
Abstract
An essential element of making integrated care successful is an appropriate reimbursement instrument, such as bundled payments. They may differ in the scope of bundling (target population, time, sectors), as well as in how the price is set (negotiation, fixed). Yet, they always go along with a specific mind set of taking responsibility for the delivered health care and transparency on the own performance
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
There are no perfect reimbursement instruments. Selecting the most appropriate payment system depends on the intended delivery of care and the incentives set through the payment form (note: payment and reimbursement will be used interchangeably in the following). The variety of traditional reimbursement instruments can be conceptualised as a continuum of delegating risks from payer to provider. Despite their dissemination, traditional forms of paying providers often do not align well with new models of care (Stokes et al. 2018). Especially in the context of pursuing health policy objectives such as improving coordination and patient-relevant health outcomes, inherent disincentives of traditional instruments impede these policy aims and thus may not work very well (OECD 2016). In consequence, many health care systems have had difficulties in improving coordination and cooperation, especially for chronic diseases and for certain acute diagnoses that require attention from inpatient and outpatient care or from acute and rehabilitative care.
Bundled payments were created in response, where payers reimburse a determined amount for an entire episode of care instead of reimbursing individual services. The transfer of risk in the payment forms described above already goes along with a degree of bundling. In the scope of integrated care, however, bundled payments refer to payments that involve various providers within the defined patient pathway. The lump-sum payment thus has to be divided among the providers and facilities involved with delivering the care (Amelung 2019).
2 Reimbursement Instruments
Reimbursement instruments are often subject to conflicting goals. Paying for health care services has a distribution and a steering function. It is supposed to enable innovations, win acceptance and create transparency (Amelung 2019). For some health care systems, it is crucial for the payments to be easily administrable (Ibid.). In consequence, health care systems are increasingly concerned over the design and structure of their payment systems.
There is a firm belief in health economics that higher quality in health care correlates with lower costs (Porter & Teisberg 2006). What may seem counter-intuitive at first is linked to the notion that health care systems work differently from other industries, where paying a higher price is—at least to a certain degree—linked to receiving a higher quality product or service (hotels, cars, shoes, etc.). Instead, low quality in health care often correlates with high prices, such as a poorly managed diabetes patient or an insufficient surgery requiring rehospitalisation or additional treatment, to only name a few. In a similar manner, studies suggest that surgeries of artificial hip replacement that achieve a higher outcome quality are associated with lower long-term costs (Fahlenbrach et al. 2011). Payment systems should thus be designed that they acknowledge performance and quality without incentivising oversupply.
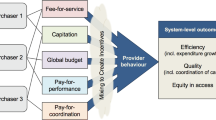
The way of paying for health care can be influenced mainly by three dimensions, (1) the degree of bundling, (2) setting the payment prospectively vs. retrospectively and (3) measuring the performance of the provider through data (Charlesworth et al. 2012). Besides this, every reimbursement system also generates unintended effects (Barnum et al. 1995). Various studies indicate that physicians, hospitals and other health care providers react to the way they are reimbursed for their services. The incentives tend to change the overall behaviour of stakeholders involved, affecting the efficiency, equity and quality of health outcomes as well as the adoption of new technologies (Breyer et al. 2013; Ellis 1998; Ex & Henschke 2019). When assessing the inherent (dis)incentives of a payment system, it may therefore be relevant to consider
-
the quality of delivered services,
-
the quantity of offered and utilised services,
-
the average costs per case,
-
the access and number of at-risk population for payer and provider, as well as
-
the sharing of risks between payer and provider (Schmid 2020).
The variety of established payment mechanisms can be conceptualised and differentiated along a risk continuum delegated from payer to provider. The risks related to an individual utilising health care services traditionally lie with the payer. In such scenario, health care services are reimbursed through a fixed salary. While such a payment serves as an incentive for providers to keep their patients healthy, it may also lead to an inefficient use of resources and long waiting times.
Compared to a salary, reimbursing services through fee-for-service slightly increases the risk for the provider, as the reimbursement includes further expenses such as investment and running costs of an office and doctor’s needs such as needles. The aim of fee-for-service is to increase productivity and to reimburse performance, even though it may come along with a substantial rise in volumes (Amelung 2019).
