
Abstract
Early mobilisation is a promising intervention in the intensive care unit with the potential to improve short- and long-term outcomes for patients requiring support for a critical illness. However, early mobilisation is complex with significant variation in uptake and practice around the world. Multiple studies have attempted to address barriers and facilitators to early mobilisation, and a variety of strategies have emerged to support the implementation of this intervention into clinical practice. This chapter summarises the current evidence relating to the effects of early mobilisation in the intensive care unit. It also provides a summary of the factors impacting implementation and provides an overview of the approaches and resources available to support successful translation to clinical practice. Finally, consideration is given to the future of early mobilisation and how this intervention may be delivered and prescribed differently as further evidence and resources emerge.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Intensive care
- Critical illness
- Early mobilisation
- Rehabilitation
- Implementation
- Intensive care unit-acquired weakness
What Is the Impact of Implementing Early Mobilisation in the Intensive Care Unit?
As critical care survivorship improves, research has increasingly focused on interventions which may prevent or manage critical illness-related morbidity [1]. Physically, intensive care impacts negatively on muscle and nerve structure and function with the literature supporting an incidence of intensive care unit-acquired weakness (ICU-AW) more than 50% in patients requiring prolonged mechanical ventilation [2, 3]. There is an association between ICU-AW and poorer outcomes including mortality, length of stay and physical function [3,4,5]. Early mobilisation (EM) has gained significant interest due to its potential to attenuate the negative effects of bed rest and thus improve service-centred and patient-centred outcomes. Whilst many studies report findings related to implementation of EM interventions, there remains no consistent definition of the term [6, 7]. Mobilisation “facilitates the movement of patients and expends energy with a goal of improving patient outcomes” [8]. Mobilisation can encompass a variety of interventions and forms one component of early rehabilitation which may also include treatments to address areas such as cognition, speech, swallowing and inspiratory muscle strength [8, 9]. In the intensive care unit (ICU), where traditionally patients have been managed with sedation and bed rest, the implementation of any mobilisation intervention during the critical illness period may have been considered early. However, it may be important to distinguish mobilisation delivered at different time points during critical illness. Mobilisation delivered early, within 48–72 hours of admission, may have the potential to stimulate muscle regeneration and consequently prevent or reduce the severity of sequelae of critical illness such as intensive care-acquired weakness (ICU-AW ) and delirium [10,11,12]. It may also contribute to reduced mechanical ventilation (MV) time, length of stay (LOS) and improved long-term outcomes for critical illness survivors [8, 12]. Conversely, the rapid onset of muscle degeneration in critically ill patients means that physical rehabilitation applied later in or after an ICU admission aims to reverse impairments to improve outcomes. Selection of EM modalities for each individual patient depends upon medical stability and whether the patient can or cannot actively participate in mobilisation [13, 14].
For patients unable to actively participate in EM, neuromuscular electrical stimulation (NMES) , cycling and passive movements are forms of rehabilitation that may be utilised in the ICU [14]. Reviews of clinical trials demonstrate that NMES may improve impairments such as muscle strength; however, there is no clear evidence for the impact of NMES on long-term outcomes [15, 16]. Two recent RCTs have investigated the effects of cycling in addition to early rehabilitation and have not demonstrated any significant changes in functional capacity, independence at hospital discharge, global muscle strength, ventilator-free days or health-related quality of life at 6 months [17, 18]. The feasibility of cycling has been demonstrated via pilot RCT, and ongoing trials are being completed in this area (NCT03471247) [19, 20]. As evidence emerges, systematic review which separately evaluates the effects of cycling and passive movement interventions may be warranted. To date, there is no available meta-analysis of the incidence of adverse events related to NMES or cycling in critically ill patients. Table 2.1 provides a summary of recent publications which have detailed the effects of passive cycling and EMS in critically ill patients.
