
Abstract
Posterior hip disorders can be challenging for clinicians to differentiate and diagnose accurately due to the location of several closely related pain generators and shared pain patterns. Such injuries can cause significant functional impairment if not treated expeditiously. The majority of posterior hip disorders can be managed successfully through conservative measures consisting of rehabilitation and, when indicated, nonoperative procedures. This chapter aims to provide clinicians with an approach to accurately diagnose and efficiently treat the most common posterior hip disorders. This chapter describes the key clinical features in the history and physical examination, appropriate diagnostic workup, and treatment options including both nonoperative and surgical interventions for each pathology.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Proximal hamstring pain
- Ischial bursitis
- Ischiofemoral impingement
- Extra-articular hip impingement
- Piriformis myofascial pain
- Soft tissue
- Musculoskeletal ultrasound
- Physical therapy
- Injections
- Rehabilitation
1 Proximal Hamstring Tendinopathy/ Tear
1.1 Synonyms
-
Hamstring tendonitis
-
Hamstring tendinosis
-
High hamstring tendinopathy
1.2 ICD-10 Codes
M76.899, S76.311, S76.309
1.3 Description
Anatomy
The hamstring myotendinous unit is frequently injured due to a bi-articular anatomic course across the hip and knee joints and the composition of mostly type II fast-twitch fibers. The proximal hamstring consists of two tendons, the semimembranosus and conjoint tendon (formed by the long head of the biceps femoris and semitendinosus). The proximal hamstring muscles originate on the lateral ischial tuberosity (IT) with the semimembranosus tendon origin lateral and anterior to the conjoint tendon. The sciatic nerve traverses in close proximity, 1–1.4 cm lateral to this origin [5]. In proximal hamstring tendinopathy, the semimembranosus tendon is most affected [4]. The paucity of blood flow at the enthesis is responsible for morbidity and delayed healing in many cases [6].
Proximal hamstring tendinopathy (PHT) is a chronic overuse injury due to repetitive microtrauma from mechanical overload and repetitive stretch on the hamstring origin at the ischial tuberosity (IT), with resultant tendon thickening, disorganization, and degeneration. It is commonly associated with enthesopathy or degenerative tears. While the onset of proximal hamstring tendinopathy is typically gradual and occurs without a traumatic event, it can be stressed acutely during eccentric contraction with the hip flexed and knee extended or an extreme stretch of the hamstring muscle–tendon unit [1]. There is maximum tension of the hamstring tendon origin at the ischial tuberosity during the terminal swing and early stance phases of the running cycle [2].
Potential risk factors for proximal hamstring tendinopathy include impact exercise overuse, muscular imbalance (particularly weakness at the hamstring and core), and lumbopelvic instability [3, 4]. Proximal hamstring tendinopathy most commonly affects runners, including sprinters, mid-distance, and long-distance runners, and athletes who participate in running sports with frequent directional changes.
Proximal hamstring tendon rupture/avulsion should be distinguished from proximal hamstring tendinopathy as acute tears that occur after forceful eccentric contraction of the hamstrings with sudden hip flexion and concurrent knee extension. Such injuries occur most frequently in high-ballistic sports such as weightlifting, water skiing, and gymnastics. Athletes may recall a pop or sensation of tearing with immediate onset of pain [3].
1.4 Clinical Presentation
Contrary to hamstring strain, proximal hamstring tendinopathy classically presents with a more insidious onset. Patients typically report gradually progressive pain at the deep buttock near the ischial tuberosity with occasional radiation of pain to the posterior thigh. Symptoms may heighten with static stretching in end range of hip flexion. Sciatic neuralgia can be present in some cases. Sitting intolerance is often present and can be quite limiting. Provocative factors include running, particularly uphill as the proximal hamstring is subjected to higher energy storage, repetitive eccentric hamstring contraction, acceleration, forward trunk flexion, deep hip flexion, and direct pressure to the ischial tuberosity [4].
1.5 Physical Examination
Full musculoskeletal (MSK) examination of the lumbar spine and hip is needed to differentiate proximal hamstring tendinopathy from other causes of posterior hip pain (Table 39.1). Lower extremity neurologic assessment is indicated to rule out a neurologic component. Depending on findings, the examination may need to expand to assess for other potential sources of pain.
Gait
Gait is typically unaffected in proximal hamstring tendinopathy. Assessment is useful to rule out other potential diagnoses. In the case of acute avulsion, patients usually have difficulty bearing weight.
Visual observation
It is important to inspect the affected area and the bulk and tone of the hamstring muscles. In acute rupture, ecchymosis may be seen at the posterior thigh.
Palpation
Direct palpation of the ischial tuberosity, gluteal muscles (including the piriformis), and hamstring muscle belly should be performed assessing for pain provocation. There may be focal tenderness at the ischial tuberosity. Taut bands and trigger points are commonly identified in the piriformis and hamstring muscles. In avulsion injuries, a palpable deformity may be appreciated on passive knee flexion in the prone position.
Range of motion (ROM)
Hip and lumbar spine ROM should be examined in all planes. ROM is preserved in proximal hamstring tendinopathy. Normal measurements for hip and lumbar spine ROM are discussed in the anterior hip chapter and spine disorders section.
