
Abstract
Spinal vascular malformation are rare lesions and can present with signs and symptoms ranging from an insidious neurologic decline to acute deterioration depending on the type of vascular malformation and mechanism of spinal cord injury. The most widely accepted classification system is four tiered and includes: Type I, dural arteriovenous fistula (AVF); Type II, intramedullary arteriovenous malformation; Type III, juvenile arteriovenous malformation; and Type IV, intradural perimedullary arteriovenous fistula. Additional spinal vascular lesions include cavernous malformations and spinal aneurysms. Given that the natural history of these lesions in the pediatric population is poorly elucidated, treatment decisions must be individualized. In most circumstances treatment is recommended, as the natural history is believed to be one of neurologic deterioration.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Spinal vascular malformation
- Spinal arteriovenous malformation
- Spinal cavernous malformation
- Spinal vascular lesion
- Spinal hemorrhage
1 Introduction
Spinal vascular malformations are rare lesions that comprise a variety of unique anomalies of the arterial and venous anatomy of the spine, nerve roots, and spinal cord. These lesions can present with insidious onset of signs and symptoms, subacute neurologic decline, or acute deterioration depending on the type of malformation and mechanism of spinal cord injury.
Virchow is credited with the first reported description of a spinal vascular malformation in a German manuscript entitled Die Krankhaften Geschwulste published in 1865, [1, 2]. He described two groups: angioma cavernosum and angioma racemosum, [1, 2]. This was an autopsy report and at the time these were felt, albeit incorrectly, to be neoplastic in origin, [1, 2]. The first operation on a spinal vascular malformation was reported by Berenbruch in 1890 where he describes a case of multiple angiolipomas in association with an “angioma” of the spinal cord [1, 3]. An advancement in the understanding of spinal vascular malformations occurred in 1912 when Charles Elsberg attempted to excise a spinal arteriovenous malformation (AVM) in a thirteen-year-old boy [1, 4]. His three-tier classification scheme of aneurysm, angioma, and dilation of veins provides insight into the relative lack of understanding of these complex lesions at the time [4]. The 1960’s ushered in a new era in the understanding of spinal vascular lesions led by the emergence of spinal angiography [1, 5].
While several classification schemes of spinal vascular malformations have been described, the following four-tier classification is the most commonly used: Type I, dural arteriovenous fistula (AVF); Type II, intramedullary arteriovenous malformation; Type III, juvenile arteriovenous malformation; and Type IV, intradural perimedullary arteriovenous fistula. Additional vascular lesions that fall outside the four-tier system but are of particular importance in the pediatric patient are cavernous malformations and spinal aneurysms.
This chapter will detail the pathophysiology, clinical features, and treatment of spinal vascular malformations with an emphasis on the pediatric patient population.
2 Dural Arteriovenous Fistulas, Type I
Type I spinal vascular lesions (also known as spinal dural arteriovenous fistulas) consist of an abnormal communication between the radicular artery in the nerve root sleeve and the intradural venous system, causing venous hypertension (Fig. 1). While they are the most common spinal vascular lesions among adults, they are generally thought to be acquired in middle-aged or elderly adults, and they are exceedingly rare in the pediatric population [6]. They will not be discussed in depth in this chapter.

Type I spinal vascular lesion, also known as a dural arteriovenous fistula. These lesions consist of an abnormal communication between the radicular artery in the nerve root sleeve and the intradural venous system [7] (Used with permission from the Barrow Neurological Institute, Phoenix, Arizona)
3 Intramedullary Arteriovenous Malformations, Type II
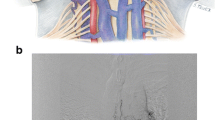
Type II spinal vascular lesions consist of intramedullary arteriovenous malformations, also known as glomus AVMs. The anatomy of Type II lesions are highly variable; the nidus may be compact or diffuse, feeding vessels may be singular or numerous and may arise from the anterior or posterior spinal arteries, and venous drainage can be simple or complex (Fig. 2). Type II lesions represent high-flow, high-pressure lesions with supply derived from the arterial system.

a Type II spinal vascular lesion, also known as an intramedullary arteriovenous malformation. These lesions consist of a nidus fed by vessels that can include branches of the anterior and/or posterior spinal arteries. Anatomy is highly variable [7] (Used with permission from the Barrow Neurological Institute, Phoenix, Arizona). b Diagnostic spinal angiogram demonstrating a Type II spinal vascular lesion involving the cervical spinal cord
3.1 Epidemiology and Clinical Features
Type II spinal vascular lesions are the second most common type of spinal vascular lesion across all age groups, accounting for just over a third of spinal vascular lesions [8, 9]. Variability in clinical presentation has likely led to under-diagnosis in the general population, and thus the true incidence is unknown. Average age of presentation is in young adulthood, [10] with approximately 20% presenting at 18 years or younger [11]. Spinal cord AVMs are located in the cervical cord in 30% of cases and in the thoracolumbar cord in 70%, which is proportional to the volume of the spinal cord at each segment [12]. Syndromic associations include neurofibromatosis, Rendu-Osler-Weber, Klippel-Trenaunay-Weber, and Parkes-Weber syndromes [13,14,15].
