
Abstract
This chapter provides an overview of self-determination theory (SDT) used in oral healthcare practice and research. Interventions promoting autonomy-supportive dental competence, relative to standard care, yielded increase in autonomous motivation, perceived dental competence, and oral hygiene behaviours (e.g. brushing, flossing, more regular meals), decrease in dental plaque and improved oral health. Moreover, the interventions affected more frequent dental attendance and oral health-related quality of life. SDT provides a strong empirical basis that demonstrates the importance of operationalising the core principles of autonomy support, basic psychological needs and motivation to enhance patients’ oral health and oral health-related quality of life.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Autonomy supportive and controlling oral healthcare professionals
- Basic psychological need satisfaction and frustration
- Autonomous motivation
- Controlled motivation
- Oral health behaviour
- Oral health
- Oral health-related quality of life
-
Learn about the importance of autonomy and self-regulation in self-determination theory (SDT) in order to improve oral health
-
Learn about why autonomy is one of the most important of moral pillars in biomedical ethics, professionalism and informed consent related to oral health choices and challenges
-
Learn about the three basic psychological needs (BPN) in SDT, and how they are connected to autonomy support, learning, motivation and mastery of oral health
-
Learn about how to give patients autonomy support related to their own oral health challenges
-
Learn about the internalisation process and how different motivational regulations are related to different oral health behaviours
1 Introduction to Self-Determination Theory (SDT)
Self-determination theory (SDT), developed by Edward L. Deci and Richard M. Ryan [1], is a modern empirical macro-theory of human motivation. SDT [2] is one of the most researched and applied theories of human motivation in the field of psychology.
Motivation lies in the human nature. When we are motivated, we are active, engaged and curious. We are inspired, and we want to learn, develop and master new skills. Most people want to make great efforts, but it is also clear that some individuals are passive and alienated [3].
SDT is anchored in Carl Rogers [5] and his humanistic perspectives such as unconditional positive regard, authenticity, warmth, empathy and patient centeredness, thus being sensitive to patients’ psychological and social needs.
The SDT theory can explain how and why motivation is important in most contexts and situations [6].
Further, SDT is concerned with how dental professionals can give autonomy support and how this generates patient’s autonomous motivation, self-regulation and relevant oral health changes.
Autonomous motivation and self-regulation, in SDT research, have shown positive impacts on oral health changes, decrease in dental anxiety, increase in well-being and oral health-related quality of life besides maintaining positive dental health behaviour over time [7,8,9,10].
A fundamental issue in SDT is how dental professionals are able to implement counsel and guide autonomy support in a non-controlling and non-conditional way [11].
SDT represents patient centredness and a holistic patient view by focusing on the biopsychosocial model by Engel and Williams & Deci [12, 13].
“Autonomy support instantiates the type of provider behavior that is widely advocated by adherents to the biopsychosocial approach to medicine” [13, p. 767].
When implementing SDT in oral health interventions, we can understand more about what lies behind motivational processes related to changes in oral health behaviour, patient’s well-being and oral health quality of life. This is fundamental in order to be able to help patients in a better way in the future to manage oral health challenges [10, 14].
1.1 Ethical Considerations Using Autonomy
The concept of autonomy has become increasingly accepted in all health contexts and has become one of the most important of moral pillars. This is considered an ethical mandate for medicine [15].
Autonomy support is a factor that makes SDT particularly useful in health care contexts because it is consistent with biomedical ethics [16], medical professionalism [17] and informed consent [17, 18]. Clinical practitioners are, therefore, obligated to respect autonomy regardless of the theoretical frame they are using [15]. Emphasis on patient autonomy has been widely embraced in physician charters [17].
Biomedical ethics claims that autonomous motivation and self-regulation are important health outcomes in itself. SDT is, therefore, consistent with tenets of clinical practice as medical professionalism and principles of biomedical ethics.
1.2 Autonomy and Self-Regulation
Autonomy is derived from the Greek words “autos” (self) and “nomos” (rule). Autonomy refers to self-regulation and self-endorsement [19]. Autonomous people experience ownership of their behaviour [2].
When people are self-ruled and self-motivated, they will be able to make volitional and personal choices which generate their own energy, implicitly feeling vital and moving forward [20].
“SDT is concerned about how autonomy develops, and how it can be either diminished or facilitated by specific biological and social conditions. SDT has attention on the interplay between inherent tendencies toward integrated vital functioning, but also pays attention to peoples vulnerabilities to being controlled” [19, p. 1562].
2 Basic Psychological Needs (BPN)
SDT focuses mainly on three basic psychological needs (BPN): competence, autonomy and relatedness. BPN are fundamental for personal growth, optimal functioning, well-being and quality of life. The satisfaction of BPN is essential for people to be fully functioning, actualise their potentials, to flourish, and being protected from stress, ill-health and maladaptive functioning [2].
Deci and Ryan [1] point out that our behaviour is governed by a desire to cover and satisfy the three inner BPN [3]. BPN can help explain why only some behaviours will enhance well-being and some will produce pathological consequences, for example, somatisation.
The three BPN are universal and fundamental to all people in all cultures [2].

