
Abstract
In this study, the authors completed a systematic review and meta-analysis that evaluated the risk of motor vehicle collisions (MVCs) or driving impairment due to dementia and using this information updated the international guidelines on driving with dementia.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Dementia
- Systematic review
- Meta-analysis
- Motor vehicle collisions (MVCs)
- Driving impairment
- International guidelines
Justin N Chee, Mark J Rapoport, Frank Molnar, Nathan Herrmann, Desmond O’Neill, Richard Marottoli, Sara Mitchell, Mark Tant, Jamie Dow, Debbie Ayotte, Krista L Lanctôt, Regina McFadden, John-Paul Taylor, Paul C Donaghy, Kirsty Olsen, Sherrilene Classen, Yoassry Elzohairy, David B Carr.
FormalPara Journal PublishedAmerican Journal of Geriatric Psychiatry.
FormalPara Year of Publication2017.
FormalPara Type of StudySystematic review and meta-analysis.
FormalPara Funding SourcesCanadian Institutes of Health Research (KRS grant 339665).
FormalPara ObjectivesTo conduct a systematic review and meta-analysis on the risk of motor vehicle collision (MVC) or driving impairment among individuals with dementia as measured by on-road testing in order to update the international guidelines on driving with dementia [1].
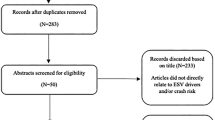
FormalPara MethodsThe investigators included primary papers that were published between 2005 and 2015. In addition, they searched the bibliographies of systematic reviews for additional studies. The investigators excluded reviews, editorials, conference proceedings, dissertations, reports that were not available in English, studies conducted among individuals with mild cognitive impairment (MCI) or among older adults without dementia, and studies that used driving simulators. The also excluded studies that used the same group of participants to report on MVC risk or driving impairment. Authors with relevant publications were not allowed to screen or extract data from their own publications.
The investigators searched Ovid MEDLINE In-Process and Other Non-Indexed Citations (October 13, 2015), Ovid MEDLINE without Revisions (1990–October Week 1, 2015), and Ovid MEDLINE (1990–1995) and subsequently adapted for CINAHL (1990–2015), Scopus (1990–2015), Cochrane Central Register of Controlled Trials (CENTRAL) (1990–2015), EMBASE (1990–2015), PsycINFO (1990–2015), and the Transportation Research Information Database (1990–2015) with the last search being run on October 30, 2015.
The investigators included studies that involved individuals with dementia that was diagnosed using any well-established criteria or as a result of a referral from a healthcare practitioner. In addition, there was no restriction based on the age of the participants or with regard to the severity of dementia. The primary outcome measures for the review were road MVCs (self- or informant-reported data and state/government accident registries and skill performance and road-test failure rates that were determined using on-road driving assessments on formal testing or in naturalistic environments). Eligible studies were independently identified by pairs of reviewers. Any disagreements between reviewers were resolved by consensus or by utilizing a third-party arbiter among the coauthors.
The quality of evidence in each of the included studies was assessed using an article grading guideline (Class I, II, III, or IV) that was developed following an in-person meeting of ten of the coauthors. The specific rating that was assigned to each of the included studies was arrived at by consensus.
The investigators conducted a meta-analysis that compared individuals with and without dementia and computed the risk ratio (RR) and 95% confidence interval (CI) associated with failing an on-road assessment. The meta-analysis was conducted using a DerSimonian and Laird random-effects model. The χ2 test and I2 statistic were used to determine the heterogeneity and its magnitude in the included studies.
The investigators included a total of nine studies in the final analysis. Eight of the studies were qualitatively described with four of the that presented a failure rate for on-road assessments being quantitatively pooled in a meta-analysis.
The two studies that examined MVC risk among individuals with dementia did not find any difference between the healthy comparison group and individuals with dementia on the percentage of individuals with MVCs or the number of MVCs per year per 10,000 miles driven in the past year (Class I). Another study found that there were no differences between the dementia group and the healthy comparison group in the percentage of individuals with MVCs, MVC rate per driver per year, or total number of MVCs in the 3 years before a baseline assessment (Class I). However, the total number of MVCs per 1000 miles driven per week was 4.72 times higher among individuals in the dementia group (8.78 MVCs) when compared to the healthy comparison group (1.86 MVCs; P < 0.01). The investigators also found that 3 years after the baseline assessment, the percentage of MVCs in the healthy comparison group was 11.0 times higher than that of the dementia group (11% versus 1%; P < 0.05). However, this difference was nullified after the distance driven per week was corrected.
Measures of on-road performance were reported in all nine of the included studies. Seven of the nine studies presented driving impairment outcomes, four studies reported on on-road assessment failure rates, and two studies reported on both the outcomes. Among seven of the studies that examined driving impairment, one study was rated as Class I for quality, whereas the other six trials were rated as Class IIb for quality. A total of six of the seven studies showed a reduced performance on at least one measure of driving behavior among individuals with dementia when compared to healthy comparators. The effect sizes in these studies ranged between 0.26 and 3.61. The effect sizes were noted to be large for 19 of the outcomes (landmark/sign identification, number of lost trips, etc.) and medium for 10 of the outcomes (total safety errors, lane observance errors, etc.)