Sensory testing
Light touch should be tested in bilateral lower extremities throughout the L1-S1 dermatomes. Sensory deficit warrants further investigation, as this is not expected in proximal hamstring tendinopathy.
Deep tendon reflexes
The following lower extremity reflexes should be tested bilaterally to assess for radiculopathy: patellar tendon (L2-L4, L4 primary), Achilles tendon (S1), and hamstring tendon (L5). Reflexes should be normal and symmetric in proximal hamstring tendinopathy.
Motor testing
It is important to test L2-S2 myotomes, specifically hip flexion (L2/L3), knee extension (L2/L3/L4), ankle dorsiflexion (L4/L5), great toe extension (L5), ankle planar flexion (S1/S2), knee flexion (S1/S2), and gluteus medius strength (L4/L5/S1), to exclude other pathology. In the prone position, resisted knee flexion should be tested at 30 degrees and 90 degrees while looking for pain provocation. Resisted hip extension can elicit pain. In the case of an avulsion injury, weakness can be seen with resisted hip extension and knee flexion.
Joint testing
Careful assessment of the hip joint with special provocative tests is important to differentiate proximal hamstring tendinopathy from intra-articular hip sources of posterior hip pain. It is also important to assess the lumbar facet and sacroiliac joints. Specifics of such testing are highlighted in the spine disorders section and anterior hip disorders chapter.
1.5.1 Special Maneuvers
Several provocative maneuvers have been shown to have high validity and reliability for proximal hamstring tendinopathy [2, 4]. These are not indicated for acute proximal hamstring ruptures.
-
Puranen-Orava test : The patient’s foot rests on an elevated support about 90 degrees to their body with the hip flexed and knee extended while they reach with their ipsilateral arm toward the foot to stretch the hamstring. Provocation of pain is associated with proximal hamstring tendinopathy.
-
Bent-knee test/modified bent-knee stretch test : With the patient supine, the examiner puts the affected side into maximum hip and knee flexion and then slowly passively extends the knee. The modified bent-knee stretch test is similar, but with rapid passive knee extension instead (Fig. 39.1). In both tests, knee extension commonly elicits pain at the proximal hamstring.
-
Single-leg deadlift : With knee slightly flexed, the patient stands on the affected leg while gradually bending forward at the hip, lifting the contralateral hip into extension to load the affected hamstring. This provokes pain.
-
Supine plank : During this loading maneuver, the patient is supine with heels and elbows resting on the table. The patient rises up on their elbows while keeping their knees in extension and raising the unaffected leg while keeping the injured side on the table to elevate the pelvis (Fig. 39.2). A positive test reproduces the patient’s index pain. Examiners may need to modify this test depending on the patient’s ability to perform the maneuver. For instance, the examiner can hold the heel of the unaffected side off the table while the patient extends the hip on the affected side and elevates the pelvis. A single-leg bridge can also substitute; however, it is important to keep in mind that this places reduced load on the hamstring.
-
Nordic hamstring exercise : The patient kneels on a flat surface with their knees flexed at 90 degrees while the examiner holds their heels. While maintaining a straight spine, the patient gradually leans forward in a controlled fashion until they have to put their hands out to catch themselves (Fig. 39.3). The patient then performs a hamstring curl to return to the starting position. In cases of proximal hamstring tendinopathy, the eccentric load on the hamstring provokes pain.

Modified bent-knee stretch test performed stepwise fashion progressing from a through d

Supine plank with single leg raise

Nordic hamstring exercise
1.6 Diagnostic Workup
For most cases, proximal hamstring tendinopathy is a clinical diagnosis. When the diagnosis is unclear, magnetic resonance imaging (MRI) and musculoskeletal ultrasound are the preferred imaging studies as they not only identify tendinosis but also characterize the severity of the injury.
X-ray
Plain radiographs of the hips and pelvis are typically inconclusive. In chronic cases, they can identify enthesopathy or intra-tendinous calcifications at the ischial tuberosity.
MRI
MRI has a higher sensitivity than musculoskeletal ultrasound. MRI findings of proximal hamstring tendinopathy may include bone edema at the ischial tuberosity, tendon thickening, intra-substance heterogeneity of the tendon, and tendinous/peritendinous edema with a distal feathery appearance (Fig. 39.4). Partial- and full-thickness tears can be identified and characterized. The degree of retraction can be important for surgical decision-making in the case of acute rupture.

MRI hip demonstrating proximal hamstring tendinopathy with increased signal intensity at the semimembranosus tendon (red arrow) near the ischial tuberosity (green star) on axial proton density fat suppression sequence
Musculoskeletal ultrasound
Ultrasound evaluation for proximal hamstring tendinopathy commonly demonstrates tendon thickening and degenerative changes along with peritendinous fluid at the site of the proximal hamstring. There may be cortical irregularity at the ischial tuberosity attachment site.
1.7 Treatment
Proximal hamstring tendinopathy can be challenging to manage. In most cases, nonoperative management can successfully return patients to activity within 3–6 months.
1.7.1 Medical Management
Pain control can be achieved with topical or oral anti-inflammatories such as nonsteroidal anti-inflammatory drugs (NSAIDs). If the patient is unable to tolerate NSAIDs, they may take acetaminophen for analgesia. In the acute phase of proximal hamstring tendinopathy, ice may be beneficial.
