
Abstract
Human fascioliasis is an important public health problem in many regions, and livestock infection is a veterinary problem worldwide. This disease is caused by the liver fluke species Fasciola hepatica of worldwide distribution and F. gigantica restricted to regions of Africa and Asia. Their two-host life cycle is similar, including specific freshwater lymnaeid snails as vectors. The major human health problems are known in Andean countries, the Caribbean, Northern Africa, Near East, Southeast Asia and Western Europe. In human hyperendemic areas, children and females are the most affected. Human fascioliasis shows a marked heterogeneity of epidemiological situations and transmission patterns. Variation of climatic factors and anthropogenic environmental modifications may give rise to different fascioliasis seasonality and long-term disease risk trends. There are many human infection sources, local diet and cultural traditions being important. The rapid and potent ability of fasciolids to suppress the immune response explains why hosts do not develop resistance and the frequency of pathogen coinfections. The disease is chiefly confined to the liver, including hepatic lesions, fibrosis and chronic inflammation. Juvenile flukes may cause ectopic fasciolosis. Clinical manifestations are evident in both invasive and biliary periods. Diagnosis is mainly made by coprological and serological techniques. Among the useful drugs, triclabendazole is of choice at present. Prognosis depends on treatment promptness. Severe complications, sequelae and death causes should be highlighted. New knowledge has allowed to improve individual infection prevention measures and community control. Challenges appear in vaccinology, indicating that a human vaccine is still far from affordable.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Human and animal fascioliasis
- Fasciola hepatica
- Fasciola gigantica
- Lymnaeid snail vectors
- Mammal reservoirs
- Epidemiology
- Immunity
- Pathology
- Clinical manifestations
- Diagnosis
- Treatment
- Prevention
- Control
6.1 Introduction
Fascioliasis is a well-known veterinary problem worldwide. Moreover, in the last two decades, many surveys have shown it to be an important public health problem as well (Chen and Mott 1990; Mas-Coma et al. 1999c, 2009a), including estimations of 2.4 million, up to 17 million people, or even higher depending from the hitherto unknown situations mainly in Asia and Africa (Mas-Coma 2004).
The number of human case reports is increasing in many countries of the five continents, many human endemic areas have already been assessed (Mas-Coma et al. 2005), and recent results of studies on pathogenicity and immunity underlie the decision to consider fascioliasis an important human parasitic disease henceforth (Mas-Coma et al. 1999b) and include it as a food-borne trematode disease priority within the agenda of the World Health Organization (World Health Organization 2013).
6.2 The Agent
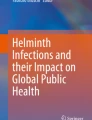
This parasitic disease is caused by two digenean trematodes, Fasciola hepatica of worldwide distribution and F. gigantica restricted to given regions of Africa and Asia. Their adult stage has a leaf-shaped body and is anatomically characterized by the branching of their caeca, testes and ovary, the very numerous small vitellaria extending bilaterally up to the hindbody and a short uterus located between the ovary and the caecal bifurcation (Fig. 6.1). The eggs are operculated, ovoid, yellow and non-embryonated when laid.

Adult stages of pure Fasciola hepatica and pure F. gigantica. Note the different size and shape; hybrid forms usually show an intermediate form. The two photographs are at the same scale (Orig. S. Mas-Coma)
Fasciola gigantica is more elongate and narrower, with lateral walls tending to be parallel and with non-existent or less marked shoulders of the cephalic cone (Fig. 6.1). The adult stage of F. hepatica has a maximum length/width of 29.0/14.1 mm, whereas F. gigantica is bigger, with a maximum size reaching 52.3/11.8 mm. Hybrid specimens may give rise to intermediate forms in those endemic areas where the two species overlap (Mas-Coma et al. 2009a).
The F. hepatica genome has proved to be among the largest known pathogen genomes at 1.3 Gb. The high polymorphism levels found have tentatively been linked to the evolutionary potential for rapid adaptation to changes in host availability, climate change or drug or vaccine interventions (Cwiklinski et al. 2015). Surprisingly, the genome of F. hepatica isolated from sheep of North America showed a markedly higher repeat content (55.29%) than the aforementioned genome of F. hepatica isolated from sheep of the United Kingdom (32.0%) (McNulty et al. 2017).
Adult worms parasitize the large biliary passages and the gallbladder of ruminants, mainly sheep, goats and cattle, and many other herbivorous domestic and wild animals, including horses, donkeys, mules and also Old and New World camelids. Buffalo, deer, wild sheep, wild pig, various marsupials, rabbit, hare and nutria are also susceptible hosts (Mas-Coma and Bargues 1997).
Sheep and cattle are the livestock species most infected by F. hepatica, whereas the buffalo appears to be the most important for F. gigantica. In human hyperendemic areas, the domestic pig (Mas-Coma et al. 2021) and equines as the donkey (Mas-Coma et al. 2020b) and the mule (Mera y Sierra et al. 2020) should also be considered among the important reservoirs.
Among wild definitive hosts in Europe, F. hepatica seems to be less adapted to the roe deer (Capreolus capreolus) when compared to other deers (red and fallow deer), and the introduced nutria (Myocastor coypus) has become an important reservoir in France and may also be so in areas of South America from where it is original.
Humans are susceptible hosts for the infection by both Fasciola species (Mas-Coma et al. 2009a).
The two-host life cycle of both fasciolids is similar and takes about 14–23 weeks. It comprises four phases (Mas-Coma and Bargues 1997):
-
(A)
The definitive host harbours fluke adults producing eggs which reach the external milieu by way of the bile and intestine; the definitive host is infected by ingestion of metacercariae; in humans, the flukes attain sexual maturity in 3–4 months and their life span is between 9 and 13.5 years.
-
(B)
The transit between definitive mammal host and intermediate snail host includes the long resistance phase of the egg and the short active phase of miracidium; eggs shed with the mammal faeces will continue their development in freshwater of appropriate physicochemical characteristics (mainly temperature of 15–25 °C).
-
(C)
The development at snail level includes miracidium penetration, sporocyst, redial generations, production of cercariae and shedding of the latter into the water; the prepatent period (38–86 days) is dependent on temperature, higher temperatures reducing the period.
-
(D)
The transit between snail and mammal host includes the short swimming phase of cercaria and the long resistance phase of metacercaria; the shedding process takes place between 9 and 26 °C, independently of light or darkness; cercariae swim for a short time until contacting a solid support, mostly leaves of water plants above or below the water line, to attach and encyst (Fig. 6.2); metacercarial cysts become infective within 24 h.

Metacercarial body of Fasciola hepatica shortly after detaching from its swimming tail and already starting encystment process (Orig. S. Mas-Coma)
Liver fluke development is very dependent of the environmental characteristics according to phases B, C and D and markedly influenceable by human activities at phase A.
Vectors of Fasciola are freshwater gastropod snails of the family Lymnaeidae. Different lymnaeid species transmit the two fasciolids, which show a marked and different specificity. There are species of Lymnaeidae which cannot transmit fasciolids, other lymnaeid species which transmit F. hepatica, other species which transmit F. gigantica and a very few which are able to transmit the two fasciolid species.
Fasciola hepatica is mainly transmitted by species of small size belonging to the so-called Galba/Fossaria group (Bargues et al. 2007, 2011a), including Galba truncatula as the main vector and the only one in Europe but also present in Africa, Asia and South America. Other species of this group act as vectors in the Americas. Lymnaea tomentosa is the transmitter in Australia. In South America, the species Lymnaea neotropica, also of the Galba/Fossaria group, has recently proved to be a very efficient transmitter also involved in the spread of the disease throughout wide regions in the lowlands, whereas Galba truncatula is the one involved in the highlands (Bargues et al. 2017).
Fasciola gigantica is transmitted by species of the genus Radix, mainly R. natalensis in Africa and varieties of R. auricularia and R. viridis in Asia. In Europe, however, Radix species do not show any epidemiological importance, given that only F. hepatica is present (Bargues et al. 2001). Pseudosuccinea is a monospecific genus including the species P. columella which has colonized all continents and appears to be able to transmit both Fasciola species (Bargues et al. 2011b).
The presence of lymnaeid vectors defines not only the distribution of fascioliasis but may also explain the distribution of human infection within a country, as has been recently observed in Venezuela (Bargues et al. 2011c) and Chile (Artigas et al. 2011), and within an endemic area, as well as its seasonality or permanent transmission (Mas-Coma et al. 1999a). Similar to other waterborne parasitic diseases, the transmission foci are patchily distributed within a human endemic area and linked to the presence of appropriate water collections, and human prevalences in schoolchildren appear to be related to the distance to water bodies presenting lymnaeids (Mas-Coma et al. 1999a).
6.3 Epidemiology of Infection
A global analysis of the geographical distribution of human cases shows that the expected correlation between animal and human fascioliasis only appears at a basic level. High prevalences in humans are not necessarily related to areas where fascioliasis is a great veterinary problem. The major human health problems are known in Andean countries (Bolivia, Peru, Chile, Ecuador), the Caribbean (Cuba), Northern Africa (Egypt), Near East (Iran and neighbouring countries), Southeast Asia (Vietnam) and Western Europe (Portugal, France and Spain) (Esteban et al. 1998; Mas-Coma et al. 2009a).
However, the worldwide distribution of fascioliasis also includes human infection risk in developed, high-income countries, in which from individual patients up to small epidemics continue to be reported, with the additional problems of the impacts by the climate and global changes (Mas-Coma 2020).
In the human hyperendemic areas, children are the most affected by the disease, with higher prevalences and intensities (with a peak in the 9–11 age group). In these areas, human infection may occur very early in life, as only a few months after being born. Moreover, child infection has been verified to occur at preschool age more frequently than previously considered (De et al. 2020).
Adult subjects are also infected in the human hyperendemic areas. Adult subjects either maintain the parasites acquired when young or can be newly infected because of the high infection risk. The gender effect in fascioliasis is worth mentioning. Prevalences and/or intensities in human hyperendemic areas appear to be significantly higher in females. In Andean countries, females shed pronouncedly and significantly more eggs than males (Esteban et al. 1999, 2002), whereas in Egypt, the prevalence in females appeared to be significantly higher than in males (Esteban et al. 2003). Interestingly, however, in preschool children, the opposite occurs, with a faster infection increase in males from 2 years onwards (De et al. 2020).
Moreover, it should be considered that the importance of this disease is not only restricted to the health aspects but also to its high economic impact mainly in the endemic rural areas (Espinoza et al. 2010).
6.3.1 Epidemiological Heterogeneity of Human Fascioliasis
After many years of studies on different areas presenting human infection by fasciolid liver flukes throughout the world, the classification of epidemiological situations proposed by Mas-Coma et al. (1999c) still appears to be fully valid and useful. This classification includes the following situations: (1) autochthonous, isolated, non-constant cases; (2) imported cases; endemic situations including (3) hypoendemic, (4) mesoendemic and (5) hyperendemic; and also epidemic situations comprising (6) epidemics in non-human endemic but animal endemic areas and (7) epidemics in human endemic areas.
Fascioliasis presents a very wide spectrum of transmission and epidemiological patterns in human hypo- to hyperendemic areas. These are related to the large diversity of environments, including different human endemic/epidemic situations; different human demographies, races, diets, habits, traditions and religions; different domestic and wild mammal reservoir species; different lymnaeid transmitting species; zones in both the Northern and Southern Hemispheres; altitudes from −27 m up to 4200 m; hot and cold weathers; seasonal and yearly constant temperatures; scarce to pronounced annual rainfall; low and high mean annual potential evapotranspiration; and from lack of dry period to lack of wet period through different dryness/humidity rates. From the landscape point of view, these areas include from altiplanos to valleys, from islands to mainlands, from natural to artificial irrigations, from lakes to lagoons, from large rivers to small streams and from permanent to temporal water bodies (Mas-Coma et al. 2003).
