
Abstract
There has been a steady increase in the incidence of osteoarthritis of the knee joint during last year. There are no treatment methods that lead to complete restoration of the structure and function of the knee joint today. Research in the field of regenerative medicine has shown that the use of cell products with MMSCs has therapeutic and regenerative effects on damaged tissues. Many works on this method have been published for the moment. We compared the results of two clinical studies on the treatment of patients with knee OA using SVF and Nanofat in our article. We conducted a comparison of the parameters: evaluation scale data (VAS, KOOS, KSS, SF-36), physical examination data, ultrasound, and MRI data of the knee joint for 24 weeks. We discuss the advantages and disadvantages of each method and make conclusions about the ways of implementation of therapeutic effects of SVF and Nanofat.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Knee osteoarthritis
- Stromal vascular fraction
- Adipose-derived stem cells
- SVF
- ADSC
- Nanofat
- Regeneration of cartilage
- Comparison of methods
-
Due to regenerative medicine development, the new, effective methods of degenerative diseases treatment of the musculoskeletal system appear.
-
Nowadays there are many studies that involve the use of regenerative cells from adipose tissue in orthopedics.
-
Many forms of cell products from adipose tissue and various methods and treatment protocols are available in different studies.
-
But there is a lack of information about comparison of their effectiveness.
-
In our study, we compare outcomes of two clinical researches that cover the treatment of patients with knee osteoarthritis using SVF and Nanofat.
-
The comparison includes the following data, collected during 24 weeks: scales (VAS, KOOS, KSS, SF-36), physical examination, ultrasound, and MRI.
-
The received materials show the high level of effectiveness of both methods.
-
The mechanism of the regenerative effect to the knee differs in SVF and Nanofat, and therefore the effectiveness of both methods appears at different times.
-
The duration of the therapeutic effect depends on the quantitative composition of the cell product and method for its obtaining.
-
The mechanism of the regenerative effect is polymorphic due to the heterogeneous composition of the final product.
-
The article contains a theoretical explanation of the regeneration mechanisms and the therapeutic effects of each of the cell product.
-
Depending on the tasks, the degree of joint damage, and technical equipment, the orthopedist chooses one or another type of cell product.
1 Introduction
Osteoarthrosis (OA) is a chronic joint disease. Over 250 million people suffer from OA worldwide. The high incidence of OA has a significant impact on the socioeconomic well-being of the population and affects the functioning of the healthcare system [1, 2]. According to the World Health Organization, OA of the knee and hip joints is the 11th leading cause of disability [3]. Vos et al. report that OA of the knee joint accounts for 83% of the total incidence of OA of large joints [2].
As OA progresses, all components of the joint are involved in the pathological process, which leads to an imbalance in the functioning of the musculoskeletal system and results in an impairment of limb function [4]. Due to its multifactorial nature, the pathogenesis and course of the disease can vary significantly.
Currently, there are no treatment methods leading to a complete restoration of the structure and function of the knee joint. The goal of conservative treatment of OA is to reduce pain by combining pharmacological and non-pharmacological methods [5]. Slight improvement can be achieved by reducing weight and increasing physical activity [6]. In severe cases to restore the joint function surgical treatment becomes necessary. In order to reduce the number of invasive interventions, the orthopedic community pays more and more attention to disease prevention, early diagnosis, and the development of individualized patient-oriented treatment methods.
One of such areas is the development of tissue regeneration strategies using cell products and stem cells [7]. Recent studies in the field of regenerative medicine have shown that the use of multipotent mesenchymal stromal cells (MMSCs) has pronounced therapeutic and regenerative effects in the treatment of various degenerative-dystrophic diseases [8]. Many works have shown the high efficacy and safety of MMSCs in the treatment of OA, post-traumatic injuries of articular cartilage, and other diseases of the musculoskeletal system [9]. In our opinion, adipose tissue is a universal source of not only MMSCs but also other cells involved in regenerative processes. The population of all nucleated cells that can be isolated from adipose tissue by fermentation process is called the stromal vascular fraction (SVF). SVF has anti-inflammatory, immunomodulating, and antiseptic effects. MMSCs of adipose tissue, as well as MMSCs of bone marrow tissue, are capable of differentiation into other types of cells of mesodermal origin (cartilage, tendons, and ligaments) [10]. SVF refers to the so-called minimally manipulated cell products that do not require cultivation. Thus, SVF is a safer and more effective material compared to MMSCs due to the absence of risk factors associated with long-term cell culturing (contamination, genetic transformation, and spontaneous differentiation) [11]. Also, due to the synergistic effect of various cell types that make up SVF, the therapeutic effect on the treatment of degenerative-dystrophic diseases develops earlier and is more pronounced [12].