A further bundling of the payment is the reimbursement through diagnosis-related groups (DRGs) that include all services of one provider related to a defined disease. Besides staff and doctor’s needs, this also covers for possible instruments and machines necessary for diagnosis and treatment. DRG systems are often used for inpatient and outpatient hospital care and usually include rehospitalisation for the same diagnosis for a certain time after discharge (Quentin et al. 2013).
In order to also incentivise better quality, concepts such as value-based care (Porter and Teisberg 2006), pay-for-performance and performance-based reimbursement (Forsberg et al. 2001) have been put forward by academia and in policy-making. With the aim to improve the value of care for the money spent on it, value-based payments for instance add premiums for top outcomes and/or deductions for outcomes below a defined threshold.
The highest form of risk delegation can be observed in capitation, where the entire risk for a defined population is handed to a provider. The group of people for whom services are bundled can vary between all insured of a region or a particular group of insured, such as the patients with the same disease (Schmid 2020). The extent of included services differs, but theoretically can include all services necessary for the care of the insured person, “including preventive and inpatient services as well as annex services” such as laboratory and radiology services or drugs (Amelung 2019). In distinction to capitation, global budgets work similarly but are paid independent of the actual volume provided (OECD 2016).
3 Reimbursing Integrated Care
Opposed to conventional health care, integrated care focuses on holistic care to improve the person’s well-being instead of an isolated illness (Goodwin et al. 2017). Many reimbursement instruments, in contrast, are linked to a particular treatment. Integrated care is often delivered in a team and organised around the patient pathway. The patient pathway is, however, often reverse to the division of health care sectors. Since the different reimbursement systems often only apply to one health care sector or only to medical services, actors are incentivised to focus on their individual element of care delivery instead of a patient-centred process. On a larger scale, this also results in diverging interests between sectors as well as between health and social care (SVR Gesundheit 2018). Furthermore, integrated care often takes place in addition to or besides standard care. This suggests that integrated care becomes necessary due to disincentives of payment systems that allow but do not facilitate cooperation or coordination nor the delivery of services as a team across providers or sectors.
In order to make integrated care work, it thus requires other concepts of reimbursement. Bundled payments—also called episode-based payments—have been developed for integrated care. While many reimbursement systems focus on one narrow specialty or organ system, bundled payments approach it through the medical condition as perceived by the patient and include common comorbidities and related complications (Porter & Kaplan 2015). Also, the treatment with medications can be incorporated into the bundle (Amelung 2019). The aim is to better integrate the care process by improving patient experiences and health outcomes as well as to reduce avoidable ill health and costs, for instance through unnecessary hospitalisation (Charlesworth et al. 2012).
Bundled payments for integrated care are defined as a “single payment to cover the care for the condition or population segment over a specified time period”, involving inpatient, outpatient and rehabilitative care (Porter & Kaplan 2015). Being paid for a defined episode of care, this allows providers to jointly assume accountability and deliver health care together. The reimbursement incentive works by paying average costs instead of actual expenses per patient. Providers thus face the risk to be reimbursed less than their expenses or instead can keep surpluses when providing care efficiently (Struijs et al. 2020). In consequence, bundled payments are thought to not lead to unnecessary rise in volumes but instead to incentivise cost-efficient procedures. What must also be considered when designing bundled payments is that usually two purchasing markets exist that influence behaviour, firstly on the level of the care group and secondly on the level of the individual provider (Struijs et al. 2017).
The reimbursement price can be set through various means. It can be based on price negotiations or is fixed. Bundled payments are often determined in advance representing the expected average costs—in this case belonging to so-called prospective payment instruments. Main challenge in this case is to determine the expenses for an episode of care, since health care providers usually do not assess costs from this perspective and may not even have applicable data. Some models therefore use evidence-based guidelines to set the expected consumption of resources and link compensation to these (Amelung 2019; Rosenthal 2008). In some cases, prices are also determined retrospectively, with an upfront fee-for-service payment to individual providers and a retrospective reconciliation period (Struijs et al. 2020).
The large difference among bundled payments is their scope. Bundled payments can include advanced value-based models or instead provide mostly the same health care as in other fields. It is thus most relevant to align the bundled payment to the health care aims. The following table differentiates four hypothetic set-ups of integrated care that demand for quite different reimbursement approaches within bundled payments (Table 22.1).