A classification of transmission patterns has been proposed (Mas-Coma 2005) and is progressively updated to offer a baseline for future research (Mas-Coma et al. 2009a). Up to the present, the following patterns have been distinguished: (1) a very high altitude pattern in Andean countries including the altiplanic pattern and the valley pattern (Valero et al. 2012a); (2) a Caribbean insular pattern; (3) a pattern related to Afro-Mediterranean lowlands; (4) a pattern related to Caspian surrounding areas; and (5) a pattern related to lowland areas in Southeast Asia.
An additional extreme pattern has been found in Argentina, involving desertic-arid and semi-arid conditions with very low yearly precipitation, which are very different from the typical fascioliasis transmission foci. In such a place, lymnaeids are confined to lateral river side floodings and small man-made irrigation systems, with water availability only depending on the rivers flowing from neighbouring mountains. This reminds the transmission foci of schistosomiasis in oases of the Sahara Desert in Africa (Bargues et al. 2016). In Uttar Pradesh, India, infection risk appears concentrated in freshwater collections where the 72.0% rate found in lymnaeids in one transmission focus appears to be the highest worldwide record of fasciolid infection in a lymnaeid population (Sunita et al. 2021).
Thus, well-known situations and patterns of fascioliasis may not always explain the disease characteristics in a given area. Only once epidemiology and transmission characteristics of the new area are sufficiently assessed may appropriate control measures be designed for the endemic area in question.
6.3.2 Seasonality and Long-Term Impacts of Climate and Global Changes
Climatic factors are decisive in the transmission of fascioliasis, mainly temperature, rainfall and/or potential evapotranspiration (Mas-Coma et al. 2009b).
Variation of mainly rainfall and temperature gives rise to different fascioliasis seasonality. In Europe, the transmission of the disease is typically bi-seasonal, due to the activity periods of the lymnaeid vectors in spring and autumn. In the Bolivian Altiplano, however, the transmission takes place throughout the year, lymnaeid vector populations being always present because of inhabiting permanent water bodies instead of temporary ones due to the high evapotranspiration rates at the very high altitude (Mas-Coma et al. 1999a). In other areas, the transmission appears mono-seasonal, due to the existence of only 1-year period with water availability.
Climate change overlaps other anthropogenic and environmental modifications which are included in the broad term of “global change” (Mas-Coma et al. 2009b). Thus, artificial field irrigation appears to be sufficient by its own to allow for fascioliasis transmission in the Peruvian Altiplano (Esteban et al. 2002). In the province of Punjab, in Pakistan, transmission includes bi-seasonality with a peak related to natural rainfall and another peak related to man-made irrigation (Afshan et al. 2014). The Punjab is the first endemic area where the emergence of human infection has been correlated with a significant increase of fascioliasis transmission risk due to an impact of climate change throughout a 20-year period (Afshan et al. 2014).
In the Northern Bolivian Altiplano human hyperendemic area, comparisons of transmission foci data from the 1990s with those of 2018 demonstrated an endemic area expansion. Altitudinal, northward and southward expansions suggest movements of livestock transporting snail vectors, with increasing temperatures transforming previously unsuitable habitats into suitable transmission areas. Important repercussions include the need to widen the area throughout which the preventive chemotherapy programmes are implemented (Bargues et al. 2020).
For the study of climate and environment influences on fascioliasis, three types of approaches are useful, including the assessment from geographical distribution and seasonality up to human and animal infection risk and forecasting methods, namely, mathematical modelling based on climate factors, remote sensing (RS) based on images and information furnished mainly by space satellites and geographic information systems (GIS) based on computer mapping by geo-positioning of different abiotic and biotic factors and characteristics. These methods allow for developments from low to very high resolution adapted to endemic areas of different characteristics (Bergquist et al. 2021).
6.3.3 Sources of Human Infection
Metacercarial infectivity is dependent upon storage time, being lower when metacercariae are older. The maximum longevity was 48 weeks. Moreover, metacercarial viability and infectivity did not show differences between isolates from different reservoir species (Valero and Mas-Coma 2000).
The ingestion of infective metacercariae by humans may occur by different ways. Several infection sources have been distinguished (Mas-Coma 2004; Mas-Coma et al. 2018). These infection sources include foods, water and combinations of both:
-
Ingestion of freshwater wild plants: main aspects to be considered are the plant markers of transmission foci, watercress, other freshwater wild plants and wild plants sold in urban markets.
-
Ingestion of freshwater cultivated plants, mainly watercress.
-
Ingestion of terrestrial cultivated plants needing frequent irrigation.
-
Ingestion of terrestrial wild plants: collected in dry habitats but which were submerged in water a few weeks or months before.
-
Ingestion of traditional local dishes made with contaminated sylvatic plants.
-
Ingestion of raw liver infected with migrating metacercariae which may keep the capacity to restart migration.
-
Drinking of contaminated water.
-
Drinking of beverages and juices made from local plants.
-
Ingestion of dishes and soups made with contaminated water.
-
Washing of vegetables, fruits, tubercles, kitchen utensils or other objects with contaminated water.
Cultural traditions prove to be important in given endemic areas. Experimental studies showed the role that plant-made foods may play in human infection in Gilan Province, Iran (Ashrafi et al. 2006). There are three methods to assess infection sources: (1) detection of metacercariae attached to plants or floating in freshwater, (2) anamnesis in individual patients and (3) questionnaire surveys in endemic areas (Mas-Coma et al. 2018).
In Mexican children, an association between fascioliasis and the habit of eating raw vegetables was identified. The link of fascioliasis risk with consumption of raw vegetables other than watercress should be highlighted, as it suggests contamination when washing terrestrial vegetables with untreated water and/or in plant cultures using natural water for irrigation (Zumaquero-Ríos et al. 2013).
6.4 The Host Response to the Parasite
Immunologically, cell- and/or antibody-mediated response varies from host to host and in the same host according to the phase of the infection. Similarly, immunity to reinfection differs greatly from host to host.
In humans, studies on immunity are limited. It is generally believed that humans are not a suitable host, most migrating flukes becoming trapped in the liver parenchyma and dying without reaching the bile ducts. Considerable tissue reaction and calcification of the bile passages due to the flukes have been recorded (Acosta-Ferreira et al. 1979).
6.4.1 Immunological Processes
Fasciolid trematodes promote their own survival through several strategies to downregulate the host’s immune response during the early phase of infection (Brady et al. 1999). Another study proved that immune response modulation occurs in advanced chronic fasciolosis too. The results indicated that during early chronic infection, there was a predominance of a Th2 response, which decreased in the advanced chronic infection characterized by a persistent immune suppression (Girones et al. 2007). Fascioliasis is a potent inducer of Th2 responses which impair the ability to mount any effective Th1 responses against bacteria and other pathogens (Brady et al. 1999; O'Neill et al. 2000; Jaffar et al. 2004).
The rapid and potent ability of fasciolids to suppress the immune response explains why infected hosts do not develop resistance. This underlies the frequent reinfections in human hyperendemic areas where the infection risk is very high (Valero et al. 2017, 2020).
Within 24 h after oral infection, peritoneal macrophages express markers for the Th2-associated phenotype and display a reduced ability to respond to Th1 stimulants. This implies that by the time the newly excysted juveniles have penetrated the intestinal wall and entered the peritoneum, they have already initiated the immune events that will dominate throughout infection. So, these early-stage parasites secrete immunomodulatory molecules that influence the function of innate cells (dendritic cells, macrophages, neutrophils, mast cells, etc.) in the intestinal wall and peritoneal cavity. A systemic antigen-specific Th2 response is firmly established already at 7 days postinfection and is characterized by the secretion of IL-4, IL-5 and IL-13 from splenocytes. As the infection develops (3 weeks), regulatory macrophages (TGF-ß and IL-10 producing) and dendritic cells (IL-10 producing) are recruited to the peritoneum, and dendritic cell maturation is inhibited. Mast cells recruited to the site of infection exhibit impaired Th1-promoting abilities. Most CD4* T cells in the peritoneum secrete IL-10 but not IL-4 or IFN-γ. IL-10-secreting Tregs are induced which exert a suppression of both Th1 and Th2 cells that become non-responsive to parasite-specific antigens, and mesenteric lymph nodes produce IL-10 and IL-5, but not IFN-γ and IL-17, in response to stimulation by parasite antigens (Dalton et al. 2013).
The chronic disease is also typified by Th2 responses and suppressed Th1 responses. Serologically, this polarity of immune response is strikingly displayed in the isotype of circulating antibodies. Fluke-infected animals secrete high titres of IgG1 antibodies and virtually no IgG2. Furthermore, blood macrophages are non-responsive to stimulation with endotoxin and exhibit elevated levels of arginase indicative of a phenotype that metabolize l-arginine and are important in promoting Th2 responses and facilitating tissue repair and fibrosis (Dalton et al. 2013).
6.4.2 Associations with Other Parasites
A consequence of liver fluke infection is the suppression of immune responses directed against concurrent pathogenic infections. The synergistic capacity of fasciolids in coinfection with other pathogenic agents is well known, immunological responses to pathogen antigens being markedly suppressed and concomitant infection being exacerbated following fascioliasis infection. The parasitological spectrum of protozoan and helminthic species found in the inhabitants of the human endemic areas, the multiparasitisms and the associations between liver fluke infection and infection by other pathogenous parasites, all appear to be similar in the different human endemic zones (Esteban et al. 1997a, 1997b, 1999, 2002, 2003; Gonzalez et al. 2011). These synergistic associations of fascioliasis with other pathogens are believed to underlie the high morbidity and mortality rates of Aymara children inhabiting the Northern Altiplano (Mas-Coma 2004).
In animals, the clinic synergistic capacity of F. hepatica in concomitant infection with other pathogenic agents is well known. In humans, the association of F. hepatica with other parasites has been assessed in recent large surveys performed in human fascioliasis endemic areas. In the Bolivian Altiplano endemic zone, among the samples positive to F. hepatica, the number of other parasite species found varied from one to eight. In 35.5% of the cases with F. hepatica eggs, the liver fluke showed to be the sole parasite species present in which a pathogenic capacity is well known. Fasciola hepatica infections associated with one (34.9%), two (23.7%), three (4.6%) and four (1.3%) of the other generally recognized pathogenic parasites were recorded. A significant positive association of great health importance in children was found with Giardia intestinalis, both in Bolivia and Peru (Esteban et al. 1997a, b, 1999, 2002).
6.5 Pathology
Pathogenesis depends on the number of flukes. However, fluke size has also proved to be an important factor when comparing the pathogenicity of F. hepatica with that by F. gigantica. Results demonstrated that F. gigantica is more pathogenic than F. hepatica, due to its bigger size and biomass. The higher F. gigantica pathogenicity contrasts with previous studies which only reflected the faster development of F. hepatica observed in short-term experiments (Valero et al. 2016).
The penetration of the duodenum or jejunum wall by metacercariae may cause focal haemorrhages and inflammation, although lesions may not be clinically evident. The fluke migration through the liver parenchyma for 4–6 weeks or longer induces the major pathological changes. Parasites digest hepatic tissue and cause extensive parenchymal destruction with intensive haemorrhagic lesions and immunological and inflammatory reactions. Migration tracks are observed in histological sections. Migratory flukes sometimes die leaving cavities filled with necrotic debris, and considerable liver areas may subsequently be replaced by scar tissue (Mas-Coma et al. 1999b, 2000).
A small proportion of the flukes may reach the bile ducts where they may live for even years. Less pathogenic effects may be caused in the bile ducts, although inflammation resulting in fibrosis, thickness and expansion is common (Fig. 6.3) (Chen and Mott 1990). The ultrastructural picture revealed bile ductular hyperplasia, fibrosis of portal tracts, widening of the interhepatic spaces by many microvilli and dilated Disse space with collagen fibres. Bile ductular hyperplasia may be the initial factor to fibrinogenesis, which subsequently enhances the development of the microvilli on the surface of the hepatocytes.

