric sphincter opens to release small amounts of acidic chyme, which stimulates the release of several hormones including Secretin, Cholecystokinin, Gastric inhibitory polypeptide and Vasoactive intestinal peptide.
The duodenum is C shaped and approximately 25–38 cm long [16]. It essentially consists of four regions; an upper, superior region called the duodenal bulb, that continues up to pyloric sphincter and the descending region that extends downwards into the abdominal cavity. About half way down the descending region is the entry point of the common bile duct and pancreatic duct which fuse before entering the duodenum. The bile and pancreatic juices are controlled entering the duodenum by a ring of muscle called the sphincter of Oddi. The horizontal section is the largest and is the main site for mineral absorption. The ascending region connects to the jejunum at the duodenojejunal flexure.
The duodenum has a mucosal lining that hosts tall columnar epithelial cells that extend into circular folds and finger-like projections, called villi. The villi increase the surface area allowing increased absorption of nutrients to occur although nutrient absorption predominantly occurs further down the small intestine.
The Jejunum
The jejunum is about 90 cm in length. It starts at the duodenojejunal flexure and ends at the ileum. There is no clear border between the jejunum and the ileum.
The jejunum has an immense surface area allowing for optimum absorption of nutrients. The wall of the jejunum consists of circular folds, villi and micro-villi that all assist with increasing surface area of the jejunum and the ileum where the villi are longer, more numerous and found at greater density. The numerous circular folds are microscopic and run parallel to each other in the mucosa of the jejunum. These deep ridges in the mucosal lining increase the absorption capacity by tripling the surface area of the absorptive mucosa in the intestinal wall. The villi, finger-like projections which can be found within the circular folds, measure 0.5–1 mm in length and multiply the surface area by 10 therefore enhancing the surface area available for nutrient absorption. The mucosal epithelial cells have thin, hair-like extensions about 0.01 mm in length; these tiny projections are known as micro-villi or brush border. There are approximately 200 million per 1 mm squared [17]. Villi have a very high rate of mitosis, so consequently are quickly replaced.
The Ileum
The ileum is the longest part of the small intestine making up to about three fifths of its total length. It is thicker and more vascular than the jejunum, and the circular folds are less dense and more separated [18]. The ileo-caecal valve can be found at the distal ileum and separates the ileum from colon. The valve is a sphincter formed of circular muscle that prevents reflux of the bacteria-rich fluid entering the colon and regulates the passage from small to large bowel.
Function of Small Bowel
As previously discussed the duodenum undertakes a large quantity of chemical digestion, as well as a small amount of nutrient absorption; however the key function for both the jejunum and the ileum is to finish chemical digestion and absorb nutrients along with water and vitamins. The mucosa of the small intestine secretes about 2 L each day of a slightly alkaline substance (pH 7.5–8) [8]. Consequently, if a patient has a high ileostomy output, they would be losing nutrients as well as bowel secretions.
To aid digestion there is a process called segmentation; where rings of circular smooth muscle hosting the villi and brush border found within the wall of both jejunum and ileum repeatedly contract and relax. Unlike peristalsis that involves rhythmic contractions of the longitudinal muscles, segmentation moves intestinal contents back and forth, distending the ileum, but this does not assist chyme through the tract; instead, it mixes it with digestive juices and then pushes it against the mucosa to allow nutrient absorption. For any patient who has undergone numerous ileal resections, and has a limited length of ileum remaining it may not be possible for them to reabsorb adequate nutrients. If a patient has less than 1 m of small bowel then it is unlikely that they will be able to reabsorb enough nutrients to maintain life without artificial feeding. It is important during surgery that following any resection of the duodenum, jejunum or ileum that the surgeon notes the length of small bowel remaining, rather than the length resected, so that an accurate future assessment can be formulated and appropriate care implemented.