2.1 The Need for Autonomy and Self-Determination
The need for autonomy is related to when you feel you can execute personal, important and volitional choices willingly. Persons feel they have a personal and valued ownership of their behaviour. The need for autonomy implies the need to experience that one is in control over one's own actions, thus self-initiating and self-regulating these actions. According to Deci and Ryan [1], individuals have an inner need to perceive themselves as the source of their own actions. Internally self-controlled and autonomous persons want to act on the basis of voluntariness related to their own interests, engagements and integrated values [1, 2, 21]. The need for autonomy means that we experience self-determination, and it contributes to make more self-conscious and more aware (mindful), strategic and meaningful choices [2]. When patients can make their own autonomous choices and develop valued and rational competence fitting into their own self, they become more and more self-regulated and appropriately competent related to their own goals and a given behaviour [21].
Example
Example of support for the need for autonomy: When patients experience receiving support for the need for autonomy, they will experience that they can freely and effortlessly convey their own thoughts , reflections and feelings. Thus, they will more easily be able to ask questions and tell about their own needs and choices. Patients experience that they can more openly discuss different treatment options with dental personnel. In this way, patients feel that they have the opportunity to make more autonomous, competence- generating and relatedness-building, self-determined and self-regulated choices. The patients experience that they more easily can be themselves and that they honestly and authentically master to convey, for example, their own frustrations by not being able to lie down in the dental treatment chair or express clearly about pain experiences or other discomforts that can occur in treatment situations [22].
2.2 The Need for Competence and Mastery
The need for competence refers to the need to master and thus be able to experience oneself as a self governed chief who is able to solve challenges and tasks, perform an appropriate behaviour and, therefore, be able to achieve the desired goals and results. Competence refers to the need to experience making important and relevant effects in the environment. Patients who feel the oral health competence need supported, know themselves as effective and skilled when executing tasks related to oral health challenges [1].
The need for competence is also related to when you feel capable and effective in interactions with people in the environment. Persons who seek optimal challenges make efforts along with strategic thinking until they master their challenges and along with this personal growth is a result [2].
The need for competence represents individuals’ desire to feel they have appropriate knowledge and at the same time perceive themselves as capable, competent and able to develop and bring about reasoned, important new skills [23]. A supported competence need involves an understanding of how to attain various external and internal outcomes, and at the same time feeling efficacious in performing the requisite behaviors.
Example
Example of support for the need for competence: When the need for competence is supported in dental treatment situations, patients experience that they master taking care of their dental health. They are able to perform their own dental home care qualitatively well. They will use their effort to master their oral challenges well, and they experience mastering the challenges in a meaningful and appropriate way.
Research has shown that positive feedback provides satisfaction for the need for competence, which signifies direct and concrete effect on mastering in different situations, thus enhancing more intrinsic autonomous and self-regulated motivation. Negative feedback conveys negative effects and tends to thwart the need for competence and thus undermine intrinsic autonomous self-regulated motivation [2].
2.3 The Need for Relatedness and Belonging
The need for relatedness is about sharing intimacy and to establish close emotional bonds and attachment with other people depending on interpersonal, friendly and warm relationships. Relatedness need is about feeling socially connected and being engaged in giving and receiving of care and attentiveness from significant people in one’s life.
Relatedness, belonging and socialising are basic human needs that help develop the opportunity for close relationships built on mutual trust, respect and benevolence, accept and recognition. Being able to experience that someone cares about you establishes social ties and when someone can be present for you, it is of significant importance in order to satisfy wellness and support for the relatedness need. Experience of cohesion with the environment and society in general is of great importance for relatedness need satisfaction [2]. Relatedness and belongingness involve developing secure and satisfying connections and collaborations with significant and important persons [24].
Example
Example of support for relatedness: When the need for relatedness is supported, the patient experiences he has a good connection and relationship with dental personnel. Patients feel safe, well, natural, authentic and relaxed in the treatment situation. Experiencing a pleasant atmosphere that helps patients feel comfortable with the dental personnel is important when building relatedness and collaboration around dental health challenges. The patients experience that the dental personnel both see them as a person and listen to what they convey during the entire treatment session. In this way, patients experience dental personnel as friendly, aware and attentive, which supports the relatedness need.
When all the three BPN are met and satisfied, patients are able to develop sufficient inner autonomous and self-regulated motivation, and they are now able to learn optimally and master challenges related to their own dental health and sustain long-lasting oral health promotion and preventive behaviour [2].
Thus, for the dental personnel, it is important to be able to satisfy all the three BPN of patients. This can be done when using the SDT guidelines (see later in this chapter).
Behaviours which lead to satisfaction of the three BPN will enhance autonomous motivation and self-regulation, personal growth and well-being [2].
The need support promotes positive emotions and more autonomous motivation to continue a given behaviour even though this behaviour sometimes can be challenging, strenuous or even boring [2].
When dental personnel are able to provide highly individualised and differentiated counseling that satisfies the three BPN, this will facilitate integration of more autonomous motivation and self-regulation . In this way, patients are more likely to achieve their oral health goals. When dental personnel thwart or frustrate psychological needs in dental treatment, negative oral health consequences will arise [25].
2.4 Need Thwarting – Need Frustration
Dental professionals who do not take into consideration patients’ individual differences or support BPNs will undermine patients personal growth. This hindering or thwarting of BPN will be associated with lower autonomous motivation, less self-regulated motivation, difficulties in mastering oral health challenges and diminished well-being [2].
