
Abstract
Conservative treatment (NSAIDs, rehabilitation, orthoses, and shock waves) resolves 90% of cases of acute lateral epicondylitis (LE), although it is less effective in chronic cases. Corticosteroid (CS) injections may be effective in the short term, but their benefit is reduced in the long term. Platelet-rich plasma (PRP) and autologous blood are more effective in the medium term than CS injections for the treatment of LE and have minimal side effects. Open, arthroscopic, and percutaneous surgical approaches are all very effective. Arthroscopic and percutaneous approaches can provide faster recovery and earlier return to work. Open surgery is the most effective long-term surgical treatment, although it is the most invasive and has the longest recovery.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
12.1 Introduction
Lateral epicondylitis (LE), or tennis elbow, is a challenging problem that can lead to significant disability and limitation not only in athletics but also in activities of daily living, affecting 1%–3% of the general population each year. LE can cause significant pain and functional impairment, and despite its relatively high prevalence, there remains a multitude of treatments due to the lack of a single gold standard solution. In the majority (80%–90%) of cases, it can be successfully treated nonsurgically. However, 4%–10% of patients will have persistent symptoms, often leading to surgical intervention that produces “good” or “excellent” results in 80%–90% of cases.
12.2 Epidemiology
LE most commonly affects adults in the fourth and fifth decade of life and is more common in the dominant arm, with no gender differences [1]. It is generally considered an overuse injury involving repeated extension of the wrist against resistance. Up to 50% of all tennis players develop symptoms due to various factors, including poor swing technique or the use of heavy rackets. It is also seen in workers who use heavy tools or perform repetitive gripping or lifting tasks.
12.3 Etiology and Pathogenesis
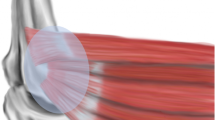
LE is mainly due to overloading by repetitive movements in wrist extension. In LE, the most frequently affected muscle is the extensor carpi radialis brevis (ECRB), at its origin (Fig. 12.1). The enthesis of the extensor digitorum communis (EDC), the extensor carpi radialis longus (ECRL), or extensor carpi ulnaris (ECU) may also be affected, but less frequently. Any activity that involves repeated activation of these muscles (screwing, typing, playing tennis, etc.) for long periods of time favors muscle overload and the appearance of tendinosis. Overuse, obesity, and smoking have been identified as risk/aggravating factors [2].
12.4 Clinical Symptoms
All patients with LE present with pain in the anterior and/or superior lateral epicondyle, radiating through the extensor musculature. The intensity of the pain can be highly variable: from pain only with certain gestures or activities to continuous disabling pain that is exacerbated at night. Typically, the pain is triggered when the patient is asked to perform wrist and finger extension against resistance. Generally, pain is less pronounced when wrist extension is performed with the elbow flexed and more when performed with the elbow extended. This is one of the most commonly used tests for the clinical diagnosis of LE.

Anatomical image of the epicondylar musculature

MRI image showing signal changes of the lateral epicondyle, with thickening, irregularity, and slight edema of the extensor digitorum communis (EDC) and extensor carpi radialis brevis (ECRB) tendons
Generally, joint balance is preserved in all patients. If this is not the case, the coexistence of added pathology should be considered [3]. The differential diagnosis should routinely rule out the following:
12.4.1 Posterolateral Instability
In all patients presenting with elbow pain, the joint should be checked for stability. A history of ulnar varus, previous surgery, or elbow dislocation should always be considered. Also, repeated corticosteroid injection may damage the lateral ligamentous complex and lead to elbow instability.
12.4.2 Posterolateral Plica
Its association with LE is very frequent. Usually, the pain is triggered by elbow extension while palpating the posterior part of the radiocapitellar joint.
12.4.3 Posterior Interosseous Nerve (PIN) Compression
Also known as radial tunnel syndrome, it produces pain of neuropathic characteristics in the lateral/posterior aspect of the forearm. Typically, the pain is not triggered by wrist extension, but it is triggered by wrist supination (due to compression of the supinator brevis over the PIN). A selective nerve block can be performed if there is any doubt about the diagnosis.