1.7.2 Rehabilitation
Postural modifications include seat cushions to offload compression at the tendon attachment site. Standing workstations are often helpful. Patients should avoid impact exercise and focus on non-impact activities as tolerated, such as cycling in the standing position, elliptical, and swimming. Soft tissue mobilization to the proximal hamstring may also be beneficial. Early engagement in physical therapy should focus on core and lumbosacral stabilization with activation of the gluteal musculature. As in other lower extremity enthesopathies, stretching of the hamstrings is not recommended for proximal hamstring tendinopathy; however, patients should focus on stretching the piriformis and hip flexors to optimize pelvic position and encourage posterior pelvic tilt. Guided by the patient’s pain, a progressive hamstring strengthening protocol should be implemented with gradual progression from isometric to isotonic exercises. Once the tendon is less reactive, eccentric exercises should be incorporated and advanced as tolerated.
1.7.3 Procedures
For refractory cases, more invasive procedures can be tried.
Trigger point injections
If myofascial pain limits rehabilitation progress, trigger point injections can target the proximal hamstring or gluteal musculature.
Ultrasound-guided percutaneous needle tenotomy with or without platelet-rich plasma (PRP)
In an attempt to incite a proinflammatory response and promote tendon healing, an ultrasound-guided percutaneous needle tenotomy can be performed with or without PRP [7].
Extracorporeal shockwave therapy (ESWT)
An alternative and effective treatment is ESWT. While treatment protocols vary, the following has been successfully utilized in a population of professional athletes—weekly radial shockwave sessions with 2500–3000 impulses per session at pressure of 4 bars and frequency of 10 shocks/second (0.18 mJ/mm2 energy flux density) for 3–4 weeks [1]. Combined therapy consisting of radial and focused shockwave can also be considered.
Ultrasound-guided corticosteroid injection
If patients are unable to fully participate in a progressive loading program, a one-time ultrasound-guided corticosteroid injection to the proximal hamstring complex tendon sheath can be performed, provided there is no evidence of a partial tear. More than one peritendinous corticosteroid injection is not recommended given potential for tenotoxicity [8].
1.7.4 Surgery
Operative management is reserved for recalcitrant cases or in patients where proximal hamstring tendinopathy progresses to high-grade partial- or full-thickness tear. In contrast, for acute proximal hamstring tendon injuries, surgical referral is indicated for complete avulsion or two-tendon injuries with >2 cm tendon retraction [2]. Early surgical repair leads to more favorable outcomes. Surgical interventions may consist of open tendon debridement and primary tendon repair. See Chap. 42 for more details on hip surgeries.
2 Ischial Bursitis
2.1 Synonyms
-
Ischial bursopathy
-
Ischiogluteal bursitis
2.2 ICD-10 Codes
M70.70
2.3 Description
Anatomy
The ischial bursa is an adventitial bursa that lies between the proximal hamstring tendon origin at the ischial tuberosity and the overlying gluteus maximus muscle, in close proximity to the sciatic nerve, posterior femoral cutaneous nerve, and pelvic vasculature. As an adventitial bursa, it is not formed during normal embryologic development but develops in response to friction and pressure between the ischial tuberosity and overlying soft tissue. Chronic irritation results in an inflammatory response with increased vascular permeability and vasodilation at the bursa [10].
The bursa is rather dynamic in that load exposure changes depending on the patient’s position. In the standing position, the gluteus maximus muscle covers the bursa. In the seated position, the gluteus maximus moves superiorly leaving only the subcutaneous tissue to protect the ischial bursa and heightening the risk for irritation.
Ischial bursitis is an infrequent cause of posterior hip pain. It is most commonly a noninfectious inflammatory process due to chronic, direct bursal irritation in the setting of prolonged sitting. It can also be reactive to chronic loading of the proximal hamstring and systemic inflammatory diseases such as rheumatoid arthritis and crystal arthropathy. Acute ischial bursitis is rare and classically occurs in the setting of trauma. Ischial bursitis most commonly affects individuals with sedentary lifestyles. Interestingly, it was previously referred to as “weaver’s” or “tailor’s bottom,” as such professions put a great amount of pressure on the ischial bursa resulting in irritation and inflammation [9]. Ischial bursitis may also affect cyclists due to repetitive irritation on the saddle. Due to reduced subcutaneous tissue in patients with cachexia or severe weight loss, the ischial bursa may be under increased pressure, raising the risk for ischial bursitis [10].
2.4 Clinical Presentation
Patients with ischial bursitis classically present with insidious onset of dull, aching pain localized to the inferior gluteal region with or without radiation down the posterior leg. Provocative maneuvers include prolonged sitting and increased hip flexion commonly seen in cycling, rowing, horseback riding, sprinting, and running uphill [9]. Sleep may be interrupted due to pain.
2.5 Physical Examination
In many ways, physical examination of a patient with suspected ischial bursitis is similar to proximal hamstring tendinopathy.
Gait
In the case of ischial bursitis, gait is rarely altered.
Visual observation
Overlying erythema is a rare finding in ischial bursitis. This finding warrants further investigation for an infectious process.