Autonomous motivation will not be facilitated when need-thwarting or need-frustrating situations arise in the course of treatment. Thwarting of BPN is a consequence of dental professionals who want to control their patients. Control are for example, negative evaluations, withdrawal of attention and criticism. Controlling personnel lead patients to become more vulnerable and this may lead to dental anxiety. As a consequence of this control, patients often will avoid dental appointments [26].
Examples also include dental professionals who dominate the conversation, minimise the patient’s choices, instruct the patient on what he/she “should or must do” or give few or no rationales for reflection. This will not be in line with giving autonomy support [15].
3 Guidelines for Autonomy Support
Autonomy support is consistent with support of the three BPN [2]. SDT guidelines can provide a basis for appropriate guidance to promote, enhance and change dental health behaviour besides preventing and decreasing dental anxiety, increasing dental well-being and oral health quality of life [10]. Research shows that patients can learn to become more autonomously motivated and self-regulated.
3.1 Autonomy Support
Autonomy support is a motivating style, and it is an important issue in SDT. Autonomy support is connected to how the three BPN (autonomy, competence and relatedness) are addressed and supported in diverse contexts [2]. Autonomy support can facilitate more self-determined regulation for uninteresting activities like tooth brushing [28].
Autonomy support is about when dental personnel are non-judgemental, aware of the patient’s feelings and perspectives, provide appropriate explanations and rationales when self-determined choices are given, and at the same time focus on minimising pressure and control in all situations [2, 26].
Autonomy support concerns making the patients more aware and involve them in their own oral health situation and encourage them to become more self-determined related to choices and decisions. Dental personnel listen to the patients’ own reflections, stimulate them to ask questions and they ask questions in order to stimulate additional reflections, thus opening up for a more meaningful dialogue. Autonomy supportive dental professionals will stimulate and promote more autonomous self-regulation and self-directed motivation towards patients’ own dental health goals [2].
Integration of appropriate dental health behaviour will, according to Deci and Ryan [21], depend on whether significant persons like dental personnel and the environment provide sufficient autonomy support.
Providing choices implies that patients are being involved in planning and discussions related to different treatment or behavioural options together with dental personnel. When patients feel they can talk more freely and authentically with their dental professionals, it will be easier for them to decide on what is the best alternative and solution for themselves [22].
3.2 Autonomy – Guiding to Choice Rather Than Control
Developing autonomous motivation, self-regulation and self-management is challenging work in many health care contexts, but first and foremost, it is all about not pressing or controlling the patient’s feelings, thoughts, choices, goals and behaviours [29].
Resistance and low autonomous motivation are natural reactions along with many change processes. It is worth to remark, if dental personnel are too eager to focus on change or outcomes, it will create a feeling of control and pressure. Patients have to feel they are going through the change process in their own way and in their own rhythm. Outcome-focused dental personnel who follow their own treatment goals instead of focusing on patient’s own goals for treatment, will be using a controlling style. This feeling of pressure will not be in line with autonomy support.
Tip
When counselling, dental professionals can be trained to develop awareness and emphasis on avoiding words as: “you could, you should or you must do” in order to be less controlling.
Autonomy support gives patients a sense of being in their own control, they are their own chief, and therefore, they feel they are in charge. This is because autonomy relates to self-control. Dental professionals can teach patients to feel in control in many ways. For example, to raise their hand in order to stop treatment, they can hold their own saliva-ejector, or hold their own X-ray holders in order to feel in control. When dental professionals stimulate patients to make choices and be more self-determined in treatment, can lead patients to be more self- conscious. Thus, over time, patients can learn to be more able to make more relevant and autonomous choices for themselves. When patients have a feeling of being in control, can result in a more authentic dialogue, because patients now feel more recognised and believed in. Because of this, patients now can express their feelings and thoughts more freely and directly. Patients will feel more in control when dental personnel ask more open-ended questions instead of close-ended questions. Asking questions about how patients are feeling, thinking and reacting in dental treatment sessions is important in order to understand and be able to communicate properly about patients needs. Dental personnel can train patients to be more aware of their own thinking and reactions. This is important in order to make appropriate plans together. These conversations can hopefully lead to more autonomous motivation in patients, being more aware of choosing of oral health promotive behaviour, which implies prevention and decrease of dental anxiety, increase in oral well-being and oral health quality of life [7,8,9, 26].
Dental professionals can provide patients with advices or recommendations when it is done in an autonomy supportive way. Dental professionals have to have in mind that it is easy for patients to view dental personnel as authorities, and therefore, understand and interpret their words as controlling, even if it is not meant to be [11].
Dental professionals are experts in their field, and therefore, they need to provide relevant, evidence-based and understandable information along with structure for their patients [2]; this in order to give patients informative, comprehensive, personally useful and appropriate information about their oral health challenges, health risks, and consequences regarding the patients’ own health goals. Important questions are: “What are the patients concerned about?” “What is important to inform patients about?” and “What is necessary to have an appropriate conversation around?” Informed consent is important to have in mind when giving this information [30].
When patients are given the opportunity to actively participate in a dialogue and reflect upon the pros and cons related to what they feel and think are important issues that matter for themselves they often will feel more involved, and hopefully more secure, satisfied and comfortable with their choices.
Feedback is importantly related to autonomy and mastery in executing different behaviours. It is only when we provide opportunities for willingness and choice that development of intrinsic autonomous motivation and self-regulation can be realised [7].