Clinical presentation can be acute, subacute, or chronic and encompass a wide range of symptoms including but not limited to pain, motor deficits, sensory disturbances, bowel and bladder dysfunction, and headache. Hemorrhage, intraparenchymal or subarachnoid, is the most common presentation [10, 16, 17], and tends to be more common among children than adults [18]. A review of over 70 cases of Type II spinal vascular lesions in the pediatric population found that 53% presented with acute symptoms as compared to 31% presenting with chronic, progressive symptomatology [6]. Re-hemorrhage appears to occur at higher rates for spinal cord AVMs as compared to brain AVMs, occurring in 10% of patients at 1 month and in 40% within the first year after the initial hemorrhage [18]. Associated aneurysms are present in 20–44% (44% includes aneurysms of the venous system) of cases and portend a higher rate of hemorrhage [10]. One retrospective series reported an associated spinal aneurysm in 20% of patients with an intramedullary AVM; all suffered subarachnoid hemorrhage [19]. Venous congestion and vascular steal can also produce symptoms in the absence of hemorrhage, [10] and likely account for the more insidious presentations associated with Type II lesions.
Conus medullaris AVMs represent a distinct subtype of Type II lesions and are characterized by multiple feeding arteries, multiple niduses, and complex venous drainage [20]. They are unique in their propensity to produce symptoms of both radiculopathy and myelopathy [20].
The primary imaging modalities involved in the diagnosis of Type II spinal vascular lesions are MRI and catheter angiography. MRI is highly sensitive for the detection of spinal AVMs [21, 22]. Typical features include a focal dilatation of the cord around the lesion, an area of low signal around the nidus on T1- and T2-weighted imaging that corresponds to hemosiderin deposition, and multiple flow voids (on axial images) and serpentine structures (on sagittal and coronal images) due to feeding and draining vessels. T2 signal change may represent cord edema due to venous congestion [23]. Catheter angiography remains the gold standard for the evaluation of spinal cord AVMs. A complete angiogram to characterize all feeding and draining vessels, look for aneurysms, and distinguish the lesion from associated normal vessels is necessary to confirm the diagnosis and plan treatment.
3.2 Management
The natural history of untreated Type II spinal vascular lesions is poorly defined. Progressive evolution of symptoms, by either worsening myelopathy or subsequent hemorrhages, is reported in 31–71% of patients observed over several years [10, 24,25,26]. Given the risk of hemorrhage and cumulative risk of neurologic deficit, treatment is generally recommended in the pediatric population when feasible.
Because spinal cord AVM anatomy is variable and the risk of potential complications is relatively high, decision making about the management of these patients is highly individualized. Patients with a spinal cord AVM consisting of a compact, surgically accessible nidus may be good candidates for surgery. Embolization may be a useful adjunct to surgery, or, in some cases, may provide symptomatic relief without necessarily obliterating the lesion.
With appropriate case selection (i.e., by operating on patients with a relatively compact, surgically accessible nidus), obliteration of the lesion can be achieved in up to 94% of cases with good functional outcome in 86% [16]. As expected, surgical results are better with compact AVMs compared with AVMs with a diffuse nidus [27]. Surgical approach is via a standard laminotomy. Exposure should extend at least one level above and one level below the lesion. A small myelotomy is done in the posterior median sulcus, and the spinal cord is split between the two posterior columns. Alternatively, a posterolateral myelotomy, done in the dorsal root entry zone between two or more nerve roots, can provide access to lateral lesions.
Rates of complete obliteration with endovascular embolization range from 24–53% with permanent complication rates of 10–14% [28]. The first-line agent for embolization of any cord AVM is generally NBCA or Onyx, provided that the microcatheter tip can be placed adjacent to or within the nidus. Particulate embolization should be reserved for cases in which the microcatheter tip is relatively proximal to the lesion (i.e., when the catheter tip cannot be placed within or directly adjacent to the nidus). Because the anterior spinal artery and it’s branches are typically <250 μm, particles ≥300 μm should be used to avoid inadvertent embolization of normal arteries [29, 30].
While early reports of stereotactic radiosurgery for the treatment of Type II lesions have been promising [31], experience with this technique is lacking in the pediatric population.