Besides applying adipose tissue regenerative cells in the form of SVF, there is also an opportunity to use NanoFat which is the product of adipose tissue mechanical grinding followed by filtration without fermentation processing. The product contains MMSCs of adipose tissue, collagen fibers, damaged adipocytes, and free triglycerides that have high lubrication properties, which is of great importance in the treatment of patients with limited movement in the joints due to degenerative inflammatory changes in the joint tissues. The use of emulsified fat significantly simplifies the process of obtaining the final product and reduces the cost of the procedure on the one hand, but this reduces the concentration of regenerative cells and the degree of regenerative effect on the other hand.
2 Materials and Methods
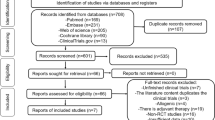
This chapter includes comparison of two clinical studies held in accordance with common protocols, the same inclusion criteria, efficacy evaluations, and follow-up observation periods.
The first study was the treatment of gonarthrosis with SVF. The work was carried out as an independent phase IIb multicenter open-label non-comparative clinical study, under protocol No. RU-LYO-OA2-11-17.
From 2015 till 2018, 48 patients were treated at the department where the investigation was conducted in accordance with the study protocol. The average age of the patients was 56 (37–68) years. The radiological classification of Kellgren and Lawrence was used for OA staging. Thirteen patients with grade 1 OA, 25 patients with grade 2 OA, and 10 patients with grade 3 OA were enrolled in the study. Patients with grade 4 OA were not included in the study. The average BMI was 29.5 (21.1–37.2), patients with a BMI of 40 or more were not enrolled in the study (Table 117.1).
The second study was the treatment of gonarthrosis with Nonfat. Seventy patients with OA of the knee joint (16 with grade 1 OA, 40 patients with grade 2 OA, and 14 patients with grade 3 OA) were enrolled in the study. The average age of the patients was 46 (34–62), the average BMI was 29 (Table 117.1).
Both studies comply with the biomedical ethics committee’s ethical standards developed in accordance with the Declaration of Helsinki and the Good Clinical Practice guidelines (GOST R 52379-2005). Documentation was approved by the Independent Interdisciplinary Committee for the Ethical Expert Evaluation of Clinical Studies.
Before starting treatment, each patient was checked for compliance with the inclusion and noninclusion criteria, after which an informed consent was signed.
Inclusion Criteria
-
1.
Men/women aged 20–85 years.
-
2.
Patients with pain in the knee joint for more than half a day with an intensity of ≥40 mm on a visual analog scale (VAS).
-
3.
The patient has at least three of the following criteria:
-
(a)
age > 20 years;
-
(b)
stiffness in the knee joint <30 min;
-
(c)
patient complaints of cracks, crunching in the joint during movement felt by the patient himself/herself;
-
(d)
bone tenderness on palpation;
-
(e)
increase in joint volume;
-
(f)
absence of hyperthermia over the joint.
-
(a)
-
4.
Patients are able to walk without assistance.
-
5.
The patient has read the information sheet and signed the informed consent form.
Contraindications
-
1.
Septic arthritis, inflammatory joint diseases, gout, severe chondrocalcinosis (pseudopodagra), Paget’s disease, ochronosis, acromegaly, hematochromatosis, Wilson’s disease, primary osteochondromatosis, osteonecrosis, hemophilia;
-
2.
Systemic disease history.
-
3.
Indications for the start of immunosuppressive therapy.
-
4.
А history of Venous thromboembolism (including pulmonary embolism) or a high risk of venous thromboembolism.
-
5.
Significant weight loss (>10% of body weight in the previous year) of unknown etiology.
-
6.
Chronic diseases of internal organs in subcompensated or decompensated forms.
-
7.
Clinically significant deviations in the results of laboratory tests.
-
8.
Patients with malignant tumors, including postoperative period on the background of chemo and/or radiation therapy.