For patients who are able to participate in active therapy, EM focuses on active exercises and functional retraining activities such as active exercises in bed or in the chair (aiming to improve muscle strength and joint mobilisation), sitting, balance, transfers, standing and walking. Multiple systematic reviews have been undertaken examining the short- and long-term effects of active participation in EM (Table 2.2). Results indicate that active participation in early rehabilitation may result in reduction in incidence of ICU-AW , hospital and ICU LOS whilst improving functional status at discharge and long-term quality of life. Three systematic reviews suggest that interventions delivered earlier during the ICU stay may be more beneficial than those delivered later during admission [21,22,23]. Ding et al. [23] identified via network meta-analysis that ideal initiation of EM is within 48–72 hours of mechanical ventilation [21,22,23]. Additionally, a systematic review of 10 RCTs examining physical rehabilitation interventions delivered after ICU discharge, either in hospital or after hospital discharge, to patients who received mechanical ventilation has demonstrated moderate evidence that these programmes do not make a difference to quality of life [24]. Meta-analysis examining safety of active EM interventions in the ICU has demonstrated that potential safety events are low and events associated with consequences are rare [25]. Based on the currently available evidence of the risks and benefits of a variety of EM interventions, clinicians should focus on delivery of mobilisation activities delivered as early as possible during the ICU admission, with active participation wherever possible.
Why Is Early Mobilisation Challenging to Implement into Clinical Practice in the Intensive Care Unit?
EM is a complex intervention and has been consistently difficult to implement in ICU in both clinical trials and clinical practice. Whilst there are concerns for patient’s safety and physiological stability, the main reported barriers to EM, such as sedation and staff levels, may be managed with multidisciplinary team input and coordination [26].
In a multicentre observational study of EM in critically ill patients, during 1288 planned early mobilisation episodes in patients on mechanical ventilation, no mobilisation occurred in 1079 (84%) of these episodes despite the presence of dedicated physical therapy staff. The main reported barrier to EM in the first 7 days after enrolment was intubation and sedation [2]. At day 7, the reported barriers also included agitation and weakness. However, EM has been shown to be safe and feasible in intubated patients and can occur in conjunction with sedation minimisation or disruption, so why does this continue to be a barrier to implementation in the clinical setting?
First, EM is easier to implement in an ICU that has a culture that prioritises and values rehabilitation and functional recovery [2]. In this case, maximising the opportunities to safely implement EM occurs with discussion on the multidisciplinary round, accompanied by clear goal setting based on the patient’s current status and with a plan to implement EM as a coordinated effort by the ICU team [12]. The type and timing of EM, as well as the specific staff and equipment required to achieve the planned activity, are all planned in advance with buy-in from the medical staff, nursing staff and physiotherapists, as well as any other staff specific to achieving that goal.
Patients have reported that during the early phase of critical illness, and particularly the first sessions of EM in ICU, they prefer a paternalistic approach to rehabilitation where the activities and the process of EM are directed by the staff delivering EM [27]. It is important to have one person leading and coordinating the EM to ensure the patient can focus clearly on instructions and to maximise safety [28].
What Solutions Are Available to Support Implementation of Early Mobilisation in the Intensive Care Unit?
The translation of research evidence into clinical practice remains a challenging aspect of evidence-based care in the intensive care unit [33, 34]. Early mobilisation is no exception with multiple observational studies demonstrating that physical activity levels in the critically ill remain very low [2, 35,36,37]. However, a number of recent publications provide potential solutions to support evidence translation and implementation of EM into daily clinical practice.
The Society of Critical Care Medicine (SCCM), American Thoracic Society & American College of Chest Physicians (ATS), the German Society of Anesthesiology and Intensive Care Medicine (DGAI) and the New South Wales Agency for Clinical Innovation (ACI) have all recently published clinical practice guidelines (CPGs) which make recommendations related to EM in the ICU [8, 28, 38, 39]. All of these CPGs support implementation of EM based on reviews of the current evidence. The recommendations of these guidelines are summarised in Table 2.3.