4 Type III, Juvenile Arteriovenous Malformations
Type III spinal vascular lesions, also known as juvenile arteriovenous malformations or spinal arteriovenous metameric syndromes, are complex AVMs that tend to affect vessels in a metameric pattern often involving the spinal cord, vertebrae, and paraspinal musculature (Fig. 3). Spinal arteriovenous metameric syndrome (SAMS) will be covered in depth in Chap. 10; we include it here for completeness. These lesions are rare and may occur as a part of Cobb Syndrome. Cobb Syndrome represents involvement of the entire metamere including an associated vascular skin nevus overlying the spinal lesion. While these terms (Type III spinal vascular lesion, juvenile AVM, and Cobb Syndrome) are often used synonymously, Cobb Syndrome has been reported in association with less complex spinal vascular lesions such as Type IV intradural perimedullary arteriovenous fistulas [32]. Therefore, type III spinal vascular lesions and Cobb syndrome are not exactly synonymous.

Type III spinal vascular lesion, also known as a juvenile arteriovenous malformation. These lesions are complex AVMs that tend to affect vessels in a metameric pattern often involving the spinal cord, vertebrae, and paraspinal musculature [7] (Used with permission from the Barrow Neurological Institute, Phoenix, Arizona)
4.1 Epidemiology and Clinical Features
The true incidence of Type III vascular lesions is difficult to estimate due to the rarity, variable presentation, and inconsistent classification of these lesions. Berenbruch is credited with the first description of the syndrome in an 1890 publication entitled Ein Fall von multiplen Angiolipomen kombiniert mit einem Angiom des Rueckenmarkes (A case of multiple angiolipoma combined with an angioma of the spinal cord) [3]. However, it was not truly recognized as a clinical entity until 1915 with the work of Stanley Cobb, a resident of Harvey Cushing [33]. An eight-year-old boy presented with acute paraplegia and was noted to have “areas of dark reddish skin” over the 9th and 12th rib [33]. The intraoperative vascular findings were termed “cavernous pial arachnoid angiomas” by Cushing [33]. Cobb reported the case and subsequently was credited with the eponym “Cobb syndrome” [32]. While the complete metatmeric syndrome has been reported in fewer than 40 patients [34], the cutaneous findings can be subtle and easily missed, leading to underestimation of the incidence. Other authors have estimated its incidence as high as 10% [35] or 20% [36] among patients with spinal vascular lesions. A male predominance has also been noted [37].
Clinical presentation is variable ranging from acute onset plegia to more insidious symptoms of pain and headache. The natural history of these lesions is poorly defined and unpredictable, making accurate prognosis difficult [34]. However, most authors agree that prognosis tends to be poor in patients with these lesions once they develop symptoms [37].
4.2 Management
The most common imaging modalities for the evaluation of Type III lesions are MRI and catheter angiography. MRI provides a sensitive and non-invasive technique for screening, with the benefit of providing high resolution anatomic detail. Catheter angiography is complementary to MRI and provides an understanding of the lesion’s complex angioarchitecture. While catheter angiography is regarded by most as the gold standard for imaging of Type III lesions, it has been compared to shining a small flashlight on an elephant in a dark room because only a part of the lesion can be seen with injection of contrast into any particular artery.
These lesions are extremely difficult to treat and treatment decisions are individualized on the basis of current neurologic function, angioarchitecture of the lesion, and risks/benefits of the proposed intervention [34]. Although complete lesion resection by staged embolization followed by surgery has been reported [38, 39], fatal complications have been reported with this approach [40]. Expectant management, surgery, endovascular embolization, radiation, and corticosteroid administration have been used in varying combinations [34]. Optimal management depends on a multidisciplinary team with a goal of alleviating the patient’s symptoms and, when possible, reducing the risk of future neurologic decline.
5 Type IV, Intradural Perimedullary Arteriovenous Fistula
Type IV spinal vascular lesions consist of a fistula between a spinal cord artery or arteries and the coronal venous plexus, often with an associated varix at the artery to vein transition point (Fig. 4). They are located on the pial surface of the spinal cord and tend to involve the ventral or lateral surface of the cord. Type IV lesions can be further subdivided into A-C based on size and drainage characteristics [20]. Type A fistulas are small shunts in which blood flow is sluggish and venous hypertension is modest. Type B and C have progressively larger shunts with Type C exhibiting a giant fistula and a markedly distended venous system.

