
Abstract
Treatment of head and neck cancers is associated with an increased risk for hyposalivation and xerostomia. Salivary glands are often unavoidable, indirect targets during radiation treatment and are damaged in a cumulative radiation dose-related fashion resulting in partial to total permanent loss of function of salivary gland tissue and patients experiencing xerostomia. Salivary gland hypofunction and xerostomia lead to negative impacts on patients’ oral environment, function, and quality of life. Treatment remedies have limited effectiveness and may be accompanied by high financial burdens. This chapter represents information regarding the prevalence, severity, and management strategies for salivary gland hypofunction and xerostomia induced by cancer therapies with particular focus on effects of radiation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
7.1 Introduction
Due to the superficial location of the salivary glands in the head and neck, salivary glands are often damaged when in the radiation treatment field for head and neck cancer. Radiation doses as low as 10 Gy have been shown to cause partial damage to the glands. The lower limit dose for total and permanent damage varies by study, but general consensus agrees that doses 60 Gy and above typically cause permanent damage to the glands. The amount of damage to the salivary glands is impacted by the cumulative amount of radiation to the area. When salivary glands are damaged, a cascade of side effects may occur in the mouth secondary to hyposalivation and resultant xerostomia. Xerostomia is a common complaint from head and neck cancer patients with a reported 93% prevalence in patients currently undergoing radiation therapy and 74–85% following radiation therapy. Other side effects of hyposalivation secondary to radiation treatment include increased bacteriogenic flora, reduced buffering capacity, increased dental caries and periodontal disease rate, and increased risk for oral infections and ulcerative lesions. Additionally, patients may experience pain, difficulty eating or speaking, and reduced quality of life. Management strategies for hyposalivation and xerostomia have been aimed at salivary gland protection, residual salivary gland stimulation, and symptomatic relief with the use of salivary substitutes and mucosal lubrication. Current management strategies are often limited by low effectiveness, high risk/benefit ratios, and/or high cost burden to patients.
7.2 Normal Salivary Gland Function and Role of Saliva
Saliva has several functions in the mouth including lubrication of the mucosal surfaces, mobilization of food debris, formation of food bolus, neutralization of oral environment acidity, remineralization of teeth, and assistance with swallowing and speech. The three major salivary glands (submandibular, parotid, and sublingual) are responsible for 90% of saliva production, while the minor salivary glands contribute the remaining 10%. The submandibular gland contains both mucous and serous glands which generate a mixed mucin-rich and protein-rich saliva, respectively. In contrast, the sublingual gland is composed mainly of mucous cells and contributes mucous-rich saliva, while the parotid gland is composed of mainly serous glands and contributes serous, protein-rich saliva. In normal conditions, the submandibular glands contribute 66% of the saliva at rest which is often referred to as the unstimulated saliva. During stimulated conditions (i.e., during mastication), the parotid gland contributes about 50% of the total saliva production. While the minor salivary glands contribute much less volume of saliva, their proper functioning is important for lubrication of the mucosal surfaces. Damage to the salivary glands leads to hyposalivation and xerostomia which often leads to detrimental consequences for the patients’ oral environment and quality of life.
7.2.1 Hyposalivation and Xerostomia
Hyposalivation represents a pathologically low state of salivary secretion and is often defined as an unstimulated flow rate of less than or equal to 0.1 mL saliva/min and/or a stimulated saliva flow rate of less than or equal to 0.7 mL/min. Hyposalivation often leads to xerostomia, the subjective feeling of oral dryness, which may occur when a patient experiences a 45–50% reduction in resting salivary production. Hyposalivation puts patients at risk for increased infections, tooth decay, periodontal disease, mucosal trauma, oral pain/discomfort, difficulty swallowing and speaking, and reduced quality of life. Notably, patients may express feelings of oral dryness without observed oral dryness or measurable hyposalivation which may reflect changes in saliva composition.
7.3 Impact of Cancer Therapy on Salivary Gland Function
7.3.1 Radiation Therapy
The majority of patients receiving radiation for head and neck cancer will experience hyposalivation and resultant xerostomia of at least a mild-moderate severity during and following radiation therapy, with a small percentage of patients reporting severe xerostomia late following radiation treatment. The extent of salivary gland damage and xerostomia is related to the cumulative dose of radiation received by the salivary gland tissue and the volume of salivary gland tissue included in the radiation field. The highest prevalence of salivary hypofunction and xerostomia may be anticipated when all salivary glands are included in the radiation field (i.e., for treatment of nasopharyngeal carcinoma) with low chance of salivary gland recovery if doses reach 60 Gy. The long-term prevalence and severity of hyposalivation and xerostomia may be reduced in patients treated unilaterally, at reduced radiation doses, and/or by sparing normal tissue from radiation fields through the use of 3D conformal radiation therapy or intensity-modulated radiation therapy (IMRT).