12.4.4 Other Pathologies
Other possibilities that should be considered in a patient with lateral elbow pain are cervical radiculopathies, overuse of the joint due to adjacent joint disease, low-grade infection, and capitellar osteochondritis.
12.5 Diagnosis
In most cases, LE can be diagnosed through anamnesis and physical examination.
However, it is not uncommon to perform complementary tests, aimed both at refining the diagnosis of tendinopathy and at ruling out the coexistence of other pathologies. In general, an anteroposterior and lateral X-ray should be requested in all patients. The presence of calcifications at the origin of the ECRB is suggestive of chronic evolution.
Ultrasonography has become an increasingly requested test that can demonstrate changes in the tendons (thickening, scarring, intrasubstance degeneration, microcalcifications, neovascularization) as well as facilitate the performance of infiltrations [4]. Magnetic resonance imaging (MRI) (Fig. 12.2) facilitates the observation of intrasubstance degenerative changes. However, the findings of the MRI do not always correlate with the severity of the clinical symptoms, and it is an expensive test, so its main indication is to rule out concomitant lesions [5]. Neurophysiological studies are indicated if there is a suspicion of a possible compression of the posterior interosseous nerve.
In general, the diagnosis of this tendinopathy relies on a good physical examination, with complementary tests being performed in case of doubt or to assess the presence of concomitant pathology.
12.6 Conservative Treatment
As a rule, LE tends to self-resolve in the vast majority of patients and therefore nonsurgical treatments are recommended for the initial management of acute LE. Conservative treatment should be performed in all patients because of its low cost and high effectiveness (up to 90% of patients improve) [5]. Currently, there is no strong evidence for the efficacy of a single nonsurgical treatment option for LE. This may explain the numerous treatment options described in the scientific literature in the last decade.
12.6.1 Rest and Postural Reeducation
Rest improves symptoms in all patients. Postural reeducation is important especially in those cases due to overuse and is a fundamental part of treatment in work and sport-related cases. Reeducation should include the shoulder and periscapular musculature, both of which are important for proper elbow function. External supports that help relax the epicondylar musculature should also be included, such as wrist supports for computer keyboarding. Tennis players may benefit from additional sport-specific advice. Technique errors thought to predispose to LE etiology are (1) faulty backhand technique with the elbow forward, (2) excessive forearm pronation during an overhead forehand swing, and (3) excessive wrist flexion during a serve. Other potential risk factors include racquet type, grip size, string tension, court surface, and ball weight. These factors affect the biomechanical loading of the elbow during tennis.
12.6.2 Exercises
A 2015 systematic review included studies with low risk of bias. The conclusion was that home strengthening exercises are more effective than a wait-and-see policy. In addition, there is no difference in outcome after a specific type of exercise (stretching, concentric, or eccentric exercises). In addition, the supervised combined stretching and strengthening protocol is superior to a comparable at-home protocol [6].
12.6.3 Orthoses
The use of orthoses provides pain relief. They are based on decreasing the tension of the wrist extensors. No differences in results have been observed between the different types of orthoses [6]. The patient must be instructed in their proper use, since improper use can lead to compression of the posterior interosseous nerve.
12.6.4 Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
There has been no consensus on the superiority of oral versus topical NSAIDs in pain control, although oral NSAIDs may cause gastrointestinal adverse effects [7]. In a Cochrane review they found low-quality evidence showing that topical NSAIDs were more effective than placebo alone in the short term (up to 4 weeks) in reducing pain versus placebo, while the evidence on oral NSAIDs was conflicting. They concluded that there is limited data on the efficacy of topical or oral NSAIDs for LE treatment [8].