Both the SCCM and ATS guidelines utilised the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology for guideline development [40]. This methodology requires a detailed assessment of the quality and certainty of the research evidence underpinning the recommendations including the risk of bias, effect size and consistency between studies with meta-analysis of results undertaken where possible. This detailed analysis revealed that whilst there is a significant body of evidence supporting the potential of EM to improve outcomes such as decreased mechanical ventilation time, improved functional independence at hospital discharge and increased strength, there remain significant limitations to the evidence for EM. There is a lack of Phase 3 evidence from large randomised controlled trials (RCTs) with the evaluation of all relevant outcomes including adverse events. Importantly, a well-powered Phase 3 RCT is required to evaluate long-term safety outcomes including mortality. There is inadequate evidence available to guide recommendations related to dosage, intervention selection or the identification of responders and nonresponders. The contrast in strength of recommendation made by the ACI guideline is likely related to the evaluation of the evidence using the NHMRC levels of evidence which classifies studies based on design only without a detailed assessment of other factors which effect quality.
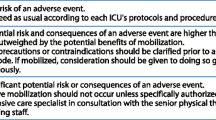
Whilst there are important limitations to the recommendations provided by existing CPGs , clinicians can utilise these documents to support changes to clinical practice. It is important to recognise that these recommendations are made via expert consensus based on careful evaluation of the risks and benefits in the context of healthcare values and therefore can represent best evidence-based practice despite a lack of high-quality research evidence [41]. Conditional recommendations are considered to apply to most patients, but significant consideration must be given to local healthcare system factors and individual patient conditions and values when implementing these recommendations. Clinicians should consider a range of factors when selecting CPG recommendations for implementation in the local context. Tools such as the Practice Guidelines Evaluation and Adaptation Cycle and the Appraisal of Guidelines Research and Evaluation II (AGREE II) Instrument can be used to identify and select recommendations of high quality and relevance to the local patient cohort and clinical practice environment [42, 43]. Preference may also be given to a CPG based on the needs of the guideline user, for example, the development of a business case compared to a local practice guideline or staff education programme. The resources provided by each guideline are summarised in Fig. 2.1.

Implementation resources provided by existing clinical practice guidelines
In addition to the resources provided by recent clinical practice guidelines , a broad range of published resources are available to support delivery of early mobilisation. These include Hanekom and colleagues [44] algorithms for patient and intervention selection, Hodgson et al. [13] expert consensus on a safety screening traffic light system and the practical guide with mobility planning pneumonic and progression chart by Green et al. [45]. Additionally, many authors have provided early mobility protocols [12, 46, 47]. However, the key limitation to translation of these guidelines and resources into daily practice is the lack of consideration given to the development of strategies to maximise applicability and provision of processes which support staff to implement the recommendations and resources locally in a sustained manner.
Existing studies investigating EM interventions in daily practice via implementation science and quality improvement projects provide important insights into which knowledge translation approaches are effective. A recent review of quality improvement studies implementing early mobilisation of mechanically ventilated patients demonstrated four key themes which related to successful outcomes: managing the change process through strong leadership, designing strategies and interventions to overcome barriers to implementation, multidisciplinary team collaboration and data collection and feedback systems [48]. Other successful strategies identified in the literature include the implementation of early mobilisation interventions within a multifaceted approach such as care bundles to minimise other barriers such as sedation and delirium [49, 50]. Studies demonstrating programmes which can be effectively translated to other institutions and sustain improvements have been based on a structured quality improvement process known as the strategy for translating evidence to practice [51,52,53,54]. Key components of this approach include local barriers analysis, development of targeted strategies to overcome these including a variety of educational and executional methods and repeated performance measurement. The final overarching theme of implementation studies is the provision of adequate resourcing of the programme via staffing and equipment, the timing of introducing this resourcing was variable between projects with some introducing additional staffing to support initial implementation, whilst other utilised positive initial results to motivate redirection of resources for sustainability of the programme. The results of these multicomponent structured quality improvement projects are in contrast to studies investigating single component interventions to improve compliance with early mobilisation which have not shown a positive effect [55]. Figure 2.2 describes the key components clinicians should utilise when developing a local EM research translation approach.

Key components to a successful EM implementation programme
Together with the resources described above, several tools are also available to support the development of these components including:
-
Patient Mobilisation Attitudes & Beliefs Survey—Intensive Care Unit (PMABS) [56].
-
Core Outcome Measures for Acute Respiratory Failure Survivors [57].
