
Abstract
By conventional definition, the lower gastrointestinal (GI) tract includes the appendix, entire colon, and anus. Diseases involving these organs are traditionally classified into nonneoplastic and neoplastic categories. Clinical application of immunohistochemistry (IHC) is most useful in the diagnosis of neoplastic lesions, with a few exceptions such as to identify of viral pathogens in infectious colitis and to facilitate diagnosis of Hirschsprung’s disease. For diagnosis of neoplasm, IHC is particularly useful in several aspects: (1) to help confirm glandular dysplasia associated with inflammatory bowel disease (IBD) and to differentiate it from sporadic adenoma in challenging cases; (2) to confirm diagnosis and grade of neuroendocrine tumors; (3) to confirm diagnosis of a poorly differentiated or undifferentiated colonic adenocarcinoma variant, such as medullary carcinoma; (4) to help differentiate commonly encountered benign and malignant primary mesenchymal tumors; (5) to differentiate primary carcinomas from various morphological mimickers from other organ systems, such as carcinomas of the gynecological and genitourinary systems; and, (6) to initiate Lynch syndrome screening in patients with diagnosed colorectal cancer.
In this chapter, we provide an overview of the most useful markers in the diagnosis of lower GI tract diseases, albeit many of them are shared with the upper GI chapter. The content is organized into 19 diagnostic issues frequently encountered in daily practice. The use of both individual markers and other relevant markers to form effective panels to address specific diagnostic challenges are illustrated in a tabular format. Concise notes with representative microscopic pictures are included whenever deemed necessary.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Colorectal adenocarcinoma
- Anal gland adenocarcinoma
- Goblet cell carcinoid
- Mixed goblet cell carcinoid/adenocarcinoma
- Hirschsprung’s disease
- Neuroendocrine tumor
- Medullary carcinoma of the colon
- Mucinous tumor of appendix
- Inflammatory bowel disease (IBD)
- Dysplasia
- Anal Paget’s disease
- Anal squamous cell carcinoma
- Beta-catenin
- CDH17
- SATB2
- CK20
- CK7
- CDX2
- MUC1
- MUC2
- SOX2
- p53
- p504S
- GLUT 1
- Claudin 1
- Calretinin
- Neuron specific enolase (NSE)
- Acetylcholine esterase
- Mismatch repair (MMR) proteins
- Microsatellite instability (MSI)
Frequently Asked Questions
Overview
-
1.
Staining patterns of commonly used markers in normal colonic mucosa (Table 29.1)
-
2.
Staining patterns of commonly used markers in usual colorectal adenocarcinoma (Table 29.2)
Appendix
-
3.
Markers helpful in differentiating common benign glandular proliferative lesions involving the appendix (Table 29.3)
-
4.
Useful markers differentiate goblet cell adenocarcinoma, classic neuroendocrine tumor, and conventional adenocarcinoma with signet ring cells (Table 29.4)
-
5.
Markers to distinguish mucinous tumors of appendiceal versus ovarian origin (Table 29.5)
Colon and Rectum
-
6.
Commonly used markers for diagnosis of Hirschsprung’s disease and potential pitfalls (Table 29.6)
-
7.
Different staining patterns between usual colorectal adenocarcinoma and some of its unique variants (Table 29.7)
-
8.
Markers to differentiate colorectal adenocarcinoma from metastatic adenocarcinomas of the breast, pancreas, and lung (Table 29.8)
-
9.
Markers to differentiate colorectal adenocarcinoma from common gynecological carcinomas (Table 29.9)
-
10.
Markers to differentiate colorectal adenocarcinoma from primary adenocarcinoma of the bladder, urachus, and prostate (Table 29.10)
-
11.
Markers to differentiate colorectal adenocarcinoma from peritoneal mesothelioma (Table 29.11).
-
12.
Markers to distinguish well-differentiated neuroendocrine tumors (WD-NETs) of colorectal origin versus other organ systems (Table 29.12)
-
13.
Markers to differentiate common colonic mucosal mesenchymal polyps (Table 29.13)
-
14.
Markers to differentiate common primary mesenchymal tumors of the colon and rectum (Table 29.14)
-
15.