12.6.5 Shock Waves
It consists of the application of a sound wave of a specific frequency directly on the origin of the musculature, although the ultimate mechanism of action is unknown. They are a possible alternative to reduce pain and medical costs associated with more invasive therapy. A meta-analysis concludes that based on existing clinical evidence, extracorporeal shock wave therapy can effectively relieve pain and functional impairment (loss of grip strength) caused by LE, with greater overall safety than other methods, especially CS injections [9]. However, another meta-analysis suggests that shock wave therapy cannot significantly reduce pain compared with placebo or control group [10].
12.6.6 Injections
12.6.6.1 Corticosteroid (CS) Injections
Corticosteroid injections are one of the most frequently used treatments due to their low cost and ease of application, which is a concern given the evidence of low cost-effectiveness and potential long-term harm. They provide rapid and significant pain relief, but their long-term results are questioned in the literature [7]. Repeated CS injections can lead to iatrogenic tendon rupture and muscle atrophy. Therefore, clinicians should be wary of CS overuse in the treatment of LE because of poor long-term efficacy and potential adverse effects. Therefore, in principle, they would only be indicated in those patients who need rapid and intense short-term pain improvement (e.g., professional athletes). Therefore, while it appears that steroid injections are effective in relieving LE pain in the short term, there does not appear to be a lasting benefit.
12.6.6.2 Autologous Blood Injections
It has been shown that autologous blood injections could trigger an inflammatory reaction around the tendon to promote tissue healing with cellular and humoral mediators [11].
12.6.6.3 Platelet-Rich Plasma (PRP) Injections
PRP contains growth factors that could be beneficial for the healing of soft tissue injuries. However, available studies have reported conflicting results, making it difficult to draw clear conclusions. A systematic review stated that the PRP injection has no obvious effects on the treatment of chronic LE [12]. They provide better medium-term pain control than CS infiltrations [13]. They also appear to have lower complication rates than corticosteroids and autologous blood injection [14]. Among its major drawbacks is the diversity of commercial kits and protocols, which makes it difficult to know which is the best formulation to use [15]. PRP injection has been shown in some studies to be effective in the management of chronic LE in the medium and long term. In a successive systematic review and meta-analysis of randomized controlled trials to compare the effectiveness of three commonly used injections – CS, PRP, and autologous blood – in the treatment of LE, Houck et al. found that corticosteroid improves functional outcomes and pain relief in the short term, while autologous blood and PRP are the most effective treatments in the medium term [13].
Tang et al.’s study concluded that PRP was associated with greater improvement in long-term pain intensity and function than corticosteroids or autologous blood. However, in the short term, CS was associated with the greatest improvement [16]. Linnanmäki et al. designed a randomized, placebo-controlled trial comparing PRP, autologous blood, and saline injections in the treatment of LE. The authors concluded that PRP or autologous blood injections did not improve pain or function at 1-year follow-up compared to those who received a saline injection, so they do not recommend their use [17]. Simental-Mendía et al. reviewed the effects of platelet-rich plasma (PRP) injection versus placebo (saline injection) on pain and joint function in LE, in five randomized placebo-controlled trials with a total of 276 patients. PRP injection was not superior to placebo. However, patients reported improvement after both interventions in clinical parameters. Further randomized trials are needed to determine whether PRP injection is clinically more effective than placebo (saline injection) [18].
A current Cochrane review concludes that PRP or autologous blood injection therapies are likely to provide little or no clinically important benefit for pain or function (moderate evidence of certainty) and cause pain and carry a small risk of infection. Without evidence of benefit, the costs and risks are not justified [19]. In addition, much more research is needed to determine the optimal PRP formulation (e.g., high or low leukocyte concentration) that is effective in providing long-term pain relief in chronic LE.
12.6.6.4 Stem Cell Injections
They can be fat-derived, bone marrow-derived, or allogeneic. All the studies are of less than 20 patients and of short follow-up, so no clear conclusions can be drawn.