Histopathological section showing a specimen of Fasciola hepatica in a rat biliary duct. See section of large sucker inside and prominent spines in the tegumental external surface of the worm (Orig. S. Mas-Coma)
Anaemia is one of the most characteristic symptoms, especially in heavier infections. Blood loss into the bile seems most probably to be an important factor contributing to severe anaemia. An association between anaemia and fluke burden (the most important), epg, fluke body area, presence of blood in faeces, IgG1 and eosinophil levels and per cent of splenic weight was verified in a multivariate analysis. These results lead to the assumption that a high risk of anaemia in subjects with a heavy parasitic burden in human hyperendemic areas is to be expected (Valero et al. 2008). These results are crucial, because although there were several reports listing anaemia in patients from endemic areas, results could only be considered with great caution because coinfections were never excluded in those papers and in fact it becomes very difficult, not to say almost impossible, to find subjects from endemic areas only infected by fascioliasis. And among those parasites coinfecting fascioliasis-affected subjects, many are also known to cause anaemia.
The process may be summarized as follows: (1) the fluke is a blood feeder but may also feed on tissue; (2) haemorrhages may occur from the erosion of the biliary epithelium due to the infection; (3) reticulocytes are increased in the peripheral blood; (4) generalized haemolysis is absent; and (5) there is no evidence of plasma iron or vitamin B12 deficiencies, although a significant reduction in serum iron has recently been detected in patients with chronic fasciolosis.
The most important pathogenic sequelae are hepatic lesions and fibrosis and chronic inflammation of the bile ducts, given that the disease is chiefly confined to the liver. Unlike clonorchiasis or opisthorchiasis, no association with biliary carcinoma has been reported (Mas-Coma and Bargues 1997).
6.5.1 Liver and Biliary Tract
The liver appears usually enlarged with a smooth or uneven surface. The most common macroscopic lesions are multiple soft, yellowish or grey-white nodules ranging from 2 to 30 mm in diameter, which correspond to eosinophilic abscesses. Nodules are also observed in the parietal peritoneum proximal to the liver and on the round liver ligament. Haemorrhagic stippling appears at the margin of the nodules. White or yellow striae, surrounded by telangiectasia, are observed on the liver capsule. Close to the nodules, ribbed or vermiform formations with similar colour and consistency as nodules are also observed under laparoscopy. Hepatic capsular thickening of varying degree appears, and in a few cases, the entire hepatic capsule appears thickened. Subcapsular lymphatic vessels are dilated. The lymph nodes near the porta hepatis may be markedly enlarged. Multiple subcapsular cavities filled with necrotic material were observed below the liver capsule in one patient who died. Several reddish-purple tracks radiated from the nodules, whereas others were greyish white and fibrous. The tracks extended from the liver capsules and ended in subcapsular cavities. Most of the lesions are less than 20 mm below the capsules (Acosta-Ferreira et al. 1979). In cases with marked involvement of the peritoneal wall and the liver surfaces, yellow and opalescent ascites was present. Apart from mild splenomegaly in two patients, no significant portal hypertension was found in laparoscopic examinations of several patients.
The common bile ducts are usually large (Fig. 6.3) and dilated, and the wall is thickened on palpation. The gallbladder wall is greatly thickened and oedematous. Multiple, greyish-white subserous nodules are present, and adhesions of the gallbladder to adjacent structures are common. The mucosal folds of the gallbladder appear prominent. The wall of the gallbladder appears thickened owing to muscular hypertrophy and perimuscular fibrosis. There is glandular epithelial hyperplasia. All layers of the wall contain patchy infiltrates with lymphocytes, plasma cells and eosinophils (Acosta-Ferreira et al. 1979).
Lithiasis, often multiple, in the common bile ducts and gallbladders is very frequent (Arjona et al. 1995), whereas cirrhosis does not appear to be so (Marcos et al. 2009). The presence of gallstones was experimentally proved to increase with infection time. Therefore, the lithogenic induction by infection becomes manifest in situations of advanced chronicity. Gallstone presence was strongly associated with the number of flukes located in the bile duct. The risk of pigment stones appears to depend mainly on factors that favour bile duct obstruction (cholangitis, fluke body development versus time, intensity of infection). Situations of undiagnosed cases, as in subjects presenting undistinguishable symptoms or in those keeping their infection for a long time because of non-treatment or of repetitive reinfections, usually in human endemic areas of developing countries, imply a higher lithiasis risk. Thus, a high gallstone risk may be expected in subjects inhabiting human hyperendemic areas where very high egg outputs detected in humans suggest that liver fluke burdens may also be very high (Valero et al. 2003).
Generally, the migration tracks can be found in the liver and other organs. The walls of the tracks in the liver often contain Charcot-Leyden crystals and eosinophils. The cavities of the tracks are filled with necrotic cellular debris, including hepatocytes, fibrin and red cells. A considerable eosinophilic infiltrate surrounds the tracks. Longer tracks can cross several hepatic lobules. In older lesions, macrophages, lymphocytes, eosinophils and fibrous tissue are observed. Focal calcification is sometimes seen in the margin of the necrotic debris. Calcifications may form the outline of a dead fluke (Acosta-Ferreira et al. 1979).
Egg granulomas have been reported. Multinuclear giant cells surround a single egg with subsequent layers of epithelioid cells and fibrous tissue, plasma cells, lymphocytes and eosinophils. The portal triads are dilated and oedematous with infiltrates of lymphocytes and eosinophils. Bile duct proliferation, periductal fibrosis, necrotizing arterial vasculitis and portal venous thrombosis are frequent (Acosta-Ferreira et al. 1979; Chen and Mott 1990).
6.5.2 Other Locations, Ectopic Fascioliasis and at Distance Effects
Juvenile flukes may deviate during migration, enter other organs and cause ectopic fascioliasis. In humans, the most frequent ectopic lesions are those of the gastrointestinal tract (Acosta-Ferreira et al. 1979). Other ectopic locations reported are the subcutaneous tissue; heart, blood vessels, lung and pleural cavity; abdominal wall; appendix; pancreas; spleen; inguinal nodes; cervical node; skeletal muscle; and epididymis. Such ectopic flukes almost never achieve maturity (Mas-Coma et al. 2014). The usual pathological effects of ectopic lesions are due to the migratory tracks causing tissue damage with inflammation and fibrosis. Parasites may be calcified or become incorporated in a granuloma (Arjona et al. 1995; Mas-Coma and Bargues 1997).
Very recently, a wide analysis has shown that neurofascioliasis or intracranial infection by Fasciola and ophthalmofascioliasis or direct affection of the eye by migrating flukes may be rare, although not sporadic as previously believed. However, manifestations including a very wide range of neurological symptoms, signs and syndromes, together with meningeal, psychiatric or neuropsychic manifestations, and ocular disorders caused at distance by flukes infecting the liver may be frequent but underestimated due to misdiagnosis, mainly in low-income regions. The impressive clinical pictures should be highlighted. They include from hemiplegia and paraplegia to disturbances and difficulties of walking capacity, speech disorders, convulsions, epilepsy and coma, amnesia or visual hallucinations and permanent blindness, only to mention a few, plus the clinical complexity of the puzzling polymorphisms, the disconcerting multifocality of the manifestations and their changes along the evolution of the disease in a same patient, as well as differences between the clinical pictures shown by different patients. Moreover, these studies emphasize post-treatment sequelae and mortality in neurological patients and the need to consider neurological fascioliasis when estimating the global burden of this disease (Mas-Coma et al. 2013, 2014).
Recently, proteomic and mass spectrometry analyses of the Fasciola hepatica excretome/secretome identified numerous, several new, plasminogen-binding proteins enhancing plasmin generation. This may underlie blood-brain barrier leakage whether by many simultaneously migrating, small-sized juvenile flukes in the acute phase or by breakage of encapsulating formations triggered by single worm tracks in the chronic phase. Blood-brain barrier leakages may subsequently occur due to a fibrinolytic system-dependent mechanism involving plasmin-dependent generation of the proinflammatory peptide bradykinin, after different plasminogen-binding protein agglomeration waves. Interactions between diverse parasitic situations and non-imbalancing fibrinolysis system alterations are for the first time proposed that explain the complexity, heterogeneity and timely variations of neurological disorders (Gonzalez-Miguel et al. 2019).
6.6 Clinical Manifestations
The following clinical periods can be distinguished: incubation period (from the ingestion of metacercariae to the appearance of the first symptoms) and infection periods including the invasive or acute phase (fluke migration up to the bile ducts), the latent phase (maturation of the parasites and starting of oviposition) and the biliary, chronic or obstructive phase. Of these four periods, the invasive or acute phase and the biliary or chronic phase are the most important and in which most of the patients are detected.
The incubation period varies considerably depending on the number of metacercariae ingested and the host’s response. The period of incubation in humans has not yet been accurately determined: only “a few” days, 6 weeks, 2–3 months or even more (Mas-Coma et al. 1999b).
The latent phase can last for months or years. The proportion of asymptomatic subjects in this phase is unknown. They are often discovered during family screening after a patient is diagnosed, confirmed after clinical suspicion or in epidemiological surveys by finding the eggs in the duodenal fluid and/or in the stool (Arjona et al. 1995). An unexplained, prominent eosinophilia may already be suggestive of infection (Gil-Benito et al. 1991). These persons may have gastrointestinal complaints or one or more relapses of the acute symptoms during this phase (Mas-Coma and Bargues 1997).
6.6.1 Invasive or Acute Phase
In this phase, the symptomatology is due mainly to the mechanical destruction of the liver tissue and of the abdominal peritoneum by the migrating larvae causing localized or generalized toxic and allergic reactions lasting 2–4 months. However, in endemic areas, F. hepatica infection is usually repetitive, and the acute lesions are superimposed on chronic disease. Thus, the acute phase may be prolonged and overlap on to a latent or an obstructive phase.
The major symptoms of this period include (Mas-Coma et al. 1999b):
-
Fever: it is usually the first symptom, usually low or moderate but may reach 40 °C and in heavily infected cases as high as 42 °C; it may be remittent, intermittent or irregular with higher temperature in the evening; in some cases, a low, recurrent fever lasted for a long time (4–18 months).
-
Abdominal pain: from mild to excruciating, sometimes vague, it may be generalized at the outset but is usually localized in the right hypochondrium or below the xiphoid.
-
Gastrointestinal disturbances: loss of appetite, abdominal flatulence, nausea and diarrhoea are common, whereas vomiting and constipation are infrequent.
-
Urticaria: it is, with dermatographia, a distinctive feature in the early stage of the fluke invasion and may be accompanied with bouts of bronchial asthma.
-
Respiratory symptoms: cough, dyspnoea, hemoptysis and chest pain occur occasionally but in some cases are the first manifestation of infection.
The following signs may appear in the invasive phase on physical examination (Mas-Coma et al. 1999b):
-
Hepatomegaly and splenomegaly: the liver is usually enlarged and tender, sometimes reaching down to the right iliac fossa, but it is never hard; the degree of hepatomegaly seems to increase during the course of the disease, and hepatic abscesses are detected; splenomegaly is not common but has been many times reported.
-
Ascites: this sign has been reported several times; it is yellow with a high leucocyte count, eosinophils predominating; the pathogenesis is considered to be an inflammatory response to a large number of juvenile flukes penetrating the intestinal walls, irritation of the peritoneum and penetration through the liver capsule during their migration rather than hepatic failure per se.
-
Anaemia: mild to moderate anaemia can be seen; pallor of the skin and mucosa are commonly associated with lassitude, dizziness, palpitation and weakness.