Markers useful to confirm dysplasia in inflammatory bowel disease (IBD) and to differentiate IBD -associated dysplasia from sporadic adenoma (Table 29.15)
-
16.
Mismatch repair (MMR) proteins markers and algorithm to assess the risk of Lynch syndrome (Table 29.16)
Anus
-
17.
Markers to differentiate adenocarcinoma of anal duct origin from small intestinal, colorectal adenocarcinoma, endocervical, and prostatic adenocarcinoma (Table 29.17)
-
18.
Markers for anal Paget’s disease versus melanoma in situ (Table 29.18)
-
19.
Markers for anal squamous carcinoma versus basal cell carcinoma versus urothelial carcinoma versus small cell carcinoma (Table 29.19)

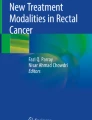
An example of metastatic colonic adenocarcinoma involving small intestinal mucosa. SATB2 nuclear immunoreactivity highlights metastatic tumor cells in the right while the normal small intestinal glands lack immunoreactivity

Goblet cell carcinoid tumor of the appendix. H&E tissue section shows the tumor cells with goblet cell morphology infiltrating the appendiceal wall (a). The tumor cells demonstrate positive nuclear immunoreactivity for CDX2 (b), CK20 (c) and CK7 (d). The tumor cells are also positive for synaptophysin and chromogranin (not shown)

Loss of calretinin immunoreactivity in hypertrophied nerve bundles in Hirschsprung’s disease. Nerves and ganglia show positive immunoreactivity for calretinin in normal control (a). In addition to the absence of ganglion cells, the thick nerve bundles in Hirschsprung’s disease exhibit loss of calretinin immunoreactivity (b)

Colonic medullary carcinoma. Hematoxylin and eosin (H&E) tissue section shows a sheet of tumors with primitive appearance (a); tumor cells show membranous immunoreactivity to CDH17 (b) and nuclear immunoreactivity to SATB2 (c). In addition, they are also strongly and diffusely positive for calretinin (d)

Schwann cell hamartoma and intestinal mucosal perineureoma. Hematoxylin and eosin (H&E)-stained sections of both lesions show spindle cell proliferation without ganglion cells. Schwann cell hamartoma, H&E stain (a) and demonstrating diffuse and strong immunoreactivity to S100 (b); intestinal mucosal perineurioma, H&E stain (c), and demonstrating positive immunoreactivity to GLUT 1 (d)

Granular cell tumor of the ascending colon. The tumor cells exhibit characteristic eosinophilic granular cytoplasm (a). They are strongly and diffusely positive for S100 (b)

Algorithm to assess the risk of Lynch syndrome in colorectal carcinoma

Anal gland adenocarcinoma. The tumor cells exhibit positive CK7 immunoreactivity

Anal Paget’s disease with underlying mucinous adenocarcinoma. The tumor cells involve the overlying epidermis with pagetoid spreading and exhibit positive CK 20 immunoreactivity
Note for All Tables:
“+”—usually greater than 70% of cases are positive; “−”—less than 5% of cases are positive; “+ or −”—usually more than 50% of cases are positive; “− or +”—less than 50% of cases are positive: ND—no data available; V—variable.
References
Mai KT, Burns BF. Development of dysplastic mucinous epithelium from endometriosis of the appendix. Histopathology. 1999;35(4):368–72.
McCluggage WG, Clements WD. Endosalpingiosis of the colon and appendix. Histopathology. 2001;39(6):465–646.
WHO classification of tumours of the digestive system. 2019. WHO Classification of Tumours Editorial Board. WHO press.
Zhang K, Meyerson C, Kassardjian A, Westbrook LM, Zheng W, Wang HL. Goblet cell carcinoid/carcinoma: an update. Adv Anat Pathol. 2019;26(2):75–83.
Vang R, Gown AM, Wu LS, et al. Immunohistochemical expression of CDX2 in primary ovarian mucinous tumors and metastatic mucinous carcinomas involving the ovary: comparison with CK20 and correlation with coordinate expression of CK7. Mod Pathol. 2006;19(11):1421–9.