As this depicts, one aim of an integrated care process may be to yield multi-professional cooperation and coordination, for instance, in the case of a diagnosis such as breast cancer. The bundled payment can thus be closely linked to the defined processes and mandate a specific person that assists with the coordination (case management). Similar cases could be stroke, acute cardiac diseases and certain cases of multi-morbidity, for instance, in combination with dementia. Depending on the circumstance, adding a value-based approach to the bundling may be relevant to incentivise investments for a better quality of care.
The bundled payment may look quite differently when piloting an innovative technology in a network of health care professionals, for instance, a digital health application where no reliable predictions exist on the quantity of use. An outcome-based approach seems most important here to evaluate the diffusion of the technology. When the challenge is rather the quality of use, for instance, in an innovative technology aimed at improving adherence, risk-sharing bundled payments may be applicable, where tiers are linked to the level of adherence in real-world use. As this suggests, the variety of bundled payments is large, so that the following will look deeper into the adoption and use of specific bundled payments in practice.
4 Bundled Payments in Use
A number of health care systems use some kind of bundled payment to reimburse integrated care. A systematic review on this matter found 32 international examples of reimbursing integrated care, with the majority described in the United States (n = 15), followed by the UK (n = 5), Canada (n = 2), Germany (n = 2), the Netherlands (n = 2) and other European countries (n = 6) (Stokes et al. 2018). Struijs et al. additionally found initiatives in Taiwan and New Zealand (2020). Most of the initiatives focus on one condition, procedure or treatment (Struijs et al. 2020). Bundled payments have been established mostly for specific disease pathways, such as for the chronic care in diabetes and different forms of cancer as well as the acute episodes of care in stroke, total hip and knee replacement, congestive heart failure and sepsis. They can thus be implemented for a mainly outpatient setting (diabetes care) as well around inpatient and post-acute care (hip replacement).
In addition to these contracts between providers and health care systems, bundled payments are also used in some systems for treatments that patients directly pay for, such as in vitro fertilisation and plastic surgery (Porter & Kaplan 2015). These payments rather resemble other individual purchasing decisions and will thus not be the focus of this paper.
A relevant requirement for bundled payments to work is the availability of data. Most bundled payments are based on a performance and a quality measurement. Despite having been discussed for some time, bundled payments are hence becoming increasingly relevant in times of digitalisation as they are more easily implementable. This can be the case for an easy data exchange between providers through an integrated patient record, through digital billing, through integrated process management and performance measurement. Data is thus a relevant element of executing and operating bundled payments in use.
Two cases of bundled payments will be displayed in more detail in the following (for a more detailed description of the Dutch case, refer to HBIC Vol. 2, Chapters 17 or 18).
4.1 Case Study I: Disease Management of Diabetes in the Netherlands
Similar to various industrial countries, the Netherlands is faced with a rising burden of chronic diseases. Four per cent of the Dutch population are diagnosed with diabetes, which is likely to increase in the coming years. With a lack of coordination between different sectors and professional groups, the Dutch health care system was not equipped to take care of chronic patients, especially so with a rising prevalence of multi-morbidity and complex health care needs among the population (Struijs et al. 2017).
In response, the Netherlands Ministry of Health, Welfare and Sport developed the first integrated care programme focussing on diabetes care that was aimed at improving the quality of care, in particular confining quality deviation, and to improve effectiveness while ensuring affordability (Ibid.). A bundled payment was initiated in 2007, first in an experimental design and by 2010 on a more permanent basis, that contracted a single service package with a group of health care providers (the Dutch abbreviation is keten-dbc) (Struijs et al. 2012). These care groups are legal entities that coordinate and execute the care process from diagnosis to after care and contract with health insurers. (Co-)owner of these care groups are often general practitioners, with practice nurses and a variety of health care professionals such as dieticians and podiatrists working as chain partners (Busetto et al. 2015). By 2010, a hundred care groups were operating in diabetes care that covered around 85–90% of all diabetes patients in the Netherlands (Struijs et al. 2012).
The bundled payments were established as packages, where the content and price of the comprehensive package are negotiated. In contrast to bundling downstream after inpatient care by limiting the need of hospital readmissions, the aim here is to focus upstream on improving primary care and thereby not requiring expensive specialist outpatient care and hospitalisation (Amelung 2019, Struijs et al. 2012).