12.6.6.5 Botulinum Toxin A Injections
Botulinum toxin A injections act by decreasing muscle tension at the tendon origin, which promotes pain improvement. Randomized studies show conflicting evidence of pain reduction, and all studies show reduced grip strength for several weeks after injection. Many patients also experience transient weakness in finger extension. This therapy does not improve quality of life and is therefore less favorable. Overall, the current evidence on the use of botulinum toxin is insufficient and further studies on optimal dosing and administration are needed.
12.6.6.6 Prolotherapy
It consists of an injection composed of a hypertonic glucose solution that is believed to stimulate healing and strengthening of degenerative tendon tissue by inciting inflammation followed by collagen deposition and remodeling. Multiple randomized studies have been conducted with conflicting evidence on efficacy, pain scores, and grip strength.
12.6.6.7 Percutaneous Radiofrequency
Percutaneous radiofrequency consists of the introduction of a radiofrequency electrode, usually guided by ultrasound at the origin of the musculature. The thermal lesion produces a micro-rupture of the tendon with subsequent repair. It shows promising results, comparable to those of open surgery [20].
12.7 Surgical Treatment
In general, surgical treatment is reserved for patients who do not improve after the application of several conservative treatment modalities (lasting more than 6 months) and provided that other concomitant pathology is ruled out. As mentioned above, the vast majority of patients tend to improve; however, 4%–10% of recalcitrant LE patients who are not satisfied with nonsurgical modalities may require surgical intervention, with “good” or “excellent” results in 80%–90% of cases.
All surgical techniques are based on debridement and resection of the angiofibroblastic tissue with or without subsequent tendon repair. This debridement can be performed open, percutaneously, or arthroscopically. There is still controversy and little evidence as to which technique is superior. Three factors affect the choice of treatment: (1) the ability to visualize the elbow joint (to rule out other pathologies), (2) the complication rate, and (3) the duration of the surgical procedure. Some surgeons perform hybrid techniques associating surgical techniques with injections.
12.7.1 Open Techniques
These are the most commonly used and aim to debride the origin of the ECRB tendon through an incision over the lateral epicondyle. In the classic Nirschl technique [21], a controlled debriding of the ECRB is performed, the fibers are divided longitudinally, and the angiofibroblastic tissue is resected. Subsequently, the tendon can be repaired or lengthened, along with various gestures such as decortication or epicondyle perforation to promote blood supply and healing. The author reported a 97.7% improvement in a series of 88 elbows.
In 2008 Dunn et al., in a retrospective study, demonstrated sustained high rates of long-term satisfaction for 139 procedures using the Nirschl mini-open surgical technique, with a 97% improvement rate over an average of 12.6 years of follow-up after surgery [22].
Coleman et al. reported their 15 years of experience in the treatment of refractory LE. Among 158 consecutive patients treated with open surgery, 94.6% achieved good or excellent results with a mean follow-up of 9.8 years [23]. However, these results were not compared with the control group.
The open technique provides direct visualization of the lesion and provides excellent results, decreasing the surgical time and the cost of surgery when compared with other surgical techniques. On the other hand, it has been observed that it presents a slight increase in the infection rate. Also, excessive tissue resection can affect the lateral ligamentous complex, producing joint instability.
12.7.2 Percutaneous Release
This procedure involves the release of the extensor carpi radialis brevis using local anesthesia at the point of origin at the epicondyle. Mill’s manipulation (full elbow extension with full forearm pronation and full wrist flexion) is then performed [24]. Nazar et al. reported good results with this technique despite being a relatively simple procedure. It is performed as an outpatient procedure and no complications have been reported, with complete pain relief in 87% off the cases. However, this procedure remains controversial [25].
In recent years, a novel technique called ultrasound-guided percutaneous tenotomy (UGPT) has been reported as a safe and effective procedure for the treatment of LE, with lasting improvements in terms of symptoms, function, and ultrasound imaging at 1-year follow-up. Seng et al. demonstrated in a series of 20 patients that this procedure provides sustained pain relief and functional improvement for recalcitrant cases at 3-year follow-up. They state that it is one of the few procedures that demonstrates positive sonographic evidence of tissue healing response [26]. Recently, Chalian et al. saw in 37 patients that UGPT significantly improves symptoms and function in patients with LE, also with long-term follow-up over 3 years. Post-procedure rehabilitation was associated with improved response to treatment and the authors suggest it should be considered after UGPT [27]. Ang et al. have shown that these UGPT results are maintained over the longer term, 90 months in 20 patients [28].