Fraggetta F, Pelosi G, Cafici A, Scollo P, Nuciforo P, Viale G. CDX2 immunoreactivity in primary and metastatic ovarian mucinous tumours. Virchows Arch. 2003;443(6):782–6.
Vang R, Gown AM, Barry TS, et al. Cytokeratins 7 and 20 in primary and secondary mucinous tumors of the ovary: analysis of coordinate immunohistochemical expression profiles and staining distribution in 179 cases. Am J Surg Pathol. 2006;30(9):1130–9.
Lee MJ, Lee HS, Kim WH, Choi Y, Yang M. Expression of mucins and cytokeratins in primary carcinomas of the digestive system. Mod Pathol. 2003;16(5):403–10.
Goldstein NS, Bassi D, Uzieblo A. WT1 is an integral component of an antibody panel to distinguish pancreaticobiliary and some ovarian epithelial neoplasms. Am J Clin Pathol. 2001;116(2):246–52.
Guerrieri C, Franlund B, Fristedt S, Gillooley JF, Boeryd B. Mucinous tumors of the vermiform appendix and ovary, and pseudomyxoma peritonei: histogenetic implications of cytokeratin 7 expression. Hum Pathol. 1997;29(9):1039–45.
Ronnett BM, Kurman RJ, Shmookler BM, Sugarbaker PH, Young RH. The morphologic spectrum of ovarian metastases of appendiceal adenocarcinomas: a clinicopathologic and immunohistochemical analysis of tumors often misinterpreted as primary ovarian tumors or metastatic tumors from other gastrointestinal sites. Am J Surg Pathol. 1997;21(10):1144–55.
Seidman JD, Elsayed AM, Sobin LH, Tavassoli FA. Association of mucinous tumors of the ovary and appendix. A clinicopathologic study of 25 cases. Am J Surg Pathol. 1993;17(1):22–34.
Elias KM, Labidi-Galy SI, Vitonis AF, et al. Prior appendectomy does not protect against subsequent development of malignant or borderline mucinous ovarian neoplasms. Gynecol Oncol. 2014;132(2):329–33.
Su MC, Yuan RH, Lin CY, Jeng YM. Cadherin-17 is a useful diagnostic marker for adenocarcinomas of the digestive system. Mod Pathol. 2008;21(11):1379–86.
Panarelli NC, Yantiss RK, Yeh MM, Liu Y, Chen YT. Tissue-specific cadherin CDH17 is a useful marker of gastrointestinal adenocarcinomas with higher sensitivity than CDX2. Am J Clin Pathol. 2012;138(2):211–22.
Magnusson K, de Wit M, Brennan DJ, et al. SATB2 in combination with cytokeratin 20 identifies over 95% of all colorectal carcinomas. Am J Surg Pathol. 2011;35(7):937–48.
Lin F, Shi J, Zhu S, et al. Cadherin-17 and SATB2 are sensitive and specific immunomarkers for medullary carcinoma of the large intestine. Arch Pathol Lab Med. 2014;138(8):1015–26.
Cathro HP, Stoler MH. Expression of cytokeratins 7 and 20 in ovarian neoplasia. Am J Clin Pathol. 2002;117(6):944–51.
Kapur RP, Reed RC, Finn L, et al. Calretinin immunohistochemisty versus acetylcholinersterase histochemistry in the elevation of suction rectal biopsies for Hirschsprung disease. Pediatr Dev Pathol. 2009;12(1):6–15.
Monforte-Munoz H, Gonzalez-Gomez I, Rowland JM, Landing BH. Increased submucosal nerve trunk caliber in aganglionosis: a “positive” and objective finding in suction biopsies and segmental resections in Hirschsprung’s disease. Arch Pathol Lab Med. 1998;122(8):721–5.
MacKenzie JM, Dixon MF. An immunohistochemical study of the enteric neural plexi in Hirschsprung’s disease. Histopathology. 1987;11(10):1055–66.
Guinard-Samuel V, Bonnard A, De Lagausie P, et al. Calretinin immunohistochemistry: a simple and efficient tool to diagnose Hirschsprung disease. Mod Pathol. 2009;22(10):1379–84.