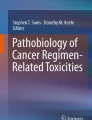
A systematic review by Jensen SB et al. found the prevalence of xerostomia from a pooled data of patients undergoing conventional radiotherapy, 3D conformational radiotherapy, and/or intensity-modulated therapy of the head and neck to be 93% during radiation with a slight reduction (73.6–85.3%) 1 month to over 2 years posttreatment. The severity of xerostomia as measured by a visual analog scale (VAS) and grades 1–4 (4 being most severe) revealed highest prevalence of grade 2 xerostomia during radiation treatment to 6 months postradiation, grade 1 xerostomia 6 months to 1 year posttreatment, and a small number of patients experiencing grade 3 and 4 xerostomia late after radiation therapy. Correlating with the timing and severity of xerostomia reported, assessment of salivary flows revealed significant decline in both unstimulated and stimulated flows during radiation treatment, declining further 1–3 months postradiation treatment and slightly improving after 6 months to 2 years after completion of radiation (Fig. 7.1). Studies revealed that stimulated flow rates were consistently higher than unstimulated flow rates, suggesting a residual capacity of salivary gland tissue and role of salivary gland stimulants for management of radiation-induced hyposalivation and xerostomia (Fig. 7.2).

Pooled and weighted prevalences of xerostomia induced by head and neck radiotherapy. RT radiotherapy, Conv. conventional, 3D-CRT three-dimensional conformal RT, IMRT intensity-modulated RT, Tx treatment, Mo. months, Yrs. years . (Reprinted by permission from Springer Nature: Jensen SB, Pedersen AM, Vissink A, Andersen E, Brown CG, Davies AN et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support Care Cancer. 2010;18(8):1039–60)

Pooled and weighted data of unstimulated and stimulated whole saliva flow changes during and after head and neck radiotherapy. Tx treatment, RT radiotherapy, Mo. months, Yrs. years, Unstim. unstimulated, Stim. stimulated. (Reprinted by permission from Springer Nature: Jensen SB, Pedersen AM, Vissink A, Andersen E, Brown CG, Davies AN et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support Care Cancer. 2010;18(8):1039–60)
7.3.2 Chemotherapy
There is insufficient data regarding the effects of chemotherapy agents on salivary gland tissue. Several chemotherapy agents are available which have varying mechanisms of action and impacts on tissue. In comparison to radiation therapy, chemotherapy and immunotherapy may induce salivary gland hypofunction to a lesser degree. Additionally, the effects of chemotherapy and immunotherapy on salivary gland tissue are more likely to be temporary and reversible.
7.3.3 Radioactive Iodine Treatment
Patients with thyroid cancer treated with radioactive iodine may experience hyposalivation and xerostomia due to the accumulation of radioactive iodine in salivary gland tissue with approximately 30–35% prevalence of dry mouth and a 33% reduction of salivary flow after therapy.
7.3.4 Conditioning Total Body Irradiation/Chemotherapy and Hematopoietic Stem Cell Transplantation
A prospective study by Laaksonen M et al. assessed xerostomia and salivary function pre- and post-hematopoietic stem cell transplantation (HSCT). Defining hyposalivation as stimulated whole salivary flow <0.7 mL/min, the prevalence of patients with hyposalivation was highest 6 months post-HSCT (53%) and dropped off to 26% by 24 months post-HSCT. A prospective study of 44 long-term survivors and their donors (median survival = 17.5 years; range = 11–26 years) post-HSCT demonstrated that 53% of patients compared to only 7% of donors reported dry mouth.
7.4 Management of Hyposalivation and Xerostomia
7.4.1 Prevention Strategies
7.4.1.1 Limiting Radiation Doses
While there is variation in the proposed minimum threshold amount of radiation that results in permanent damage to salivary gland tissue, there is general agreement in the literature that radiation doses >60 Gy result in permanent damage. Studies suggest that mean doses ranging from <26 to <40 Gy may result in preservation of some parotid gland function, while mean doses <39 Gy may result in potential preservation of submandibular gland function. Treatments aimed at selective targeting of cancerous cells, such as with IMRT, may assist in limiting cumulative radiation dose to normal tissue by better isolation of target tissue.