a Type IV spinal vascular lesion, also known as an intradural perimedullary arteriovenous fistula, involving the conus medullaris. These lesions consist of a fistula between a spinal cord artery or arteries and the coronal venous plexus, often with an associated varix at the artery to vein transition point [7] (Used with permission from the Barrow Neurological Institute, Phoenix, Arizona). b Diagnostic spinal angiogram demonstrating a Type IV spinal vascular lesion involving the cervical spinal cord
5.1 Epidemiology and Clinical Features
Intradural perimedullary arteriovenous fistulas are thought to account for 10–20% of all spinal vascular lesions [9, 10]. Within the pediatric population, Type IV lesions rank only behind Type II lesions in incidence comprising just over 20% of spinal vascular malfomations [6]. Type IV lesions are strongly associated with HHT [37, 41]. The location of these lesions along the spinal axis is bimodal, with most occurring at the thoracolumbar junction, particularly at the conus, and to a lesser extent, the upper cervical region [42].
Average age of presentation is in early adulthood but there are reports of diagnosis in infancy [9, 43, 44]. Pediatric patients with Type IV lesions present with acute versus chronic symptoms in roughly equal proportions [6]. While most patients present with symptoms attributable to venous hypertension or mass effect, subarachnoid hemorrhage may occur.
5.2 Management
Imaging of Type IV lesions most often involves MRI and catheter angiography, and to a lesser extent CT angiography and myelography. Type B and C lesions characteristically demonstrate large flow void on MRI [44]. However, it is important to note that type A lesions may not be apparent on MRI [45], and myelography or angiography should be done if a type IV-A lesion is suspected but not visualized on MRI. Catheter angiography remains the gold standard for the evaluation of a Type IV lesion and should be completed to confirm the diagnosis and plan therapy.
The natural history of intradural perimedullary AVFs is thought to be one of progressive neurologic decline and thus most authors recommend prompt diagnosis and treatment. The goal of treatment is disconnection or occlusion at the site of the fistula, which can be accomplished by surgery, embolization, or a combination of both. Treatment decisions must be individualized and are largely determined by the angioarchitecture of the lesion.
6 Cavernous Malformations
Cavernous malformations are well-circumscribed lobulated lesions composed of dilated, thin-walled vascular structures with a gross appearance of a mulberry (Fig. 5). They can occur sporadically or in association with a familial form of the disease. Cavernous malformations are located throughout the central nervous system (CNS), according to the volume of the CNS compartment [46].

a Sagittal T2 weighted MRI of the cervical spine demonstrating an intramedullary cavernous malformation; note the “popcorn like” appearance. b Axial T2 weighted MRI of the cervical spine demonstrating an intramedullary cavernous malformation
6.1 Epidemiology and Clinical Features
Cavernous malformations of the CNS have an estimated incidence of 0.37–0.53% in the pediatric population [47]. Approximately 5% of these are located in the spine, making these lesions quite rare among the general population [48]. Within the spine, a cervical or thoracic location is the most commonly reported [48,49,50].
The majority of pediatric patients present with an acute neurologic decline related to hemorrhage [49, 51]. Typical signs and symptoms include acute onset myelopathy and pain. The natural history of spinal cavernous malformations in the pediatric population is not known. Annual rates of symptomatic re-hemorrhage vary widely [52, 53]. However, given the eloquence of the parenchyma of the spinal cord and the risk of acute and profound neurologic deterioration, surgical resection of accessible lesions is advocated by most authors [54].
6.2 Management
MRI is the radiographic technique of choice for the diagnosis and follow-up of cavernous malformations. Characteristic findings include discrete areas of mixed signal intensity surrounded by a black rim of diminished signal intensity, often referred to as “popcorn like”. Catheter angiography is not necessary, as these lesions are classically “angiographically occult”.
Complete microsurgical resection remains the proven therapeutic modality for treatment of spinal cavernous malformations. Most intramedullary cavernous malformations are approached dorsally with a midline myelotomy for deep, midline lesions, or entry into the dorsal root entry zone for more laterally located lesions. Surgical results are usually good, with one study reporting improvement of stabilization of symptoms in over 80% of patients [49]. While stereotactic radiosurgery has been used to treat cavernous malformations, its utility is not established and it is generally not recommended for the treatment of the pediatric patient.
6.3 Familial Cavernous Malformations
The familial form is typically manifests as multiple lesions in the setting of a positive family history. Genetic mode of inheritance is autosomal dominant. Three genes have been identified: CCM1 on chromosome 7q, CCM2 on 7p, and CCM3 on 3q [55,56,57,58]. No differences in clinical presentation have been identified among the three different mutations. While the incidence of spine lesions associated with the familial form is not known, multiple lesions are found in over half of patients [59,60,61].
