
Abstract
Hawai‘i’s history goes back to Pō, the beginning of time in the Hawaiian Islands. Centuries later, under Kamehameha the island nation unified into a state known as the Kingdom of Hawai‘i. It became a liberal democracy welcoming all races into society. Before the turn of the nineteenth century, the Hawaii Islands were taken in violation of international law by the United States. American colonization was imposed and continues today. Cultural loss, oppression, historical trauma, and forced assimilation persist in both the material realities and national memory of Hawaiians.
In a small but predominantly Hawaiian community, Hale Na`au Pono, broke many of the State-Federal controlled behavioral health system principles and found its expression of an indigenous liberation encapsulated in the acronym OLA, a unifying reference point for Pacific islanders and other social groups in circumstances envisaging a treatment milieu as well as an expression of health and life. This is in juxtaposition to the deep culture of D.I.E. (Domination, Individualism, and Exclusion) which pervades American society. This is a small yet persistent struggle for national self-determination expressed in the field of behavioral health.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Decolonization
- Deep culture
- Ho`oponopono
- Traditional practices
- Spirituality
- Hawaiian
- Health
- Indigenous knowledge
Hawaiʻi is an archipelago, which consists of eight major islands, several atolls, numerous smaller islets, and seamounts in the North Pacific Ocean that extend some 1500 miles (with an additional 200 miles running along the outer lines of the archipelago in accordance with the Law of the Seas Convention) from the island of Hawaiʻi in the south to northernmost Kure Atoll (Van Dyke et al., 1988). It is here where the Hawaiians established themselves followin4g years of exploration across the world from Asia throughout the Pacific that the history of Native Hawaiians originates. According to the traditional Hawaiian Kumulipo chant, the genealogy of the islands’ people began before time, in what is known as Pō or darkness, and out of that darkness came light, the separation of the waters from the land, and the many living forms, including eventually the kanaka or people (Kamakau, 1992). The gods created the lands of Hawaiʻi as well as the people who traveled to these islands and formed societies, becoming the Hawaiian people. These inhabitants’ (Nā Kanaka Maoli) ancient chants and other sources indicate that people were called Kanaka, which means person, people, or individual(s) which is also ancient based on the legendary mystical northern land called “Hawaiki” (Dudley, 1990; Fornander, 1996). They touched upon many lands including the most isolated land mass in the world: Hawaiʻi. Hawaiians conducted commerce with other Polynesians in the Pacific many years after arriving in Hawaiʻi and had infrequent contacts with Japan, the Great Turtle Island (today “North America”), South America, and other Pacific rim peoples. The people of these islands spoke a common language with some dialectic variations and followed generally common rules of conduct or kapu (prohibitions) that formed the social norms of conduct for this nation. The society was divided into a class structure of aliʻi (with authority due to a combination of mana, spiritual descent from gods or lesser gods), kahuna (priests), makaʻainana (general people), and kauwa (lower-level servants) (Kamakau, 1992). Hawaiʻi remained relatively unknown to Europe until January 25, 1778, when British Navy Captain James Cook arrived to find a highly developed society, kindling widespread knowledge of the islands and its people to the American and European world. Once this door was opened, immigrants from all parts of the world came to Hawaiʻi. Sailors from Europe and North America married into Hawaiian families and became part of the Hawaiian society, while Chinese and Japanese laborers came to work on sugar plantations or accompanied such workers (McDermott & Andrade, 2011). Christian missionaries also came to Hawaiʻi, with some remaining even after their formal missions were terminated, taking important roles in Hawaiian society (Merry, 2000). Many others, including those of African descent and other Polynesians, also established homes in Hawaiʻi (Jackson, 2005). As they did this, many renounced their former citizenship and took up Hawaiian citizenship (see also Husted, 1890).
In 1810, Hawaiʻi became united as a nation-state under the unification of Kamehameha I (1779–1819). The ensuing global influx to Hawaiʻi coincided with trade exchanges between Hawaiʻi and China, Great Britain, and the United States as well as other nations (Gonschor, 2019). In 1840, Hawaiʻi’s first written constitution was passed, containing a declaration of rights often referred to as the Hawaiian Magna Carta, that effectively transitioned the Hawaiian state from an “absolute monarchy” to a constitutional monarchy (Sai, 2013). For the next 70 years, the kingdom transformed from an elitist society based on the rule and rank authority of aliʻi and kahuna to an egalitarian one in which high-ranking chiefs and commoners were viewed as equal before the law (Osorio, 2002). The government also developed a system of schools, boosting Hawaiʻi’s literacy rate to one of the highest in the world (Sai, 2013). It was a modern society with a public health system and even had electricity and telephones at its ʻIolani Palace before the US White House. Its international stature as an independent nation (99 counselor and diplomatic posts) was without question holding treaties and executive agreements with almost every nation-state that existed at the time (Hawaiian Islands, 1887): from the German Empire to the lesser known country of Bremen, and from the imperial superpowers Great Britain and the United States to the “has been” imperial powers of Portugal and Spain. From 1810 until 1893, Hawaiʻi underwent many changes in its political formation, economy, demographics, educational quality, and international presence (McGregor & MacKenzie, 2014). Hawaiʻi was undergoing its course of development, unfolding into its future based on its own internal culture, hopes, and dreams for its future so that by 1892 it was a vibrant multiracial, multicultural nation engaged in intellectual and economic commerce throughout the world (Gonschor, 2019; Husted, 1890); but due to outside forces, this development did not continue.