Research shows that when patients have the opportunity to make their own choices, long-lasting changes in behaviour can occur [31].
3.3 Competence – Providing Meaningful Rationales and Explaining Purposes
Competence is about creating a meaningful rationale. Meaningful and appropriate rationales have to be constructed in collaboration with the patients. The patients have to understand why a behaviour is important to perform. A meaningful and appropriate rationale is for example explaining: “Why is it important to brush our teeth?”
When dental personnel guide patients to change behaviour, it is important to provide meaningful and appropriate justifications.
Patients who feel sufficiently informed can develop relevant competence and mastery in order to make significant and appropriate choices for themselves. Dental personnel can encourage exploration when choices are to be made and thus help with appraisals and decisions. Dental personnel, who are counselling in order to give the patients the possibility to develop experience of self-regulation, self-control, personal valuable competence and efficiency of the activity, will probably succeed more often in helping patients to improve their oral health.
A constructive collaboration between patients and dental personnel is a valuable opportunity to build trusting relationships and to activate and motivate patients in order to develop their own meaningful and appropriate competence.
It is important for dental personnel to familiarise with the perspectives and assumptions that form the basis for patients being able to understand and apply knowledge and information that is provided in oral health care contexts, and thereafter build new perspectives and more effective competence together with patients [8, 32].
It is important to support patients’ own progress (in most cases, this takes time) related to their own autonomous goals they are pursuing and when self-determined competence is developing at the same time.
To improve perception of competence, the tasks ought to be tailored to the capacity, ability and resources of the patients, but at the same time one can give support to patients optimal challenges and believe in their ability to achieve their own goals [2]. With optimal challenges and goals, dental personnel show confidence in patients’ efficiency, believing they can manage their own oral health challenges.
The experience of being able to choose and being able to make self-determined decisions relates to the experience of being competent and this leads to the patient’s personal growth [14].
Dental professionals who optimise competence and support needs will significantly be contributing to patients, making a greater effort to learn more about their oral health and improve their own skills. This can contribute to better perception of their own ability, their own effects on oral health, and thus facilitate more autonomous self-regulated motivation [33].
Research supports the importance of supporting the patient’s autonomous motivation, competence conceptualisation and development of new skills and how patients can use their capacities efficiently to emphasise greater control over their oral health and the factors that create promotion of oral health [7].
For dental professionals, it is important to consider what relevant competence is especially important for different patient groups to learn about?
“The highest quality of conceptual learning seems to occur under the same motivational conditions that promote personal growth and adjustment” [34, p. 326].
3.4 Relatedness – Acknowledging the Patient’s Feelings and Perspectives
Dental professionals, who take into consideration patient’s feelings, perspectives and respect their frame of reference, will support relatedness and the feeling of belonging. Along with this understanding, dental personnel have to be nonjudgemental [35].
Empathy is central and important in the feeling of relatedness. Dental professionals who emphasise empathic and compassionate styles will be able to take into consideration the patient's feelings, experiences and personal considerations in an easier way.
Dental professionals who listen carefully, are present, aware/mindful, sensitive, attentive and supportive of the patient's own thoughts, experiences, feelings, actions, goals and behaviours will give support to the need of relatedness.
When dental professionals are aware, pay extra attention to, and take into consideration every step in the treatment session [36], they learn more of the patient’s own feelings and reactions, besides they become more aware of their own feelings and reactions to these issues. For example, personnel have to take into consideration when patients expresses their feelings and reactions related to their experience of pain and discomfort, anxiety, traumas, depression, or other vulnerabilities.
Importantly, emphasising these factors can lead to increased levels of confidence and trust between patients and dental personnel, which in turn could help patients overcome fear and anxiety. Thus, this increases the patients feeling of confidence and trust [37].
Facilitating a near, accepting and warm relationship can create better cooperation and safer treatment alliances which is an important prerequisite for all patient and health personnel relationships. Focus on developing and building relatedness, related to trust and confidence, will affect learning and self-training positively and result in patients becoming more autonomously motivated, self-determined and self-regulated. This will in turn facilitate oral health competence and oral health promotion (see Nutbeam, [38], and ► Chap. 5).
The context is characterised by mutual respect when dental personnel communicate with their patients. Dental professionals who take into consideration the patient’s challenges, values and plans related to taking care of their own dental health will build more consistent and valuable relations with patients. While patients learn about their own oral health and how they can relate to this in the best possible way, the need for relatedness is important to take into consideration for dental personnel [7,8,9, 26, 32].
Dental professionals who create predictability and structure [39] will often contribute more to patients’ engagement and desire for more involvement in future activities. Positive feedback is needed for relatedness, feeling of mastery and developing competence and supporting development of more autonomy and self-regulation. Patients choosing to be more self-determined is directly connected to patients being able to take more responsibility for their own choices related to oral health. In general, dental professionals who take into account patients’ individual differences when counselling, using SDT related to autonomous motivation in learning processes, more often succeed in motivating the patients taking their own relevant oral health changes. Lack of time and stress will be a threat when patients are learning about oral health promoting issues and tasks.
Research has shown that relevant health changes are likely to occur and last over time when dental personnel are autonomy supportive and patients have integrated and accepted the options, opportunities and information given in a counselling dialogue, often followed up over time [2]. Autonomy support will facilitate internalisation of more autonomous motivation and at the same time prevent and decrease dental anxiety [26].