Patients were followed up for 6 months. According to the study protocol, each patient completed seven visits, where visit No. 1 was screening and enrollment of the patient in the study, visit No. 1 was manipulation (adipose tissue sampling, isolation, and certification of SVF or NanoFat, intra-articular administration of the cell product). Visit 2 was at week 1, visit 3 at week 4, visit 4 at week 5, visit 6 at week 12, and visit 5 at week 24 after the administration of the cell product into the knee joint.
Adipose tissue was taken by standard syringe tumescent liposuction. The volume of adipose tissue was 110–150 mL.
2.1 Obtaining SVF
In a laminar box, adipose tissue was transferred from syringes into a sterile disposable container and washed three times with Hartman’s solution (Hemofarm, Serbia). For fermentation process, a 0.15% type 2 collagenase solution (Sigma, USA) was added to the container in an amount equal to the amount of washed adipose tissue. The container was closed with a lid and incubated in a shaker for 30 min at 37 °C. Subsequently, the resulting cell suspension was filtered through a sieve with a pore diameter of 100 μm, transferred to sterile tubes, and washed three times to get rid of collagenase with Hartman’s solution, followed by centrifugation for 7 min at 300 × g. Then the cell sediment was dissolved in 5 mL of Hartman’s solution and 0.5 mL was taken for the sample certification. The remaining 4.5 mL of the cell suspension was transferred into a sterile syringe, which was labeled and placed in a sterile secondary packaging.
To obtain the Nanofat product, adipose tissue was taken in the same way in a volume of 20 mL. In the operation room, the syringe with the collected product was connected to a syringe of the same volume through a specially designed connector. By moving the product 60 times from one syringe to another, large fatty grafts were mechanically ground to an emulsion state. The resulting emulsion was cleaned of large components through a sterile filter with a pore size of 15 μm (Fig. 117.1). The final Nanofat product is an emulsion with particle sizes of less than 0.2 mm (adipose tissue fragments and cell elements) that passes through a needle with a minimum diameter of 0.25 mm.


Device for grinding large fat grafts
The injection of SVF or NanoFAT into the knee joint is performed through a standard lateral suprapatellar access. Puncture of the knee joint is performed in a clean dressing room, in aseptic conditions (Fig. 117.2).


Injection of NanoFAT into the knee joint
2.2 Certification of Samples
2.2.1 SVF
Certification of samples was carried out in accordance with the developed Standard Operating Procedure and included a mandatory description of the total number of cells, viability, and subpopulation composition. Cells were counted according to standard methods using a hemocytometer and trypan blue staining to determine viability. To determine the subpopulation composition of the obtained cell products, the cell suspension was stained with fluorochrome-labeled antibodies to surface markers (CD3, 4, 14, 31, 34, 45, 90, 105, 146, all by Becton Dickinson, USA) in accordance with the manufacturer’s instructions. Then, immunophenotyping of the samples was carried out in a BD FACS CantoII flow cytometer (Becton Dickinson, USA).
2.2.2 Nanofat
For Nanofat, subpopulations were not counted due to the composition of the final product (a large number of stroma and low percentage of cells). The concentration of the total number of cells was counted on a NucleoCounter-200 device.
2.3 Statistical Analysis
Statistical analysis of the results was performed in program R 3.2.4 (R foundation).
Given the small number of observations, an analysis of the distribution of the studied attribute values was not carried out.
Evaluation of the treatment efficacy was carried out by comparing the numerical values of the treatment efficacy criteria at visits 2.6 compared with the values recorded at visit 1 (two-sided Wilcoxon test was used for dependent groups).
To describe ordinal attributes, the median was used as an indicator of the central tendency, and 25 and 75 percentile as a measure of the attribute variability (interquartile range, if the sample did not contain a value corresponding to 25, 50, or 75 percentile, for the median value, the upper and lower quartiles were taken as the average of the two nearest values. For binary attributes, relative frequencies and their 95% confidence intervals are given.
2.4 Efficacy Assessment
To assess the efficacy, at each visit, a physical examination of the patient was carried out, with the results of the examination recorded in the CRF; to objectively assess the condition of the knee joint, patients filled out the following questionnaires: VAS, KOOS, KSS, SF-36, and patients had an ultrasound of the knee joint performed. Also, at the beginning and end of the study, all patients underwent MRI and X-ray of the knee joint.