Avaricious desire for wealth and power among remnants of the Christian missionaries, who aligned with US military interests, resulted in a conspiracy to land US forces in Hawaiʻi, wresting the power from the constitutional monarch, Queen Liliʻuokalani, and placing it in the hands of the “Missionary Boys,” who then became known as the provisional government (Dudley & Agard, 1990). The provisional government (PG) attempted to cede Hawaiʻi to the United States in a treaty of annexation, but President Cleveland intervened and rejected the treaty. Previously formed by proclamation, the PG ratified a self-serving constitution, blocked the vast number of Hawaiians from participating, changed its name to the Republic of Hawaiʻi, and resubmitted another annexation treaty when a new president, McKinley, took charge 4 years later. The treaty was again resisted by widespread Hawaiian protest (Minton & Silva, 1998) as well as by those in the United States who recalled Cleveland’s Congressional address (Cleveland, 1893). Realizing the “treaty” could not get the 2/3 Senate approval required of the US Constitution, the conspirators circumvented that requirement and settled for only a joint resolution of Congress, known as the Newlands Resolution, which, over the outcry of the vast majority of people, was passed in Hawaiʻi on July 7, 1898 (30 Stat. 750; 2 Supp. R.S. 895). The McKinley administration circumvented the constitution (Art. 2, Sec. 2, Clause 2, US Constitution) and declared Hawaiʻi annexed by a joint resolution of both houses of Congress (Richardson, 1908). It took up a third of the Hawaiian lands for its military and imposed its colonial control over all public education , travel outside of Hawaiʻi, and international trade. In addition, the US president appointed a territorial governor, all judges to courts, and instituted taxes on the Hawaiian people. The United States would obtain the choicest lands and harbors for their Pacific armada. Queen Liliʻuokalani’s protests that the occupation was a breach of treaties international law were simply ignored (Liliʻuokalani, 1898).
When the United Nations was formed in 1945, territories such as Hawaiʻi were to be given three options: independence, free association, or integration (UN Charter, Article 73; UN G.A. Resolution 66(1) 1946). The United States took no action toward the option of independence or free association, leaving only integration as the “choice,” i.e., remaining a territory of the United States or become the “State of Hawaiʻi” (Admission Act of March 18, 1959, Pub L 86–3, 73 Stat. 4; see also Laenui et al., 2020).
In 1993, the United States adopted an apology resolution (Pub L 103–150, 107 Stat. 1510)—echoing the sentiment of President Grover Cleveland (Gillis, 1897)—admitting its wrongdoing nearly 100 years after the Queen’s government was overthrown. The “Apology Bill,” as it became known as, was symbolic in meaning but without legal traction in the court of US law, so although granting a major concession that validates the grievances of Native Hawaiians was welcome, legal, and just, it does little to assuage the material realities faced by Hawaiians as a consequence of the illegal overthrow of the Kingdom (SB 2899 & HB 4909, 106th Congress, second Session).
It is against this historic backdrop that mental health or behavioral health services are situated in the Hawaiian Islands—once administrated by the kingdom’s government, they are now controlled by the US government and the State of Hawaiʻi. The social, political, environmental, economic, health, and educational systems impinging upon behavioral health services are no longer under the functional control of the kingdom’s government.
DIE Culture in Contemporary “Systems of Care” and OLA Cultural Care Models
There are cultural codes in the collective subconscious of all societies that define what is right and wrong, what is moral and natural, and which forms of behavior are appropriate in any given circumstances (Laenui, 1997a). These codes derive from myths and legends, deep national memories, environmental conditions, and internal conflicts, along with a multitude of other processes that have occurred over long periods in a society (Laenui, 2013). These codes are not to be found in a constitutive document or in some explicit statement but are generally unwritten and usually unspoken; yet they are so ingrained in a society; they become its very driving force. You can often observe these norms and beliefs in the routines and habits of people, in their fears and pleasures, in their dreams and expectations, and in their systems of reasoning. In Hawaiʻi, at least two distinct deep cultures touch on every area of life. One is prominent in the formal and the other in the informal systems of community life. The first of these cultural codes, identified by the acronym DIE (Domination, Individualism, and Exclusion) (Laenui, 1997b), is emblematic of the Americanized social order and wedded to the Hawaiʻi Islands as a multiethnic colony (Baumhofer & Yamane, 2019; Fojas et al., 2018; Fujikane & Okamura, 2008; Irwin & Umemoto, 2016; Kaholokula et al., 2020):
Domination—especially reflected in the formal economic, education, political, military, and judicial systems. Central to this colonialist characteristic is the idea of expansion in terms of an ever-widening territory, market, or other field of conquest as part of the natural order of things. Colonialism has for years led Indigenous people to believe they are outside of, and unwelcome in, mainstream culture while diluting the influence of a traditional Indigenous influence at the same time (Blume, 2020; Duran, 2019; Muller, 2020). This social control and cultural containment structure is a reflection of the multiethnic dominance of the State bureaucracy extending its governance to colonial-induced poverty and inequities as well as the over-incarceration synergistically contributing to the systemic and systematic “clientization” of (darker-skinned and poorer) Native Hawaiians (Office of Hawaiian Affairs (OHA), 2019). As a result, Native Hawaiians are grossly overrepresented as subjects of “treatment” within the State’s human services in addition to its criminal justice and social welfare systems (OHA et al., 2010; OHA, 2019). Hawaiians, who are thereby redefined as “clients,” “consumers,” and “patients,” are human bodies signifying value—reconstituted as Medicaid (Med-Quest) sponsored commodities—integral to the fiscal viability of many public (and private) substance abuse treatment and behavioral health programs. Subsidized by the State, treatment programs and human services agencies form part of the social control infrastructure within State apparatuses and can be viewed as a modern form of colonial domination. Top-down administrations of contemporary “systems of care” generally replicate forms of control, containment, regulation, punishment, penalty, and coercion of Indigenous people as a feature of colonial bureaucracies (Blume, 2020; Muller, 2020). Moreover, any program bearing the term of culturally integrated usually means that Native Hawaiian practice is, at best, offered separately on a parallel treatment track and consequentially fragmented within the treating agency (Williams et al., 2019). As a certain eventuality of colonization and coloniality, Hawaiian cultural practices are subordinated to the cultural dominance of Western/American approaches and not given full recognition; that is, the language, history, protocol, values, and healing traditions are largely ignored, excluded, or tokenistic in “systems of care” (see also Williams, Rezentes et al., in press). Conversely, cultural practices may be visibly displayed and touted in treatment programs while processed through top-down bureaucratic control mechanisms and conducted in such a fashion as to institutionally undermine the legitimate value of Native Hawaiian cultural practices as a form of treatment (Williams, 2019; Williams et al., 2019).