Absorption
Within a 24 hour period it is estimated that about 8 litres of water from dietary ingestion as well as GI secretions and juices, (see table 4.1) along with several hundred grams of carbohydrates, ≥100 g of fat, 50–100 g of amino acids and 50–100 g of salt ions pass through the wall of the small intestine and into the blood [17, 20]. An individual living with an ileostomy may experience a high output which is classified as an output exceeding 1500 in 24 h period [21]; however opinions regarding the volume of the definition of high output do vary. Baker [22] suggests that patients with an output of between 1200–2000 mls/24 hours should have normal diet, fluids and salt, but may also require additional treatment. Please see ASCN UK guidelines of management of high output stoma in both hospital and community setting for further guidance on the complex issue [23].
Nutrients are transported across membranes of the intestinal epithelial cells into the villi, and then into blood capillaries and lacteals, which can occur either passively or actively. A lacteal is a lymphatic capillary that absorbs dietary fats in the villi of the small intestine. Passive transport requires no energy and involves the diffusion of simple molecules along a concentration gradient—moving from an area of high concentration to a lower concentration—in this case, the blood [17].
In the small intestine the villi present absorb a large percentage of all proteins, carbohydrates and fats. Carbohydrates are absorbed as monosaccharides (simple sugars) 80% of which is glucose [17]. Protein (amino acid) is absorbed via the capillaries into the portal vein and liver. Fats as fatty acids and glycerol pass into the lymph within the villi and drain into the lymphatic capillaries [8, 12].
Water and some vitamins can cross the gut wall passively. Some molecules—such as glucose, amino acids and vitamin B12—have their own carriers or transporters, which they use to ‘piggyback’ across the gut wall into the bloodstream [17]. This is an important consideration if caring for a patient suffering short bowel or experiencing severe diarrhoea/high faecal output requiring rehydration therapy. Rehydration therapy is only effective if it comprises of glucose and sodium within the water, as glucose is needed for sodium uptake.
In starvation, the intestinal epithelial cells shrink, resulting in the villi reducing in size (sometimes by half) which consequently reduces the absorption capacity of the small intestine. This is an important consideration following post-operative ileus or in the presence of a small bowel fistula. This effect can be reversed when enteric feeding is commenced. Damage to such cells can be seen in Coeliac disease, Crohn’s Disease or due to radiation damage [8, 24].
Gall Bladder
The gall bladder is a hollow pear-shaped organ approximately 8–10 cm in length, that is situated underneath the liver to the right of the stomach. The primary function is to store and concentrate bile secreted by the liver. The gall bladder acts as a reservoir for the unused bile whilst it is not being used for digestion. When food stuff enters the small bowel, a hormone called cholecystokinin is secreted. This causes the gall bladder to contract consequently pushing the bile into the duodenum to emulsify the fatty food [1, 25].
Pancreas
The pancreas is an important organ. It plays key roles in both the regulation of blood glucose levels and digestion [26]. It comprises of an endocrine and an exocrine portion. The endocrine function is responsible for the production of key hormones that control blood sugar levels and regulation of appetite and the exocrine which is the digestive portion of the pancreas [26]. The exocrine acinar cells secrete up to 1.5 L of pancreatic secretions daily. The secretions are released following a stimulation by hormones such as secretin that is released by intestinal mucosa [1]. This pancreatic secretion contains enzymes such as Trypsinogen, lipase and amylase. Trypsinogen is used to breakdown protein, amylase hydrolyses polysaccahirides to disaccaharides and lipases digest fat [8].
Large Intestine
The large intestine comprises of the caecum, colon (made of ascending, transverse, descending and sigmoid colon), rectum, anal canal and anus. It is approximately 1.5 metres in length and 7 cm in diameter at caecum reducing down to 2.5 cm at sigmoid colon [1]. Its structure is relatively similar to that of the small intestine except that its mucosa is entirely void of villi.
The caecum is a 6 cm long tubular sac made up of lymphoid tissue extending towards the appendix, now thought to be an obsolete organ.
Within the colon, haustra or pouches are formed as a result of 3 separate longitudinal ribbons of smooth muscle on the outside of the ascending, transverse, descending and sigmoid colons. They are visible and can be seen just below the serosa or fibrosa. They run the length of the colon but slightly shorter, causing a gathering effect and pouching (haustra) appearance of the colon.