-
Chest signs: on auscultation, dry or moist rales can occasionally be elicited upon coughing at the base of the right lung probably due to migration of the juvenile flukes; pleural rub with effusion and even spontaneous pneumothorax have been reported; parenchymal infiltrates resembling the Loeffler syndrome and pleural effusion are the most common radiologic manifestations; pyopneumothorax has been also reported.
-
Jaundice: it is infrequent, and when it appears, it is milder than that seen in the chronic phase.
In human endemic zones, there is usually a decrease of the prevalence from children and young subjects to adult subjects. Despite this, results demonstrate that adult subjects either maintain the parasites acquired when young or can be newly infected as the consequence of inhabiting a zone of high infection risk (Esteban et al. 1999). It must be considered here that the life span of the adult fluke in humans is between 9 and 13.5 years (Mas-Coma and Bargues 1997). Such a picture suggests that, in those areas, the majority of adult subjects should be in the biliary period, acute lesions by repetitive infections being superimposed on chronic disease with relative frequency. Thus, the acute period may be prolonged and overlap with both latent and biliary periods.
6.6.2 Biliary or Chronic Phase
This phase may develop after months to years of infection. Adult flukes in the bile ducts cause inflammation and hyperplasia of the epithelium. There is thickening and dilatation of the ducts, and the gallbladder walls ensue. The resulting cholangitis and cholecystitis, combined with the large body of the flukes, are sufficient to cause mechanical obstruction of the biliary duct which is comparatively small in diameter. The proportion of those whose infection develops into the obstructive phase or their prognosis has not been defined.
In this phase, biliary colic, epigastric pain, fatty food intolerance, nausea, jaundice, pruritus, right upper-quadrant abdominal tenderness, etc. are clinical manifestations indistinguishable from cholangitis, cholecystitis and cholelithiasis of origins other than Fasciola infection. Hepatic enlargement may be associated with an enlarged spleen or ascites (Acosta-Ferreira et al. 1979).
The common bile ducts are usually seen as distended and thickened. The diameters are 1.5–3.0 times normal size. The most frequent site of obstruction is the common bile duct. A diverticulum in this duct has been observed, and the head of the pancreas was enlarged and firm.
In case of obstruction, the gallbladder is usually enlarged and oedematous with thickening of the wall. The gallbladder may measure 12 × 7 × 7 cm and the lower edge reaches the umbilicus. Fibrous adhesions of the gallbladder to adjacent organs are common. Lithiasis of the bile duct or the gallbladder is frequent and the stones are usually small and multiple (Chen and Mott 1990; Arjona et al. 1995). The bile duct and the gallbladder may contain blood mixed with bile (haemobilia), blood clots and fibrinous plugs.
Symptomatology in children from human endemic areas of Peru includes abdominal pain localized in the epigastrium, the Murphy symptom and jaundice as the most frequent clinical biliary characteristics, the rest of the symptoms being non-specific (Marcos Raymundo et al. 2002).
The duration and intensity of fasciolid infection and liver damage have been experimentally verified to be associated with bacterobilia by Escherichia coli (45% of cases), Enterococcus faecalis (45%) and Klebsiella pneumoniae (10%). This supports that the obstruction caused by advanced chronic fasciolosis may be related to biliary sepsis. These results lead to a reconsideration of treatment features in human disease, i.e. therapeutic strategies should also consider the possibility of bacterial coinfection (Valero et al. 2006b).
6.6.3 Clinical Laboratory Analyses
The outstanding abnormal laboratory findings concern leucocytosis, eosinophilia, anaemia, erythrocyte sedimentation rate, hepatic functions and serum immunoglobulin levels (Chen and Mott 1990; Mas-Coma et al. 1999b, 2000).
-
Leucocytosis and eosinophilia: In the acute phase, the leucocyte counts are usually over 10,000 up to 43,000/mm3. The eosinophil count is nearly always greater than 5% of the total leucocytes and may be as high as 83%. In a developed country, blood eosinophilia and the ingestion of watercress or any other suggestive freshwater plant in anamnesis are extremely useful in guiding towards a fascioliasis diagnosis. Unfortunately, these two aspects are usually not helpful in human endemic areas of developing countries, where eosinophilia may be also caused by other helminth infections and local food traditions including the ingestion of many uncooked plants may mask liver fluke infection sources (Mas-Coma et al. 2014).
-
Anaemia: Anaemia is common but usually not very severe and mostly between 7.0 and 13.5 g dl−1 haemoglobin. Levels as low as 2.8 and 4.0 g dl−1 have been reported.
-
Erythrocyte sedimentation rate: The erythrocyte sedimentation rate may be high in the acute phase, reaching 165 mm in an hour, normal in the latent phase and normal or only moderately high in the obstructive phase.
-
Hepatic functions: Abnormal results in liver function tests may be found both in the invasive and biliary periods.
-
In the invasive period, data are inconsistent. Abnormal results may be obtained in hepatic function tests. In the acute phase, results sometimes include a rise of the two aminotransferases (formerly transaminases) most frequently utilized, namely, alanine aminotransferase (ALT, formerly serum glutamic pyruvate transaminase—SGPT) and aspartate aminotransferase (AST, formerly serum glutamate oxaloacetic transaminase—SGOT), as well as elevated thymol turbidity, zinc sulphate turbidity, serum globulin and serum bilirubin. In other cases, tests give normal results, with the exception of alkaline phosphatase (AKP or ALP). Serum electrophoresis may show an increase of α2- and γ-globulins. Serum triglycerides and very-low-density lipoproteins have been seen to increase, while total serum cholesterol, high-density lipoprotein cholesterol and low-density lipoprotein cholesterol exhibited a significant decrease. These changes were due to the degenerative necrotic damage of the hepatocytes. Other reported findings include abnormally high levels of β-glucuronidase.
-
In the biliary period, jaundice is a prominent feature. Serum bilirubin levels between 2.0 and 8.6 have been reported. Biliary colic is usually followed by a higher level of serum bilirubin as well as dark urine positive for bilirubin. Serum bilirubin may be normal in this phase and between attacks of biliary colic. AKP, GPT, GOT and serum globulin (mainly γ-globulin) are often elevated in this phase, while albumin is decreased.
-
-
Immunoglobulins: Levels for IgG, IgM and IgE are usually elevated. Specific IgE antibodies were detected in 48% of the patients. Total and specific IgE levels have been shown to be positively correlated with the egg burden, age, clinical features and degree of eosinophilia. IgA levels are usually normal but may be sometimes elevated.
6.7 Diagnosis
Several suggestive clinical presentation aspects may be useful, mainly in human endemic areas where physicians are aware about liver fluke infection risk in humans. However, verification needs the use of at least one among the direct parasitological techniques or indirect immunological tests. Other non-invasive diagnostic techniques presently available may be additionally helpful. Non-invasive diagnostic techniques which can be used for human diagnosis are radiology, radioisotope scanning, ultrasound, computed tomography and magnetic resonance (see reviews in Esteban et al. 1998 and Hillyer 1999).
For the differential diagnosis of F. hepatica and F. gigantica, clinical, pathological, coprological or immunological methods are useless. This is a problem in overlapping areas because this differential diagnosis is very important owing to the different pathological, transmission and epidemiological characteristics of the two fasciolids, as well as due to intermediate forms in which egg measurements may overlap. Despite the recent development of many molecular tests, DNA marker sequencing still remains as the only appropriate method for both haplotyping of the two pure fasciolid species, as well as for the detection of hybridization in intermediate forms. For such a purpose, the complete sequences of the two rDNA spacers ITS-2 and ITS-1 together with those of the complete mtDNA genes cox1 and nad1 have so far proved to be the markers of choice, and an exhaustive baseline and nomenclature for these four markers have already been provided (Mas-Coma et al. 2009a).
The main diagnostic tools continue to rely on stool and blood techniques and have been improved in the last two decades. Present availabilities for human diagnosis have recently been reviewed exhaustively, focusing on advantages and weaknesses, sample management, egg differentiation, qualitative and quantitative diagnosis, antibody and antigen detection, post-treatment monitoring and post-control surveillance (Mas-Coma et al. 2014). Main conclusions referred to the pronounced difficulties of diagnosing fascioliasis given the different infection phases and parasite migration capacities, clinical heterogeneity, immunological complexity, different epidemiological situations and transmission patterns and finally lack of a diagnostic technique covering all needs and situations (Mas-Coma et al. 2014).
In livestock, it should be distinguished between (1) diagnosis of animal infection, (2) evaluation of drug efficacy and (3) evaluation of drug resistance. A number of tests are therefore available, including a few tests allowing for burden estimation by quantification by faecal egg counts, serological and coprological methods, egg hatch assays, molecular techniques and even histological methods (Fairweather et al. 2020).
6.7.1 Direct Techniques
Detection and identification of fasciolid eggs in stool sample, duodenal contents or bile continues to be the most appropriate diagnostic strategy for both detection of infection and estimation of intensity. This is even in spite of the recognized lower sensitivity of egg detection in faecal samples and its uselessness for the diagnosis of patients in the acute period, as well as the lack of an accurate relationship between egg counts per gram of faeces and the fluke burden (Valero et al. 2006a, 2009). Identifying fluke adults obtained during an endoscopy after surgical intervention either by microscopic morphometry (Periago et al. 2006) or molecular tools (Mas-Coma et al. 2009a) may also be performed nowadays, although such occasions are evidently not frequent at all. Moreover, the infrastructure for endoscopy or surgery is in general not available in rural endemic areas.
Techniques ranging from a simple direct smear to different concentration methods may be used. Egg concentration has been achieved by flotation and sedimentation techniques. The sedimentation techniques appear to be more accurate and sensitive than flotation techniques (Esteban et al. 1998; Mas-Coma et al. 1999c).
The size of the fluke eggs has always been used for human diagnosis. Basing on studies in livestock, the borderlines allowing differentiation between the two species were traditionally considered to be 150 μm in length and 90 μm in width, lower values representing F. hepatica and higher values F. gigantica. A study on morphometric traits of fasciolid eggs from different continents revealed that eggs shed by humans show traits different from eggs shed by animals. In humans, F. hepatica eggs are bigger and F. gigantica eggs are smaller than reported to date from livestock, and their measurements overlap when compared. Measurements of F. hepatica and F. gigantica eggs originating from humans and animals from sympatric areas overlap, and, therefore, they do not allow differential diagnosis when within this overlapping range (Valero et al. 2009; Mas-Coma et al. 2014). These new results should aid clinicians since the application of the classic egg size range in human samples may lead to erroneous conclusions. Consequently, fasciolid egg size in human stool samples ought to be corrected in books and monographs as well as in guides of medical parasitology and tropical medicine.
Quantitative coprological analyses become important in epidemiological surveys as well as post-treatment monitoring. Egg burden is also crucial in the moment of deciding the appropriate treatment dose. The 400-epg threshold has been proposed for identifying high-intensity infections. To avoid risk of colic, a repeated, timely spaciated mid-dose is recommended in patients shedding more than 400 eggs (WHO 2007; Valero et al. 2012b). The second half of the regimen is administered 24 h later, once the absence of secondary effects is verified. The Kato-Katz technique appears to be appropriate, because of its simplicity, very low cost and reproducibility (Mas-Coma et al. 1999b). Its low sensitivity may be solved by repeated application.
Besides eggs in coprological analyses, adults and eggs may be also found elsewhere by means of other invasive techniques: obtaining duodenal fluid, duodenal and biliary aspirates; surgery (laparotomy, cholecystectomy, sphincterotomy); and histological examination of the liver and/or other organ biopsy materials (Mas-Coma et al. 1999b).
6.7.2 Indirect Techniques
Numerous serological, intradermal and stool antigen detection tests have been developed. Immunological techniques present the advantages of being applicable during all periods of the disease, but fundamentally during the invasive or acute period, as well as to the other situations in which coprological techniques may present problems. However, immunological techniques offer other types of problems related mainly to sensibility and specificity and are not able to differentiate between infection by F. hepatica and that by F. gigantica.