Individualism—protected in the legal system, elevated in the expression of history, and dominant in Western philosophies. Central to this formal characteristic is the idea of singularity—a continual separate parceling and fragmenting of things, concepts, and people. Although the treatment modalities in most treatment settings may include groups, for instance, the treatment is clearly targeted at individual clients (Blume, 2020; Duran, 2019; Linklater, 2014; Muller, 2020). Hence, treatment models focus on individuals avoiding risk (exposure to people, places, environs, re-experiencing tragic moment which brings up sense of guilt, substance use, etc.) rather than on decision-making at the familial and community level (Blume, 2020). All aspects of care, from treatment plans and goals to specific care regimes, are focused on the individual. Although this perspective is necessary to a large extent given the Americanized “systems of care” and its expression of cultural values, expectations, and norms, it is in itself incomplete and certainly does not fit in the worldviews of Native Hawaiians. The more traditional view of Native Hawaiians is to perceive health and well-being collectively in relation to the societal contexts of family and community in an interplay between relational pressures and health-related norms impacting both treatment and Hawaiians receiving services. Additionally, from a more complete historical perspective of continuing American occupation of Hawaiʻi—coloniality—and the associated intergenerational trauma is essential. As a subject of treatment recovery as well as a material reality to be confronted and engaged in as a means of therapy (e.g., see Williams, Makini Jr., & Rezentes III, 2021), the fact of coloniality in the Hawaiʻi Islands and its health-related ramifications are largely absent from conventional behavioral health and drug treatment procedures, processes, and outcome measures. The contemporary form of mental, behavioral, and addiction treatments is often directed to experiences and training that emanate from colonial societies and their “best practices” as “proven” and normalized to a colonial culture and society. Ultimately, this becomes another attempt to impose a set of values and beliefs—a morality—on the Hawaiian person that can be self-sabotaging and antithetical to Hawaiian cultural identity and nationalism. Successful adaptation to the conditions of State-sanctioned incarceration is contingent on self-preservation or a highly selfish survival-oriented morality, for example, State-subsidized drug abuse treatment programs and the State’s criminal justice system coercively compel Hawaiian people into abstinence-oriented lifestyles and regard any substance use—whether for spiritual reasons, communal bonding, cultural revitalization of indigenous psychoactive drug use, or motivated by other social activity with therapeutic purpose (e.g., Williams, Davis, et al., 2021; Williams, Makini Jr., & Rezentes III, 2021; Williams et al., in press)—as problematic and emblematic of failure worthy of treatment termination and warranting suspension of free will.
Exclusion—often accomplished by the depersonalization of the “other,” the stranger. One patent colonial technique is to refer to others as nonhuman entities—“heathens,” “pagans,” or “savages”—as missionaries did in the early nineteenth century when they clashed with native ways of being and the persisting traditional religion of Hawaiʻi, known commonly as the kapu or mana belief system (Merry, 2000). The colonial system elevates academic achievements in specialized fields and the accumulated entitlements from academic circles while contemporary traditional healers of the Hawaiian community, the kupuna, kahuna, and kanaka makua (identified as people with the maturity of parents) are erased, degraded, and generally eliminated from the treatment community. Their “credentials” of experience and training in fishing, farming, warfare, hunting and gathering, and their resolution of inter-family or inter-gang conflicts in communities are given no credibility in the State’s colonial “systems of care.” The tools of traditional healers such as prayer, hoʻoponopono practices, laʻau lapaʻau (herbal and other traditional medicine including water treatments), laʻau kahea (treatment by the use of a “call,” such as a chant or prayer, used to work on the spiritual level), or other counseling activities conducted by such traditional healers are discredited and therefore not reimbursed. The healers have no regular place to practice their treatment, which is generally performed in informal community settings such as farms (Hoaʻaina o Makaha) or fishing training facilities (ʻOpelu Project) or on ocean vessels (Hokuleʻa, Hikianaliʻa, etc.).
Moreover, agencies buttress their services on individual assumptions, emphasizing the client’s individual psychology at the expense of the client’s relational concerns within their environment and the political positioning and/or economic situation. For instance, mainstream treatment practices may coexist with “Native Hawaiian culture” under the auspices of cultural competence and cultural humility, but the individualized treatment model lies outside the legacies of forced acculturation and intergenerational trauma of the American colonization of Hawaiʻi negatively reverberating on Hawaiian genealogies of the past, present, and future. This, however, is at the foreground of Hawaiians’ cultural understandings of mental health and well-being regarding the root causes of the psychological, cultural, social, environmental, political, and economic losses pervading Hawaiian communities (Rezentes III, 1996). Lacking a communalistic focus, treatment modalities create a fundamental cultural mismatch that excludes the material realities of Hawaiians and results in a mode of treatment that casts behavior as a discrete function of individual autonomy and individual beliefs through the paradigms of motivational enhancement and behavioral modification (Blume, 2020). Further, these treatment modalities are employed in an office-based setting that undermines the communal embeddedness of the individual as a whole being and do not materialize improvement in community conditions or the attendant social problems elevating risk for mental illness and drug misuse (Duran, 2019). As such, service delivery for Native Hawaiians compartmentalizes the individual and largely ignores or excludes the person’s familial and communal interdependence—a reductionist paradigm of the Hawaiian psyche/psychology (Rezentes III, 1996). While State funding of human services and other treating agencies mostly benefit non-Hawaiian employees representing “systems of care,” the State nonetheless highlights in its own reports the total funds exceedingly “expended for Native Hawaiians” as (a hypocritically self-congratulatory) testament to its commitment to cultural sensitivity toward a “special group” (e.g., see Alcohol and Drug Treatment Services Report issued by the Department of Health’s Alcohol and Drug Abuse Division (ADAD), 2021; see also Williams, 2019).