The primary function of the colon is to absorb excess water and electrolytes converting semi-solid/liquid faeces into firmer faeces in readiness for evacuation. The presence of food residue in the colon stimulates haustral contractions which occur approximately every 30 minutes. Each contraction, causes the haustrum to distend and contract, pushing the food residue along to the next haustrum. The contractions facilitate the mixing of the food residues, thereby facilitating the absorption of water.
About 1500 mls of waste/fluid residue enters the caecum every 24 hours, but only 150 mls of this becomes faeces—it contains mostly bacteria and decaying epithelial cells, along with inorganic waste, undigested food matter and fibre, as well as water to help it pass smoothly through the remaining large intestine.
Colonic Movement
Food in the stomach and a distended caecum triggers a gastric colic reflex and colonic mass movements begin. Hustral contractions in the colon assist to propel the predominantly dehydrated contents through the colon into the rectum towards the anus. Such actions are usually initiated 3 or 4 times a day after meals. The strongest movement is suggested to be in the first hour after breakfast [24] resulting in a common time for people to open their bowels.
Colonic mass movements fill the rectum, resulting in an urge to defecate. This urge should not be ignored as once the movement has passed, the urge also ceases. If the urge to defecate is ignored for an extended period of time, the rectum overfills, the large intestine absorbs more fluid resulting in the faeces becoming drier and harder resulting in constipation [27].
Normal bowel emptying patterns vary greatly between individuals, from three times per day to three times per week [28].
The rectum itself is about 15 cm long, although this can vary depending on the literature consulted. Faeces entering the rectum are usually solid. The rectum can hold approximately 400 mls faeces [11]. As faeces enter the rectum, it begins to stretch; this action stimulates an impulse which is sent to the nervous system within the spinal cord to initiate a defaecation reflex. This results in the relaxation of the internal anal sphincter (involuntary control), allowing a small amount of faeces to pass into the anus. The anus is able to identify if the material is gaseous or solid and reacts accordingly. If the stool is solid and if it is convenient to defecate the external anal sphincter will relax and open, which is a voluntary control in most adults. If it is inconvenient to open bowels at that time the individual can consciously delay defecation until a more convenient time.
Anal Canal
The anal canal is approximately 2.5–4 cm in length from the ano-rectal junction to anus. The anal sphincter is comprised of two sphincter complexes; the internal anal sphincter, which is controlled by involuntary muscles and the external anal sphincter, which is made of skeletal muscle and is under voluntary control. Except during defecation, both anal sphincters normally remain closed.
Gut Microbiota
Gut microbiota or microbiome are the community of microorganisms including bacteria, archaea and fungi that live in the GI tract. As previously highlighted, the GI tract has an extremely large surface area which enhances the processes of digestion and absorption, and functions as an appropriate environment for microbial attachment and colonisation.
Previous and contemporary discussion suggests that it has been recognised that the bacteria living in the gut such as Escherichia coli (E coli), perform essential functions, such as the biosynthesis of Vitamin K, however, it is more recently – within last 10 years that the complex relationship between the micro-organisms of the gut microbiota and human tissues is slowly being understood.
Gut bacteria can have a direct influence on the immune system and the body’s ability to deal with disease and infection. Antibiotic therapies, poor diet and psychosocial stress, as well as exposure to pathogenic organisms can also have an impact on gut microbionta [26].
Although there is some evidence regarding the effectiveness of probiotics, it is often contradictory, but stool pills and faecal transplant appear to be effective in reducing clostridium difficile infection and colitis [29]. Probiotics are live microorganisms that are intended to have health benefits when consumed or applied to the body, although given the limited data currently available they are not recommended for use in the majority of clinical settings. Further research is required to understand more fully the role of gut microbiota and its role in GI tract health. This inevitably will assist the SSCN to understand the importance of this part of GI tract function to patient health and GI disease management.
Diseases and the GI Tract
Inflammatory bowel disease (IBD) is a collective term used to describe chronic inflammatory disorders of the gastrointestinal (GI) tract, most notably ulcerative colitis (UC) and Crohn’s disease (CD) [30].