Efforts have been concentrated in obtaining purified excretory/secretory antigens and/or recombinant molecules to improve serological tests, owing to the problems of the parasitological diagnosis because of the delay in its usefulness in the acute period (coprological examination positive only after 3–4 months postinfection), intermittent egg output dynamics, very low or even absence of egg shedding in cases of only one or a few fluke adults and old chronic infections, ectopic infections, “false” fascioliasis related to eggs in transit after ingestion of infected liver from domestic animals or flukes unable to attain maturity in human subjects in non-human endemic areas (Esteban et al. 1998; Mas-Coma et al. 1999b).
Cysteine proteinases offer highly sensitive and specific markers for human fascioliasis serodiagnosis for F. hepatica (O'Neill et al. 1999; Strauss et al. 1999; Espinoza et al. 2007; Mezo et al. 2004) as well as for F. gigantica infection (Maleewong et al. 1999; Intapan et al. 1998; Tantrawatpan et al. 2005). Fasciola hepatica recombinant cysteine proteinases produced in yeast (O'Neill et al. 1999) or in Escherichia coli (Carnevale et al. 2001) have been used in ELISA methods for human infection diagnosis.
Studies in Bolivia and Peru have shown that the MM3 coproantigen-detection test allows for high sensitivity and specificity, fast large mass screening capacity, detection in the chronic period, early detection of treatment failure or reinfection in post-treated subjects and usefulness for surveillance programmes. However, this technique falls short when evaluating the fluke burden on its own (Valero et al. 2012b). The use of a new preservative/diluent CoproGuard™, developed for preservation of Fasciola coproantigens, proved to enhance coproantigen extraction and the antigenicity throughout the complete observation period (Ubeira et al. 2009).
The commercialized DRG Fasciola hepatica IgG (human) ELISA proved to be highly sensitive and specific, with a high negative predictive value but a low positive predictive value. No correlation with egg output was observed. This test may be used both as an individual serodiagnostic test when backed up by a compatible clinical history together with a second diagnostic technique for other cross-reactive helminth infections and in future large-scale epidemiological studies (Valero et al. 2012c).
A new lateral flow test (SeroFluke) for human diagnosis appears to be a useful step forward (Martinez-Sernandez et al. 2011). In comparison with an ELISA test (MM3-SERO), the SeroFluke test showed maximal specificity and sensitivity and the advantage of being applicable to both serum and whole blood samples. Its simplicity allows it to be used in major hospitals as well as in endemic/hyperendemic regions.
6.8 Treatment
Emetine and the better tolerated dehydroemetine were used widely and still continue to be used today, given intramuscularly or subcutaneously at doses of 1–10 mg/kg a day for 10 days. However, the use of emetine was progressively abandoned due to their toxic side effects involving the heart, liver and digestive tract (Mas-Coma et al. 2014).
Chloroquine improved the symptoms when applied in the acute phase. Bithionol was proposed as the drug of choice for fascioliasis treatment during the last three decades of the last century. It was usually applied at a dose of 30–50 mg/kg daily, divided into three oral doses on alternate days for 20–30 days. Occasionally, the patients required a second course to obtain a complete cure. The side effects were usually mild (Chen and Mott 1990; Esteban et al. 1998).
Regarding praziquantel, it is generally accepted today that Fasciola may be the only trematode genus that has practically no response to praziquantel. Metronidazole and albendazole and sporadically also mebendazole have been also applied for human fascioliasis treatment with more or less success.
Triclabendazole (Egaten®) has become the drug of choice for human fascioliasis caused by both F. hepatica and F. gigantica at present (Savioli et al. 1999; Gandhi et al. 2019). This drug is better adsorbed if administered after meals (Lecaillon et al. 1998). The recommended dosage is two separate regimens of 10 mg/kg. A cure rate of 79.2% when first used and 100% after a second round of therapy was found in Chile (Apt et al. 1995) and 79.4% and 93.9%, respectively, in Egypt (El-Morshedy et al. 1999). Triclabendazole appears to keep its efficiency at standard regimes in human endemic areas after years (Talaie et al. 2004), although the need for a third dose has been reported in Cuba (Millan et al. 2000). This drug has moreover recently proved to be safe in the treatment of very small children (De et al. 2020).
Unfortunately, the risk of appearance of resistance to triclabendazole cannot be forgotten. Triclabendazole resistance was first described in Australia and later in European countries such as Ireland, Scotland, the Netherlands and Spain (see review in Mas-Coma et al. 2007). Very recently, it has also been found in southern Brazil (Oliveira et al. 2008) and Argentina (Olaechea et al. 2011). Up to that moment, triclabendazole resistance only concerned livestock in animal endemic areas, but unfortunately, it has very recently been also described (Ortiz et al. 2013) in a human highly endemic area such as Cajamarca, Peru (Gonzalez et al. 2011). Our understanding of the triclabendazole resistance mechanism remains far from complete, so that there is even a knowledge gap regarding its spreading capacity. A multigenic resistance origin has been suggested to underlie this resistance. Strategies to minimize the development of resistance include the use of synergistic drug combinations (Fairweather et al. 2020). Combinations of flukicides, anthelmintics and other drugs may be also useful. A number of existing flukicides for veterinary use are active against triclabendazole-resistant fasciolids, including albendazole, clorsulon, closantel, nitroxynil and oxyclozanide, although these alternatives do not act against migrating juveniles (Fairweather et al. 2020).
Nitazoxanide is a good alternative to triclabendazole, at least for the chronic stage of fascioliasis, mainly in those countries where Egaten® is still not registered but nitazoxanide is since several years. Nitazoxanide had demonstrated its efficacity against human fascioliasis in a few trials, in Egypt (Rossignol et al. 1998; Kabil et al. 2000) and Peru (Favennec et al. 2003). Its long 7-day treatment course may nevertheless become a problem. However, its usefulness for the treatment of human cases not responding to triclabendazole (Gargala et al. 2005) is of important additional value. A good nitazoxanide efficacy has recently been reported when applied to liver fluke-infected children in Mexico (Zumaquero-Ríos et al. 2013). However, differences in fasciolid susceptibility to nitazoxanide may exist depending on geographical strains. Thus, no response to nitazoxanide treatment was reported in 24 cases of liver fluke infection in Esmeralda, Camagüey, Cuba (Del Risco et al. 2001), and a triclabendazole-resistant F. hepatica-infected patient not responding to nitazoxanide treatment has recently been reported in the Netherlands (Winkelhagen et al. 2012).
A deep analysis of all the drugs presently available for the treatment of fascioliasis in both animals and humans has been recently published. Egg formation, production, development and viability are crucial in fascioliasis transmission and sensitive to drug action. A number of protocols or egg hatch tests have been developed to study drug action impact on the development and hatching of fasciolid eggs, but there is no standardized method (Fairweather et al. 2020).
6.9 Prognosis, Complications, Sequelae and Death Causes
The prognosis of fascioliasis depends on the promptness of the treatment. At the phase of hepatic invasion (acute phase), the treatment most usually gives rise to cure without sequelae. However, when treated late, the prognosis becomes subordinated to the importance of the affection of the biliary ducts.
With regard to cure criteria, from the clinical point of view, the improvement of the general condition of the patient with fever disappearance and weight recovery indicates a good prognosis, although one should be cautious as relapses are possible. The normalization of blood eosinophilia as best criterion in all cases, the disappearance of eggs in stools in cases of patients diagnosed in the biliary phase and the progressive disappearance of hepatic function test abnormalities are helpful indicators of treatment effectivity (Mas-Coma et al. 2014).
One complication may be bleeding. Subcapsular haematoma and severe haemobilia have been reported. Haematemesis and melaena were associated with obstructive jaundice, epigastric pain and severe anaemia. The sources of the bleeding were all identified from laparotomy, and other causes of upper gastrointestinal bleeding have been carefully ruled out. In one case, bleeding occurred due to an ulcer in the common bile duct, and in other cases, no single bleeding point was detected in the common bile ducts and/or in the gallbladders.
Biliary cirrhosis is another complication. During the course of the infection, inflammation, hyperplasia and hypertrophy of the bile duct epithelia may induce periductal fibrosis. Prolonged heavy infection rarely leads to biliary cirrhosis. The outstanding findings on physical examinations were firm untender hepatomegaly with or without jaundice and ascites. Splenomegaly was not prominent. Sclerosing cholangitis with biliary cirrhosis was detected by endoscopic retrograde cholangiopancreatography.
Another severe complication is the multiple extrahepatic venous thrombosis. In the post-mortem examination of one patient who died suddenly, multiple thrombosis of the ovaric, suprahepatic, mesenteric and myocardial veins, along with massive pulmonary embolism, was disclosed. During the invasion period, another patient developed a complete thrombosis of the superior vena cava (Mas-Coma et al. 1999b, 2000).
The severity of fascioliasis was emphasized in many cases, with regard to the progressive general deterioration of the patients with slimming, anorexia and physical and neuropsychic asthenia, as well as the fact that cure does not mean total recovery but that fascioliasis left them as handicapped and frail subjects. In several patients presenting neurological and ocular manifestations, given sequelae were noted to persist despite treatment. These sequelae were sometimes important, even making difficult or impeding the professional activity of the patient (Mas-Coma et al. 2014).
Several deaths related to fasciolosis have been reported in the recent literature. Post-mortem examination of a patient who died from an acute liver condition showed F. hepatica to be responsible for blockage of the bile duct. More than 40 flukes were detected from the liver of a patient at autopsy. Between 1 and 14 flukes were found in each liver at post-mortem in 81 inhabitants of the Samarkand region in 1968–1986, although deaths were not presumed to be due to fasciolosis. However, in human hyperendemic zones with depauperate socio-economic status, unhygienic conditions and high child morbidity and mortality, studies are still needed to ascertain whether fasciolosis may be related to death, above all in very young children (Mas-Coma and Bargues 1997; Mas-Coma et al. 2000). Many fatal cases have been reported among patients suffering from neurological disorders, whether due to direct or indirect affection of the central nervous system (Mas-Coma et al. 2013, 2014).
6.10 Prevention and Control
Studies on human endemic areas performed in the last two decades have shown that traditional epidemiological patterns of animal fascioliasis may not always explain the characteristics of human infection in a given area. Therefore, control measures for human fascioliasis should consider the results of the ecoepidemiological studies previously undertaken in the area concerned (Mas-Coma et al. 2009a). This is the reason why the World Health Organization (WHO) launched a worldwide initiative against this disease including different control strategies depending on the human endemic areas and countries. A recent complete analysis of individual and general preventive measures to avoid human infection has shown a scenario more complicated than that considered in the past (Mas-Coma et al. 2018).
6.10.1 Prevention of Human Infection
The prevention of human infection may be achieved by strict control of the human infection sources, mainly with regard to watercress and other aquatic plants for human consumption, especially in endemic zones. Unfortunately, potassium permanganate, which had been suggested to be the most effective preventive tool for killing metacercariae attached to leaves and vegetables used in salads, has been shown to have no effectivity on metacercarial viability, even at very high doses (Ashrafi et al. 2006).
Moreover, it should be considered that infection risks shall not be restricted to only ingestion of freshwater vegetables, as always mentioned. The different human infection sources may be taken into account, mainly in human endemic areas. Drinking of natural freshwater should be avoided in human endemic areas. In the Nile Delta region, persons living in houses where piped water is present showed to have a higher infection risk (Curtale et al. 2003).
The possibility of human infection in urban areas should not be neglected. Thanks to transport of vegetables (both aquatic and terrestrial) from rural endemic zones to cities, plants carrying metacercariae can be sold in non-controlled city markets giving rise to urban infection (Fig. 6.4) (Mas-Coma 2004).