3 Results
None of the patients in the SVF group had any serious adverse events or adverse reactions, their relative frequency was 0.0%, 95% confidence interval [0.0%; 0.119%]. Two patients (4.1%) noted the occurrence of nonserious adverse reactions in the form of mild hyperemia and tenderness of soft tissues in the area of the knee joint puncture. These adverse events disappeared without treatment within 5–7 days and had appeared most likely due to the action of residual collagenase concentrations in the final cell product. Also, in 3 (6.2%) patients with grade 3 OA, the occurrence of collateral ligament tendonitis in the area of their contact with marginal osteophytes was noted at visits 2 and 3. This event appeared due to the increased physical activity of patients due to a general improvement in the condition of the knee joint, and as a result, overload of the collateral ligaments. This adverse event disappeared without treatment within 1–2 weeks by decreasing activity. In 60 (85.7%) patients in the NanoFat group, synovitis of the knee joint was observed at visit 1, which disappeared within 3–7 days.
The average number of cells in the SVF was 230 × 106 (89 × 106–410 × 106). The total number of nucleated cells was 56.3 × 106 (9 × 106–75 × 106).
In NanoFat, one milliliter of the final product contained 1–3 million cells with a viability of 45–65%. The volume of the product administered was 10.0 mL and the total number of cells was 20 × 106.
3.1 Data of Rating Scales
There was a statistically significant (p < 0.05) difference in VAS scores in group 1 and 2 patients. In patients with OA 1-on 6 visits, OA 2-on 4 visits, OA 3-on 2, 3, and 5 visits (Fig. 117.3, Table 117.2).


Dynamics of indicators of pain intensity by VAS. Marker-median, “box”—upper and lower quartiles, “whiskers”—minimum and maximum; *—differences in comparison with the values recorded at the screening (visit-1) are significant, p < 0.05 (Wilcoxon criterion for dependent groups). Green column—NanoFAT, red column—SVF
Assessment of the function of the knee joint on the KOOS scale revealed an improvement after intra-articular administration of SVF and NanoFat. There was a statistically significant (p < 0.05) difference scores in group 1 and 2 patients. In patients with OA 1-on 4 visits, OA 2-on 2 visits. In patient with OA 3, there was not a statistically significant difference (Fig. 117.4, Table 117.2).


Dynamics of indicators of knee function by KOOS. Marker-median, “box”—upper and lower quartiles, “whiskers”—minimum and maximum; *—differences in comparison with the values recorded at the screening (visit-1) are significant, p < 0.05 (Wilcoxon criterion for dependent groups). Green column—NanoFAT, red column—SVF
Assessment of the function of the knee joint on the KSS scale (overall assessment) revealed an improvement after intra-articular administration of SVF and NanoFat. There was a statistically significant (p < 0.05) difference scores in group 1 and 2 patients. In patients with OA 1-on 5 visits, OA 2-on 4 and 6 visits, OA 3-on 2 and 5 visits (Fig. 117.5, Table 117.2).


Dynamics of indicators of knee function by KSS overall score. Marker-median, “box”—upper and lower quartiles, “whiskers”—minimum and maximum; *—differences in comparison with the values recorded at the screening (visit-1) are significant, p < 0.05 (Wilcoxon criterion for dependent groups). Green column—NanoFAT, red column—SVF
When assessing the quality of life using the SF-36 questionnaire, an improvement in the physical health component after intra-articular administration of SVF and NanoFat. There was a statistically significant (p < 0.05) difference scores in group 1 and 2 patients. In patients with OA 1-on 2 visits, OA 2-on 2 visits, OA 3-on 4, 5, and 6 visits (Fig. 117.6, Table 117.2).


SF-36 Physical health. The differences compared with the values recorded at screening are significant, p < 0.05 (Wilcoxon test for dependent groups). Green column—NanoFAT, red column—SVF
3.2 Physical Examination
The comparison of the results of examination and palpation of the knee joints of patients at the screening and final visits showed a decrease in swelling of the surrounding soft tissues, restoration of normal anatomical outlines of the knee joint, and an increase in the circumference of the thigh at the level of the lower third; on palpation, there was a decrease in the amount of excess intra-articular fluid, the absence of hyperthermia in the knee joint area, a reduction of pain on palpation of the patella and condyles of the femur and tibia, as well as of the lateral and medial articular cavities, an increased range of movements, the disappearance of enthesopathies of collateral ligaments and pain in the Hamstring muscle tendons (Figs. 117.7 and 117.8). However, these results were more pronounced and detected earlier in patients who received treatment with SVF than in patients treated with NanoFat, and the improvements were kept up until the end of the observation period, while in patients of group 2, some of the symptoms returned by the sixth month after the start of the study. It is worth noting however that in most patients of group 2, the range of movements in the knee joint increased immediately after the administration of NanoFat into the knee joint.