Ulcerative Colitis (UC)
is an inflammatory disease that affects the mucous membrane of some or all of the large bowel (colon) and rectum. Inflammation and ulceration starts at the rectum and extends proximally in continuity [31].
UC is characterised by episodes of acute exacerbation and remission. The time period of the remissions can vary greatly from just weeks to sometimes years. The exact aetiology of UC is not known although it is believed to involve interactions between the environment, immune system, gut microbiome and a genetic predisposition to the disease [32].
It is estimated around 1 in every 420 people living in the UK has ulcerative colitis. This amounts to around 146,000 people. However, this figure is also beginning to rise in developing nations (https://www.crohnsandcolitis.org.uk/about-crohns-and-colitis/publications/ulcerative-colitis) [33].
UC has a bimodal age distribution with an incidence peak in the second or third decades and a second peak between 50 and 80 years [34].
The signs and symptoms individuals with UC can experience range from bloody diarrhoea, frequency and urgency often relieved by defaecation, pyrexia, weight loss, abdominal pain and lethargy. The cure for ulcerative colitis is to have the colon surgically removed (total colectomy) with the rectum removed as well (panproctocolectomy) or possibly have reconstruction surgery such as ileo-anal pouch/ restorative proctocolectomy/J pouch/ileal pouch anal anastomosis/IPAA. Many patients are managed extremely effectively with a range of pharmacological therapies.
5-aminosalicylic acid compounds (5-ASA) drugs represent the main therapies for mild to moderately active UC, and optimising patients’ adherence to any given drug regime is important. The introduction of the Inflammatory Bowel Disease Nurse Specialist role has been fundamental in this provision of care [35].
In UC patients with inadequate response to 5-ASA, immunosuppressive or biologic therapies are indicated, and choice is dependent on multiple factors, including patient choice [34]. However, all drugs have side effects which may impact on the health of the patients.
Crohn’s Disease
Crohn’s disease was thought to be an autoimmune disorder in which the immune system attacked the body’s own gut lining. Contemporary theories suggest that there is evidence indicating that the immune system overzealously attacks a microbial antigen on the gut lining [36]. Crohn’s Disease can affect any part of the GI tract from lips to anus, but most commonly seen in the distal ileum and proximal colon. One very notable difference with Crohn’s Disease when compared to UC is the presence of “skip lesions”; these are areas of ulceration interrupted by sections of healthy tissue.
It is estimated that Crohn’s Disease affects about one in every 650 people in the UK.
Crohn’s disease can start at any age, but usually appears for the first time between the ages of 10 and 40, although recent studies suggest there is a small peak in the number of people diagnosed over the age of 60.
Crohn’s disease is more common in urban than rural areas, and in Northern hemisphere countries such as Northern Europe and North America, although the numbers are beginning to increase in developing nations.
A theme from contemporary surveys suggest that more new cases of Crohn’s disease are being diagnosed in recent years, particularly among teenagers and children. The reason for this is not clear. Crohn’s disease appears to be slightly more common in women than in men. It is also more common in smokers [33].
There is no cure for Crohn’s Disease, however timely interventions, careful assessment and appropriate drug therapies can minimise complications, induce remission and reduce the need for surgery. First line drug therapy for IBD is 5-ASAs along with steroids to gain disease remission. The second line of therapy is immunosuppression and then third line is biologic drug therapy [37].
Signs and symptoms can initially be quite vague and intermittent depending on the site of the ulceration within GI tract, which can result in a delay in diagnosis. Signs and symptoms can include; diarrhoea, fatigue, anorexia and abdominal pain. In patients who are experiencing a partial obstruction their abdominal pain will be described as crampy or cramping and intermittent, but an acute flare up, an exacerbation (possibly abscess or fistula) of Crohn’s Disease will result in an individual experiencing prolonged persistent pain, associated with abdominal tenderness. Diarrhoea will be a consistent sign, but unlike in UC it is unlikely to be bloody.