-
Under development: Physical Rehabilitation Core Outcomes in Critical Illness (PRACTICE) [58].
-
The Surgical Intensive Care Unit Optimal Mobility Score (SOMS) [59].
-
The ICU Mobility Scale [60].
-
The ICU Liberation Resources [61].
How Will Early Mobilisation Be Delivered in the Future?
New ideas and concepts are being developed and discussed for intensive care, including living ICUs, where the historical technological focus of medicine will be complemented by a patient- and family-centred care approach. Focusing on the future of EM, three key domains are expected to play a major role: regulation, personnel resources and technology and biomedical development.
Currently, EM is recommended by some medical societies [8, 38, 39], is part of quality indicators for intensive care in some countries [62] and is one part of the ICU liberation strategy using the ABCDEF bundle [63]. The results of the TEAM RCT (https://www.teamtrial.org.au, NCT03133377), investigating early active mobilisation in ventilated patients using a published algorithm, will have a major impact on the future directions for EM. If the TEAM RCT provides evidence of a positive effect on mortality or days alive and out of hospital within 180 days, it is likely that in addition to patient advocacy groups, regulatory entities will step in and mandate a protocolised active EM regime. To provide such active and protocolised care, it will be necessary to provide far more resources than that are currently available for EM. Most developed countries already struggle with physical therapy and nursing staffing. A possible solution might be to reduce the number of healthcare providers necessary to mobilise a patient safely. Mobilisation typically needs at least two people; with technology, such as robotic assistance, this might be reduced. For example, tilt tables have been modified to be connected to a robotic mobilisation system [64] so that a critically ill patient stays in a (special) bed that can be attached to and used by a robotic mobilisation system. Since the patient is not transferred out of the bed, there is potential for the system to allow one person to complete mobilisation treatments alone. Even then, the system is still limited by the required personnel resources, such as time to set up the system, and the patients’ low exercise capacity. Therefore, we should aim to develop systems which require only a single application and can be automatically and repeatedly activated. This could support the neuromuscular system of the patient whilst accounting for the individual training capacity and regeneration phases necessary without further staff supervision of the intervention. Imagine a futuristic advanced exoskeleton or just a suit in contact with the skin with sensors and stimulation capacities.
Besides such technological advances, in the patient- and family-centred ICU, patients would ideally be liberated from sedation to maximise their participation in care and decision-making [38]. They would have the opportunity to be surrounded by their regular social environment, such as family members, to support their psychological well-being and the (self-)healing process. The social construct could be a motivator and allow family to act as therapists by providing EM to the patient. This process already has started locally in some locations, where family members are encouraged to be part of mobilisation sessions, support therapy or provide passive mobilisation to their loved ones.
How Will Early Mobilisation Be Prescribed in the Future?
Independent of the TEAM RCT results, more questions must be answered to guide clinicians prescribing EM interventions in the future to achieve the greatest impact on patient- and service-centred outcomes and to maximise the efficiency of resource use. Firstly, what is the optimal dose of EM? We have seen that the dose of EM may influence the outcome of our patients following a stroke and the resources needed are dose-dependent [65]. There is an ongoing international collaboration preparing a study to answer this question. Secondly, do patients who have been functionally dependent before the hospital admission benefit from EM in a similar way? Are the pathomechanisms in this cohort the same? Is the goal of EM for such patients to prevent further functional decline? If yes, is the prevention of a decline possible and what resources are necessary to achieve this? Emerging investigation into measures, such as frailty, which allow stratification of cohorts may assist in the identification of responders and nonresponders to interventions such as EM. Finally, what is the impact of staff expertise on the delivery and outcomes of EM interventions? To date, most EM trials have utilised highly experienced staff for delivery of EM treatments. As intervention uptake increases and spreads to centres with minimal exposure to this complex intervention, it will be important to consider the impact of confidence and training on outcomes.
In summary, the coming years will be exciting for EM of critically ill patients. Ideally, the future will hold a clearer perspective for clinicians with the availability of selection criteria for the most appropriate patient cohort. Algorithms need to be developed to identify dosage, monitoring and stopping criteria based on clear evidence from trials. Key areas for improvement include improved follow-up and an understanding of both the dose–response relationship to EM and the expertise needed to successfully deliver these programmes. This will benefit critically ill cohorts around the globe.