7.4.1.2 Intensity-Modulated Radiation Therapy (IMRT)
When available, IMRT is a currently recommended standard treatment for head and neck cancer patients aimed at treatment of disease while preventing xerostomia and salivary gland hypofunction. IMRT uses multiple beams with varying intensity profiles geared at targeting cancer cells while minimizing radiation to normal tissue, such as the salivary glands. As a result, salivary gland tissue may receive less cumulative dose of radiation, and function may be spared. Studies reveal that parotid-sparing IMRT may serve to reduce the prevalence and severity of parotid hyposalivation with resultant reduction in patient experience of xerostomia when patients were followed for more than 1 year. In contrast to patients treated with conventional radiation therapy, patients treated with IMRT showed better improvement of salivary flows over time postradiation indicating that these patients have higher levels of active residual gland remaining posttreatment. Additionally, patients with early-stage disease and unilateral involvement may have sparing of the contralateral submandibular gland with the use of IMRT, though practices are limited to select cases that do not require bilateral radiation. For patients that have advanced disease requiring bilateral radiation and/or radiation to critical lymphatics, IMRT may not be able to spare the function of submandibular gland tissue which results in reduction in unstimulated flow and altered saliva composition. In a recent study by Lalla et al., preliminary results for a larger prospective study of 577 head and neck cancer patients indicated stimulated whole salivary flow declined significantly from 1.09 mL/min pre-RT to 0.47 mL/min 6 months post-RT in head and neck cancer patients treated with IMRT or newer RT modalities. The mean stimulated whole salivary flow at 6 months post-RT for the different RT treatments included 3D conformal RT = 0.38 mL/min, IMRT with or without image guidance = 0.54–0.56 mL/min, and proton therapy = 0.80 mL/min.
7.4.1.3 Amifostine
Amifostine is a radical scavenger that has been shown in rat models to preferably accumulate in salivary gland tissue and have a radioprotective effect. A recent Cochrane Review concluded that there is low-quality evidence to support the use of amifostine to reduce xerostomia at the end of RT and up to 3 months post-RT. Limitations with the use of amifostine, clinically, include possible coincident radioprotection on tumor cells and severe adverse effects including hypotension, nausea, vomiting, and allergy particularly when administered intravenously.
7.4.2 Secretory Stimulants: Muscarinic Agonists
Both pilocarpine and cevimeline are parasympathomimetics that can improve salivary flow and decrease xerostomia. Pilocarpine has been approved for the treatment of radiation-induced xerostomia in several countries. The use of parasympathomimetics is dependent on residual capacity of salivary gland tissue function as the medication works by stimulating the tissue to secrete saliva via targeting agonism of muscarinic receptors on the cell surface. Pilocarpine is commonly prescribed in dosage of 5 mg four times per day with maximum recommended dose being 10 mg per dose and up to 30 mg daily. Cevimeline (30 mg tabs) can be prescribed up to three times per day. Literature data suggests that 50% of patients will benefit from oral pilocarpine postradiation with optimum benefits occurring after 8–12 weeks of use. Topical use of pilocarpine in the forms of pastilles, lozenges, and mouthwashes has also shown promise for treatment of postradiation xerostomia. Benefits of parasympathomimetics are use-dependent and observed improvements in hyposalivation and xerostomia decline with cessation of the medication. Side effects of parasympathomimetics include sweating, headache, increased urinary frequency, vasodilatation, dizziness, dyspepsia, lacrimation, and nausea, and the medications are contraindicated for use in patients with narrow-angle glaucoma, uncontrolled asthma, and gastric ulcers. Close monitoring is required for patients with cardiovascular disease and pulmonary disease. Potential medication interactions should be reviewed prior to use.
7.4.3 Gustatory and Masticatory Salivary Stimulants
For patients that maintain residual function of salivary gland tissue, the use of sugar-free candies and lozenges may increase whole saliva and improve oral dryness postradiation; however, acidic lozenges increase risk of hard tissue damage (i.e., teeth), and care should be taken with use. Masticatory stimulation with the use of gum is another approach to manage dry mouth, but poses an increased risk for development of myalgia and temporomandibular disorder. Use of gum may be limited if such symptoms develop. Residual salivary gland function is required in order for gustatory and masticatory approaches to be successful.