Surgery is indicated when medical therapies are not adequately maintaining good quality of life for patient or if the patient experiences severe symptoms that are unmanageable through medical intervention. Occasionally such symptoms can be life threatening such as bowel perforation. Surgery would necessitate the resection of any diseased bowel; this could be ileal or colonic depending on the site of the active disease. It is important for the surgeon to record the length of bowel the patient has left insitu, as this will allow for accurate assessment to take place should there be a requirement in the future if considering re-anastomosis or if additional supplementary nutrition is required.
Please see colorectal surgery Chap. 6 for the specifics of surgery performed for Crohns disease.
Extra- Manifestations of IBD
Aetiology for UC and Crohn’s Disease is not fully understood, however it is suggested that in both conditions the equilibrium of the intestinal mucosa as a host to antigens is disturbed. This disturbance results in chronic over expression of the immune response and over production of cytokines within the gastrointestinal mucosa leading to chronic inflammation [30, 38].
This increased response of the immune system may affect other organs, including the liver, skin, and eyes, causing inflammation within these structures and resulting in the development of extraintestinal manifestations of IBD [39, 40]; Williams [41] estimate that up to 40% of patients with IBD will experience extra intestinal manifestations. Common extra intestinal manifestations include peripheral arthritis, aphthous stomatitis (mouth ulcers), uveitis, and erythema nodosum [30, 39].
Other extra-manifestations that are commonly seen by SSCNs are in relation to skin, both Crohn’s Disease ulceration as well as peristomal pyoderma gangrenosum (PPG). PPG is a rare, ulcerative inflammatory skin disorder. Common presentation includes a pustule that originates centrally and has a blue tinge to the surrounding skin [42]. Further information on PPG see Chap. 8 Managing complicated stomas.
Familial Adenomatous Polyposis
Familial Adenomatous Polyposis (FAP) is an autosomal dominant inherited condition (50:50) that can result in numerous adenomatous polyps developing within the large intestine. An autosomal dominant inherited condition means that a person affected has a 50 percent chance of passing the altered gene to each child, as well as a 50 percent chance that a child will not inherit the altered gene.
The polyps are frequently benign, however if left untreated they will develop into a malignant colonic cancer. Treatment is usually in the form of surgery. All patients will need some form of surgical intervention to rid them of the polyps. The exact surgical procedure needs careful consideration and can very much depend on age, hobbies and indeed what stage they are at in life, as FAP is predominantly diagnosed in young adulthood. Some patients may opt to have panproctocolectomy with a permanent ileostomy, others may choose to have a total colectomy and ileostomy formation initially, before deciding whether to have completion proctectomy resulting in a permanent ileostomy or opt for an ileo-anal pouch reconstruction or possibly an ileo-rectal anastomosis. Regardless of which procedure the patient chooses, if they have decided to have a surgical procedure which retains rectum then careful and regular assessment should be made of any retained rectum for the occurrence of polyps.
The genetic determinant in FAP can also predispose patients to other associated malignancies such as duodenal and stomach cancers. Other extra-intestinal manifestations include congenital hypertrophy of retinal pigment epithelium (CHRPE), jaw cysts, osteomata and fibromas.
Polyposis registries throughout the world are now in existence to allow for the careful monitoring, tracking and surveillance of family members of affected individuals. St Mark’s registry in London was the first, in existence since 1924.
Diverticular Disease
Diverticular disease is commonly seen within the sigmoid colon of older people living in the western world. Small pouches called diverticula can form on small weakened areas of the intestinal walls as a result of increased pressure perhaps as a result of straining during defecation. Diverticulitis is seen when any of the diverticula pouches become inflamed and possibly infected. This tends to occur when bacteria have built up in diverticula blocked by faeces/waste material. Diverticular bleeding may result. Treatment is usually given in the form of antibiotics. Surgery may be required as an emergency if the diverticulitis becomes severe resulting in bowel perforation. (See Chap. 6 on surgical procedures).