7 Spinal Aneurysms
Aneurysms within the spinal canal are exceedingly rare, with a recent systematic review identifying only 140 spinal aneurysms reported over the last 70 years [62]. Although some spinal aneurysms occur as an isolated lesion, most are thought to arise in association with an AVM or coarctation of the aorta [19, 62,63,64]. Isolated spinal aneurysms tend to occur in older patients and are more likely to present with hemorrhage [62]. It is important to note that intracranial subarachnoid hemorrhage, with a negative diagnostic cerebral angiogram, can be encountered in a significant portion of these patients [62]. Thus it is imperative to consider the possibility of a spinal aneurysm during the evaluation of a cerebral angiogram-negative subarachnoid hemorrhage.
7.1 Spinal Aneurysms Associated with AVM
Spinal aneurysms complicate approximately 20% of spinal AVMs and appear to have a strong association with developmental vascular anomalies, such as metameric angiomatosis [19]. Ten percent of all spinal aneurysms occur in children less than 10 year of age; patients with spinal aneurysms associated with an AVMs tend to be younger than those presenting with isolated spinal aneurysms [62]. The presence of a spinal aneurysm in association with an AVM is felt to carry an increased risk of hemorrhage as compared to an isolated AMV [62]. Location of the aneurysm influences its rupture risk with intranidal aneurysms tending to hemorrhage more often than feeding artery aneurysms [62]. While the majority of patients present with signs and symptoms related to hemorrhage, up to 20% can present with complaints not attributable to a hemorrhage [62]. This tends to be more common among young patients [62, 65]. Spinal aneurysms associated with AVMs can be treated with microsurgery or endovascular techniques and treatment decisions should account for the associated AVM. Therapeutic outcome is largely related to the type of associated AVM, with extramedullary AVMs or AVFs faring better than intramedullary AVMs [62]. Resolution or a decrease in size of an aneurysm has been reported following treatment of the associated AVM [66].
7.2 Isolated Spinal Aneurysms
Isolated spinal artery aneurysms are rare lesions typically affecting adults with an average age of presentation of 49 years [62]. They tend to be associated with coartaction of the aorta, connective tissue diseases, autoimmune diseases, and renal transplant [62]. The vast majority of patients presents with signs and symptoms of hemorrhage including headache, back pain, myelopathy, and vomiting [62]. However, particularly large aneurysms may presents with signs and symptoms of myelopathy or radiculopathy due to mass effect [67]. The most common location for an isolated spinal aneurysm is the anterior spinal artery, followed by radicular/radiculopial arteries [62]. Both microsurgery and endovascular techniques have demonstrated efficacy in the treatment of isolated spinal aneurysms; treatment should be tailored based on the angiographic characteristic of the lesion and the clinical situation [62]. Presentation with hemorrhage, cord dysfunction, or associated comorbid conditions predict a poor outcome [62].
8 Conclusions
Spinal vascular lesions are rare entities but pose significant risk to the pediatric patient. The pediatric patient is more likely to have an associated syndromic abnormality (i.e. HHT) and is more likely to presents with an acute neurologic decline. Given that the natural history of these lesions is poorly elucidated, treatment decisions must be individualized. The presumed risk of neurologic decline related to the lesion must be weighed against the risk of therapy. In most circumstances treatment is recommended, as the natural history is believed to be one of neurologic deterioration.
References
Black P. Spinal vascular malformations: an historical perspective. Neurosurg Focus. 2006;21:E11.
Virchow R. Die krankhaften Geschwülste, Bd. 2, 19. Vorlesung. Berlin: August Hirschwald. 1864;65.
Berenbruch K. Ein fall von multiplen Angio-Lipomen Kombiniert mit einem angiom des Rückenmarks. Doctoral thesis, Universität Tübingen;1890.
Elsberg C. Diagnosis and treatment of surgical diseases of the spinal cord and its membranes. Philadelphia: WB Saunders;1916.
DI Chiro G, Doppman J, Ommaya AK. Selective arteriography of arteriovenous aneurysms of spinal cord. Radiology. 1967;88:1065–77.
Du J, Ling F, Chen M, Zhang H. Clinical characteristic of spinal vascular malformation in pediatric patients. Childs Nerv Syst. 2009;25:473–8.
Dashti SR, Toledo M, Kim LJ, Spetzler RF. Classification of spinal arteriovenous lesions: arteriovenous fistulas and arteriovenous malformations. In: HR W editor. Youmans textbook of neurological surgery. Philadelphia, PA:Elsevier;2011. p. 6e.
Bao YH, Ling F. Classification and therapeutic modalities of spinal vascular malformations in 80 patients. Neurosurgery. 1997;40:75–81.