7.4.4 Saliva Substitutes/Mucosal Lubricants
Saliva substitutes and mucosal lubricants are often used for symptomatic relief of salivary hypostimulation and xerostomia. Products are available in various forms such a mouthwashes, sprays, and gels. These substitutes are composed of various constituents that serve to resemble the glycoprotein and antimicrobial components of saliva such as carboxymethylcellulose and mucin. Saliva substitutes are most beneficial when used in patients with severe xerostomia compared to mild-moderate xerostomia. Higher viscosity products such as gels may provide better, longer lasting nighttime relief, while less viscous substitutes may be preferred during the day. Due to the substitutes’ limitations including short duration of relief and cumulative cost burden over time, patients may prefer frequent use of water. A Cochrane Review from 2011 reported that there is insufficient evidence that saliva substitutes are better or worse than placebos. Thus, recommendations for use may be made according to individual patient preference and perceived benefit.
7.4.5 Alternative Management Options
7.4.5.1 Surgical Transfer of Submandibular Gland/Seikaly-Jha Procedure
Surgical transfer of a submandibular gland into the submental space may be considered for patients treated with radiation that does not include the submental space. A recent phase II study of 40 patients receiving submandibular gland transfer demonstrated good results in the rate of dry mouth and loss of salivary flow from baseline. The technique has been shown to preserve some submandibular function and reduce radiation-induced xerostomia. Preliminary data is promising, though careful considerations for case selection, cost, and surgical risks must be considered.
7.4.5.2 Acupuncture
In patients that have some residual salivary gland function, preliminary research reveals that acupuncture may have a role in improving salivary flow rates, reducing xerostomia, and improving patient quality of life. A systematic review of three randomized controlled trials indicated an improvement of xerostomia compared to control groups and some improvement in salivary flow. Additional studies have reported improvements in xerostomia (55% decrease in patients undergoing IMRT) with sustained effects lasting up to 3 years. The use of acupuncture may be beneficial with low risks of side effects, though more information is needed to substantiate the preliminary research findings.
7.4.5.3 Hyperbaric Oxygen (HBO) Treatment
A cohort of 80 head and neck cancer patients treated with HBO therapy post-radiotherapy demonstrated improvement in dry mouth complaints and a slight increase in unstimulated and stimulated salivary flows. These patients were treated for the prevention or treatment of osteoradionecrosis or soft tissue radiation injury. Two earlier reports reviewed revealed possible decrease in xerostomia when patients were being treated with HBO perioperatively for prevention of osteoradionecrosis of the jaw. Logistics, cost, and side effects will need to be considered before recommending HBO therapy solely for the management of xerostomia and salivary hypofunction.
7.5 Discussion and Conclusion
Salivary gland hypofunction and hyposalivation are common problems for patients being treated for head and neck cancer and lead to deleterious impacts on patients’ oral health and quality of life. Prevention and treatment strategies for hyposalivation and xerostomia are limited by low and temporary efficacy, potentially high risk/benefit ratios, and high cumulative cost burdens. To date, the most commonly recommended treatment strategies are prevention of salivary damage via radiation dose-reduction methods such as IMRT with a combination of patient behavioral modifications including increased hydration and use of salivary substitutes. More research needs to be done in order to improve prevention and treatment of hyposalivation and xerostomia in a more effective, lower cost manner.
Bibliography
Deasy JO, Moiseenko V, Marks L, Chao KS, Nam J, Eisbruch A. Radiotherapy dose-volume effects on salivary gland function. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):S58–63. https://doi.org/10.1016/j.ijrobp.2009.06.090.
Jensen SB, Pedersen AM, Vissink A, Andersen E, Brown CG, Davies AN, et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support Care Cancer. 2010;18(8):1039–60.
Pedersen AM, Bardow A, Jensen SB, Nauntofte B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis. 2002;8(3):117–29.
Dawes C, Ong BY. Circadian rhythms in the flow rate and proportional contribution of parotid to whole saliva volume in man. Arch Oral Biol. 1973;18(9):1145–53.
Dawes C, Wood CM. The contribution of oral minor mucous gland secretions to the volume of whole saliva in man. Arch Oral Biol. 1973;18(3):337–42.
Sreebny LM. Saliva in health and disease: an appraisal and update. Int Dent J. 2000;50(3):140–61.
Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66(Special Issue):648–53.
Yeh SA, Huang YJ. Dose escalation for patients with locally advanced nasopharyngeal carcinoma treated with radiotherapy alone. Am J Clin Oncol. 2007;30(4):401–5. https://doi.org/10.1097/COC.0b013e31803377b3.