Patient with OA 2, visit-1. Knee joint with signs of synovitis and inflammation before SVF injection. Arrow—the location of the puncture


Patient with OA 2, visit 6. The comparison of the results of examination and palpation of the knee joints of patients at the screening and final visits showed a decrease in swelling of the surrounding soft tissues, restoration of normal anatomical outlines of the knee joint. Arrow—the location of the puncture
3.3 Instrumental Diagnostic Methods
The comparison of MRI data obtained at visit 6 versus screening showed a decrease in the amount of free intra-articular fluid in most patients of group 1. There was a reduction or disappearance of foci of bone tissue swelling in the condyles of the femur and tibia. The area of the chondral defects did not change, but the signs of changes in the subchondral bone in the area of the defect regressed, and the chondral defect was covered with tissue similar to cartilaginous one as judged by the quality of an MR signal. The thickness of cartilaginous tissue on the loaded surface of the condyles of the femur and tibia was also noted (Figs. 117.9 and 117.10). As for patients of group 2, such pronounced changes in MRI were not observed and only the amount of excess intra-articular fluid decreased.




MRI data of a 74-year-old patient with grade 2 OA, at visits-1 and 5. (a, c, e, g, i)—visit-1; (b, d, f, h, g)—visit 6 (all in the text of a clinical example)




MRI data of a 65-year-old patient with grade 3 OA. (a, c, e, g)—visit-1. (b, d, f, h)—visit 5. (b, d, f, h)—COR T1 increase in cartilage thickness on the loaded surfaces of the condyles of the femur and tibia. (d, f)—MRI SAG T2 complete repair of a defect in the cartilaginous tissue and underlying bone tissue in the anterior lateral femoral condyle; (g, h)—COR PD + FS—an increase in the thickness of the articular cavity in the lateral regions
4 Discussion of the Results
Currently, clinicians have a wide range of proven methods for treating OA of the knee joint such as intra-articular injections of hyaluronic acid and glucocorticoids. However, the long-term results of the application of these methods can hardly be considered satisfactory enough, which necessitates the development of new treatment methods.
Presently, in the available literature, there is a large number of clinical studies on the use of various cell products for the treatment of OA. These products include SVF, NanoFat, MicroFat, ADSC, BMC, PRP, and others. However, different researchers apply different methods for obtaining cell material, and also have different criteria for evaluating the efficacy of treatment methods, so it is not possible to analyze the results of the studies properly.
The results of this clinical study confirm the safety of intra-articular administration of adipose tissue products in the treatment of OA, as evidenced by the absence of serious adverse events and reactions among all patients included in the protocol. However, the frequency of nonserious adverse events in the SVF group (10.6%) is significantly lower than in the NanoFat group (85.7%). Adverse events in the SVF group occur largely due to both pathological changes in the knee joint in the presence of OA and increased patient activity after SVF treatment, but not due to the influence of the cell product itself, whereas patients of group 2 are diagnosed with synovitis directly due to the pro-inflammatory effect of the cell product on the knee joint at the early stages.
The efficacy of intra-articular injection of both cell products is confirmed by the positive dynamics of all the parameters evaluated—physical examination data, rating scales, and instrumental investigation data. However, the degree of parameter change has different dynamics in each group.
So, the physical examination and assessment of local status showed that the regression of OA symptoms occurred faster (starting from visit 1) in the SVF group and positive dynamics was maintained throughout the observation period. The NanoFat group also showed pronounced positive dynamics starting from visit 1 however by visit 6 some patients had some OA symptoms back. On the other hand, patients of group 2 showed a pronounced increase in the range of movements in the knee joint immediately after the administration of NanoFat. This was caused by the lubricating effect of the action due to a decrease in the coefficient of friction between the articular surfaces. Because of this, the pain syndrome decreases, the range of movements in the joint increases, which leads to additional neurotrophic stimulation of the soft tissues of the affected joint.