References
Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, Zawistowski C, Bemis-Dougherty A, Berney SC, Bienvenu OJ, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012;40:502–9.
Team Study Investigators, Hodgson C, Bellomo R, Berney S, Bailey M, Buhr H, Denehy L, Harrold M, Higgins A, Presneill J, et al. Early mobilization and recovery in mechanically ventilated patients in the ICU: a bi-national, multi-centre, prospective cohort study. Crit Care. 2015;19:81.
Hermans G, Van Mechelen H, Clerckx B, Vanhullebusch T, Mesotten D, Wilmer A, Casaer MP, Meersseman P, Debaveye Y, Van Cromphaut S, et al. Acute outcomes and 1-year mortality of intensive care unit-acquired weakness. A cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2014;190:410–20.
Herridge MS. Legacy of intensive care unit-acquired weakness. Crit Care Med. 2009;37:S457–61.
Fan E, Dowdy DW, Colantuoni E, Mendez-Tellez PA, Sevransky JE, Shanholtz C, Himmelfarb CR, Desai SV, Ciesla N, Herridge MS, et al. Physical complications in acute lung injury survivors: a two-year longitudinal prospective study. Crit Care Med. 2014;42:849–59.
Clarissa C, Salisbury L, Rodgers S, Kean S. Early mobilisation in mechanically ventilated patients: a systematic integrative review of definitions and activities. J Intensive Care. 2019;7:3.
Amidei C. Mobilisation in critical care: a concept analysis. Intensive Crit Care Nurs. 2012;28:73–81.
Devlin JW, Skrobik Y, Gelinas C, Needham DM, Slooter AJC, Pandharipande PP, Watson PL, Weinhouse GL, Nunnally ME, Rochwerg B, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46:e825–73.
Reid JC, Unger J, McCaskell D, Childerhose L, Zorko DJ, Kho ME. Physical rehabilitation interventions in the intensive care unit: a scoping review of 117 studies. J Intensive Care. 2018;6:80.
Hodgson CL, Tipping CJ. Physiotherapy management of intensive care unit-acquired weakness. J Physiother. 2017;63:4–10.
Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373:1874–82.
Schaller SJ, Anstey M, Blobner M, Edrich T, Grabitz SD, Gradwohl-Matis I, Heim M, Houle T, Kurth T, Latronico N, et al. Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016;388:1377–88.
Hodgson CL, Stiller K, Needham DM, Tipping CJ, Harrold M, Baldwin CE, Bradley S, Berney S, Caruana LR, Elliott D, et al. Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Crit Care. 2014;18:658.
Sommers J, Engelbert RH, Dettling-Ihnenfeldt D, Gosselink R, Spronk PE, Nollet F, van der Schaaf M. Physiotherapy in the intensive care unit: an evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin Rehabil. 2015;29:1051–63.
Parry SM, Berney S, Granger CL, Koopman R, El-Ansary D, Denehy L. Electrical muscle stimulation in the intensive care setting: a systematic review. Crit Care Med. 2013;41:2406–18.
Zayed Y, Kheiri B, Barbarawi M, Chahine A, Rashdan L, Chintalapati S, Bachuwa G, Al-Sanouri I. Effects of neuromuscular electrical stimulation in critically ill patients: a systematic review and meta-analysis of randomised controlled trials. Aust Crit Care. 2019;50:280.
Fossat G, Baudin F, Courtes L, Bobet S, Dupont A, Bretagnol A, Benzekri-Lefevre D, Kamel T, Muller G, Bercault N, et al. Effect of in-bed leg cycling and electrical stimulation of the quadriceps on global muscle strength in critically ill adults: a randomized clinical trial. JAMA. 2018;320:368–78.
Eggmann S, Verra ML, Luder G, Takala J, Jakob SM. Effects of early, combined endurance and resistance training in mechanically ventilated, critically ill patients: a randomised controlled trial. PLoS One. 2018;13:e0207428.