The second deep culture stream contains elements of the following characteristics:
ʻOluʻolu—a person who is amiable and agreeable and who creates harmonious relationships; who displays a high degree of respect and trust when interrelating with others, even their competitor; the ability to find contentment with what one has; of staying within the bounds of one’s kuleana (territory, property, or responsibility). One way to ensure ʻOluʻolu in the behavioral health center is to include the voices of service recipients in ways that allow their worldview to positively shape and impact the development of services. This can be partially achieved by gathering data either from feedback-informed treatment or measurement-based practice, asking the Native Hawaiians who have experienced treatment to rate the benefits of various components of it (Williams et al., 2019). Such measures do not refer to any subjective “satisfaction,” but aim to discover which components have been beneficial in achieving recovery. Respondents could also be asked to suggest changes they believe should be made and to mention any instances of feeling demeaned or disrespected by providers. Specific areas where the answers cluster can prove illuminating and serve in identifying which program components are helpful and which are not. Once the salient topics are identified, many of the constructs could be quantified on a Likert scale. If the construct is “real,” it should be measurable and can be grouped and scored. ʻOluʻolu also entails gathering information grounded in the needs and preferences to tailor treatment matching, where deemed culturally appropriate by Native Hawaiians in terms of ascribing: procedures (e.g., use of Hawaiian cultural protocols monitored and supervised by cultural experts), processes (e.g., behavioral health interventions meet Hawaiian people where they are at; in their respective communities and families), and outcome measures (e.g., a rise in Hawaiian national consciousness linked to improved mental health or remission of drug misuse).
Lokahi—a collective effort, with many working toward a common goal that leads to a clearer view of the wider implications of all things, both large and small. Similarly, positive outcome measures for wellness could include how “systems of care” have impacted the individual’s holistic well-being as well as that of their families and communities. Efforts toward recovery are too commonly institutionally controlled and directed in a situation isolated from the relationships to (extended) families and the broader environment/land that surround and support Hawaiians, rather than community grounded (Rezentes III, 1996). Moreover, an individual’s positive treatment outcome would mean an improvement in their overall quality of life (Blume, 2020), to include acknowledging and addressing the consequences of coloniality and the mental health impact of the continual US occupation of the Hawaiian Islands affecting Native Hawaiian cultural well-being.
Aloha—a propensity toward the inclusion of other people and different philosophies; a search for the humanity within others and an effort to draw that humanity to the surface of relationships. The all-inclusive Aloha draws into the family all of the surrounding environmental elements, which carry a spirituality that unites the family to the whole environment. From a Hawaiian perspective, recovery means restoring the correct relationships with the Hawaiian Islands as Indigenous people, alongside the healing in the proper relationships that are central to the holistic frameworks of the sovereignty, political self-determination, independence, and autonomy essential to wellness and recovery. Treatment therefore includes the haumana or client and others associated with the client (including the spouse, partner, boss, and children). Together with an addiction expert, cultural informant, nurse, etc., they can impart a program of recovery that ideally would include certain cultural features relevant to the specific condition of the haumana.
Taken together, this “OLA” is generally attributed to the underlying Hawaiian culture and the multiplicity of added cultures to Hawaiʻi. Entrenched in the informal economy of sharing and caring, the spirit of OLA infuses the nonformal education as well as the traditional healing and the indigenous methods for resolving disputes; it also influences the organization of the community. In the Hawaiian language, as in other Polynesian languages, OLA means both health and life. The word itself is sometimes used in healing prayers when the healer breathes it into the hands and then spreads them over the places that need healing. The acronym DIE is an easy reminder of the elements of that deep culture stream, which is prevalent in the formal systems, even within the religious and healthcare practices. It would, of course, be rare to find a purely DIE or OLA perspective in the general community, as these ingrained cultures constantly mix, conflict, and sometimes work together within and between individuals and families, as well as within certain systems and situations. The presence of these beneficial practices and beliefs justifies a cultural assessment of the entire treatment setting to provide a framework of culturally appropriate ideas on which to build mutual relationships, pursue a healthy interaction with the environment, and reshape attitudes to time, family justice, sharing and caring, and medicine (Rezentes III, 1996). The acronym DIE is also a reminder that colonial practice is essentially one based on DIE at its core (see also Laenui, 2000b).
Hale Na‘au Pono: Cultivating OLA Against the Forces of DIE
Since the 1960s, a vibrant development of indigenous and Hawaiian national consciousness has occurred that questions the sanctity of American entitlements across the world and the superiority of moral stature in US territories (Laenui, 1993). This Hawaiian cultural awakening has underscored questions and implications related to Native Hawaiian self-determination, independence, and sovereignty (Laenui, 1996). This momentum raised questions concerning primary and behavioral healthcare as it came to the attention of Waiʻanae, which is a community of the largest number of Native Hawaiians in Hawaiʻi.
Hawaiʻi was undergoing changes in mental health treatment as part of the Community Mental Health Act of 1963 (also known as the Mental Retardation and Community Mental Health Centers Construction Act of 1963), which drastically altered the delivery of mental health services and inspired a new era of optimism in mental healthcare. It established comprehensive community mental health centers throughout the State and helped people with mental illnesses who were “warehoused” in hospitals and institutions to reintegrate into their communities.