12.7.3 Arthroscopic Technique
In recent years, the arthroscopic technique has become increasingly popular. The patient is placed in lateral or supine decubitus and two portals are usually used. Both debridement and tendon repair can be performed arthroscopically. The main advantage, in addition to the lower aggressiveness, is that it allows assessment and treatment of concomitant intra-articular pathology, such as plicae or osteochondritis dissecans. However, arthroscopy has a high learning curve, prolongs surgical time, and is not exempt from producing iatrogenesis (e.g., injury to the lateral ulnar collateral ligament or the posterior interosseous nerve). Also, tissue resection may be incomplete. Jerosch et al. reported good results for this technique in Germany [29]. Baker described improvement in 26 of 30 (97%) patients in whom pathologic tissue is debrided by arthroscopy at a mean follow-up of 130 months, suggesting that the long-term benefits of arthroscopic release are sustained over time [30]. Behazin and Kachooei described, in a prospective study of 11 patients, the use of a no. 11 scalpel to cut the ECRB tendon perpendicular to its fibers at the level of the radiocapitellar joint, which requires a shorter operating time compared to tissue debridement [31].
In general, excellent results have been reported with the arthroscopic technique, similar in effectiveness to those of open techniques [32]. The vast majority of patients who undergo surgery present good clinical results. However, there are a number of cases with no improvement despite the surgical treatment. Among the causes of surgical failure are infection, technical errors (over- or under-resection/repair), the patient’s occupational interests, or failure to diagnose concomitant pathology.
12.8 Results
12.8.1 Surgical Versus Nonsurgical
The main dispute about surgical interventions for LE concerns their effectiveness compared to wait-and-see, conservative, or less invasive procedures. A recent systematic review by Bateman et al. suggests that surgical interventions are no more effective than nonsurgical and sham interventions. Procedural modifications may improve the comparative effectiveness of surgical interventions. High-quality randomized controlled trials are lacking, and specifically none has compared surgery with a placebo intervention [33].
Merolla et al. performed a prospective study of 101 patients randomized to PRP injection or arthroscopic ECRB release and found that PRP patients experienced significant worsening of pain at 2 years, while arthroscopic release ensured better long-term outcomes in terms of pain relief and recovery of grip strength [34]. Watt et al. performed a prospective study randomizing LE patients to open surgical release (41 patients) or leukocyte-rich PRP injection (40 patients). Leukocyte-rich PRP and surgery produced an equivalent functional outcome, but surgery may result in lower pain scores at 12 months. Seventy percent of patients treated with platelet-rich plasma avoided surgery [35]. Boden et al. retrospectively compared the effects of PRP versus UGPT procedures in the treatment of medial and lateral epicondylitis. No statistically significant differences were found between the two treatment modalities. They concluded that PRP and UGPT procedures were effective regarding pain relief, improvement of function, and quality of life [36].
12.8.2 Open Versus Arthroscopic
Overall, a small number of comparative studies suggest that open and arthroscopic techniques are comparable and highly effective for the treatment of chronic LE. Moradi et al. in a systematic review of clinical outcomes of open versus arthroscopic surgery for LE suggested that, despite no superiority for either technique in terms of pain relief, subjective function, and better rehabilitation, postoperative complications were significantly higher in the open group compared to the arthroscopic procedure (57.3% vs. 33.4%; p = 0.001) [37].
Wang et al. performed a systematic review and meta-analysis of trials comparing arthroscopic versus open debridement. There was no significant difference between arthroscopic and open surgery with respect to failure rate, functional outcome score, and complication rate. The meta-analysis found that arthroscopic surgery had a longer operative time than open surgery for LE [38].