Colorectal Cancer Please See Chap. 5
Peptic Ulceration
Peptic Ulceration is an umbrella term used to describe ulcers occurring in the stomach and/or duodenum. It is believed that stress and poor diet, especially spicy and greasy foods are contributing factors for the development of such ulcers. It is now also recognised that infections relating to Helicobacter pylori (H. pylori) is the major contributing factor. The use of NSAID’s also increases the risk of peptic ulcers [43].
Patients will often report signs and symptoms of burning, epigastric pain and can often pin point the exact location of their pain. However, the only definitive way to locate a peptic ulcer is to visualise it via endoscopic route. Peptic ulcers must be treated as the risk of perforation can lead to life-threatening complications such as peritonitis and/or sepsis. Treatment is commonly offered in form of proton pump inhibitor drugs to reduce acid secretion and two antibiotics to eradicate H. pylori infection (triple therapy) [44].
Conclusion
As a SSCN, having a detailed knowledge and understanding of the anatomy and physiology of the GI tract is fundamental to ensure that the care of stoma patients is underpinned with a sound theoretical framework, enabling the SSCN to critically evaluate disease processes and treatments within the specialist colorectal field. This advanced level of knowledge leads to proactive management of patients and an intuitive recognition of potential complications or any deviations from a normal treatment trajectory which may occur.
References
McGrath A. Anatomy and physiology of the bowel and urinary systems. In: McGrath PT, editor. Stoma care. essential clinical skills for nurses. Blackwell Publishing; 2005.
der Flier V, Laurens G, Clevers H. Stem cells, self-renewal, and differentiation in the intestinal epithelium. Annu Rev Physiol. 2009;71:241–60. https://doi.org/10.1146/annurev.physiol.010908.163145. ISSN 1545-1585
Trowers E., Tischler M. Form and function: the physiological implications of the anatomy of the gastrointestinal system. In: Gastrointestinal physiology. Springer, Cham. 2014, https://doi.org/10.1007/978-3-319-07164-0_2.
Mahadevan V. Anatomy of the stomach. Surgery. 2014;32(11):571–4.
Daniels, Allum. The anatomy and physiology of the stomach. In: Fielding JWL, Hallissey MT, editors. Upper gastrointestinal surgery. London: Springer Verlag; 2005.
Snell RS. Clinical anatomy for medical students. 7th ed. London: Lippincott; Williams and Wilkins; 2004.
Kong F, Singh RP. Disintegration of solid foods in human stomach. J Food Sci. 2008;73:5,R67-R80.
Burch J. Stoma care. Wiley-Blackwell; 2008.
Tortora GJ, Derrickson B. Principles of anatomy ans physiology. 11th ed. New Jersey: John Wiley & Sons Inc; 2006.
Marieb, Hoehn. Human anatomy and physiology. London: Pearson; 2015.
Black PK, Hyde CH. Diverticular disease. London: Whurr; 2005.
Watson R. Anatomy and physiology for nurses. 11th ed. London: Balliere Tindall; 2002.
Power M, Schulkin J. Anticipatory physiological regulation in feeding biology: cephalic phase responses. Elsevier; 2008.
Zhu, et al. Bacterial killing in gastric juice—effect of pH and pepsin on Escherichia coli and Helicobacter pylori. J Med Microbiol. 2006;55(Pt9):1265–70.
Burch J, Collins B. Oxford handbook of gastrointestinal nursing. Oxford: Oxford University Press; 2021.
Lopez PP, Gogna S, Khorasani-Zadeh A. 2019. https://europepmc.org/article/nbk/nbk482390#free-full-text
Nagam Y. Gastrointestinal tract 4: anatomy and role of the jejunum and ileum. Nurs Times. [online]. 2019;115(9):43–6.
Keuchal M, et al. Normal small bowel. Video journal and Encyclopedia of GI. Endoscopy. 2013;1(1):261–3.
Gennari J, Weise W. Acid-base disturbances in gastrointestinal disease. CJASN. 2008;3(6):1861–8. https://doi.org/10.2215/CJN.02450508.
Hall JE. Digestion and absorption in the gastrointestinal tract. In: Guyton and hall textbook of medical physiology. Philadelphia, PA: Saunders; 2011.