Franzen L, Funegard U, Ericson T, Henriksson R. Parotid gland function during and following radiotherapy of malignancies in the head and neck. A consecutive study of salivary flow and patient discomfort. Eur J Cancer. 1992;28(2–3):457–62.
Jensen SB, Pedersen AM, Vissink A, Andersen E, Brown CG, Davies AN, et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: management strategies and economic impact. Support Care Cancer. 2010;18(8):1061–79.
Jeong SY, Kim HW, Lee SW, Ahn BC, Lee J. Salivary gland function 5 years after radioactive iodine ablation in patients with differentiated thyroid cancer: direct comparison of pre- and postablation scintigraphies and their relation to xerostomia symptoms. Thyroid. 2013;23(5):609–16. https://doi.org/10.1089/thy.2012.0106.
Soo Roh S, Wook Kim D, Jin Baek H. Association of xerostomia and ultrasonographic features of the major salivary glands after radioactive iodine ablation for papillary thyroid carcinoma. AJR Am J Roentgenol. 2016;207(5):1077–81. https://doi.org/10.2214/AJR.15.15776.
Laaksonen M, Ramseier AM, Rovo A, Jensen SB, Raber-Durlacher JE, Zitzmann NU, et al. Longitudinal assessment of hematopoietic stem cell transplantation and hyposalivation. J Dent Res. 2011;90(10):1177–82. https://doi.org/10.1177/0022034511414156.
Daikeler T, Mauramo M, Rovo A, Stern M, Halter J, Buser A, et al. Sicca symptoms and their impact on quality of life among very long-term survivors after hematopoietic SCT. Bone Marrow Transplant. 2013;48(7):988–93. https://doi.org/10.1038/bmt.2012.260.
Chao KS, Deasy JO, Markman J, Haynie J, Perez CA, Purdy JA, et al. A prospective study of salivary function sparing in patients with head-and-neck cancers receiving intensity-modulated or three-dimensional radiation therapy: initial results. Int J Radiat Oncol Biol Phys. 2001;49(4):907–16. S0360-3016(00)01441-3 [pii].
Eisbruch A, Ten Haken RK, Kim HM, Marsh LH, Ship JA. Dose, volume, and function relationships in parotid salivary glands following conformal and intensity-modulated irradiation of head and neck cancer. Int J Radiat Oncol Biol Phys. 1999;45(3):577–87.
Blanco AI, Chao KS, El Naqa I, Franklin GE, Zakarian K, Vicic M, et al. Dose-volume modeling of salivary function in patients with head-and-neck cancer receiving radiotherapy. Int J Radiat Oncol Biol Phys. 2005;62(4):1055–69. https://doi.org/10.1016/j.ijrobp.2004.12.076.
Saarilahti K, Kouri M, Collan J, Hamalainen T, Atula T, Joensuu H, et al. Intensity modulated radiotherapy for head and neck cancer: evidence for preserved salivary gland function. Radiother Oncol. 2005;74(3):251–8. https://doi.org/10.1016/j.radonc.2004.11.004.
Li Y, Taylor JM, Ten Haken RK, Eisbruch A. The impact of dose on parotid salivary recovery in head and neck cancer patients treated with radiation therapy. Int J Radiat Oncol Biol Phys. 2007;67(3):660–9. S0360-3016(06)02988-9 [pii]. https://doi.org/10.1016/j.ijrobp.2006.09.021.
Munter MW, Karger CP, Hoffner SG, Hof H, Thilmann C, Rudat V, et al. Evaluation of salivary gland function after treatment of head-and-neck tumors with intensity-modulated radiotherapy by quantitative pertechnetate scintigraphy. Int J Radiat Oncol Biol Phys. 2004;58(1):175–84.
Liu WS, Lee SP, Lee JK, Su MC, Chen GD, Lee HS, et al. Factors influencing the parotid function in nasopharyngeal carcinoma treated with parotid-sparing radiotherapy. Jpn J Clin Oncol. 2006;36(10):626–31. https://doi.org/10.1093/jjco/hyl098.
Roesink JM, Moerland MA, Battermann JJ, Hordijk GJ, Terhaard CH. Quantitative dose-volume response analysis of changes in parotid gland function after radiotherapy in the head-and-neck region. Int J Radiat Oncol Biol Phys. 2001;51(4):938–46.