Research shows that when people are autonomously motivated they are more deeply engaged and productive, and they are more freely and willingly developing their own appropriate competence capital. Being autonomously motivated gives patients the possibility to make better plans in order to gain their own chosen oral health goals [40]. Autonomous motivation is related to fuller and more optimal functioning, which is essential for personal growth and mental health [21, 41].
SDT gives the opportunity to understand more of how significant persons can support and contribute related to how patients can develop optimal health function, increase their own health by using their own capacities and resources, increase general health, mental and psychological well-being and general quality of life [2].
4 Internalisation Process
The internalisation process is unique in SDT [1]. This process gives the possibility to understand different qualities of motivation. This quality is reflected in how and to what extent and degree a person is regulating his or her behaviour autonomously. Ryan and Deci [2] maintain that motivation is qualitatively different if a person is extrinsically versus intrinsically regulated, controlled versus autonomously motivated, and these concepts are predictors of health behaviours, well-being, and quality of life. Many theories of motivation have treated motivation, when only focusing on the amount of motivation, but SDT is the only theory which differentiates between qualitative types of motivation [42]. Quality of motivation is, therefore, a main theme in SDT related to the internalisation process.
Internalisation and integration is a process when a person is active and can transform an external regulation into more inner self-regulated behaviour connected with the self and their own values [43]. This process is successful if the behaviour functions optimally, when people can be able to identify with the importance of autonomous self-regulations, assimilate these regulations into their sense of self, and thus fully accept them as their own.
Autonomous self-regulation will contribute to patients being able to give more effort, have greater engagement and persistence with health behaviours [15] and oral health behaviours [32].
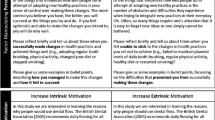
The internalisation process is presented as a continuum (◘ Fig. 8.2). This internalisation continuum shows how a person's behaviour, by different qualities, can become more autonomously self-regulated, or how persons can move up and down on this continuum.
Different extrinsic forms of regulations represent the internalisation process in SDT. The SDT refers to four different types of extrinsic motivations in the internalisation process. The four external forms start as an initiation from the outside, for example, from persons or norms from cultural contexts. In this way, the internalisation process starts from the “outside”. When individuals have become autonomously and inner motivated, they have integrated a behaviour through the internalisation process. Intrinsic motivation represents behaviour sustained with engagement and without external rewards. The rewarding experiences lie within people and we can say they are the most genuine intrinsically- motivated individuals. Amotivation refers to missing or lack of motivation [2].
4.1 Amotivation
Amotivation represents no regulation, no motivation and lack of intentions to act [2]. Patients will think they will not be doing anything, because nothing will lead to desired outcomes anyway. They feel powerless and helpless. The patients seem uninterested and indifferent. They lack the feeling of competence and mastery, either in a sense of efficacy or they have a feeling of lack of self-control [44]. A motivated patients often develop anxiety and depression [2].
Example
Example of an amotivated patient: He feels powerless and helpless, perhaps because having to “fix his teeth” feels like too much of a challenge.
4.2 Four Different Types of Extrinsic Motivation
Deci and Ryan [1] describe four different types of extrinsic motivation. Below we will consider all four regulations. Extrinsic regulations are intentional and motivated.
External and introjected regulations are called controlled motivation, while identified and integrated regulation are called autonomous motivation [45].
The process of internalisation shows how a behaviour that was originally initiated by an external influence, eventually can end up with more self-determined and autonomously motivated behaviour, which corresponds to a person who acts more self-regulated [45].
4.2.1 External Regulation
External regulation is the first of the four extrinsic motivations and the least self-determined motivation. The behaviour is controlled by external stimuli, which means that the behaviour is initiated by other people or of a context outside the person. The individual's behaviour is mainly governed by a desire related to a reward or to avoid punishment. In this regulation, other people's assessments or judgements of what the person is thinking, feeling or doing, become important [46].
Behaviour, like brushing the teeth, starts as an external regulation. Thus, this behaviour starts as an external “requirement”. Demands to perform an action can come from parents, family or friends but can also be a normative demand that lies in the environment or in the culture. Brushing our teeth is, therefore, not governed by an independent autonomous motivation from the beginning but can become an integrated, accepted and valued behaviour over time.
Example
Example of a patient with external regulation: Brushing is performed out of duty. Patients often want to “satisfy” dental personnel by being a “good” and clever patient. Patients perform their dental home care in order to avoid criticism or to get praise from dental personnel.
4.2.2 Introjected Regulation
Introjected regulation is the second type of extrinsic motivation on the internalisation continuum and is still characterised as controlled motivation. Patients have partially accepted the behaviour as their own. Introjected regulation is conceptualised as “partial internalisation” [28] and refers to patients who have “taken in” the behaviour, but who have not fully accepted it as their own. The behaviour is not self-regulated. The behaviour is still not integrated.
The patient acts mainly due to bad conscience like shame and guilt. The patient experiences that he should or must act in certain ways. Or, patients do not perform the behaviour they feel they should have executed. Introjected patients often feel an inner stress and pressure themselves to act.
Example
Example of a patient with introjected regulation: The person experiences that he should or must brush his teeth, but he really does not like to perform this behaviour. The brushing act is often executed in a mechanical and instrumental way and often performed as a self-imposed duty. Or they refrain from doing the behaviour, but at the same time they feel guilt and shame by not doing this behaviour .