12.8.3 Open Versus Arthroscopic Versus Percutaneous
All three surgical techniques for the treatment of LE demonstrate excellent results. There is moderate evidence that there are no clinically significant differences between the three surgical techniques (open, arthroscopic, and percutaneous) in terms of functional outcome (Disabilities of the Arm, Shoulder, and Hand [DASH]), pain intensity (visual analog scale [VAS]), and patient satisfaction at 1-year follow-up [39]. In contrast, Pierce et al. found that open and arthroscopic approaches resulted in higher DASH scores than the percutaneous approach, with no difference in satisfaction or complication rates. Of note, the open approach was also associated with more postoperative pain and a slightly higher risk of infection [40].
Some of the limitations of these studies include a small population size and lack of randomization. Overall, the current evidence suggests that all three surgical approaches are highly effective in the treatment of LE, and larger randomized clinical trials are needed to delineate any clinically meaningful differences between the approaches.
12.9 Conclusions
Conservative treatment resolves 90% of cases of LE. Conservative treatments can reduce the need for surgical intervention in LE. This has important cost-saving implications, as the surgical cost for LE is estimated to be between $10,000 and $12,000 [41]. NSAIDs, rehab, orthoses, and shock waves are less effective for chronic cases. CS injection, which was initially considered the gold standard treatment, may be effective in the short term, but has reduced benefit in the long term, which may be related to structural weakening of the tendon and inhibition of tenocytes. There is controversy about its effect on tendonocyte structure and healing. PRP and autologous blood are more effective in the medium term than steroids for the treatment of LE and have minimal side effects.
Controversy still persists over the best surgical approach for the management of LE. Current evidence demonstrates that open, arthroscopic, and percutaneous surgical approaches are all very effective. Arthroscopic and percutaneous approaches may provide faster recovery and earlier return to work. Open surgery is the most effective in the long term, but is the most invasive and has the longest recovery.
References
Smidt N, van der Windt DAWM. Tennis elbow in primary care. BMJ. 2006;333:927–8.
Shiri R, Viikari-Juntura E, Varonen H, Heliövaara M. Prevalence and determinants of lateral and medial epicondylitis: a population study. Am J Epidemiol. 2006;164:1065–74.
Orchard J, Kountouris A. The management of tennis elbow. BMJ. 2011;342:d2687.
Shergill R, Choudur HN. Ultrasound-guided interventions in lateral epicondylitis. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis. 2019;25:e27–34.
Sasaki K, Tamakawa M, Onda K, Iba K, Sonoda T, Yamashita T, et al. The detection of the capsular tear at the undersurface of the extensor carpi radialis brevis tendon in chronic tennis elbow: the value of magnetic resonance imaging and computed tomography arthrography. J Shoulder Elb Surg. 2011;20:420–5.
Menta R, Randhawa K, Côté P, Wong JJ, Yu H, Sutton D, et al. The effectiveness of exercise for the management of musculoskeletal disorders and injuries of the elbow, forearm, wrist, and hand: a systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) collaboration. J Manip Physiol Ther. 2015;38:507–20.
Ma KL, Wang HQ. Management of lateral epicondylitis: a narrative literature review. Pain Res Manag. 2020;2020:6965381.
Pattanittum P, Turner T, Green S, Buchbinder R. Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database Syst Rev. 2013;5:CD003686.
Yao G, Chen J, Duan Y, Chen X. Efficacy of extracorporeal shock wave therapy for lateral epicondylitis: a systematic review and meta-analysis. Biomed Res Int. 2020;2020:2064781.
Zheng C, Zeng D, Chen J, Liu S, Li J, Ruan Z, et al. Effectiveness of extracorporeal shock wave therapy in patients with tennis elbow: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2020;99(30):e21189.
Calandruccio JH, Steiner MM. Autologous blood and platelet-rich plasma injections for treatment of lateral epicondylitis. Orthop Clin North Am. 2017;48:351–7.
de Vos RJ, Windt J, Weir A. Strong evidence against platelet-rich plasma injections for chronic lateral epicondylar tendinopathy: a systematic review. Br J Sports Med. 2014;48:952–6.