Taliano RJ, LeGolvan M, Resnick MB. Immunohistochemistry of colorectal carcinoma: current practice and evolving applications. Hum Pathol. 2013;44(2):151–63.
Winn B, Tavares R, Fanion J, et al. Differentiating the undifferentiated: immunohistochemical profile of medullary carcinoma of the colon with an emphasis on intestinal differentiation. Hum Pathol. 2009;40(3):398–404.
Lugli A, Tzankov A, Zlobec I, Terracciano LM. Differential diagnostic and functional role of the multi-marker phenotype CDX2/CK20/CK7 in colorectal cancer stratified by mismatch repair status. Mod Pathol. 2008;21(11):1403–12.
Hinoi T, Tani M, Lucas PC, et al. Loss of CDX2 expression and microsatellite instability are prominent features of large cell minimally differentiated carcinomas of the colon. Am J Pathol. 2001;159(6):2239–48.
McGregor DK, Wu TT, Rashid A, Luthra R, Hamilton SR. Reduced expression of cytokeratin 20 in colorectal carcinomas with high levels of microsatellite instability. Am J Surg Pathol. 2004;29(6):712–8.
Wright CL, Stewart ID. Histopathology and mismatch repair status of 458 consecutive colorectal carcinomas. Am J Surg Pathol. 2003;27(11):1393–406.
Sakamoto K, Watanabe M, De La Gruz C, et al. Primary invasive micropapillary carcinoma of the colon. Histopathology. 2005;47(5):479–84.
Wen P, Xu Y, Frankel WL, Shen R. Invasive micropapillary carcinoma of the sigmoid colon: distinct morphology and aggressive behavior. Int J Clin Exp Pathol. 2008;1(5):457–60.
Inamura K, Satoh Y, Okumura S, et al. Pulmonary adenocarcinomas with enteric differentiation: histologic and immunohistochemical characteristics compared with metastatic colorectal cancers and usual pulmonary adenocarcinomas. Am J Surg Pathol. 2005;29(5):660–5.
Tan J, Sidhu G, Greco MA, Ballard H, Wieczorek R. Villin, cytokeratin 7, and cytokeratin 20 expression in pulmonary adenocarcinoma with ultrastructural evidence of microvilli with rootlets. Hum Pathol. 1998;29(4):390–6.
Yatabe Y, Koga T, Mitsudomi T, Takahashi T. CK20 expression, CDX2 expression, K-ras mutation, and goblet cell morphology in a subset of lung adenocarcinomas. J Pathol. 2004;203(2):645–52.
Liu H, Shi J, Wilkerson M, et al. Immunohistochemical evaluation of GATA3 expression in tumors and normal tissues: a useful immunomarker for breast and urothelial carcinomas. Am J Clin Pathol. 2012;138(1):57–64.
Nishizuka S, Chen ST, Gwadry FG, et al. Diagnostic markers that distinguish colon and ovarian adenocarcinomas: identification by genomic, proteomic, and tissue array profiling. Cancer Res. 2003;63(17):5243–50.
Kriegsmann M, Harms A, Longuespée R, Muley T, Winter H, Kriegsmann K, Kazdal D, Goeppert B, Pathil A, Warth A. Role of conventional immunomarkers, HNF4-α and SATB2, in the differential diagnosis of pulmonary and colorectal adenocarcinomas. Histopathology. 2018;72:997–1006.
Suh N, Yang XJ, Tretiakova MS, Humphrey PA, Wang HL. Value of CDX2, villin, and alpha-methylacyl coenzyme A racemase immunostains in the distinction between primary adenocarcinoma of the bladder and secondary colorectal adenocarcinoma. Mod Pathol. 2005;18(9):1217–22.
Wang HL, Lu DW, Yerian LM, et al. Immunohistochemical distinction between primary adenocarcinoma of the bladder and secondary colorectal adenocarcinoma. Am J Surg Pathol. 2001;25(11):1380–7.