The analysis of the questionnaire data also shows a positive dynamics in patients of both groups suffering from OA of all grades throughout the observation period. However, the degrees of their severity vary at different visits. When assessing the intensity of pain using the VAS, a statistically significant difference was found in patients with OA 1 at visits 6, OA 2 at visits 6, and OA 3 at visits 2, 3, and 5.
When assessing the function of the knee joint using the KSS and KOOS scales, general patterns are observed in patients of both groups with different grades of OA. When analyzing the data on the KOOS scale, a statistically significant difference was found in patients with OA 1 at visits 4, OA 2 at visits 2, but in patient with OA 3 there was not a statistically significant difference. When analyzing the function of the knee joint using the KSS scale (overall score), a statistically significant difference was found in patients with OA 1 at visits 5, OA 2 at visits 4 and 6, and OA 3 at visits 2 and 5.
When assessing the quality of life using the SF-36 scale, there was no difference in the mental health component in patients of both groups; however, when assessing the physical health component, a statistically significant difference was found in patients with OA 1 at visits 2, OA 2 at visits 2, and OA 3 at visits 3, 4, and 6.
The most striking differences in patients of both groups are noted in the analysis of MRI data. After intra-articular administration of SVF, a decrease in proliferative-inflammatory events is noted, the replacement of chondral defects by tissue that coincides in density and structure with hyaline cartilage, as well as an increase in the thickness of the cartilage along the edges of the defect, restoration of the structure of the underlying subchondral bone, a decrease in the degree of subchondral sclerosis in the lesion and a restoration of trophism of the condyles of the femur and tibia which were swollen before treatment are visualized. That is, morphological changes in the structural components of the knee joint are noted. Whereas in contrast, after intra-articular administration of NanoFat, such changes are not observed and the MRI data at screening and at visit 6 are almost identical.
The therapeutic effects and instrumental investigation data described by the authors convincingly indicate activation of the cartilaginous tissue formation processes at the lesion location in patients of group 1. The formation of cartilaginous tissue can be associated with effects caused by intra-articular administration of SVF. According to modern researches, most scientists consider MMSCs that are part of SVF the main acting agent. In the works of Zuk et al. in 2002, the possibility of MMSC involvement in skeletal tissue regeneration processes was shown [13].
However, there is no unequivocal opinion on the mechanism of therapeutic action and which cell population is considered to be the main one for implementing the effect [16]. At the same time, there is a number of theories of the therapeutic effect of MMSCs themselves. The clinical effect can be achieved due to the paracrine action of MMSCs—the development of a significant number of growth factors and cytokines [17], these proteins have an angiogenic, neurotropic, neuroprotective, anti-inflammatory effect, prevent scarring, activate tissue regeneration, stimulate tissue formation; it can also be achieved by direct grafting of MMSCs and their differentiation into various specialized types of cells, including chondrocytes [18] or by the simultaneous implementation of these mechanisms—secretion of cytokines by MMSCs, which stimulate, among other things, differentiation of resident cells and differentiation of MMSCs themselves into tissue-specific progenitor cells [19, 20].
It is known from the pathophysiology of degenerative changes in the articular cartilage that the main causes of its destruction are inflammation and trophic disorders of the subchondral bone. The presence of leukocytes, tissue macrophages, endothelium, and other cells in the cell product under conditions of active secretion of growth factors by MMSCs contributes to the relief of inflammatory reactions, stimulation of neoangiogenesis in subchondral bone tissue, and reduction of sclerotic changes.
The regenerative effect of a cell product from adipose tissue is polymorphic. Therefore, the method of its implementation, the timing, and degree of impact on the knee joint depends on the composition of the cell product and the concentration of regenerative cells. This causes a difference in the dynamics and degree of the therapeutic effect, as well as the timing of the positive effects of the use of SVF and NanoFat.
Analyzing the results of treatment of OA with SVF and NanoFat, we can conclude that the positive clinical effect in the short-term observation period, evaluated using functional scales, is to a greater extent caused by the action of growth factors and cytokines secreted by MMSCs themselves and other regenerative cells contained in SVF and NanoFat. This is also confirmed by the similar dynamics in the development of a positive therapeutic effect. But in turn, the therapeutic effect in the medium-term observation period, as well as the presence of morpho-functional changes in the cartilaginous tissue and in other structures of the knee joint revealed by MRI is directly due to the effect of MMSCs. Moreover, the degree of the effect directly depends on the concentration of MMSCs in the cell product. Patients treated with SVF received a larger absolute number of MMSCs (on average 56.3 × 106 cells). They noted positive morphological and functional changes found during MRI of the knee joint.