In the 1970s, the State opened a clinic to service the population of approximately 40,000 residents of Waiʻanae. A community elder, Marie Olson, who wanted to gauge the utilization of services, spent a week sitting in the waiting room of the clinic, counting the number of clients who attended for service; but she counted only three in the course of the week. Olson and other community elders petitioned the Hawaiʻi State Department of Health to devolve service responsibility to the community. The State took up this opportunity, agreeing to spin off the Waiʻanae “catchment area” to a not-for-profit community entity, using this experience to see whether a model could be established for community empowerment in mental health services. With this “go ahead” from the State, the community organized a not-for-profit organization, the Waiʻanae Coast Community Mental Health Center, and obtained a 4-year grant to develop a center to reflect the possibility for a model for communities to run their own centers for behavioral healthcare. The new organization adopted a name, Hale Na′au Pono (House for Inner Balance), and over a period of several years transitioned with personnel, leadership, and a clear statement of its community and cultural connection to services. It began a private funding campaign for a modern building in the heart of the community and, through its location, established a central presence there. Hale Na′au Pono’s community-based board of directors selected a member of the community who had previously served as a volunteer board member to steer the organization through the coming years. Several unique approaches and services to the community were rolled out while still operating within the confines of an Americanized model of behavioral health practice and a colonized system of healthcare delivery. As Hale Na′au Pono proceeded to develop its Waiʻanae style of practice, it had to begin with the basic format of the practice already established by the State system and its regulators/standard-setters (Laenui, 2001a). Upon that established practice, Hale Na′au Pono adopted a number of unique principles and processes—traditions, as part of its effort to imbue an OLA approach to health (Laenui, 2001b), which are listed in the following section.
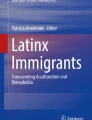
The ABC Triangle of Peace and Violence
The practice of behavioral health services can be thought of as a twofold challenge: understanding and/or altering behavior, then bringing such behavior within an acceptable range for the target community or wider society (Laenui, 2002). Hale Na′au Pono (HNP) borrowed from Johan Galtung, distinguished professor of peace studies and HNP’s executive director, to understand and appreciate peace and violence as simply as ABC.
The apices of an equilateral triangle—A, B, and C—help us set the framework for an understanding of peace, violence, and other behaviors, as well as the possibilities for change: Point A for attitudes at the left lower side, B at the top for behavior, and C on the right lower end for conditions. At Point A, position basic attitudes, assumptions, and aspirations on the individual, community, or societal levels. Point A describes frames of mind that cause people to project anger, assume an argumentative stance, project a peaceful nature, submit, or any combination thereof. At Point A, we find cultural belief systems so deeply rooted within people that they are usually accepted as normal and natural, part of the make-up of life. This rootedness is a result of upbringing; living conditions; model behavior of elders, peers, and national figures; and social propaganda. Male superiority, the attitude of “payback,” property as a measure of individual worth, physical strength as a determinant of one’s value, and the idea of triumphant psychology are all examples of such beliefs and goals that are presumed to be the natural order!
Point B stands for Behavior: direct and indirect. Direct behavior is the direct conduct and physical violence including aggressive national acts (e.g., fighting, shooting, stabbing, bombing raids). In response, we create institutions to imprison, develop programs to modify direct behavior, and continually develop different techniques to suppress direct physical violence. Indirect conduct is violence to the human spirit. This behavior takes the form of disparate treatment based on race, religion, size, gender, sexual orientation, etc. Examples of indirect violence are continual nagging, teasing, harassing, and other forms of verbal and psychological abuse. On a national scale, it may be “economic sanctions” or demonizing a national leader at international conferences. Often, this indirect violence begets responsive direct violence, which society immediately reacts to and chastises as being the primary fault.
Point C is where we place conditions, conflicts, and contradictions. This point may include the hypocrisy between a nation’s creed and deeds—proclaiming equality for all men while prohibiting Black Americans from registering to vote, attending white schools, or sitting at the front of buses. It can also be a society whose government admits to the theft of one’s national life contrary to accepted international norms but thumbs its nose at any call for effective remedy, forcing the victims to conform to the imposed colonial structure. Additionally, it can describe the economic situation of an ohana (family) in which the father lost his job 6 months ago, including family esteem, and begins to use physical violence on his wife and children to regain his stature.
Recall that Point B (Behavior) is at the top. Thus, behavior is a direct result of either or both A and C. Thus, if we hope to change behaviors, we need to address Points A and C for individuals, communities, and their institutions, keeping in mind the way in which culture—and the conditions surrounding and affecting the other—impacts the wider influences upon individuals and societies. Actions that respond to violence by merely criminalizing or suppressing behavior, by separating offenders from the rest of the community, or through other responses limited to dealing solely with behavior without tackling the deeper problems of attitudes and conditions are of no long-term value and will not lead to appropriate provision of services.
Hoʻoponopono
Hoʻoponopono, a traditional Native Hawaiian healing practice of reconciliation and forgiveness, brings things or relations back into pono (proper balance, repair) (Laenui, 2000a). This could mean restoring relationships or cleaning away the hihia, or entanglement, that has caused problems. All the many styles of Hoʻoponopono all seem to involve invoking spiritual forces. One style which comes from Kaʻu on Hawaiʻi Island involves a very orderly “group therapy”: calling together all family members involved, as well as invoking ancestor spirits, family guardian spirits (aumakua), and God or gods. Another form of Hoʻoponopono is a specialized process or order of prayers, led by one with a special power (Shook, 2002).