4.2 Case Study II: The Bundled Payments for Care Improvement (BPCI) Initiative by Medicare in the United States
Medicare traditionally reimburses providers for each service individually (fee-for-services). As has been described above, it noticed that this can lead to fragmented care with too little coordination, awarding quantity instead of quality (Centres for Medicare and Medicaid Services, CMS 2020a). The Centre for Medicare and Medicaid Innovation was thus established in 2010 to test innovative payment and care delivery models (Micklos et al. 2020).
It developed the Bundled Payments for Care Improvement (BPCI) Initiative in 2013, initially running through September 2018 (CMS 2020b), NEJM Catalyst (2018). In 2015, the Medicare Access and CHIP Reauthorization Act additionally created financial incentives for providers to participate in these advanced payment models. The BPCI offered four models of participation, depending on the area of service delivery. Target prices were set prospectively based on the expected costs of services and items during the episode of care. The models varied in funding the expected costs on the historical performance of the provider, on local or regional spending, or on a combination thereof (CMS 2020a).
However, some models would be considered as regular diagnosis-related groups from international perspective, since the United States does usually not include physician salaries or readmissions in their DRGs, while many other health care systems do (Quentin et al. 2013). Only the most comprehensive Model 2, involving Part A and Part B services for the initial hospital care, all post-acute care and readmissions (Romley and Ginsburg 2018), would be considered as bundled payment in the context of this paper. The model differed in the scope of rehospitalisation, either ending 30, 60 or 90 days after hospital discharge (CMS 2020b). The provider payment in Model 2 was actual expenditures were reconciled retrospectively against the episode’s target price (CMS 2020c).
A total of 699 participants were involved in BPCI Model 2 (Centres for Medicare and Medicaid Services 2020b), equivalent to around 85% of the provider groups from all models (Romley and Ginsburg 2018). Of the participants triggering an episode of care in Model 2, almost two thirds were acute care hospitals and one third physician group practices. In contrast to the approach taken in the Netherlands, the BPCI initiative involved up to 48 different medical and surgical conditions (Chen et al. 2015). Awardees could select the clinical episodes they participated in. Due to the aim of the Innovation Centre to test new models of care, provider groups could try various model definitions that best fit to their institution.
Based on the experiences made above, CMS developed the BPCI advanced, which has been running since January 2018. It involves a single retrospective bundled payment with a 90-day episode duration. Providers receive payments when their total spending for the episode lays below the determined target price. Additionally, prices can be adjusted for quality indicators by 10% (CMS 2020c). There are 29 inpatient and three outpatient clinical episodes that providers can sign up for (CMS 2020b). It has attracted 1299 participating providers as of September 2019.
5 Effects of Bundled Payments
The effects and eventually the success of managed care-instruments largely depend on their specific design. Various studies thus investigate in what circumstances bundled payments lead to the intended effects. Three different groups of effects are plausible, firstly yielding better health care delivery including better patient-reported outcomes, secondly improving the work of health care professionals and thirdly to reduce costs. A current meta-analysis found 35 papers empirically analysing the impact of 11 bundled payment initiatives (Struijs et al. 2020). All of these used an observational design, most often with a pre- and post-measurement without control group, some also used a difference-in-difference approach (Ibid.).
Some studies suggest that integrated care with bundled payments was associated with aligning health care delivery along patient pathways and with protocol adherence (Struijs 2017). A first step towards achieving may be a higher transparency of health care quality, which was studied and found by Tol et al. (2013). However, results are mixed mostly between positive effects and no effects when analysing the impact on quality of care as a whole (Struijs et al. 2020). Bundled payments involve the willingness to deliver health care in teams and cooperate with other professions, in particular also new professional roles in the clinical pathway. Ruggeri et al. (2018) found an association between high levels of patient satisfaction and involvement of new professional roles for the case of breast cancer and, in the case of countries with innovative models of health care delivery, also for type 2 diabetes. Overall, patient experiences are rarely measured in empirical studies on bundled payments (Struijs et al. 2020). Struijs et al. (2017) also found increased training of subcontracted providers in the studied integrated care programmes, which was aimed to facilitate protocol-driven work processes.