Palpation
Direct palpation of the ischial tuberosity will generally reproduce index pain in ischial bursitis. If swelling or a mass is detected, further studies should be initiated to rule out malignancy, abscess, and hematoma [9]. Clinicians should also include palpation at the following landmarks: origin, muscle belly, and insertion points of the gluteal, piriformis, and hamstring muscles.
Range of motion
Hip and lumbar spine ROM should be examined in all planes.
Sensory testing
A complete lower extremity sensory exam should be performed as part of the neurologic assessment. Sensory deficits are not detected in isolated ischial bursitis.
Deep tendon reflexes
The following lower extremity reflexes should be performed—patellar tendon (L2-L4, L4 primary), Achilles tendon (S1), and hamstring tendon (L5). Reflexes are preserved in ischial bursitis.
Motor testing
Strength assessment of the L2-S1 myotomes should be performed.
Joint testing
Careful examination of the hip joint, sacroiliac joint, and lumbar facets is important to differentiate ischial bursitis from other causes of posterior hip pain.
Special Maneuvers
There are no specific physical examination maneuvers for ischial bursitis. It is important to perform the special maneuvers for proximal hamstring tear (discussed above) to differentiate ischial bursitis from proximal hamstring tendinopathy. These maneuvers are less likely to produce pain in isolated ischial bursitis.
2.6 Diagnostic Workup
X-ray
Plain radiographs of the pelvis are generally normal in ischial bursitis. Occasionally, there may be nonspecific findings of cortical irregularity or calcifications at the ischial tuberosity.
MRI
MRI of the hip or pelvis is the gold standard imaging study for cases of ischial bursitis associated with a palpable mass in order to rule out malignancy, abscess, cyst, or hematoma. Ischial bursitis presents similarly to other forms of bursitis on MRI with high signal intensity and bursal distention on fluid-sensitive sequences. Unique to ischial bursitis is the cystic appearance of the bursa, with frequent internal hemorrhage due to shearing, irritative forces placed on the ischial tuberosity (Fig. 39.5) [9]. Ischial bursitis can be differentiated from neoplasm based on bursal contents. The bursa in ischial bursitis contains only fluid with soft tissue components confined to the bursal wall. On the contrary, neoplasms are predominantly composed of solid tissue [11].

MRI hip demonstrating ischial bursitis with high signal intensity and distention of the ischial bursa (outlined in red) in relation to the ischium (green star) on coronal (a) and axial (b) STIR sequences
Musculoskeletal ultrasound
Point-of-care ultrasound can be useful for real-time evaluation of the compressible and cystic nature of the ischial bursitis [11].
Diagnostic ultrasound-guided local anesthetic injection
In cases where the diagnosis is unclear, a diagnostic ultrasound-guided intra-bursal anesthetic injection can be helpful [12].
2.7 Treatment
2.7.1 Medical Management
Ischial bursitis is typically managed conservatively with a course of either topical or oral anti-inflammatories and cold compresses.
2.7.2 Rehabilitation
The rehabilitation course for ischial bursitis is very similar to proximal hamstring tendinopathy. Activity modifications include avoidance of impact exercise and provocative positions such as prolonged sitting. Patients are encouraged to resume non-impact exercises as tolerated for cardiovascular fitness. Soft tissue mobilization to the proximal hamstrings and gluteal muscles may alleviate reactive myofascial pain. Stretching of the piriformis, gluteal muscles, and hamstrings is recommended as well as core and lumbosacral stabilization with implementation of a progressive gluteal and hamstring strengthening protocol.
2.7.3 Procedures
Ultrasound-guided corticosteroid injection
For refractory cases, ultrasound-guided procedures may be helpful for therapeutic purposes. Ultrasound-guided corticosteroid injection to the ischial bursa can be performed with the patient lying in the lateral decubitus position with their hips flexed to 90 degrees to increase the distance between the ischial bursa and sciatic nerve [12].
2.7.4 Surgery
Surgery is generally not indicated for this diagnosis. In cases of refractory symptoms affecting quality of life, ischial bursectomy has been described.
3 Ischiofemoral Impingement
3.1 Synonyms
-
Quadratus femoris (QF) impingement
-
Extra-articular hip impingement
3.2 ICD-10 Codes
M25.859, M24.859
3.3 Description
Anatomy
It is important to note the boundaries of the ischiofemoral space (IFS) and quadratus femoris space (QFS). As mentioned, the ischiofemoral space is the distance between the ischium and lesser trochanter. The quadratus femoris space is the area between the superolateral aspect of the hamstring tendons and the posteromedial aspect of the iliopsoas tendon; the functional space for the quadratus femoris muscle originates from the anterior ischial tuberosity and inserts on the posteromedial proximal femur. The primary function of the quadratus femoris is hip adduction and external rotation. The sciatic nerve lies just superficial to the quadratus femoris within the ischiofemoral space.
Ischiofemoral impingement (IFI) is an extra-articular impingement of the soft tissues, namely, the quadratus femoris (QF) muscle, between the lesser trochanter of the femur and the ischial tuberosity. There are several factors, including congenital, positional, and acquired, which contribute to narrowing of the ischiofemoral space (IFS). Congenital factors consist of hip dysplasia and alignment abnormalities, specifically coxa valga. The ischiofemoral space is narrowed with hip extension, external rotation, and adduction [13]. Hip abductor weakness contributes to dynamic adduction and ischiofemoral space narrowing. Acquired anatomic changes, specifically hypertrophy of the superomedial aspect of the femur seen in hip osteoarthritis, total hip arthroplasty, lesser trochanter fractures/avulsions, proximal hamstring tendinopathy and enthesopathy, and regional osteochondromas, may also contribute to ischiofemoral space narrowing and impingement [14].