Kho ME, Molloy AJ, Clarke FJ, Reid JC, Herridge MS, Karachi T, Rochwerg B, Fox-Robichaud AE, Seely AJ, Mathur S, et al. Multicentre pilot randomised clinical trial of early in-bed cycle ergometry with ventilated patients. BMJ Open Respir Res. 2019;6:e000383.
McCaskell DS, Molloy AJ, Childerhose L, Costigan FA, Reid JC, McCaughan M, Clarke F, Cook DJ, Rudkowski JC, Farley C, et al. Project management lessons learned from the multicentre CYCLE pilot randomized controlled trial. Trials. 2019;20:532.
Tipping CJ, Harrold M, Holland A, Romero L, Nisbet T, Hodgson CL. The effects of active mobilisation and rehabilitation in ICU on mortality and function: a systematic review. Intensive Care Med. 2017;43:171–83.
Zang K, Chen B, Wang M, Chen D, Hui L, Guo S, Ji T, Shang F. The effect of early mobilization in critically ill patients: a meta-analysis. Nurs Crit Care. 2019.
Ding N, Zhang Z, Zhang C, Yao L, Yang L, Jiang B, Wu Y, Jiang L, Tian J. What is the optimum time for initiation of early mobilization in mechanically ventilated patients? A network meta-analysis. PLoS One. 2019;14:e0223151.
Taito S, Yamauchi K, Tsujimoto Y, Banno M, Tsujimoto H, Kataoka Y. Does enhanced physical rehabilitation following intensive care unit discharge improve outcomes in patients who received mechanical ventilation? A systematic review and meta-analysis. BMJ Open. 2019;9:e026075.
Nydahl P, Sricharoenchai T, Chandra S, Kundt FS, Huang M, Fischill M, Needham DM. Safety of patient mobilization and rehabilitation in the intensive care unit. Systematic review with meta-analysis. Ann Am Thorac Soc. 2017;14:766–77.
Parry SM, Knight LD, Connolly B, Baldwin C, Puthucheary Z, Morris P, Mortimore J, Hart N, Denehy L, Granger CL. Factors influencing physical activity and rehabilitation in survivors of critical illness: a systematic review of quantitative and qualitative studies. Intensive Care Med. 2017;43:531–42.
Corner EJ, Murray EJ, Brett SJ. Qualitative, grounded theory exploration of patients’ experience of early mobilisation, rehabilitation and recovery after critical illness. BMJ Open. 2019;9:e026348.
Berry AB, Bennett, J.; Chaseling, W.; Cross, Y.; Cushway, S.; Hassan, A.; Jones, S.; Longhurst, E.; Moore, R.; Phillips, D.; Plowman, E.; Scott, J.; Smith, K.; Thomas, L.; Elliott, D. Physical activity and movement: a guideline for critically lll adults. (Government AfCIN ed. 2017).
Wollersheim T, Grunow JJ, Carbon NM, Haas K, Malleike J, Ramme SF, Schneider J, Spies CD, Mardian S, Mai K, et al. Muscle wasting and function after muscle activation and early protocol-based physiotherapy: an explorative trial. J Cachexia Sarcopenia Muscle. 2019;10:734–47.
Grunow JJ, Goll M, Carbon NM, Liebl ME, Weber-Carstens S, Wollersheim T. Differential contractile response of critically ill patients to neuromuscular electrical stimulation. Crit Care. 2019;23:308.
Fuke R, Hifumi T, Kondo Y, Hatakeyama J, Takei T, Yamakawa K, Inoue S, Nishida O. Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: a systematic review and meta-analysis. BMJ Open. 2018;8:e019998.
Doiron KA, Hoffmann TC, Beller EM. Early intervention (mobilization or active exercise) for critically ill adults in the intensive care unit. Cochrane Database Syst Rev. 2018;3:CD010754.
Kahn JM, Rubenfeld GD. Translating evidence into practice in the intensive care unit: the need for a systems-based approach. J Crit Care. 2005;20:204–6.
Pronovost PJ, Murphy DJ, Needham DM. The science of translating research into practice in intensive care. Am J Respir Crit Care Med. 2010;182:1463–4.