Uncontrolled sale of vegetables involved in the transmission of human fascioliasis in a city market in Quy Nhon, Vietnam (Orig. S. Mas-Coma)
Education should always be included within general control measures to be applied in human endemic areas, mainly to let inhabitants know about the human infection sources. The community should be appropriately informed about the disease, its pathogenicity, its transmission and where to go for diagnosis if suggestive symptoms appear.
6.10.2 Control Measures at Community Level
The availability of triclabendazole prompted the WHO to launch a decisive step forward within its worldwide initiative against human fascioliasis (WHO 2007, 2008) in recent years. This initiative includes action in human fascioliasis endemic areas presenting different epidemiological situations and transmission patterns (Mas-Coma 2005; Mas-Coma et al. 2009a). Pilot schemes were designed to assess the best control strategies according to the different epidemiological situations and transmission patterns in the way to decrease morbidity, mainly in children. Selective patient treatment after passive detection in hospitals was the strategy applied in Vietnam and infected subject treatment after active detection in surveys the one applied in Egypt. The Northern Altiplano in Bolivia was chosen as an example of the altiplanic pattern, while Cajamarca, Peru, was chosen as an example of the valley pattern. The pilot interventions in these two Andean areas demonstrated the absence of severe side effects in triclabendazole treatments of schoolchildren (Villegas et al. 2012), which subsequently allowed for the launching of mass treatments. Many other countries are nowadays receiving yearly triclabendazole donations through WHO for the treatment of their patients, in an expansion of the aforementioned WHO initiative.
In countries where watercress is included in food traditions, such as France, commercial growing of watercress should be carried out under completely controlled conditions, without access for ruminants and snail vectors to the watercress cultures.
In Egypt, the construction and utilization of the so-called washing units, in which the water was appropriately filtered, gave rise to a marked decrease of human infection in a locality of the Nile Delta region where a high prevalence in humans was initially found (Mas-Coma 2004).
The World Health Organization is recently launching an initiative to assess One Health control action to complement the preventive chemotherapy campaigns in human endemic areas, with the aim to decrease the infection and reinfection risk in between the yearly triclabendazole mono-dose mass treatments. This initiative comprises several multidisciplinary axes, including the environment, snail vectors, animal reservoirs and humans, all together considered from the dynamic point of view of the changes induced by climate change and global change factors (Bargues et al. 2020, 2021; Mas-Coma et al. 2020a, b, 2021).
6.10.3 Progress in Vaccinology
Initial research focused on the identification of molecules of fasciolid parasites that played critical functions at the host-parasite interface, by way of isolating and characterizing the molecules that were secreted by the flukes. ES products from adult worms showed two fractions: a > 200 kDa fraction including several proteins and other molecules and a 40 kDa fraction consisting of cathepsin L cysteine peptidases subsequently fractioned into two subfractions presenting distinct enzymatic activities—cathepsin L1 (FhCL1) and cathepsin L2 (FhCL2) (Dalton et al. 1996). Cattle vaccination with FhCL1 induced protection levels of up to 69.5%, and combination vaccines reached a 72.4%. These vaccines also exhibited significant anti-fecundity effects of reduced egg output and lower egg viability in up to 98%. Thus, vaccines were showing for the first time that they could potentially block the transmission of the disease. Assays were further developed by using different adjuvants.
The development of high-level protective vaccines that can also impact on disease transmission may require combinations of various parasite molecules. Therefore, two new important vaccine candidates have been identified, peroxidase (FhPrx) and helminth defence molecule (FhHDM), that also perform potent immunomodulatory functions (Robinson et al. 2013). Several other Fasciola molecules hold promise as components of combination vaccines, including glutathione S-transferase (FhGST), cathepsin B (FhCB1–10), fatty acid-binding protein (FhFABP) and leucine aminopeptidase (FhLAP) (Spithill et al. 2012).
In sheep, FhLAP was shown to induce protective responses both alone and in combination with FhCL1 and FhCL2 in native form (Piacenza et al. 1999). Moreover, impressive levels of protection have been observed in sheep (up to 87%) vaccinated with a recombinant FhLAP formulated in adjuvants that induce high-titre IgG1 and IgG2 (Maggioli et al. 2011).
Unfortunately, two challenges appear far from being solved at present. The first is the rapid and potent ability of F. hepatica to suppress the protective arm of the immune response, which explains why infected hosts do not develop immune resistance and provides a reasonable explanation for why efforts have been largely unsuccessful in developing efficacious vaccines against Fasciola in animals. Indeed, fluke-induced immunomodulation/immunosuppression is induced rapidly upon Fasciola invasion and maintained through the chronic infection. It is mediated by fluke molecules that alter the function of innate immune cells (dendritic cells, macrophages, mast cells) and the quality and magnitude of adaptive immune cell (T and B cells) responses (Dalton et al. 2013). The second challenge refers to the differences in cell- and/or antibody-mediated responses depending on host species, which means that even being successful in obtaining an effective vaccine against animal infections, this will not allow for a direct extrapolation to a vaccine for humans. However, the wide knowledge obtained on the immunological processes and molecules involved will undoubtedly facilitate the development of a vaccine for human use in the future.
6.11 Acknowledgements
Review of human fascioliasis carried out within the Health Research Project No. PI16/00520, Subprograma Estatal de Generación de Conocimiento de la Acción Estratégica en Salud (AES) y Fondos FEDER, Plan Estatal de Investigación Científica y Técnica y de Innovación, ISCIII-MINECO, Madrid, Spain; ISCIII-RETIC RD12/0018/0013, Red de Investigación de Centros de Enfermedades Tropicales (RICET), of the Program of Redes Temáticas de Investigación Cooperativa RETICS/FEDER, Ministry of Health and Consumption, Madrid, Spain; and PROMETEO/2016/099, of the Program of Ayudas para Grupos de Investigación de Excelencia, Generalitat Valenciana, Valencia, Spain
References
Acosta-Ferreira W, Vercelli-Retta J, Falconi LM (1979) Fasciola hepatica human infection. Histopathological study of sixteen cases. Virchows Arch A (Pathological Anatomy and Histology) 383:319–327
Afshan K, Fortes-Lima CA, Artigas P, Valero MA, Qayyum M, Mas-Coma S (2014) Impact of climate change and man-made irrigation systems on the transmission risk, long-term trend and seasonality of human and animal fascioliasis in Pakistan. Geospat Health 8:317–334
Apt W, Aguilera X, Vega F, Miranda C, Zulantay I, Perez C, Gabor M, Apt P (1995) Treatment of human chronic fascioliasis with triclabendazole: drug efficacy and serologic response. Am J Trop Med Hyg 52:532–535
Arjona R, Riancho JA, Aguado JM, Salesa R, Gonzalez-Macias J (1995) Fascioliasis in developed countries: a review of classic and aberrant forms of the disease. Medicine (Baltimore) 74:13–23
Artigas P, Bargues MD, Mera y Sierra R, Agramunt VH, Mas-Coma S (2011) Characterisation of fascioliasis lymnaeid intermediate hosts from Chile by DNA sequencing, with emphasis on Lymnaea viator and Galba truncatula. Acta Trop 120:245–257
Ashrafi K, Valero MA, Massoud J, Sobhani AR, Solaymani-Mohammadi S, Conde P, Khoubbane M, Bargues MD, Mas-Coma S (2006) Plant-borne human contamination by fascioliasis. Am J Trop Med Hyg 75:295–302
Bargues MD, Vigo M, Horak P, Dvorak J, Patzner RA, Pointier JP, Jackiewicz M, Meier-Brook C, Mas-Coma S (2001) European Lymnaeidae (Mollusca: Gastropoda), intermediate hosts of trematodiases, based on nuclear ribosomal DNA ITS-2 sequences. Infect Genet Evol 1(2):85–107
Bargues MD, Artigas P, Mera y Sierra RL, Pointier JP, Mas-Coma S (2007) Characterisation of Lymnaea cubensis, L. viatrix and L. neotropica n. sp., the main vectors of Fasciola hepatica in Latin America, by analysis of their ribosomal and mitochondrial DNA. Ann Trop Med Parasit 101:621–641
Bargues MD, Artigas P, Khoubbane M, Flores R, Glöer P, Rojas-Garcia R, Ashrafi K, Falkner G, Mas-Coma S (2011a) Lymnaea schirazensis, an overlooked snail distorting fascioliasis data: genotype, phenotype, ecology, worldwide spread, susceptibility, applicability. PLoS One 6(9):e24567. (33 pp. + 3 Suppl. Tables + 5 Suppl. Figures)
Bargues MD, Artigas P, Khoubbane M, Mas-Coma S (2011b) DNA sequence characterisation and phylogeography of Lymnaea cousini and related species, vectors of fascioliasis in northern Andean countries, with description of L. meridensis n. sp. (Gastropoda: Lymnaeidae). Parasite Vect 4:132. (22 pp.)
Bargues MD, Gonzalez C, Artigas P, Mas-Coma S (2011c) A new baseline for fascioliasis in Venezuela: lymnaeid vectors ascertained by DNA sequencing and analysis of their relationships with human and animal infection. Parasite Vect 4:200. (18 pp.)