4.2.3 Identified Regulation
This is the third type of extrinsic regulation. Identified regulation is the first autonomous regulation. The behaviour is now self-determined, self-regulated and the patients are therefore self- motivated. Persons feel the behaviour is important to execute for themselves, and they recognise and accept the underlying value of a behaviour. The internalisation process is now fuller than with an introjection.
Example
Example of a patient with identified regulation: The patient thinks that it is important to perform regular dental home care in an efficient and quality-conscious manner. The patient thinks it is important to care for his teeth and meet regularly with dental personnel. Patients naturally think it is important to achieve their own oral health goals; besides, they are concerned about their own oral well-being and their oral health quality of life.
4.2.4 Integrated Regulation
This regulation represents the last of the four extrinsic regulations. This is the most autonomous and self-regulated of the external regulations. The behaviour is now fully integrated within the person’s sense of self. The behaviour is consistent and in harmony with the person’s value system and other personal goals. We say the behaviour is integrated into their own value system.
Patients now experience the behaviour as their own and self-chosen and they think the behaviour is important and valuable to perform. Dental behaviour is executed out of self-interest and patients are valuing the behaviour. The priorities lie in the good feelings and experiences with doing this behaviour. When the behaviour is integrated, dental personnel do not have to inform the patients about why it is important to do this explicit behaviour, because patients now know themselves. Integrated behaviour is usually maintained over longer periods of time.
The behaviour is accepted and connected to the underlying value of this behaviour. This behaviour is executed without conflicts and it is more easy for these patients to take personal responsibility for their own oral health challenges [7, 28]. The result is integrated autonomously self-determined motivation.
Example
Example of a patient with integrated regulation: The patient values performing dental home care regularly, efficiently , qualitatively and consciously. Patients can reflect upon why oral health promotion is valuable and important and what type of behaviours which leads to good oral health. Patients have high awareness about how to care for their own dental health. Patients’ attitudes and beliefs are carried out in the best way and they will be eager to solve their own dental challenges and problems. Patients will follow up their own dental visits regularly and take responsibility as a natural habit in an appropriate manner to achieve the best possible oral health. Patients often do their own research around oral health issues and tasks to perform. They ask questions and are eager to learn about their oral health and they want to solve their own challenges . They are now autonomous and self-motivated (self-regulated).
4.3 Intrinsic Motivation
This is the motivation Deci and Ryan [1] describe as the most genuine. This intrinsic regulation is as highly autonomous motivation and the activity starts from within a person. Therefore, it differs from the four exterinsic regulations/motivations which are initiated from outside a person. Intrinsic motivation is characterised when a person chooses, on an independent basis the behaviour that he or she finds interesting and wants to perform. As an example, we can observe the intrinsic motivation in infants who grab a rattle without being told if it is an important behaviour. According to Ryan and Deci [2], intrinsic motivation is our natural motivation that arises spontaneously, is exploratory and is stimulated and initiated by our own curiosity and a feeling of mastery is followed when we executing optimally challenging tasks.
Intrinsic motivation comes from within a person and it reflects an inner driving force, energy and vitality which leads to behaviours that we really want to engage in. Here, the only reward is when executing the performance (for example, mountain climbing). The feelings of flow, spontaneity and authentic enjoyment that accompany the performance are characteristics related to genuine intrinsic motivation [2].
5 Self-Determination Theory and Dental Health Research
Several of the studies from Halvari et al. [7,8,9,10, 14, 22, 26, 32] refer to autonomy support versus controlling dental personnel and how this is related to different patient motivation.
Autonomy support is positively associated with the patient's oral well-being, reappraisal and decrease of anxiety, oral well-being and oral health-related quality of life and increased dental health, as reduction of plaque and gingivitis, and attending dental treatment. When patients perceive dental professionals as controlling, the results are shown to be the opposite. The results from these studies show that autonomy-support from dental professionals give important and valid results over time. Building relevant oral health competence and mastery is important in order to contribute to more autonomous motivation, improved oral health, thereby helping patients to feel more wellness related to their oral health and understand how they can increase the oral health quality of life [10].
Summary
-
This chapter has provided a theoretical framework using self- determination theory (SDT).
-
First, the chapter gives a brief introduction of SDT.
-
Further, the importance of autonomy is presented as a professional and ethical issue. Autonomy is directly related to informed consent which is a duty for all dental professionals to provide.
-
Autonomy is importantly related to professional patient care, thus it is important to integrate into all dental health care contexts.
-
Autonomous motivation implies to be self-determined, self-regulated, self-ruled and self-motivated.
-
The three basic psychological needs (SDT- BPN); competence, autonomy and relatedness are described thoroughly and related to examples in the dental field.
-
Supporting SDT-BPN is shown to be fundamental in order to create a motivational climate and to facilitate internalisation of a behaviour.
-
The SDT-BPN are essential to be included and taken into consideration when dental professionals give autonomy support.
-
Autonomy support and support of basic psychological needs are:
-
1.
Focus on patient-centred communication.
-
2.
Building oral health relevant competence with choices and options related to patients own oral health challenges.
-
3.
Building relatedness, empathy and trust related to successful prevention of pain and understanding of patients vulnerabilities.
-
4.
Support of patient’s feelings and perspectives. Patients are given self-control (autonomy). They are not pressured or controlled to do something they do not want to do.