Scrimger R. Salivary gland sparing in the treatment of head and neck cancer. Expert Rev Anticancer Ther. 2011;11(9):1437–48. https://doi.org/10.1586/era.11.101.
Chao KS, Majhail N, Huang CJ, Simpson JR, Perez CA, Haughey B, et al. Intensity-modulated radiation therapy reduces late salivary toxicity without compromising tumor control in patients with oropharyngeal carcinoma: a comparison with conventional techniques. Radiother Oncol. 2001;61(3):275–80.
Wang ZH, Yan C, Zhang ZY, Zhang CP, Hu HS, Tu WY, et al. Impact of salivary gland dosimetry on post-IMRT recovery of saliva output and xerostomia grade for head-and-neck cancer patients treated with or without contralateral submandibular gland sparing: a longitudinal study. Int J Radiat Oncol Biol Phys. 2011;81(5):1479–87. https://doi.org/10.1016/j.ijrobp.2010.07.1990.
Saarilahti K, Kouri M, Collan J, Kangasmaki A, Atula T, Joensuu H, et al. Sparing of the submandibular glands by intensity modulated radiotherapy in the treatment of head and neck cancer. Radiother Oncol. 2006;78(3):270–5. https://doi.org/10.1016/j.radonc.2006.02.017.
Lalla RV, Treister N, Sollecito T, Schmidt B, Patton LL, Mohammadi K, et al. Oral complications at 6 months after radiation therapy for head and neck cancer. Oral Dis. 2017; https://doi.org/10.1111/odi.12710.
Brizel DM, Wasserman TH, Henke M, Strnad V, Rudat V, Monnier A, et al. Phase III randomized trial of amifostine as a radioprotector in head and neck cancer. J Clin Oncol. 2000;18(19):3339–45.
Wasserman TH, Brizel DM, Henke M, Monnier A, Eschwege F, Sauer R, et al. Influence of intravenous amifostine on xerostomia, tumor control, and survival after radiotherapy for head-and-neck cancer: 2-year follow-up of a prospective, randomized, phase III trial. Int J Radiat Oncol Biol Phys. 2005;63(4):985–90. https://doi.org/10.1016/j.ijrobp.2005.07.966.
Hensley ML, Hagerty KL, Kewalramani T, Green DM, Meropol NJ, Wasserman TH, et al. American Society of Clinical Oncology 2008 clinical practice guideline update: use of chemotherapy and radiation therapy protectants. J Clin Oncol. 2009;27(1):127–45. https://doi.org/10.1200/JCO.2008.17.2627.
Brizel DM, Overgaard J. Does amifostine have a role in chemoradiation treatment? Lancet Oncol. 2003;4(6):378–81.
Riley P, Glenny AM, Hua F, Worthington HV. Pharmacological interventions for preventing dry mouth and salivary gland dysfunction following radiotherapy. Cochrane Database Syst Rev. 2017;7:CD012744. https://doi.org/10.1002/14651858.CD012744.
Takahashi I, Nagai T, Miyaishi K, Maehara Y, Niibe H. Clinical study of the radioprotective effects of Amifostine (YM-08310, WR-2721) on chronic radiation injury. Int J Radiat Oncol Biol Phys. 1986;12(6):935–8.
Ozsahin M, Betz M, Matzinger O, Bron L, Luthi F, Pasche P, et al. Feasibility and efficacy of subcutaneous amifostine therapy in patients with head and neck cancer treated with curative accelerated concomitant-boost radiation therapy. Arch Otolaryngol Head Neck Surg. 2006;132(2):141–5. https://doi.org/10.1001/archotol.132.2.141.
Law A, Kennedy T, Pellitteri P, Wood C, Christie D, Yumen O. Efficacy and safety of subcutaneous amifostine in minimizing radiation-induced toxicities in patients receiving combined-modality treatment for squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys. 2007;69(5):1361–8. https://doi.org/10.1016/j.ijrobp.2007.05.052.
Chambers MS, Posner M, Jones CU, Biel MA, Hodge KM, Vitti R, et al. Cevimeline for the treatment of postirradiation xerostomia in patients with head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;68(4):1102–9. S0360-3016(07)00149-6 [pii]. https://doi.org/10.1016/j.ijrobp.2007.01.019.
Chambers MS, Jones CU, Biel MA, Weber RS, Hodge KM, Chen Y, et al. Open-label, long-term safety study of cevimeline in the treatment of postirradiation xerostomia. Int J Radiat Oncol Biol Phys. 2007;69(5):1369–76. https://doi.org/10.1016/j.ijrobp.2007.05.024.