Mourier KL, Gobin YP, George B, Lot G, Merland JJ. Intradural perimedullary arteriovenous fistulae: results of surgical and endovascular treatment in a series of 35 cases. Neurosurgery. 1993;32(6):885–91. (discussion 891).
Rosenblum B, Oldfield EH, Doppman JL, DI Chiro. Spinal arteriovenous malformations: a comparison of dural arteriovenous fistulas and intradural AVM’s in 81 patients. J Neurosurg. 1987;67:795–802.
Lad SP, Santarelli JG, Patil CG, Steinberg GK, Boakye M. National trends in spinal arteriovenous malformations. Neurosurg Focus. 2009;26:1–5.
Niimi Y, Berenstein A. Endovascular treatment of spinal vascular malformations. Neurosurg Clin N Am. 1999;10:47–71.
Djindjian M, Djindjian R, Hurth M, Rey A, Houdart R. Spinal cord arteriovenous malformations and the Klippel-Trenaunay-Weber syndrome. Surg Neurol. 1977;8:229–37.
Lasjaunias PL. Spinal arteriovenous shunts. Berlin: Springer-Verlag;1997.
Poisson A, Vasdev A, Brunelle F, Plauchu H, Dupuis-Girod S, French Italian HHTN. Acute paraplegia due to spinal arteriovenous fistula in two patients with hereditary hemorrhagic telangiectasia. Eur J Pediatr. 2009;168:135–9.
Connolly Jr ES, Zubay GP, McCormick PC, Stein BM. The posterior approach to a series of glomus (Type II) intramedullary spinal cord arteriovenous malformations. Neurosurgery. 1998 Apr 1;42(4):774–84. (discussion 785–6).
Tobin WD, Layton DD. The diagnosis and natural history of spinal cord arteriovenous malformations. Mayo Clin Proc. 1976;51:637–46.
Berenstein A, Lasjaunias P. Spine and spinal cord vascular lesions. In: Berenstein A, Lasjaunias P, editors. Endovascular treatment of spine and spinal cord lesions Surgical Neuroangiography, vol. 5). Berlin:Springer-Verlag;1992.
Biondi A, Merland JJ, Hodes JE, Pruvo JP, Reizine D. Aneurysms of spinal arteries associated with intramedullary arteriovenous malformations. I. Angiographic and clinical aspects. AJNR Am J Neuroradiol. 1992;13:913–22.
Spetzler RF, Detwiler PW, Riina HA, Porter RW. Modified classification of spinal cord vascular lesions. J Neurosurg. 2002;96:145–56.
Dormont D, Gelbert F, Assouline E, Reizine D, Helias A, Riche MC, Chiras J, Bories J, Merland JJ. MR imaging of spinal cord arteriovenous malformations at 0.5 T: study of 34 cases. AJNR Am J Neuroradiol. 1988;9:833–8.
Minami S, Sagoh T, Nishimura K, Yamashita K, Fujisawa I, Noma S, Itoh K, Togashi K, Oda Y, Matsumoto M, et al. Spinal arteriovenous malformation: MR imaging. Radiology. 1988;169:109–15.
Kataoka H, Miyamoto S, Nagata I, Ueba T, Hashimoto N. Venous congestion is a major cause of neurological deterioration in spinal arteriovenous malformations. Neurosurgery. 2001;48(6):1224–30. (discussion 1229–30).
Biondi A, Merland JJ, Reizine D, Aymard A, Hodes JE, Lecoz P, Rey A. Embolization with particles in thoracic intramedullary arteriovenous malformations: long-term angiographic and clinical results. Radiology. 1990;177:651–8.
Riche MC, Modenesi-Freitas J, Djindjian M, Merland JJ. Arteriovenous malformations (AVM) of the spinal cord in children. A review of 38 cases. Neuroradiology. 1982;22:171–80.
Yasargil MG, Symon L, Teddy PJ. Arteriovenous malformations of the spinal cord. Adv Tech Stand Neurosurg. 1984;11:61–102.
Zozulya YP, Slin'ko EI, Al-Qashqish II. Spinal arteriovenous malformations: new classification and surgical treatment. Neurosurg Focus. 2006;20:E7.
Rodesch G, Lasjaunias P, Berenstein A. Embolization of arteriovenous malformations of the spinal cord. In: Valavanis A, editor. Interventional neuroradiology. Berlin:Springer-Verlag;1993.
Manke C, Bretschneider T, Lenhart M, Strotzer M, Neumann C, Gmeinwieser J, Feuerbach S. Spinal metastases from renal cell carcinoma: effect of preoperative particle embolization on intraoperative blood loss. AJNR Am J Neuroradiol. 2001;22:997–1003.