Gopalan A, Sharp DS, Fine SW, et al. Urachal carcinoma: a clinicopathologic analysis of 24 cases with outcome correlation. Am J Surg Pathol. 2009;33(5):659–68.
Paner GP, Mckenney JK, Barkan GA, et al. Immunohistochemical analysis in a morphologic spectrum of urachal epithelial neoplasms: diagnostic implication and pitfalls. Am J Surg Pathol. 2011;35(6):787–98.
Pancione M, Forte N, Fucci A, et al. Prognostic role of beta-catenin and p53 expression in the metastatic progression of sporadic colorectal cancer. Hum Pathol. 2010;41(6):867–76.
Gurel B, Ali TZ, Montgomery EA, et al. NKX3.1 as a marker of prostate origin in metastatic tumors. Am J Surg Pathol. 2010;34(8):1097–105.
Hameed O, Humphrey PA. Immunohistochemistry in diagnostic surgical pathology of prostate. Semin Diagn Pathol. 2005;22(1):88–104.
Chu AY, Litzky LA, Pasha TL, Acs G, Zhang PJ. Utility of D2-40, a novel mesothelial marker, in the diagnosis of malignant mesothelioma. Mod Pathol. 2005;18(1):105–10.
Ordonez NG. Immunohistochemical diagnosis of epithelioid mesothelioma: an update. Arch Pathol Lab Med. 2005;129(11):1407–14.
Ordonez NG. Value of cytokeratin 5/6 immunostaining in distinguishing epithelial mesothelioma of the pleura from lung adenocarcinoma. Am J Surg Pathol. 1998;22(10):1215–21.
Barbareschi M, Roldo C, Zamboni G, et al. CDX-2 homeobox gene product expression in neuroendocrine tumors: its role as a marker of intestinal neuroendocrine tumors. Am J Surg Pathol. 2004;29(9):1169–76.
Chan ES, Alexander J, Swanson PE, Jain D, Yeh MM. PDX-1, CDX-2, TTF-1, and CK7: a reliable immunohistochemical panel for pancreatic neuroendocrine neoplasms. Am J Surg Pathol. 2012;36(5):737–43.
Denby KS, Briones AJ, Bourne PA, et al. IMP3, NESP55, TTF-1 and CDX2 serve as an immunohistochemical panel in the distinction among small-cell carcinoma, gastrointestinal carcinoid, and pancreatic endocrine tumor metastasized to the liver. Appl Immunohistochem Mol Morphol. 2012;20(6):573–9.
Li Z, Zhou K, Mei K, Kang Q, Cao D. SATB2 is a highly sensitive marker for hindgut well-differentiated neuroendocrine tumors [USCAP abstract 682]. Mod Pathol. 2013;26(S2):164A.
Gibson JA, Hornick JL. Mucosal Schwann cell “hamartoma”: clinicopathologic study of 26 neural colorectal polyps distinct from neurofibromas and mucosal neuromas. Am J Surg Pathol. 2009;33(5):781–7.
Hornick JL, Fletcher CD. Intestinal perineuriomas: clinicopathologic definition of a new anatomic subset in a series of 10 cases. Am J Surg Pathol. 2005;29(7):859–65.
Groisman GM, Polak-Charcon S. Fibroblastic polyp of the colon and colonic perineurioma: 2 names for a single entity? Am J Surg Pathol. 2008;32(7):1088–94.
Agaimy A, Stoehr R, Vieth M, et al. Benign serrated colorectal fibroblastic polyps/intramucosal perineuriomas are true mixed epithelial-stromal polyps (hybrid hyperplastic polyp/mucosal perineurioma) with frequent BRAF mutations. Am J Surg Pathol. 2010;34(11):1663–71.
Miettinen M, Sobin LH, Sarlomo-Rikala M. Immunohistochemical spectrum of GISTs at different sites and their differential diagnosis with a reference to CD117 (KIT). Mod Pathol. 2000;13(10):1134–42.
Miettinen M, Furlong M, Sarlomo-Rikala M, Burke A, Sobin LH, Lasota J. Gastrointestinal stromal tumors, intramural leiomyomas, and leiomyosarcomas in the rectum and anus: a clinicopathologic, immunohistochemical, and molecular genetic study of 144 cases. Am J Surg Pathol. 2001;25(9):1121–33.