Houck DA, Kraeutler MJ, Thornton LB, McCarty EC, Bravman JT. Treatment of lateral epicondylitis with autologous blood, platelet-rich plasma, or corticosteroid injections: a systematic review of overlapping meta-analyses. Orthop J Sports Med. 2019;7:2325967119831052.
Arirachakaran A, Sukthuayat A, Sisayanarane T, Laoratanavoraphong S, Kanchanatawan W, Kongtharvonskul J. Platelet-rich plasma versus autologous blood versus steroid injection in lateral epicondylitis: systematic review and network meta-analysis. J Orthop Traumatol Off J Ital Soc Orthop Traumatol. 2016;17:101–12.
Vaquero-Picado A, Barco R, Antuña SA. Lateral epicondylitis of the elbow. EFORT Open Rev. 2016;1:391–7.
Tang S, Wang X, Wu P, Wu P, Yang J, Du Z, et al. Platelet-rich plasma vs autologous blood vs corticosteroid injections in the treatment of lateral epicondylitis: a systematic review, pairwise and network meta-analysis of randomized controlled trials. PM R. 2020;12:397–409.
Linnanmäki L, Kanto K, Karjalainen T, Leppänen OV, Lehtinen J. Platelet-rich plasma or autologous blood do not reduce pain or improve function in patients with lateral epicondylitis: a randomized controlled trial. Clin Orthop Relat Res. 2020;478:1892–900.
Simental-Mendía M, Vilchez-Cavazos F, Álvarez-Villalobos N, Blázquez-Saldaña J, Peña-Martínez V, Villarreal-Villarreal G, et al. Clinical efficacy of platelet-rich plasma in the treatment of lateral epicondylitis: a systematic review and meta-analysis of randomized placebo-controlled clinical trials. Clin Rheumatol. 2020;39:2255–65.
Karjalainen TV, Silagy M, O’Bryan E, Johnston RV, Cyril S, Buchbinder R. Autologous blood and platelet-rich plasma injection therapy for lateral elbow pain. Cochrane Database Syst Rev. 2021;9(9):CD010951.
Lee J-H, Park I, Hyun H-S, Shin S-J. A comparison of radiofrequency-based microtenotomy and arthroscopic release of the extensor carpi radialis brevis tendon in recalcitrant lateral epicondylitis: a prospective randomized controlled study. Arthroscopy. 2018;34:1439–46.
Nirschl RT. Lateral epicondylitis/tendinosis. In: Morrey B, Sanchez-Sotelo J, Morrey M, editors. Morrey’s the elbow and its disorders. Elsevier; 2018. p. 574–81.
Dunn JH, Kim JJ, Davis L, Nirschl RP. Ten- to 14-year follow-up of the Nirschl surgical technique for lateral epicondylitis. Am J Sports Med. 2008;36:261–6.
Coleman B, Quinlan JF, Matheson JA. Surgical treatment for lateral epicondylitis: a long-term follow-up of results. J Shoulder Elb Surg. 2010;19:363–7.
Yigit Ş. Medium-term results after treatment of percutaneous tennis elbow release under local anaesthesia. Acta Biomed. 2020;91:305–39.
Nazar M, Lipscombe S, Morapudi S, Tuvo G, Kebrle R, Marlow W, et al. Percutaneous tennis elbow release under local anaesthesia. Open Orthop J. 2012;6:129–32.
Seng C, Mohan PC, Koh SBJ, Howe TS, Lim YG, Lee BP, et al. Ultrasonic percutaneous tenotomy for recalcitrant lateral elbow tendinopathy. Am J Sports Med. 2015;44:504–10.
Chalian M, Nacey NC, Rawat U, Knight J, Lancaster T, Deal DN, et al. Ultrasound-guided percutaneous needle tenotomy using Tenex system for refractory lateral epicondylitis; short and long-term effectiveness and contributing factors. Skelet Radiol. 2021;50:2049–57.