3.4 Clinical Presentation
Patients often present with insidious onset of deep gluteal and/or groin pain with occasional radiation down the posterior leg due to the close proximity of the quadratus femoris muscle to the sciatic nerve. Pain may be exacerbated with weight-bearing activity and hip adduction, extension, and external rotation [13]. Mechanical impingement symptoms may occur during exaggerated hip extension as seen in running or long-stride walking [14]. Ischiofemoral impingement may affect individuals of any age but most commonly affects adult females [14]. This predilection may be attributed to the frequency of hip abduction weakness in women. Approximately 25–40% of cases have bilateral involvement [14].
3.5 Physical Examination
Gait
Patients may report pain and/or a snapping/locking sensation of the posterior hip region during the long-stride walking test, which has a sensitivity of 92% and specificity of 82% [14]. Patients may also demonstrate compensatory hip abduction to increase the ischiofemoral space.
Visual observation
Inspection of the affected area should be normal.
Palpation
Clinicians should palpate the ischial tuberosity, quadratus femoris, gluteal muscles, piriformis muscle, and hamstring muscle belly for tenderness. Typically, the palpatory exam is normal in ischiofemoral impingement. In cases of concurrent proximal hamstring tendinopathy, there may be tenderness of the ischial tuberosity.
Range of motion
It is important to assess ROM for the lumbar spine and hip joint. Patients with ischiofemoral impingement classically report pain in hip extension, adduction, and external rotation.
Sensory testing
Due to similar pain patterns between ischiofemoral impingement and lumbar radiculopathy, it is important to perform a sensory examination including L1-S1 dermatomes. Sensory deficits should not be present in ischiofemoral impingement. Rare sciatic neuropathy has been described.
Deep tendon reflexes
Reflexes should be normal and symmetric in ischiofemoral impingement.
Motor testing
Lower extremity motor strength testing should be carried out for L2-S1 myotomes to rule out a neurologic component. Strength should be preserved in ischiofemoral impingement with the rare exception of associated sciatic neuropathy, where hamstring and/or calf weakness may be seen.
Joint testing
Assessment of the hip joint, lumbar facets, and sacroiliac joint should be performed to rule out other causes of posterior hip pain.
Special maneuvers
Pain may be elicited with a combination of passive hip extension, adduction, and external rotation and generally alleviated with hip abduction as this widens the ischiofemoral space. This maneuver is occasionally referred to as the “ischiofemoral impingement test” and is performed in a lateral decubitus position. However, it is common to not find pain provocation on examination.
3.6 Diagnostic Workup
X-ray
Plain radiographs of the pelvis and hip can assess intra-articular hip pathology. Plain radiographs are used to identify bony morphologic changes that may contribute to ischiofemoral impingement (discussed above).
MRI
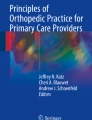
MRI of the hip/pelvis may demonstrate characteristic findings including ischiofemoral space and quadratus femoris narrowing with adjacent quadratus femoris muscle edema, suggestive of acute or chronic inflammation due to impingement (Fig. 39.6). Proximal hamstring tendinopathy with tendon thickening contributing to ischiofemoral space narrowing may also be seen [15]. An ischiofemoral space of <15 mm is the radiographic criteria utilized for ischiofemoral impingement [14, 16, 17]. It may not correlate with symptomatology.

Plain AP pelvic radiograph demonstrating ischiofemoral space (black line) between the lesser trochanter (red arrow) and ischial tuberosity (green arrow) (a). Axial T2-weighted MRI hip with narrowed ischiofemoral space (black line) with quadratus femoris muscle edema (blue star), which can be seen in ischiofemoral impingement (b). MRI is used to diagnose ischiofemoral impingement while radiograph is not
Musculoskeletal ultrasound
Dynamic ultrasound evaluation can be useful to demonstrate soft tissue impingement between the ischial tuberosity and lesser trochanter during hip external rotation. While MRI is the gold standard, ultrasound can be considered to measure the ischiofemoral space in the hands of an advanced ultrasonographer. It is helpful to perform side-by-side evaluations to determine if such impingement is a normal variant or the primary pain generator.
3.7 Treatment
3.7.1 Medical Management
NSAIDs or acetaminophen can be utilized for pain management. Aggravating factors such as long-stride walking should be avoided.
3.7.2 Rehabilitation
Patients should avoid movements that narrow the ischiofemoral space, including hip extension, adduction, and external rotation. While it is recommended to restrict weight-bearing exercise, patients may continue with non-impact exercise. Manual therapy to the gluteal muscles, including the piriformis and quadratus femoris, can mitigate reactive myofascial pain. A progressive core and lumbopelvic stabilization program with an emphasis on strengthening the hip abductors and external rotators and optimizing hip biomechanics should be started once pain is controlled.
