
Abstract
Considering the great demand for aesthetic treatments in the dental hard tissues, the wide availability of whitening gels and light sources, as well as the concern with the harmful effects that the increase in temperature can bring to biological tissues, this study verified the changes in temperature of dental enamel, root dentin and pulp chamber during the in-office tooth whitening procedure with different light sources and whitening gels. Sixty recently-extracted lower human incisor teeth were prepared and randomly distributed among six experimental groups for treatments: G1-red whitening gel without light; G2-green gel without light; G3-red gel and exposed to blue LED light; G4-red gel and exposed to green LED light; G5-green gel and exposed to blue LED lighting; G6-green gel and exposed to red laser light. During the treatments, as well as one minute after finishing them, the pulp and surface temperature variations of the enamel and root dentin were monitored using four thermocouples. The pulp temperature changes were 0.3 °C (G1), 0.8 °C (G2), 1.8 ± 0.5 °C (G3), 1.9 ± 0.5 °C (G4), 3.35 ± 0.6 °C (G5), 0.34 ± 0.1 °C (G6). The temperature differences at the interface between gel and enamel were 0.3 °C (G1), 0.9 °C (G2), 4.42 ± 0.9 °C (G3), 4.9 ± 1.1 °C (G4), 4.7 ± 1.1 °C (G5) and 1.5 ± 0.2 °C (G6). The root surface temperature differences were 0.3 °C (G1), 0.6 °C (G2), 3.05 ± 0.87 °C (G3), 2.6 ± 0.96 °C (G4), 3.8 ± 0.27 °C (G5) and 0.30 ± 0.1 °C (G6) and the temperature differences on the enamel side were 0.25 °C (G1), 0.46 °C (G2), 3.2 ± 0.7 °C (G3), 2.97 ± 0.6 °C (G4), 5.13 ± 1.2 °C (G5) and 0.70 ± 0.25 °C (G6). None of the configurations of the experimental groups causes permanent damage to the dental tissues, however the combination of green gel + blue LED should be avoided, since it is the one that promotes greater temperature increases in these tissues.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Tooth darkening can be caused by extrinsic (eating habits, smoking and use of medications, among others) or intrinsic agents (such as hypomineralization). The extrinsic pigments can bond to the dental surface and change the color of the teeth. Intrinsic factors are related to the formation of enamel and dentin, which are the most difficult to remove [1].
A whitening gel is basically composed of hydrogen peroxide or carbamide peroxide, one of the precursors of hydrogen peroxide. The whitening action of the gel occurs through its contact with the tooth, promoting an oxidation reaction by decomposition in water and highly reactive oxygen [2]. For the activation of whitening gels, the light sources are not indispensable, since the gels are activated by small temperature changes. However, they are widely used for decreasing the time of treatments. It is known that an increase in temperature of 5.5 °C is capable of causing damage to the pulp tissue, while an increase of 16 °C can lead to its complete necrosis [3]. Considering the periodontal ligament, a temperature augment of 10 °C cannot be acceptable [4]. Despite the protective function of the gel, there is still a probability of an increase in temperature above the limit of 5.5 °C in the pulp chamber, thus making studies on the interaction between light sources and gels indispensable [5].
Considering the variety of gels and light sources available for in-office tooth whitening, this study aimed to assess the surface temperature of the coronary enamel and root dentin, as well as the pulp temperature of human teeth subjected to the in-office tooth whitening process, using different light sources and whitening gels.
2 Material and Method
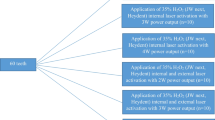
After approval of the present study by the Research Ethics Committee of the Federal University of ABC (CEP-UFABC, CAAE 49,456,215.7.0000.5594), a blind in vitro study was conducted in which 60 recently-extracted lower human incisor teeth were used. After cleaning, disinfecting and removing periodontal and pulp tissues, root chambers were filled with a thermo-conductive paste and the samples were randomly distributed into 6 different experimental groups (n = 10) for in-office dental bleaching treatments (Table 1).