Jolley SE, Moss M, Needham DM, Caldwell E, Morris PE, Miller RR, Ringwood N, Anders M, Koo KK, Gundel SE, et al. Point prevalence study of mobilization practices for acute respiratory failure patients in the United States. Crit Care Med. 2017;45:205–15.
Nydahl P, Ruhl AP, Bartoszek G, Dubb R, Filipovic S, Flohr HJ, Kaltwasser A, Mende H, Rothaug O, Schuchhardt D, et al. Early mobilization of mechanically ventilated patients: a 1-day point-prevalence study in Germany. Crit Care Med. 2014;42:1178–86.
Sibilla A, Nydahl P, Greco N, Mungo G, Ott N, Unger I, Rezek S, Gemperle S, Needham DM, Kudchadkar SR. Mobilization of mechanically ventilated patients in Switzerland. J Intensive Care Med. 2017;35(1):55–62. https://doi.org/10.1177/0885066617728486.
Girard TD, Alhazzani W, Kress JP, Ouellette DR, Schmidt GA, Truwit JD, Burns SM, Epstein SK, Esteban A, Fan E, et al. An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation protocols, ventilator liberation protocols, and cuff leak tests. Am J Respir Crit Care Med. 2017;195:120–33.
Bein T, Bischoff M, Bruckner U, Gebhardt K, Henzler D, Hermes C, Lewandowski K, Max M, Nothacker M, Staudinger T, et al. S2e guideline: positioning and early mobilisation in prophylaxis or therapy of pulmonary disorders : Revision 2015: S2e guideline of the German Society of Anaesthesiology and Intensive Care Medicine (DGAI). Anaesthesist. 2015;64 Suppl 1:1–26.
The GRADE Working Group: GRADE handbook for grading quality of evidence and strength of recommendations. Schunemann HB, J.; Guyatt, G.; Oxman, A.; ed. Available from guidelinedevelopment.org/handbook. 2013.
Djulbegovic B, Guyatt G. Evidence vs consensus in clinical practice guidelines. JAMA. 2019;322:725.
AGREE Next Steps Consortium: The AGREE II instrument user manual. 2009.
Graham ID, Harrison MB. Evaluation and adaptation of clinical practice guidelines. Evid Based Nurs. 2005;8:68–72.
Hanekom S, Gosselink R, Dean E, van Aswegen H, Roos R, Ambrosino N, Louw Q. The development of a clinical management algorithm for early physical activity and mobilization of critically ill patients: synthesis of evidence and expert opinion and its translation into practice. Clin Rehabil. 2011;25:771–87.
Green M, Marzano V, Leditschke IA, Mitchell I, Bissett B. Mobilization of intensive care patients: a multidisciplinary practical guide for clinicians. J Multidiscip Healthc. 2016;9:247–56.
Morris PE, Goad A, Thompson C, Taylor K, Harry B, Passmore L, Ross A, Anderson L, Baker S, Sanchez M, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure*. Crit Care Med. 2008;36:2238–43.
Hodgson CL, Bailey M, Bellomo R, Berney S, Buhr H, Denehy L, Gabbe B, Harrold M, Higgins A, Iwashyna TJ, et al. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU*. Crit Care Med. 2016;44:1145–52.
Phelan S, Lin F, Mitchell M, Chaboyer W. Implementing early mobilisation in the intensive care unit: an integrative review. Int J Nurs Stud. 2018;77:91–105.
Balas MC, Burke WJ, Gannon D, Cohen MZ, Colburn L, Bevil C, Franz D, Olsen KM, Ely EW, Vasilevskis EE. Implementing the awakening and breathing coordination, delirium monitoring/management, and early exercise/mobility bundle into everyday care: opportunities, challenges, and lessons learned for implementing the ICU Pain, Agitation, and Delirium Guidelines. Crit Care Med. 2013;41:S116–27.
Bassett R, Adams KM, Danesh V, Groat PM, Haugen A, Kiewel A, Small C, Van-Leuven M, Venus S, Ely EW. Rethinking critical care: decreasing sedation, increasing delirium monitoring, and increasing patient mobility. Jt Comm J Qual Patient Saf. 2015;41:62–74.