A detailed study of the composition of SVF and NanoFat is necessary to understand the mechanisms of their therapeutic effect. Also, the individual characteristics of the cell product will allow us to identify the effect on the therapeutic potential of such parameters as the volume of lipoaspirate, the characteristics of adipose tissue from various anatomical locations, as well as the effect of gender, age, bad habits, and medical history data on the composition of the product.
5 Conclusion
Adipose tissue of an adult is a rich source of regenerative cells that can be used to treat degenerative diseases of the musculoskeletal system. The results of the study prove the efficacy and safety of treating gonarthrosis with regenerative cells from adipose tissue. Many different forms of cell products from adipose tissue are available to a modern orthopedist. The mechanism of the regenerative effect is polymorphic due to the heterogeneous composition of the final product. The efficacy of intra-articular injection of cell products is confirmed by an improvement in the quality of life and a decrease in the severity of pain throughout the observation period of patients and an improvement in knee function. Therefore, depending on the tasks, the degree of joint damage, and technical equipment, the orthopedist chooses one or another type of cell product. Given the low economic cost and the production of cell material in a disposable closed bedside system, the NanoFat can be considered a safe and effective method for treating OA of the knee. However, it is obvious that the larger the volume of material taken, and the higher the concentration of regenerative cells, the more pronounced and long-lasting the regenerative effect. Therefore, treatment of OA with SVF is the most effective technique, despite the relatively high cost of obtaining the final cell product.
References
Hunter DJ, Schofield D, Callander E. The individual and socioeconomic impact of osteoarthritis. Nat Rev Rheumatol. 2014;10:437–41.
Vos T, Barber RM, Bell B, Bertozzi-Villa A, Biryukov S, Bolliger I, Charlson F, Davis A, Degenhardt L, Dicker D, Duan L, Erskine H, Feigin VL, Ferrari AJ, Fitzmaurice C, Fleming T, Graetz N, Guinovart C, Haagsma J, Hansen GM. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–96.
Lohmander LS. Knee replacement for osteoarthritis: facts, hopes, and fears. Medicographia. 2013;35:181–8.
Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012a;64:1697–707.
Turk DC, Wilson HD, Cahana A. Treatment of chronic non-cancer pain. Lancet. 2011;377:2226–35. https://doi.org/10.1016/S0140-6736(11)60402-9.
Messier SP, Loeser RF, Miller GD, Morgan TM, Rejeski WJ, Sevick MA, Ettinger WH, Pahor M, Williamson JD. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial. Arthritis Rheum. 2004;50:1501–10. https://doi.org/10.1002/art.20256.
Johnstone B, Alini M, Cucchiarini M, Dodge GR, Eglin D, Guilak F, Madry H, Mata A, Mauck RL, Semino CE, Stoddart MJ. Tissue engineering for articular cartilage repair—the state of the art. Eur Cell Mater. 2013;25:248–67.
Sato M, Uchida K, Nakajima H, Miyazaki T, Guerrero AR, Watanabe S, Roberts S, Baba H. Direct transplantation of mesenchymal stem cells into the knee joints of Hartley strain guinea pigs with spontaneous osteoarthritis. Arthritis Res Ther. 2012;14:R31. https://doi.org/10.1186/ar3735.
Strioga M, Viswanathan S, Darinskas A, Slaby O, Michalek J. Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived mesenchymal stem and stromal cells. Stem Cells Dev. 2012;21:2724–52. https://doi.org/10.1089/scd.2011.0722.
Vangsness CT, Farr J, Boyd J, Dellaero DT, Mills CR, LeRoux-Williams M. Adult human mesenchymal stem cells delivered via intra-articular injection to the knee following partial medial meniscectomy: a randomized, double-blind, controlled study. J Bone Joint Surg Am. 2014;96:90–8. https://doi.org/10.2106/JBJS.M.00058.
Bernardo ME, Locatelli F, Fibbe WE. Mesenchymal stromal cells: a novel treatment modality for tissue repair. Ann N Y Acad Sci. 2009;1176:101–17. https://doi.org/10.1111/j.1749-6632.2009.04607.x.