In groups 1, 3 and 4, bleaching gel based on hydrogen peroxide (35%) with red thickener (Whiteness HP, FGM, Brazil) was used; in groups 2, 5 and 6, bleaching gel based on hydrogen peroxide (35%) with green thickener (Total Laser, Clean Line, Brazil) was used. Both gels were manipulated using 1 drop of thickener to 3 drops of hydrogen peroxide, according to the manufacturers’ instructions. Three light sources were used in the treatments. In groups 3 and 5, the Whitening Lase II device (DMC Equipamentos, Brazil) was used, which has 6 LEDs emitting blue light (λ = 470 ± 10 nm). During the experiments, only the central LED was used, the other LEDs were covered with black tape. In group 4, a non-commercial green LED was used (λ = 515 nm). In group 6, the Brite Laser Max device (Clean Line, Brazil) was used, (λ = 654 nm).
In the bleaching process, a uniform layer of approximately 1 mm of bleaching gel was applied to the vestibular region of the enamel of each sample. The samples were irradiated at a distance of 5 mm by the light source, 30 s after the application of the gel. The procedure for whitening consisted of alternating 1 min with the light source on and 1 min with it off, until a total of 2 min of irradiation, that is, in minutes 0–1, and 2–3, the light source remained on and, from 1 to 2 min, the light was off. After the treatment, the gel was removed from the surfaces by drying with absorbent paper.
During the treatments, as well as one minute after the end of them, the temperature monitoring was performed using a K-type thermocouple (chromel–alumel, 0.05 mm diameter, resolution of 0.2 °C e sensibility from 0.1–100 °C) and a NI USB9162 acquisition board (National Instruments, USA). Four channels were used to perform temperature measurements at four different points in the sample (Fig. 1).

Positioning of the four type-K thermocouples in a sample
The bleaching gels and light sources were also characterized regarding their absorption and emission wavelengths, respectively, using a spectrophotometer (Biospectro SP-220, Brazil) and a USB-650 Red Tide Spectrometer (Ocean Optics, EUA). The optical power of the light sources was measured using a powermeter (FieldMax II TOP, Coherent, USA).
The results obtained were statistically evaluated using Kruskal–Wallis and Student–Newman–Keuls, at a significance level of 5%.
3 Results
Figure 2 show the comparisons between the emission wavelength of the blue and green light sources and the absorbance of the red thickener, and between the emission wavelength of the blue and red light sources and the absorbance of the green thickener.

Absorbance of thickeners and emission wavelength of the three different light sources used in this study
The optical power values found were 44 mW for the blue LED, 27.8 mW for the green LED and 51.7 mW for the red laser. Table 2 summarizes the characteristics of the light sources used in the present study.
Immediately after the application of the gel on the tooth surface, it was observed a drop in temperature on the surface in contact with the gel (channel 1), followed by a drop in temperature in the other channels (Fig. 3). In groups 1 and 2, the temperature drop occurred throughout the acquisition period. In the other experimental groups, it was observed that channel 1 showed the highest temperature rise. The second largest temperature variation was observed in channel 3, while channels 0 and 2 showed the smallest variations.

Temperature variation observed in all channels of thermocouples, for all experimental groups
The means of temperature variations (ΔT) during irradiations for groups 1 to 6 and their respective standard deviation values are shown in Table 3. The temperature variations observed in groups 1 and 2 (without using a light source) were negative, resulting from the application of the bleaching gel. It was observed that there was no significant difference between the groups treated with gel with red thickener, regardless of the source of light used, for all regions evaluated. In this way, the light source does not interfere with pulp, enamel and periodontal temperature when used with a red thickener gel. However, group 5, which used gel with green thickener and blue LED, showed the highest temperature values when compared to the other experimental groups, except for channel 1. The group that used gel with green thickener and red laser was the which that presented lower temperature values when compared to all other experimental groups. Thus, for the gel with green thickener, it is observed that the light source is important at the temperatures generated during the whitening procedure, being statistically lower if red laser is used.