Wilson MA, Cooke DL, Ghodke B, Mirza SK. Retrospective analysis of preoperative embolization of spinal tumors. AJNR Am J Neuroradiol. 2010;31:656–60.
Sinclair J, Chang SD, Gibbs IC, Adler Jr JR. Multisession CyberKnife radiosurgery for intramedullary spinal cord arteriovenous malformations. Neurosurgery. 2006;58(6):1081–9. (discussion 1081–9).
Maramattom BV, Cohen-Gadol AA, Wijdicks EF, Kallmes D. Segmental cutaneous hemangioma and spinal arteriovenous malformation (Cobb syndrome). Case report and historical perspective. J Neurosurg Spine. 2005;3:249–52.
Cobb S. Hemangioma of the spinal cord associated with skin naevi of the same metamer. Ann Surg. 1915;65:641–9.
Clark MT, Brooks EL, Chong W, Pappas C, Fahey M. Cobb syndrome: a case report and systematic review of the literature. Pediatr Neurol. 2008;39:423–5.
Rodesch G, Hurth M, Alvarez H, Tadié M, Lasjaunias P. Classification of spinal cord arteriovenous shunts: proposal for a reappraisal—the Bicetre experience with 155 consecutive patients treated between 1981 and 1999. Neurosurgery. 2002;51(2):374–9. (discussion 379–80).
Doppman JL, Wirth FP, DI Chiro Jr G, Ommaya AK. Value of cutaneous angiomas in the arteriographic localization of spinal-cord arteriovenous malformations. N Engl J Med. 1969;281:1440–4.
Cullen S, Krings T, Ozanne A, Alvarez H, Rodesch G, Lasjaunias P. Diagnosis and endovascular treatment of pediatric spinal arteriovenous shunts. Neuroimaging Clin N Am. 2007;17:207–21.
Menku A, Akdemir H, Durak AC, Oktem IS. Successful surgical excision of juvenile-type spinal arteriovenous malformation in two stages following partial embolization. Minim Invasive Neurosurg. 2005;48:57–62.
Spetzler RF, Zabramski JM, Flom RA. Management of juvenile spinal AVM’s by embolization and operative excision. Case report J Neurosurg. 1989;70:628–32.
Ferch RD, Morgan MK, Sears WR. Spinal arteriovenous malformations: a review with case illustrations. J Clin Neurosci. 2001;8:299–304.
Krings T, Ozanne A, Chng SM, Alvarez H, Rodesch G, Lasjaunias PL. Neurovascular phenotypes in hereditary haemorrhagic telangiectasia patients according to age. Review of 50 consecutive patients aged 1 day-60 years. Neuroradiology. 2005;47:711–20.
Djindjian M, Djindjian R, Rey A, Hurth M, Houdart R. Intradural extramedullary spinal arterio-venous malformations fed by the anterior spinal artery. Surg Neurol. 1977;8:85–93.
Barrow DL, Colohan AR, Dawson R. Intradural perimedullary arteriovenous fistulas (type IV spinal cord arteriovenous malformations). J Neurosurg. 1994;81:221–9.
Halbach VV, Higashida RT, Dowd CF, Fraser KW, Edwards MS, Barnwell SL. Treatment of giant intradural (perimedullary) arteriovenous fistulas. Neurosurgery. 1993 Dec 1;33(6):972–9. (discussion 979–80).
Dillon WP, Norman D, Newton TH, Bolla K, Mark A. Intradural spinal cord lesions: Gd-DTPA-enhanced MR imaging. Radiology. 1989;170:229–37.
Robinson JR, Awad IA, Little JR. Natural history of the cavernous angioma. J Neurosurg. 1991;75:709–14.
Mottolese C, Hermier M, Stan H, Jouvet A, Saint-Pierre G, Froment JC, Bret P, Lapras C. Central nervous system cavernomas in the pediatric age group. Neurosurgical review. 2001;24(2):55–71. (discussion 72–3).
Acciarri N, Galassi E, Giulioni M, Pozzati E, Grasso V, Palandri G, Badaloni F, Zucchelli M, Calbucci F. Cavernous malformations of the central nervous system in the pediatric age group. Pediatr Neurosurg. 2009;45:81–104.
Deutsch H, Jallo GI, Faktorovich A, Epstein F. Spinal intramedullary cavernoma: clinical presentation and surgical outcome. J Neurosurg. 2000;93:65–70.
Lena G, Ternier J, Paz-Paredes A, Scavarda D. Central nervous system cavernomas in children. Neurochirurgie. 2007;53:223–37.
Noudel R, Litre F, Vinchon M, Patey M, Rousseaux P. Intramedullary spinal cord cavernous angioma in children: case report and literature review. Childs Nerv Syst. 2008;24:259–63.