Bargues MD, Malandrini JB, Artigas P, Soria CC, Velasquez JN, Carnevale S, Mateo L, Khoubbane M, Mas-Coma S (2016) Human fascioliasis endemic areas in Argentina: multigene characterisation of the lymnaeid vectors and climatic-environmental assessment of the transmission pattern. Parasit Vectors 9:306
Bargues MD, Gayo V, Sanchis J, Artigas P, Khoubbane M, Birriel S, Mas-Coma S (2017) DNA multigene characterization of Fasciola hepatica and Lymnaea neotropica and its fascioliasis transmission capacity in Uruguay, with historical correlation, human report review and infection risk analysis. PLoS Negl Trop Dis 11:e0005352
Bargues MD, Artigas P, Angles R, Osca D, Duran P, Buchon P, Gonzales-Pomar RK, Pinto-Mendieta J, Mas-Coma S (2020) Genetic uniformity, geographical spread and anthropogenic habitat modifications of lymnaeid vectors found in a One Health initiative in the highest human fascioliasis hyperendemic of the Bolivian Altiplano. Parasit Vectors 13:171
Bargues MD, Angles R, Coello J, Artigas P, Funatsu IR, Cuervo PF, Buchon P, Mas-Coma S (2021) One Health initiative in the Bolivian Altiplano human fascioliasis hyperendemic area: Lymnaeid biology, population dynamics, microecology and climatic factor influences. Braz J Vet Parasitol 30:e025620
Brady MT, O’Nneill SM, Dalton JP, Mills KH (1999) Fasciola hepatica suppresses a protective Th1 response against Bordetella pertussis. Infect Immun 67:5372–5378
Bergquist R, Luvall JC, Malone JB (2021) The changing risk of vector-borne diseases: global satellite remote sensing and geospatial surveillance at the forefront. Geospat Health 16:1047
Carnevale S, Rodriguez MI, Guarnera EA, Carmona C, Tanos T, Angel SO (2001) Immunodiagnosis of fasciolosis using recombinant procathepsin L cysteine proteinase. Diagn Microbiol Infect Dis 41:43–49
Chen MG, Mott KE (1990) Progress in assessment of morbidity due to Fasciola hepatica infection: a review of recent literature. Trop Dis Bull 87(4):R1–R38
Curtale F, Mas-Coma S, Hassanein YAE, Barduagni P, Pezzotti P, Savioli L (2003) Clinical signs and household characteristics associated with human fascioliasis among rural population in Egypt: a case-control study. Parassitologia 45:5–11
Cwiklinski K, Dalton JP, Dufresne PJ, La Course J, Williams DJL, Hodgkinson J, Paterson S (2015) The Fasciola hepatica genome: gene duplication and polymorphism reveals adaptation to the host environment and the capacity for rapid evolution. Genome Biol 16:71
Dalton JP, McConigle S, Rolph TP, Andrews SJ (1996) Induction of protective immunity in cattle against infection with Fasciola hepatica by vaccination with cathepsin L proteinases and with hemoglobin. Infect Immun 64:5066–5074
Dalton JP, Robinson MW, Mulcahy G, O'Neill SM, Donnelly S (2013) Immunomodulatory molecules of Fasciola hepatica: candidates for both vaccine and immunotherapeutic development. Vet Parasitol 195:272–285
Del Risco BU, Vazquez Drake CT, Garcia Gonzalez G, Sanchen Casa A (2001) Evaluación de la excreción de huevos de Fasciola hepatica por tres esquemas terapéuticos. Rev Electr Arch Méd Camagüey 5(4):4
De NV, Le TH, Agramunt VH, Mas-Coma S (2020) Early postnatal and preschool age infection by Fasciola spp.: report of five cases from Vietnam and worldwide review. Am J Trop Med Hyg 103:1578–1589
El-Morshedy H, Farghaly A, Sharaf S, Abou-Basha L, Barakat R (1999) Triclabendazole in the treatment of human fascioliasis: a community-based study. East Medit Health J 5:888–894
Espinoza JR, Maco V, Marcos L, Saez S, Neyra V, Terashima A, Samalvides F, Gotuzzo E, Chavarry E, Huaman C, Bargues MD, Valero MA, Mas-Coma S (2007) Evaluation of Fas2-ELISA for the serological detection of Fasciola hepatica infection in humans. Am J Trop Med Hyg 76:977–982
Espinoza JR, Terashima A, Herrera-Velit P, Marcos LA (2010) Fasciolosis humana yanimal en el Perú: Impacto en la economía de las zonas endémicas. Rev Peru Med Exp Salud Públ 27:604–612
Esteban JG, Flores A, Aguirre C, Strauss W, Angles R, Mas-Coma S (1997a) Presence of very high prevalence and intensity of infection with Fasciola hepatica among Aymara children from the northern Bolivian Altiplano. Acta Trop 66:1–14
Esteban JG, Flores A, Angles R, Strauss W, Aguirre C, Mas-Coma S (1997b) A population-based coprological study of human fascioliasis in a hyperendemic area of the Bolivian Altiplano. Trop Med Int Health 2:695–699
Esteban JG, Bargues MD, Mas-Coma S (1998) Geographical distribution, diagnosis and treatment of human fascioliasis: a review. Res Rev Parasitol 58:13–42
Esteban JG, Flores A, Angles R, Mas-Coma S (1999) High endemicity of human fascioliasis between Lake Titicaca and La Paz valley, Bolivia. Trans R Soc Trop Med Hyg 93:151–156
Esteban JG, Gonzalez C, Bargues MD, Angles R, Sanchez C, Naquira C, Mas-Coma S (2002) High fascioliasis infection in children linked to a man-made irrigation zone in Peru. Trop Med Int Health 7:339–348
Esteban JG, Gonzalez C, Curtale F, Muñoz-Antoli C, Valero MA, Bargues MD, El Sayed M, El Wakeel A, Abdel-Wahab Y, Montresor A, Engels D, Savioli L, Mas-Coma S (2003) Hyperendemic fascioliasis associated with schistosomiasis in villages of the Nile Delta, Egypt. Am J Trop Med Hyg 69:429–437
Fairweather I, Brennan GP, Hanna REB, Robinson MW, Skuce PJ (2020) Drug resistance in liver flukes. Int J Parasitol Drugs Drug Resist 12:39–59
Favennec L, Jave Ortiz J, Gargala G, Lopez Chegne N, Ayoub A (2003) Double blind, randomized, placebo-controlled study of nitazoxanide in the treatment of fascioliasis in adults and children from northern Peru. Alim Pharmacol Ther 17:265–270
Gandhi P, Schmitt EK, Chen CW, Samantray S, Venishetty VK, Hughes D (2019) Triclabendazole in the treatment of human fascioliasis: a review. Trans R Soc Trop Med Hyg 113:797–804
Gargala G, Abboud P, Borsa-Lebas F, Courchay E, Koning E, Favennec L, Caron F (2005) Case report of successful treatment of triclabendazole resistant fascioliasis by nitazoxanide. In Medicine and health in the tropics (XVIth International Congress for tropical medicine and malaria, Marseille, France, 11–15 Sept. 2005), Abstract Book, P680: 283
Gil-Benito A, Ciolkovitch A, Mas-Coma S, Quilici M (1991) Enquête sur la distomatose à Fasciola hepatica en Corse. Méditerranée Médicale (Marseille) 403:21–25
Girones N, Valero MA, Garcia-Bodelon MA, Chico-Calero MI, Punzon C, Fresno M, Mas-Coma S (2007) Immune suppression in advanced chronic fascioliasis: an experimental study in a rat model. J Infect Dis 195:1504–1512
Gonzalez LC, Esteban JG, Bargues MD, Valero MA, Ortiz P, Naquira C, Mas-Coma S (2011) Hyperendemic human fascioliasis in Andean valleys: an altitudinal transect analysis in children of Cajamarca province, Peru. Acta Trop 120:119–129
Gonzalez-Miguel J, Valero MA, Reguera-Gomez M, Mas-Bargues C, Bargues MD, Simon-Martin F, Mas-Coma S (2019) Numerous Fasciola plasminogen-binding proteins may underlie blood-brain barrier leakage and explain neurological disorder complexity and heterogeneity in the acute and chronic phases of human fascioliasis. Parasitology 146:284–298
Hillyer GV (1999) Immunodiagnosis of human and animal fasciolosis. In: Dalton JP (ed) Fasciolosis. CAB International Publishing, Wallingford, pp 435–447
Intapan PM, Mallewong W, Wongkham C, Tomanakarn K, Ieamviteevanich K, Pipitgool V, Sukolapong V (1998) Excretory-secretory antigen components of adult Fasciola gigantica recognized by infected human sera. Southeast As J Trop Med Publ Health 29:579–583
Jaffar Z, Sivakuru T, Roberts K (2004) CD4(+)CD25(+) T cells regulate airway eosinophilic inflammation by modulating the Th2 cell phenotype. J Immunol 172:3842–3849
Kabil SM, El Ashry E, Ashraf NK (2000) An open-label clinical study of nitazoxanide in the treatment of human fascioliasis. Curr Ther Res 61:339–345
Lecaillon JB, Gobdillon J, Campestrini J (1998) Effect of food on bioavailability of triclabendazole in patients with fascioliasis. Br J Clin Pharmacol 45:601–604
Maggioli G, Acosta D, Silveira F, Rossi S, Giacaman S, Basika T, Gayo V, Rosadilla D, Roche L, Tort J, Carmona C (2011) The recombinant gut-associated M17 leucine aminopeptidase in combination with different adjuvants confers a high level of protection against Fasciola hepatica in sheep. Vaccine 29:9057–9063
Maleewong W, Wongkham C, Intapan PM, Pipitgol V (1999) Fasciola gigantica-specific antigens: purification by a continuous-elution method and its evaluation for the diagnosis of human fascioliasis. Am J Trop Med Hyg 61:648–651
Marcos Raymundo LA, Maco Flores V, Terashima Iwashita A, Samalvides Cuba F, Gotuzzo Herencia E (2002) Características clínicas de la infección crómica por Fasciola hepatica en niños. Rev Gastroenterol Peru 22:228–233
Marcos LA, Busalleu A, Terashima A, Espinoza JR (2009) Detection of antibodies against Fasciola hepatica in cirrhotic patients from Peru. J Helminthol 83:23–26
Martinez-Sernandez V, Muiño L, Perteguer MJ, Garate T, Mezo M, Gonzalez-Warleta M, Muro A, Correia da Costa JM, Romaris F, Ubeira FM (2011) Development and evaluation of a new lateral flow immunoassay for serodiagnosis of human fasciolosis. PLoS Negl Trop Dis 5(11):e1376
Mas-Coma S (2004) Human fascioliasis. In: Cotruvo JA, Dufour A, Rees G, Bartram J, Carr R, Cliver DO, Craun GF, Fayer R, Gannon VPJ (eds) World Health Organization (WHO), waterborne Zoonoses: identification, causes and control. IWA Publishing, London, pp 305–322
Mas-Coma S (2005) Epidemiology of fascioliasis in human endemic areas. J Helminthol 79:207–216
Mas-Coma S (2020) Human fascioliasis emergence risks in developed countries: from individual patients and small epidemics to climate and global change impacts. Enf Infec Microbiol Clín 38(6):253–256
Mas-Coma S, Bargues MD (1997) Human liver flukes: a review. Res Rev Parasitol 57:145–218
Mas-Coma S, Angles R, Esteban JG, Bargues MD, Buchon P, Franken M, Strauss W (1999a) The northern Bolivian Altiplano: a region highly endemic for human fascioliasis. Trop Med Int Health 4:454–467
Mas-Coma S, Bargues MD, Esteban JG (1999b) Human Fasciolosis. In: Dalton JP (ed) Fasciolosis. CAB International Publishing, Wallingford, pp 411–434
Mas-Coma S, Esteban JG, Bargues MD (1999c) Epidemiology of human fascioliasis: a review and proposed new classification. Bull WHO 77:340–346
Mas-Coma S, Bargues MD, Marty AM, Neafie RC (2000) Hepatic Trematodiases. In: Meyers WM, Neafie RC, Marty AM, Wear DJ (eds) Pathology of infectious diseases, Vol. 1 helminthiases armed forces. Institute of Pathology and American Registry of Pathology, Washington DC, pp 69–92
Mas-Coma S, Bargues MD, Valero MA, Fuentes MV (2003) Adaptation capacities of Fasciola hepatica and their relationships with human fascioliasis: from below sea level up to the very high altitude. In: Combes C, Jourdane J (eds) Taxonomy, ecology and evolution of metazoan parasites, vol 2. Presses Universitaires de Perpignan, Perpignan, pp 81–123
Mas-Coma S, Bargues MD, Valero MA (2005) Fascioliasis and other plant-borne trematode zoonoses. Int J Parasitol 35:1255–1278
Mas-Coma S, Bargues MD, Valero MA (2007) Plant-borne trematode zoonoses: fascioliasis and fasciolopsiasis. In: Murrell D, Fried B (eds) World class parasites, Vol. 11. Food-borne parasites, fish and plant-borne parasites, vol 11. Springer Verlag, New York, pp 293–334