Oke SM Nightingale JM and Gabe SN. Mistakes in short bowel and how to avoid them. UEG Education 7–11 2018.
Baker M, Greening L. Practical management to reduce and treat complications of high output stoma. GI Nurs. 2009;7(6):10–7.
ASCN UK Clinical Guidelines. 2019.
Richards A. Intestinal physiology and its implications for patients with bowel stomas. In: Breckman B, editor. Stoma care and rehabilitation. London: Elsevier Churchill Livingstone; 2005.
Page, M ed 2001 the human body. Dorling Kindersley London as cited in McGrath A 2005 in Anatomy and Physiology of the bowel and urinary systems. In: Porrett T. McGrath 2005 Stoma Care. Essential Clinical Skills for Nurses. Blackwell Publishing.
Knight J. Gastrointestinal tract 6: the effects of gut microbionta on human health. Nurs Times. 2019;115:11.
Nagam Y. Gastrointestinal tract 5: the anatomy and functions of the large intestine. Nurs Times. [online]. 2019;115:10.
Walter SA, et al. Assessment of normal bowel habits in the general adult population: the Popcol study. Scand J Gastroenterol. 2010;45(5):556–66.
Mayor S. Faecal transplant given in oral capsule reduces recurrent c difficile shows study. Br Med J. 359:j5501.
Younge L. Dermatological complications to consider when managing IBD patients. Gastrointest Nurs. 2015;13:4.
Jewell DP, Chapman RGW, Mortenson N. Ulcerative colitis and Crohn’s disease. London: Churchill Livingstone; 1992.
Kobayashi T, Siegmund B, Le Berre C, et al. Ulcerative colitis. Nat Rev Dis Prim. 2020;6:74.
https://www.crohnsandcolitis.org.uk/about-crohns-and-colitis/publications/ulcerative-colitis
Segal. Ulcerative Colitis: an update. 2021., https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8002778/
Mason I, Holbrook K, Kemp K, Garrick V, Johns K, Kane M. Inflammatory bowel disease nursing: results of an audit exploring the roles, responsibilities and activity of nurses with specialist/advanced roles. London: Royal College of Nursing; 2012.
Torres J, et al. Crohn’s disease. Lancet. 2017;389(10080):1741–55.
https://www.bsg.org.uk/clinical-resource/bsg-consensus-guidelines-on-the-management-of-inflammatory-bowel-disease-in-adults/ accessed on 23/02/2022.
Hanauer SB. Inflammatory bowel disease: epidemiology, pathogenesis, and therapeutic opportunities. Inflamm Bowel Dis. 2006;12(Suppl 1):S3–9.
Danese S, Semeraro S, Papa A, et al. Extraintestinal manifestations in inflammatory bowel disease. World J Gastroenterol. 2005;11(46):7227–36.
Ardizzone S, Sarzi Puttini P, Cassinotti A, Bianchi Porro G. Extraintestinal manifestations of inflammatory bowel disease. Dig Liver Dis. 2008;40(Supplement 2):S253–9.
Williams H, Walker D, Orchard TR. Extraintestinal manifestations of inflammatory bowel disease. Curr Gastroenterol Rep. 2008;10(6):597–605.
Smith A, Lyons C. Abdominal stomas and their skin disorders. London: Martin Dunitz; 2001.
Kaur A, et al. Peptic ulcer; a review on etiogy and pathogenesis. Int Res J Pharm. 2012;3(6):34–8.
Narayanan M, et al. Peptic ulcer disease and H. Pylori infection. Mo Medicine. 2018;115(3):219–24.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Perrin, A. (2023). Anatomy and Physiology of the Gastrointestinal Tract and Associated Disease Processes. In: White, M., Perrin, A. (eds) Stoma Care Specialist Nursing: A Guide for Clinical Practice. Springer, Cham. https://doi.org/10.1007/978-3-031-07799-9_4
Download citation
DOI: https://doi.org/10.1007/978-3-031-07799-9_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-07798-2
Online ISBN: 978-3-031-07799-9
eBook Packages: MedicineMedicine (R0)