Literature has confirmed that bundled payments are associated with increased multidisciplinary cooperation (Struijs 2017; Tol et al. 2013). Especially younger generations of physicians have an overall higher expectation in working together in teams, which suits well for integrated care contexts. However, integrated care and bundled payments also have a competitive component included, through transparency on treatment outcomes and being accountable for the own (measured) results. Furthermore, bundled payments may bring a higher efficiency of care, while the defined processes may go along with an increase in administration (Tol et al. 2013). The additional administration and management in integrated care can be addressed through digital tools to connect health professionals in an intelligent way. Studies suggest that implementing interoperability between the patient data banks to allow data exchange and analysis is currently one of the main challenges (Busetto et al. 2015).
Lastly, integrated care has been often connected to the expectation to reduce costs. This can be achieved through reducing unnecessary hospitalisation and readmissions as well as by reducing post-discharge costs. Iorio et al. studied the effects of the Model 2 bundled payment in the US Medicare programme for total joint replacement implemented in a tertiary urban academic medical centre and observed a decrease of discharges to inpatient facilities from 71 to 44% (2016). Navathe et al. studied the same BPCI Model for lower extremity joint replacement in a US health system, finding that average Medicare episode expenditures declined by 20.8% over the 3942 patients treated between 2008 and 2015 (2017). Evaluating the Netherlands, de Bakker et al. found large price variations among care groups that could not be fully explained by the amount of care provided (de Bakker et al. 2012). The Netherlands were the only country in a meta-analysis where medical spending increased in the first two years of implementing the Dutch bundled payment (Struijs et al. 2020). The factors of unnecessary hospitalisation and readmissions have a cost-component as well as a quality of life-component. Busetto et al. (2015) found in their interviews that some payers were mainly interested in costs, while other payers focused on costs in addition to quality of care.
Overall, a clear distinction between the effect caused by the model of integrated care vs. caused by the payment is—in addition to all scientific considerations on causality—barely possible. However, integrated care has often been not very successful when attempted through standard payment instruments. If the bundled payment is considered a requirement or auxiliary for the model of care to work, the described effects are achieved through integrated care paid by bundled payments.
6 Discussion
An essential element of making integrated care successful is an appropriate reimbursement instrument, such as bundled payments. They may differ in the scope of bundling (target population, time, sectors), as well as in how the price is set (negotiation, fixed). Yet, they always go along with a specific mindset of taking responsibility for the delivered health care and transparency on the own performance.
The basic notion of integrated care is to define patient pathways along an episode of care. This can be understood as translating evidence-based guidelines into a clinical protocol for the praxis of how to provide health care with a certain diagnosis. The assessment, pondering and negotiation on how to steer patients best through the care remains as important as ever and is a first relevant aspect of integrated care. Having come to an agreement on that, the merit of bundled payments is that they delegate accountability, yet only for the scope of personal and organisational expertise. Too often, it has been attempted to convince providers to follow a defined pathway or protocol through narrow-minded quality management or legal threats. The advantage with bundled payments is that they do not only mandate the content of health care provision, but link this to responsibility and reimbursement. One can understand bundled payments as a response to the disincentives of existing reimbursement systems; overgeneralising, fee-for-service lead to waste, DRGs cause egoisms, and capitation is often too broad. Bundled payments are not perfect, but they do achieve quite well to honorary those who deliver an excellent performance (OECD 2016).
The controversial analyses in how far bundled payments led to the wanted effects when applied suggest that their success largely depends on the specific design. If it is not mandatory to participate in them, one relevant achievement in this context is that providers actually participate, as bundled payments are often an alternative to standard care. Examples in the United States describe that despite establishing bundled payments, some providers perceived many barriers such as administrative burdens and state regulatory uncertainty and thus did not sign in (Ridgely et al. 2014) and facing substantial challenges in implementation, such as the complexity of the particular bundled payments that is built on the existing fee-for-service payment (Hussey et al. 2011). Moreover, what has to be considered is how to correct other fields of health care financing for the bundled payments. This again is especially the case when bundled payments are added on top of other reimbursement instruments.