Ramos da Silva S, Bacchi MM, Bacchi CE, Elgui de Oliveira D. Human bcl-2 expression, cleaved caspase-3, and KSHV LANA-1 in Kaposi sarcoma lesions. Am J Clin Pathol. 2007;129(5):794–802.
Shekitka KM, Sobin LH. Ganglioneuromas of the gastrointestinal tract. Relation to Von Recklinghausen disease and other multiple tumor syndromes. Am J Surg Pathol. 1994;18(3):250–7.
Parfitt JR, Rodriguez-Justo M, Feakins R, Novelli MR. Gastrointestinal Kaposi’s sarcoma: CD117 expression and the potential for misdiagnosis as gastrointestinal stromal tumour. Histopathology. 2008;52(7):816–23.
Shidham VB, Chivukula M, Gupta D, Rao RN, Komorowski R. Immunohistochemical comparison of gastrointestinal stromal tumor and solitary fibrous tumor. Arch Pathol Lab Med. 2002;126(10):1189–92.
Marx A, Wandrey T, Simon P, et al. Combined alpha-methylacyl coenzyme A racemase/p53 analysis to identify dysplasia in inflammatory bowel disease. Hum Pathol. 2009;40(2):166–73.
Dorer R, Odze RD. AMACR immunostaining is useful in detecting dysplastic epithelium in Barrett’s esophagus, ulcerative colitis, and Crohn’s disease. Am J Surg Pathol. 2006;30(7):871–7.
Wong NA, Mayer NJ, MacKell S, Gilmour HM, Harrison DJ. Immunohistochemical assessment of Ki67 and p53 expression assists the diagnosis and grading of ulcerative colitis-related dysplasia. Histopathology. 2000;37(2):108–14.
Harpaz N, Peck AL, Yin J, et al. p53 protein expression in ulcerative colitis-associated colorectal dysplasia and carcinoma. Hum Pathol. 1994;25(10):1069–74.
Bruwer M, Schmid KW, Senninger N, Schurmann G. Immunohistochemical expression of P53 and oncogenes in ulcerative colitis-associated colorectal carcinoma. World J Surg. 2002;26(3):390–6.
Walsh SV, Load M, Torres CM, Antoioli D, Odze RD. p53 and beta-catenin expression in chronic ulcerative colitis-associated polypoid dysplasia and sporadic adenomas:an immunohistochemical study. Am J Surg Pathol. 1999;23(8):963–9.
Noffshinger AE, Belli JM, Miller MA, Fenoglio-Preiser CM. A unique basal pattern of p53 expression in ulcerative colitis is associated with mutation in the p53 gene. Histopathology. 2001;39(5):482–92.
Van Schaik FD, et al. Role of immunohistochemical markers in predicting progression of dysplasia to advanced neoplasia in patients with ulcerative colitis. Inflamm Bowel Dis. 2012;18(3):480–8.
Xie H. Diagnostic utility of TP53 and cytokeratin 7 immunohistochemistry in idiopathic inflammatory bowel disease-associated neoplasia. Mod Pathol. 2014;27(2):303–13.
Ma C, Henn P, Miller C, Herbst C, Hartman DJ, Pai RK. Loss of SATB2 expression is a biomarker of inflammatory bowel disease-associated colorectal dysplasia and adenocarcinoma. Am J Surg Pathol. 2019;43(10):1314–22.
Shia J. An update on tumors of the anal canal. Arch Pathol Lab Med. 2010;134(11):1601–11.
Hobbs CM, Lowry MA, Owen D, Sobin LH. Anal gland carcinoma. Cancer. 2001;92(8):2045–9.
Lisovsky M, Patel K, Cymes K, Chase D, Bhuiya T, Morgenstern N. Immunophenotypic characterization of anal gland carcinoma: loss of p63 and cytokeratin 5/6. Arch Pathol Lab Med. 2007;131(8):1304–11.