Ang BFH, Mohan PC, Png MA, Allen JC Jr, Howe TS, Koh JSB, et al. Ultrasonic percutaneous tenotomy for recalcitrant lateral elbow tendinopathy: clinical and sonographic results at 90 months. Am J Sports Med. 2021;49:1854–60.
Jerosch J, Schunck J. Arthroscopic treatment of lateral epicondylitis: indication, technique and early results. Knee Surg Sports Traumatol Arthrosc. 2006;14:379–82.
Baker CL Jr, Baker CL 3rd. Long-term follow-up of arthroscopic treatment of lateral epicondylitis. Am J Sports Med. 2008;36:254–60.
Behazin M, Kachooei AR. Arthroscopic recession technique in the surgery of tennis elbow by sharp cutting the extensor carpi radialis brevis (ECRB) tendon origin. Arch Bone Jt Surg. 2021;9:174–9.
Savoie FH, O’Brien MJ. Arthroscopic tennis elbow release. Instr Course Lect. 2015;64:225–30.
Bateman M, Littlewood C, Rawson B, Tambe AA. Surgery for tennis elbow: a systematic review. Shoulder Elbow. 2019;11:35–44.
Merolla G, Dellabiancia F, Ricci A, Mussoni MP, Nucci S, Zanoli G, et al. Arthroscopic debridement versus platelet-rich plasma injection: a prospective, randomized, comparative study of chronic lateral epicondylitis with a nearly 2-year follow-up. Arthroscopy. 2017;33:1320–9.
Watts AC, Morgan BW, Birch A, Nuttall D, Trail IA. Comparing leukocyte-rich platelet-rich plasma injection with surgical intervention for the management of refractory tennis elbow. A prospective randomised trial. Shoulder Elbow. 2020;12:46–53.
Boden AL, Scott MT, Dalwadi PP, Mautner K, Mason RA, Gottschalk MB. Platelet-rich plasma versus Tenex in the treatment of medial and lateral epicondylitis. J Shoulder Elb Surg. 2019;28:112–9.
Moradi A, Pasdar P, Mehrad-Majd H, Ebrahimzadeh MH. Clinical outcomes of open versus arthroscopic surgery for lateral epicondylitis: evidence from a systematic review. Arch Bone Jt Surg. 2019;7:91–104.
Wang W, Chen J, Lou J, Shentu G, Xu G. Comparison of arthroscopic debridement and open debridement in the management of lateral epicondylitis: a systematic review and meta-analysis. Medicine (Baltimore). 2019;98(44):e17668.
Burn MB, Mitchell RJ, Liberman SR, Lintner DM, Harris JD, McCulloch PC. Open, arthroscopic, and percutaneous surgical treatment of lateral epicondylitis: a systematic review. Hand (N Y). 2018;13:264–74.
Pierce TP, Issa K, Gilbert BT, Hanly B, Festa A, McInerney VK, et al. A systematic review of tennis elbow surgery: open versus arthroscopic versus percutaneous release of the common extensor origin. Arthroscopy. 2017;33:1260–8.
Lai WC, Erickson BJ, Mlynarek RA, Wang D. Chronic lateral epicondylitis: challenges and solutions. Open Access J Sports Med. 2018;9:243–51.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Encinas-Ullán, C.A., Gómez-Cardero, P., Rodríguez-Merchán, E.C. (2022). Controversies in Tennis Elbow in Adults: Should We Ever Operate?. In: Rodríguez-Merchán, E.C., Moreno-Garcìa, A. (eds) Controversies in Orthopedic Surgery of The Upper Limb . Springer, Cham. https://doi.org/10.1007/978-3-031-04907-1_12
Download citation
DOI: https://doi.org/10.1007/978-3-031-04907-1_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-04906-4
Online ISBN: 978-3-031-04907-1
eBook Packages: MedicineMedicine (R0)