Jham BC, Teixeira IV, Aboud CG, Carvalho AL, Coelho Mde M, Freire AR. A randomized phase III prospective trial of bethanechol to prevent radiotherapy-induced salivary gland damage in patients with head and neck cancer. Oral Oncol. 2007;43(2):137–42. https://doi.org/10.1016/j.oraloncology.2006.01.013.
Mercadante V, Al Hamad A, Lodi G, Porter S, Fedele S. Interventions for the management of radiotherapy-induced xerostomia and hyposalivation: a systematic review and meta-analysis. Oral Oncol. 2017;66:64–74. https://doi.org/10.1016/j.oraloncology.2016.12.031.
Wiseman LR, Faulds D. Oral pilocarpine: a review of its pharmacological properties and clinical potential in xerostomia. Drugs. 1995;49(1):143–56.
Fox PC, Atkinson JC, Macynski AA, Wolff A, Kung DS, Valdez IH, et al. Pilocarpine treatment of salivary gland hypofunction and dry mouth (xerostomia). Arch Intern Med. 1991;151(6):1149–52.
Johnson JT, Ferretti GA, Nethery WJ, Valdez IH, Fox PC, Ng D, et al. Oral pilocarpine for post-irradiation xerostomia in patients with head and neck cancer. N Engl J Med. 1993;329(6):390–5.
LeVeque FG, Montgomery M, Potter D, Zimmer MB, Rieke JW, Steiger BW, et al. A multicenter, randomized, double-blind, placebo-controlled, dose-titration study of oral pilocarpine for treatment of radiation-induced xerostomia in head and neck cancer patients. J Clin Oncol. 1993;11(6):1124–31.
Davies AN, Singer J. A comparison of artificial saliva and pilocarpine in radiation-induced xerostomia. J Laryngol Otol. 1994;108(8):663–5.
Hamlar DD, Schuller DE, Gahbauer RA, Buerki RA, Staubus AE, Hall J, et al. Determination of the efficacy of topical oral pilocarpine for postirradiation xerostomia in patients with head and neck carcinoma. Laryngoscope. 1996;106(8):972–6.
Taweechaisupapong S, Pesee M, Aromdee C, Laopaiboon M, Khunkitti W. Efficacy of pilocarpine lozenge for post-radiation xerostomia in patients with head and neck cancer. Aust Dent J. 2006;51(4):333–7.
Bernardi R, Perin C, Becker FL, Ramos GZ, Gheno GZ, Lopes LR, et al. Effect of pilocarpine mouthwash on salivary flow. Braz J Med Biol Res. 2002;35(1):105–10.
Daniels TE, Wu AJ. Xerostomia—clinical evaluation and treatment in general practice. J Calif Dent Assoc. 2000;28(12):933–41.
Senahayake F, Piggott K, Hamilton-Miller JM. A pilot study of Salix SST (saliva-stimulating lozenges) in post-irradiation xerostomia. Curr Med Res Opin. 1998;14(3):155–9. https://doi.org/10.1185/03007999809113355.
Jensdottir T, Nauntofte B, Buchwald C, Hansen HS, Bardow A. Effects of sucking acidic candies on saliva in unilaterally irradiated pharyngeal cancer patients. Oral Oncol. 2006;42(3):317–22. https://doi.org/10.1016/j.oraloncology.2005.08.009.
S-Gravenmade EJ, Roukema PA, Panders AK. The effect of mucin-containing artificial saliva on severe xerostomia. Int J Oral Surg. 1974;3(6):435–9.
Regelink G, Vissink A, Reintsema H, Nauta JM. Efficacy of a synthetic polymer saliva substitute in reducing oral complaints of patients suffering from irradiation-induced xerostomia. Quintessence Int. 1998;29(6):383–8.
Epstein JB, Stevenson-Moore P. A clinical comparative trial of saliva substitutes in radiation-induced salivary gland hypofunction. Spec Care Dentist. 1992;12(1):21–3.
Furness S, Worthington HV, Bryan G, Birchenough S, McMillan R. Interventions for the management of dry mouth: topical therapies. Cochrane Database Syst Rev. 2011;12:CD008934. https://doi.org/10.1002/14651858.CD008934.pub2.