Kharkar S, Shuck J, Conway J, Rigamonti D. The natural history of conservatively managed symptomatic intramedullary spinal cord cavernomas. Neurosurgery. 2007;60(5):865–72. (discussion 865–72).
Sandalcioglu IE, Wiedemayer H, Gasser T, Asgari S, Engelhorn T, Stolke D. Intramedullary spinal cord cavernous malformations: clinical features and risk of hemorrhage. Neurosurg Rev. 2003;26:253–6.
Ghogawala Z, Ogilvy CS. Intramedullary cavernous malformations of the spinal cord. Neurosurg Clin N Am. 1999;10:101–11.
Craig HD, Gunel M, Cepeda O, Johnson EW, Ptacek L, Steinberg GK, Ogilvy CS, Berg MJ, Crawford SC, Scott RM, Steichen-Gersdorf E, Sabroe R, Kennedy CT, Mettler G, Beis MJ, Fryer A, Awad IA, Lifton RP. Multilocus linkage identifies two new loci for a mendelian form of stroke, cerebral cavernous malformation, at 7p15-13 and 3q25.2-27. Hum Mol Genet. 1998;7:1851–8.
Dubovsky J, Zabramski JM, Kurth J, Spetzler RF, Rich SS, Orr HT, Weber JL. A gene responsible for cavernous malformations of the brain maps to chromosome 7q. Hum Mol Genet. 1995;4:453–8.
Gunel M, Awad IA, Anson J, Lifton RP. Mapping a gene causing cerebral cavernous malformation to 7q11.2-q21. Proc Natl Acad Sci USA. 1995;92:6620–4.
Marchuk DA, Gallione CJ, Morrison LA, Clericuzio CL, Hart BL, Kosofsky BE, Louis DN, Gusella JF, Davis LE, Prenger VL. A locus for cerebral cavernous malformations maps to chromosome 7q in two families. Genomics. 1995;28:311–4.
Dobyns WB, Michels VV, Groover RV, Mokri B, Trautmann JC, Forbes GS, Laws ER, JR. . Familial cavernous malformations of the central nervous system and retina. Ann Neurol. 1987;21:578–83.
Rigamonti D, Hadley MN, Drayer BP, Johnson PC, Hoenig-Rigamonti K, Knight JT, Spetzler RF. Cerebral cavernous malformations. Incidence and familial occurrence. N Engl J Med. 1988;319:343–7.
Zabramski JM, Wascher TM, Spetzler RF, Johnson B, Golfinos J, Drayer BP, Brown B, Rigamonti D, Brown G. The natural history of familial cavernous malformations: results of an ongoing study. J Neurosurg. 1994;80:422–32.
Madhugiri VS, Ambekar S, Roopesh kumar VR, Sasidharan GM, Nanda A. Spinal aneurysms: clinicoradiological features and management paradigms. J Neurosurg Spine. 2013;19:34–48.
Aoun SG, EL Ahmadieh TY, Soltanolkotabi M, Ansari SA, Marden FA, Batjer HH, Bendok BR. Ruptured spinal artery aneurysm associated with coarctation of the aorta. World Neurosurg. 2014;81(441):e17–22.
Berlis A, Scheufler KM, Schmahl C, Rauer S, Gotz F, Schumacher M. Solitary spinal artery aneurysms as a rare source of spinal subarachnoid hemorrhage: potential etiology and treatment strategy. AJNR Am J Neuroradiol. 2005;26:405–10.
Binder B, Eng GD, Milhorat TH, Galioto F. Spinal arteriovenous malformations in an infant: unusual symptomology and pathology. Dev Med Child Neurol. 1982;24:380–5.
Biondi A, Merland JJ, Hodes JE, Aymard A, Reizine D. Aneurysms of spinal arteries associated with intramedullary arteriovenous malformations. II. Results of AVM endovascular treatment and hemodynamic considerations. AJNR Am J Neuroradiol. 1992;13:923–31.
EL Mahdi MA, Rudwan MA, Khaffaji SM, Jadallah FA. A giant spinal aneurysm with cord and root compression. J Neurol Neurosurg Psychiatry. 1989;52:532–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Foreman, P.M., Schmalz, P.G.R., Deveikis, J.P., Harrigan, M.R. (2021). Vascular Malformations of the Spine. In: Agrawal, A., Britz, G. (eds) Pediatric Vascular Neurosurgery. Springer, Cham. https://doi.org/10.1007/978-3-030-74749-7_12
Download citation
DOI: https://doi.org/10.1007/978-3-030-74749-7_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-74748-0
Online ISBN: 978-3-030-74749-7
eBook Packages: MedicineMedicine (R0)