Balachandra B, Marcus V, Jass JR. Poorly differentiated tumors of the anal canal: a diagnostic strategy for the surgical pathologist. Histopathology. 2007;50(1):163–74.
Meriden Z, Montgomery EA. Anal duct carcinoma: a report of 5 cases. Hum Pathol. 2012;43(2):216–20.
Ohnishi T, Watanabe S. The use of cytokeratins 7 and 20 in the diagnosis of primary and secondary extramammary Paget’s disease. Br J Dermatol. 2000;142(2):243–7.
Nowak MA, Guerriere-Kovach P, Pathan A, Campbell TE, Deppisch LM. Perianal Paget’s disease: distinguishing primary and secondary lesions using immunohistochemical studies including gross cystic disease fluid protein-15 and cytokeratin 20 expression. Arch Pathol Lab Med. 1998;122(12):1077–81.
Goldblum JR, Hart WR. Perianal Paget’s disease: a histologic and immunohistochemical study of 11 cases with and without associated rectal adenocarcinoma. Am J Surg Pathol. 1998;22(2):170–9.
Battles OE, Page DL, Johnson JE. Cytokeratins, CEA, and mucin histochemistry in the diagnosis and characterization of extramammary Paget’s disease. Am J Clin Pathol. 1997;108(1):6–12.
Smith KJ, Tuur S, Corvette D, Lupton GP, Skelton HG. Cytokeratin 7 staining in mammary and extramammary Paget’s disease. Mod Pathol. 1997;10(11):1069–74.
De la Garza Bravo MM, Curry JL, Torres-Cabala CA, et al. Pigmented extramammary Paget disease of the thigh mimicking a melanocytic tumor: report of a case and review of the literature. J Cutan Pathol. 2014;41(6):529–35.
Kaufmann O, Fietze E, Mengs J, Dietel M. Value of p63 and cytokeratin 5/6 as immunohistochemical markers for the differential diagnosis of poorly differentiated and undifferentiated carcinomas. Am J Clin Pathol. 2001;116(6):823–30.
Longacre TA, Kong CS, Welton ML. Diagnostic problems in anal pathology. Adv Anat Pathol. 2008;15(5):263–78.
Chute DJ, Cousar JB, Mills SE. Anorectal malignant melanoma: morphologic and immunohistochemical features. Am J Clin Pathol. 2006;126(1):93–100.
Owens SR, Greenson JK. Immunohistochemical staining for p63 is useful in the diagnosis of anal squamous cell carcinomas. Am J Surg Pathol. 2007;31(2):295–0.
Long KB, Hornick JL. SOX2 is highly expressed in squamous cell carcinomas of the gastrointestinal tract. Hum Pathol. 2009;40(12):1768–3.
Patil DT, Goldblum JR, Billings SD. Clinicopathological analysis of basal cell carcinoma of the anal region and its distinction from basaloid squamous cell carcinoma. Mod Pathol. 2013;26(10):1382–9.
Nazarian RM, Primiani A, Doyle LA, et al. Cytokeratin 17: an adjunctive marker of invasion in squamous neoplastic lesions of the anus. Am J Surg Pathol. 2014;38(1):78–85.
Linskey KR, Gimbel DC, Zukerberg LR, Duncan LM, Sadow PM, Nazarian RM. BerEp4, cytokeratin 14, and cytokeratin 17 immunohistochemical staining aid in differentiation of basaloid squamous cell carcinoma from basal cell carcinoma with squamous metaplasia. Arch Pathol Lab Med. 2013;137(11):1591–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Geisinger Clinic
About this chapter

Cite this chapter
Chen, G., Li, J., Chen, Z.E., Li, J., Lin, F. (2022). Lower Gastrointestinal Tract and Microsatellite Instability (MSI). In: Lin, F., Prichard, J.W., Liu, H., Wilkerson, M.L. (eds) Handbook of Practical Immunohistochemistry. Springer, Cham. https://doi.org/10.1007/978-3-030-83328-2_29
Download citation
DOI: https://doi.org/10.1007/978-3-030-83328-2_29
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-83327-5
Online ISBN: 978-3-030-83328-2
eBook Packages: MedicineMedicine (R0)