Despite the relevance of integrated care in health care systems, bundled payments have not been broadly adopted. One central reason may be the current payment mechanisms that do not incite providers to change and act in more uncertainty. Patients may be interested, but there are often large information deficits, especially when patients are not used to being addressed to enter into different model of care. Main interest of integrated care lies with the payer, while the incentive to save expenditures promptly may sometimes be in the way to develop integrated care. Therefore, the main question that remains is how to incentivise health care systems to foster integrated care. It may thus make sense as health system to consider bundled payments as sole payment for specific public health relevant diagnoses.
References
Amelung, V. (2019). Healthcare management. Berlin, Heidelberg: Springer.
Barnum, H., Kutzin, J., & Saxenian, H. (1995). Incentives and provider payment methods. International Journal of Health Planning and Management, 10(1), 23–45.
Benstetter, F., Lauerer, M., Negele, D., & Schmid, A. (2020). Prospektive regionale Gesundheitsbudgets. Internationale Erfahrungen und Implikationen für Deutschland. Heidelberg: medhochzwei.
Breyer, F., Zweifel, P., & Kifmann, M. (2013). Gesundheitsökonomik. Berlin, Heidelberg: Springer.
Busetto, L., Luijkx, K., Huizing, A., & Vrijhoef, H. (2015). Implementation of integrated care for diabetes mellitus type 2 by two Dutch care groups: A case study. BMC Family Practice, 16(105).
Centers for Medicare & Medicaid Services, CMS. (2020a). Bundled payments for care improvement (BPCI) initiative. Available under https://innovation.cms.gov/innovation-models/bundled-payments. Last accessed on March 25, 2020.
Centers for Medicare & Medicaid Services, CMS. (2020b). CMS innovation center. Episode payment models. Available under https://innovation.cms.gov/innovation-models/bundled-payments. Last accessed on April 9, 2020.
Centers for Medicare & Medicaid Services, CMS. (2020c). Quality measures fact sheet. Available under https://innovation.cms.gov/files/fact-sheet/bpciadvanced-fs-nqf1550.pdf. Last accessed on April 9, 2020.
Charlesworth, A., Davies, A., & Dixon, J. (2012). Reforming payment for health care in Europe to achieve better value. Nuffield trust research report.
Chen, L., Meara, E., & Birkmeyer, J. (2015). Medicare’s bundled payments for care improvement (BPCI) initiative: Expanding enrollment suggests potential for large impact. The American Journal of Managed Care, 21(11), 814–820.
De Bakker, D., Struijs, J., Baan, C., Raams, J., de Wildt, J. E., Vrijhoef, H., & Schut, F. (2012). Early results from adoption of bundled payments for diabetes care in the netherlands show improvement in care coordination. Health Affairs, 31(2), 426–433.
Ellis, R. (1998). Creaming, skinping and dumping: Provider competition on the intensive and extensive margins. Journal of Health Economics, 17(5), 537–555.
Ex, P., & Henschke, C. (2019). Changing payment instruments and the utilisation of new medical technologies. The European Journal of Health Economics, 20, 1029–1039.
Fahlenbrach, C., et al. (2011). Bonus ohne Extrakosten. Gute Ergebnisse bei Hüft-OPs senken die Behandlungskosten im Folgejahr. Gesundheit und Gesellschaft, 9, 34–39.
Forsberg, E., Axelsson, R., & Arnetz, B. (2001). Financial incentives in health care. The impact of performance-based reimbursement. Health Policy, 58(3), 243–262.
Goodwin, N., Stein, V., & Amelung, V. (2017). What is integrated care? In V. Amelung, V. Stein, N. Goodwin, R. Balicer, E. Nolte, & E. Suter (Eds.), Handbook integrated care. Cham: Springer.
Hussey, P., Ridgely, S., & Rosenthal, M. (2011). The PROMETHEUS bundled payment experiment: slow start shows problems in implementing new payment models. Health Affairs, 30(11), 2116–2124.
Iorio, R., Clair, A., Inneh, I., Slover, J., Bosco, J., & Zuckerman, J. (2016). Early results of medicare’s bundled payment initiative for a 90-day total joint arthroplasty episode of care. Health Affairs, 31(2), 343–350.
Micklos, J., Pierce-Wrobel, C., & Traylor, J. (2020). The center for medicare and medicaid innovation can be a powerful force to accelerate change, but not without key reforms. Health Affairs Blog.