4 Discussion
In-office dental whitening with photoactivation leads to an increase in the surface temperature of the enamel and, consequently, to an augment in the temperature of adjacent structures, such as the root and pulp chamber. This phenomenon can be dangerous as it can lead to inflammation of dental and periodontal tissues, in addition to causing post-operative pain and sensitivity. Thus, the study of the temperature changes caused during tooth bleaching is important to prevent tissue damage from occurring due to the procedure [5]. It is known that reversible changes can happen to the pulp tissue when subjected to temperature variations greater than 3.3 °C, while temperature variations above 5.5 °C can cause loss of vitality and changes greater than 16 °C cause total necrosis of the pulp. Temperature variations above 10 °C in the periodontum can also lead to damage to these tissues (bone and periodontal ligament) [3, 4].
The in-office dental whitening procedure is a very common and widespread aesthetic procedure with studies evaluating the effects on the temperature of dental tissues older than 20 years [6]. Therefore, the literature is vast in showing temperature variations during tooth whitening with different light sources (halogen lamps, high and low power lasers, LEDs, plasm arc lamps, non-thermal atmospheric pressure plasmas, UV lamps) and distinct wavelengths, as well as diverse treatment protocols and gels of dissimilar colors and compositions. Still, different evaluation methodologies are used, such as thermocouples and thermographic cameras. Because of this, the reported results are conflicting and there are still doubts about the real effects of light absorption on the temperature generated during the procedure.
Another point to be emphasized is that, often, the dentist has different products for teeth whitening in his office, but not always the most adequate light source for a specific gel. Thus, clinical use of the same gel with different light sources is frequent, or vice versa. There are previously published works that tested activations of the same gel using different light sources [7, 8] and often use sources of the same central emission wavelength, but with different radiant powers, or compare LEDs with halogen lamps [9] or distinct laser systems [10, 11], which have very different collimation characteristics. Yet, although there are some studies that compare different gels with light sources of distinct emission wavelengths [12, 13], some of them used sources with characteristics dissimilar from each other (such as the comparison between a broadband LED with emission between 400 and 760 nm and a femtosecond laser with emission in 770 nm but with power density 4 times higher than the compared LED) [13]. Such equipment is difficult to access clinically and quite different from each other and, therefore, studies with more accessible sources are necessary. The justification for the use of different light sources, mainly related of the use of high power lasers that heat the irradiated surface [12] refers to the attempt to increase the effectiveness of diverse types of gels, with present distinct pH values; also, it is necessary to eliminate different types of pigments from the tooth surface, mainly those related to tetracycline, with is difficult to be removed in a clinical situation. Thus, the present study sought to assess whether the activation of commercially colored gels by economically accessible LEDs or low power laser of different emission wavelengths could alter the temperature generated during a standard clinical procedure, which could guide a professional regarding the safety of the procedure clinical even when the light source used is not the most absorbed by the gel in question.
During the clinical procedure, the temperature variation is influenced by several factors, such as the type of pigment contained in the gel, as well as the characteristics of the light source, irradiation time, the amount of the gel and thickness of the enamel and dentin. It is for this reason that, in the present study, human lower incisor teeth were used, as these are the teeth with less enamel and dentin thickness and, thus, the conduction of heat to the pulp tissue is facilitated [4]. Still, a thermally conductive paste was used inside the pulp chamber, in order to detect the highest possible temperature rise. Such detection attends as a safety parameter for future clinical extrapolation, considering that the pulp blood flow, as well as the presence of saliva and gingival fluid facilitate the loss of heat and, therefore, the temperatures detected in an in vivo study are certainly smaller than those of an in vitro model.