Koh YG, Choi YJ, Kwon SK, Kim YS, Yeo JE. Clinical results and second-look arthroscopic findings after treatment with adipose-derived stem cells for knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1308–16. https://doi.org/10.1007/s00167-013-2807-2.
Zuk PA, Zhu M, Ashjian P. Human adipose tissue is a source of multipotent stem cells. Mol Biol Cell. 2002;13:4279–95. https://doi.org/10.1091/mbc.E02-02-0105.
de Girolamo L, Grassi M, Viganò M, Orfei CP, Montrasio UA, Usuelli F. Treatment of achilles tendinopathy with autologous adipose-derived stromal vascular fraction: results of a randomized prospective clinical trial. Orthop J Sports Med. 2016;4(7 Suppl 4) https://doi.org/10.1177/2325967116S00128.
Pak J, Lee JH, Park KS, Park M, Kang LW, Lee SH. Current use of autologous adipose tissue-derived stromal vascular fraction cells for orthopedic applications. J Biomed Sci. 2017;24(1):9. https://doi.org/10.1186/s12929-017-0318-z.
Lee SY, Kim W, Lim C, Chung SG. Treatment of lateral epicondylosis by using allogeneic adipose-derived mesenchymal stem cells: a pilot study. Stem Cells. 2015;33(10):2995–3005. https://doi.org/10.1002/stem.2110.
Cai L, Johnstone BH, Cook TG, Liang Z, Traktuev D, Cornetta K, Ingram DA, Rosen ED, March KL. Suppression of hepatocyte growth factor production impairs the ability of adipose-derived stem cells to promote ischemic tissue revascularization. Stem Cells. 2007;25(12):3234–43. https://doi.org/10.1634/stemcells.2007-0388.
Ong E, Chimutengwende-Gordon M, Khan W. Stem cell therapy for knee ligament, articular cartilage and meniscal injuries. Curr Stem Cell Res Ther. 2013;8(6):422–8.
Caplan AI, Dennis JE. Mesenchymal stem cells as trophic mediators. J Cell Biochem. 2006;98(5):1076–84. https://doi.org/10.1002/jcb.20886.
Yeo RWY, Lai RC, Tan KH, Lim SK. Exosome: a novel and safer therapeutic refinement of mesenchymal stem cell. Exosomes Microvesicl. 2013;1(7):1–12. https://doi.org/10.5772/57460.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
1 Electronic Supplementary Materials
Video 117.1
Injection—the Injection of SVF or NanoFAT into the knee joint is performed through a standard lateral suprapatellar access. Puncture of the knee joint is performed in a clean dressing room, in aseptic conditions (MP4 54831 kb)
Video 117.2
Liposuction—liposuction is performed in the operating room under local or General anesthesia under aseptic conditions through paraumbilical access (MP4 51168 kb)
Video 117.3
Transportation—syringes with lipoaspirate are Packed in a sterile bag and then placed in a shipping container. The accompanying documentation is sent along with the syringes. It indicates gender, age, blood type, medical history number, volume of lipoaspirate, and donor area. After that, the container is sent to the laboratory for SVF isolation (MP4 39618 kb)
Video 117.4
Preparation of NanoFAT—to obtain the Nanofat product, adipose tissue was taken in the same way in a volume of 20 mL. In the operation room, the syringe with the collected product was connected to a syringe of the same volume through a specially designed connector. By moving the product 60 times from one syringe to another, large fatty grafts were mechanically ground to an emulsion state. The resulting emulsion was cleaned of large components through a sterile filter with a pore size of 15 μm (Fig. 117.1). The final Nanofat product is an emulsion with particle sizes of less than 0.2 mm (adipose tissue fragments and cell elements) that passes through a needle with a minimum diameter of 0.25 mm (MP4 105 kb)
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter
Cite this chapter
Smyshlyaev, I.A. et al. (2022). Osteoarthritis of the Knee: Comparison Between Intra-articular Injection of Adipose-Derived Stromal Vascular Fraction and Nanofat. In: Kalaaji, A. (eds) Plastic and Aesthetic Regenerative Surgery and Fat Grafting. Springer, Cham. https://doi.org/10.1007/978-3-030-77455-4_117
Download citation
DOI: https://doi.org/10.1007/978-3-030-77455-4_117
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-77454-7
Online ISBN: 978-3-030-77455-4
eBook Packages: MedicineMedicine (R0)