Navathe, A., Troxel, A., Liao, J., Nan, N., Zhu, J., Zhong, W., & Emanuel, E. (2017). Cost of joint replacement using bundled payment models. JAMA Internal Medicine, 177(2), 214–222.
NEJM Catalyst. (2018). Innovations in care delivery. What are bundled payments? Available under https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0247. Last accessed on March 19, 2020.
OECD. (2016). Focus on better ways to pay for health care. OECD White Paper.
Porter, M. E., & Teisberg, E. O. (2006). Redefining health care: Creating value-based competition on results. Boston: Harvard Business School Press.
Porter, M. E., & Kaplan, R. S. (2015). How should we pay for health care? Working paper from the Harvard Business School (15-041). Available under https://www.researchgate.net/profile/Sarah_Blackstone/publication/296618989_What_Does_the_Patient_Want/links/5728f84508ae057b0a033c9a/What-Does-the-Patient-Want.pdf. Last accessed on March 25, 2020.
Quentin, W., Scheller-Kreinsen, D., Blümel, M., Geissler, A., & Busse, R. (2012). Hospital payment based on diagnosis-related groups differs in Europe and holds lessons for the United States. Health Affairs, 32(4), 713–723.
Ridgely, S., de Vries, D., Bozic, K., & Hussey, P. (2014). Bundled payment fails to gain a foothold in California: The experience of the IHA bundled payment demonstration. Health Affairs, 33(8), 1354–1352.
Romley, J., & Ginsburg, P. (2018). Improving bundled payments in the Medicare program. USC-Brookings Schaeffer Initiative for Health Policy. Available under https://www.brookings.edu/wp-content/uploads/2018/05/bundling-white-paper_formatted-ad-5-22-18.pdf. Last accessed on April 9, 2020.
Rosenthal, M. (2008). Beyond pay for performance—Emerging models of provider-payment reform. The New England Journal of Medicine, 359(12), 1197–1200.
Ruggeri, M., Drago, C., Moramarco, V., Coretti, S., Köppen, J., Islam, M., et al. (2018). New professional roles and patient satisfaction: Evidence from a European survey along three clinical pathways. Health Policy, 122(10), 1078–1084.
Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen. (2018). Bedarfsgerechte Steuerung der Gesundheitsversorgung. Available under https://www.svr-gesundheit.de/fileadmin/user_upload/Gutachten/2018/SVR-Gutachten_2018_WEBSEITE.pdf. Last accessed on March 21, 2020.
Stokes, J., Struckmann, V., Kristensen, S., van Ginneken, E., Tsiachristas, A., van Mölken, M., & Sutton, M. (2018). Towards incentivising integration: A typology of payments for integrated care. Health Policy, 122(9), 963–969.
Struijs, J., de Jong-van, T. J., Lemmens, L., Drewes, H., de Bruin, S., & Baan, C. (2012). Three years of bundled payment for diabetes care in the Netherlands. Impact on health care delivery process and the quality of care. Bilthoven: National Institute for Public Health and the Environment.
Struijs, J., Drewes, H., Heijink, R., & Baan, C. (2017) Netherlands: The potentials of integrating care via payment reforms. The case of dutch diabetes care. In V. Amelung, V. Stein, N. Goodwin, R. Balicer, E. Nolte, & E. Suter (Eds.) Handbook integrated care. Cham: Springer Nature.
Struijs, J., de Vries, E., Baan, C., van Gils, P., & Rosenthal, M. (2020). Bundled-payment models around the world: How they work and what their impact has been. commonwealth fund, April 2020.
Tol, J., Swinkels, I. C. S., Struijs, J. N., Veenhof, C., & de Bakker D. H. (2013). Integrating care by implementation of bundled payments: Results from a national survey on the experience of Dutch dietitians. Int J Integr Care. Oct–Dec.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ex, P. (2021). Reimbursing Integrated Care Through Bundled Payments. In: Amelung, V., Stein, V., Suter, E., Goodwin, N., Nolte, E., Balicer, R. (eds) Handbook Integrated Care. Springer, Cham. https://doi.org/10.1007/978-3-030-69262-9_22
Download citation
DOI: https://doi.org/10.1007/978-3-030-69262-9_22
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-69261-2
Online ISBN: 978-3-030-69262-9
eBook Packages: Business and ManagementBusiness and Management (R0)