3.7.3 Procedures
Ultrasound-guided injection
For refractory cases, more invasive ultrasound-guided procedures can be trialed for diagnostic and therapeutic purposes. For cases where the diagnosis is unclear or patients are unable to fully participate in a course of physical therapy due to pain, an ultrasound-guided trigger point injection targeting the quadratus femoris with local anesthesia alone or in combination with corticosteroid can be performed, with careful attention to avoid the sciatic nerve.
3.7.4 Surgery
Ischiofemoral impingement is treated almost entirely with conservative measures. Surgical referral is recommended only when pain is severe and persistent despite rehabilitation and injection therapy and limits quality of life. The goal of surgical intervention for ischiofemoral impingement is to increase the ischiofemoral space through resection of the lesser trochanter [18, 19]. See Chap. 42 for more details on hip surgeries.
4 Piriformis Myofascial Pain
4.1 Synonyms
-
Piriformis syndrome
-
Deep gluteal syndrome
-
Extra-spinal sciatica
4.2 ICD-10 Codes
G57.00
4.3 Description
Anatomy
The piriformis muscle is pyramidal shaped and originates from the anterior aspect of the sacrum (S2-S4), courses through the greater sciatic notch, and inserts on the greater trochanter. The function of the piriformis muscle varies with hip position. In hip extension, it functions as a hip external rotator; in hip flexion, it predominantly serves as a hip abductor. The anatomic relationship between the sciatic nerve and piriformis muscle is variable. Traditionally, the sciatic nerve travels inferior to the piriformis muscle. Anatomic variants of the nerve course with relation to the piriformis muscle can further predispose it to entrapment [22].
Piriformis myofascial pain (PMP) is a common cause of posterior hip pain. It can be a source of extra-spinal sciatic neuralgia, referred to as “non-discogenic sciatica,” due to compression of the sciatic nerve under the spastic piriformis muscle [20]. Piriformis myofascial pain typically results from repetitive hip flexion, internal rotation, and adduction, which is theorized to cause cumulative microtrauma to the piriformis muscle leading to myofascial pain. Such biomechanics are seen in cyclists, dancers, gymnasts, and skiers [21]. Though the pathophysiology is largely unknown, it is theorized that gluteal weakness/fatigue leads to compensatory piriformis overuse [20]. Piriformis myofascial pain may also present in the setting of acute traumatic fall or penetrating injury. Individuals with leg length discrepancy, pelvic obliquity, or scoliosis may demonstrate compensatory gait mechanics that heighten the risk for piriformis myofascial pain [21]. Additionally, piriformis myofascial pain may be more common in women due to biomechanics associated with a larger quadriceps angle (Q angle) [22]. Piriformis myofascial pain is frequently seen in association with spine (scoliosis) and hip joint pathology and proximal hamstring tendinopathy. The exact prevalence is unknown, due in part to variable diagnostic criteria.
4.4 Clinical Presentation
Piriformis myofascial pain typically presents with gradual onset of deep gluteal pain and may be associated with radiating pain down the posterior limb and paresthesias in the distribution of the sciatic nerve. Patients may describe pain provocation with sitting or maneuvers that strain the piriformis muscle such as hip flexion, internal rotation, and adduction.
4.5 Physical Examination
Gait
Generally, gait is unaffected in piriformis myofascial pain; however, in cases attributed to a leg length discrepancy, there can be increased internal rotation or adduction [21].
Visual observation
The affected area will appear normal in most cases of piriformis pain. Static and dynamic knee valgus should be noted as a greater degree of valgus angulation may be associated with piriformis pain.
Palpation
Patient can be examined in side-lying or prone position. In most cases, pain is reproduced with deep palpation of the piriformis muscle, with one hand over the greater trochanter and the other hand on the sacral sulcus with the thumbs overlying over the piriformis muscle fibers (in particular with simultaneous dynamic hip internal external rotation in prone examination). Taut bands and/or trigger points may be palpated along the gluteal and piriformis muscles (Fig. 39.7). While palpating this muscle, one should examine the distal sacroiliac joint, which is the closest axial structure to the piriformis muscle. It is important to palpate the contralateral piriformis muscle as it may be normally tender and not necessarily pathologic.

Side-lying palpatory examination of the piriformis muscle. The examiner’s left hand is on the greater trochanter, while the medial portion of the examiner’s right hand is on the sacral sulcus. The examiner’s thumbs overlie the fibers of the piriformis muscle
Range of motion
ROM is generally preserved in piriformis myofascial pain.
Sensory testing
Lower extremity sensory examination of L4-S1 dermatomes should be performed to exclude more common lumbar spine pathologies as sensation is preserved in piriformis myofascial pain.
Deep tendon reflexes
Reflexes are normal and symmetric in piriformis myofascial pain.
Motor testing
Motor strength testing of bilateral lower extremities is carried out to exclude other causes of posterior hip pain.
Joint testing
Assessment of the hip, sacroiliac joint, and lumbar facets is warranted.
4.5.1 Special Maneuvers
There are several special maneuvers that passively stretch the piriformis muscle and may reproduce symptoms:
-
Pace test or passive seated piriformis test : During this test, the patient is seated with hips flexed to 90 degrees followed by resisted hip abduction. Pain may be elicited. This test has a sensitivity of 0.53 and specificity of 0.90 [22].