In this study, groups not exposed to any light source (G1 and G2) showed a sudden drop in temperature in the region in contact with the gel (channel 1) immediately after application, with no significant temperature increase during the acquisition period. This fact was expected, considering that the gel was stored in a closed environment protected from light, preventing its photodecomposition. Thus, it is likely that the gel is at a lower temperature than the dental element and, therefore, due to the heat transfer, a slight cooling of the tooth surface occurs when in contact with the whitening gel.
Comparing the results obtained from the G3 and G4, both with the use of red thickener, it is noted that, despite the lower power presented by the green LED (G4), the temperature increase on the gel surface was greater when irradiated by the green LED compared to irradiation by the blue LED. The temperatures on the enamel side and root dentin, however, were lower and, although the pulp temperature was slightly higher, the difference was not significant (about 0.05 °C). The greater heating of the gel in the group exposed to the green LED can be justified by the absorption spectrum of the thickener. The red thickener has its absorption peak at 516 nm, presenting an absorption about 50% lower near 450 nm, which consequently causes less heating when using light sources with wavelengths close to blue [14].
Group 5 showed the highest temperature differences in pulp, enamel side and root surface among all groups; this group also presented temperature slightly higher in gel surface when compared to G3 (red thickener and with irradiation of blue LED). The average pulp temperature difference obtained in G5 is sufficient to cause reversible damage to the pulp and therefore this association should not be used in a clinical procedure. The discrepancy between pulp, periodontal and enamel side temperature variations observed in the comparison between groups 3 and 5 suggests that the efficient absorption of light by the thickener (such as that which occurred in G3) resulted in less heat propagation to the adjacent tissues, whereas, in G5, there was no absorption of photons by the thickener and, consequently, they were transmitted to other regions, generating greater temperature increases in these regions. Such data reinforce, once again, that the association between green thickener and blue light should not be used clinically, as there is a risk of overheating regions distant from those of the irradiation site.
Group 6 (treated with green thickener gel and red laser) showed the lowest temperature variation among all irradiated groups. The green gel shows high absorption in the red region [5], with an absorption peak close to 630 nm; however, the absorption at 657 nm is lower, which justifies the variation temperature of only 1.5 °C. Yet, there was also no significant absorption by the adjacent tissues in the samples, which remained with variations below 1 °C. The use of gel with green thickener and 660 nm light proved to be an efficient method in a previous study carried out by Pleffken et al. [15], also showing low pulp temperature variation. The low risk of injury due to increased pulp temperature together with its good performance makes the treatment with the green gel followed by red light exposition as a good option for tooth whitening.
In the study, among all groups, only group 5 had an average pulp temperature difference above 3.3 °C. There were no samples in which the pulp temperature variation reached values above 5.5 °C; however, a single sample from group 3 and a significant number of samples from group 5 showed variations above 3.3 °C. The greatest temperature variation among all channels was approximately 5.1 °C, which also rules out possible lesions in the periodontal tissues, as these occur only with temperature variations above 10 °C.
The temperature differences obtained in this study can be considered low; however, in an in vivo study, these values may be even lower due to the arrangement of the teeth in the dental arch and the protection provided by the gingiva, which prevent the possible direct irradiation of the enamel side and root surface. Also, the presence of blood circulation and gingival fluid also contributes to the control of temperature [5].
5 Conclusions
It was possible to conclude that one of the experimental groups showed pulp temperature variations that present a potential risk to the vitality of the pulp and periodontal tissues. The treatment with green whitening gel associated with blue LED lighting, however, showed temperature rises in pulp chamber that can cause reversible damage to this tissue and, in this way, it is not recommended for clinical application. Among all configurations evaluated, the use of green thickener gel associated to red laser was the safest for clinical use. Based on the results achieved, in-office whitening is harmless as long as the proposed application times are respected.