Hoʻoponopono can be useful in the gap where “traditional” healing ends. A war veteran came into HNP. He said the Veteran Administration services told him they could not help him any further and that he should seek help from HNP. Asked what was his pilikia (trouble), he said, “I lost my soul in the war in Vietnam and don’t know how to call it back!” One of the forms of Hoʻoponopono spiritual work is called ʻuhane hele (spirit travel). A Hawaiian Hoʻoponopono practitioner, kahuna pule (prayer specialist, generally also Christian), may either ask the client to explain his pilikia or may simply observe the individual(s) to see the spiritual forces that have entered the room or detect other problems or tensions brought by the client(s) (Pukui et al., 1979).
Before beginning the prayer, one approach is a cleansing. A mixture of water, sea salt, ʻolena (turmeric root), and the young shoot of the ki or tea plant is prepared and blessed by the kahuna pule. Then, it is dabbed on the client’s shoulders and the back of their neck. Then, the client sips the mixture. The kahuna (or a helper) will begin the prayer, and the kahuna will receive the “showing” or revelation of the problem. In the case of a person who has suffered from ʻuhane hele, the spirit can be called back after understanding why the spirit traveled and the conditions for its return. In one circumstance, a Japanese mother died at a train station in the United States, but her spirit would not return home to Hawaiʻi. When the spirit was asked why she would not return, the spirit replied it was because there was too much hilahila (shame) as her son had left his wife and gone with another woman. So, her spirit chose to remain away from her home. A similar spirit consultation would be done for the Vietnam War veteran. Then the appropriate procedure or rites would be done.
Practitioners of Hoʻoponopono use a variety of tools. In addition to water or a liquid mixture as mentioned above, just the force of words—hua ʻolelo (fruit of speech)—can be sufficient to form and carry the spiritual significance of the practice. This can be done via the Christian Bible, having God speak to them through the open Bible (wehe i ka paipala). Others use prayers, revelations, or visions that come to them. All these practices incorporate words from the person leading the process and/or the participating parties to the process. These elements carry strong representations of features of God. Indeed, the awareness of a higher spiritual power than the participants is always present, often in the form of ancestral spirits and in a God element (Pukui et al., 1972).
Environment and Spirituality
Another area of cultural consideration for Hale Na′au Pono’s care model lies in the overlap between the environment and spirituality unfolded into addiction and serious mental illness recovery pathways, especially the aspect of balance or harmony (Laenui, 2006). Returning a client to the ocean is often a washing away of tensions and negative spiritual moods, a spiritual cleansing via an immersion into the original amniotic fluid (i.e., the Pacific Ocean) (Rezentes III, 1996). Some would explain this cleansing as the balancing of the Yin and Yang energies, where the Yang/land energy needed the opposite, softer, calming energy that the Yin/ocean energy provided. In addition to the ocean, the mountains and valleys provide healing for many clients, as do plants. The belief is that natural elements (e.g., plants) carry mana (spiritual energy), assisting in healing by correcting energy imbalances (Rezentes III, 1996).
Conclusion
The manner in which Hawaiʻi’s sovereignty was lost to illegal colonization is constitutive in the national history and memory that is carried by Hawaiians to this day (Blaisdell, 2002; Crabbe, 2007; Laenui 2019). This reality is still profoundly felt and expressed through strong oral traditions, tight-knit communities, and expansive familial networks that span the Hawaiian archipelago (Paglinawan et al., 2020; Trask, 1999).
This chapter has underscored the Hawaiian national consciousness in the practice of behavioral health, highlighting a collection of experiences, practices, readings, discussions, and consultations distilled into the Hale Na′au Pono training materials developed for its Adult Mental Health Division. Hale Na′au Pono adopted an OLA cultural care model for application in the indigenous context—centralizing the cultural views of the community and family, emphasizing spirituality and the environment, and adopting general models such as the ABC triangle and Hoʻoponopono. Specifically, this model follows a basic structure called the Kumu Ola Pono (Waiʻanae Wellness Model) that calls for balance among three realms: the spiritual, the personal/familial, and the environmental (Laenui, 2006). Each is harmonious within itself and between the others. Hale Na′au Pono’s system of OLA evolved within the broader constraints of a DIE culture propagated through State and federal laws and regulations that stress risk management, liability, and solving individual problems by taking a deficits-based approach. The system uses a so-called strengths-based perspective with a psychocentric focus on individuation and with office-based funded interventions defining the discrete and siloed nature of service provisions. At odds with the assumptions underlying the treatment modalities cultivated by the philosophy of OLA, those ontological strands of a DIE culture represent challenges, especially in terms of funding—the colonial bureaucratic hammer, if you will—through which the State has controlled the development of programs as well as orchestrating pressure and punishment (i.e., financial duress) to channel the efforts of Hale Na′au Pono into conformity. Other Indigenous scholars with direct practice experience in Canada, America, and Australia have alluded to some of the contaminants of DIE or noxious cultural pollutants generated and present within colonized “systems of care” (Blume, 2020; Duran, 2019; Linklater, 2014; Muller, 2020).
In gleaning the potential differences in mental health and addiction treatment services informed by OLA, compared to that underpinned by DIE, we hope this chapter will overall be of interest to any practitioner operating within a context of colonization and coloniality, implementing locally developed behavioral health models that offset the cultural infringements of DIE. While the focus of this chapter has been on the Hawaiian psyche/psychology in relationship to health services, the dimensions of DIE/OLA—a conceptual framework—is also a unifying reference point for Indigenous people and other social groups in circumstances envisaging a treatment milieu conducive to OLA as they struggle to express their own self-determination for community strength, mental health, and traditions.