Needham DM, Korupolu R, Zanni JM, Pradhan P, Colantuoni E, Palmer JB, Brower RG, Fan E. Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project. Arch Phys Med Rehabil. 2010;91:536–42.
McWilliams D, Snelson C, Goddard H, Attwood B. Introducing early and structured rehabilitation in critical care: a quality improvement project. Intensive Crit Care Nurs. 2019;53:79–83.
McWilliams D, Weblin J, Atkins G, Bion J, Williams J, Elliott C, Whitehouse T, Snelson C. Enhancing rehabilitation of mechanically ventilated patients in the intensive care unit: a quality improvement project. J Crit Care. 2015;30:13–8.
Pronovost PJ, Berenholtz SM, Needham DM. Translating evidence into practice: a model for large scale knowledge translation. BMJ. 2008;337:a1714.
Capell EL, Tipping CJ, Hodgson CL. Barriers to implementing expert safety recommendations for early mobilisation in intensive care unit during mechanical ventilation: a prospective observational study. Aust Crit Care. 2019;32:185–90.
Goodson CM, Friedman LA, Mantheiy E, Heckle K, Lavezza A, Toonstra A, Parker AM, Seltzer J, Velaetis M, Glover M, et al. Perceived barriers to mobility in a medical ICU: the patient mobilization attitudes & beliefs survey for the ICU. J Intensive Care Med. 2018;35(10):1026–31.
Needham DM, Sepulveda KA, Dinglas VD, Chessare CM, Friedman LA, Bingham CO 3rd, Turnbull AE. Core outcome measures for clinical research in acute respiratory failure survivors. An International Modified Delphi Consensus Study. Am J Respir Crit Care Med. 2017;196:1122–30.
Connolly B, Denehy L, Hart N, Pattison N, Williamson P, Blackwood B. Physical Rehabilitation Core Outcomes In Critical illness (PRACTICE): protocol for development of a core outcome set. Trials. 2018;19:294.
Schaller SJ, Stauble CG, Suemasa M, Heim M, Duarte IM, Mensch O, Bogdanski R, Lewald H, Eikermann M, Blobner M. The German validation study of the surgical intensive care unit optimal mobility score. J Crit Care. 2016;32:201–6.
Hodgson C, Needham D, Haines K, Bailey M, Ward A, Harrold M, Young P, Zanni J, Buhr H, Higgins A, et al. Feasibility and inter-rater reliability of the ICU Mobility Scale. Heart Lung. 2014;43:19–24.
ICU Liberation Resources. https://www.sccm.org/ICULiberation/ResourceCategory?categoryid=119.
Kumpf O, Braun JP, Brinkmann A, Bause H, Bellgardt M, Bloos F, Dubb R, Greim C, Kaltwasser A, Marx G, et al. Quality indicators in intensive care medicine for Germany – third edition 2017. Ger Med Sci. 2017;15:Doc10.
Ely EW. The ABCDEF bundle: science and philosophy of how ICU liberation serves patients and families. Crit Care Med. 2017;45:321–30.
Kuznetsov AN, Rybalko NV, Daminov VD, Luft AR. Early poststroke rehabilitation using a robotic tilt-table stepper and functional electrical stimulation. Stroke Res Treat. 2013;2013:946056.
Bernhardt J, Churilov L, Ellery F, Collier J, Chamberlain J, Langhorne P, Lindley RI, Moodie M, Dewey H, Thrift AG, et al. Prespecified dose-response analysis for A Very Early Rehabilitation Trial (AVERT). Neurology. 2016;86:2138–45.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Lang, J.K., Schaller, S.J., Hodgson, C.L. (2021). Implementing Early Mobilisation in the Intensive Care Unit. In: Haines, K.J., McPeake, J., Sevin, C.M. (eds) Improving Critical Care Survivorship. Springer, Cham. https://doi.org/10.1007/978-3-030-68680-2_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-68680-2_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-68679-6
Online ISBN: 978-3-030-68680-2
eBook Packages: MedicineMedicine (R0)