References
Coutinho DS et al (2009) Comparison of temperature increase in in vitro human tooth pulp by different light sources in the dental whitening process. Lasers Med Sci 24:179–185
Nakamura T, Saito O, Ko T, Maruyama T (2001) The effects of polishing and bleaching on the colour of discoloured teeth in vivo. J Oral Rehabil 28:1080–1084
Zach L, Cohen G (1965) Pulp response to externally applied heat. Oral Surg Oral Med Oral Pathol 19:515–530
Eriksson A, Albrektsson T, Grane B, McQueen D (1982) Thermal injury to bone. A vital-microscopic description of heat effects. Int. J Oral Surg. 11:115–121
Kabbach W, Zezell DM, Bandeca MC, Pereira TM, Andrade MF (2010) An in vitro thermal analysis during different light-activated hydrogen peroxide bleaching. Laser Phys 20:1833–1837
Reyto R (1998) Laser tooth whitening. Dent Clin North Am 42:755–762
Coutinho DS, Silveira L, Nicolau RA, Zanin F, Brugnera A (2009) Comparison of temperature increase in in vitro human tooth pulp by different light sources in the dental whitening process. Lasers Med Sci 24:179–185
Mondelli RFL, Soares AF, Pangrazio EGK, Wang L, Ishikiriama SK, Bombonatti JFS (2016) Evaluation of temperature increase during in-office bleaching. J Appl Oral Sci 24:136–141
Carrasco TG, Carrasco-Guerisoli LD, Fröner IC (2008) In vitro study of the pulp chamber temperature rise during light-activated bleaching. J Appl Oral Sci 16:355–359
Sulieman M, Addy M, Rees JS (2005) Surface and intra-pulpal temperature rises during tooth bleaching: an in vitro study. Br Dent J 199:37–40
Sari T, Celik G, Usumez A (2015) Temperature rise in pulp and gel during laser-activated bleaching: in vitro. Lasers Med Sci 30:577–582
Gao Y, Zhao Z, Li L, Zhang K, Liu Q (2020) In Vitro Evaluation of the Effectiveness of Bleaching Agents Activated by KTP and Nd:YAG laser. Photodiagnosis Photodyn Ther 31:101900. https://doi.org/10.1016/j.pdpdt.2020.101900
Klaric E, Rakic M, Sever I, Tarle Z (2015) Temperature rise during experimental light-activated bleaching. Lasers Med Sci 30:567–576
Coutinho DS, Silveira L Jr (2006) Comparação dos Coeficientes de Absorção da Luz Emitida por um LED Verde e um LED Azul em um Espessante na Cor Vermelha. Rev Assoc Bras Odontol 2:12–13
Pleffken PR et al (2012) The Effectiveness of Low-Intensity Red Laser for Activating a Bleaching Gel and Its Effect in Temperature of the Bleaching Gel and the Dental Pulp. J Esthet Rest Dent 24:126–132
Acknowledgements
To PROCAD-CAPES (88881.068505/2014-01), National Institute of Photonics (CNPq/INCT 465763/2014-6), FAPESP (2017-21887-4), Multiuser Central Facilities (CEM-UFABC) and IPEN-CNEN/SP.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this paper

Cite this paper
Rodrigues, F.M., de Moura, L.A., Ana, P.A. (2022). Evaluation of Temperature Changes Promoted in Dental Enamel, Dentin and Pulp During the Tooth Whitening with Different Light Sources. In: Bastos-Filho, T.F., de Oliveira Caldeira, E.M., Frizera-Neto, A. (eds) XXVII Brazilian Congress on Biomedical Engineering. CBEB 2020. IFMBE Proceedings, vol 83. Springer, Cham. https://doi.org/10.1007/978-3-030-70601-2_154
Download citation
DOI: https://doi.org/10.1007/978-3-030-70601-2_154
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-70600-5
Online ISBN: 978-3-030-70601-2
eBook Packages: EngineeringEngineering (R0)