References
Alcohol and Drug Abuse Division [ADAD]. (2021). Alcohol and Drug Treatment Services Report. https://health.hawaii.gov/substance-abuse/prevention-treatment/treatment/
Baumhofer, K. N., & Yamane, C. (2019). Multilevel racism and native Hawaiian health. In C. L. Ford, D. M. Griffith, M. A. Bruce, & K. L. Gilbert (Eds.), Racism: Science and tools for the public health professional (pp. 1–17). American Public Health Association Press. https://doi.org/10.2105/9780875533049ch19
Blaisdell, K. (2002). Historical and cultural aspects of Native Hawaiian health. In P. Spickard, J. L. Rondilla, & D. H. Wright (Eds.), Pacific diaspora: Island peoples in the United States and across the Pacific (pp. 279–285). University of Hawai‘i Press.
Blume, A. W. (2020). A new psychology based on community, equality, and care of the earth: An indigenous American perspective. Praeger.
Cleveland, G. (1893, December 18). Message about Hawaiʻi [Speech]. Senate and House of Representatives. https://www.congress.gov/congressional-record
Crabbe, K. O. M. (2007). Kupa'a I ke kahua o Hawaiʻi: Stand firmly behind the foundations of Hawaiʻi. Journal of Pacific Rim Psychology, 1(2), 25–30.
Dudley, M. K. (1990). A Hawaiian Nation I: Man, gods, and nature. Nā Kāne O Ka Malo Press.
Dudley, M. K., & Agard, K. K. (1990). A Hawaiian Nation II: A call for Hawaiian sovereignty. Nā Kāne O Ka Malo Press.
Duran, E. (2019). Healing the soul wound: Trauma-informed counseling for Indigenous communities (2nd ed.). Teachers College Press.
Fojas, C., Guevarra, R. P., & Sharma, N. T. (2018). New politics of race in Hawai‘i. In C. Fojas, R. P. Guevarra Jr., & N. T. Sharma (Eds.), Beyond ethnicity: New politics of race in Hawai‘i (pp. 1–18). University of Hawai‘i Press.
Fornander, A. (1996). Ancient history of the Hawaiian people to the times of Kamehameha I. Mutual Publishing.
Fujikane, C., & Okamura, J. Y. (Eds.). (2008). Asian settler colonialism: From local governance to the habits of everyday life in Hawai’i. University of Hawai‘i Press.
Gillis, J. A. (1897). The Hawaiian incident: An examination of Mr. Cleveland’s attitude toward the revolution of 1893. Lee and Shepard.
Gonschor, L. (2019). A power in the world: The Hawaiian kingdom in Oceania. University of Hawaiʻi Press.
Hawaiian Islands. (1887). Treaties and conventions concluded between the Hawaiian kingdom and other powers since, 1825. Elele book, card and job print.
Husted. (1890). 1892: Directory and handbook of the kingdom of Hawaiʻi. F.M. Husted.
Irwin, K., & Umemoto, K. (2016). Jacked up and unjust: Pacific islander teens confront violent legacies. University of California Press.
Jackson, M. M. (Ed.). (2005). They followed the trade winds: African American in Hawai‘i (Rev. ed.). University of Hawai‘i Press.
Kaholokula, J. K., Miyamoto, R. E. S., Hermosura, A. H., & Inada, M. (2020). Prejudice, stigma, and oppression on the behavioral health of Native Hawaiians and Pacific islanders. In L. Benuto, M. Duckworth, A. Masuda, & W. O’Donohue (Eds.), Prejudice, stigma, and oppression (pp. 107–134). Springer.
Kamakau, S. M. (1992). Ruling chiefs of Hawaiʻi (Rev. ed.). The Kamehameha Schools Press.
Laenui, P. (1993). The rediscovery of Hawaiian sovereignty. American Indian Culture and Research Journal, 17, 79–102. https://doi.org/10.17953/aicr.17.1.v520565l30116036
Laenui, P. (1996, August 16). Statehood and sovereignty [Speech transcript]. Hawaiʻi Public Television.
Laenui, P. (1997a, January 27). DIE & OLA: Two deep cultures in Hawai‘i. Institute for the Advancement of Hawaiian Affairs.
Laenui, P. (1997b, October 22). On deep cultures and colonization: A Hawai‘i case study. Institute for the Advancement of Hawaiian Affairs. http://www.Hawaiʻianperspectives.org/
Laenui, P. (2000a). Correcting wrongs: Ho‘oponopono [Paper presentation]. Church of the Cross Roads, Honolulu, Hawaiʻi. Institute for the Advancement of Hawaiian Affairs. http://www.Hawaiʻianperspectives.org/
Laenui, P. (2000b). Processes of decolonization. In M. Battiste (Ed.), Reclaiming indigenous voice and vision (pp. 150–160). UBC Press.
Laenui, P. (2001a, March 8). Asian Pacific Americans and our political involvement, access and future [Paper presentation]. UCLA School of Law.
Laenui, P. (2001b, March 9). Walking the crooked path straight. Hale Na’au Pono, Wai’anae Coast Community Mental Health Center. http://www.Hawaiʻianperspectives.org/walking-crooked-path-in-ms-word-updated-2020/
Laenui, P. (2002, September 25). The ABC triangle of peace and violence. Institute for the Advancement of Hawaiian Affairs. http://www.Hawaiʻianperspectives.org/
Laenui, P. (2006). Voyage to recovery. Hale Na’au Pono, Wai’anae coast community mental health center. Institute for the Advancement of Hawaiian Affairs. http://www.Hawaiʻianperspectives.org/
Laenui, P. (2013). Cultural sensitivity in delivery of social services. Journal of Indigenous Social Development, 2(1), 1–9.
Laenui, P. (2019). The 2016 Na‘i Aupuni congregation: A brief study in a practice of indigenous self-determination. Hūlili: Multidisciplinary Research on Hawaiian Well-Being, 11(1), 83–154.