Mas-Coma S, Valero MA, Bargues MD (2009a) Fasciola, lymnaeids and human fascioliasis, with a global overview on disease transmission, epidemiology, evolutionary genetics, molecular epidemiology and control. Adv Parasitol 69:41–146
Mas-Coma S, Valero MA, Bargues MD (2009b) Climate change effects on trematodiases, with emphasis on zoonotic fascioliasis and schistosomiasis. Vet Parasitol 163:264–280
Mas-Coma S, Agramunt VH, Valero MA (2013) Direct and indirect affection of the central nervous system by Fasciola infection. Handb Clin Neurol 114:297–310
Mas-Coma S, Agramunt VH, Valero MA (2014) Neurological and ocular fascioliasis in humans. Adv Parasitol 84:27–149
Mas-Coma S, Bargues MD, Valero MA (2018) Human fascioliasis infection sources, their diversity, incidence factors, analytical methods and prevention measures. Parasitology 145(13,Special Issue):1665–1699
Mas-Coma S, Buchon P, Funatsu IR, Angles R, Artigas P, Valero MA, Bargues MD (2020a) Sheep and cattle reservoirs in the highest human fascioliasis hyperendemic area: experimental transmission capacity, field epidemiology, and control within a One Health initiative in Bolivia. Front Vet Sci 7:583204
Mas-Coma S, Buchon P, Funatsu IR, Angles R, Mas-Bargues C, Artigas P, Valero MA, Bargues MD (2020b) Donkey fascioliasis within a One Health control action: transmission capacity, field epidemiology, and reservoir role in a human hyperendemic area. Front Vet Sci 7:591384
Mas-Coma S, Funatsu IR, Angles R, Buchon P, Mas-Bargues C, Artigas P, Valero MA, Bargues MD (2021) Domestic pig prioritized in one health action against fascioliasis in human endemic areas: experimental assessment of transmission capacity and epidemiological evaluation of reservoir role. One Health 13:100249
McNulty SN, Tort JF, Rinaldi G, Fischer K, Rosa BA, Smircich P, Fontenla S, Choi YJ, Tyagi R, Hallsworth-Pepin K, Mann VH, Kammili L, Latham PS, Dell’Oca N, Dominguez F, Carmona C, Fischer PU, Brindley PJ, Mitreva M (2017) Genomes of Fasciola hepatica from the Americas reveal colonization with Neorickettsia endobacteria related to the agents of Potomac horse and human Sennetsu fevers. PLoS Genet 13:e1006537
Mera y Sierra R, Neira G, Bargues MD, Cuervo PF, Artigas P, Logarzo L, Cortiñas G, Ibaceta DEJ, Lopez Garrido A, Bisutti IE, Mas-Coma S (2020) Equines as reservoirs of human fascioliasis: transmission capacity, epidemiology and pathogenicity in Fasciola hepatica infected mules. J Helminthol 94:e189
Mezo M, Gonzalez-Warleta M, Carro C, Ubeira FM (2004) An ultrasensitive capture ELISA for detection of Fasciola hepatica coproantigens in sheep and cattle using a new monoclonal antibody (MM3). J Parasitol 90:845–852
Millan JC, Mull R, Freise S, Richter J (2000) The efficacy and tolerability of triclabendazole in Cuban patients with latent and chronic Fasciola hepatica infection. Am J Trop Med Hyg 63:264–269
Olaechea F, Lovera V, Larroza M, Raffo F, Cabrera R (2011) Resistance of Fasciola hepatica against Triclabendazole in cattle in Patagonia (Argentina). Vet Parasitol 178:364–366
Oliveira DR, Ferreira DM, Stival CC, Romero F, Cavagnolli F, Kloss A, Araujo F, Molento MB (2008) Triclabendazole resistance involving Fasciola hepatica in sheep and goats during an outbreak in Almirante Tamandare, Parana, Brazil. Rev Brasil Parasitol Vet 17(Supl. 1):149–153
O'Neill SM, Parkinson SM, Dowd AJ, Strauss W, Angles R, Dalton JP (1999) Immunodiagnosis of human fascioliasis using recombinant Fasciola hepatica cathepsin L1 cysteine proteinase. Am J Trop Med Hyg 60:749–751
O'Neill SM, Brady MT, Callanan JJ, Mulcahy G, Joyce P, Mills KH, Dalton JP (2000) Fasciola hepatica infection downregulates Th1 responses in mice. Parasite Immunol 22:147–155
Ortiz P, Scarcella S, Cerna C, Rosales C, Cabrera M, Guzman M, Lamenza P, Solana H (2013) Resistance of Fasciola hepatica against triclabendazole in cattle in Cajamarca (Peru): a clinical trial and in vive efficacy test in sheep. Vet Parasitol 91(1–2):153–158. https://doi.org/10.1016/j.vetpar.2013.01.001
Periago MV, Valero MA, Panova M, Mas-Coma S (2006) Phenotypic comparison of allopatric populations of Fasciola hepatica and Fasciola gigantica from European and African bovines using a computer image analysis system (CIAS). Parasitol Res 99:368–378
Piacenza L, Acosta D, Basmadjian L, Dalton JP, Carmona C (1999) Vaccination with cathepsin L proteinases and with leucine aminopeptidase induces high levels of protection against fascioliasis in sheep. Infect Immun 67:1954–1961
Robinson MW, Dalton JP, O'Brien BA, Donelly S (2013) Fasciola hepatica: the therapeutic potential of a worm secretome. Int. J. Parasitol 43:283–291
Rossignol JF, Abaza H, Friedman H (1998) Successful treatment of human fascioliasis with nitazoxanide. Trans R Soc Trop Med Hyg 92:103–104
Savioli L, Chistulo L, Montresor A (1999) New opportunities for the control of fascioliasis. Bull WHO 77:300
Spithill TW, Carmona C, Piedrafita D, Smooker PM (2012) Prospects for immunoprophylaxis against Fasciola hepatica (liver fluke). In: Caffrey CR, Selzer PM (eds) Parasitic helminths: targets, screens, drugs and vaccines. Wiley-VCH Verlag GmbH & Co, Weinheim
Strauss W, O’Neill SM, Parkinson M, Angles R, Dalton JP (1999) Diagnosis of human fascioliasis: detection of anti-cathepsin L antibodies in blood samples collected on filter paper. Am J Trop Med Hyg 60:746–748
Sunita K, Mas-Coma S, Bargues MD, Sadaf, Khan MA, Habib M, Mustafa S, Husain SA (2021) Buffalo infection by Fasciola gigantica transmitted by Radix acuminata in Uttar Pradesh, India: a molecular tool to improve snail vector epidemiology assessments and control surveillance. Acta Parasitol 66:1396–1405
Talaie H, Emami H, Yadegarinia D, Nava-Ocampo AA, Massoud J, Azmoudeh M, Mas-Coma S (2004) Randomized trial of a single, double and triple dose of 10 mg/kg of a human formulation of triclabendazole in patients with fascioliasis. Clin Exp Pharmacol Physiol 31:777–782
Tantrawatpan C, Maleewong W, Wongkham C, Wongkham S, Intapan PM, Nakashima K (2005) Serodiagnosis of human fascioliasis by cystatin capture enzyme-linked immunosorbent assay with recombinant Fasciola gigantica capthespsin L antigen. Am J Trop Med Hyg 72:82–86
Ubeira FM, Muiño L, Valero MA, Periago MV, Perez-Crespo I, Mezo M, Gonzalez-Warleta M, Romaris F, Paniagua E, Cortizo S, Llovo J, Mas-Coma S (2009) MM3-ELISA detection of Fasciola hepatica coproantigens in preserved human stool samples. Am J Trop Med Hyg 81:156–162
Valero MA, Mas-Coma S (2000) Comparative infectivity of Fasciola hepatica metacercariae from isolates of the main and secondary reservoir animal host species in the Bolivian Altiplano high human endemic region. Folia Parasitol 47:17–22
Valero MA, Santana M, Morales M, Hernandez JL, Mas-Coma S (2003) Risk of gallstone disease in advanced chronic phase of fascioliasis: an experimental study in a rat model. J Infect Dis 188:787–793
Valero MA, De Renzi M, Panova M, Garcia-Bodelon MA, Periago MV, Ordoñez D, Mas-Coma S (2006a) Crowding effect on adult growth, pre-patent period and egg shedding of Fasciola hepatica. Parasitology 133:453–463
Valero MA, Navarro M, Garcia-Bodelon MA, Marcilla A, Morales M, Garcia JE, Hernandez JL, Mas-Coma S (2006b) High risk of bacterobilia in advanced experimental chronic fasciolosis. Acta Trop 100:17–23
Valero MA, Girones N, Garcia-Bodelon MA, Periago MV, Chico-Calero I, Khoubbane M, Fresno M, Mas-Coma S (2008) Anaemia in advanced chronic fasciolosis. Acta Trop 108:35–43
Valero MA, Perez-Crespo I, Periago MV, Khoubbane M, Mas-Coma S (2009) Fluke egg characteristics for the diagnosis of human and animal fascioliasis by Fasciola hepatica and F. gigantica. Acta Trop 111:150–159
Valero MA, Perez-Crespo I, Khoubbane M, Artigas P, Panova M, Ortiz P, Maco V, Espinoza JR, Mas-Coma S (2012a) Fasciola hepatica phenotypic characterisation in Andean human endemic areas: valley versus altiplanic patterns analysed in liver flukes from sheep from Cajamarca and Mantaro, Peru. Infect Genet Evol 12:403–410
Valero MA, Periago MV, Perez-Crespo I, Angles R, Villegas F, Aguirre C, Strauss W, Espinoza JR, Herrera P, Terashima A, Tamayo H, Engels D, Gabrielli AF, Mas-Coma S (2012b) Field evaluation of a coproantigen detection test for fascioliasis diagnosis and surveillance in human hyperendemic areas of Andean countries. PLoS Negl Trop Dis 6(9):e1812. (11 pp.)
Valero MA, Periago MV, Perez-Crespo I, Rodriguez E, Perteguer MJ, Garate T, Gonzalez-Barbera EM, Mas-Coma S (2012c) Assessing the validity of an ELISA test for the serological diagnosis of human fascioliasis in different epidemiological situations. Trop Med Int Health 17:630–636
Valero MA, Bargues MD, Khoubbane M, Artigas P, Quesada C, Berinde L, Ubeira FM, Mezo M, Hernandez JL, Agramunt VH, Mas-Coma S (2016) Higher physiopathogenicity by Fasciola gigantica than by the genetically close F. hepatica: experimental long-term follow-up of biochemical markers. Trans Roy Soc Trop Med Hyg (Special Issue) 110(1):55–66
Valero MA, Perez-Crespo I, Chillon-Marinas C, Khoubbane M, Quesada C, Reguera-Gomez M, Mas-Coma S, Fresno M, Girones N (2017) Fasciola hepatica reinfection potentiates a mixed Th1/Th2/Th17/Treg response and correlates with the clinical phenotypes of anemia. PLoS One 12(3):e0173456. (23 pp)
Valero MA, Girones N, Reguera-Gomez M, Perez-Crespo I, Lopez-Garcia MP, Quesada C, Bargues MD, Fresno M, Mas-Coma S (2020) Impact of fascioliasis reinfection on Fasciola hepatica egg shedding: relationship with the immune-regulatory response. Acta Trop 209:105518
Villegas F, Angles R, Barrientos R, Barrios G, Valero MA, Hamed K, Grueningr H, Ault SK, Montresor A, Engels D, Mas-Coma S, Gabrielli AF (2012) Administration of triclabendazole is safe and effective in controlling fascioliasis in an endemic community of the Bolivian Altiplano. PLoS Negl Trop Dis 6(8):e1720. (7 pp.)
Winkelhagen AJS, Mank T, de Vries PJ, Soetekouw R (2012) Apparent triclabendazole-resistant human Fasciola hepatica infection, the Netherlands. Emerg Infect Dis 18:1028–1029
World Health Organization (2007) Report of the WHO Informal Meeting on use of triclabendazole in fascioliasis control. World Health Organization, Headquarters Geneva, 17–18 October 2006: WHO/CDS/NTD/PCT/2007.1
World Health Organization (2008) Fact sheet on fascioliasis. In: Action against Worms, World Health Organization, Headquarters Geneva (December 2007), Newsletter, 10: 1–8
World Health Organization (2013) Sustaining the drive to overcome the global impact of neglected tropical diseases. World Health Organization, WHO Headquarters, Geneva, p 138
Zumaquero-Ríos JL, Sarracent-Pérez J, Rojas-García R, Rojas-Rivero L, Martínez-Tovilla Y, Valero MA, Mas-Coma S (2013) Fascioliasis and intestinal parasitoses affecting schoolchildren in Atlixco, Puebla State, Mexico: epidemiology and treatment with nitazoxanide. PLoS Negl Trop Dis 7(11):e2553
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Mas-Coma, S., Bargues, M.D., Valero, M.A. (2022). Fascioliasis. In: Bruschi, F. (eds) Helminth Infections and their Impact on Global Public Health. Springer, Cham. https://doi.org/10.1007/978-3-031-00303-5_6
Download citation
DOI: https://doi.org/10.1007/978-3-031-00303-5_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-00302-8
Online ISBN: 978-3-031-00303-5
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)