-
1.
-
Dental professionals who emphasise empathy, friendliness, acceptance, patient’s involvement and personal choices in relation to patient’s competence building, learning and personal growth will support relatedness, autonomy and mastery of oral health.
-
Competence-building and sufficient oral health understanding is appropriate in order to be able to promote, prevent and reduce oral health problems.
-
Dental personnel can counsel, guide, teach and train patients to be more autonomously self-motivated by using guidelines related to autonomy support.
-
Patients can learn to be more autonomous, self-motivated and self-regulated, conscious and intentional about their oral health behaviour.
-
Self-determined and autonomously motivated behaviour is in line with promotion of oral health.
-
The chapter shows with examples how dental personnel can learn to give autonomy support and be less controlling.
-
A model (◘ Fig. 8.3) shows how autonomous support versus controlling dental personnel is associated with psychological and mental health outcomes in patients.
-
The internalisation process in SDT is described with examples from the dental field, helping dental personnel to understand different motivational processes.
-
The internalisation process shows qualitatively different motivations related to the integration of a behaviour. This quality is reflected in how and to what extent and degree a person is regulating his or her behaviour autonomously.
-
Autonomously motivated patients will develop more long term goals and maintain more relevant dental behaviour over time.
-
This chapter shows how dental professionals can use SDT research and the understanding of qualitatively different motivations and regulations and integrate the practical consequences into the dental health field.
-
By focusing on how important autonomous motivation is and how this relates to human behaviours, we can probably be able to help more patients in the future. This is in order to help patients to better succeed in managing their own oral health challenges.
-
An important issue to understand more of in the future, is how SDT and motivation influences patients’ attitudes, behaviours, choices and goals.
-
A theory like SDT is concerned about the what, how and why of motivation [45]. Because of this, SDT has been increasingly used in many health research designs [15].

The Internalization Continuum [2, p. 193]

This oral health promotion model is supported by a lot of research [2]. This model shows how autonomy support versus control given by dental professionals will influence the three SDT-Basic Psychological Needs; autonomy, competence and relatedness, and how satisfaction versus frustration of these SDT - needs will imply different motivations and regulations and different positive versus negative outcomes related to mental and physical health
References
Deci E, Ryan R. Intrinsic motivation and self-determination in human behaviour. Rochester, New York: Springer; 1985.
Ryan RM, Deci EL. Self-determination theory: basic psychological needs in motivation, development, and wellness. NY: Guilford Publications; 2017.
Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68.
Niemiec CP, Ryan RM. Autonomy, competence, and relatedness in the classroom: applying self-determination theory to educational practice. Theory Res Educ. 2009;7(2):133–44.
Rogers CR. On becoming a person: a therapist’s view of psychotherapy. Boston: Houghton Mifflin Company; 1961.
Ryan RM, Deci EL. Brick by brick: the origins, development, and future of self-determination theory. In: Elliot, A. (Ed.) Advances in motivation science. Vol. 6. Pp. 111–56. Cambridge: Elsevier, 2019.
Halvari AEM, Halvari H, Bjørnebekk G, Deci EL. Motivation and anxiety for dental treatment: testing a self-determination theory model of oral self-care behaviour and dental clinic attendance. Motiv Emot. 2010;34(1):15–33.
Halvari AEM, Halvari H, Bjørnebekk G, Deci EL. Motivation for dental home care: testing a self-determination theory model 1. J Appl Soc Psychol. 2012;42(1):1–39.
Halvari AEM, Halvari H, Bjørnebekk G, Deci EL. Oral health and dental well-being: testing a self-determination theory model. J Appl Soc Psychol. 2013;43(2):275–92.
Halvari AEM, Halvari H, Deci EL. Dental anxiety, oral health-related quality of life, and general well-being: a self-determination theory perspective. J Appl Soc Psychol. 2019;49(5):295–306.
Deci EL, Ryan RM. Self-determination theory in health care and its relations to motivational interviewing: a few comments. Int J Behav Nutr Phys Act. 2012;9(1):1–6.
Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–36.
Williams GC, Deci EL. Internalization of biopsychosocial values by medical students: a test of self-determination theory. J Pers Soc Psychol. 1996;70(4):767.
Halvari AEM, Halvari H, Deci EL, Williams GC. Autonomy-supportive dental treatment, oral health-related eudaimonic well-being and oral health: a randomized clinical trial. Psychol Health. 2019;34(12):1421–36.
Patrick H, Williams GC. Self-determination theory: its application to health behavior and complementarity with motivational interviewing. Int J Behav Nutr Phys Act. 2012;9(1):1–12.
Beauchamp TL, Childress JF. Principles of biomedical ethics. New York: Oxford University Press; 2001.
Cassel CK, Hood V, Bauer W. A physician charter: the tenth anniversary. Ann Intern Med. 2012;21:290–91.
Woolf SH, Chan EC, Harris R, Sheridan SL, Braddock III CH, Kaplan RM, et al. Promoting informed choice: transforming health care to dispense knowledge for decision making. Ann Intern Med. 2005;143:293–300.
Ryan RM, Deci EL. Self-regulation and the problem of human autonomy: does psychology need choice, self-determination, and will? J Pers. 2006;74(6):1557–86.