-
Freiberg maneuver : This maneuver can reproduce symptoms as the hip is extended and then passively internally rotated to stretch the piriformis (sensitivity and specificity unknown).
-
Beatty test : With the patient side-lying on the unaffected side, the affected hip is flexed to 90 degrees with resisted hip abduction (sensitivity and specificity unknown).
-
FAIR test : The details of this maneuver are highlighted in the anterior hip chapter. In many instances of piriformis myofascial pain, pain in the gluteal region may be elicited with the FAIR test with a sensitivity of 0.88 and specificity of 0.83 [22].
-
Straight leg raise (Lasegue sign), seated slump : Such tests place neural tension along the sciatic nerve and commonly reproduce symptoms in patients with PMP. At 90 degrees of hip flexion with the knee extended, the patient may report buttock and posterior thigh pain [22]. The straight leg raise has a sensitivity of 0.15 and a specificity of 0.95 [22].
4.6 Diagnostic Workup
Piriformis myofascial pain is a clinical diagnosis. Referred pain from the lumbar spine should be excluded. Imaging studies are obtained to rule out other causes of posterior hip pain.
X-ray
Plain radiographs of the lumbar spine, pelvis, and hip are considered to look for other sources of pain.
MRI
MRI of the lumbar spine may rule out sources of referred pain from the L5-S1 disc as S1 radiculopathy may have a gluteal pain component. MRI of the pelvis may demonstrate anatomic variants associated with a predisposition for piriformis pain. Some studies have proposed that the piriformis muscle may appear enlarged in cases of piriformis myofascial pain, but this is not pathognomonic, and most MRI studies are unremarkable [21, 22]. MR neurography may have a role in this diagnosis, but availability may be limited.
MSK ultrasound
Ultrasound evaluation of the sciatic nerve (with comparison to contralateral side) including cross-sectional area and sono-palpation of the piriformis muscle can be useful in making a diagnosis of piriformis myofascial pain and less-frequent coexisting sciatic neuralgia.
Diagnostic ultrasound-guided local anesthetic injection
A diagnostic anesthetic injection can be considered to guide further management.
Electrodiagnostic testing (EMG/NCS)
Electrodiagnostic testing is done primarily to exclude lumbosacral radiculopathy. Interestingly, studies have demonstrated a prolonged H-reflex in some cases of piriformis myofascial pain with sciatic neuralgia. However, electrodiagnostic sciatic neuropathy is generally not seen and studies are most often normal [22, 24].
4.7 Treatment
4.7.1 Medical Management
Pain control may be accomplished with NSAIDs and neuropathic agents including gabapentin and pregabalin.
4.7.2 Rehabilitation
It is recommended to avoid aggravating positions including prolonged sitting and frequent hip flexion, internal rotation, and adduction. Non-impact exercise is encouraged. Manual treatment for myofascial pain includes osteopathic manipulative treatment (OMT), proprioceptive neuromuscular facilitation (PNF), and soft tissue mobilization with deep tissue or self-massage of the piriformis and gluteal musculature. Dry needling of the piriformis and gluteal muscles can be utilized for pain management. Piriformis stretching can also be beneficial. Piriformis myofascial pain is often compensatory to deficiencies in gluteal strength and core control; therefore, a strengthening protocol should focus on lumbosacral and core stability with strengthening of the gluteal muscles and hip, particularly the hip extensors and abductors.
4.7.3 Procedures
Piriformis muscle trigger point injections
Palpation-guided trigger point injections to the gluteal and piriformis muscles with local anesthesia can provide a longer duration of relief compared to dry needling [23]. Such injections can facilitate rehabilitation. If done under ultrasound, twitch response may be visualized in either the gluteus maximums or piriformis muscle.
Ultrasound-guided corticosteroid injection
A corticosteroid injection to the piriformis muscle and/or muscle sheath can be performed for diagnostic and therapeutic measures.
Botulinum toxin
If there is reduction in pain from an ultrasound-guided diagnostic injection, a botulinum toxin injection to the piriformis muscle can be considered for refractory cases [22]. Cost and side effects usually prohibit this as a first-line treatment.
4.7.4 Surgery
In very rare instances of chronic, recalcitrant pain, surgical release of the piriformis with decompression of the sciatic nerve can be considered. Diagnostic tools for piriformis syndrome remain obscure, and careful selection of patients for surgery is necessary to obtain good outcomes. Current surgical methods include open or endoscopic decompression of the sciatic nerve by release of the piriformis muscle [21, 24]. In a study of surgical resection of the piriformis muscle in 64 patients, it has obtained 82% initial and 76% long-term good or excellent outcomes [25].
References
Cacchio A, Rompe JD, Furia JP, Susi P, Santilli V, De Paulis F. Shockwave therapy for the treatment of chronic proximal hamstring tendinopathy in professional athletes. Am J Sports Med. 2011;39(1):146–53.
Arner JW, McClincy MP, Bradley JP. Hamstring injuries in athletes: evidence-based treatment. J Am Acad Orthop Surg. 2019;27(23):868–77.
Degen RM. Proximal hamstring injuries: management of tendinopathy and avulsion injuries. Curr Rev Musculoskelet Med. 2019;12(2):138–46.
Chu SK, Rho ME. Hamstring injuries in the athlete: diagnosis, treatment, and return to play: diagnosis, treatment, and return to play. Curr Sports Med Rep. 2016;15(3):184–90.