The meta-analysis included four studies that included data for on-road failure rate. Two of the studies were rated as Class I for quality, and two studies were rated as Class IIb for quality. The results indicated that individuals with dementia were much more likely to fail a road assessment than healthy comparison group (RR: 10.77, 95% CI: 3.00–38.62, z = 3.65, P < 0.001). The investigators did not find any significant heterogeneity among the study findings (χ2 = 1.50, P = 0.68, I2 = 0%). Additionally, there was no publication bias noted as there were no asymmetries in the funnel plot. One study did not conceptualize marginal or probably safe/unsafe cases separately than passing or failing cases, which differed from the three other studies. When the sensitivity analysis was completed without including data from this study, the results were similar (RR: 6.77, 95% CI: 1.24–36.96, z = 2.21, P < 0.03). There was no significant heterogeneity noted (χ2 = 0.80, P = 0.67, I2 = 0%). The two studies that presented failure rates separately for the clinical dementia rating scale (CDR) 0.5, CDR 1, and control participants found that the absolute increase in risk for CDR 0.5 ranged from 11% to 12% which corresponded with a relative risk of 5–11%. The absolute increase in risk for CDR 1 ranged from 18% to 22% which corresponded with a relative risk of 8–20%.
Data from two studies indicated that individuals with dementia have a fourfold increase in MVCs per 1000 miles driven per week in the 3 years prior to baseline assessment. Additionally, medium to large effects were noted for the presence of dementia on driving abilities in six of the seven seven recent studies that evaluated driving impairment. Furthermore, individuals with dementia were more likely to fail a road test than healthy controls. Individuals with even mild stages of dementia are at higher risk for failing a performance-based road test and of demonstrating impaired driving abilities on the road.
FormalPara Strengths of the Study-
1.
This was a well-designed and well-conducted systematic review and meta-analysis.
-
2.
The results are easy to interpret and the discussion is robust with strengths and weaknesses of the paper being clearly discussed.
-
3.
This study identified an important gap in the literature where there is very little available data on drivers with moderate dementia.
-
1.
Only nine studies included in the final review.
-
2.
The investigators did not search gray literature, i.e., conference presentations and proceedings, dissertations and unpublished manuscripts, and technical reports, and did not include papers that were published in languages other than in English.
-
3.
Individuals with mild cognitive impairment were not included in the review [2].
-
4.
Only one of the included studies was longitudinal.
-
5.
In all the included studies, the control groups were younger than the dementia groups. In addition, there were less men in the control groups when compared to the dementia group, in all but one study.
-
6.
There may be some reporting bias in the studies as many individuals may stop driving independently or are taken off the road prior to an MVC. In addition, there may be underreporting of MVCs among individuals with dementia.
-
7.
There is a significant risk for type II error (error of omission/false negative) as the sample sizes in these studies were small.
Individuals with dementia exhibit on-road driving impairment, driving errors, and failure on on-road tests when compared to controls. These risks are most likely due to memory impairment, visuospatial perception difficulties, reduced hand-eye coordination, and delayed reaction time.
FormalPara Practical Application of the Take-Home PointsClinicians evaluating individuals with dementia should discuss driving abilities with the individual with dementia and their caregivers. The discussion should involve a review of available evidence regarding this topic, the importance of executive dysfunction, the caregiver concern about driving, and the pros and cons of continued driving as dementia is a progressive illness. Specialized on-road testing should be recommended when driving safety is uncertain in individuals with dementia.
References
Chee JN, Rapoport MJ, Molnar F, Herrmann N, O’Neill D, Marottoli R, Mitchell S, Tant M, Dow J, Ayotte D, Lanctôt KL, McFadden R, Taylor JP, Donaghy PC, Olsen K, Classen S, Elzohairy Y, Carr DB. Update on the risk of motor vehicle collision or driving impairment with dementia: a collaborative international systematic review and meta-analysis. Am J Geriatr Psychiatry. 2017;25(12):1376–90.
Rapoport MJ, Naglie G, Herrmann N, Zucchero Sarracini C, Mulsant BH, Frank C, Kiss A, Seitz D, Vrkljan B, Masellis M, Tang-Wai D, Pimlott N, Molnar F. Developing physician consensus on the reporting of patients with mild cognitive impairment and mild dementia to transportation authorities in a region with mandatory reporting legislation. Am J Geriatr Psychiatry. 2014;22(12):1530–43.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Phelps, E.B., Swantek, S. (2022). Update on the Risk of Motor Vehicle Collision or Driving Impairment with Dementia: A Collaborative International Systematic Review and Meta-analysis. In: Tampi, R.R., Tampi, D.J., Young, J.J., Balasubramaniam, M., Joshi, P. (eds) Essential Reviews in Geriatric Psychiatry. Springer, Cham. https://doi.org/10.1007/978-3-030-94960-0_63
Download citation
DOI: https://doi.org/10.1007/978-3-030-94960-0_63
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-94959-4
Online ISBN: 978-3-030-94960-0
eBook Packages: MedicineMedicine (R0)