Scrimger RA, Seikaly H, Vos LJ, Harris J, O’Connell D, Ghosh S, et al. Combination of submandibular salivary gland transfer and intensity-modulated radiotherapy to reduce dryness of mouth (xerostomia) in patients with head and neck cancer. Head Neck. 2018; https://doi.org/10.1002/hed.25339.
Jha N, Seikaly H, Harris J, Williams D, Liu R, McGaw T, et al. Prevention of radiation induced xerostomia by surgical transfer of submandibular salivary gland into the submental space. Radiother Oncol. 2003;66(3):283–9.
Pathak KA, Bhalavat RL, Mistry RC, Deshpande MS, Bhalla V, Desai SB, et al. Upfront submandibular salivary gland transfer in pharyngeal cancers. Oral Oncol. 2004;40(9):960–3. https://doi.org/10.1016/j.oraloncology.2004.04.016.
Seikaly H, Jha N, Harris JR, Barnaby P, Liu R, Williams D, et al. Long-term outcomes of submandibular gland transfer for prevention of postradiation xerostomia. Arch Otolaryngol Head Neck Surg. 2004;130(8):956–61. https://doi.org/10.1001/archotol.130.8.956.
Al-Qahtani K, Hier MP, Sultanum K, Black MJ. The role of submandibular salivary gland transfer in preventing xerostomia in the chemoradiotherapy patient. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101(6):753–6. https://doi.org/10.1016/j.tripleo.2005.12.017.
Johnstone PA, Peng YP, May BC, Inouye WS, Niemtzow RC. Acupuncture for pilocarpine-resistant xerostomia following radiotherapy for head and neck malignancies. Int J Radiat Oncol Biol Phys. 2001;50(2):353–7.
Blom M, Dawidson I, Fernberg JO, Johnson G, Angmar-Mansson B. Acupuncture treatment of patients with radiation-induced xerostomia. Eur J Cancer B Oral Oncol. 1996;32B(3):182–90.
Blom M, Lundeberg T. Long-term follow-up of patients treated with acupuncture for xerostomia and the influence of additional treatment. Oral Dis. 2000;6(1):15–24.
Cho JH, Chung WK, Kang W, Choi SM, Cho CK, Son CG. Manual acupuncture improved quality of life in cancer patients with radiation-induced xerostomia. J Altern Complement Med. 2008;14(5):523–6. https://doi.org/10.1089/acm.2007.0793.
Zhuang L, Yang Z, Zeng X, Zhua X, Chen Z, Liu L, et al. The preventive and therapeutic effect of acupuncture for radiation-induced xerostomia in patients with head and neck cancer: a systematic review. Integr Cancer Ther. 2013;12(3):197–205. https://doi.org/10.1177/1534735412451321.
Forner L, Hyldegaard O, von Brockdorff AS, Specht L, Andersen E, Jansen EC, et al. Does hyperbaric oxygen treatment have the potential to increase salivary flow rate and reduce xerostomia in previously irradiated head and neck cancer patients? A pilot study. Oral Oncol. 2011;47(6):546–51. https://doi.org/10.1016/j.oraloncology.2011.03.021.
Gerlach NL, Barkhuysen R, Kaanders JH, Janssens GO, Sterk W, Merkx MA. The effect of hyperbaric oxygen therapy on quality of life in oral and oropharyngeal cancer patients treated with radiotherapy. Int J Oral Maxillofac Surg. 2008;37(3):255–9. https://doi.org/10.1016/j.ijom.2007.11.013.
Harding SA, Hodder SC, Courtney DJ, Bryson PJ. Impact of perioperative hyperbaric oxygen therapy on the quality of life of maxillofacial patients who undergo surgery in irradiated fields. Int J Oral Maxillofac Surg. 2008;37(7):617–24. https://doi.org/10.1016/j.ijom.2008.04.004.
Sasportas LS, Hosford DN, Sodini MA, Waters DJ, Zambricki EA, Barral JK, et al. Cost-effectiveness landscape analysis of treatments addressing xerostomia in patients receiving head and neck radiation therapy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116(1):e37–51. https://doi.org/10.1016/j.oooo.2013.02.017.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Rigert, J., Brennan, M.T. (2022). Salivary Gland Diseases, Hyposalivation, and Xerostomia in Head and Neck Cancer Patients. In: Nair, R. (eds) Orofacial Supportive Care in Cancer . Springer, Cham. https://doi.org/10.1007/978-3-030-86510-8_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-86510-8_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-86509-2
Online ISBN: 978-3-030-86510-8
eBook Packages: MedicineMedicine (R0)