Laenui, P., Dudley, K., Siu, L. K., & de Zayas, A. (2020, April 20). A call for review of the historical facts surrounding UNGA resolution of 1959 that recognized attainment of self-government for Hawaiʻi. Transcend Media Service: Solutions-Oriented Peace Journalism. https://www.transcend.org/tms/?s=Poka+Laenui
Liliʻuokalani. (1898). Hawaiʻi’s story by Hawaiʻi’s Queen. Lee & Shepard. https://digital.library.upenn.edu/women/liliuokalani/Hawaiʻi/Hawaiʻi.html
Linklater, R. (2014). Decolonizing trauma work: Indigenous stories and strategies. Fernwood Publishing.
McDermott, J. F., & Andrade, N. N. (Eds.). (2011). People and cultures of Hawai‘i: The evolution of cultures and ethnicity. University of Hawai‘i Press.
McGregor, D. P., & MacKenzie, M. K. (2014). Mo‘olelo Ea O Nā Hawai‘i: History of native Hawaiian governance in Hawai‘i. Office of Hawaiian Affairs.
Merry, S. E. (2000). Colonizing Hawai‘i: The cultural power of law. Princeton University Press.
Minton, N., & Silva, N. K. (1998). Kū‘ē: The Hui Aloha ‘Āina Anti-Annexation Petitions, 1897–1898. http://libweb.Hawaiʻi.edu/digicoll/annexation/petition/pet-intro.php
Muller, L. (2020). A theory for indigenous Australian health and human service work: Connecting indigenous knowledge and practice. Routledge.
Office of Hawaiian Affairs. (2014). Income inequality and Native Hawaiian communities in the wake of the great recession: 2005 to 2013. http://www.oha.org
Office of Hawaiian Affairs. (2017). Native Hawaiian health fact sheet 2017: Native Hawaiian health status (Vol. 4.1). http://www.oha.org
Office of Hawaiian Affairs. (2019). Native Hawaiian data book. http://www.ohadatabook.com/DB2019.html
Office of Hawaiian Affairs, Justice Policy Institute, University of Hawai‘i, and Georgetown University. (2010). The disparate treatment of Native Hawaiians in the criminal justice system. http://www.oha.org
Osorio, J. K. K. (2002). Dismembering lāhui: A history of the Hawaiian nation to 1887. University of Hawai‘i Press.
Paglinawan, L. K., Paglinawan, R. L., Kauahi, D., & Kanuha, V. K. (2020). Nānā I Ke Kumu—Look to the source (Vol. 3). Lili‘uokalani Trust.
Pukui, M. K., Haertig, E. W., & Lee, C. A. (1972). Nānā I Ke Kumu—Look to the source (Vol. I). Hui Hānai.
Pukui, M. K., Haertig, E. W., & Lee, C. A. (1979). Nānā I Ke Kumu—Look to the source (Vol. II). Queen Liliuokalani Children’s Center.
Rezentes, W. C., III. (1996). Ka Lama Kukui–Hawaiian psychology: An introduction. ‘A’ali’i Books.
Richardson, J. D. (1908). A compilation of the messages and papers of the presidents: 1789–1908 (Vol. 11) and index (1908). Bureau of National Literature and Art.
Sai, D. K. (2013). Ua mau ke ea–Sovereignty endures: An overview of the political and legal history of the Hawaiian Islands (2nd ed.). Pū‘ā Foundation.
Shook, V. E. (2002). Ho’oponopono: Contemporary uses of a Hawaiian problem-solving process. University of Hawai‘i Press.
Trask, H. -K. (1999). From a Native daughter: Colonialism and sovereignty in Hawai‘i (Rev. ed.). University of Hawai‘i Press.
Van Dyke, J. M., Morgan, J. R., & Gurish, J. (1988). The exclusive economic zone of the Northwestern Hawaiian Islands: When do uninhabited islands generate an EEZ? San Diego Law Review, 25, 425–494.
Williams, I. L. (2019). Does Native Hawaiian culture-based treatment deserve more funding than treatment-as-usual? Journal of Ethnic & Cultural Diversity in Social Work, 28, 246–261. https://doi.org/10.1080/15313204.2018.1555500
Williams, I. L., Laenui, P., Makini, G. K., Jr., & Rezentes, W. C., III. (2019). Native Hawaiian culturally based treatment: Considerations and clarifications. Journal of Ethnicity in Substance Abuse. Advance online publication. https://doi.org/10.1080/15332640.2019.1679315.
Williams, I. L., Makini, G. K., Jr., & Rezentes, W. C., III. (2021). Indigenous Hawaiian psychoactive drug use before European contact, and after 1778. Journal of Psychoactive Drugs, 53(2), 111–126. https://doi.org/10.1080/02791072.2020.1833114
Williams, I. L., Rezentes, W. C., III, Nunes, A., & Makini, G. K., Jr. (in press). Native Hawaiian healing to treat substance misuse: History through the looking glass. Journal of Social Work Practice in the Addictions. https://doi.org/10.1080/1533256X.2021.1933844
Williams, M. T., Davis, A. K., Xin, Y., Sepeda, N. D., Grigas, P. C., Sinnott, S., & Haeny, A. M. (2021). People of color in North America report improvements in racial trauma and mental health symptoms following psychedelic experiences. Drugs: Education, Prevention and Policy, 28(3), 215–226. https://doi.org/10.1080/09687637.2020.1854688
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Laenui, P., Williams, I. (2022). Hawaiian National Re-emergence from US Colonization: Community Strength, Mental Health, and Traditions. In: Rich, G.J., Ramkumar, N.A. (eds) Psychology in Oceania and the Caribbean. International and Cultural Psychology. Springer, Cham. https://doi.org/10.1007/978-3-030-87763-7_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-87763-7_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-87762-0
Online ISBN: 978-3-030-87763-7
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)