Miller SL, Gill J, Webb GR. The proximal origin of the hamstrings and surrounding anatomy encountered during repair: a cadaveric study. J Bone Joint Surg Am. 2007;89(1):44–8.
Sharma P, Maffulli N. Biology of tendon injury: healing, modeling and remodeling. J Musculoskelet Neuronal Interact. 2006;6(2):181–90.
Fader RR, Mitchell JJ, Traub S, Nichols R, Roper M, Mei Dan O, et al. Platelet-rich plasma treatment improves outcomes for chronic proximal hamstring injuries in an athletic population. Muscles Ligaments Tendons J. 2014;4(4):461–6.
Auriemma MJ, Tenforde AS, Harris A, McInnis KC. Platelet-rich plasma for treatment of chronic proximal hamstring tendinopathy. Regen Med. 2020;15(4):1509–18.
Cho KH, Lee SM, Lee YH, Suh KJ, Kim SM, Shin MJ, et al. Non-infectious ischiogluteal bursitis: MRI findings. Korean J Radiol. 2004;5(4):280–6.
Van Mieghem IM, Boets A, Sciot R, Van Breuseghem I. Ischiogluteal bursitis: an uncommon type of bursitis. Skelet Radiol. 2004;33(7):413–6.
Kim SM, Shin MJ, Kim KS, Ahn JM, Cho KH, Chang JS, et al. Imaging features of ischial bursitis with an emphasis on ultrasonography. Skelet Radiol. 2002;31(11):631–6.
Wisniewski SJ, Hurdle M, Erickson JM, Finnoff JT, Smith J. Ultrasound-guided ischial bursa injection: technique and positioning considerations. PM R. 2014;6(1):56–60.
Finnoff JT, Johnson AC, Hollman JH. Can ultrasound accurately assess ischiofemoral space dimensions? A validation study. PM R. 2017;9(4):392–7.
Gollwitzer H, Banke IJ, Schauwecker J, Gerdesmeyer L, Suren C. How to address ischiofemoral impingement? Treatment algorithm and review of the literature. J Hip Preserv Surg. 2017;4(4):289–98.
Torriani M, Souto SCL, Thomas BJ, Ouellette H, Bredella MA. Ischiofemoral impingement syndrome: an entity with hip pain and abnormalities of the quadratus femoris muscle. AJR Am J Roentgenol. 2009;193(1):186–90.
Singer AD, Subhawong TK, Jose J, Tresley J, Clifford PD. Ischiofemoral impingement syndrome: a meta-analysis. Skelet Radiol. 2015;44(6):831–7.
Finnoff JT, Johnson AC, Hollman JH. Can ultrasound accurately assess Ischiofemoral space dimensions? A validation study. PM&R. 2016;9(4):392–7.
de Sa D, Alradwan H, Cargnelli S, Thawer Z, Simunovic N, Cadet E, et al. Extra-articular hip impingement: a systematic review examining operative treatment of psoas, subspine, ischiofemoral, and greater trochanteric/pelvic impingement. Arthroscopy. 2014;30(8):1026–41.
Wilson MD, Keene JS. Treatment of ischiofemoral impingement: results of diagnostic injections and arthroscopic resection of the lesser trochanter. J Hip Preserv Surg. 2016;3(2):146–53.
Cassidy L, Walters A, Bubb K, Shoja MM, Shane Tubbs R, Loukas M. Piriformis syndrome: implications of anatomical variations, diagnostic techniques, and treatment options. Surg Radiol Anat. 2012;34(6):479–86.
Byrd JWT. Piriformis syndrome. Oper Tech Sports Med. 2005;13(1):71–9.
Probst D, Stout A, Hunt D. Piriformis syndrome: a narrative review of the anatomy, diagnosis, and treatment. PM&R. 2019;11(S1):S54–63.
Hong CZ. Lidocaine injection versus dry needling to myofascial trigger point: the importance of the local twitch response. Am J Phys Med Rehabil. 1994;73(4):256–63.
Hopayian K, Song F, Riera R, Sambandan S. The clinical features of the piriformis syndrome: a systematic review. Eur Spine J. 2010;19(12):2095–109.
Filler AG, Haynes J, Jordan SE, Prager J, Villablanca JP, Farahani K, McBride DQ, Tsuruda JS, Morisoli B, Batzdorf U, Johnson JP. Sciatica of nondisc origin and piriformis syndrome: diagnosis by magnetic resonance neurography and interventional magnetic resonance imaging with outcome study of resulting treatment. J Neurosurg Spine. 2005;2(2):99–115. https://doi.org/10.3171/spi.2005.2.2.0099. PMID: 15739520.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
DeLuca, S., Borgstrom, H., McInnis, K.C. (2022). Posterior Hip Disorders. In: Mostoufi, S.A., George, T.K., Tria Jr., A.J. (eds) Clinical Guide to Musculoskeletal Medicine. Springer, Cham. https://doi.org/10.1007/978-3-030-92042-5_39
Download citation
DOI: https://doi.org/10.1007/978-3-030-92042-5_39
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-92041-8
Online ISBN: 978-3-030-92042-5
eBook Packages: MedicineMedicine (R0)