Ryan RM, Deci EL, Vansteenkiste M. Autonomy and autonomy disturbances in self-development and psychopathology: research on motivation, attachment, and clinical process. Dev Psychopathol. 2016;1:385–438.
Deci EL, Ryan RM. Handbook of self-determination research. Rochester, NY: University of Rochester Press; 2004.
Halvari AEM, Halvari H, Deci EL. The roles of patients’ authenticity and accepting external influence, and clinicians’ treatment styles in predicting patients’ dental anxiety and avoidance of dental appointments. Eur J Psychol. 2020;16(1):45.
White RW. Motivation reconsidered: the concept of competence. Psychol Rev. 1959;66(5):297.
Baumeister RF, Leary MR. The need to belong: desire for interpersonal attachments as a fundamental human motivation. Psychol Bull. 1995;117(3):497.
Deci EL, Ryan RM. Facilitating optimal motivation and psychological well-being across life's domains. Can Psychol. 2008;49(1):14.
Münster Halvari A, Halvari H, Deci E. Attending and avoiding dental appointments: do “bright” and “dark” motivational paths have a role? Int J Dent Hyg. 2018;16(2):286–97.
DeCharms R. Personal causation: the internal affective determinants of behavior/R. Charms. New York: Academic Press; 1968.
Deci EL, Eghrari H, Patrick BC, Leone DR. Facilitating internalization: the self-determination theory perspective. J Pers. 1994;62(1):119–42.
Vansteenkiste M, Niemiec CP, Soenens B. The development of the five mini-theories of self-determination theory: an historical overview, emerging trends, and future directions. In: Karabenick, S, & Urdan, T. C. (Eds.), The decade ahead: theoretical perspectives on motivation and achievement (Pp. 105–65). Bingley, UK: Emerald, 2010.
Kadam RA. Informed consent process: a step further towards making it meaningful! Perspect Clin Res. 2017;8(3):107.
Ryan RM, Patrick H, Deci EL, Williams GC. Facilitating health behaviour change and its maintenance: interventions based on self-determination theory. Eur Health Psychol. 2008;10(1):2–5.
Münster Halvari AE, Halvari H, Bjørnebekk G, Deci EL. Self-determined motivational predictors of increases in dental behaviors, decreases in dental plaque, and improvement in oral health: a randomized clinical trial. Health Psychol. 2012;31(6):777.
Jang H, Reeve J, Deci EL. Engaging students in learning activities: it is not autonomy support or structure but autonomy support and structure. J Educ Psychol. 2010;102(3):588.
Deci EL, Vallerand RJ, Pelletier LG, Ryan RM. Motivation and education: the self-determination perspective. Educ Psychol. 1991;26(3-4):325–46.
Ryan RM, Lynch MF, Vansteenkiste M, Deci EL. Motivation and autonomy in counseling, psychotherapy, and behavior change: a look at theory and practice 1ψ7. Couns Psychol. 2011;39(2):193–260.
Kranstad V, Søftestad S, Fredriksen TV, Willumsen T. Being considerate every step of the way: a qualitative study analysing trauma-sensitive dental treatment for childhood sexual abuse survivors. Eur J Oral Sci. 2019;127(6):539–46.
Tessier D, Sarrazin P, Ntoumanis N. The effect of an intervention to improve newly qualified teachers’ interpersonal style, students motivation and psychological need satisfaction in sport-based physical education. Contemp Educ Psychol. 2010;35(4):242–53.
Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67(12):2072–8.
Taylor IM, Ntoumanis N. Teacher motivational strategies and student self-determination in physical education. J Educ Psychol. 2007;99(4):747.
Van den Broeck A, Vansteenkiste M, De Witte H, Lens W. Explaining the relationships between job characteristics, burnout, and engagement: the role of basic psychological need satisfaction. Work Stress. 2008;22(3):277–94.
Ryan RM, Deci EL, Grolnick WS, La Guardia JG. The significance of autonomy and autonomy support in psychological development and psychopathology. In: Cicchetti, D., & Cohen, D. J. (Eds.). The developmental psychopathology: Theory and method (pp. 795–849). Hoboken, NJ: Wiley, 2006.
Deci EL, Ryan RM. Self-determination theory: a macrotheory of human motivation, development, and health. Can Psychol. 2008;49(3):182.
Ryan RM, Rigby S, King K. Two types of religious internalization and their relations to religious orientations and mental health. J Pers Soc Psychol. 1993;65(3):586.
Pelletier LG, Dion S, Tuson K, Green-Demers I. Why do people fail to adopt environmental protective behaviors? Toward a taxonomy of environmental amotivation 1. J Appl Soc Psychol. 1999;29(12):2481–504.
Deci EL, Ryan RM. The" what" and" why" of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–68.
Ryan RM, Connell JP. Perceived locus of causality and internalization: examining reasons for acting in two domains. J Pers Soc Psychol. 1989;57(5):749.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Halvari, A.E.M. (2022). Self-Determination Theory – Autonomy Support and Improving Oral Health. In: Willumsen, T., Lein, J.P.Å., Gorter, R.C., Myran, L. (eds) Oral Health Psychology. Textbooks in Contemporary Dentistry. Springer, Cham. https://doi.org/10.1007/978-3-031-04248-5_8
Download citation
DOI: https://doi.org/10.1007/978-3-031-04248-5_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-04247-8
Online ISBN: 978-3-031-04248-5
eBook Packages: MedicineMedicine (R0)